

A Scoping Review of the Clinical Evidence for the Health Benefits of Culinary Doses of Herbs and Spices for the Prevention and Treatment of Metabolic Syndrome



Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
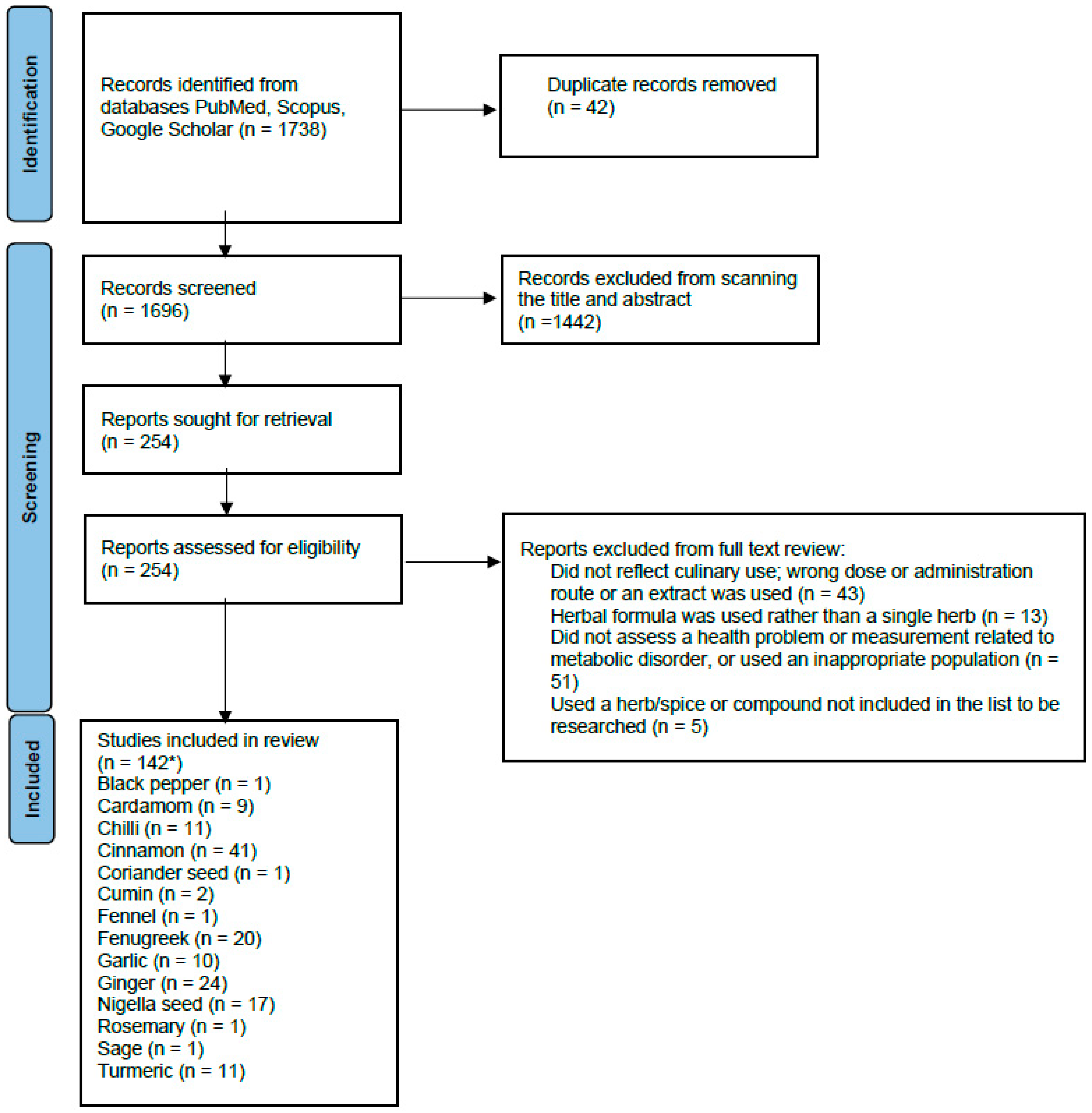
2.3. Study Selection and Data Collection
3. Results
3.1. Black Pepper, Cardamom and Chilli
3.2. Cinnamon
3.3. Coriander Seed, Cumin and Fennel
3.4. Fenugreek
3.5. Garlic
3.6. Ginger
3.7. Nigella Seeds
3.8. Rosemary, Sage and Turmeric
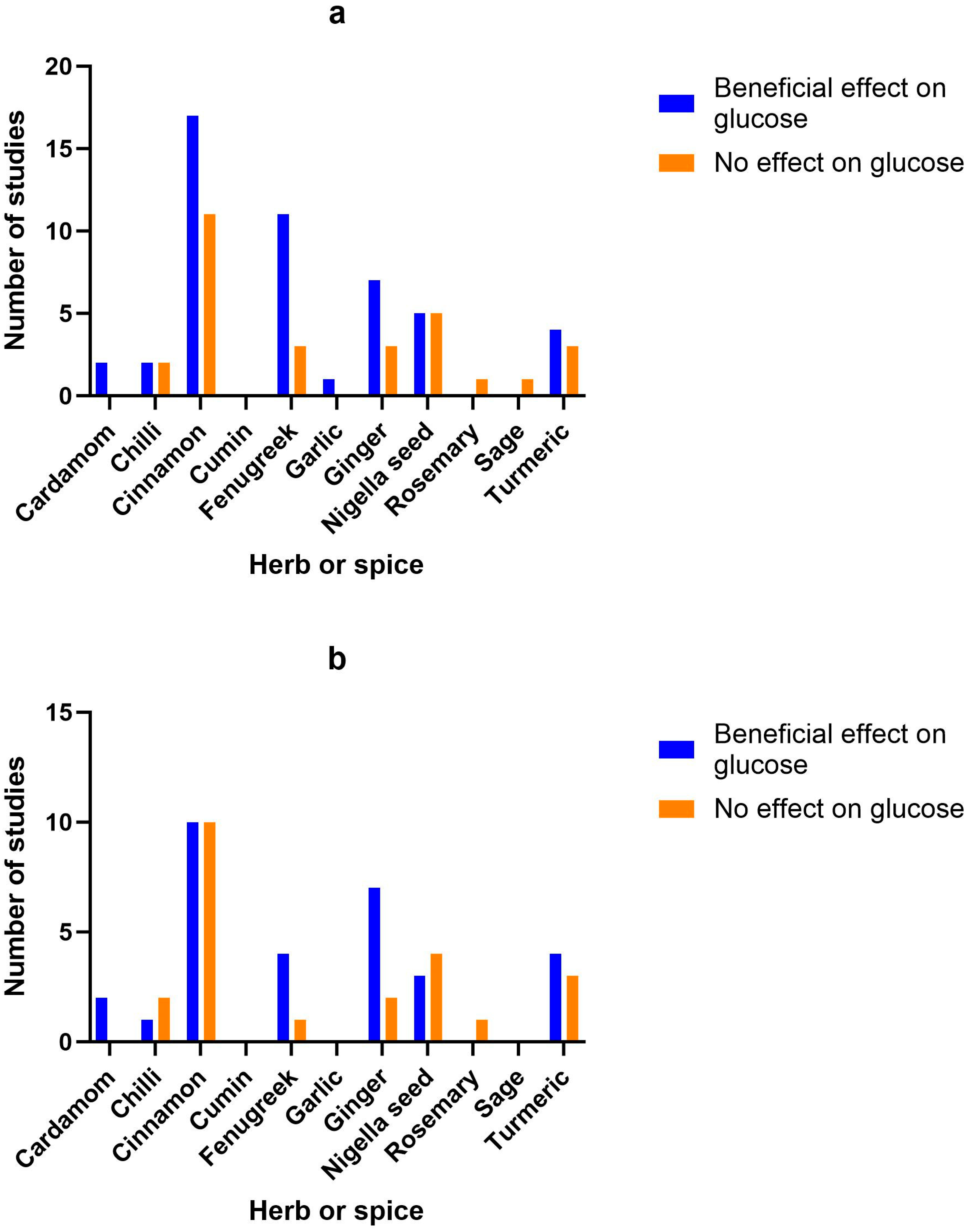
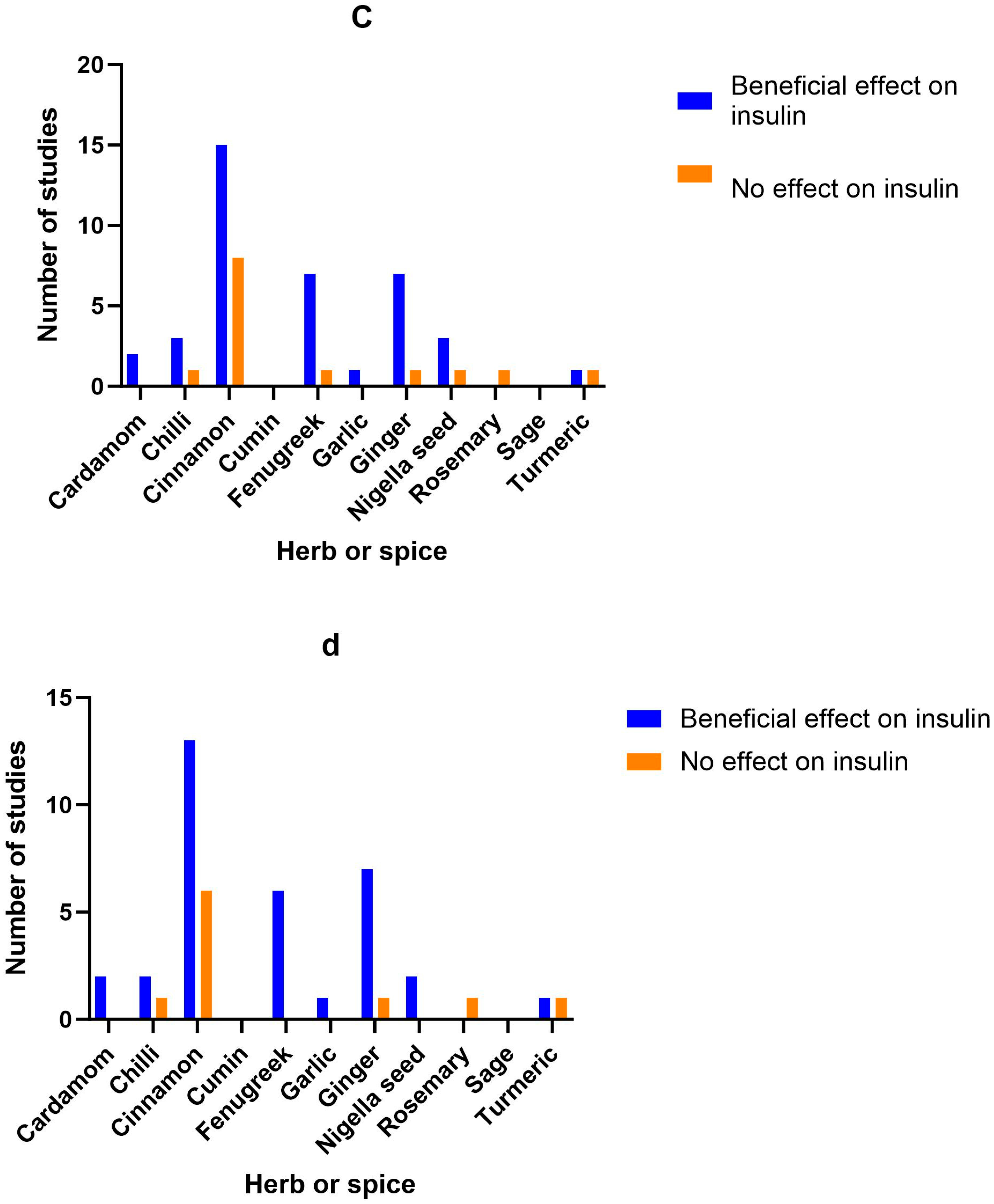
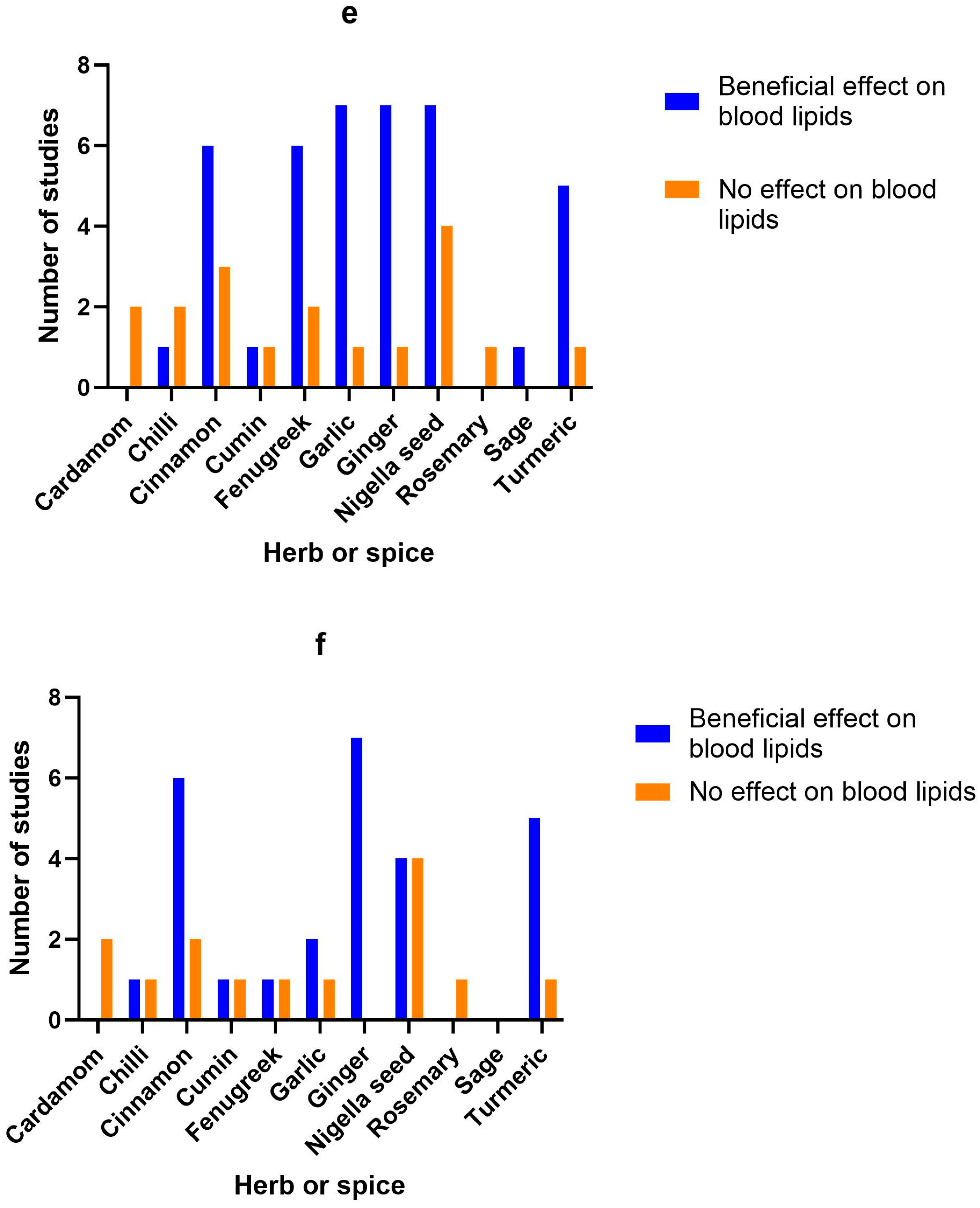
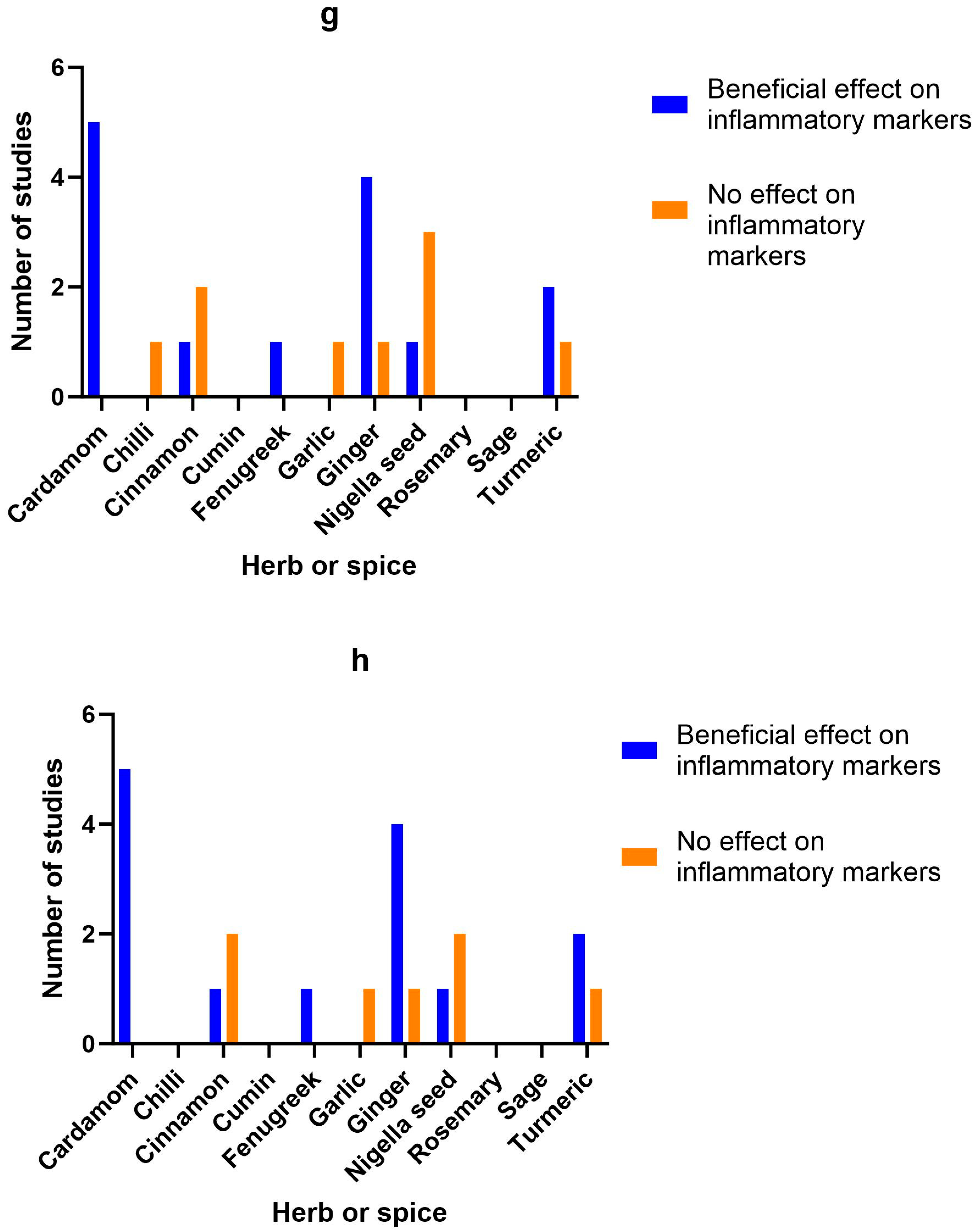
3.9. Herb/Spice Efficacy
3.10. Adverse Effects
3.11. Study Quality
4. Discussion
Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chew, N.W.S.; Ng, C.H.; Tan, D.J.H.; Kong, G.; Lin, C.; Chin, Y.H.; Lim, W.H.; Huang, D.Q.; Quek, J.; Fu, C.E.; et al. The global burden of metabolic disease: Data from 2000 to 2019. Cell Metab. 2023, 35, 414–428.e3. [Google Scholar] [CrossRef] [PubMed]
- Alkhatib, D.H.; Jaleel, A.; Tariq, M.N.M.; Feehan, J.; Apostolopoulos, V.; Cheikh Ismail, L.; Stojanovska, L.; Al Dhaheri, A.S. The role of bioactive compounds from dietary spices in the management of metabolic syndrome: An overview. Nutrients 2021, 14, 175. [Google Scholar] [CrossRef] [PubMed]
- Jiang, T.A. Health benefits of culinary herbs and spices. J. AOAC Int. 2019, 102, 395–411. [Google Scholar] [CrossRef] [PubMed]
- Pallauf, K.; Giller, K.; Huebbe, P.; Rimbach, G. Nutrition and healthy ageing: Calorie restriction or polyphenol-rich “MediterrAsian” diet? Oxid. Med. Cell Longev. 2013, 2013, 707421. [Google Scholar] [CrossRef] [PubMed]
- Bahadoran, Z.; Golzarand, M.; Mirmiran, P.; Saadati, N.; Azizi, F. The association of dietary phytochemical index and cardiometabolic risk factors in adults: Tehran Lipid and Glucose Study. J. Hum. Nutr. Diet. 2013, 26 (Suppl. 1), 145–153. [Google Scholar] [CrossRef]
- Dzah, C.S.; Asante-Donyinah, D.; Letsyo, E.; Dzikunoo, J.; Adams, Z.S. Dietary polyphenols and obesity: A review of polyphenol effects on lipid and glucose metabolism, mitochondrial homeostasis, and starch digestibility and absorption. Plant Foods Hum. Nutr. 2022, 78, 1–12. [Google Scholar] [CrossRef]
- Haldar, S.; Chia, S.C.; Henry, C.J. Polyphenol-rich curry made with mixed spices and vegetables increases postprandial plasma GLP-1 concentration in a dose-dependent manner. Eur. J. Clin. Nutr. 2018, 72, 297–300. [Google Scholar] [CrossRef]
- Huang, Y.; Tsai, M.F.; Thorat, R.S.; Xiao, D.; Zhang, X.; Sandhu, A.K.; Edirisinghe, I.; Burton-Freeman, B.M. Endothelial function and postprandial glucose control in response to test-meals containing herbs and spices in adults with overweight/obesity. Front. Nutr. 2022, 9, 811433. [Google Scholar] [CrossRef]
- Kroff, J.; Hume, D.J.; Pienaar, P.; Tucker, R.; Lambert, E.V.; Rae, D.E. The metabolic effects of a commercially available chicken peri-peri (African bird’s eye chilli) meal in overweight individuals. Br. J. Nutr. 2017, 117, 635–644. [Google Scholar] [CrossRef]
- McCrea, C.E.; West, S.G.; Kris-Etherton, P.M.; Lambert, J.D.; Gaugler, T.L.; Teeter, D.L.; Sauder, K.A.; Gu, Y.; Glisan, S.L.; Skulas-Ray, A.C. Effects of culinary spices and psychological stress on postprandial lipemia and lipase activity: Results of a randomized crossover study and in vitro experiments. J. Transl. Med. 2015, 13, 7. [Google Scholar] [CrossRef]
- Nakayama, H.; Tsuge, N.; Sawada, H.; Masamura, N.; Yamada, S.; Satomi, S.; Higashi, Y. A single consumption of curry improved postprandial endothelial function in healthy male subjects: A randomized, controlled crossover trial. Nutr. J. 2014, 13, 67. [Google Scholar] [CrossRef] [PubMed]
- Oh, E.S.; Petersen, K.S.; Kris-Etherton, P.M.; Rogers, C.J. Spices in a high-saturated-fat, high-carbohydrate meal reduce postprandial proinflammatory cytokine secretion in men with overweight or obesity: A 3-period, crossover, randomized controlled trial. J. Nutr. 2020, 150, 1600–1609. [Google Scholar] [CrossRef] [PubMed]
- Petersen, K.S.; Rogers, C.J.; West, S.G.; Proctor, D.N.; Kris-Etherton, P.M. The effect of culinary doses of spices in a high-saturated fat, high-carbohydrate meal on postprandial lipemia and endothelial function: A randomized, controlled, crossover pilot trial. Food Funct. 2020, 11, 3191–3200. [Google Scholar] [CrossRef] [PubMed]
- Petersen, K.S.; Davis, K.M.; Rogers, C.J.; Proctor, D.N.; West, S.G.; Kris-Etherton, P.M. Herbs and spices at a relatively high culinary dosage improves 24-hour ambulatory blood pressure in adults at risk of cardiometabolic diseases: A randomized, crossover, controlled-feeding study. Am. J. Clin. Nutr. 2021, 114, 1936–1948. [Google Scholar] [CrossRef]
- Zanzer, Y.C.; Plaza, M.; Dougkas, A.; Turner, C.; Östman, E. Black pepper-based beverage induced appetite-suppressing effects without altering postprandial glycaemia, gut and thyroid hormones or gastrointestinal well-being: A randomized crossover study in healthy subjects. Food Funct. 2018, 9, 2774–2786. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Marnie, C.; Colquhoun, H.; Garritty, C.M.; Hempel, S.; Horsley, T.; Langlois, E.V.; Lillie, E.; O’Brien, K.K.; Tunçalp, Ö.; et al. Scoping reviews: Reinforcing and advancing the methodology and application. Syst. Rev. 2021, 10, 263. [Google Scholar] [CrossRef]
- Cacchione, P.Z. The evolving methodology of scoping reviews. Clin. Nurs. Res. 2016, 25, 115–119. [Google Scholar] [CrossRef]
- Agarwal, A.K. Spice up your life: Adipose tissue and inflammation. J. Lipids 2014, 2014, 182575. [Google Scholar] [CrossRef]
- Akhter, S. Low to no cost remedies for the management of diabetes mellitus; global health concern. J. Diabetes Metab. Disord. 2021, 20, 951–962. [Google Scholar] [CrossRef]
- Bower, A.; Marquez, S.; de Mejia, E.G. The health benefits of selected culinary herbs and spices found in the traditional mediterranean diet. Crit. Rev. Food Sci. Nutr. 2016, 56, 2728–2746. [Google Scholar] [CrossRef]
- Deekshith, C.; Jois, M.; Radcliffe, J.; Thomas, J. Effects of culinary herbs and spices on obesity: A systematic literature review of clinical trials. J. Funct. Foods 2021, 81, 104449. [Google Scholar] [CrossRef]
- Gupta, K.; Testa, H.; Greenwood, T.; Kostek, M.; Haushalter, K.; Kris-Etherton, P.M.; Petersen, K.S. The effect of herbs and spices on risk factors for cardiometabolic diseases: A review of human clinical trials. Nutr. Rev. 2022, 80, 400–427. [Google Scholar] [CrossRef] [PubMed]
- Opara, E.I. Culinary herbs and spices: What can human studies tell us about their role in the prevention of chronic non-communicable diseases? J. Sci. Food Agric. 2019, 99, 4511–4517. [Google Scholar] [CrossRef] [PubMed]
- Opara, E.I.; Chohan, M. Culinary herbs and spices: Their bioactive properties, the contribution of polyphenols and the challenges in deducing their true health benefits. Int. J. Mol. Sci. 2014, 15, 19183–19202. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Olivo, S.A.; Macedo, L.G.; Gadotti, I.C.; Fuentes, J.; Stanton, T.; Magee, D.J. Scales to assess the quality of randomized controlled trials: A systematic review. Phys. Ther. 2008, 88, 156–175. [Google Scholar] [CrossRef]
- Verma, S.K.; Jain, V.; Katewa, S.S. Blood pressure lowering, fibrinolysis enhancing and antioxidant activities of cardamom (Elettaria cardamomum). Indian J. Biochem. Biophys. 2009, 46, 503–506. [Google Scholar]
- Kazemi, S.; Yaghooblou, F.; Siassi, F.; Rahimi Foroushani, A.; Ghavipour, M.; Koohdani, F.; Sotoudeh, G. Cardamom supplementation improves inflammatory and oxidative stress biomarkers in hyperlipidemic, overweight, and obese pre-diabetic women: A randomized double-blind clinical trial. J. Sci. Food Agric. 2017, 97, 5296–5301. [Google Scholar] [CrossRef]
- Aghasi, M.; Koohdani, F.; Qorbani, M.; Nasli-Esfahani, E.; Ghazi-Zahedi, S.; Khoshamal, H.; Keshavarz, A.; Sotoudeh, G. Beneficial effects of green cardamom on serum SIRT1, glycemic indices and triglyceride levels in patients with type 2 diabetes mellitus: A randomized double-blind placebo controlled clinical trial. J. Sci. Food Agric. 2019, 99, 3933–3940. [Google Scholar] [CrossRef]
- Daneshi-Maskooni, M.; Keshavarz, S.A.; Qorbani, M.; Mansouri, S.; Alavian, S.M.; Badri-Fariman, M.; Jazayeri-Tehrani, S.A.; Sotoudeh, G. Green cardamom supplementation improves serum irisin, glucose indices, and lipid profiles in overweight or obese non-alcoholic fatty liver disease patients: A double-blind randomized placebo-controlled clinical trial. BMC Complement. Altern. Med. 2019, 19, 59. [Google Scholar] [CrossRef]
- Ghazi Zahedi, S.; Koohdani, F.; Qorbani, M.; Nasli-Esfahani, E.; Aghasi, M.; Khoshamal, H.; Keshavarz, A.; Sotoudeh, G. Effects of green cardamom supplementation on serum levels of Hs-CRP, dimethylarginine, nitric oxide and blood pressure in patients with type 2 diabetes: A randomized, double-blind, placebo controlled, clinical trial. J. Herb. Med. 2022, 32, 100555. [Google Scholar] [CrossRef]
- Ghazi Zahedi, S.; Koohdani, F.; Qorbani, M.; Nasli-Esfahani, E.; Aghasi, M.; Khoshamal, H.; Sotoudeh, G. The effects of Elettaria cardamom supplementation on inflammatory markers and vascular function in patients with type 2 diabetes mellitus: A mechanism -based randomized clinical trial. J. Herb. Med. 2021, 25, 100403. [Google Scholar] [CrossRef]
- Daneshi-Maskooni, M.; Keshavarz, S.A.; Qorbani, M.; Mansouri, S.; Alavian, S.M.; Badri-Fariman, M.; Jazayeri-Tehrani, S.A.; Sotoudeh, G. Green cardamom increases Sirtuin-1 and reduces inflammation in overweight or obese patients with non-alcoholic fatty liver disease: A double-blind randomized placebo-controlled clinical trial. Nutr. Metab. 2018, 15, 63. [Google Scholar] [CrossRef]
- Cheshmeh, S.; Elahi, N.; Ghayyem, M.; Mosaieby, E.; Moradi, S.; Pasdar, Y.; Tahmasebi, S.; Moradinazar, M. Effect of green cardamom on the expression of genes implicated in obesity and diabetes among obese women with polycystic ovary syndrome: A double blind randomized controlled trial. Genes. Nutr. 2022, 17, 17. [Google Scholar] [CrossRef] [PubMed]
- Cheshmeh, S.; Ghayyem, M.; Khamooshi, F.; Heidarzadeh-Esfahani, N.; Rahmani, N.; Hojati, N.; Mosaieby, E.; Moradi, S.; Pasdar, Y. Green cardamom plus low-calorie diet can decrease the expression of inflammatory genes among obese women with polycystic ovary syndrome: A double-blind randomized clinical trial. Eat. Weight. Disord. 2022, 27, 821–830. [Google Scholar] [CrossRef]
- Clegg, M.E.; Golsorkhi, M.; Henry, C.J. Combined medium-chain triglyceride and chilli feeding increases diet-induced thermogenesis in normal-weight humans. Eur. J. Nutr. 2013, 52, 1579–1585. [Google Scholar] [CrossRef]
- Ahuja, K.D.; Robertson, I.K.; Geraghty, D.P.; Ball, M.J. Effects of chili consumption on postprandial glucose, insulin, and energy metabolism. Am. J. Clin. Nutr. 2006, 84, 63–69. [Google Scholar] [CrossRef]
- Ahuja, K.D.; Ball, M.J. Effects of daily ingestion of chilli on serum lipoprotein oxidation in adult men and women. Br. J. Nutr. 2006, 96, 239–242. [Google Scholar] [CrossRef]
- Ahuja, K.D.; Robertson, I.K.; Geraghty, D.P.; Ball, M.J. The effect of 4-week chilli supplementation on metabolic and arterial function in humans. Eur. J. Clin. Nutr. 2007, 61, 326–333. [Google Scholar] [CrossRef]
- Reinbach, H.C.; Martinussen, T.; Møller, P. Effects of hot spices on energy intake, appetite and sensory specific desires in humans. Food Qual. Prefer. 2010, 21, 655–661. [Google Scholar] [CrossRef]
- Kang, C.; Zhang, Y.; Zhu, X.; Liu, K.; Wang, X.; Chen, M.; Wang, J.; Chen, H.; Hui, S.; Huang, L.; et al. Healthy subjects differentially respond to dietary capsaicin correlating with specific gut enterotypes. J. Clin. Endocrinol. Metab. 2016, 101, 4681–4689. [Google Scholar] [CrossRef] [PubMed]
- Yuan, L.J.; Qin, Y.; Wang, L.; Zeng, Y.; Chang, H.; Wang, J.; Chen, S.-H.; Zhang, Q.-Y.; Zhu, J.-D.; Zhou, Y.; et al. Capsaicin-containing chili improved postprandial hyperglycemia, hyperinsulinemia, and fasting lipid disorders in women with gestational diabetes mellitus and lowered the incidence of large-for-gestational-age newborns. Clin. Nutr. 2016, 35, 388–393. [Google Scholar] [CrossRef]
