
Urinary Hydration Biomarkers and Water Sources in Older Adults with Neurocognitive Disorder
 , , ,
, , ,  , ,
, ,
Abstract

1. Introduction
2. Materials and Methods
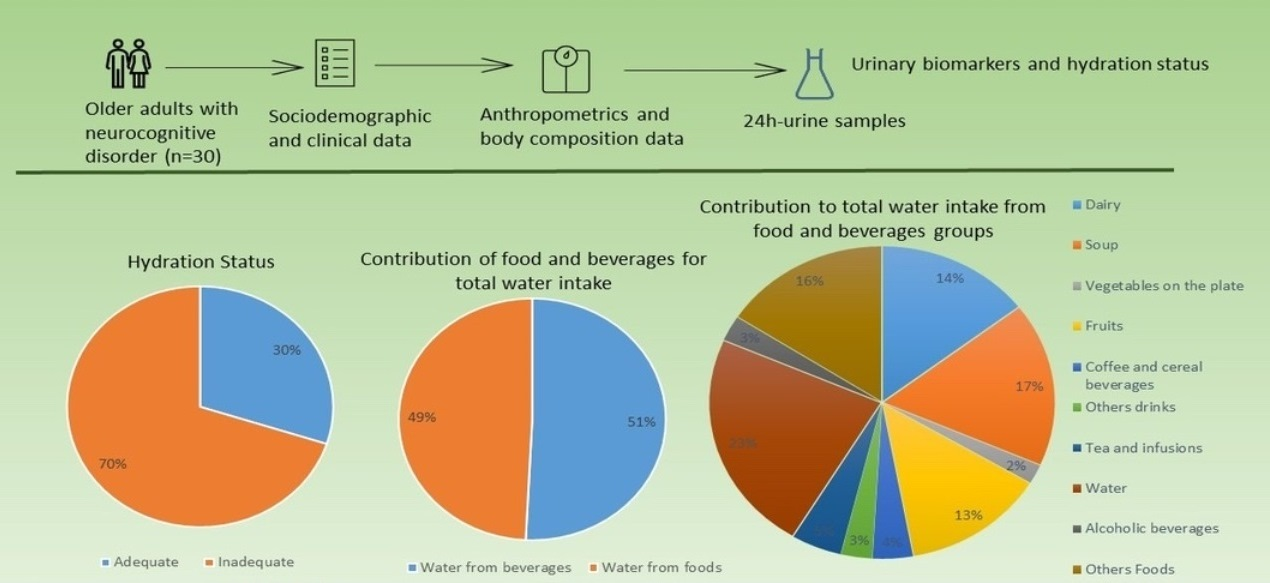
2.1. Population and Study Design
2.2. Sociodemographic and Clinical Data
2.3. Urinary Biomarkers and Hydration Status
2.4. Anthropometrics Data and Body Composition
2.5. Instrumental Activities of Daily Living
2.6. Physical Activity
2.7. Quality of Life
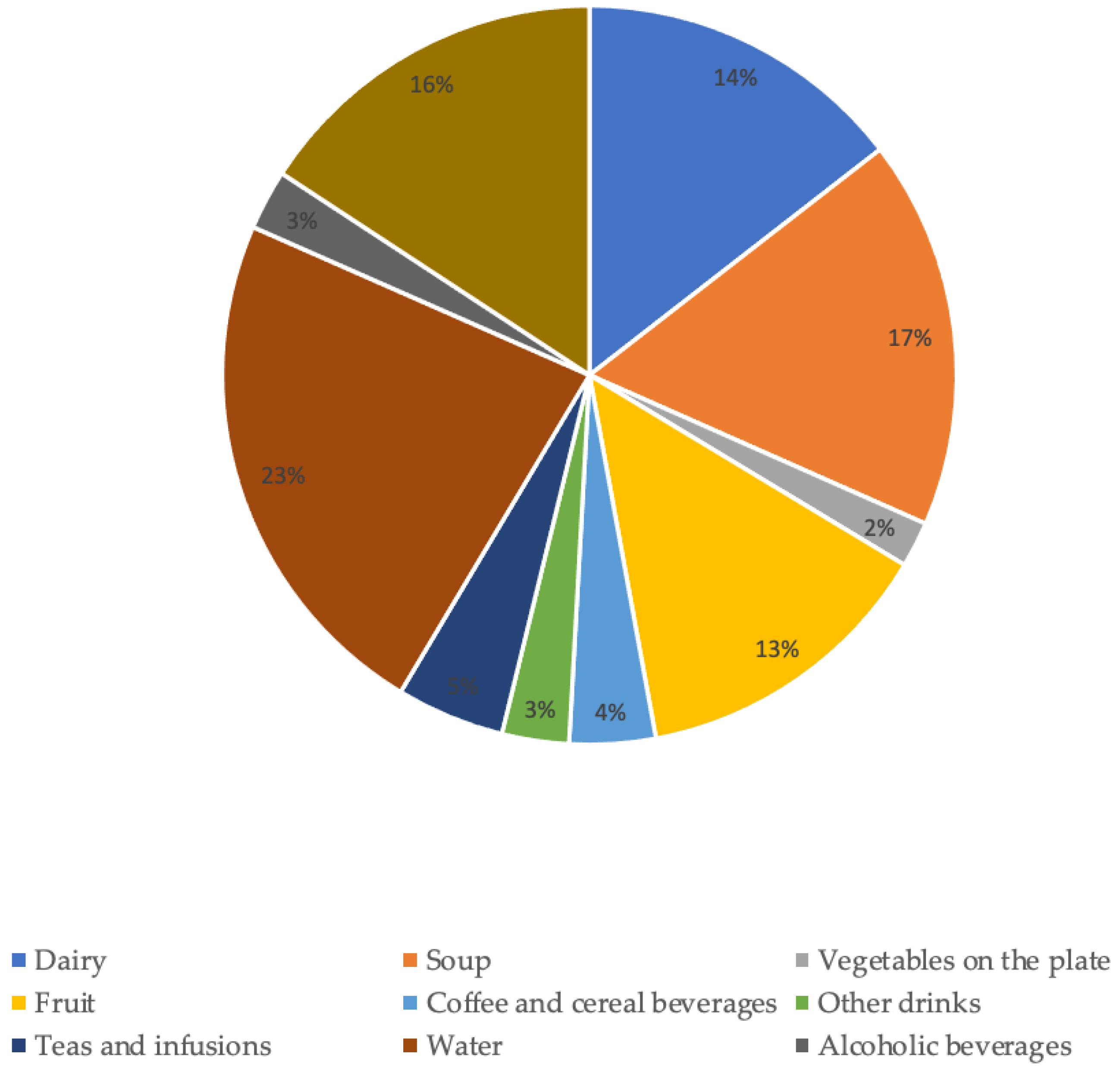
2.8. Contribution of Food and Beverages to Total Water Intake
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Characteristics of the Participants | Severity of Major NCD, n (%) | ||||
|---|---|---|---|---|---|
| Sample | Questionable NCD–Mild NCD | Moderate NCD–Severe NCD | p | ||
| Sex, n (%) | Female | 20 (66.7) | 11 (55%) | 9 (45%) | 1 |
| Age (years), mean (SD) | 76.4 (7.3) | 75.4 (6.4) | 77.5 (8.3) | 0.4 | |
| Education level, n (%) | No formal education | 9 (32.2) | 5 (55.6%) | 4 (44.4%) | 1 |
| Formal education | 19 (67.8) | 11 (57.9%) | 8 (42.1%) | ||
| Marital status, n (%) | Married/civil union | 19 (63.3) | 8 (42.1%) | 11 (57.9%) | 0.1 |
| Single/Widow | 11 (36.7) | 8 (72.7%) | 3 (22.3%) | ||
| Living situation, n (%) | Family member | 23 (76.7) | 10 (43.5%) | 13 (55.6%) | 0.1 |
| Living in residential units/nursing homes | 6 (20) | 5 (83.3%) | 1 (16.7%) | ||
| Alone | 1 (3.3) | 1 (100%) | 0 (0%) | ||
| Aetiological subtypes, n (%) | Mild NCD | 4 (14.8) | n.a | n.a | 0.6 |
| Major NCD due to Alzheimer’s disease | 5 (18.5) | 2 (40%) | 3 (60%) | ||
| Major NCD due to vascular disease | 3 (11.1) | 3 (100%) | 0 (0%) | ||
| Major NCD due to multiple aetiologies | 5 (18.5) | 3 (60%) | 2 (40%) | ||
| Major NCD due to unspecified condition | 9 (33.3) | 5 (55.6%) | 4 (44.4%) | ||
| Major NCD due to substance/medication-induced | 1 (3.7) | 0 (0%) | 1 (100%) | ||
| Number of comorbidities, mean (SD) | 4.0 (2.2) | 4.8 (2.3) | 3 (1.2) | 0.02 | |
| Number of drugs intake, mean (SD) | 8 (3.4) | 8.8 (2.3) | 6.8 (4.5) | 0.1 | |
| Sodium excretion, n (%) | Excessive | 21(70) | 12 (57.1%) | 9 (42.9%) | 0.7 |
| Potassium excretion, n (%) | Insufficient | 29(96.7) | 15 (51.7%) | 14 (48.3%) | 1 |
| Na/K ratio excretion, n (%) | Excessive | 28(93.3) | 15 (53.6%) | 13 (46.4%) | 1 |
| Body mass index, n (%) | Under weight–Normal weight | 6 (20.6) | 3 (50%) | 3 (50%) | 1 |
| Overweight–Obese | 22 (79.4) | 12 (54.5%) | 10 (45.5%) | ||
| Waist circumference, n (%) | No risk | 7 (26) | 2 (28.6%) | 5 (71.4%) | 0.4 |
| Hight risk–Very High risk | 20 (74) | 11 (55%) | 9 (45%) | ||
| Waist-Hip ratio, n (%) | No risk increase | 4 (16.0) | 2 (55%) | 2 (55%) | 1 |
| Substantially increased risk | 21 (84.0) | 11 (52.4%) | 10 (47.6%) | ||
| Fat-free mass %, mean (SD) | 39.26 (6.4) | 39.8 (7.2) | 38.7 (5.7) | 0.6 | |
| Fat mass %, mean (SD) | 39.50 (8) | 39.8 (7.2) | 38.7 (5.6) | 0.8 | |
