


Role of Nutrition in Pediatric Patients with Cancer
 , ,
, ,  ,
, 

Abstract
1. Introduction
2. Pathogenesis of Malnutrition in Childhood Cancer
3. Methods to Analyze Nutritional Status in Children with Cancer
4. Prevalence of Undernutrition in Different Cancer Types
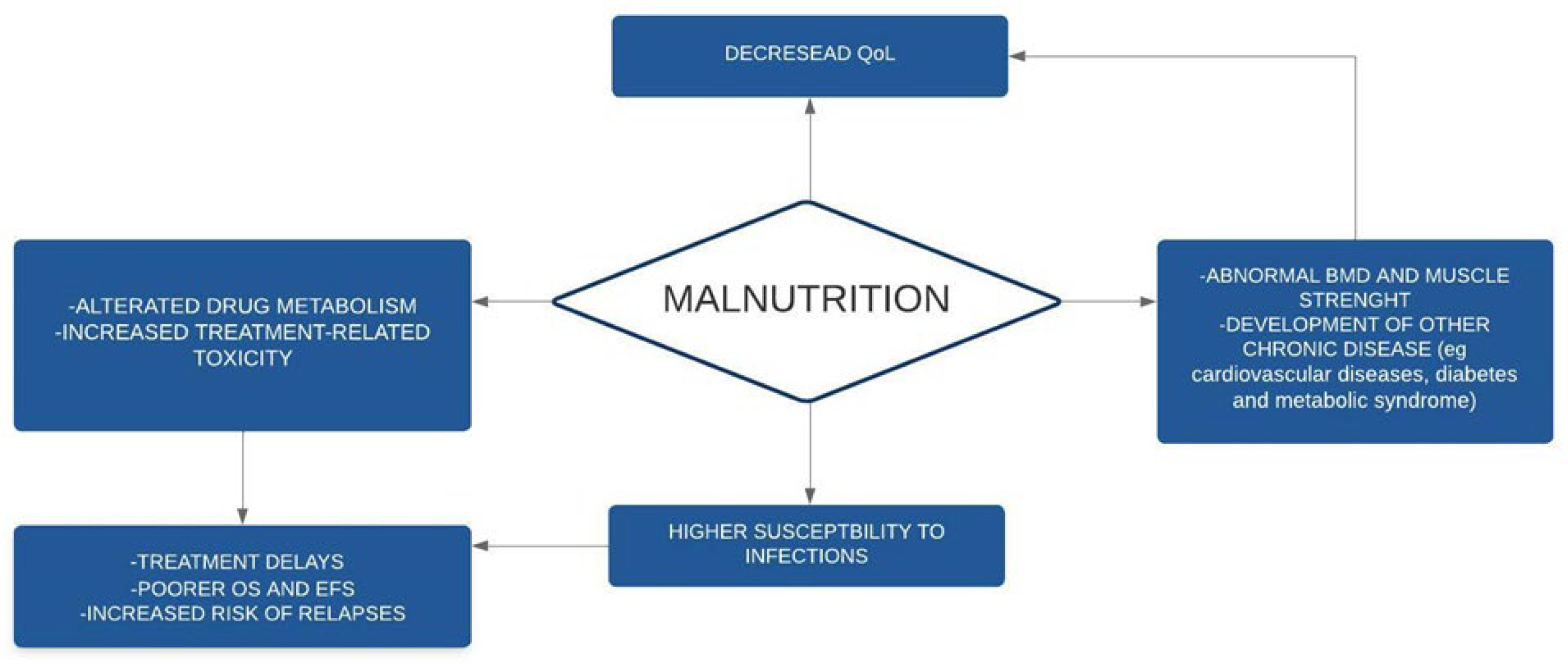
5. Consequences of Undernutrition in Children with Cancer
5.1. Effect of Nutrition on Drug Pharmacokinetics
5.2. Impact on Survival Rate
5.3. Undernutrition and Infections
5.4. Impact on the Psychological Sphere and QoL and Other Long-Term Consequences of Malnutrition
6. Targeting Undernutrition
7. Nutrition and Gut Microbiome
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Diakatou, V.; Vassilakou, T. Nutritional Status of Pediatric Cancer Patients at Diagnosis and Correlations with Treatment, Clinical Outcome and the Long-Term Growth and Health of Survivors. Children 2020, 7, 218. [Google Scholar] [CrossRef]
- WHO. Double Burder of Malnutrition. Available online: www.who.int/nutrition/double-burden-malnutriotion/en/ (accessed on 1 July 2022).
- WHO. Malnutrition in Children. Available online: https://www.who.int/data/nutrition/nlis/info/malnutrition-in-children/ (accessed on 1 July 2022).
