
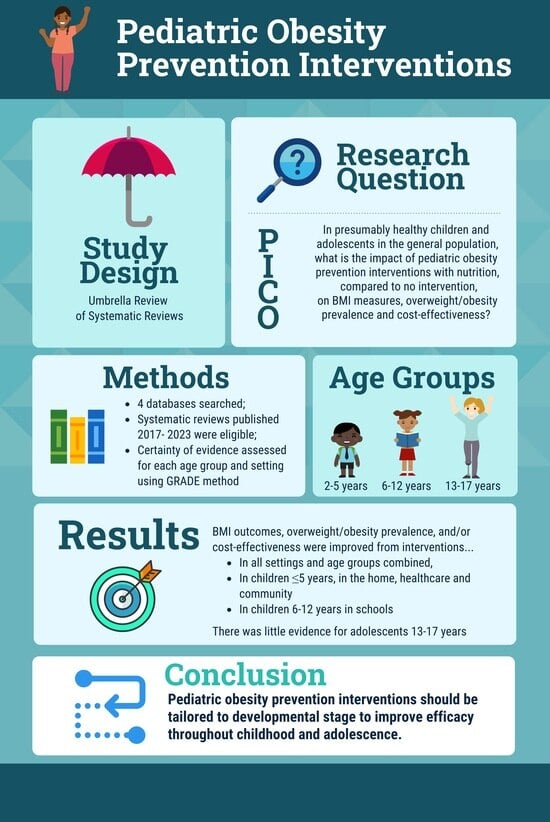
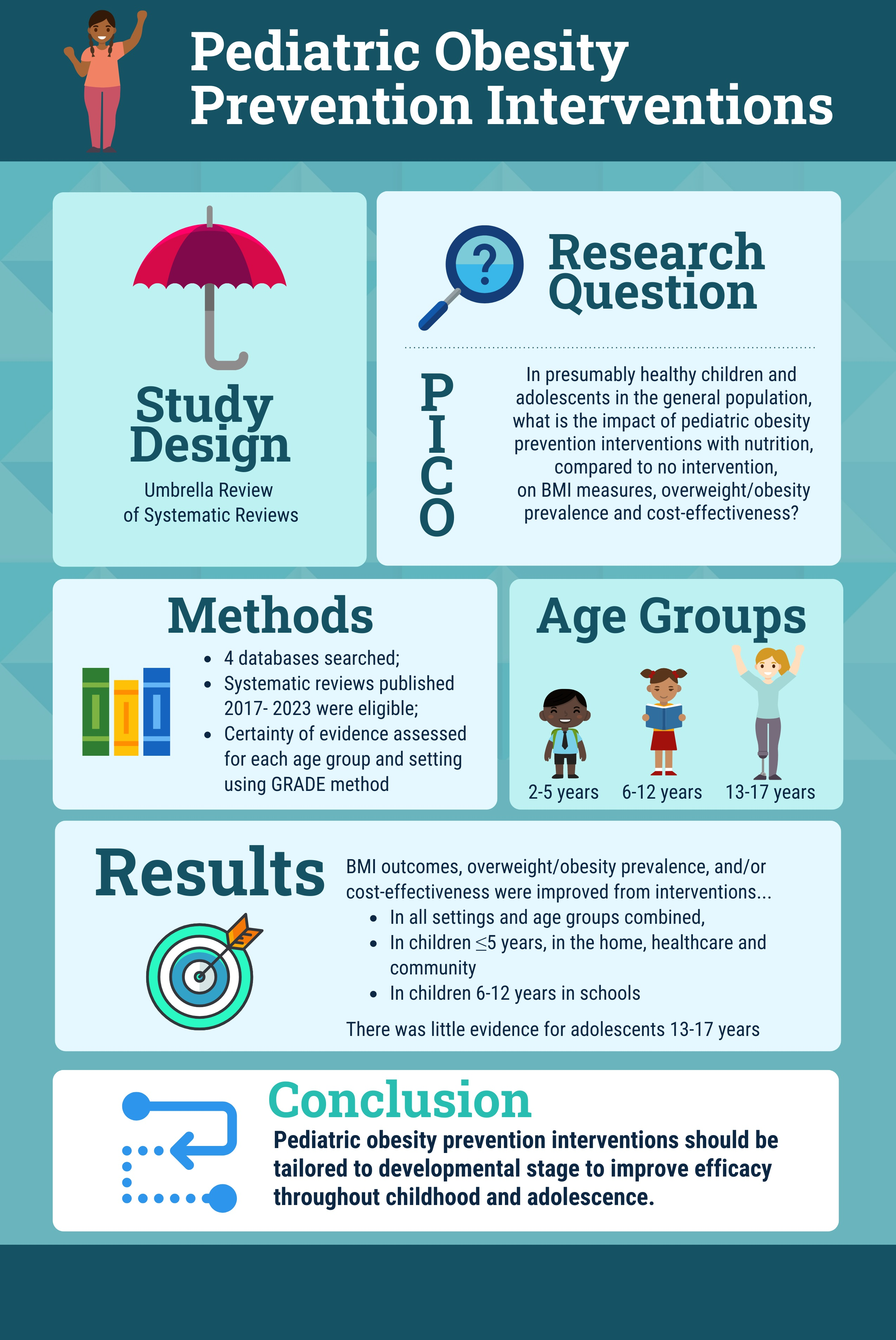
Nutrition Interventions for Pediatric Obesity Prevention: An Umbrella Review of Systematic Reviews


Abstract
:
1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Information Sources
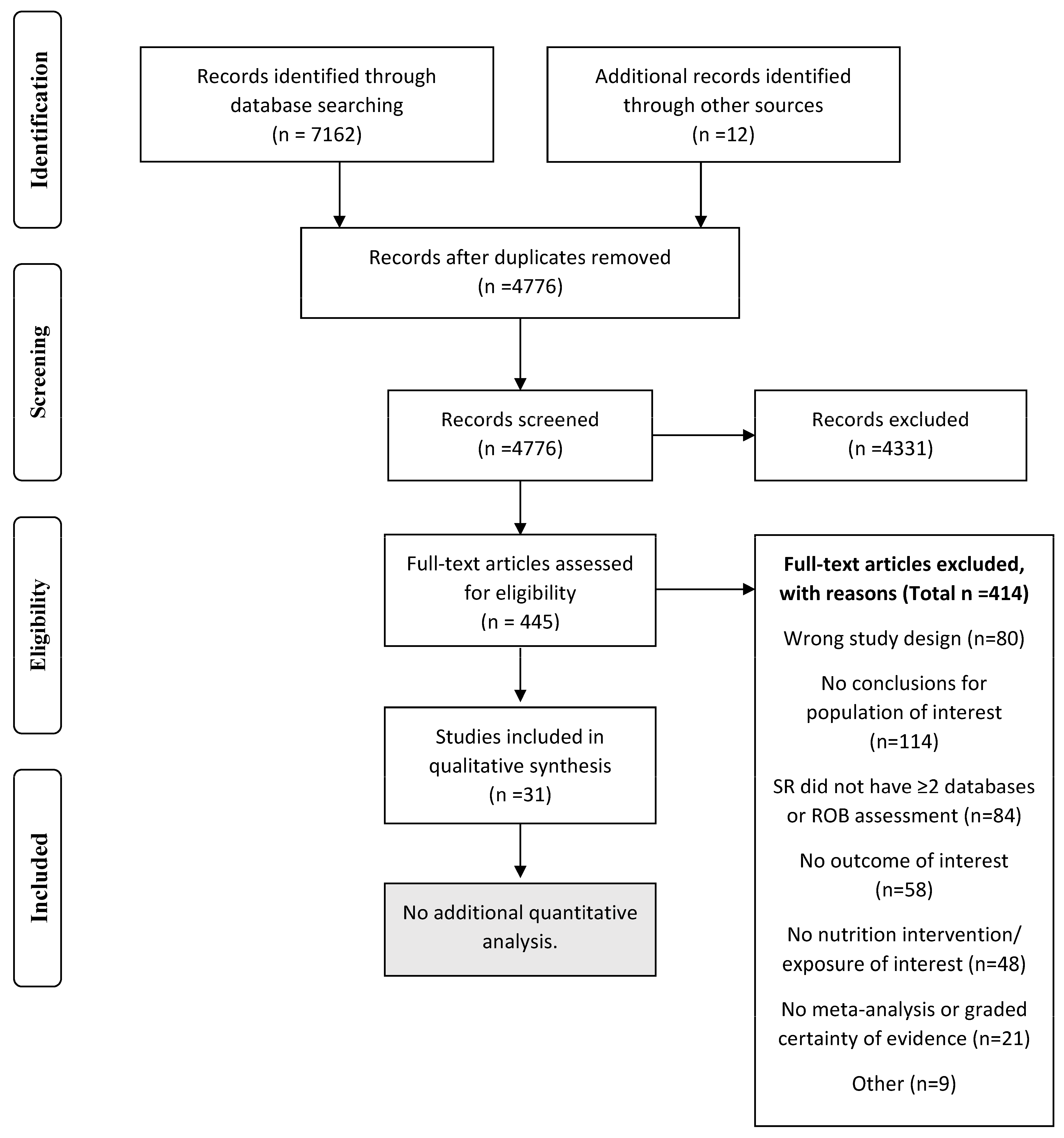
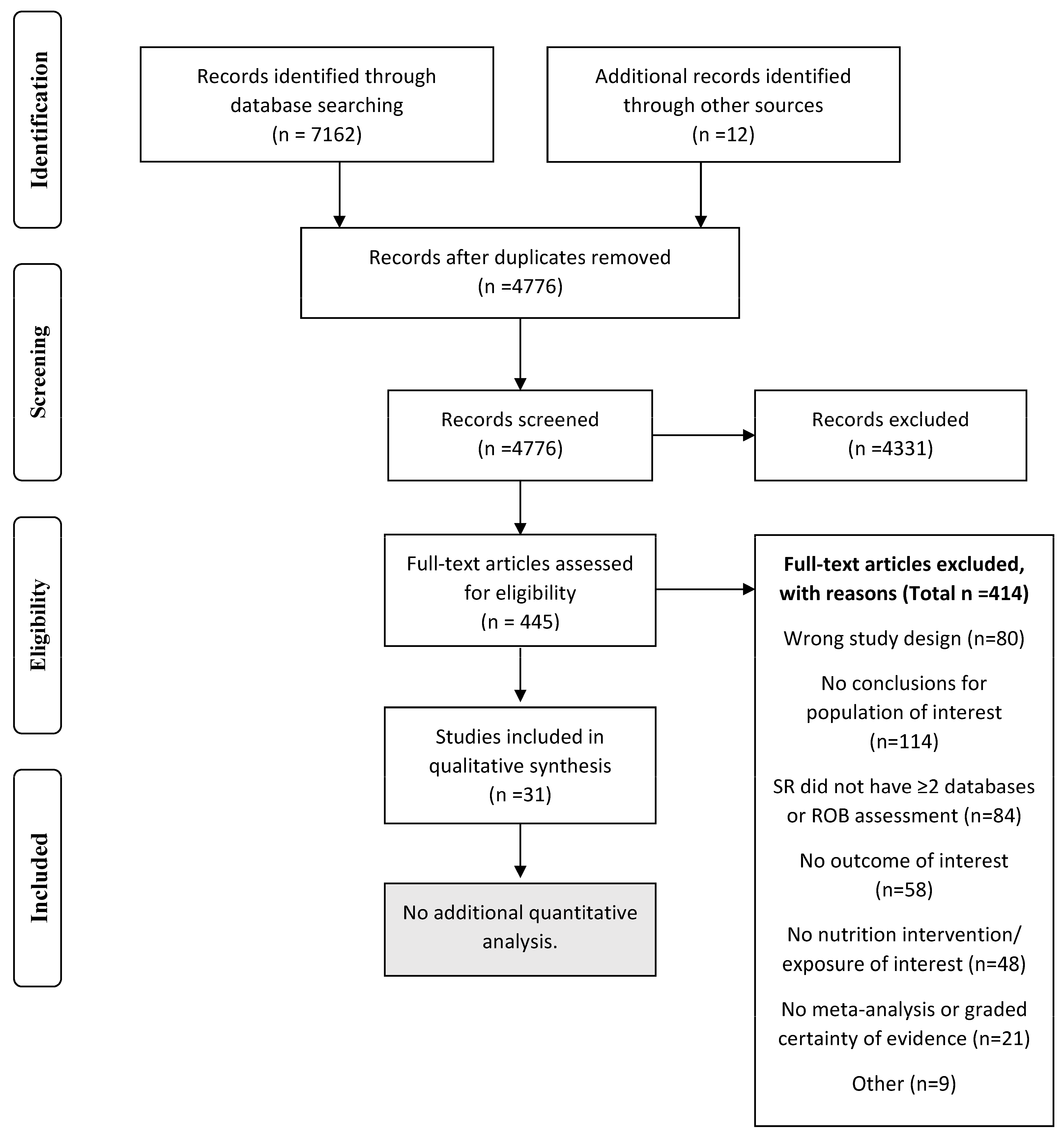
2.3. Study Selection
2.4. Data Collection
2.5. Quality Assessment
2.6. Synthesis of Results and Certainty Assessment
3. Results
3.1. All Settings
3.1.1. Age Groups Combined
3.1.2. Specific Age Groups
3.2. Home and Family Setting
3.2.1. Age Groups Combined
3.2.2. Specific Age Groups
3.3. Healthcare Setting
3.3.1. Age Groups Combined
3.3.2. Specific Age Groups
3.4. School Setting
3.4.1. Age Groups Combined
3.4.2. Specific Age Groups
3.5. Community Setting
3.5.1. All Age Groups
3.5.2. Specific Age Groups
3.6. Federal Food Assistance Programs
3.6.1. All Age Groups
3.6.2. Specific Age Groups
3.7. Electronic Interventions
4. Discussion
4.1. Strengths and Limitations
4.2. Implications for Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Acknowledgments
Conflicts of Interest
References
- Balasundaram, P.; Krishna, S. Obesity Effects on Child Health. StatPerls. 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK570613/ (accessed on 1 December 2023).
- U.S. Department of Health and Human Services. Healthy People 2030. Available online: https://health.gov/healthypeople/objectives-and-data/browse-objectives/overweight-and-obesity/reduce-proportion-children-and-adolescents-obesity-nws-04 (accessed on 18 October 2023).