| Instrumental activities of daily living, n (%) | Independent | 20 (3.4%) | 13 (65%) | 7 (35%) | 0.2 |
| Slightly dependent | 6 (20.7%) | 3 (50%) | 3 (50%) | ||
| Moderately dependent | 2 (6.9%) | 0 (0%) | 2 (100%) | ||
| Severely dependent | 1 (3.4%) | 0 (0%) | 1 (100%) | ||
| Physical activity *, median (P25; P75) | 3.25 (2.5; 4.3) | 2.9 (2.5; 4.2) | 3.5 (2.6; 4.3) | 0.6 | |
| Quality of life, mean (SD) | 30.4 (4.5) | 31.8 (3.7) | 28.6 (4.9) | 0.1 | |
References
- Gonçalves, A.; Silva, J.; Carvalho, J.; Moreira, P.; Padrão, P. Hydration status and water sources in free-living physically active elderly. Nutr. Hosp. 2015, 32, 33. [Google Scholar] [CrossRef]
- Edmonds, C.J.; Foglia, E.; Booth, P.; Fu, C.H.Y.; Gardner, M. Dehydration in older people: A systematic review of the effects of dehydration on health outcomes, healthcare costs and cognitive performance. Arch. Gerontol. Geriatr. 2021, 95, 104380. [Google Scholar] [CrossRef]
- Perrier, E.T.; Buendia-Jimenez, I.; Vecchio, M.; Armstrong, L.E.; Tack, I.; Klein, A. Twenty-four-hour urine osmolality as a physiological index of adequate water intake. Dis. Markers 2015, 2015, 231063. [Google Scholar] [CrossRef] [PubMed]
- Casado, Á.; Ramos, P.; Rodríguez, J.; Moreno, N.; Gil, P. Types and characteristics of drinking water for hydration in the elderly. Crit. Rev. Food Sci. Nutr. 2015, 55, 1633–1641. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.R.; Cote, T.R.; Lawhorne, L.; Levenson, S.A.; Rubenstein, L.Z.; Smith, D.A.; Stefanacci, R.G.; Tangalos, E.G.; Morley, J.E. Understanding clinical dehydration and its treatment. J. Am. Med. Dir. Assoc. 2008, 9, 292–301. [Google Scholar] [CrossRef]
- Jacques, P.F.; Rogers, G.; Stookey, J.D.; Perrier, E.T. Water Intake and Markers of Hydration Are Related to Cardiometabolic Risk Biomarkers in Community-Dwelling Older Adults: A Cross-Sectional Analysis. J. Nutr. 2021, 151, 3205–3213. [Google Scholar] [CrossRef]
- Miller, H.J. Dehydration in the Older Adult. J. Gerontol. Nurs. 2015, 41, 8–13. [Google Scholar] [CrossRef]
- Gamba, M.; Moreira, P.; Borges, N.; Santos, A.; Afonso, C.; Amaral, T.F.; Padrão, P. Are older adults with excessive sodium intake at increased risk of hypohydration? J. Hum. Nutr. Diet. 2021, 34, 834–840. [Google Scholar] [CrossRef]
- Bossingham, M.J.; Carnell, N.S.; Campbell, W.W. Water balance, hydration status, and fat-free mass hydration in younger and older adults. Am. J. Clin. Nutr. 2005, 81, 1342–1350. [Google Scholar] [CrossRef]
- Perrier, E.; Vergne, S.; Klein, A.; Poupin, M.; Rondeau, P.; Le Bellego, L.; Armstrong, L.E.; Lang, F.; Stookey, J.; Tack, I. Hydration biomarkers in free-living adults with different levels of habitual fluid consumption. Br. J. Nutr. 2013, 109, 1678–1687. [Google Scholar] [CrossRef]
- Godfrey, H.; Cloete, J.; Dymond, E.; Long, A. An exploration of the hydration care of older people: A qualitative study. Int. J. Nurs. Stud. 2012, 49, 1200–1211. [Google Scholar] [CrossRef] [PubMed]