- WHO. BMI-for-Age (5–19 Years). Available online: https://www.who.int/tools/growth-reference-data-for-5to19-years/indicators/bmi-for-age/ (accessed on 1 July 2022).
- Henry, M.; Sung, L. Supportive care in pediatric oncology: Oncologic emergencies and management of fever and neutropenia. Pediatr. Clin. 2015, 62, 27–46. [Google Scholar]
- Albano, E.A.; Odom, L.F. Supportive care in pediatric oncology. Curr. Opin. Pediatr. 1993, 5, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Joffe, L.; Ladas, E.J. Nutrition during childhood cancer treatment: Current understanding and a path for future research. Lancet Child Adolesc. Health 2020, 4, 465–475. [Google Scholar] [CrossRef] [PubMed]
- Sala, A.; Pencharz, P.; Barr, R.D. Children, cancer, and nutrition—A dynamic triangle in review. Cancer 2004, 100, 677–687. [Google Scholar] [CrossRef]
- Viani, K.; Barr, R.D.; Odone Filho, V.; Ladas, E.J. Nutritional status at diagnosis among children with cancer referred to a nutritional service in Brazil. Hematol. Transfus. Cell Ther. 2021, 43, 389–395. [Google Scholar] [CrossRef]
- Barr, R.D.; Stevens, M.C. The influence of nutrition on clinical outcomes in children with cancer. Pediatr. Blood Cancer 2020, 67, e28117. [Google Scholar] [CrossRef]
- Hansen, B.A.; Wendelbo, Ø.; Bruserud, Ø.; Hemsing, A.L.; Mosevoll, K.A.; Reikvam, H. Febrile Neutropenia in Acute Leukemia. Epidemiology, Etiology, Pathophysiology and Treatment. Mediterr. J. Hematol. Infect. Dis. 2020, 12, 1. [Google Scholar] [CrossRef] [PubMed]
- Grimes, A.; Mohamed, A.; Sopfe, J.; Hill, R.; Lynch, J. Hyperglycemia during childhood cancer therapy: Incidence, implications, and impact on outcomes. JNCI Monogr. 2019, 2019, 132–138. [Google Scholar] [CrossRef]
- Dare, J.M.; Moppett, J.P.; Shield, J.P.; Hunt, L.P.; Stevens, M.C. The impact of hyperglycemia on risk of infection and early death during induction therapy for acute lymphoblastic leukemia (ALL). Pediatr. Blood Cancer 2013, 60, E157–E159. [Google Scholar] [CrossRef]
- McCormick, M.C.; Sharp, E.; Kalpatthi, R.; Zullo, J.; Gurtunca, N.; Zhang, J.; Krafty, R.; Raman, S. Hyperglycemia requiring insulin during acute lymphoblastic leukemia induction chemotherapy is associated with increased adverse outcomes and healthcare costs. Pediatr. Blood Cancer 2020, 67, e28475. [Google Scholar] [CrossRef] [PubMed]
- Tripodi, S.I.; Bergami, E.; Panigari, A.; Caissutti, V.; Brovia, C.; De Cicco, M.; Cereda, E.; Caccialanza, R.; Zecca, M. The role of nutrition in children with cancer. Tumori J. 2022, 03008916221084740. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.; Jürgens, H.; Frühwald, M.C. Important aspects of nutrition in children with cancer. Adv. Nutr. 2011, 2, 67–77. [Google Scholar] [CrossRef] [PubMed]
- Santarpia, L.; Contaldo, F.; Pasanisi, F. Nutritional screening and early treatment of malnutrition in cancer patients. J. Cachexia Sarcopenia Muscle 2011, 2, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Triarico, S.; Rinninella, E.; Cintoni, M.; Capozza, M.A.; Mastrangelo, S.; Mele, M.C.; Ruggiero, A. Impact of malnutrition on survival and infections among pediatric patients with cancer: A retrospective study. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 1165–1175. [Google Scholar] [PubMed]
- Co-Reyes, E.; Li, R.; Huh, W.; Chandra, J. Malnutrition and obesity in pediatric oncology patients: Causes, consequences, and interventions. Pediatr. Blood Cancer 2012, 59, 1160–1167. [Google Scholar] [CrossRef]
- Lalla, R.V.; Sonis, S.T.; Peterson, D.E. Management of oral mucositis in patients who have cancer. Dent. Clin. N. Am. 2008, 52, 61–77. [Google Scholar] [CrossRef] [PubMed]