- Grossman, D.C.; Bibbins-Domingo, K.; Curry, S.J.; Barry, M.J.; Davidson, K.W.; Doubeni, C.A.; Epling, J.W., Jr.; Kemper, A.R.; Krist, A.H.; Kurth, A.E.; et al. Screening for Obesity in Children and Adolescents: US Preventive Services Task Force Recommendation Statement. JAMA 2017, 317, 2417–2426. [Google Scholar] [CrossRef] [PubMed]
- Hoelscher, D.M.; Brann, L.S.; O’Brien, S.; Handu, D.; Rozga, M. Prevention of Pediatric Overweight and Obesity: Position of the Academy of Nutrition and Dietetics Based on an Umbrella Review of Systematic Reviews. J. Acad. Nutr. Diet 2022, 122, 410–423.e416. [Google Scholar] [CrossRef] [PubMed]
- Satter, E. Child Feeding Ages and Stages. Available online: https://www.ellynsatterinstitute.org/how-to-feed/child-feeding-ages-and-stages/ (accessed on 18 October 2023).
- Denova-Gutiérrez, E.; González-Rocha, A.; Méndez-Sánchez, L.; Araiza-Nava, B.; Balderas, N.; López, G.; Tolentino-Mayo, L.; Jauregui, A.; Hernández, L.; Unikel, C.; et al. Overview of Systematic Reviews of Health Interventions for the Prevention and Treatment of Overweight and Obesity in Children. Nutrients 2023, 15, 773. [Google Scholar] [CrossRef] [PubMed]
- Bahia, L.; Schaan, C.W.; Sparrenberger, K.; Abreu, G.A.; Barufaldi, L.A.; Coutinho, W.; Schaan, B.D. Overview of meta-analysis on prevention and treatment of childhood obesity. J. Pediatr. 2019, 95, 385–400. [Google Scholar] [CrossRef] [PubMed]
- Rozga, M.; Handu, D. Current Systems-Level Evidence on Nutrition Interventions to Prevent and Treat Cardiometabolic Risk in the Pediatric Population: An Evidence Analysis Center Scoping Review. J. Acad. Nutr. Diet 2021, 121, 2501–2523. [Google Scholar] [CrossRef] [PubMed]
- Flodgren, G.M.; Helleve, A.; Lobstein, T.; Rutter, H.; Klepp, K.-I. Primary prevention of overweight and obesity in adolescents: An overview of systematic reviews. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2020, 21, e13102. [Google Scholar] [CrossRef] [PubMed]
- Ohri-Vachaspati, P.; DeLia, D.; DeWeese, R.S.; Crespo, N.C.; Todd, M.; Yedidia, M.J. The relative contribution of layers of the Social Ecological Model to childhood obesity. Public Health Nutr. 2015, 18, 2055–2066. [Google Scholar] [CrossRef]
- Pollock, M.F.R.; Becker, L.A.; Pieper, D.; Hartling, L. Chapter V: Overviews of Reviews. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.2; Higgins, J.P.T.T.J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2021; Available online: https://training.cochrane.org/handbook/current/chapter-v (accessed on 30 November 2023).
- Handu, D.; Moloney, L.; Wolfram, T.; Ziegler, P.; Acosta, A.; Steiber, A. Academy of Nutrition and Dietetics Methodology for Conducting Systematic Reviews for the Evidence Analysis Library. J. Acad. Nutr. Diet 2016, 116, 311–318. [Google Scholar] [CrossRef]
- Gates, M.; Gates, A.; Pieper, D.; Fernandes, R.M.; Tricco, A.C.; Moher, D.; Brennan, S.E.; Li, T.; Pollock, M.; Lunny, C.; et al. Reporting guideline for overviews of reviews of healthcare interventions: Development of the PRIOR statement. BMJ 2022, 378, e070849. [Google Scholar] [CrossRef]
- Rozga, M.; Handu, D. Interventions to Prevent Pediatric Overweight and Obesity: An Umbrella Review of Systematic Reviews. Available online: https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=443033 (accessed on 13 October 2023).
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Academy of Nutrition and Dietetics Evidence Analysis Library. Pediatric Overweight and Obesity Prevention. Available online: https://www.andeal.org/topic.cfm?menu=5296&cat=6132 (accessed on 18 October 2023).
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Abdel Rahman, A.; Jomaa, L.; Kahale, L.A.; Adair, P.; Pine, C. Effectiveness of behavioral interventions to reduce the intake of sugar-sweetened beverages in children and adolescents: A systematic review and meta-analysis. Nutr. Rev. 2018, 76, 88–107. [Google Scholar] [CrossRef]
- Ananthapavan, J.; Nguyen, P.K.; Bowe, S.J.; Sacks, G.; Mantilla Herrera, A.M.; Swinburn, B.; Brown, V.; Sweeney, R.; Lal, A.; Strugnell, C.; et al. Cost-effectiveness of community-based childhood obesity prevention interventions in Australia. Int. J. Obes. 2019, 43, 1102–1112. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.; Moore, T.H.; Hooper, L.; Gao, Y.; Zayegh, A.; Ijaz, S.; Elwenspoek, M.; Foxen, S.C.; Magee, L.; O’Malley, C.; et al. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2019, 7, Cd001871. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, L.R.; Wethington, H.R.; Finnie, R.K.C.; Mercer, S.L.; Merlo, C.; Michael, S.; Sliwa, S.; Pratt, C.A.; Ochiai, E. A Community Guide Systematic Review: School Dietary and Physical Activity Interventions. Am. J. Prev. Med. 2023, 64, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Caulfield, L.E.; Bennett, W.L.; Gross, S.M.; Hurley, K.M.; Ogunwole, S.M.; Venkataramani, M.; Lerman, J.L.; Zhang, A.; Sharma, R.; Bass, E.B. AHRQ Comparative Effectiveness Reviews. In Maternal and Child Outcomes Associated With the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC); Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2022. [Google Scholar]
- Cerrato-Carretero, P.; Roncero-Martín, R.; Pedrera-Zamorano, J.D.; López-Espuela, F.; Puerto-Parejo, L.M.; Sánchez-Fernández, A.; Canal-Macías, M.L.; Moran, J.M.; Lavado-García, J.M. Long-Term Dietary and Physical Activity Interventions in the School Setting and Their Effects on BMI in Children Aged 6–12 Years: Meta-Analysis of Randomized Controlled Clinical Trials. Healthcare 2021, 9, 396. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.F.W.; Hecht, A.A.; McLoughlin, G.M.; Turner, L.; Schwartz, M.B. Universal School Meals and Associations with Student Participation, Attendance, Academic Performance, Diet Quality, Food Security, and Body Mass Index: A Systematic Review. Nutrients 2021, 13, 911. [Google Scholar] [CrossRef] [PubMed]
- Dabravolskaj, J.; Montemurro, G.; Ekwaru, J.P.; Wu, X.Y.; Storey, K.; Campbell, S.; Veugelers, P.J.; Ohinmaa, A. Effectiveness of school-based health promotion interventions prioritized by stakeholders from health and education sectors: A systematic review and meta-analysis. Prev. Med. Rep. 2020, 19, 101138. [Google Scholar] [CrossRef]