- Puga, A.M.; Partearroyo, T.; Varela-Moreiras, G. Hydration status, drug interactions, and determinants in a Spanish elderly population: A pilot study. J. Physiol. Biochem. 2018, 74, 139–151. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, S.; Silva, J.; Severo, M.; Inácio, C.; Padrão, P.; Lopes, C.; Carvalho, J.; do Carmo, I.; Moreira, P. Validation analysis of a geriatric dehydration screening tool in community-dwelling and institutionalized elderly people. Int. J. Environ. Res. Public Health 2015, 12, 2700–2717. [Google Scholar] [CrossRef] [PubMed]
- Hoen, L.; Pfeffer, D.; Zapf, R.; Raabe, A.; Hildebrand, J.; Kraft, J.; Kalkhof, S. Association of Drug Application and Hydration Status in Elderly Patients. Nutrients 2021, 13, 1929. [Google Scholar] [CrossRef] [PubMed]
- Hodgkinson, B.; Evans, D.; Wood, J. Maintaining oral hydration in older adults: A systematic review. Int. J. Nurs. Pract. 2003, 9, S19–S28. [Google Scholar] [CrossRef]
- Masot, O.; Iglesias Millán, A.; Nuin, C.; Miranda, J.; Lavedán, A.; Botigué, T. How to improve hydration and fluid intake in institutionalized older people? A scientific literature review. Nutr. Hosp. 2018, 35, 1441–1449. [Google Scholar] [CrossRef]
- Moore, K.; Hughes, C.F.; Ward, M.; Hoey, L.; McNulty, H. Diet, nutrition and the ageing brain: Current evidence and new directions. Proc. Nutr. Soc. 2018, 77, 152–163. [Google Scholar] [CrossRef]
- Stephen, R.; Barbera, M.; Peters, R.; Ee, N.; Zheng, L.; Lehtisalo, J.; Kulmala, J.; Håkansson, K.; Chowdhary, N.; Dua, T.; et al. Development of the First WHO Guidelines for Risk Reduction of Cognitive Decline and Dementia: Lessons Learned and Future Directions. Front. Neurol. 2021, 12, 763573. [Google Scholar] [CrossRef]
- Volkert, D.; Chourdakis, M.; Faxen-Irving, G.; Frühwald, T.; Landi, F.; Suominen, M.H.; Vandewoude, M.; Wirth, R.; Schneider, S.M. ESPEN guidelines on nutrition in dementia. Clin. Nutr. 2015, 34, 1052–1073. [Google Scholar] [CrossRef]
- Wang, Z.; Li, N.; Heizhati, M.; Wang, L.; Li, M.; Pan, F.; Yang, Z.; Abudureyimu, R.; Hong, J.; Sun, L.; et al. Association between 24-h urinary sodium to potassium ratio and mild cognitive impairment in community-based general population. Public Health Nutr. 2021, 24, 5795–5804. [Google Scholar] [CrossRef]
- Moreira, P.; Sousa, A.S.; Guerra, R.S.; Santos, A.; Borges, N.; Afonso, C.; Amaral, T.F.; Padrão, P. Sodium and potassium urinary excretion and their ratio in the elderly: Results from the Nutrition UP 65 study. Food Nutr. Res. 2018, 62, 1288. [Google Scholar] [CrossRef] [PubMed]
- Mohan, D.; Yap, K.H.; Reidpath, D.; Soh, Y.C.; McGrattan, A.; Stephan, B.C.M.; Robinson, L.; Chaiyakunapruk, N.; Siervo, M. Link Between Dietary Sodium Intake, Cognitive Function, and Dementia Risk in Middle-Aged and Older Adults: A Systematic Review. J. Alzheimers Dis. 2020, 76, 1347–1373. [Google Scholar] [CrossRef] [PubMed]