- Kuiken, N.S.; Rings, E.H.; van den Heuvel-Eibrink, M.M.; Van De Wetering, M.D.; Tissing, W.J. Feeding strategies in pediatric cancer patients with gastrointestinal mucositis: A multicenter prospective observational study and international survey. Support. Care Cancer 2017, 25, 3075–3083. [Google Scholar] [CrossRef] [PubMed]
- Raber, M.; Wu, J.; Donnella, H.; Knouse, P.; Pise, M.; Munsell, M.; Liu, D.; Chandra, J. Cellular oxidative stress in pediatric leukemia and lymphoma patients undergoing treatment is associated with protein consumption. Nutrients 2019, 12, 75. [Google Scholar] [CrossRef]
- Den Broeder, E.; Oeseburg, B.; Lippens, R.J.J.; Van Staveren, W.A.; Sengers, R.C.A.; van’t Hof, M.A.; Tolboom, J.J.M. Basal metabolic rate in children with a solid tumour. Eur. J. Clin. Nutr. 2001, 55, 673–681. [Google Scholar] [CrossRef]
- Schmid, I.; Schmitt, M.; Streiter, M.; Meilbeck, R.; Haas, R.J.; Stachel, D.K. Effects of soluble TNF receptor II (sTNF-RII), IL-1 receptor antagonist (IL-1 ra), tumor load and hypermetabolism on malnutrition in children with acute leukemia. Eur. J. Med. Res. 2005, 10, 457. [Google Scholar]
- Bond, S.A.; Han, A.M.; Wootton, S.A.; Kohler, J.A. Energy intake and basal metabolic rate during maintenance chemotherapy. Arch. Dis. Child. 1992, 67, 229–232. [Google Scholar] [CrossRef] [PubMed]
- Knox, L.S.; Crosby, L.O.; Feurer, I.D.; Buzby, G.P.; Miller, C.L.; Mullen, J.L. Energy expenditure in malnourished cancer patients. Ann. Surg. 1983, 197, 152. [Google Scholar] [CrossRef] [PubMed]
- Vatner, R.E.; Niemierko, A.; Misra, M.; Weyman, E.A.; Goebel, C.P.; Ebb, D.H.; Jones, R.M.; Huang, M.S.; Mahajan, A.; Grosshans, D.R. Endocrine deficiency as a function of radiation dose to the hypothalamus and pituitary in pediatric and young adult patients with brain tumors. J. Clin. Oncol. 2018, 36, 2854. [Google Scholar] [CrossRef] [PubMed]
- Ross, J.A.; Oeffinger, K.C.; Davies, S.M.; Mertens, A.C.; Langer, E.K.; Kiffmeyer, W.R.; Sklar, C.A.; Stovall, M.; Yasui, Y.; Robison, L.L. Genetic variation in the leptin receptor gene and obesity in survivors of childhood acute lymphoblastic leukemia: A report from the Childhood Cancer Survivor Study. J. Clin. Oncol. 2004, 22, 3558–3562. [Google Scholar] [CrossRef]
- Fabozzi, F.; Trovato, C.M.; Diamanti, A.; Mastronuzzi, A.; Zecca, M.; Tripodi, S.I.; Masetti, R.; Leardini, D.; Muratore, E.; Barat, V. Management of Nutritional Needs in Pediatric Oncology: A Consensus Statement. Cancers 2022, 14, 3378. [Google Scholar] [CrossRef]
- Pizzo, P.A.; Poplack, D.G. Principles and Practice of Pediatric Oncology; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2015. [Google Scholar]
- Viani, K.; Trehan, A.; Manzoli, B.; Schoeman, J. Assessment of nutritional status in children with cancer: A narrative review. Pediatr. Blood Cancer 2020, 67, e28211. [Google Scholar] [CrossRef]
- Ladas, E.J.; Arora, B.; Howard, S.C.; Rogers, P.C.; Mosby, T.T.; Barr, R.D. A framework for adapted nutritional therapy for children with cancer in low-and middle-income countries: A report from the SIOP PODC Nutrition Working Group. Pediatr. Blood Cancer 2016, 63, 1339–1348. [Google Scholar] [CrossRef]
- Joffe, L.; Schadler, K.L.; Shen, W.; Ladas, E.J. Body composition in pediatric solid tumors: State of the science and future directions. JNCI Monogr. 2019, 2019, 144–148. [Google Scholar] [CrossRef]
- Goodenough, C.G.; Partin, R.E.; Ness, K.K. Skeletal muscle and childhood cancer: Where are we now and where we go from here. Aging Cancer 2021, 2, 13–35. [Google Scholar] [CrossRef]
- Pencharz, P.B. Assessment of protein nutritional status in children. Pediatr. Blood Cancer 2008, 50, 445–446. [Google Scholar] [CrossRef] [PubMed]
- Ladas, E.J.; Sacks, N.; Meacham, L.; Henry, D.; Enriquez, L.; Lowry, G.; Hawkes, R.; Dadd, G.; Rogers, P. A multidisciplinary review of nutrition considerations in the pediatric oncology population: A perspective from children’s oncology group. Nutr. Clin. Pract. 2005, 20, 377–393. [Google Scholar] [CrossRef] [PubMed]