- Durão, S.; Wilkinson, M.; Davids, E.L.; Gerritsen, A.; Kredo, T. Effects of policies or interventions that influence the school food environment on children’s health and nonhealth outcomes: A systematic review. Nutr. Rev. 2023, nuad059. [Google Scholar] [CrossRef]
- Gonçalves, V.S.S.; Figueiredo, A.; Silva, S.A.; Silva, S.U.; Ronca, D.B.; Dutra, E.S.; Carvalho, K.M.B. The food environment in schools and their immediate vicinities associated with excess weight in adolescence: A systematic review and meta-analysis. Health Place 2021, 71, 102664. [Google Scholar] [CrossRef] [PubMed]
- Hayba, N.; Elkheir, S.; Hu, J.; Allman-Farinelli, M. Effectiveness of Lifestyle Interventions for Prevention of Harmful Weight Gain among Adolescents from Ethnic Minorities: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 6059. [Google Scholar] [CrossRef] [PubMed]
- Hudak, K.M.; Racine, E.F. The Supplemental Nutrition Assistance Program and Child Weight Status: A Review. Am. J. Prev. Med. 2019, 56, 882–893. [Google Scholar] [CrossRef] [PubMed]
- Kenney, E.L.; Tucker, K.; Plummer, R.S.; Mita, C.; Andreyeva, T. The Child and Adult Care Food Program and young children’s health: A systematic review. Nutr. Rev. 2023, 81, nuad016. [Google Scholar] [CrossRef] [PubMed]
- Kornet-van der Aa, D.A.; Altenburg, T.M.; van Randeraad-van der Zee, C.H.; Chinapaw, M.J. The effectiveness and promising strategies of obesity prevention and treatment programmes among adolescents from disadvantaged backgrounds: A systematic review. Obes. Rev. 2017, 18, 581–593. [Google Scholar] [CrossRef] [PubMed]
- Long, Q.; Zhang, T.; Chen, F.; Wang, W.; Chen, X.; Ma, M. Effectiveness of dietary interventions on weight outcomes in childhood: A systematic review meta-analysis of randomized controlled trials. Transl. Pediatr. 2021, 10, 701–714. [Google Scholar] [CrossRef] [PubMed]
- Morgan, E.H.; Schoonees, A.; Sriram, U.; Faure, M.; Seguin-Fowler, R.A. Caregiver involvement in interventions for improving children’s dietary intake and physical activity behaviors. Cochrane Database Syst. Rev. 2020, 1, Cd012547. [Google Scholar] [CrossRef]
- Nally, S.; Carlin, A.; Blackburn, N.E.; Baird, J.S.; Salmon, J.; Murphy, M.H.; Gallagher, A.M. The Effectiveness of School-Based Interventions on Obesity-Related Behaviours in Primary School Children: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Children 2021, 8, 489. [Google Scholar] [CrossRef]
- Narzisi, K.; Simons, J. Interventions that prevent or reduce obesity in children from birth to five years of age: A systematic review. J. Child Health Care 2020, 25, 320–334. [Google Scholar] [CrossRef]
- Nury, E.; Stadelmaier, J.; Morze, J.; Nagavci, B.; Grummich, K.; Schwarzer, G.; Hoffmann, G.; Angele, C.M.; Steinacker, J.M.; Wendt, J.; et al. Effects of nutritional intervention strategies in the primary prevention of overweight and obesity in school settings: Systematic review and network meta-analysis. BMJ Med. 2022, 1, e000346. [Google Scholar] [CrossRef] [PubMed]
- Olstad, D.L.; Ancilotto, R.; Teychenne, M.; Minaker, L.M.; Taber, D.R.; Raine, K.D.; Nykiforuk, C.I.J.; Ball, K. Can targeted policies reduce obesity and improve obesity-related behaviours in socioeconomically disadvantaged populations? A systematic review. Obes. Rev. 2017, 18, 791–807. [Google Scholar] [CrossRef] [PubMed]
- Pineda, E.; Bascunan, J.; Sassi, F. Improving the school food environment for the prevention of childhood obesity: What works and what doesn’t. Obes. Rev. 2021, 22, e13176. [Google Scholar] [CrossRef] [PubMed]
- Qi, Y.; Hamzah, S.H.; Gu, E.; Wang, H.; Xi, Y.; Sun, M.; Rong, S.; Lin, Q. Is School Gardening Combined with Physical Activity Intervention Effective for Improving Childhood Obesity? A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 2605. [Google Scholar] [CrossRef] [PubMed]
- Rochira, A.; Tedesco, D.; Ubiali, A.; Fantini, M.P.; Gori, D. School Gardening Activities Aimed at Obesity Prevention Improve Body Mass Index and Waist Circumference Parameters in School-Aged Children: A Systematic Review and Meta-Analysis. Child. Obes. 2020, 16, 154–173. [Google Scholar] [CrossRef]
- Salam, R.A.; Padhani, Z.A.; Das, J.K.; Shaikh, A.Y.; Hoodbhoy, Z.; Jeelani, S.M.; Lassi, Z.S.; Bhutta, Z.A. Effects of Lifestyle Modification Interventions to Prevent and Manage Child and Adolescent Obesity: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 2208. [Google Scholar] [CrossRef]
- Seral-Cortes, M.; De Miguel-Etayo, P.; Zapata, P.; Miguel-Berges, M.L.; Moreno, L.A. Effectiveness and process evaluation in obesity and type 2 diabetes prevention programs in children: A systematic review and meta-analysis. BMC Public Health 2021, 21, 348. [Google Scholar] [CrossRef]
- Beck Silva, K.B.; Miranda Pereira, E.; Santana, M.L.P.; Costa, P.R.F.; Silva, R.C.R. Effects of computer-based interventions on food consumption and anthropometric parameters of adolescents: A systematic review and metanalysis. Crit. Rev. Food Sci. Nutr. 2022, 1–13. [Google Scholar] [CrossRef]
- Smit, M.S.; Boelens, M.; Mölenberg, F.J.M.; Raat, H.; Jansen, W. The long-term effects of primary school-based obesity prevention interventions in children: A systematic review and meta-analysis. Pediatr. Obes. 2023, 18, e12997. [Google Scholar] [CrossRef]
- Specchia, M.L.; Barbara, A.; Campanella, P.; Parente, P.; Mogini, V.; Ricciardi, W.; Damiani, G. Highly-integrated programs for the prevention of obesity and overweight in children and adolescents: Results from a systematic review and meta-analysis. Ann. Ist. Super Sanita 2018, 54, 332–339. [Google Scholar] [CrossRef]
- Suleiman-Martos, N.; García-Lara, R.A.; Martos-Cabrera, M.B.; Albendín-García, L.; Romero-Béjar, J.L.; Cañadas-De la Fuente, G.A.; Gómez-Urquiza, J.L. Gamification for the Improvement of Diet, Nutritional Habits, and Body Composition in Children and Adolescents: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 2478. [Google Scholar] [CrossRef] [PubMed]