- Hooper, L.; Bunn, D.K.; Abdelhamid, A.; Gillings, R.; Jennings, A.; Maas, K.; Millar, S.; Twomlow, E.; Hunter, P.R.; Shepstone, L.; et al. Water-loss (intracellular) dehydration assessed using urinary tests: How well do they work? Diagnostic accuracy in older people. Am. J. Clin. Nutr. 2016, 104, 121–131. [Google Scholar] [CrossRef]
- Volkert, D.; Beck, A.M.; Cederholm, T.; Cruz-Jentoft, A.; Hooper, L.; Kiesswetter, E.; Maggio, M.; Raynaud-Simon, A.; Sieber, C.; Sobotka, L.; et al. ESPEN practical guideline: Clinical nutrition and hydration in geriatrics. Clin. Nutr. 2022, 41, 958–989. [Google Scholar] [CrossRef] [PubMed]
- Baron, S.; Courbebaisse, M.; Lepicard, E.M.; Friedlander, G. Assessment of hydration status in a large population. Br. J. Nutr. 2015, 113, 147–158. [Google Scholar] [CrossRef]
- Jéquier, E.; Constant, F. Water as an essential nutrient: The physiological basis of hydration. Eur. J. Clin. Nutr. 2010, 64, 115–123. [Google Scholar] [CrossRef]
- Lacey, J.; Corbett, J.; Forni, L.; Hooper, L.; Hughes, F.; Minto, G.; Moss, C.; Price, S.; Whyte, G.; Woodcock, T.; et al. A multidisciplinary consensus on dehydration: Definitions, diagnostic methods and clinical implications. Ann. Med. 2019, 51, 232–251. [Google Scholar] [CrossRef]
- Stuver, S.O.; Lyons, J.; Coviello, A.; Fredman, L. Feasibility of 24-Hr Urine Collection for Measurement of Biomarkers in Community-Dwelling Older Adults. J. Appl. Gerontol. 2017, 36, 1393–1408. [Google Scholar] [CrossRef]
- Białecka-Dębek, A.; Pietruszka, B. The association between hydration status and cognitive function among free-living elderly volunteers. Aging Clin. Exp. Res. 2019, 31, 695–703. [Google Scholar] [CrossRef]
- Bunn, D.K.; Abdelhamid, A.; Copley, M.; Cowap, V.; Dickinson, A.; Howe, A.; Killett, A.; Poland, F.; Potter, J.F.; Richardson, K.; et al. Effectiveness of interventions to indirectly support food and drink intake in people with dementia: Eating and Drinking Well IN dementiA (EDWINA) systematic review. BMC Geriatr. 2016, 16, 89. [Google Scholar] [CrossRef]
- Carvalho, J.; Borges-Machado, F.; Barros, D.; Sampaio, A.; Marques-Aleixo, I.; Bohn, L.; Pizarro, A.; Teixeira, L.; Magalhães, J.; Ribeiro, Ó. “Body & Brain”: Effects of a multicomponent exercise intervention on physical and cognitive function of adults with dementia—Study protocol for a quasi-experimental controlled trial. BMC Geriatr. 2021, 21, 156. [Google Scholar] [CrossRef]
- American Psychiatric Association. Neurocognitive disorder. In DSM-5: Diagnostic and Statistical Manueal of Mental Disorders; American Psychiatric Association Publishing: Washington, DC, USA, 2013; Volume 5. [Google Scholar]
- World Health Organization. ICD-10: International Statistical Classification of Diseases and Related Health Problems; WHO: Geneva, Switzerland, 2004. [Google Scholar]