- Chaiyasit, K.; Khovidhunkit, W.; Wittayalertpanya, S. Pharmacokinetic and the effect of capsaicin in Capsicum frutescens on decreasing plasma glucose level. J. Med. Assoc. Thai. 2009, 92, 108–113. [Google Scholar] [PubMed]
- Janssens, P.L.; Hursel, R.; Martens, E.A.; Westerterp-Plantenga, M.S. Acute effects of capsaicin on energy expenditure and fat oxidation in negative energy balance. PLoS ONE 2013, 8, e67786. [Google Scholar] [CrossRef] [PubMed]
- Janssens, P.L.; Hursel, R.; Westerterp-Plantenga, M.S. Capsaicin increases sensation of fullness in energy balance, and decreases desire to eat after dinner in negative energy balance. Appetite 2014, 77, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Solomon, T.P.; Blannin, A.K. Changes in glucose tolerance and insulin sensitivity following 2 weeks of daily cinnamon ingestion in healthy humans. Eur. J. Appl. Physiol. 2009, 105, 969–976. [Google Scholar] [CrossRef]
- Vanschoonbeek, K.; Thomassen, B.J.; Senden, J.M.; Wodzig, W.K.; van Loon, L.J. Cinnamon supplementation does not improve glycemic control in postmenopausal type 2 diabetes patients. J. Nutr. 2006, 136, 977–980. [Google Scholar] [CrossRef]
- Solomon, T.P.; Blannin, A.K. Effects of short-term cinnamon ingestion on in vivo glucose tolerance. Diabetes Obes. Metab. 2007, 9, 895–901. [Google Scholar] [CrossRef]
- Hlebowicz, J.; Hlebowicz, A.; Lindstedt, S.; Björgell, O.; Höglund, P.; Holst, J.J.; Darwiche, G.; Almér, L.-O. Effects of 1 and 3 g cinnamon on gastric emptying, satiety, and postprandial blood glucose, insulin, glucose-dependent insulinotropic polypeptide, glucagon-like peptide 1, and ghrelin concentrations in healthy subjects. Am. J. Clin. Nutr. 2009, 89, 815–821. [Google Scholar] [CrossRef]
- Markey, O.; McClean, C.M.; Medlow, P.; Davison, G.W.; Trinick, T.R.; Duly, E.; Shafat, A. Effect of cinnamon on gastric emptying, arterial stiffness, postprandial lipemia, glycemia, and appetite responses to high-fat breakfast. Cardiovasc. Diabetol. 2011, 10, 78. [Google Scholar] [CrossRef]
- Wickenberg, J.; Lindstedt, S.; Berntorp, K.; Nilsson, J.; Hlebowicz, J. Ceylon cinnamon does not affect postprandial plasma glucose or insulin in subjects with impaired glucose tolerance. Br. J. Nutr. 2012, 107, 1845–1849. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, J.L.; Bowden, R.G.; Willoughby, D.S. Cassia cinnamon supplementation reduces peak blood glucose responses but does not improve insulin resistance and sensitivity in young, sedentary, obese women. J. Diet. Suppl. 2016, 13, 461–471. [Google Scholar] [CrossRef] [PubMed]
- Sahib, A.S. Anti-diabetic and antioxidant effect of cinnamon in poorly controlled type-2 diabetic Iraqi patients: A randomized, placebo-controlled clinical trial. J. Intercult. Ethnopharmacol. 2016, 5, 108–113. [Google Scholar] [CrossRef]
- Magistrelli, A.; Chezem, J.C. Effect of ground cinnamon on postprandial blood glucose concentration in normal-weight and obese adults. J. Acad. Nutr. Diet. 2012, 112, 1806–1809. [Google Scholar] [CrossRef]
- Bernardo, M.A.; Silva, M.L.; Santos, E.; Moncada, M.M.; Brito, J.; Proença, L.; Singh, J.; de Mesquita, M.F. Effect of cinnamon tea on postprandial glucose concentration. J. Diabetes Res. 2015, 2015, 913651. [Google Scholar] [CrossRef] [PubMed]
- Hlebowicz, J.; Darwiche, G.; Björgell, O.; Almér, L.O. Effect of cinnamon on postprandial blood glucose, gastric emptying, and satiety in healthy subjects. Am. J. Clin. Nutr. 2007, 85, 1552–1556. [Google Scholar] [CrossRef]
- Atkinson, F.S.; Stockmann, K.S.; Ek, K.L.; Brand-Miller, J.C. Cassia but not cinnamon reduces postprandial glucose and insulin responses to oatmeal in lean, young adults. Asia Pacific J. Clin. Nutr. 2008, 17, S137. [Google Scholar]
- Kort, D.H.; Lobo, R.A. Preliminary evidence that cinnamon improves menstrual cyclicity in women with polycystic ovary syndrome: A randomized controlled trial. Am. J. Obstet. Gynecol. 2014, 211, e1–e6. [Google Scholar] [CrossRef]
- Crawford, P. Effectiveness of cinnamon for lowering hemoglobin A1C in patients with type 2 diabetes: A randomized, controlled trial. J. Am. Board. Fam. Med. 2009, 22, 507–512. [Google Scholar] [CrossRef]
- Suppapitiporn, S.; Kanpaksi, N.; Suppapitiporn, S. The effect of cinnamon cassia powder in type 2 diabetes mellitus. J. Med. Assoc. Thai. 2006, 89 (Suppl. 3), S200–S205. [Google Scholar]
- Blevins, S.M.; Leyva, M.J.; Brown, J.; Wright, J.; Scofield, R.H.; Aston, C.E. Effect of cinnamon on glucose and lipid levels in non insulin-dependent type 2 diabetes. Diabetes Care 2007, 30, 2236–2237. [Google Scholar] [CrossRef] [PubMed]
- Askari, F.; Rashidkhani, B.; Hekmatdoost, A. Cinnamon may have therapeutic benefits on lipid profile, liver enzymes, insulin resistance, and high-sensitivity C-reactive protein in nonalcoholic fatty liver disease patients. Nutr. Res. 2014, 34, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Talaei, B.; Amouzegar, A.; Sahranavard, S.; Hedayati, M.; Mirmiran, P.; Azizi, F. Effects of cinnamon consumption on glycemic indicators, advanced glycation end products, and antioxidant status in type 2 diabetic patients. Nutrients 2017, 9, 991. [Google Scholar] [CrossRef]
- Mirmiran, P.; Davari, M.; Hashemi, R.; Hedayati, M.; Sahranavard, S.; Bahreini, S.; Tavakoly, R.; Talaei, B. A randomized controlled trial to determining the effect of cinnamon on the plasma levels of soluble forms of vascular adhesion molecules in type 2 diabetes mellitus. Eur. J. Clin. Nutr. 2019, 73, 1605–1612. [Google Scholar] [CrossRef]
- Khan, A.A.; Begum, W. Efficacy of Darchini in the management of polycystic ovarian syndrome: A randomized clinical study. J. Herb. Med. 2019, 15, 100249. [Google Scholar] [CrossRef]
- Davari, M.; Hashemi, R.; Mirmiran, P.; Hedayati, M.; Sahranavard, S.; Bahreini, S.; Tavakoly, R.; Talaei, B. Effects of cinnamon supplementation on expression of systemic inflammation factors, NF-kB and sirtuin-1 (SIRT1) in type 2 diabetes: A randomized, double blind, and controlled clinical trial. Nutr. J. 2020, 19, 1. [Google Scholar] [CrossRef]
- Altschuler, J.A.; Casella, S.J.; MacKenzie, T.A.; Curtis, K.M. The effect of cinnamon on A1C among adolescents with type 1 diabetes. Diabetes Care 2007, 30, 813–816. [Google Scholar] [CrossRef]
- Akilen, R.; Tsiami, A.; Devendra, D.; Robinson, N. Glycated haemoglobin and blood pressure-lowering effect of cinnamon in multi-ethnic Type 2 diabetic patients in the UK: A randomized, placebo-controlled, double-blind clinical trial. Diabet. Med. 2010, 27, 1159–1167. [Google Scholar] [CrossRef]
- Wainstein, J.; Stern, N.; Heller, S.; Boaz, M. Dietary cinnamon supplementation and changes in systolic blood pressure in subjects with type 2 diabetes. J. Med. Food 2011, 14, 1505–1510. [Google Scholar] [CrossRef]
- Zahedifar, A.; Khodashenas, M.; Bijari, B.; Zahedifar, F. Effects of cinnamon on fasting blood sugar and hemoglobin A1C in patients with type II diabetes mellitus: A randomized clinical trial. [In Persian]. J. Mazandaran Univ. Med. Sci. 2018, 27, 80–88. [Google Scholar]
- Zahmatkesh, M.; Fallah Huseini, H.; Hajiaghaee, R.; Heidari, M.; Mehrafarin, A.; Tavakoli-far, B. The effects of Cinnamomum zeylanicum J. Presl on blood glucose level in patients with type 2 diabetes, a double-blind clinical trial. J. Med. Plants 2012, 11 (Suppl. 8), 258–263. [Google Scholar]
- Borzoei, A.; Rafraf, M.; Niromanesh, S.; Farzadi, L.; Narimani, F.; Doostan, F. Effects of cinnamon supplementation on antioxidant status and serum lipids in women with polycystic ovary syndrome. J. Tradit. Complement. Med. 2017, 8, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Borzoei, A.; Rafraf, M.; Asghari-Jafarabadi, M. Cinnamon improves metabolic factors without detectable effects on adiponectin in women with polycystic ovary syndrome. Asia Pac. J. Clin. Nutr. 2018, 27, 556–563. [Google Scholar]
- Mirfeizi, M.; Mehdizadeh Tourzani, Z.; Mirfeizi, S.Z.; Asghari Jafarabadi, M.; Rezvani, H.R.; Afzali, M. Controlling type 2 diabetes mellitus with herbal medicines: A triple-blind randomized clinical trial of efficacy and safety. J. Diabetes. 2016, 8, 647–656. [Google Scholar] [CrossRef]
- Mirmiranpour, H.; Huseini, H.F.; Derakhshanian, H.; Khodaii, Z.; Tavakoli-Far, B. Effects of probiotic, cinnamon, and synbiotic supplementation on glycemic control and antioxidant status in people with type 2 diabetes; a randomized, double-blind, placebo-controlled study. J. Diabetes Metab. Disord. 2019, 19, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Safdar, M.; Ali Khan, M.M.; Khattak, K.N.; Anderson, R.A. Cinnamon improves glucose and lipids of people with type 2 diabetes. Diabetes Care 2003, 26, 3215–3218. [Google Scholar] [CrossRef]
- Gupta Jain, S.; Puri, S.; Misra, A.; Gulati, S.; Mani, K. Effect of oral cinnamon intervention on metabolic profile and body composition of Asian Indians with metabolic syndrome: A randomized double -blind control trial. Lipids Health Dis. 2017, 16, 113. [Google Scholar] [CrossRef]
- Lira Neto, J.C.G.; Damasceno, M.M.C.; Ciol, M.A.; de Freitas, R.W.J.F.; de Araújo, M.F.M.; Teixeira, C.R.S.; Carvalho, G.C.N.; Lisboa, K.W.S.C.; Marques, R.L.L.; Alencar, A.M.P.G.; et al. Efficacy of cinnamon as an adjuvant in reducing the glycemic biomarkers of type 2 diabetes mellitus: A three-month, randomized, triple-blind, placebo-controlled clinical trial. J. Am. Nutr. Assoc. 2022, 41, 266–274. [Google Scholar] [CrossRef]
- Zare, R.; Nadjarzadeh, A.; Zarshenas, M.M.; Shams, M.; Heydari, M. Efficacy of cinnamon in patients with type II diabetes mellitus: A randomized controlled clinical trial. Clin. Nutr. 2019, 38, 549–556. [Google Scholar] [CrossRef]
- Hajimonfarednejad, M.; Nimrouzi, M.; Heydari, M.; Zarshenas, M.M.; Raee, M.J.; Jahromi, B.N. Insulin resistance improvement by cinnamon powder in polycystic ovary syndrome: A randomized double-blind placebo controlled clinical trial. Phytother. Res. 2018, 32, 276–283. [Google Scholar] [CrossRef]
- Soares, A.P.D.C.; de Faria, N.C.; Graciano, G.F.; Dos Santos, A.L.S.; Valenzuela, V.D.C.; Toulson Davisson Correia, M.I.; Cosenza, G.P.; Anastácio, L.R. Cinnamon infusion reduces satiety and increases energy intake: A randomized crossover trial. Ann. Nutr. Metab. 2022, 78, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Mettler, S.; Schwarz, I.; Colombani, P.C. Additive postprandial blood glucose-attenuating and satiety-enhancing effect of cinnamon and acetic acid. Nutr. Res. 2009, 29, 723–727. [Google Scholar] [CrossRef] [PubMed]
- Dastgheib, M.; Barati-Boldaji, R.; Bahrampour, N.; Taheri, R.; Borghei, M.; Amooee, S.; Mohammadi-Sartang, M.; Wong, A.; Babajafari, S.; Mazloomi, S.M. A comparison of the effects of cinnamon, ginger, and metformin consumption on metabolic health, anthropometric indices, and sexual hormone levels in women with poly cystic ovary syndrome: A randomized double-blinded placebo-controlled clinical trial. Front. Nutr. 2022, 9, 1071515. [Google Scholar] [CrossRef] [PubMed]
- Azimi, P.; Ghiasvand, R.; Feizi, A.; Hosseinzadeh, J.; Bahreynian, M.; Hariri, M.; Khosravi-Boroujeni, H. Effect of cinnamon, cardamom, saffron and ginger consumption on blood pressure and a marker of endothelial function in patients with type 2 diabetes mellitus: A randomized controlled clinical trial. Blood Press. 2016, 25, 133–140. [Google Scholar] [CrossRef]
- Zare, R.; Heshmati, F.; Fallahzadeh, H.; Nadjarzadeh, A. Effect of cumin powder on body composition and lipid profile in overweight and obese women. Complement. Ther. Clin. Pract. 2014, 20, 297–301. [Google Scholar] [CrossRef]
- Pishdad, S.; Nadjarzadeh, A.; Salehi Abargouei, A.; Karimi Nazari, E.; Papoli, M. Effect of cumin and cinnamon on lipid profile in middle-aged women with dyslipidemia: A double blind, randomized controlled clinical trial. Progr. Nutr. 2018, 20, 232–237. [Google Scholar]
- Bae, J.; Kim, J.; Choue, R.; Lim, H. Fennel (Foeniculum vulgare) and fenugreek (Trigonella foenum-graecum) tea drinking suppresses subjective short-term appetite in overweight women. Clin. Nutr. Res. 2015, 4, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Sowmya, P.; Rajyalakshmi, P. Hypocholesterolemic effect of germinated fenugreek seeds in human subjects. Plant Foods Hum. Nutr. 1999, 53, 359–365. [Google Scholar] [CrossRef]