- Tissot, H.; Pfarrwaller, E.; Haller, D.M. Primary care prevention of cardiovascular risk behaviors in adolescents: A systematic review. Prev. Med. 2021, 142, 106346. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, L.; Kabdebo, I.; Dunham, M.; Quinn, R.; Hummelshoj, J.; George, C.; Denney-Wilson, E. The effectiveness of nurse-led interventions to prevent childhood and adolescent overweight and obesity: A systematic review of randomised trials. J. Adv. Nurs. 2021, 77, 4612–4631. [Google Scholar] [CrossRef] [PubMed]
- Hayba, N.; Rissel, C.; Allman Farinelli, M. Effectiveness of lifestyle interventions in preventing harmful weight gain among adolescents: A systematic review of systematic reviews. Obes. Rev. 2021, 22, e13109. [Google Scholar] [CrossRef]
- Durao, S.; Visser, M.E.; Ramokolo, V.; Oliveira, J.M.; Schmidt, B.-M.; Balakrishna, Y.; Brand, A.; Kristjansson, E.; Schoonees, A. Community-level interventions for improving access to food in low- and middle-income countries. Cochrane Database Syst. Rev. 2020, 8, CD011504. [Google Scholar] [CrossRef] [PubMed]
- Sultana, M.; Nichols, M.; Moodie, M.; Allender, S.; Brown, V. A systematic review of economic evidence for community-based obesity prevention interventions in children. Obes. Rev. 2023, 24, e13592. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services. 2008 Physical Activity Guidelines for Americans; U.S. Department of Health and Human Services: Washington, DC, USA, 2008. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Peer-Review Status | Peer-reviewed | Non-peer-reviewed articles |
| Population | Humans Children and adolescents (aged 2 to 17 years) | Animal studies Children aged < 2 years or adults ≥ 18 years old |
| Setting | Any settings, including those in the home and family, healthcare, school, and community settings. | Inpatient or acute care, inpatient rehab. |
| Health Status | Presumably healthy (no major co-morbidities) or part of the “general” population (e.g., school setting). | Studies targeting participants with any condition or disease that limits application to the general population, including but not limited to individuals with ADD/ADHD; asthma; autism; celiac disease/IBD/IBS; critical illness; eating disorders or disordered eating; food allergies; pregnancy; CKD, ESRD and/or renal dialysis; cancer, current or survived; heart failure; spinal cord injury; cachexia; liver disease; past surgery, including bariatric surgery; current respiratory therapy; type 1 diabetes mellitus. |
| Interventions/ Exposures | Nutrition interventions, with or without physical activity or other components. Programs such as food assistance programs or school nutrition programs. | SRs examining observational exposures other than programs or policies implemented in the settings indicated. SRs not requiring a nutrition component. |
| Comparators | Includes either comparison to a control group or pre–post measurements for longitudinal cohort studies for programs. | No comparison (e.g., prevalence of nutrition outcomes only). SRs include primarily cross-sectional studies with no stratification for longitudinal studies. |
| Study Design Preferences | SRs and meta-analysis SRs must search at least two databases and assess risk of bias/quality for each included study. SRs must conduct meta-analysis and/or grade the certainty of evidence. SRs not conducting meta-analysis or grading certainty of evidence will only be included if no other SRs are available for the specific setting and outcome examined. | Narrative reviews, commentary/letters to the editor; primary studies; guidelines not based on a systematic review. SRs that describe a population only (e.g., prevalence of malnutrition) or are based on cross-sectional studies only. Umbrella reviews (SRs of SRs). SRs not reporting meta-analysis or certainty of evidence when higher-quality evidence is available. |
| Outcome | BMI measures, prevalence, and incidence of overweight or obesity, cost-effectiveness. | Outcomes not specified in inclusion criteria. |
| Year Range | January 2017–8 June 2023 | Prior to January 2017 or later than the search date of 8 June 2023 |
| Language | Limited to articles in English. | Articles not published in English. |
| Location | Includes studies from countries with developed economies. | Does not include countries with developed economies. |
| Systematic Review | Population | Study Designs Included | Intervention | Setting or Context | Outcomes of Interest Reported | Outcomes with Meta-Analysis | Outcomes with Certainty of Evidence | RoB Tool | Overall Confidence in Results from AMSTAR2 |
|---|---|---|---|---|---|---|---|---|---|
| Abdel Rahman et al., 2018 [20] | Aged 4–16 years | RCTs | Educational or behavioral interventions to reduce sugar-sweetened beverage intake | School, Home and Family | BMI z-score, Obesity Prevalence | BMI z-score | None | Cochrane Risk of Bias tool | Critically Low |
| Ananthapavan et al., 2018 [21] | Aged 5–18 years | RCTs, Cluster-RCTs, quasi-experimental, cohort | Community-based obesity prevention interventions | Community | BMI z-score, Cost-effectiveness | BMI z-score | None | Effective Public Health Practice Project Quality Assessment | Critically Low |
| Brown et al., 2019 [22] | Aged 0–5, 6–12, and 13–18 years | RCTs | Educational, health promotion, psychological, family, behavioral therapy, counseling, management strategies | Community, school, home, healthcare | BMI z-score, BMI | BMI z-score, BMI | BMI z-score, BMI | Risk of Bias tool (Cochrane) | High |
| Buchanan et al., 2023 [23] | Aged, 5–18 years | Controlled trials, quasi-experimental with a comparison group, time–series, before –after study, or post-only studies with a comparison group | Programs or policies aimed at school meals, or fruit/vegetable snack programs with physical activity/education | School | BMI z-score, Overweight/Obesity Prevalence | BMI z-score, Overweight/Obesity Prevalence | None | Community Preventive Services | Critically Low |
| Caulfield et al., 2022 [24] | Aged <5 years | Quantitative and qualitative studies | WIC participation | Food Assistance | Obesity prevalence | None | Obesity Prevalence | Effective Public Health Practice Project | Moderate |
| Cerrato-Carretero et al., 2021 [25] | Aged 6–12 years | RCTs | Dietary interventions or education combined with physical activity | School | BMI | BMI | None | Risk of Bias tool (Cochrane) | Critically Low |