- McKhann, G.; Drachman, D.; Folstein, M.; Katzman, R.; Price, D.; Stadlan, E.M. Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology 1984, 34, 939–944. [Google Scholar] [CrossRef]
- Perneczky, R.; Wagenpfeil, S.; Komossa, K.; Grimmer, T.; Diehl, J.; Kurz, A. Mapping scores onto stages: Mini-mental state examination and clinical dementia rating. Am. J. Geriatr. Psychiatry 2006, 14, 139–144. [Google Scholar] [CrossRef]
- ARUP laboratories. Laboratory Test Directory-Creatinine 24-Hour Urine. Available online: https://ltd.aruplab.com/Tests/Pub/0020473 (accessed on 7 May 2022).
- European Food Safety Authority. Scientific Opinion on Dietary Reference Values for water. EFSA J. 2010, 8, 1459. [Google Scholar] [CrossRef]
- Manz, F.; Wentz, A. 24-h hydration status: Parameters, epidemiology and recommendations. Eur. J. Clin. Nutr. 2003, 57, S10–S18. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guideline: Potassium Intake for Adults and Children; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- World Health Organization. Guideline: Sodium Intake for Adults and Children; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- WHO Consultation on Obesity. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation; WHO: Geneva, Switzerland, 2000; Volume 894, pp. 1–253. [Google Scholar]
- Lean, M.E.; Han, T.S.; Morrison, C.E. Waist circumference as a measure for indicating need for weight management. BMJ 1995, 311, 158–161. [Google Scholar] [CrossRef]
- World Health Organization. Waist Circumference and Waist–Hip Ratio: Report of a WHO Expert Consultation; WHO: Geneva, Switzerland, 2008. [Google Scholar]
- Sequeira, C. Cuidar de Idosos Dependentes; Quarteto Editora: Coimbra, Portugal, 2007. [Google Scholar]
- Almeida, M.C.B.; Ribeiro, J.L.P. Adaptação do Habitual Physical Activity Questionnaire (Baecke), versão modificada, para a população portuguesa. Rev. Enferm. Ref. 2014, IV, 27–36. [Google Scholar] [CrossRef]
- Bárrios, H.; Verdelho, A.; Narciso, S.; Gonçalves-Pereira, M.; Logsdon, R.; de Mendonça, A. Quality of life in patients with cognitive impairment: Validation of the Quality of Life-Alzheimer’s Disease scale in Portugal. Int. Psychogeriatr. 2013, 25, 1085–1096. [Google Scholar] [CrossRef]
- Sauvaget, C.; Yamada, M.; Fujiwara, S.; Sasaki, H.; Mimori, Y. Dementia as a predictor of functional disability: A four-year follow-up study. Gerontology 2002, 48, 226–233. [Google Scholar] [CrossRef]
- Masot, O.; Lavedán, A.; Nuin, C.; Escobar-Bravo, M.A.; Miranda, J.; Botigué, T. Risk factors associated with dehydration in older people living in nursing homes: Scoping review. Int. J. Nurs. Stud. 2018, 82, 90–98. [Google Scholar] [CrossRef]
- Ijaopo, E.O.; Ijaopo, R.O. Tube Feeding in Individuals with Advanced Dementia: A Review of Its Burdens and Perceived Benefits. J. Aging Res. 2019, 2019, 7272067. [Google Scholar] [CrossRef] [PubMed]