- Yaprak, D.S.; Yalçın, B.; Pınar, A.A.; Büyükpamukçu, M. Assessment of nutritional status in children with cancer: Significance of arm anthropometry and serum visceral proteins. Pediatr. Blood Cancer 2021, 68, e28752. [Google Scholar] [CrossRef] [PubMed]
- Keller, U. Nutritional laboratory markers in malnutrition. J. Clin. Med. 2019, 8, 775. [Google Scholar] [CrossRef]
- Huysentruyt, K.; Alliet, P.; Muyshont, L.; Rossignol, R.; Devreker, T.; Bontems, P.; Dejonckheere, J.; Vandenplas, Y.; De Schepper, J. The STRONGkids nutritional screening tool in hospitalized children: A validation study. Nutrition 2013, 29, 1356–1361. [Google Scholar] [CrossRef]
- de la Torre, M.J.V.; Stein, K.; Garibay, E.M.V.; Ichikawa, M.R.K.; Sanromán, R.T.; Salcedo-Flores, A.G.; Sánchez-Zubieta, F.A. Patient-Generated Subjective Global Assessment of nutritional status in pediatric patients with recent cancer diagnosis. Nutr. Hosp. 2017, 34, 1050–1058. [Google Scholar]
- Aarnivala, H.; Pokka, T.; Soininen, R.; Möttönen, M.; Harila-Saari, A.; Niinimäki, R. Trends in age-and sex-adjusted body mass index and the prevalence of malnutrition in children with cancer over 42 months after diagnosis: A single-center cohort study. Eur. J. Pediatr. 2020, 179, 91–98. [Google Scholar] [CrossRef]
- Brinksma, A.; Huizinga, G.; Sulkers, E.; Kamps, W.; Roodbol, P.; Tissing, W. Malnutrition in childhood cancer patients: A review on its prevalence and possible causes. Crit. Rev. Oncol./Hematol. 2012, 83, 249–275. [Google Scholar] [CrossRef]
- Reilly, J.J.; Weir, J.; McColl, J.H.; Gibson, B.E. Prevalence of protein-energy malnutrition at diagnosis in children with acute lymphoblastic leukemia. J. Pediatr. Gastroenterol. Nutr. 1999, 29, 194–197. [Google Scholar] [CrossRef]
- Lange, B.J.; Gerbing, R.B.; Feusner, J.; Skolnik, J.; Sacks, N.; Smith, F.O.; Alonzo, T.A. Mortality in overweight and underweight children with acute myeloid leukemia. JAMA 2005, 293, 203–211. [Google Scholar] [CrossRef]
- Green, G.J.; Weitzman, S.S.; Pencharz, P.B. Resting energy expenditure in children newly diagnosed with stage IV neuroblastoma. Pediatr. Res. 2008, 63, 332–336. [Google Scholar] [CrossRef] [PubMed]
- Bakish, J.; Hargrave, D.; Tariq, N.; Laperriere, N.; Rutka, J.T.; Bouffet, E. Evaluation of dietetic intervention in children with medulloblastoma or supratentorial primitive neuroectodermal tumors. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2003, 98, 1014–1020. [Google Scholar] [CrossRef] [PubMed]
- Orgel, E.; Genkinger, J.M.; Aggarwal, D.; Sung, L.; Nieder, M.; Ladas, E.J. Association of body mass index and survival in pediatric leukemia: A meta-analysis. Am. J. Clin. Nutr. 2016, 103, 808–817. [Google Scholar] [CrossRef]
- Orgel, E.; Mueske, N.M.; Sposto, R.; Gilsanz, V.; Freyer, D.R.; Mittelman, S.D. Limitations of body mass index to assess body composition due to sarcopenic obesity during leukemia therapy. Leuk. Lymphoma 2018, 59, 138–145. [Google Scholar] [CrossRef]
- Orgel, E.; Sposto, R.; Malvar, J.; Seibel, N.L.; Ladas, E.; Gaynon, P.S.; Freyer, D.R. Impact on survival and toxicity by duration of weight extremes during treatment for pediatric acute lymphoblastic leukemia: A report from the Children’s Oncology Group. J. Clin. Oncol. 2014, 32, 1331. [Google Scholar] [CrossRef] [PubMed]
- Amankwah, E.K.; Saenz, A.M.; Hale, G.A.; Brown, P.A. Association between body mass index at diagnosis and pediatric leukemia mortality and relapse: A systematic review and meta-analysis. Leuk. Lymphoma 2016, 57, 1140–1148. [Google Scholar] [CrossRef]