| Cohen et al., 2021 [26] | Aged 5–18 years | Quantitative research articles | Universal school meals | Food Assistance Programs, School | BMI | None | None | Newcastle-Ottawa Scale | Low |
| Dabravolskaj et al., 2020 [27] | Aged 4–18 years | RCTs, cohort, and quasi-experimental | School-based | School | BMI z-score, BMI, Overweight/Obesity Prevalence | BMI z-score, BMI, Overweight/Obesity Prevalence | None | Downs and Black checklist | Critically Low |
| Durão et al., 2023 [28] | Aged 2–18 years | RCTs, Interrupted time–series, prospective controlled studies | Policies or interventions that influence the school food environment | School | BMI Overweight/Obesity Prevalence | None | Overweight/Obesity Prevalence | Risk of Bias tool (Cochrane) | Moderate |
| Goncalves et al., 2021 [29] | Aged 10–19 years | Observational studies | Food environment in and around schools | School | BMI, Obesity Prevalence | Obesity Prevalence | None | The Joanna Briggs Institute | Moderate |
| Hayba et al., 2021 [51] | Aged 13–18 years, Racial/ethnic minorities | RCTs | Lifestyle factors, including nutrition and physical activity | Any | BMI, Overweight/Obesity Prevalence | None | BMI | Risk of Bias tool (Cochrane) | High |
| Hudak et al., 2019 [31] | Aged 2–18 years, participants in SNAP | Not described (mostly cross-sectional) | SNAP | Food Assistance Program | Overweight/Obesity Prevalence | None | None | Strength of Design framework | Critically Low |
| Kenney et al., 2023 [32] | Aged 2–18 years | Not described (studies with a comparison group) | Child and Adult Care Food Program | Food Assistance Program | Overweight/Obesity Prevalence | None | None | National Institutes of Health (NIH) quality assessment tool for observational cohort and cross-sectional studies | Critically Low |
| Kornet-van der Aa et al., 2017 [33] | Aged 12–18 years from disadvantaged backgrounds | RCTs, NRCTs | Any obesity prevention intervention | Any | BMI z-score, BMI, Overweight/Obesity Prevalence | None | None | Effective Public Health Practice Project | Moderate |
| Long et al., 2021 [34] | Aged <18 years | RCTs | Medical health education containing dietary contents | Any | BMI z-score, BMI | BMI z-score, BMI | None | Risk of Bias tool (Cochrane) | Critically Low |
| Morgan et al., 2020 [35] | Aged 2–18 years | RCTs, quasi-RCTs | Caregivers involved in at least one aspect of the intervention | Home and Family | BMI, Overweight/Obesity Prevalence | BMI, Overweight/Obesity Prevalence | None | Cochrane methods for cluster-RCTs | High |
| Nally et al., 2021 [36] | Aged 5–12 years | RCTs | School-based interventions | School | BMI z-score, BMI | BMI z-score, BMI | None | Risk of Bias tool (Cochrane) | Critically Low |
| Narzisi et al., 2020 [37] | Aged 0–5 years | RCTs | Lifestyle interventions to prevent obesity | Healthcare | Overweight Prevalence | No | No | JBI | Critically Low |
| Nury et al., 2021 [38] | Aged 4–18 years | Cluster-RCTs | Nutritional intervention strategies in the school setting | School | BMI z-score, BMI, Overweight/Obesity Prevalence | BMI z-score, BMI, Overweight/Obesity Prevalence | BMI z-score, BMI, Overweight/Obesity Prevalence | RoB2 tool (Cochrane) | High |
| Olstad et al., 2017 [39] | Aged 2–18 years from disadvantaged backgrounds | RCTs, quasi-experimental, controlled pre–post studies | Food Assistance Programs | Food Assistance Programs | BMI z-score, BMI | No | No | Effective Public Health Practice Project Quality | Moderate |
| Pineda et al., 2021 [40] | Aged ≤19 years | RCTs and Quasi-experimental studies | Interventions that focus on the school food environment | School | BMI z-score | BMI z-score | None | RoB2 ROBINS-I (Cochrane) | Critically Low |
| Qi et al., 2021 [41] | Aged 7–12 years | RCTs | School gardening | School | BMI z-score, BMI | BMI z-score, BMI | None | RoB2 (Cochrane) | Critically Low |
| Rochira et al., 2020 [42] | Aged 6–13 years | RCTs, quasi-experimental studies, observational studies | School gardening | School | BMI z-score, BMI percentile, BMI | BMI z-score, BMI Percentile, BMI | No | Cochrane Tool for Quality Assessment, STROBE | Critically Low |
| Salam et al., 2020 [43] | Aged 0–19 years | RCTs and Quasi-experimental studies | Lifestyle interventions, including dietary, physical activity, behavioral therapy, or any combination of these | Any | BMI z-score, Overweight/Obesity Prevalence, Cost-effectiveness | BMI z-score, Overweight/Obesity Prevalence | None | Risk of Bias tool (Cochrane) | Low |
| Seral-Cortes et al., 2021 [44] | Aged 6–12 years | RCTs | Health programs preventing obesity and T2DM with diet, physical activity, and behavioral support | Any | BMI z-score, BMI | BMI z-score, BMI | None | Risk of Bias tool (Cochrane) | Critically Low |
| Silva et al., 2022 [45] | Aged 10–19 years | RCTs and quasi-experimental studies | Computer-based nutrition interventions carried out in school | Electronic | BMI | BMI | BMI | Center for Reviews and Dissemination | Critically Low |
| Smit et al., 2023 [46] | Aged 6–12 years | RCTs and NRCTs | Primary school-based obesity prevention interventions | School | BMI z-score, BMI, Overweight/Obesity Prevalence | BMI z-score, BMI | BMI z-score, BMI, Overweight/Obesity Prevalence | RoB2 ROBINS-I (Cochrane) | High |
| Specchia et al., 2018 [47] | Aged <18 years | Not described | Multi-component, multi-level, or multi-setting | Any | Overweight/Obesity Prevalence | Overweight/Obesity Prevalence | None | Risk of Bias tool (Cochrane) | Low |
| Suleiman-Martos et al., 2021 [48] | Children or Adolescents | RCTs | Game-based interventions (gamification) | Electronic | BMI z-scores | Yes | No | Cochrane’s ROB | Critically Low |
| Tissot et al., 2021 [49] | Aged 10–19 years | RCTs and cluster-RCTs | Delivered in primary care | Healthcare | BMI z-scores, BMI percentiles | None | None | Risk of Bias tool (Cochrane) | Moderate |
| Whitehead et al., 2021 [50] | Aged ≤18 years | RCTs | Nurse-led interventions to prevent overweight or obesity | Healthcare | BMI, BMI-SDS | None | None | RoB2 | Low |
| Author, Year | Setting | Outcome | N Studies | N Participants | Effect Size Type | Effect Size | 95% CI | CoE a | SR Quality |
|---|---|---|---|---|---|---|---|---|---|