- Archibald, C. Promoting hydration in patients with dementia in healthcare settings. Nurs. Stand. 2006, 20, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Bickel, H.; Hendlmeier, I.; Heßler, J.B.; Junge, M.N.; Leonhardt-Achilles, S.; Weber, J.; Schäufele, M. The Prevalence of Dementia and Cognitive Impairment in Hospitals. Dtsch. Arztebl. Int. 2018, 115, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Fogg, C.; Griffiths, P.; Meredith, P.; Bridges, J. Hospital outcomes of older people with cognitive impairment: An integrative review. Int. J. Geriatr. Psychiatry 2018, 33, 1177–1197. [Google Scholar] [CrossRef]
- Basu, I.; Mukhopadhyay, S. Neuropsychiatric symptoms of dementia and caregivers’ burden: A study among Indian caregivers. Dement. Neuropsychol. 2022, 16, 332–340. [Google Scholar] [CrossRef]
- Emmady, P.D.; Schoo, C.; Tadi, P.; Del Pozo, E. Major Neurocognitive Disorder (Dementia) (Nursing). In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Arendts, G.; Chenoweth, L.; Hayes, B.J.; Campbell, E.; Agar, M.; Etherton-Beer, C.; Spilsbury, K.; Howard, K.; Braitberg, G.; Cubitt, M.; et al. CELPI: Trial protocol for a randomised controlled trial of a Carer End of Life Planning Intervention in people dying with dementia. BMC Geriatr. 2022, 22, 869. [Google Scholar] [CrossRef]
- Huijten, D.C.M.; Bolt, S.R.; Meesterberends, E.; Meijers, J.M.M. Nurses’ support needs in providing high-quality palliative care to persons with dementia in the hospital setting: A cross-sectional survey study. J. Nurs. Scholarsh. 2022, in press. [Google Scholar] [CrossRef]
- Faculdade de Ciências da Nutrição e Alimentação da Universidade do Porto. Nutrition UP 65| Nutritional Strategies Facing an Older Demography. 2018. Available online: https://nutritionup65.up.pt/wp-content/uploads/sites/165/2018/10/Relatorio-EN.pdf (accessed on 7 May 2022).
- Malisova, O.; Athanasatou, A.; Pepa, A.; Husemann, M.; Domnik, K.; Braun, H.; Mora-Rodriguez, R.; Ortega, J.F.; Fernandez-Elias, V.E.; Kapsokefalou, M. Water Intake and Hydration Indices in Healthy European Adults: The European Hydration Research Study (EHRS). Nutrients 2016, 8, 204. [Google Scholar] [CrossRef]
- Guelinckx, I.; Tavoularis, G.; König, J.; Morin, C.; Gharbi, H.; Gandy, J. Contribution of Water from Food and Fluids to Total Water Intake: Analysis of a French and UK Population Surveys. Nutrients 2016, 8, 630. [Google Scholar] [CrossRef]
- Jimoh, O.F.; Brown, T.J.; Bunn, D.; Hooper, L. Beverage Intake and Drinking Patterns-Clues to Support Older People Living in Long-Term Care to Drink Well: DRIE and FISE Studies. Nutrients 2019, 11, 447. [Google Scholar] [CrossRef]
- Lopes, C.; Torres, D.; Oliveira, A.; Severo, M.; Alarcão, V.; Guiomar, S.; Mota, J.; Teixeira, P.; Rodrigues, S.; Lobato, L.; et al. Inquérito Alimentar e de Atividade Física, IAN-AF 2015–2016: Relatório de Resultados. 2017. Available online: https://www.ian-af.up.pt (accessed on 13 May 2022).