- Sharma, R.D.; Raghuram, T.C.; Rao, N.S. Effect of fenugreek seeds on blood glucose and serum lipids in type I diabetes. Eur. J. Clin. Nutr. 1990, 44, 301–306. [Google Scholar]
- Madar, Z.; Abel, R.; Samish, S.; Arad, J. Glucose-lowering effect of fenugreek in non-insulin dependent diabetics. Eur. J. Clin. Nutr. 1988, 42, 51–54. [Google Scholar]
- Kiss, R.; Szabó, K.; Gesztelyi, R.; Somodi, S.; Kovács, P.; Szabó, Z.; Németh, J.; Priksz, D.; Kurucz, A.; Juhász, B.; et al. Insulin-sensitizer effects of fenugreek seeds in parallel with changes in plasma MCH levels in healthy volunteers. Int. J. Mol. Sci. 2018, 19, 771. [Google Scholar] [CrossRef] [PubMed]
- Gopalpura, P.B.; Jayanthi, C.; Dubey, S. Effect of Trigonella foenum-graecum seeds on the glycemic index of food: A clinical evaluation. Int. J. Diabetes Dev. Ctries. 2007, 27, 41–45. [Google Scholar] [CrossRef]
- Kassaian, N.; Azadbakht, L.; Forghani, B.; Amini, M. Effect of fenugreek seeds on blood glucose and lipid profiles in type 2 diabetic patients. Int. J. Vitam. Nutr. Res. 2009, 79, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Losso, J.N.; Holliday, D.L.; Finley, J.W.; Martin, R.J.; Rood, J.C.; Yu, Y.; Greenway, F.L. Fenugreek bread: A treatment for diabetes mellitus. J. Med. Food. 2009, 12, 1046–1049. [Google Scholar] [CrossRef] [PubMed]
- Robert, S.D.; Ismail, A.A.; Rosli, W.I. Reduction of postprandial blood glucose in healthy subjects by buns and flatbreads incorporated with fenugreek seed powder. Eur. J. Nutr. 2016, 55, 2275–2280. [Google Scholar] [CrossRef]
- Najdi, R.A.; Hagras, M.M.; Kamel, F.O.; Magadmi, R.M. A randomized controlled clinical trial evaluating the effect of Trigonella foenum-graecum (fenugreek) versus glibenclamide in patients with diabetes. Afr. Health Sci. 2019, 19, 1594–1601. [Google Scholar] [CrossRef]
- Tavakoly, R.; Maracy, M.R.; Karimifar, M.; Entezari, M.H. Does fenugreek (Trigonella foenum-graecum) seed improve inflammation, and oxidative stress in patients with type 2 diabetes mellitus? A parallel group randomized clinical trial. Eur. J. Integr. Med. 2018, 18, 13–17. [Google Scholar] [CrossRef]
- Sharma, R.D.; Sarkar, A.; Hazra, D.K.; Misra, B.; Singh, J.B.; Maheshwari, B.B.; Sharma, S.K. Hypolipidaemic effect of fenugreek seeds: A chronic study in non-insulin dependent diabetic patients. Phytother. Res. 1996, 10, 332–334. [Google Scholar] [CrossRef]
- Bhadauria, S.S.; Kushwah, A. Fenugreek seeds as a therapeutic supplement for patients with noninsulin dependent diabetes mellitus: A cross-sectional study. J. Clin. Diagn. Res. 2021, 15, BC21–BC23. [Google Scholar] [CrossRef]
- Hadi, A.; Arab, A.; Hajianfar, H.; Talaei, B.; Miraghajani, M.; Babajafari, S.; Marx, W.; Tavakoly, R. The effect of fenugreek seed supplementation on serum irisin levels, blood pressure, and liver and kidney function in patients with type 2 diabetes mellitus: A parallel randomized clinical trial. Complement. Ther. Med. 2020, 49, 102315. [Google Scholar] [CrossRef]
- Geberemeskel, G.A.; Debebe, Y.G.; Nguse, N.A. Antidiabetic effect of fenugreek seed powder solution (Trigonella foenum-graecum L.) on hyperlipidemia in diabetic patients. J. Diabetes Res. 2019, 2019, 8507453. [Google Scholar] [CrossRef] [PubMed]
- Yousefi, E.; Zareiy, S.; Zavoshy, R.; Noroozi, M.; Jahanihashemi, H.; Ardalani, H. Fenugreek: A therapeutic complement for patients with borderline hyperlipidemia: A randomised, double-blind, placebo-controlled, clinical trial. Adv. Integr. Med. 2017, 4, 31–35. [Google Scholar] [CrossRef]
- Rafraf, M.; Malekiyan, M.; Asghari-Jafarabadi, M.; Aliasgarzadeh, A. Effect of fenugreek seeds on serum metabolic factors and adiponectin levels in type 2 diabetic patients. Int. J. Vitam. Nutr. Res. 2014, 84, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Hassani, S.S.; Arezodar, F.F.; Esmaeili, S.S.; Gholami-Fesharaki, M. The effect of combined therapy with fenugreek and nutrition training based on iranian traditional medicine on FBS, HGA1C, BMI, and waist circumference in type 2 diabetic patients: A randomized double-blinded clinical trial. J. Adv. Med. Biomed. Res. 2019, 27, 37–42. [Google Scholar] [CrossRef]
- Hassani, S.S.; Fallahi Arezodar, F.; Esmaeili, S.S.; Gholami-Fesharaki, M. Effect of fenugreek use on fasting blood glucose, glycosylated hemoglobin, body mass index, waist circumference, blood pressure and quality of life in patients with type 2 diabetes mellitus: A randomized, double-blinded, placebo-controlled clinical trials. Galen. Med. J. 2019, 8, e1432. [Google Scholar] [CrossRef]
- Sharma, R.D. Effect of fenugreek seeds and leaves on blood glucose and serum insulin responses in human subjects. Nutr. Res. 1986, 6, 1353–1364. [Google Scholar] [CrossRef]
- Choudhary, P.R.; Jani, R.D.; Sharma, M.S. Effect of raw crushed garlic (Allium sativum L.) on components of metabolic syndrome. J. Diet Suppl. 2018, 15, 499–506. [Google Scholar] [CrossRef]
- Bakhsh, R.; Chughtai, M.I. Influence of garlic on serum cholesterol, serum triglycerides, serum total lipids and serum glucose in human subjects. Food/Nahrung 1984, 28, 159–163. [Google Scholar] [CrossRef]
- Roberts, K.; Jahner, D.K.W.; Buddington, R.K. Influence of garlic supplementation on human fecal flora and serum lipid levels. FASEB J. 1998, 12, A876. [Google Scholar]
- Scharbert, G.; Kalb, M.L.; Duris, M.; Marschalek, C.; Kozek-Langenecker, S.A. Garlic at dietary doses does not impair platelet function. Anesth. Analg. 2007, 105, 1214–1218. [Google Scholar] [CrossRef]
- Aslani, N.; Entezari, M.H.; Askari, G.; Maghsoudi, Z.; Maracy, M.R. Effect of garlic and lemon juice mixture on lipid profile and some cardiovascular risk factors in people 30–60 years old with moderate hyperlipidaemia: A randomized clinical trial. Int. J. Prev. Med. 2016, 7, 95. [Google Scholar] [PubMed]
- van Doorn, M.B.; Espirito Santo, S.M.; Meijer, P.; Kamerling, I.M.; Schoemaker, R.C.; Dirsch, V.; Vollmar, A.; Haffner, T.; Gebhardt, R.; Cohen, A.F.; et al. Effect of garlic powder on C-reactive protein and plasma lipids in overweight and smoking subjects. Am. J. Clin. Nutr. 2006, 84, 1324–1329. [Google Scholar] [CrossRef] [PubMed]
- Sangouni, A.A.; Mohammad Hosseini Azar, M.R.; Alizadeh, M. Effect of garlic powder supplementation on hepatic steatosis, liver enzymes and lipid profile in patients with non-alcoholic fatty liver disease: A double-blind randomised controlled clinical trial. Br. J. Nutr. 2020, 124, 450–456. [Google Scholar] [CrossRef]
- Sangouni, A.A.; Mohammad Hosseini Azar, M.R.; Alizadeh, M. Effects of garlic powder supplementation on insulin resistance, oxidative stress, and body composition in patients with non-alcoholic fatty liver disease: A randomized controlled clinical trial. Complement. Ther. Med. 2020, 51, 102428. [Google Scholar] [CrossRef] [PubMed]
- Sangouni, A.A.; Alizadeh, M.; Jamalzehi, A.; Parastouei, K. Effects of garlic powder supplementation on metabolic syndrome components, insulin resistance, fatty liver index, and appetite in subjects with metabolic syndrome: A randomized clinical trial. Phytother. Res. 2021, 35, 4433–4441. [Google Scholar] [CrossRef]
- Zeb, F.; Safdar, M.; Fatima, S.; Khan, S.; Alam, S.; Muhammad, M.; Syed, A.; Habib, F.; Shakoor, H. Supplementation of garlic and coriander seed powder: Impact on body mass index, lipid profile and blood pressure of hyperlipidemic patients. Pak. J. Pharm. Sci. 2018, 31, 1935–1941. [Google Scholar] [PubMed]
- Kamari, N.; Moradinazar, M.; Qasemi, M.; Khosravy, T.; Samadi, M.; Abdolahzad, H. Combination of the effect of ginger and anti-inflammatory diet on children with obesity with nonalcoholic fatty liver disease: A randomized clinical trial. Food Sci. Nutr. 2023, 11, 1846–1859. [Google Scholar] [CrossRef]
- Miyamoto, M.; Matsuzaki, K.; Katakura, M.; Hara, T.; Tanabe, Y.; Shido, O. Oral intake of encapsulated dried ginger root powder hardly affects human thermoregulatory function, but appears to facilitate fat utilization. Int. J. Biometeorol. 2015, 59, 1461–1474. [Google Scholar] [CrossRef]
- Janssen, P.L.; Meyboom, S.; van Staveren, W.A.; de Vegt, F.; Katan, M.B. Consumption of ginger (Zingiber officinale roscoe) does not affect ex vivo platelet thromboxane production in humans. Eur. J. Clin. Nutr. 1996, 50, 772–774. [Google Scholar]
- Mansour, M.S.; Ni, Y.M.; Roberts, A.L.; Kelleman, M.; Roychoudhury, A.; St-Onge, M.P. Ginger consumption enhances the thermic effect of food and promotes feelings of satiety without affecting metabolic and hormonal parameters in overweight men: A pilot study. Metabolism 2012, 61, 1347–1352. [Google Scholar] [CrossRef]
- Shidfar, F.; Rajab, A.; Rahideh, T.; Khandouzi, N.; Hosseini, S.; Shidfar, S. The effect of ginger (Zingiber officinale) on glycemic markers in patients with type 2 diabetes. J. Complement. Integr. Med. 2015, 12, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Zarezadeh, M.; Saedisomeolia, A.; Khorshidi, M.; Kord Varkane, H.; Makhdoomi Arzati, M.; Abdollahi, M.; Yekaninejad, M.S.; Hashemi, R.; Effatpanah, M.; Honarvar, N.M. Asymmetric dimethylarginine and soluble inter-cellular adhesion molecule-1 serum levels alteration following ginger supplementation in patients with type 2 diabetes: A randomized double-blind, placebo-controlled clinical trial. J. Complement. Integr. Med. 2018, 16, 20180019. [Google Scholar] [CrossRef] [PubMed]
- Rafie Hosseini, S.A.; Hajiani, E.; Saki Malehi, A.; Mard, S.A. Effect of ginger powder supplementation in patients with non-alcoholic fatty liver disease: A randomized clinical trial. Clin. Exp. Gastroenterol. 2020, 13, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Mohammadzadeh Honarvar, N.; Zarezadeh, M.; Khorshidi, M.; Makhdoomi Arzati, M.; Yekaninejad, M.S.; Abdollahi, M.; Effatpanah, M.; Hashemi, R.; Saedisomeolia, A. The effect of an oral ginger supplementation on NF-κB concentration in peripheral blood mononuclear cells and anthropomorphic data of patients with type 2 diabetes: A randomized double-blind, placebo-controlled clinical trial. Complement. Ther. Med. 2019, 42, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Mahluji, S.; Ostadrahimi, A.; Mobasseri, M.; Ebrahimzade Attari, V.; Payahoo, L. Anti-inflammatory effects of Zingiber officinale in type 2 diabetic patients. Adv. Pharm. Bull. 2013, 3, 273–276. [Google Scholar]
- Mahluji, S.; Attari, V.E.; Mobasseri, M.; Payahoo, L.; Ostadrahimi, A.; Golzari, S.E. Effects of ginger (Zingiber officinale) on plasma glucose level, HbA1c and insulin sensitivity in type 2 diabetic patients. Int. J. Food Sci. Nutr. 2013, 64, 682–686. [Google Scholar] [CrossRef] [PubMed]
- Mozaffari-Khosravi, H.; Talaei, B.; Jalali, B.A.; Najarzadeh, A.; Mozayan, M.R. The effect of ginger powder supplementation on insulin resistance and glycemic indices in patients with type 2 diabetes: A randomized, double-blind, placebo-controlled trial. Complement. Ther. Med. 2014, 22, 9–16. [Google Scholar] [CrossRef]
- Ebrahimzadeh Attari, V.; Asghari Jafarabadi, M.; Zemestani, M.; Ostadrahimi, A. Effect of Zingiber officinale supplementation on obesity management with respect to the uncoupling protein 1 -3826A>G and ß3-adrenergic receptor Trp64Arg polymorphism. Phytother. Res. 2015, 29, 1032–1039. [Google Scholar] [CrossRef]
- Hajimoosayi, F.; Jahanian Sadatmahalleh, S.; Kazemnejad, A.; Pirjani, R. Effect of ginger on the blood glucose level of women with gestational diabetes mellitus (GDM) with impaired glucose tolerance test (GTT): A randomized double-blind placebo-controlled trial. BMC Complement. Med. Ther. 2020, 20, 116. [Google Scholar] [CrossRef]
- Ebrahimzadeh Attari, V.; Mahluji, S.; Asghari Jafarabadi, M.; Ostadrahimi, A. Effects of supplementation with ginger (Zingiber officinale Roscoe) on serum glucose, lipid profile and oxidative stress in obese women: A randomized, placebo-controlled clinical trial. Pharm. Sci. 2015, 21, 184–191. [Google Scholar] [CrossRef]
- Ashraf, H.; Heydari, M.; Shams, M.; Zarshenas, M.M.; Tavakoli, A.; Sayadi, M. Efficacy of ginger supplementation in relieving persistent hypothyroid symptoms in patients with controlled primary hypothyroidism: A pilot randomized, double-blind, placebo-controlled clinical trial. Evid. Based Complement. Alt. Med. 2022, 2022, 5456855. [Google Scholar] [CrossRef] [PubMed]