- Joffe, L.; Dwyer, S.; Bender, J.L.G.; Frazier, A.L.; Ladas, E.J. Nutritional status and clinical outcomes in pediatric patients with solid tumors: A systematic review of the literature. In Seminars in Oncology; Elsevier: Amsterdam, The Netherlands, 2019; pp. 48–56. [Google Scholar]
- Loeffen, E.A.; Brinksma, A.; Miedema, K.G.; De Bock, G.H.; Tissing, W.J. Clinical implications of malnutrition in childhood cancer patients—Infections and mortality. Support. Care Cancer 2015, 23, 143–150. [Google Scholar] [CrossRef]
- Barr, R.D.; Gomez-Almaguer, D.; Jaime-Perez, J.C.; Ruiz-Argüelles, G.J. Importance of Nutrition in the Treatment of Leukemia in Children and Adolescents. Arch. Med. Res. 2016, 47, 585–592. [Google Scholar] [CrossRef]
- Iniesta, R.R.; Paciarotti, I.; Brougham, M.F.; McKenzie, J.M.; Wilson, D.C. Effects of pediatric cancer and its treatment on nutritional status: A systematic review. Nutr. Rev. 2015, 73, 276–295. [Google Scholar] [CrossRef]
- Iniesta, R.R.; Paciarotti, I.; Davidson, I.; McKenzie, J.M.; Brougham, M.F.; Wilson, D.C. Nutritional status of children and adolescents with cancer in Scotland: A prospective cohort study. Clin. Nutr. 2019, 32, 96–106. [Google Scholar]
- Swartz, M.C.; Allen, K.; Deer, R.R.; Lyons, E.J.; Swartz, M.D.; Clifford, T. A narrative review on the potential of red beetroot as an adjuvant strategy to counter fatigue in children with cancer. Nutrients 2019, 11, 3003. [Google Scholar] [CrossRef]
- Brinksma, A.; Roodbol, P.F.; Sulkers, E.; Kamps, W.A.; de Bont, E.S.; Boot, A.M.; Burgerhof, J.G.; Tamminga, R.Y.; Tissing, W.J. Changes in nutritional status in childhood cancer patients: A prospective cohort study. Clin. Nutr. 2015, 34, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Barg, E.; Połubok, J.; Hetman, M.; Gonera, A.; Jasielska, O.; Sęga-Pondel, D.; Galant, K.; Kazanowska, B. Metabolic Disturbances in Children Treated for Solid Tumors. Nutrients 2019, 11, 3062. [Google Scholar] [CrossRef] [PubMed]
- Bis, G.; Szlasa, W.; Sondaj, K.; Zendran, I.; Mielcarek-Siedziuk, M.; Barg, E. Lipid complications after hematopoietic stem cell transplantation (HSCT) in pediatric patients. Nutrients 2020, 12, 2500. [Google Scholar] [CrossRef] [PubMed]
- Belle, F.N.; Schindera, C.; Guessous, I.; Beck Popovic, M.; Ansari, M.; Kuehni, C.E.; Bochud, M. Sodium and potassium intakes and cardiovascular risk profiles in childhood cancer survivors: The sccss-nutrition study. Nutrients 2019, 12, 57. [Google Scholar] [CrossRef]
- Zhang, F.F.; Rodday, A.M.; Kelly, M.J.; Must, A.; MacPherson, C.; Roberts, S.B.; Saltzman, E.; Parsons, S.K. Predictors of being overweight or obese in survivors of pediatric acute lymphoblastic leukemia (ALL). Pediatr. Blood Cancer 2014, 61, 1263–1269. [Google Scholar] [CrossRef]
- Muscaritoli, M.; Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Hütterer, E.; Isenring, E.; Kaasa, S. ESPEN practical guideline: Clinical Nutrition in cancer. Clin. Nutr. 2021, 40, 2898–2913. [Google Scholar] [CrossRef]
- Bendelsmith, C.R.; Linabery, A.M.; Nickel, A.J.; Laquere, R.M.; Ingram, K.M.; Hansen, M.B.; Pape-Blabolil, J.A.; Skrypek, M.M.; Bendel, A.E. Effects of proactive and rescue enteral tube feedings on weight change in children undergoing treatment for high-grade CNS tumors. Neuro-Oncol. Pract. 2020, 7, 428–438. [Google Scholar] [CrossRef]
- Zama, D.; Muratore, E.; Biagi, E.; Forchielli, M.L.; Rondelli, R.; Candela, M.; Prete, A.; Pession, A.; Masetti, R. Enteral nutrition protects children undergoing allogeneic hematopoietic stem cell transplantation from blood stream infections. Nutr. J. 2020, 19, 29. [Google Scholar] [CrossRef]
- Zama, D.; Gori, D.; Muratore, E.; Leardini, D.; Rallo, F.; Turroni, S.; Prete, A.; Brigidi, P.; Pession, A.; Masetti, R. Enteral versus parenteral nutrition as nutritional support after allogeneic hematopoietic stem cell transplantation: A systematic review and meta-analysis. Transplant. Cell. Ther. 2021, 27, 180.e1–180.e8. [Google Scholar] [CrossRef]