- Zhang, J.; Ma, G.; Du, S.; Zhang, N. The Relationships between Water Intake and Hydration Biomarkers and the Applications for Assessing Adequate Total Water Intake among Young Adults in Hebei, China. Nutrients 2021, 13, 3805. [Google Scholar] [CrossRef] [PubMed]
- Rosinger, A.Y.; Pontzer, H.; Raichlen, D.A.; Wood, B.M.; Tanner, S.N.; Sands, J.M. Age-related decline in urine concentration may not be universal: Comparative study from the U.S. and two small-scale societies. Am. J. Phys. Anthropol. 2019, 168, 705–716. [Google Scholar] [CrossRef] [PubMed]
- Roigk, P. Nutrition and Hydration. In Fragility Fracture Nursing: Holistic Care and Management of the Orthogeriatric Patient; Hertz, K., Santy-Tomlinson, J., Eds.; Springer: Cham, Switzerland, 2018; pp. 95–107. [Google Scholar]

| Beverage/Food Groups | Food Included |
|---|---|
| Water | Bottled water (with or without gas) and tap water. |
| Teas and infusions | Teas and infusions. |
| Coffee and cereal beverages | Coffee and cereal beverages. |
| Other drinks | Soft drinks (carbonated or non-carbonated), fruit juices, and other commercial beverages with or without sugar or sweetener. |
| Alcoholic beverages | Wine, beer, and spirits. |
| Soup | All Soups of all kinds with vegetables (with or without potatoes). |
| Vegetables | Vegetables (excluding the ones in the soup): raw, cooked, canned, and frozen. |
| Fruits | Fresh fruit. |
| Dairy | Milk and yogurt. |
| Other foods | Meat, fish, eggs, pasta, rice, potatoes (excluding potato soup), pulses, breakfast cereals, cheeses, pastries (cakes, cookies, and jams), sugar and fat added, and gelatin. |
| Characteristics of the Participants | Urinary Osmolality (mOsm/Kg) | ||||
|---|---|---|---|---|---|
| Sample | ≤437.5 | >437.5 | p | ||
| Sex, n (%) | Female | 20 (66.7) | 11 (55.0) | 9 (45.0) | 0.7 |
| Age (years), mean (SD) | 76.4 (7.3) | 78.9 (5.3) | 73.9 (8.2) | 0.06 | |
| Education level, n (%) | No formal education | 9 (32.2) | 6 (66.7) | 3 (33.3) | 0.3 |
| Formal education | 19 (67.8) | 7 (36.8) | 12 (63.2) | ||
| Marital status, n (%) | Married/civil union | 19 (63.3) | 7 (36.8) | 12 (63.2) | 0.1 |
| Single/Widow | 11 (36.7) | 8 (72.7) | 3 (27.3) | ||
| Living situation, n (%) | Family member | 23 (76.7) | 10 (43.5) | 13 (56.5) | 0.4 |
| Living in residential units/nursing homes | 6 (20) | 4 (66.7) | 2 (33.3) | ||
| Alone | 1 (3.3) | 1 (100) | 0 (0) | ||
| Aetiological subtypes, n (%) | Mild NCD | 4 (14.8) | 2 (50) | 2 (50) | 0.9 |
| Major NCD due to Alzheimer’s disease | 5 (18.5) | 2 (40) | 3 (60) | ||
| Major NCD due to vascular disease | 3 (11.1) | 1 (33.3) | 2 (66.7) | ||
| Major NCD due to Multiple aetiologies | 5 (18.5) | 2 (40) | 3 (60) | ||
| Major NCD due to unspecified condition | 9 (33.3) | 6 (66.7) | 3 (33.3) | ||
| NCD due to substance or medication-induced | 1 (3.7) | 0 (0) | 1 (100) | ||
| Number of comorbidities, mean (SD) | 4.0 (2.2) | 4.5 (2.4) | 3.7 (1.9) | 0.3 | |
| Number of drugs intake, mean (SD) | 8 (3.4) | 8.3 (2.8) | 7.7 (4) | 0.6 | |
| Severity of major NCD, n (%) | Questionable NCD–Mild NCD | 16 (53.3) | 8 (50) | 8 (50) | 1 |
| Moderate NCD–Severe NCD | 14 (46.7) | 7 (50) | 7 (50) | ||
| Sodium excretion, n (%) | Excessive | 21(70) | 10 (47.6) | 11 (52.4) | 1 |
| Potassium excretion, n (%) | Insufficient | 29(96.7) | 15 (51.7) | 14 (48.3) | 1 |
| Na/K ratio excretion, n (%) | Excessive | 28(93.3) | 14 (50) | 14 (50) | 1 |
| Body mass index, n (%) | Under weight–Normal weight | 6 (20.6) | 1 (16.7) | 5 (83.3) | 0.2 |
| Overweight–Obese | 22 (79.4) | 13 (59.1) | 9 (11) | ||
| Waist circumference, n (%) | No risk | 7 (26) | 2 (50) | 2 (50) | 1 |