- Arablou, T.; Aryaeian, N.; Valizadeh, M.; Sharifi, F.; Hosseini, A.; Djalali, M. The effect of ginger consumption on glycemic status, lipid profile and some inflammatory markers in patients with type 2 diabetes mellitus. Int. J. Food Sci. Nutr. 2014, 65, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimzadeh Attari, V.; Ostadrahimi, A.; Asghari Jafarabadi, M.; Mehralizadeh, S.; Mahluji, S. Changes of serum adipocytokines and body weight following Zingiber officinale supplementation in obese women: A RCT. Eur. J. Nutr. 2016, 55, 2129–2136. [Google Scholar] [CrossRef]
- Carvalho, G.C.N.; Lira-Neto, J.C.G.; Araújo, M.F.M.; Freitas, R.W.J.F.; Zanetti, M.L.; Damasceno, M.M.C. Effectiveness of ginger in reducing metabolic levels in people with diabetes: A randomized clinical trial. Rev. Lat. Am. Enfermagem. 2020, 28, e3369. [Google Scholar] [CrossRef] [PubMed]
- Khandouzi, N.; Shidfar, F.; Rajab, A.; Rahideh, T.; Hosseini, P.; Mir Taheri, M. The effects of ginger on fasting blood sugar, hemoglobin a1c, apolipoprotein B, apolipoprotein a-I and malondialdehyde in type 2 diabetic patients. Iran. J. Pharm. Res. 2015, 14, 131–140. [Google Scholar] [PubMed]
- Alizadeh-Navaei, R.; Roozbeh, F.; Saravi, M.; Pouramir, M.; Jalali, F.; Moghadamnia, A.A. Investigation of the effect of ginger on the lipid levels. A double blind controlled clinical trial. Saudi Med. J. 2008, 29, 1280–1284. [Google Scholar] [PubMed]
- Bordia, A.; Verma, S.K.; Srivastava, K.C. Effect of ginger (Zingiber officinale Rosc.) and fenugreek (Trigonella foenumgraecum L.) on blood lipids, blood sugar and platelet aggregation in patients with coronary artery disease. Prostaglandins Leukot. Essent. Fatty Acids. 1997, 56, 379–384. [Google Scholar] [CrossRef]
- Gregersen, N.T.; Belza, A.; Jensen, M.G.; Ritz, C.; Bitz, C.; Hels, O.; Frandsen, E.; Mela, D.J.; Astrup, A. Acute effects of mustard, horseradish, black pepper and ginger on energy expenditure, appetite, ad libitum energy intake and energy balance in human subjects. Br. J. Nutr. 2013, 109, 556–563. [Google Scholar] [CrossRef]
- Mohtashami, A. Effects of bread with Nigella Sativa on blood glucose, blood pressure and anthropometric indices in patients with metabolic syndrome. Clin. Nutr. Res. 2019, 8, 138–147. [Google Scholar] [CrossRef]
- Mohtashami, A.; Mahaki, B.; Azadbakht, L.; Entezari, M.H. Effects of bread with Nigella sativa on lipid profiles, apolipoproteins and inflammatory factor in metabolic syndrome patients. Clin. Nutr. Res. 2016, 5, 89–95. [Google Scholar] [CrossRef]
- Pelegrin, S.; Galtier, F.; Chalançon, A.; Gagnol, J.P.; Barbanel, A.M.; Pélissier, Y.; Larroque, M.; Lepape, S.; Faucanié, M.; Gabillaud, I.; et al. Effects of Nigella sativa seeds (black cumin) on insulin secretion and lipid profile: A pilot study in healthy volunteers. Br. J. Clin. Pharmacol. 2019, 85, 1607–1611. [Google Scholar] [CrossRef] [PubMed]
- Bamosa, A.O.; Kaatabi, H.; Lebdaa, F.M.; Elq, A.M.; Al-Sultanb, A. Effect of Nigella sativa seeds on the glycemic control of patients with type 2 diabetes mellitus. Indian J. Physiol. Pharmacol. 2010, 54, 344–354. [Google Scholar] [PubMed]
- Ibrahim, R.M.; Hamdan, N.S.; Ismail, M.; Saini, S.M.; Abd Rashid, S.N.; Abd Latiff, L.; Mahmud, R. Protective effects of Nigella sativa on metabolic syndrome in menopausal women. Adv. Pharm. Bull. 2014, 4, 29–33. [Google Scholar] [PubMed]
- Ibrahim, R.M.; Hamdan, N.S.; Mahmud, R.; Imam, M.U.; Saini, S.M.; Rashid, S.N.; Ghafar, S.A.; Latiff, L.A.; Ismail, M. A randomised controlled trial on hypolipidemic effects of Nigella sativa seeds powder in menopausal women. J. Transl. Med. 2014, 12, 82. [Google Scholar] [CrossRef]
- Badar, A.; Kaatabi, H.; Bamosa, A.; Al-Elq, A.; Abou-Hozaifa, B.; Lebda, F.; Alkhadra, A.; Al-Almaie, S. Effect of Nigella sativa supplementation over a one-year period on lipid levels, blood pressure and heart rate in type-2 diabetic patients receiving oral hypoglycemic agents: Nonrandomized clinical trial. Ann. Saudi Med. 2017, 37, 56–63. [Google Scholar] [CrossRef]
- Qidwai, W.; Hamza, H.B.; Qureshi, R.; Gilani, A. Effectiveness, safety, and tolerability of powdered Nigella sativa (kalonji) seed in capsules on serum lipid levels, blood sugar, blood pressure, and body weight in adults: Results of a randomized, double-blind controlled trial. J. Altern. Complement. Med. 2009, 15, 639–644. [Google Scholar] [CrossRef]
- Farhangi, M.A.; Dehghan, P.; Tajmiri, S.; Abbasi, M.M. The effects of Nigella sativa on thyroid function, serum vascular endothelial growth factor (VEGF)-1, Nesfatin-1 and anthropometric features in patients with Hashimoto’s thyroiditis: A randomized controlled trial. BMC Complement. Altern. Med. 2016, 16, 471. [Google Scholar] [CrossRef]
- Darand, M.; Darabi, Z.; Yari, Z.; Saadati, S.; Hedayati, M.; Khoncheh, A.; Hosseini-Ahangar, B.; Alavian, S.M.; Hekmatdoost, A. Nigella sativa and inflammatory biomarkers in patients with non-alcoholic fatty liver disease: Results from a randomized, double-blind, placebo-controlled, clinical trial. Complement. Ther. Med. 2019, 44, 204–209. [Google Scholar]
- Darand, M.; Darabi, Z.; Yari, Z.; Hedayati, M.; Shahrbaf, M.A.; Khoncheh, A.; Hosseini-Ahangar, B.; Alavian, S.M.; Hekmatdoost, A. The effects of black seed supplementation on cardiovascular risk factors in patients with nonalcoholic fatty liver disease: A randomized, double-blind, placebo-controlled clinical trial. Phytother. Res. 2019, 33, 2369–2377. [Google Scholar] [CrossRef]
- Farhangi, M.A.; Tajmiri, S. The effects of powdered black cumin seeds on markers of oxidative stress, intracellular adhesion molecule (ICAM)-1 and vascular cell adhesion molecule (VCAM)-1 in patients with Hashimoto’s thyroiditis. Clin. Nutr. ESPEN 2020, 37, 207–212. [Google Scholar] [CrossRef]
- Kaatabi, H.; Bamosa, A.O.; Badar, A.; Al-Elq, A.; Abou-Hozaifa, B.; Lebda, F.; Al-Khadra, A.; Al-Almaie, S. Nigella sativa improves glycemic control and ameliorates oxidative stress in patients with type 2 diabetes mellitus: Placebo controlled participant blinded clinical trial. PLoS ONE 2015, 10, e0113486. [Google Scholar] [CrossRef] [PubMed]
- Shirazi, M.; Khodakarami, F.; Feizabad, E.; Ghaemi, M. The effects of Nigella sativa on anthropometric and biochemical indices in postmenopausal women with metabolic syndrome. Endocrine 2020, 69, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Datau, E.A.; Wardhana Surachmanto, E.E.; Pandelaki, K.; Langi, J.A. Efficacy of Nigella sativa on serum free testosterone and metabolic disturbances in central obese male. Acta Med. Indones. 2010, 42, 130–134. [Google Scholar] [PubMed]
- Sabzghabaee, A.M.; Dianatkhah, M.; Sarrafzadegan, N.; Asgary, S.; Ghannadi, A. Clinical evaluation of Nigella sativa seeds for the treatment of hyperlipidemia: A randomized, placebo controlled clinical trial. Med. Arch. 2012, 66, 198–200. [Google Scholar] [CrossRef] [PubMed]
- Akbari, S.; Sohouli, M.H.; Ebrahimzadeh, S.; Ghanaei, F.M.; Hosseini, A.F.; Aryaeian, N. Effect of rosemary leaf powder with weight loss diet on lipid profile, glycemic status, and liver enzymes in patients with nonalcoholic fatty liver disease: A randomized, double-blind clinical trial. Phytother. Res. 2022, 36, 2186–2196. [Google Scholar] [CrossRef] [PubMed]
- Sá, C.M.; Ramos, A.A.; Azevedo, M.F.; Lima, C.F.; Fernandes-Ferreira, M.; Pereira-Wilson, C. Sage tea drinking improves lipid profile and antioxidant defences in humans. Int. J. Mol. Sci. 2009, 10, 3937–3950. [Google Scholar] [CrossRef]
- Darmian, M.A.; Hoseini, R.; Amiri, E.; Golshani, S. How combined and separate aerobic training and turmeric supplementation alter lipid profile and glycemic status? A clinical trial in middle-aged females with type 2 diabetes and hyperlipidemia. Int. Cardiovasc. Res. J. 2021, 15, e118791. [Google Scholar]
- Wickenberg, J.; Ingemansson, S.L.; Hlebowicz, J. Effects of Curcuma longa (turmeric) on postprandial plasma glucose and insulin in healthy subjects. Nutr. J. 2010, 9, 43. [Google Scholar] [CrossRef]
- Maithili Karpaga Selvi, N.; Sridhar, M.G.; Swaminathan, R.P.; Sripradha, R. Efficacy of turmeric as adjuvant therapy in type 2 diabetic patients. Indian J. Clin. Biochem. 2015, 30, 180–186. [Google Scholar] [CrossRef]
- Kandikattu, H.K.; Rachitha, P.; Jayashree, G.V.; Krupashree, K.; Sukhith, M.; Majid, A.; Amruta, N.; Khanum, F. Anti-inflammatory and anti-oxidant effects of cardamom (Elettaria repens (Sonn.) Baill) and its phytochemical analysis by 4D GCXGC TOF-MS. Biomed. Pharmacother. 2017, 91, 191–201. [Google Scholar] [CrossRef]
- Darmian, M.A.; Hoseini, R.; Amiri, E.; Golshani, S. Downregulated hs-CRP and MAD, upregulated GSH and TAC, and improved metabolic status following combined exercise and turmeric supplementation: A clinical trial in middle-aged women with hyperlipidemic type 2 diabetes. J. Diabetes Metab. Disord. 2022, 21, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Adab, Z.; Eghtesadi, S.; Vafa, M.R.; Heydari, I.; Shojaii, A.; Haqqani, H.; Arablou, T.; Eghtesadi, M. Effect of turmeric on glycemic status, lipid profile, hs-CRP, and total antioxidant capacity in hyperlipidemic type 2 diabetes mellitus patients. Phytother. Res. 2019, 33, 1173–1181. [Google Scholar] [CrossRef] [PubMed]
- Navekar, R.; Rafraf, M.; Ghaffari, A.; Asghari-Jafarabadi, M.; Khoshbaten, M. Turmeric supplementation improves serum glucose indices and leptin levels in patients with nonalcoholic fatty liver diseases. J. Am. Coll. Nutr. 2017, 36, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, A.; Selvarajan, S.; Kamalanathan, S.; Kadhiravan, T.; Prasanna Lakshmi, N.C.; Adithan, S. Effect of Curcuma longa on vascular function in native Tamilians with type 2 diabetes mellitus: A randomized, double-blind, parallel arm, placebo-controlled trial. Phytother. Res. 2019, 33, 1898–1911. [Google Scholar] [CrossRef] [PubMed]
- Amin, F.; Islam, N.; Anila, N.; Gilani, A.H. Clinical efficacy of the co-administration of Turmeric and Black seeds (Kalongi) in metabolic syndrome—A double blind randomized controlled trial—TAK-MetS trial. Complement. Ther. Med. 2015, 23, 165–174. [Google Scholar] [CrossRef]
- Lee, M.S.; Wahlqvist, M.L.; Chou, Y.C.; Fang, W.H.; Lee, J.T.; Kuan, J.C.; Liu, H.-Y.; Lu, T.-M.; Xiu, L.; Hsu, C.-C.; et al. Turmeric improves post-prandial working memory in pre-diabetes independent of insulin. Asia Pac. J. Clin. Nutr. 2014, 23, 581–591. [Google Scholar]
- Nieman, D.C.; Cialdella-Kam, L.; Knab, A.M.; Shanely, R.A. Influence of red pepper spice and turmeric on inflammation and oxidative stress biomarkers in overweight females: A metabolomics approach. Plant Foods Hum. Nutr. 2012, 67, 415–421. [Google Scholar] [CrossRef]
- Charron, C.S.; Dawson, H.D.; Albaugh, G.P.; Solverson, P.M.; Vinyard, B.T.; Solano-Aguilar, G.I.; Molokin, A.; Novotny, J.A. A single meal containing raw, crushed garlic influences expression of immunity- and cancer-related genes in whole blood of humans. J. Nutr. 2015, 145, 2448–2455. [Google Scholar] [CrossRef]
- Jarhahzadeh, M.; Alavinejad, P.; Farsi, F.; Husain, D.; Rezazadeh, A. The effect of turmeric on lipid profile, malondialdehyde, liver echogenicity and enzymes among patients with nonalcoholic fatty liver disease: A randomized double blind clinical trial. Diabetol. Metab. Syndr. 2021, 13, 112. [Google Scholar] [CrossRef]
- Yahyazadeh, R.; Ghasemzadeh Rahbardar, M.; Razavi, B.M.; Karimi, G.; Hosseinzadeh, H. The effect of Elettaria cardamomum (cardamom) on the metabolic syndrome: Narrative review. Iran. J. Basic. Med. Sci. 2021, 24, 1462–1469. [Google Scholar]
- Panchal, S.K.; Bliss, E.; Brown, L. Capsaicin in metabolic syndrome. Nutrients 2018, 10, 630. [Google Scholar] [CrossRef] [PubMed]
- Akilen, R.; Tsiami, A.; Devendra, D.; Robinson, N. Cinnamon in glycaemic control: Systematic review and meta analysis. Clin. Nutr. 2012, 31, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Mandal, A.; Kant, R.; Jachak, S.; Jagzape, M. Is cinnamon efficacious for glycaemic control in type-2 diabetes mellitus? J. Pak. Med. Assoc. 2020, 70, 2065–2069. [Google Scholar] [PubMed]