- Iebba, V.; Totino, V.; Gagliardi, A.; Santangelo, F.; Cacciotti, F.; Trancassini, M.; Mancini, C.; Cicerone, C.; Corazziari, E.; Pantanella, F. Eubiosis and dysbiosis: The two sides of the microbiota. New Microbiol. 2016, 39, 1–12. [Google Scholar] [PubMed]
- Weiss, G.A.; Hennet, T. Mechanisms and consequences of intestinal dysbiosis. Cell. Mol. Life Sci. 2017, 74, 2959–2977. [Google Scholar] [CrossRef] [PubMed]
- Bai, J.; Behera, M.; Bruner, D.W. The gut microbiome, symptoms, and targeted interventions in children with cancer: A systematic review. Support. Care Cancer 2018, 26, 427–439. [Google Scholar] [CrossRef] [PubMed]
- Masetti, R.; Muratore, E.; Leardini, D.; Zama, D.; Turroni, S.; Brigidi, P.; Esposito, S.; Pession, A. Gut microbiome in pediatric acute leukemia: From predisposition to cure. Blood Adv. 2021, 5, 4619–4629. [Google Scholar] [CrossRef] [PubMed]
- Rajagopala, S.V.; Yooseph, S.; Harkins, D.M.; Moncera, K.J.; Zabokrtsky, K.B.; Torralba, M.G.; Tovchigrechko, A.; Highlander, S.K.; Pieper, R.; Sender, L. Gastrointestinal microbial populations can distinguish pediatric and adolescent Acute Lymphoblastic Leukemia (ALL) at the time of disease diagnosis. BMC Genom. 2016, 17, 635. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, C.; Spiro, A.; Ahern, R.; Emery, P.W. Oral nutritional interventions in malnourished patients with cancer: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2012, 104, 371–385. [Google Scholar] [CrossRef]
- Klement, R.J.; Pazienza, V. Impact of different types of diet on gut microbiota profiles and cancer prevention and treatment. Medicina 2019, 55, 84. [Google Scholar] [CrossRef]
- Masetti, R.; Zama, D.; Leardini, D.; Muratore, E.; Turroni, S.; Brigidi, P.; Pession, A. Microbiome-derived metabolites in allogeneic hematopoietic stem cell transplantation. Int. J. Mol. Sci. 2021, 22, 1197. [Google Scholar] [CrossRef]
- Podpeskar, A.; Crazzolara, R.; Kropshofer, G.; Hetzer, B.; Meister, B.; Müller, T.; Salvador, C. Omega-3 Fatty Acids and Their Role in Pediatric Cancer. Nutrients 2021, 13, 1800. [Google Scholar] [CrossRef]
- D’Amico, F.; Biagi, E.; Rampelli, S.; Fiori, J.; Zama, D.; Soverini, M.; Barone, M.; Leardini, D.; Muratore, E.; Prete, A. Enteral nutrition in pediatric patients undergoing hematopoietic SCT promotes the recovery of gut microbiome homeostasis. Nutrients 2019, 11, 2958. [Google Scholar] [CrossRef]
- Moody, K.M.; Baker, R.A.; Santizo, R.O.; Olmez, I.; Spies, J.M.; Buthmann, A.; Granowetter, L.; Dulman, R.Y.; Ayyanar, K.; Gill, J.B. A randomized trial of the effectiveness of the neutropenic diet versus food safety guidelines on infection rate in pediatric oncology patients. Pediatr. Blood Cancer 2018, 65, e26711. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Gupta, A.K.; Meena, J.P.; Khan, M.A.; Agarwala, A.; Seth, R. A Pilot Randomised Controlled Trial Examining the Benefit of a Neutropenic Diet for Children Undergoing Cancer Treatment. Nutr. Cancer 2022, 74, 2930–2936. [Google Scholar] [CrossRef]
- Maia, J.E.; da Cruz, L.B.; Gregianin, L.J. Microbiological profile and nutritional quality of a regular diet compared to a neutropenic diet in a pediatric oncology unit. Pediatr. Blood Cancer 2018, 65, e26828. [Google Scholar] [CrossRef] [PubMed]
- Braun, L.E.; Chen, H.; Frangoul, H. Significant inconsistency among pediatric oncologists in the use of the neutropenic diet. Pediatr. Blood Cancer 2014, 61, 1806–1810. [Google Scholar] [CrossRef] [PubMed]
- Sonbol, M.B.; Firwana, B.; Diab, M.; Zarzour, A.; Witzig, T.E. The effect of a neutropenic diet on infection and mortality rates in cancer patients: A meta-analysis. Nutr. Cancer 2015, 67, 1232–1240. [Google Scholar] [CrossRef]