| Hight risk–Very High risk | 20 (74) | 11 (52.4) | 10 (47.6) | ||
| Waist-Hip ratio, n (%) | No risk increase | 4 (16.0) | 2 (28.6) | 5 (71.4) | 0.4 |
| Substantially increased risk | 21 (84.0) | 11 (55.0) | 9 (45.0) | ||
| Fat-free mass %, mean (SD) | 39.26 (6.4) | 40.5 (6.7) | 38 (6.2) | 0.3 | |
| Fat mass %, mean (SD) | 39.50 (8) | 40.9 (8.3) | 38.1 (7.8) | 0.4 | |
| Instrumental activities of daily living, n (%) | Independent | 20 (3.4%) | 8 (53.3%) | 12 (85.7%) | 0.1 |
| Slightly dependent | 6 (20.7%) | 5 (33.3%) | 1 (7.1%) | ||
| Moderately dependent | 2 (6.9%) | 1 (6.7%) | 1 (7.1%) | ||
| Severely dependent | 1 (3.4%) | 1 (6.7%) | 0 (0%) | ||
| Physical activity *, median (P25; P75) | 3.25 (2.5; 4.3) | 3.25 (2.5; 3.6) | 3.13 (2.7; 4.3) | 0.8 | |
| Quality of life, mean (SD) | 30.4 (4.5) | 29.3 (5.2) | 31.5 (3.5) | 0.2 | |
| Contribution of Water from Beverages and Food | Urinary Osmolality (mOsm/Kg) | |||
|---|---|---|---|---|
| ≤437.5 | >437.5 | p | ||
| Water, mean (SD) | % | 24.4 (13.1) | 21.7 (11.7) | 0.6 |
| Soup, mean (SD) | 19.0 (10.5) | 15.4 (11.4) | 0.4 | |
| Others foods, mean (SD) | 15.0 (6.8) | 16.2 (5.4) | 0.8 | |
| Dairy, mean (SD) | 13.7 (10.3) | 15.3 (13.2) | 0.7 | |
| Fruits, mean (SD) | 13.3 (7.5) | 13.7 (10.6) | 0.9 | |
| Teas and infusions *, median (P25, 75) | 0 (0; 11.2) | 0 (0; 11.1) | 0.9 | |
| Coffee and cereal beverages *, median (P25, 75) | 3.8 (0.1; 8.2) | 2.0 (0.1; 5.5) | 0.5 | |
| Alcoholic beverages *, median (P25, 75) | 0 (0; 0) | 0 (0; 5) | 0.2 | |
| Other drinks *, median (P25, 75) | 0 (0; 3.8) | 0 (0; 4.4) | 0.7 | |
| Vegetables on the plate *, median (P25, 75) | 0.5 (0; 2.8) | 2.4 (0.9; 3.7) | 0.1 | |
| Dietary intake | ||||
| Total water intake, mean (SD) | mL | 2076 (950) | 1947 (737) | 0.7 |
| Energy, mean (SD) | Kcal | 1607 (444) | 1806 (568) | 0.3 |
| Protein *, median (P25; P75) | G | 60.8 (45.5; 73.2) | 66.9 (56.2; 86.1) | 0.1 |
| Fat, mean (SD) | 40.4 (14.5) | 46.4 (15.3) | 0.3 | |
| SFA, mean (SD) | 10.4 (5) | 13 (6.9) | 0.3 | |
| Carbohydrates, mean (SD) | 213.1 (65.4) | 252.8 (94.6) | 0.2 | |
| Protein *, median (P25; P75) | %TEI | 15.1 (12.6; 18) | 16.2 (14.4; 18) | 0.3 |
| Fat, mean (SD) | 22.9 (6.2) | 23.6 (5.6) | 0.8 | |
| SFA, mean (SD) | 5.8 (2.3) | 6.6 (3.1) | 0.5 | |
| Carbohydrates, mean (SD) | 52.9 (7.7) | 55.6 (11.4) | 0.5 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Queirós, C.; Machado, F.B.; Barros, D.; Sampaio, J.; Sampaio, A.; Barros, R.; Moreira, P.; Ribeiro, Ó.; Carvalho, J.; Padrão, P. Urinary Hydration Biomarkers and Water Sources in Older Adults with Neurocognitive Disorder. Nutrients 2023, 15, 548. https://doi.org/10.3390/nu15030548
Queirós C, Machado FB, Barros D, Sampaio J, Sampaio A, Barros R, Moreira P, Ribeiro Ó, Carvalho J, Padrão P. Urinary Hydration Biomarkers and Water Sources in Older Adults with Neurocognitive Disorder. Nutrients. 2023; 15(3):548. https://doi.org/10.3390/nu15030548
Chicago/Turabian StyleQueirós, Cátia, Flávia Borges Machado, Duarte Barros, Joana Sampaio, Arnaldina Sampaio, Renata Barros, Pedro Moreira, Óscar Ribeiro, Joana Carvalho, and Patrícia Padrão. 2023. "Urinary Hydration Biomarkers and Water Sources in Older Adults with Neurocognitive Disorder" Nutrients 15, no. 3: 548. https://doi.org/10.3390/nu15030548
APA StyleQueirós, C., Machado, F. B., Barros, D., Sampaio, J., Sampaio, A., Barros, R., Moreira, P., Ribeiro, Ó., Carvalho, J., & Padrão, P. (2023). Urinary Hydration Biomarkers and Water Sources in Older Adults with Neurocognitive Disorder. Nutrients, 15(3), 548. https://doi.org/10.3390/nu15030548