| Combined Age Groups | |||||||||
| Abdel Rahman et al., 2018 [20] | All settings | BMI z-score | 3 | 3475 | MD | −0.01 | −0.05, 0.03 | - | Critically Low |
| Long et al., 2021 [34] | All settings | BMI z-score | 17 | 16,351 | MD | −0.04 | −0.06, −0.02 | - | Critically Low |
| Salam et al., 2020 [43] | All settings | BMI z-score | 32 | 33,039 | MD | −0.12 | −0.18, −0.06 | Low | Low |
| Long et al., 2021 [34] | All settings | BMI | 20 | 21,334 | MD | −0.12 | −0.20, −0.05 | - | Critically Low |
| Salam et al., 2020 [43] | All settings | BMI | 35 | 47,499 | MR | −0.41 | −0.60, −0.21 | Low | Low |
| Salam et al., 2020 [43] | All settings | Overweight/Obesity Prevalence | 12 | NR | - | - | - | - | Low |
| Specchia et al., 2018 [47] | All settings | Overweight/Obesity Prevalence | 11 | 137,058 | MD (%) | −0.03 | −0.04, −0.01 | - | Low |
| Salam et al., 2020 [43] | All settings | Cost-effectiveness | 6 | NR | - | Four studies showed cost-efficacy, one study showed cost savings, and one was unclear. | - | - | Low |
| Ananthapavan et al., 2019 [21] | Community | BMI z-score | 9 | Unclear | MD | −0.07 | −0.13, −0.01 | - | Critically Low |
| Ananthapavan et al., 2019 [21] | Community | Cost-effectiveness | Modeling | Modeling | HALY, ICER, AUD/HALY gained | Probability of intervention being cost-effective was 95% | - | - | Critically Low |
| Suleiman-Martos et al., 2021 [48] | Electronic | BMI z-score | 2 | 571 | MD | −0.05 | −0.21, 0.11 | - | Critically Low |
| Silva et al., 2022 [45] | Electronic | BMI | 3 | 3542 | MD | −0.02 | −0.18, 0.14 | Moderate | Critically Low |
| Whitehead et al., 2021 [50] | Healthcare | BMI z-score | 1 | 552 | MD | −0.14 | −0.26, −0.02 | - | Low |
| Tissot et al., 2021 [49] | Healthcare | BMI | 9 | NR | - | Mixed findings | - | - | Moderate |
| Narzisi et al., 2020 [37] | Healthcare | Overweight Prevalence | 1 | NR | - | No difference between groups | - | - | Critically Low |
| Morgan et al., 2020 [35] | Home and Family | BMI | 4 | 1861 | SMD | 0.05 | −0.04, 0.15 | - | High |
| Morgan et al., 2020 [35] | Home and Family | Overweight/Obesity Prevalence | 3 | 1866 | RR | 1.02 | 0.89, 1.17 | - | High |
| Abdel Rahman et al., 2018 [20] | School | BMI z-score | 2 | 3384 | MD | −0.04 | −0.15, 0.06 | - | Critically Low |
| Buchanan et al., 2023 [23] | School | BMI z-score | 10 | NR | Median (IQR) | −0.07 | −0.19, −0.02 | - | Critically Low |
| Dabravolskaj 2020 [27] | School 1 | BMI z-score | 9 | 17,105 | MD | −0.016 | −0.04, 0.01 | - | Critically Low |
| Dabravolskaj 2020 [27] | School 3 | BMI z-score | 3 | 1,069,346 | MD | −0.006 | −0.02, 0.008 | - | Critically Low |
| Dabravolskaj 2020 [27] | School 4 | BMI z-score | 2 | 1526 | MD | 0.05 | −0.05, 0.15 | - | Critically Low |
| Nury et al., 2021 [38] | School | BMI z-score | 8 | 8174 | MD | −0.09 | −0.18, 0.00 | Low | High |
| Pineda et al., 2021 [40] | School | BMI z-score | 5 | NR | MD | −0.12 | −0.15, −0.10 | - | Critically Low |
| Dabravolskaj 2020 [27] | School 1 | BMI | 8 | 15,018 | MD | −0.26 | −0.40, −0.12 | - | Critically Low |
| Dabravolskaj 2020 [27] | School 2 | BMI | 1 | 320 | MD | −0.33 | −0.94, 0.28 | - | Critically Low |
| Nury et al., 2021 [38] | School | BMI | 10 | 12,067 | MD | 0.03 | −0.10, 0.16 | Low | High |
| Dabravolskaj 2020 [27] | School 2 | BMI percentile | 2 | 740 | MD | −7.92 | −16.53, 0.70 | - | Critically Low |
| Durão et al., 2023 [28] | School | Overweight/Obesity Prevalence | 3 | 67,841 | - | Mixed Findings | - | Very Low | Moderate |
| Buchanan et al., 2023 [23] | School | Overweight/Obesity Prevalence | 9 | NR | Median (IQR) (%) | −2.5 | −8.1, −1.6 | - | Critically Low |
| Dabravolskaj 2020 [27] | School 1 | Overweight/Obesity Prevalence | 3 | 8848 | OR | 0.85 | 0.71, 1.01 | - | Critically Low |
| Dabravolskaj 2020 [27] | School 3 | Overweight/Obesity Prevalence | 2 | 1,068,512 | OR | 0.96 | 0.86, 1.06 | - | Critically Low |
| Dabravolskaj 2020 [27] | School 4 | Overweight/Obesity Prevalence | 1 | 1362 | OR | 1.21 | 0.95, 1.55 | - | Critically Low |
| Goncalves et al., 2023 [29] | School 1 | Overweight/Obesity Prevalence | 5 | 88,530 | OR | 1.14 | 1.01, 1.28 | - | Moderate |
| Goncalves et al., 2023 [29] | School 2 | Overweight/Obesity Prevalence | 4 | 80,864 | OR | 0.89 | 0.82, 0.96 | - | Moderate |
| Goncalves et al., 2023 [29] | School 3 | Overweight/Obesity Prevalence | 3 | 10,377 | OR | 0.70 | 0.40, 1.22 | - | Moderate |
| Nury et al., 2021 [38] | School | Overweight/Obesity Prevalence | 3 | 901 | OR | 1.19 | 0.95, 1.49 | Very Low | High |
| Ages 2–5 years | |||||||||
| Brown et al., 2019 [22] | All settings | BMI z-score | 16 | 6261 | MD | −0.07 | −0.14, −0.01 | Moderate | High |
| Brown et al., 2019 [22] | All settings | BMI | 11 | 5536 | MD | −0.11 | −0.21, 0 | Moderate | High |
| Brown et al., 2019 [22] | Community | BMI z-score | 2 | 632 | MD | −0.02 | −0.13, 0.09 | - | High |
| Brown et al., 2019 [22] | Community | BMI | 1 | 75 | MD | −0.59 | −0.94, −0.24 | - | High |
| Brown et al., 2019 [22] | Healthcare | BMI z-score | 1 | 121 | MD | −0.24 | −0.26, −0.02 | - | High |
| Brown et al., 2019 [22] | Home and Family | BMI z-score | 3 | 595 | MD | −0.13 | −0.35, 0.09 | - | High |
| Brown et al., 2019 [22] | Home and Family | BMI | 2 | 778 | MD | −0.33 | −0.55, −0.1 | - | High |
| Brown et al., 2019 [22] | School/Childcare | BMI z-score | 10 | 4913 | MD | −0.04 | −0.09, 0.01 | - | High |
| Brown et al., 2019 [22] | School/Childcare | BMI | 9 | 4683 | MD | −0.05 | −0.14, 0.05 | - | High |
| Ages 6–12 years | |||||||||
| Brown et al., 2019 [22] | All settings | BMI z-score | 20 | 24,043 | MD | −0.05 | −0.1, −0.01 | Low | High |
| Seral-Cortes 2021 [44] | All settings | BMI z-score | 16 | 17,989 | SMD | −0.06 | −0.12, 0.01 | - | Critically Low |
| Brown et al., 2019 [22] | All settings | BMI | 25 | 19,498 | MD | −0.05 | −0.11, 0.01 | Low | High |
| Seral-Cortes 2021 [44] | All settings | BMI | 30 | 13,128 | SMD | −0.01 | −0.14, 0.13 | - | Critically Low |
| Ananthapavan et al., 2019 [21] | Community | BMI z-score | 5 | NR | MD | −0.12 | −0.23, −0.01 | - | Critically Low |
| Brown et al., 2019 [22] | Community | BMI z-score | 4 | 657 | MD | −0.04 | −0.39, 0.31 | - | High |