- Silva, M.L.; Bernardo, M.A.; Singh, J.; de Mesquita, M.F. Cinnamon as a complementary therapeutic approach for dysglycemia and dyslipidemia control in type 2 diabetes mellitus and its molecular mechanism of action: A review. Nutrients 2022, 14, 2773. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.; Lu, K.; Cao, X.; Xia, H.; Wang, S.; Sun, G.; Chen, L.; Liao, W. The effect of cinnamon on glycolipid metabolism: A dose-response meta-analysis of randomized controlled trials. Nutrients 2023, 15, 2983. [Google Scholar] [CrossRef]
- Allen, R.W.; Schwartzman, E.; Baker, W.L.; Coleman, C.I.; Phung, O.J. Cinnamon use in type 2 diabetes: An updated systematic review and meta-analysis. Ann. Fam. Med. 2013, 11, 452–459. [Google Scholar] [CrossRef]
- Baker, W.L.; Gutierrez-Williams, G.; White, C.M.; Kluger, J.; Coleman, C.I. Effect of cinnamon on glucose control and lipid parameters. Diabetes Care 2008, 31, 41–43. [Google Scholar] [CrossRef]
- Davis, P.A.; Yokoyama, W. Cinnamon intake lowers fasting blood glucose: Meta-analysis. J. Med. Food 2011, 14, 884–889. [Google Scholar] [CrossRef]
- Deyno, S.; Eneyew, K.; Seyfe, S.; Tuyiringire, N.; Peter, E.L.; Muluye, R.A.; Tolo, C.U.; Ogwang, P.E. Efficacy and safety of cinnamon in type 2 diabetes mellitus and pre-diabetes patients: A meta-analysis and meta-regression. Diabetes Res. Clin. Pract. 2019, 156, 107815. [Google Scholar] [CrossRef]
- Jamali, N.; Kazemi, A.; Saffari-Chaleshtori, J.; Samare-Najaf, M.; Mohammadi, V.; Clark, C.C.T. The effect of cinnamon supplementation on lipid profiles in patients with type 2 diabetes: A systematic review and meta-analysis of clinical trials. Complement. Ther. Med. 2020, 55, 102571. [Google Scholar] [CrossRef]
- Leach, M.J.; Kumar, S. Cinnamon for diabetes mellitus. Cochrane Database Syst. Rev. 2012, 2012, CD007170. [Google Scholar] [CrossRef]
- Ranasinghe, P.; Jayawardana, R.; Galappaththy, P.; Constantine, G.R.; de Vas Gunawardana, N.; Katulanda, P. Efficacy and safety of ‘true’ cinnamon (Cinnamomum zeylanicum) as a pharmaceutical agent in diabetes: A systematic review and meta-analysis. Diabet. Med. 2012, 29, 1480–1492. [Google Scholar] [CrossRef] [PubMed]
- Heydarpour, F.; Hemati, N.; Hadi, A.; Moradi, S.; Mohammadi, E.; Farzaei, M.H. Effects of cinnamon on controlling metabolic parameters of polycystic ovary syndrome: A systematic review and meta-analysis. J. Ethnopharmacol. 2020, 254, 112741. [Google Scholar] [CrossRef]
- Kutbi, E.H.; Sohouli, M.H.; Fatahi, S.; Lari, A.; Shidfar, F.; Aljhdali, M.M.; Alhoshan, F.M.; Elahi, S.S.; Almusa, H.A.; Abu-Zaid, A. The beneficial effects of cinnamon among patients with metabolic diseases: A systematic review and dose-response meta-analysis of randomized-controlled trials. Crit. Rev. Food Sci. Nutr. 2022, 62, 6113–6131. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Huang, W.; He, M.; Yue, R. Effects of cinnamon supplementation on lipid profiles among patients with metabolic syndrome and related disorders: A systematic review and meta-analysis. Complement. Ther. Clin. Pract. 2022, 49, 101625. [Google Scholar] [CrossRef] [PubMed]
- Krittanawong, C.; Isath, A.; Scott, C.Z.; Wang, Z.; Kaplin, S.; Jneid, H.; Lavie, C.J.; Virani, S.S. Association between cinnamon consumption and risk of cardiovascular health: A systematic review and meta-analysis. Am. J. Med. 2022, 135, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Maierean, S.M.; Serban, M.C.; Sahebkar, A.; Ursoniu, S.; Serban, A.; Penson, P.; Banach, M.; Lipid and Blood Pressure Meta-analysis Collaboration (LBPMC) Group. The effects of cinnamon supplementation on blood lipid concentrations: A systematic review and meta-analysis. J. Clin. Lipidol. 2017, 11, 1393–1406. [Google Scholar] [CrossRef]
- Valussi, M. Functional foods with digestion-enhancing properties. Int. J. Food Sci. Nutr. 2012, 63 (Suppl. 1), 82–89. [Google Scholar] [CrossRef]
- Neelakantan, N.; Narayanan, M.; de Souza, R.J.; van Dam, R.M. Effect of fenugreek (Trigonella foenum-graecum L.) intake on glycemia: A meta-analysis of clinical trials. Nutr. J. 2014, 13, 7. [Google Scholar] [CrossRef]
- Askarpour, M.; Alami, F.; Campbell, M.S.; Venkatakrishnan, K.; Hadi, A.; Ghaedi, E. Effect of fenugreek supplementation on blood lipids and body weight: A systematic review and meta-analysis of randomized controlled trials. J. Ethnopharmacol. 2020, 253, 112538. [Google Scholar] [CrossRef]
- Shabil, M.; Bushi, G.; Bodige, P.K.; Maradi, P.S.; Patra, B.P.; Padhi, B.K.; Khubchandani, J. Effect of fenugreek on hyperglycemia: A systematic review and meta-analysis. Medicina 2023, 59, 248. [Google Scholar] [CrossRef] [PubMed]
- Amini, M.R.; Payandeh, N.; Sheikhhossein, F.; Pourreza, S.; Ghalandari, H.; Askarpour, M.; Hekmatdoost, A. The effects of fenugreek seed consumption on blood pressure: A systematic review and meta-analysis of randomized controlled trials. High. Blood Press. Cardiovasc. Prev. 2023, 30, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Correia, A.G.D.S.; Alencar, M.B.; Dos Santos, A.N.; da Paixão, D.C.B.; Sandes, F.L.F.; Andrade, B.; Castro, Y.; de Andrade, J.S. Effect of saffron and fenugreek on lowering blood glucose: A systematic review with meta-analysis. Phytother. Res. 2023, 37, 2092–2101. [Google Scholar] [CrossRef] [PubMed]
- Fakhr, L.; Chehregosha, F.; Zarezadeh, M.; Chaboksafar, M.; Tarighat-Esfanjani, A. Effects of fenugreek supplementation on the components of metabolic syndrome: A systematic review and dose-response meta-analysis of randomized clinical trials. Pharmacol. Res. 2023, 187, 106594. [Google Scholar] [CrossRef]
- Gong, J.; Fang, K.; Dong, H.; Wang, D.; Hu, M.; Lu, F. Effect of fenugreek on hyperglycaemia and hyperlipidemia in diabetes and prediabetes: A meta-analysis. J. Ethnopharmacol. 2016, 194, 260–268. [Google Scholar] [CrossRef]
- Heshmat-Ghahdarijani, K.; Mashayekhiasl, N.; Amerizadeh, A.; Teimouri Jervekani, Z.; Sadeghi, M. Effect of fenugreek consumption on serum lipid profile: A systematic review and meta-analysis. Phytother. Res. 2020, 34, 2230–2245. [Google Scholar] [CrossRef]
- Khodamoradi, K.; Khosropanah, M.H.; Ayati, Z.; Chang, D.; Nasli-Esfahani, E.; Ayati, M.H.; Namazi, N. The effects of fenugreek on cardiometabolic risk factors in adults: A systematic review and meta-analysis. Complement. Ther. Med. 2020, 52, 102416. [Google Scholar] [CrossRef]
- Gadidala, S.K.; Johny, E.; Thomas, C.; Nadella, M.; Undela, K.; Adela, R. Effect of garlic extract on markers of lipid metabolism and inflammation in coronary artery disease (CAD) patients: A systematic review and meta-analysis. Phytother. Res. 2023, 37, 2242–2254. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Missbach, B.; Hoffmann, G. An umbrella review of garlic intake and risk of cardiovascular disease. Phytomedicine 2016, 23, 1127–1133. [Google Scholar] [CrossRef]
- Varshney, R.; Budoff, M.J. Garlic and Heart Disease. J. Nutr. 2016, 146, 416S–421S. [Google Scholar] [CrossRef]
- Sobenin, I.A.; Myasoedova, V.A.; Iltchuk, M.I.; Zhang, D.W.; Orekhov, A.N. Therapeutic effects of garlic in cardiovascular atherosclerotic disease. Chin. J. Nat. Med. 2019, 17, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Westerterp-Plantenga, M.; Diepvens, K.; Joosen, A.M.; Bérubé-Parent, S.; Tremblay, A. Metabolic effects of spices, teas, and caffeine. Physiol. Behav. 2006, 89, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, A.; Husain, A.; Mujeeb, M.; Khan, S.A.; Najmi, A.K.; Siddique, N.A.; Damanhouri, Z.A.; Anwar, F. A review on therapeutic potential of Nigella sativa: A miracle herb. Asian Pac. J. Trop. Biomed. 2013, 3, 337–352. [Google Scholar] [CrossRef]
- Dalli, M.; Bekkouch, O.; Azizi, S.E.; Azghar, A.; Gseyra, N.; Kim, B. Nigella sativa L. phytochemistry and pharmacological activities: A review (2019–2021). Biomolecules 2021, 12, 20. [Google Scholar] [CrossRef]
- Salehi, B.; Quispe, C.; Imran, M.; Ul-Haq, I.; Živković, J.; Abu-Reidah, I.M.; Sen, S.; Taheri, Y.; Acharya, K.; Azadi, H.; et al. Nigella plants—Traditional uses, bioactive phytoconstituents, preclinical and clinical studies. Front. Pharmacol. 2021, 12, 625386. [Google Scholar] [CrossRef] [PubMed]
- Daryabeygi-Khotbehsara, R.; Golzarand, M.; Ghaffari, M.P.; Djafarian, K. Nigella sativa improves glucose homeostasis and serum lipids in type 2 diabetes: A systematic review and meta-analysis. Complement. Ther. Med. 2017, 35, 6–13. [Google Scholar] [CrossRef]
- Sahebkar, A.; Soranna, D.; Liu, X.; Thomopoulos, C.; Simental-Mendia, L.E.; Derosa, G.; Maffioli, P.; Parati, G. A systematic review and meta-analysis of randomized controlled trials investigating the effects of supplementation with Nigella sativa (black seed) on blood pressure. J. Hypertens. 2016, 34, 2127–2135. [Google Scholar] [CrossRef]
- Askari, G.; Rouhani, M.H.; Ghaedi, E.; Ghavami, A.; Nouri, M.; Mohammadi, H. Effect of Nigella sativa (black seed) supplementation on glycemic control: A systematic review and meta-analysis of clinical trials. Phytother. Res. 2019, 33, 1341–1352. [Google Scholar] [CrossRef]
- Hallajzadeh, J.; Milajerdi, A.; Mobini, M.; Amirani, E.; Azizi, S.; Nikkhah, E.; Bahadori, B.; Sheikhsoleimani, R.; Mirhashemi, S.M. Effects of Nigella sativa on glycemic control, lipid profiles, and biomarkers of inflammatory and oxidative stress: A systematic review and meta-analysis of randomized controlled clinical trials. Phytother. Res. 2020, 34, 2586–2608. [Google Scholar] [CrossRef]
- Kavyani, Z.; Musazadeh, V.; Golpour-Hamedani, S.; Moridpour, A.H.; Vajdi, M.; Askari, G. The effect of Nigella sativa (black seed) on biomarkers of inflammation and oxidative stress: An updated systematic review and meta-analysis of randomized controlled trials. Inflammopharmacology 2023, 31, 1149–1165. [Google Scholar] [CrossRef]
- Montazeri, R.S.; Fatahi, S.; Sohouli, M.H.; Abu-Zaid, A.; Santos, H.O.; Găman, M.A.; Shidfar, F. The effect of Nigella sativa on biomarkers of inflammation and oxidative stress: A systematic review and meta-analysis of randomized controlled trials. J. Food Biochem. 2021, 45, e13625. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, S.M.; Sheikhi, A.; Varkaneh, H.K.; Zarezadeh, M.; Rahmani, J.; Milajerdi, A. Effect of Nigella sativa supplementation on obesity indices: A systematic review and meta-analysis of randomized controlled trials. Complement. Ther. Med. 2018, 38, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Namazi, N.; Larijani, B.; Ayati, M.H.; Abdollahi, M. The effects of Nigella sativa L. on obesity: A systematic review and meta-analysis. J. Ethnopharmacol. 2018, 219, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Tang, G.; Zhang, L.; Tao, J.; Wei, Z. Effect of Nigella sativa in the treatment of nonalcoholic fatty liver disease: A systematic review and meta-analysis of randomized controlled trials. Phytother. Res. 2021, 35, 4183–4193. [Google Scholar] [CrossRef]
- Tavakoly, R.; Arab, A.; Vallianou, N.; Clark, C.C.T.; Hadi, A.; Ghaedi, E.; Ghavami, A. The effect of Nigella sativa L. supplementation on serum C-reactive protein: A systematic review and meta-analysis of randomized controlled trials. Complement. Ther. Med. 2019, 45, 149–155. [Google Scholar] [CrossRef]
- Rolfe, V.; Mackonochie, M.; Mills, S.; MacLennan, E. Turmeric/curcumin health outcomes: A meta-review of systematic reviews. Eur. J. Integr. Med. 2020, 40, 101252. [Google Scholar] [CrossRef]
- Dei Cas, M.; Ghidoni, R. Dietary curcumin: Correlation between bioavailability and health potential. Nutrients 2019, 11, 2147. [Google Scholar] [CrossRef]
- Sahebkar, A. Are curcuminoids effective C-reactive protein-lowering agents in clinical practice? Evidence from a meta-analysis. Phytother. Res. 2014, 28, 633–642. [Google Scholar] [CrossRef]
- Sakkas, H.; Papadopoulou, C. Antimicrobial activity of basil, oregano, and thyme essential oils. J. Microbiol. Biotechnol. 2017, 27, 429–438. [Google Scholar] [CrossRef]
- El-Kased, R.F.; El-Kersh, D.M. GC-MS profiling of naturally extracted essential oils: Antimicrobial and beverage preservative actions. Life 2022, 12, 1587. [Google Scholar] [CrossRef]
- Wightman, E.L.; Reay, J.L.; Haskell, C.F.; Williamson, G.; Dew, T.P.; Kennedy, D.O. Effects of resveratrol alone or in combination with piperine on cerebral blood flow parameters and cognitive performance in human subjects: A randomised, double-blind, placebo-controlled, cross-over investigation. Br. J. Nutr. 2014, 112, 203–213. [Google Scholar] [CrossRef] [PubMed]