- Muratore, E.; Leardini, D.; Baccelli, F.; Venturelli, F.; Prete, A.; Masetti, R. Nutritional modulation of the gut microbiome in allogeneic hematopoietic stem cell transplantation recipients. Front. Nutr. 2022, 9, 993668. [Google Scholar] [CrossRef]
- Zama, D.; Bossù, G.; Leardini, D.; Muratore, E.; Biagi, E.; Prete, A.; Pession, A.; Masetti, R. Insights into the role of intestinal microbiota in hematopoietic stem-cell transplantation. Ther. Adv. Hematol. 2020, 11, 2040620719896961. [Google Scholar] [CrossRef]
- Iddrisu, I.; Monteagudo-Mera, A.; Poveda, C.; Pyle, S.; Shahzad, M.; Andrews, S.; Walton, G.E. Malnutrition and gut microbiota in children. Nutrients 2021, 13, 2727. [Google Scholar] [CrossRef]
- Prasad, M.; Tandon, S.; Gala, R.; Kannan, S.; Chinnaswamy, G.; Narula, G.; Vora, T.; Banavali, S.; Mehta, S.; Paradkar, A. Efficacy of ready-to-use therapeutic food in malnourished children with cancer: Results of a randomized, open-label phase 3 trial. Pediatr. Blood Cancer 2021, 68, e29197. [Google Scholar] [CrossRef]
- Schoonees, A.; Lombard, M.J.; Musekiwa, A.; Nel, E.; Volmink, J. Ready-to-use therapeutic food (RUTF) for home-based nutritional rehabilitation of severe acute malnutrition in children from six months to five years of age. Cochrane Database Syst. Rev. 2019, 5, CD009000. [Google Scholar] [CrossRef]
- Wada, M.; Nagata, S.; Saito, M.; Shimizu, T.; Yamashiro, Y.; Matsuki, T.; Asahara, T.; Nomoto, K. Effects of the enteral administration of Bifidobacterium breve on patients undergoing chemotherapy for pediatric malignancies. Support. Care Cancer 2010, 18, 751–759. [Google Scholar] [CrossRef] [PubMed]
- Zheng, S.; Steenhout, P.; Kuiran, D.; Qihong, W.; Weiping, W.; Hager, C.; Haschke, F.; Clemens, R.A. Nutritional support of pediatric patients with cancer consuming an enteral formula with fructooligosaccharides. Nutr. Res. 2006, 26, 154–162. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Undernutrition | Acute undernutrition or wasting: WFH < −2 SD |
| Chronic undernutrition or stunting: HFA < −2 SD | |
| Overweight | <5 years: WFH > +2 SD |
| 5–19 years: BMI-for-age > +1 SD | |
| Obesity | <5 years: WFH > +3 SD |
| 5–19 years: BMI-for-age > +2 SD |
| Treatment Required | Proposal |
|---|---|
| Intensive treatment or high risk of undernutrition | Every 3–4 weeks |
| Less intensive treatment | Every 3 months Every 6–12 months during maintenance |
| Children admitted to ICU | More frequent reassessments |
| Nutritional Risk | Proposal |
|---|---|
| No nutritional risks | First year: every 6 months After first year: annually |
| Presence of nutritional risk (i.e., inadequate eating habits, sedentary lifestyle, hypertriglyceridemia, high cholesterol levels) or well-nourished | First year: every 3 months Second to fifth year: every 6 months From fifth year onward: annually |
| Undernourished | Monthly assessment until normal nutrition status |
| Obese | Every 3 months |
| Assessment | Advantages | Disadvantages | |
|---|---|---|---|
| Anthropometric measures [8,16,33] | BMI, MUAC, TSFT, waist circumference, head circumference | Easily obtained | Measurement error and variability BMI may be altered in presence of oedema or of abdominal tumor mass |
| BIA | Rapid, easy, inexpensive, no radiation exposure | No precision with oscillating hydration status and in chronically ill patients Standardization of execution required | |
| DXA | Accurate, less expensive than CT and MRI | Exposure to radiation albeit to a lesser extent than CT. It does not distinguish visceral from subcutaneous fat. | |
| CT | Accurate Lean body mass, subcutaneous fat, and visceral fat can be directly assessed | Exposure to radiation Expensive | |
| MRI | Accurate, no radiation exposure Lean body mass, subcutaneous fat, and visceral fat can be directly assessed | Expensive, longer image acquisition time | |