| Brown et al., 2019 [22] | Community | BMI | 9 | 742 | MD | −0.08 | −0.29, 0.23 | - | High |
| Abdel Rahman et al., 2018 [20] | Home and Family | BMI z-score | 1 | 93 | MD | 0.02 | −0.02, 0.06 | - | Critically Low |
| Brown et al., 2019 [22] | Home and Family | BMI z-score | 1 | 134 | MD | 0.03 | −0.04, 0.1 | - | High |
| Brown et al., 2019 [22] | School | BMI z-score | 15 | 22,879 | MD | −0.05 | −0.1, 0.01 | - | High |
| Nally et al., 2021 [36] | School | BMI z-score | 20 | 16,787 | SMD | −0.05 | −0.08, −0.02 | - | Critically Low |
| Qi et al., 2021 [41] | School | BMI z-score | 5 | 4285 | MD | −0.12 | −0.26, 0.02 | - | Critically Low |
| Rochira et al., 2020 [42] | School | BMI z-score | 4 | 1996 | MD | −0.09 | −0.19, 0.01 | - | Critically Low |
| Smit et al., 2023 [46] | School | BMI z-score | 3 | 2730 | MD | −0.08 | −0.20, 0.05 | Very Low | High |
| Brown et al., 2019 [22] | School | BMI | 16 | 18,488 | MD | −0.04 | −0.1, 0.02 | - | High |
| Cerrato-Carretero et al. 2021 [25] | School | BMI | 11 | 17,446 | SMD | −0.00 | −0.05, 0.04 | - | Critically Low |
| Nally et al., 2021 [36] | School | BMI | 21 | 14,101 | MD | −0.39 | −0.47, −0.30 | - | Critically Low |
| Qi et al., 2021 [41] | School | BMI | 5 | 3991 | MD | −0.49 | −1.63, 0.65 | - | Critically Low |
| Rochira et al., 2020 [42] | School | BMI | 2 | 188 | MD | 0.13 | −0.94, 1.20 | - | Critically Low |
| Smit et al., 2023 [46] | School | BMI | 6 | 5453 | MD | 0.06 | −0.38, 0.50 | Very Low | High |
| Rochira et al., 2020 [42] | School | BMI percentile | 4 | 4593 | MD | −1.37 | −2.38, 0.37 | - | Critically Low |
| Smit et al., 2023 [46] | School | Overweight/Obesity Prevalence | 9 | 7059 | - | - | - | Very Low | High |
| Ages 13–17 years | |||||||||
| Brown et al., 2019 [22] | All settings | BMI z-score | 6 | 16,543 | MD | 0.01 | −0.05, 0.07 | Low | High |
| Brown et al., 2019 [22] | All settings | BMI | 8 | 16,583 | MD | −0.02 | −0.1, 0.05 | Low | High |
| Hayba 2021 [51] | All settings | BMI | 7 | 2763 | - | No difference between groups | - | Low | High |
| Kornet-van der Aa 2017 [33] | All settings | Overweight/Obesity Prevalence | 1 | 235 | MD (%) | Percent with overweight/obesity decreased in intervention | - | - | Moderate |
| Ananthapavan et al., 2019 [21] | Community | BMI z-score | 4 | NR | MD | −0.02 | −0.07, 0.03 | - | |
| Brown et al., 2019 [22] | Home and Family | BMI z-score | 1 | 75 | MD | 0.06 | −0.13, 0.26 | - | High |
| Brown et al., 2019 [22] | School | BMI z-score | 5 | 16,173 | MD | 0 | −0.06, 0.06 | - | High |
| Brown et al., 2019 [22] | School | BMI | 8 | 16,347 | MD | −0.02 | −0.1, 0.05 | - | High |
| Outcome No. of Participants (Studies) | Anticipated Absolute Effects (95% CI) | Certainty | What Happens |
|---|---|---|---|
| Difference | |||
| All Age Groups | |||
| BMI z-score [43] No. of participants: 33,039 (32 RCTs) | MD 0.12 lower (0.18 lower to 0.06 lower) | ⨁⨁◯◯ LOW a | In pediatric individuals, diet and physical activity interventions may reduce BMI z-score. |
| BMI [43] No. of participants: 47,499 (35 RCTs) | MD 0.41 kg/m2 lower (0.6 lower to 0.21 lower) | ⨁⨁◯◯ LOW a | In pediatric individuals, diet and physical activity interventions may reduce BMI. |
| Overweight/Obesity Prevalence [47] No. of participants: 137,058 (11 RCTs) | MD 0.03% lower (0.04 lower to 0.01 lower) | ⨁⨁◯◯ LOW b | In pediatric individuals, highly integrated overweight/obesity prevention programs may reduce the prevalence of overweight/obesity. |
| Cost-effectiveness [43] No. of participants: Unclear (6 RCTs) | NR | ⨁⨁◯◯ LOW c,d | In pediatric individuals, diet and physical activity interventions may be cost-effective. |
| Ages 0–5 years | |||
| BMI z-score [22] No. of participants: 6261 (16 RCTs) | MD 0.07 lower (0.14 lower to 0.01 lower) | ⨁⨁⨁◯ MODERATE a | Diet and physical activity interventions combined likely reduce BMI z-scores in individuals 0–5 years old. |
| BMI [22] No. of participants: 5536 (11 RCTs) | MD 0.11 kg/m2 lower (0.21 lower to 0) | ⨁⨁⨁◯ MODERATE a | Diet and physical activity interventions combined likely result in little to no difference in BMI in individuals 0–5 years old. |
| Ages 6–12 years | |||
| BMI z-score [22] No. of participants: 24,043 (20 RCTs) | MD 0.05 lower (0.11 lower to 0.01 lower) | ⨁⨁◯◯ LOW a | Diet and physical activity interventions combined may reduce BMI z-score in individuals 6–12 years old. |
| BMI [22] No. of participants: 19,498 (25 RCTs) | MD 0.05 kg/m2 lower (0.11 lower to 0.01 higher) | ⨁⨁◯◯ LOW b | Diet and physical activity interventions combined may result in little to no difference in BMI in individuals 6–12 years old. |
| Ages 13–17 years | |||
| BMI z-score [22] No. of participants: 16,453 (6 RCTs) | MD 0.01 higher (0.05 lower to 0.07 higher) | ⨁⨁◯◯ LOW a | Combined diet and physical activity interventions may result in little to no difference in BMI z-score in individuals 13–18 years old. |
| BMI [22] No. of participants: 16,583 (8 RCTs) | MD 0.02 lower (0.1 lower to 0.05 higher) | ⨁⨁◯◯ LOW a,b | Combined diet and physical activity interventions may result in little to no difference in BMI in individuals 13–18 years old. |
| Overweight and Obesity Prevalence [33] No. of participants: 235 (1 RCT) | NR | ⨁⨁⨁◯ VERY LOW b,c,d | In adolescents 12–18 years old, one RCT reported that obesity prevention interventions may reduce the percentage of participants with overweight or obesity. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rozga, M.; Handu, D. Nutrition Interventions for Pediatric Obesity Prevention: An Umbrella Review of Systematic Reviews. Nutrients 2023, 15, 5097. https://doi.org/10.3390/nu15245097
Rozga M, Handu D. Nutrition Interventions for Pediatric Obesity Prevention: An Umbrella Review of Systematic Reviews. Nutrients. 2023; 15(24):5097. https://doi.org/10.3390/nu15245097
Chicago/Turabian StyleRozga, Mary, and Deepa Handu. 2023. "Nutrition Interventions for Pediatric Obesity Prevention: An Umbrella Review of Systematic Reviews" Nutrients 15, no. 24: 5097. https://doi.org/10.3390/nu15245097
APA StyleRozga, M., & Handu, D. (2023). Nutrition Interventions for Pediatric Obesity Prevention: An Umbrella Review of Systematic Reviews. Nutrients, 15(24), 5097. https://doi.org/10.3390/nu15245097