- Ajazuddin; Alexander, A.; Qureshi, A.; Kumari, L.; Vaishnav, P.; Sharma, M.; Saraf, S.; Saraf, S. Role of herbal bioactives as a potential bioavailability enhancer for active pharmaceutical ingredients. Fitoterapia 2014, 97, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Chiavaroli, L.; Lee, D.; Ahmed, A.; Cheung, A.; Khan, T.A.; Blanco, S.; Mirrahimi, A.; Jenkins, D.J.A.; Livesey, G.; Wolever, T.M.S.; et al. Effect of low glycaemic index or load dietary patterns on glycaemic control and cardiometabolic risk factors in diabetes: Systematic review and meta-analysis of randomised controlled trials. BMJ 2021, 374, n1651. [Google Scholar] [CrossRef] [PubMed]
- Mensink, R.P.; Aro, A.; Den Hond, E.; German, J.B.; Griffin, B.A.; ten Meer, H.-U.; Mutanen, M.; Pannemans, D.; Stahl, W. PASSCLAIM–Diet-related cardiovascular disease. Eur. J. Nutr. 2003, 42 (Suppl. 1), 1/6–1/27. [Google Scholar] [CrossRef] [PubMed]
- Edmands, W.M.; Ferrari, P.; Rothwell, J.A.; Rinaldi, S.; Slimani, N.; Barupal, D.K.; Biessy, C.; Jenab, M.; Clavel-Chapelon, F.; Fagherazzi, G.; et al. Polyphenol metabolome in human urine and its association with intake of polyphenol-rich foods across European countries. Am. J. Clin. Nutr. 2015, 102, 905–913. [Google Scholar] [CrossRef]
- Shahwan, M.; Alhumaydhi, F.; Ashraf, G.M.; Hasan, P.M.Z.; Shamsi, A. Role of polyphenols in combating type 2 diabetes and insulin resistance. Int. J. Biol. Macromol. 2022, 206, 567–579. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Herb or Spice | Reference | Study Type | Population | Dose and Formulation | Length of Intervention | Findings | Study Quality |
|---|---|---|---|---|---|---|---|
| Cardamom | [27] | Single-blind clinical trial | 20 individuals with hypertension | 3 g/day in capsules | 12 weeks | BP decreased and fibrinolytic activity increased. Fibrinogen and lipid levels did not change. | Low |
| [28] | Double-blind RCT | 80 prediabetic subjects | 3 g/day in capsules | 8 weeks | Inflammatory markers CRP, CRP:IL-6 ratio and oxidative stress marker MDA were all decreased. | High | |
| [29] | Double-blind RCT | 83 overweight or obese diabetic pts | 3 g/day in capsules | 10 weeks | There was an improvement in HbA1c, insulin control and TG and an increase in Sirt1. Cholesterol levels did not change. | High | |
| [30] | Double-blind RCT | 87 overweight or obese pts with NAFLD | 3 g/day in capsules | 12 weeks | Cardamom improved fatty liver grade, blood glucose, lipids and irisin, but BMI, total cholesterol and FBG were not changed. | High | |
| [31] | Double-blind RCT | 83 pts with type 2 diabetes | 3 g/day in capsules | 10 weeks | Cardamom led to a decrease in CRP and systolic BP, and an increase in serum NO. Serum ADMA and diastolic BP did not change. | High | |
| [32] | Double-blind RCT | 83 overweight pts with type 2 diabetes | 3 g/day in capsules | 10 weeks | VCAM, ICAM, E-selectin and IL-6 were decreased in the cardamom group. MMP-9 and CD163 levels were unchanged. | High | |
| [33] | Double-blind RCT | 87 pts with NAFLD | 3 g/day in capsules | 12 weeks | Cardamom increased Sirt1 and decreased inflammatory markers hs-CRP, IL-6, TNFα and liver marker ALT, as well as improving the degree of fatty liver. Weight, BMI and AST did not change. | High | |
| [34] | Double-blind RCT | 194 obese women with PCOS | 3 g/day in capsules | 16 weeks | Anthropometric indices decreased. Glycemic indices and androgen hormones improved. | High | |
| [35] | Double-blind RCT | 194 obese women with PCOS | 3 g/day in capsules | 16 weeks | LH, androstenedione and dehydroepiandrosterone were decreased. FSH increased. Inflammatory markers TNFα, IL-6 and CRP were decreased. | High | |
| Chilli | [36] | Cross-over clinical trial | 7 healthy volunteers | 30 g fresh chilli | Single dose | A combination of chilli and medium-chain TG increased diet-induced thermogenesis. | Low |
| [37] | Randomised cross-over study | 36 healthy participants | 30 g/day chilli in food | 8 weeks | When participants with a BMI > 26 consumed a chilli-containing meal after 4 weeks of daily chilli, there was reduced C-peptide and insulin and higher hepatic clearance of insulin. But blood glucose and energy expended were not changed. | High | |
| [38] | Randomised cross-over study | 27 healthy adults | 30 g/day chilli in food | 8 weeks | Consumption of chilli increased the resistance of lipoproteins to oxidation, but had no effect on serum lipids, lipoproteins and total antioxidant score. | Low | |
| [39] | Randomised cross-over study | 36 healthy participants | 30 g/day chilli in food | 8 weeks | There were no effects on metabolic or vascular parameters (glucose, lipids, BP, insulin). However, in men, chilli decreased resting heart rate and increased myocardial perfusion time. | High | |
| [9] | Randomised cross-over study | 34 healthy overweight volunteers | Meal containing chilli with 5.82 mg total capsaicinoids | Single dose | Chilli decreased post-prandial insulin when added to a meal. Metabolic rate, core temperature, CRP and microvascular reactivity were unchanged. | Low | |
| [40] | Cross-over clinical trial | 40 healthy adults | 0.6 g in food | Single dose | Eating a meal with chilli in increased the desire to eat sweet food, but had no impact on energy intake | Low | |
| [41] | Randomised cross-over study | 12 healthy adults | 10 mg capsaicinoids/day in capsules | 5 weeks | There was no change in anthropometric and metabolic measurements from chilli consumption. Chilli increased the firmicutes/bacteroidetes ratio and faecalibacterium abundance that coincided with the increase in plasma levels of GLP-1 and GIP and the decrease in plasma ghrelin level. Benefits were linked to gut enterotypes. | Low | |
| [42] | Double-blind RCT | 42 pregnant women with gestational diabetes | 1.25 g/day added to food | 4 weeks | Postprandial glucose, insulin and insulin resistance were reduced by chilli. Serum cholesterol and triglyceride were also reduced by chilli. Serum calcitonin gene-related peptide was increased by chilli. When the babies were born, chilli had reduced the incidence of large-for-gestational age newborns. | High | |
| [43] | Cross-over clinical trial | 12 healthy adults | 5 g in capsules | Single dose | When 5 g of chilli was administered in a capsule after a glucose challenge, plasma glucose levels were lower after 30 and 45 min than those in the placebo group. Insulin levels in the chilli group were higher than in the placebo group at 1 and 2 h after glucose challenge. | Low | |
| [44] | Single-blind, randomised, cross-over trial | 14 healthy volunteers | 3.09 g/day in food | 36 h | Chilli increased fat oxidation and prevented reductions in sleeping metabolic rate, diet-induced thermogenesis or resting energy expenditure that were caused by restricting food intake. This indicates a potential beneficial effect in dieting individuals. There was no effect of chilli on BP. | Low | |
| [45] | Single-blinded, randomised, cross-over design | 15 healthy adults | 3.09 g/day in food | 36 h | Chilli decreased the desire to eat and increased satiety and fullness, particularly when participants under-ate. | Low | |
| Cinnamon | [46] | Single-blind randomised cross-over study | 8 sedentary, healthy males | 3 g/day in capsules | 2 weeks | Cinnamon reduced glucose response to a glucose challenge and improved insulin sensitivity, but effects were not long-lasting once cinnamon consumption ceased. | High |
| [47] | Double-blind RCT | 25 post-menopausal women with type 2 diabetes | 1.5 g/day in capsules | 7 weeks | Cinnamon did not improve fasting plasma glucose or insulin concentrations, whole-body oral glucose tolerance or blood lipid profiles. | Low | |
| [48] | Randomised cross-over study | 7 lean, healthy adults | 5 g in capsules | Single dose | Cinnamon reduced plasma glucose responses to glucose tolerance tests and improved insulin sensitivity. | Low | |
| [49] | Randomised cross-over study | 15 healthy adults | 1 or 3 g/day in food | Single dose | Ingestion of 3 g cinnamon reduced postprandial serum insulin and increased GLP-1 concentrations without affecting blood glucose, GIP, the ghrelin concentration, satiety or GER in healthy subjects. Amounts of 1 g did not have an effect. | High | |
| [50] | Single-blind randomised cross-over study | 9 healthy young adults | 3 g in capsules | Single dose | Amounts of 3 g cinnamon did not alter the postprandial response to a high-fat test meal. No change in gastric emptying, glucose response, arterial function, oxidative stress or appetite. | High | |
| [51] | Double-blind cross-over RCT | 10 individuals with impaired glucose tolerance | 6 g in capsules | Single dose | No differences in glucose or insulin responses compared with placebo. | High | |
| [52] | Double-blind cross-over RCT | 10 young, sedentary obese women | 5 g in capsules | Single dose | Peak blood glucose was lower in the cinnamon group, but blood insulin and insulin sensitivity/resistance were not affected. | High | |
| [53] | Double-blind RCT | 26 pts with type 2 diabetes | 1 g/day in capsules | 12 weeks | Cinnamon reduced FBG by 6 weeks and this was maintained for the whole 12 weeks of the study. The decrease in HbA1c was not significant. Serum glutathione and superoxide dismutase were increased by cinnamon at 12 weeks, while MDA was reduced, indicating an overall antioxidant effect. | Low | |
| [54] | Randomised cross-over study | 30 healthy obese or normal weight individuals | 6 g powder in food | Single dose | Cinnamon reduced blood glucose in obese and healthy weight individuals. | Low | |
| [55] | Randomised clinical trial | 30 healthy adults | 100 mL cinnamon tea | Single dose | Cinnamon decreased postprandial maximal glucose level. | Low | |
| [56] | Crossover clinical study | 14 healthy individuals | 6 g powder in food | Single dose | Cinnamon reduced the postprandial glucose response and the gastric emptying rate. | Low | |
| [57] | Randomised crossover study | 10 healthy individuals | 6 g in food | Single dose | Cassia cinnamon, but not Ceylon cinnamon, reduced postprandial insulin and glucose responses. | Low | |
| [58] | Double-blind RCT | 45 women with PCOS | 1.5 g/day in capsules | 24 weeks | Menstrual cyclicity improved for women taking cinnamon with no effect on insulin resistance or serum androgens. | High | |
| [59] | Single-blind RCT | 109 adults with diabetes | 1 g/day in capsules | 12 weeks | Cinnamon lowered HbA1c. | High | |
| [60] | Single-blind RCT | 60 pts with type 2 diabetes | 1.5 g/day | 12 weeks | Cinnamon had no impact on fasting plasma glucose, HbA1c or serum lipids. | ||
| [61] | Double-blind RCT | 43 individuals with diabetes | 1 g/day in capsules | 12 weeks | Cinnamon produced no significant change in fasting glucose, lipid, A1C or insulin levels. | High | |
| [62] | Double-blind RCT | 50 pts with NAFLD | 1.5 g/day in capsules | 12 weeks | There were decreases in HOMA index, fasting blood glucose, total cholesterol, triglyceride, ALT, AST, GGT and high-sensitivity CRP with cinnamon. | High | |
| [63] | Double-blind RCT | 39 adults with diabetes | 3 g/day in capsules | 8 weeks | Cinnamon had no effect on glycaemic and inflammatory markers. | High | |
| [64] | Double-blind RCT | 44 adults with diabetes | 3 g/day in capsules | 8 weeks | Cinnamon had no effect on soluble vascular adhesion molecules. | High | |
| [65] | Single-blind RCT | 40 women with PCOS | 1.5 g of Ceylon cinnamon in capsules | 8 weeks | There was an improvement in cyclicity with cinnamon, which was equivalent to metformin. No change in fasting blood glucose or serum progesterone or androgen levels. | High | |
| [66] | Double-blind RCT | 39 adults with diabetes | 3 g/day in capsules | 8 weeks | Cinnamon had no effect on inflammatory markers. | High | |
| [67] | Double-blind RCT | 57 adolescents with diabetes | 1 g/day in capsules | 12 weeks | Cinnamon had no effect on A1c or insulin sensitivity. | High | |
| [68] | Double-blind RCT | 58 pts with type 2 diabetes | 2 g/day in capsules | 12 weeks | Intake of 2 g of cinnamon reduced the HbA1c, SBP and DBP among poorly controlled type 2 diabetes pts | High | |