| Biochemistry exams [7,8,29] | Liver and renal function test Lipid and glucose panel Serum protein concentration (prealbumin, albumin, RBP, transferrin) Micronutrients (B vitamins, vitamin D, calcium, zinc etc.) | Easily obtained (except for more specific laboratory exams, e.g., RBP dosage) | Influence of tumor itself or treatments More specific laboratory exams are not available in all centres |
| Clinical evaluation [31] | Muscle wasting Subcutaneous fat loss or excess Skin and hair changes Recent weight variation Presence of oedema Mucous membrane dryness Evidence of vitamin and mineral deficiencies Side-effect of cancer treatment affecting oral food intake | Easily obtained | Need for careful clinical examination and periodic re-evaluation |
| Dietary intake [36] | Intake of macro- and micro-nutrients Food aversions and preference Allergies or intolerances Current eating patterns Changes in physical activity level Family behavior and food hygiene at home | Allows dietary recommendations to be adapted to the patient’s needs and requirements | Need for expert personnel, such as dietitians or clinical nutritionists with expertise in this area, not available in all centers Need for periodic evaluation |
| Type of Tumor | Average Prevalence of Undernutrition |
|---|---|
| Leukemia | 5–10% Undernutrition ALL 7% Overnutrition ALL 2.9% Undernutrition AML 10.9% Overnutrition AML 14.9% |
| Neuroblastoma | 20–50% |
| Solid tumors | 34.3% |
| Brain tumors | 31% Overnutrition 42.6% Obesity 40.4% |
| Other tumors | 30% |
| References | Dietary Compound | Outcomes |
|---|---|---|
| Klement et al. [72] | Mediterranean diet | It decreases inflammatory signaling, producing SCFA that positively influences cancer prevention and treatment |
| Gupta et al. [77] Maia et al. [78] | Neutropenic diet | It does not bring benefits and does not contain a bacterial load lower than a normal diet |
| Barr et al. [53] Rajagopala et al. [70] Iddrisu et al. [83] Prasad et al. [84] | RUTFs | They can modulate the GM, restoring eubiosis, have a significant role in correcting an unbalanced microbiota, improving the NS of the patients, and can guarantee greater weight gain, improve body composition, and decrease episodes of FN |
| Bai et al. [68] Masetti et al. [69] | Probiotics | They can influence the prophylaxis of infections in cancer patients, but more safety data are needed regarding probiotics, especially due to the lack of knowledge about the risk of infections in giving live microorganisms to immunocompromised children |
| Zheng et al. [87] | FOS | They stimulate the synthesis of IgA, increasing the production of mucins, modulating inflammatory cytokines, which leads to a decrease in the inflammatory state and a positive physical growth |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pedretti, L.; Massa, S.; Leardini, D.; Muratore, E.; Rahman, S.; Pession, A.; Esposito, S.; Masetti, R. Role of Nutrition in Pediatric Patients with Cancer. Nutrients 2023, 15, 710. https://doi.org/10.3390/nu15030710
Pedretti L, Massa S, Leardini D, Muratore E, Rahman S, Pession A, Esposito S, Masetti R. Role of Nutrition in Pediatric Patients with Cancer. Nutrients. 2023; 15(3):710. https://doi.org/10.3390/nu15030710
Chicago/Turabian StylePedretti, Laura, Serena Massa, Davide Leardini, Edoardo Muratore, Sofia Rahman, Andrea Pession, Susanna Esposito, and Riccardo Masetti. 2023. "Role of Nutrition in Pediatric Patients with Cancer" Nutrients 15, no. 3: 710. https://doi.org/10.3390/nu15030710
APA StylePedretti, L., Massa, S., Leardini, D., Muratore, E., Rahman, S., Pession, A., Esposito, S., & Masetti, R. (2023). Role of Nutrition in Pediatric Patients with Cancer. Nutrients, 15(3), 710. https://doi.org/10.3390/nu15030710