| [69] | Double-blind RCT | 59 adults with type 2 diabetes | 1.2 g/day in capsules | 12 weeks | There was no significant change in SBP from baseline when cinnamon was compared with placebo. | High | |
| [70] | Double-blind RCT | 136 individuals with type 2 diabetes | 1.5 g/day in capsules | 90 days | HbA1c was reduced by cinnamon, but there was no effect on FBG. | High | |
| [71] | Double-blind RCT | 61 pts with type 2 diabetes | 2 g/day in capsules | 8 weeks | Cinnamon did not improve FBG, HbA1c, blood lipids. | High | |
| [72] | Double-blind RCT | 84 overweight individuals with PCOS | 1.5 g/day in capsules | 8 weeks | Cinnamon increased serum antioxidant capacity and improved total cholesterol, LDL and HDL. | High | |
| [73] | Double-blind RCT | 84 overweight individuals with PCOS | 1.5 g in capsules | 8 weeks | Cinnamon decreased serum FBG, insulin, homeostatic model assessment for insulin resistance, total cholesterol and LDL-cholesterol and weight and increased HDL-cholesterol compared with placebo. | High | |
| [74] | Triple-blind RCT | 105 pts with type 2 diabetes | 1 g/day in capsules | 12 weeks | Cinnamon improved glucose control and reduced BMI. | High | |
| [75] | Double-blind RCT | 115 pts with type 2 diabetes | 0.5 g/day in capsules | 12 weeks | Cinnamon reduced FBG, HbA1c and hepatic enzymes. Probiotics were also effective. | High | |
| [76] | Double-blind RCT | 60 people with type 2 diabetes | 1, 3, or 6 g/day in capsules | 40 days | Intake of 1, 3 or 6 g of cinnamon per day reduces serum glucose, triglyceride, LDL-cholesterol and total cholesterol in people with type 2 diabetes. | High | |
| [77] | Double-blind RCT | 116 Asian Indians with MetS | 3 g/day | 16 weeks | FBG, HbA1c, waist circumference and BMI were reduced by cinnamon. Waist–hip ratio, BP, serum total cholesterol, LDL-cholesterol, serum triglycerides and HDL-cholesterol were also improved. | High | |
| [78] | Triple-blind RCT | 160 people with type 2 diabetes | 3 g/day | 12 weeks | Cinnamon reduced HbA1c and blood glucose. | High | |
| [79] | Triple-blind RCT | 140 pts with diabetes | 1 g/day | 12 weeks | Cinnamon supplementation led to improvement in all anthropometric (BMI, body fat and visceral fat), glycemic (FBG, 2hpp, HbA1C, fasting insulin and insulin resistance) and lipids (cholesterol, LDL-c and HDL-c) outcomes (except for triglycerides). | High | |
| [80] | Double-blind RCT | 59 women with PCOS | 1.5 g/day | 12 weeks | Fasting insulin, HOMA-IR, LDL and HDL were reduced in the cinnamon group. Changes in blood sugar, serum androgen levels and anthropometric measures were not significant. | High | |
| [81] | Open, randomised, cross-over clinical trial | 21 healthy volunteers | 2 g in 200 mL hot water | Single dose | No difference in energy expenditure, dietary-induced thermogenesis, hunger fullness and desire to eat. However, cinnamon tea decreased satiety and increased food intake in the subsequent meal. | Low | |
| [82] | Randomised cross-over study | 18 healthy adults | 4 g | Single dose | Cinnamon decreased blood glucose and satiety 15 min after test meal, but did not decrease blood sugar overall. | Low | |
| Cinnamon and ginger | [83] | Double-blind RCT | 83 women with PCOS | 1.5 g of cinnamon or ginger | 8 weeks | Cinnamon and ginger both decreased weight and BMI. Insulin resistance decreased, but only in the cinnamon group. FSH and LH decreased in the ginger group, while testosterone was reduced in the cinnamon group. | High |
| Cinnamon, cardamom, saffron, ginger | [84] | Single-blind RCT | 208 pts with type 2 diabetes | 3 g | 8 weeks | No difference in BP, serum soluble (s)ICAM-1 concentrations and anthropometric measures. | High |
| Cumin | [85] | Randomised clinical trial | 88 overweight/obese women | 6 g/day | 12 weeks | Cumin powder reduced serum levels of fasting cholesterol, triglyceride and LDL and increased HDL. Weight, BMI, waist circumference, fat mass and its percentage significantly reduced. | High |
| Cumin and cinnamon | [86] | Double-blind RCT | 99 women with dyslipidemia | 3 g/day | 8 weeks | Cumin and cinnamon both significantly reduced total cholesterol compared with placebo. Differences in triglycerides, HDL and LDL were not significant. | High |
| Fennel and fenugreek | [87] | Single-blinded cross-over trial | 9 healthy women | 2 g fennel infused in 250 mL of water and strained. 24 g of fenugreek, infused in 250 mL of water and strained. | Single dose (with 1-week washout between each arm of the study) | Both fennel and fenugreek increased feelings of fullness and decreased desire to eat food; however, there were no changes in amount of food consumed after drinking either tea compared with placebo tea. | Low |
| Fenugreek | [88] | Clinical trial | 20 adults with hypercholesterolemia | 12.5–18 g/day | 4 weeks | Total cholesterol and LDL cholesterol decreased at both doses. | Low |
| [89] | Clinical trial | pts with type 1 diabetes | 100 g/day | 10 days | Fenugreek reduced fasting blood sugar, improved glucose tolerance and reduced LDL, total cholesterol and triglycerides. | ||
| [90] | Clinical trial | Type 2 diabetics | 15 g | Single dose | Postprandial glucose was decreased, but there was no impact on insulin or lipids. | ||
| [91] | Double-blind RCT | 13 healthy volunteers | 3 g/day | 10 days | Fenugreek improved glucose tolerance and insulin sensitivity (as shown by reduction in melanin-concentrating hormone). | High | |
| [92] | Double-blind cross-over RCT | 10 healthy volunteers and 6 pts with type 2 diabetes | Bread with 10% fenugreek | Single dose | Adding fenugreek (1 part to 9 parts of wheat flour) reduced the glycaemic response and GI of bread in both healthy volunteers and diabetics. | Low | |
| [93] | Clinical trial | 18 pts with type 2 diabetes | 10 g/day | 8 weeks | FBS, TG and VLDL-C decreased (25%, 30% and 30.6%, respectively) after taking fenugreek seed soaked in hot water whereas there were no changes in lab parameters in cases who consumed it mixed with yoghurt. | Low | |
| [94] | Double-blind RCT | 8 pts with diabetes | 5.6 g in bread | Single dose | Blood glucose was not changed, but total insulin concentration decreased. | High | |
| [95] | Randomised cross-over study | 10 healthy adults | Bread with 10% fenugreek | Single dose | Adding fenugreek reduced the glycaemic response and GI of bread. | Low | |
| [96] | Randomised clinical trial | 12 pts with uncontrolled diabetes | 2 g/day | 12 weeks | Blood glucose was not changed, but fasting insulin level increased. The ratio of HDL:LDL decreased. | Low | |
| [97] | Parallel randomised study | 48 pts with type 2 diabetes | 15 g/day fenugreek powder | 8 weeks | Fenugreek decreased CRP and increased superoxide dismutase. There was no effect on glutathione peroxidase activity, total antioxidant capacity, IL-6 or TNFα. | High | |
| [98] | Clinical trial | 60 type 2 diabetics | 25 g/day | 24 weeks | Serum cholesterol and triglyceride were reduced. | Low | |
| [99] | Cross-sectional observational study | 25 pts with type 2 diabetes | 5 g/day | 12 weeks | Fasting blood glucose was decreased by month 2. Postprandial blood glucose level was lower by month 3. | ||
| [100] | Parallel randomised study | 50 pts with type 2 diabetes | 15 g/day fenugreek powder | 8 weeks | Fenugreek decreased fasting blood glucose, and liver enzymes, serum ALT and alkaline phosphatase, compared with baseline. Compared with control group, SBP, AST and irisin (a marker of metabolic health) were decreased. | High | |
| [101] | RCT | 114 pts with type 2 diabetes | 50 g/day | 4 weeks | Fenugreek improved lipid metabolism. | Low | |
| [102] | Double-blind RCT | 56 adults with borderline hyperlipidemia | 8 g/day | 8 weeks | TG, LDL, total cholesterol and FBG were decreased by fenugreek. | High | |
| [103] | Triple-blind RCT | 88 pts with type 2 diabetes | 10 g/day | 8 weeks | Fenugreek seeds decreased FBG and HbA1c, serum levels of insulin, HOMA-IR, total cholesterol and TG and increased serum levels of adiponectin. | High | |
| [104] | Double-blind RCT | 125 pts with type 2 diabetes | 10 g/day | 8 weeks | Fenugreek alone and fenugreek combined with nutrition training decreased FBG, HbA1c, BMI and waist circumference compared with placebo. | High | |
| [105] | Double-blind RCT | 62 pts with type 2 diabetes | 10 g/day fenugreek powder | 8 weeks | Fenugreek improved mean FBG, HgA1C, BMI, waist circumference, DBP and quality of life | High | |
| [106] | Randomised cross-over study | 8 healthy individuals | 25 g | single dose | Fenugreek seeds reduced the rise in blood glucose and insulin caused by a meal. | Low | |
| Garlic | [107] | Clinical trial | 40 pts with MetS | 100 mg/kg bodyweight crushed garlic | 4 weeks | Raw crushed garlic reduced waist circumference, SBP and DBP, TG, FBG and significantly increased serum HDL cholesterol. There was no significant difference found in BMI. | Low |
| [108] | Clinical trial | 4 healthy adults | 40 g fresh garlic | 1 week | Garlic reduced the serum cholesterol and triglycerides when consumed with a high-fat diet. | Low | |
| [109] | Clinical trial | 20 healthy individuals | 3 g/day | 90 days | Garlic reduced total cholesterol and LDL, but had no impact on total bacterial faecal count. | ||
| [110] | Single-blind randomised cross-over study | 18 healthy volunteers | 4.2 g | 1 week | Baseline values of platelet function were within normal range in all volunteers. Platelet function was not impaired by single and repeated oral consumption of Greek tsatsiki containing raw garlic. | Low | |
| [111] | Randomised clinical trial | 112 hyperlipidemic pts | 20 g/day | 8 weeks | Garlic and a combination of garlic and lemon reduced blood lipids (total cholesterol, TG and LDL) and BP, while increasing HDL. | Low | |
| [112] | Double-blind RCT | 90 overweight smokers | 2.1 g/day | 12 weeks | Garlic had no effect on inflammatory biomarkers, endothelial function or lipid profile in normolipidemic subjects with risk factors for CVD. | High | |
| [113] | Double-blind RCT | 90 pts with NAFLD | 1.6 g/day | 12 weeks | Garlic decreased hepatic steatosis, liver enzymes and blood lipids (total cholesterol, TG, HDL and LDL). | High | |
| [114] | Double-blind RCT | 90 pts with NAFLD | 1.6 g/day | 12 weeks | Waist circumference, body fat, FBG, insulin and insulin resistance improved. Skeletal muscle mass increased and antioxidant capacity increased. | High | |
| [115] | Double-blind RCT | 90 pts with MetS | 1.6 g/day | 12 weeks | Garlic increased HDL. There were decreases in waist circumference, BP, TG, insulin and appetite. | High | |
| Garlic and coriander seed | [116] | Single-blind RCT | 80 pts with hyperlipidemia | 2 g/day | 40 days | Garlic and coriander improved BMI, total cholesterol, HDL and LDL. Garlic powder was more effective than coriander | Low |
| Ginger | [117] | Double-blind RCT | 160 obese children with NAFLD | 1 g/day | 12 weeks | Serum FBG and CRP, BMI, waist circumference, AST, hepatic steatosis, total cholesterol and LDL decreased with ginger. | High |
| [118] | Placebo-controlled study | 23 healthy male volunteers | 1 g | Single dose | Ginger had no effect on thermoregulatory function, but increased fat utilisation in the morning. | High | |
| [119] | Randomised cross-over study | 18 healthy volunteers | 15 g raw ginger or 40 g cooked ginger | 2 weeks | Ginger did not affect thromboxane production. | High | |
| [120] | Randomised cross-over study | 10 healthy men | 2 g | 2 days | Ginger enhanced thermogenesis and reduced hunger and food intake. | Low | |
| [121] | Double-blind RCT | 20 60-year-old pts with diabetes | 3 g | 12 weeks | Improvements found in blood glucose, insulin resistance, inflammatory and oxidative markers (CRP and MDA). | High | |
| [122] | Double-blind RCT | 45 diabetic pts | 2 g/day | 10 weeks | Ginger supplementation decreased ADMA serum levels (although this change was not significantly different to placebo), but had no effect on sICAM-1. | High | |
| [123] | Double-blind RCT | 50 pts with NAFLD | 1.5 g/day of ginger | 12 weeks | No difference between ginger and placebo for anthropometric measurements or liver markers. However, FBG and insulin resistance were improved by ginger. Serum lipids (total cholesterol and LDL) and CRP decreased in the ginger group. | High | |
| [124] | Double-blind RCT | 45 diabetic pts | 2 g/day | 10 weeks | No effect of ginger on anthropometric measurements or NFκB | High | |
| [125] | Double-blind RCT | 64 pts with type 2 diabetes | 2 g/day | 8 weeks | TNFα and hs-CRP were reduced by ginger. IL-6 was reduced by ginger compared with baseline, but not compared with placebo. | High | |
| [126] | Double-blind RCT | 64 pts with diabetes | 2 g/day | 8 weeks | Ginger supplementation significantly lowered the levels of insulin, LDL-cholesterol, TG and the HOMA index and increased the QUICKI index, but had no effect on FBG, total cholesterol, HDL-C and HbA1c. | High | |
| [127] | Double-blind RCT | 88 diabetics | 3 g/day | 8 weeks | Ginger improved fasting blood glucose, insulin levels and insulin sensitivity. | High | |
| [128] | Double-blind RCT | 80 healthy obese women | 2 g/day | 12 weeks | Ginger decreased anthropometric measurements and appetite. | High | |
| [129] | Double-blind RCT | 70 women with gestational diabetes | 1.5 g/day | 6 weeks | Ginger treatment reduced the levels of FBS, serum insulin and HOMA index, but did not affect postprandial blood sugar. | High | |
| [130] | Double-blind RCT | 70 Obese women | 2 g/day | 12 weeks | Ginger reduced blood glucose, total cholesterol, TG and LDL/HDL, while increasing MDA and HDL. Body weight, waist circumference and BMI were also reduced without any difference in energy and macronutrient intake between groups. | High | |
| [131] | Pilot double-blind RCT | 60 hypothyroid pts with normal serum TSH | 1 g/day | 30 days | Ginger reduced the thyroid symptom score. Additionally, weight gain, cold intolerance, constipation, dry skin, appetite, memory loss, concentration disturbance and feeling giddy or dizzy domains also improved. Ginger supplementation also led to a decrease in body weight, BMI, waist circumference, serum TSH, FBG, TG, and total cholesterol levels compared to the placebo. | High | |
| [132] | Double-blind RCT | 70 pts with type 2 diabetes | 1.6 g | 12 weeks | Ginger reduced multiple markers of metabolic health (blood glucose, insulin, insulin resistance, cholesterol) and inflammation (CRP and prostaglandin). | High | |
| [133] | Double-blind RCT | 80 Obese women | 2 g | 12 weeks | There was a reduction in BMI, serum insulin and HOMA-IR. | High | |
| [134] | Double-blind RCT | 103 pts with diabetes | 1.2 g/day | 12 weeks | Ginger reduced fasting blood glucose and total cholesterol. | High | |
| [135] | Double-blind RCT | 41 pts with type 2 diabetes | 2 g/day | 12 weeks | Ginger supplementation reduced the levels of fasting blood sugar, HbA1c, apolipoprotein B, apolipoprotein B/apolipoprotein A-I and MDA in the ginger group in comparison to baseline, as well as the control group, while it increased the level of apolipoprotein A-I. | High | |
| [136] | Double-blind RCT | 85 pts with hyperlipidemia | 3 g/day | 45 days | TG and cholesterol levels were lower in the ginger group than placebo. Changes in LDL and HDL were not significant between the two groups. | High | |
| Ginger and fenugreek | [137] | Placebo-controlled study | 30 pts with coronary artery disease and 30 healthy individuals | 4 g/day or 10 g one-off dose of ginger. 5 g/day fenugreek | 12 weeks | Ginger did not affect platelet aggregation when given at 4 g/day, but 10 g single dose reduced platelet aggregation. Ginger had no effect on blood sugar or blood lipids. Fenugreek had no effect on cholesterol, TG or blood sugar in healthy individuals, but reduced cholesterol and triglycerides in pts with coronary artery disease and diabetes. | Low |
| Mustard, black pepper, ginger, horseradish | [138] | Single-blind cross-over trial | 22 young, healthy males | 20 g ginger or 1.3 g of black pepper | Single dose | Ginger and black pepper had no effect on appetite, energy intake or diet-induced thermogenesis. | High |
| Nigella seeds | [139] | Double-blind cross-over RCT | 51 pts with MetS | 3 g/day | 8 weeks | Nigella had no effect on BP, weight, waist circumference, FBG and BMI. | High |
| [140] | Double-blind cross-over RCT | 51 pts with MetS | 3 g/day | 8 weeks | No effect of nigella on blood lipids, apolipoproteins and inflammatory factor. | High | |
| [141] | Double-blind RCT | 30 healthy male volunteers | 1 g/day | 4 weeks | Nigella seeds had no effect on glycaemia or insulin. Total cholesterol and LDL-cholesterol were decreased with no effect on triglycerides or HDL-cholesterol. | Low | |
| [142] | Clinical trial | 94 pts with type 2 diabetes | 1, 2 or 3 g/day | 12 weeks | Reductions in FBG, postprandial glucose, HbA1c and insulin resistance from 2 g/day. No effect on serum C-peptide or body weight. | Low | |
| [143] | Placebo-controlled study | 35 menopausal women with MetS | 1 g/day | 8 weeks | No change in body weight. Nigella reduced FBG. Total cholesterol, TG and LDL were reduced. HDL change was not significant. | Low | |
| [144] | Randomised controlled trial | 37 menopausal women with moderate risk of hyperlipidemia | 1 g/day | 8 weeks | Decrease in hyperlipidemia from nigella seeds. | Low | |
| [145] | Single-blind, non-randomised trial | 114 pts with type 2 diabetes | 2 g/day | one year | Nigella seed group had a significant decline in TC, LDL-cholesterol, total cholesterol/HDL-C and LDL/HDL ratios, as well as DBP, mean arterial pressure and heart rate. | High | |
| [146] | Double-blind RCT | 73 adults with hyperlipidemia | 2 g/day | 6 weeks | No effects were seen for blood sugar or lipids. | High | |
| [147] | Double-blind RCT | 40 pts with Hashimoto’s thyroiditis | 2 g/day | 8 weeks | Nigella sativa supplementation significantly reduced anthropometric variables including weight, BMI and waist circumference. Serum TSH and anti-TPO concentrations reduced while serum T3 increased in Nigella sativa treated group. VEGF also decreased in the nigella group. | High | |
| [148] | Double-blind RCT | 50 pts with NAFLD | 2 g/day | 12 weeks | Levels of CRP and NFκB were decreased by nigella. No change in hepatic steatosis or TNFα. | High | |
| [149] | Double-blind RCT | 50 pts with NAFLD | 2 g/day | 12 weeks | Reduction in glucose, insulin and insulin resistance, but no change to lipid profile. Percentage of hepatic steatosis also decreased. | High | |
| [150] | Double-blind RCT | 40 pts with Hashimoto’s thyroiditis | 2 g/day | 8 weeks | Nigella seeds decreased TG, LDL, weight and BMI, and increased SOD and total antioxidant capacity. | High | |
| [151] | Double-blind RCT | 114 pts with type 2 diabetes | 2 g/day | one year | No change to BMI. Nigella led to a decrease in FBG, HbA1c and insulin resistance. | High | |
| [152] | Double-blind RCT | 140 menopausal women with MetS | 500 mg/day | 8 weeks | LDL-cholesterol, TG, total cholesterol and FBG decreased. | High | |
| [153] | Double-blind RCT | 39 men with obesity | 3 g/day | 12 weeks | There was no change in serum-free testosterone, FBG, TG and inflammatory markers. However, body weight, waist circumference and BP did improve. | High | |
| [154] | Randomised, placebo-controlled trial | 74 individuals with hypercholesterolemia | 2 g/day | 4 weeks | Nigella seed lowered triglycerides, LDL and cholesterol compared with baseline, but had no effect on blood glucose or HDL. | High | |
| Rosemary | [155] | Double-blind RCT | 110 pts with NAFLD | 4 g/day | 8 weeks | There were no effects on liver enzymes, anthropometric measurements, FBG, insulin, insulin resistance and blood lipids from rosemary when compared with placebo. | High |
| Sage | [156] | Non-randomised cross-over trial | 6 healthy female volunteers | 600 mL sage tea/day | 4 weeks | No effects on blood glucose, but LDL and total cholesterol decreased, while HDL increased. Lymphocyte hsp70 expression also increased. | Low |
| Turmeric | [157] | Single-blinded RCT | 42 women with type 2 diabetes and hyperlipidemia | 2.1 g/day | 8 weeks | There was an improvement in body composition, lipid profile and glycemic status in the turmeric group and the aerobic training or the aerobic training plus turmeric groups compared with control group. The combined group also had lower blood lipids, blood glucose and insulin than turmeric alone group. | High |
| [158] | Randomised cross-over study | 14 healthy volunteers | 6 g | Single dose | Turmeric increased postprandial insulin without affecting plasma glucose. | High | |
| [159] | Open-label, randomised clinical trial | 60 diabetic pts on metformin | 2 g/day | 4 weeks | Turmeric reduced fasting plasma glucose, but had no effect on post-prandial glucose. Turmeric also increased glutathione, MDA and CRP compared with baseline. LDL cholesterol was decreased compared with baseline. | High | |
| [160] | Double-blind RCT | 46 pts with NAFLD | 3 g/day | 12 weeks | Turmeric consumption decreased serum levels of glucose, insulin, HOMA-IR and leptin. Changes in weight, BMI and liver enzymes were not significant | High | |
| [161] | Randomised, single-blinded placebo-controlled trial | 42 hyperlipidemic pts with type 2 diabetes | 2.1 g/day | 8 weeks | Turmeric alone and turmeric plus aerobic training sig decreased waist circumference, FBG, TG and BP, while HDL cholesterol increased. MetS Z score and inflammatory markers improved in both turmeric groups. | High | |
| [162] | Double-blind RCT | 80 type 2 diabetes mellitus pts (30–70 years old) | 2.1 g/day turmeric powder | 8 weeks | Turmeric was found to decrease body weight, TG and total cholesterol. | High | |
| [163] | Double-blind RCT | 64 pts with NAFLD | 2 g/day | 8 weeks | Turmeric reduced liver enzymes AST, ALT and GGT compared with placebo. Triglycerides, LDL, HDL and MDA decreased from baseline, but were not different from placebo. | High | |
| [164] | Double-blind RCT | 114 pts with type 2 diabetes | 1.2 g/day | 12 weeks | Turmeric reduced arterial stiffness. No change was found in markers of endothelial function. | High | |
| Turmeric and nigella seed | [165] | Double-blind RCT | 250 healthy men with MetS | 1.5 g/day nigella, 2.4 g/day turmeric | 8 weeks | Nigella seed led to improvement in triglycerides, total cholesterol, LDL and HDL, but no change to anthropometric measures, blood glucose, BP or inflammation. Turmeric improved cholesterol, LDL and inflammation, but not TG, HDL, anthropometric measures, BP or blood glucose. | High |
| Turmeric and cinnamon | [166] | Double-blind RCT | 48 people >60 years with prediabetes | 1 g turmeric or 2 g of cinnamon | Single dose | Co-ingestion of turmeric with white bread increases working memory independent of body fatness, glycaemia, insulin or AD biomarkers. Cinnamon had no impact on working memory. Use of turmeric or cinnamon regularly had no impact on glycaemia or insulin responses to breakfast. | High |
| Turmeric and red pepper spice | [167] | Double-blind cross-over RCT | 98 overweight or obese women | 2.8 g turmeric/day | 4 weeks | Turmeric does not alter oxidative stress or inflammation in overweight/obese females with systemic inflammation or cause a significant shift in the global metabolic profile. | High |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mackonochie, M.; Rodriguez-Mateos, A.; Mills, S.; Rolfe, V. A Scoping Review of the Clinical Evidence for the Health Benefits of Culinary Doses of Herbs and Spices for the Prevention and Treatment of Metabolic Syndrome. Nutrients 2023, 15, 4867. https://doi.org/10.3390/nu15234867
Mackonochie M, Rodriguez-Mateos A, Mills S, Rolfe V. A Scoping Review of the Clinical Evidence for the Health Benefits of Culinary Doses of Herbs and Spices for the Prevention and Treatment of Metabolic Syndrome. Nutrients. 2023; 15(23):4867. https://doi.org/10.3390/nu15234867
Chicago/Turabian StyleMackonochie, Marion, Ana Rodriguez-Mateos, Simon Mills, and Vivien Rolfe. 2023. "A Scoping Review of the Clinical Evidence for the Health Benefits of Culinary Doses of Herbs and Spices for the Prevention and Treatment of Metabolic Syndrome" Nutrients 15, no. 23: 4867. https://doi.org/10.3390/nu15234867
APA StyleMackonochie, M., Rodriguez-Mateos, A., Mills, S., & Rolfe, V. (2023). A Scoping Review of the Clinical Evidence for the Health Benefits of Culinary Doses of Herbs and Spices for the Prevention and Treatment of Metabolic Syndrome. Nutrients, 15(23), 4867. https://doi.org/10.3390/nu15234867