
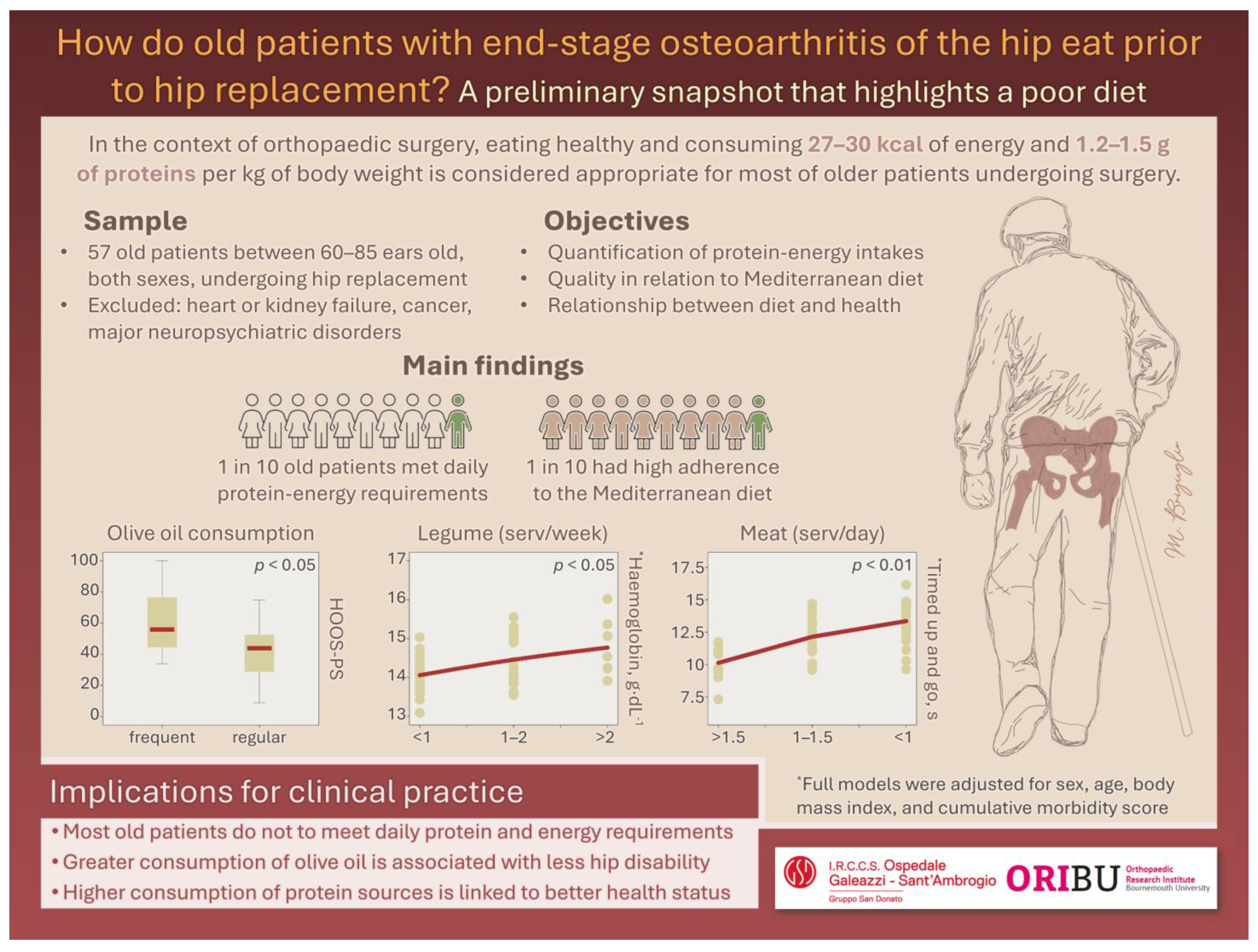
How Do Older Patients with End-Stage Osteoarthritis of the Hip Eat Prior to Hip Replacement? A Preliminary Snapshot That Highlights a Poor Diet

 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Eligibility Criteria
2.2. Dietary Assessment and Laboratory Parameters
2.3. Functional Status
2.4. Statistics
3. Results
3.1. Descriptives, Associations, and Differences in Cohort Descriptors
3.2. Predictions of Clinical Conditions from Dietary Scores
4. Discussion
Limitations
5. Conclusions
6. Future Perspectives
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Briguglio, M.; Wainwright, T.W.; Southern, K.; Riso, P.; Porrini, M.; Middleton, R.G. Healthy Eating for Elective Major Orthopedic Surgery: Quality, Quantity, and Timing. J. Multidiscip. Healthc. 2023, 16, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- Van Elswyk, M.E.; Teo, L.; Lau, C.S.; Shanahan, C.J. Dietary Patterns and the Risk of Sarcopenia: A Systematic Review and Meta-Analysis. Curr. Dev. Nutr. 2022, 6, nzac001. [Google Scholar] [CrossRef]
- Shin, W.Y.; Kim, J.H. Poor diet quality is associated with self-reported knee pain in community-dwelling women aged 50 years and older. PLoS ONE 2021, 16, e0245630. [Google Scholar] [CrossRef] [PubMed]
- Chopp-Hurley, J.N.; Wiebenga, E.G.; Keller, H.H.; Maly, M.R. Diet and Nutrition Risk Affect Mobility and General Health in Osteoarthritis: Data from the Canadian Longitudinal Study on Aging. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 2147–2155. [Google Scholar] [CrossRef]
- Warensjö Lemming, E.; Byberg, L. Is a Healthy Diet Also Suitable for the Prevention of Fragility Fractures? Nutrients 2020, 12, 2642. [Google Scholar] [CrossRef]
- Tavassoli, N.; de Souto Barreto, P.; Berbon, C.; Mathieu, C.; de Kerimel, J.; Lafont, C.; Takeda, C.; Carrie, I.; Piau, A.; Jouffrey, T.; et al. Implementation of the WHO integrated care for older people (ICOPE) programme in clinical practice: A prospective study. Lancet Healthy Longev. 2022, 3, e394–e404. [Google Scholar] [CrossRef] [PubMed]
- Wei, N.; Dai, Z. The Role of Nutrition in Osteoarthritis: A Literature Review. Clin. Geriatr. Med. 2022, 38, 303–322. [Google Scholar] [CrossRef]
- Thomas, S.; Browne, H.; Mobasheri, A.; Rayman, M.P. What is the evidence for a role for diet and nutrition in osteoarthritis? Rheumatology 2018, 57, iv61–iv74. [Google Scholar] [CrossRef]
- Briguglio, M.; Wainwright, T.W. Nutritional and Physical Prehabilitation in Elective Orthopedic Surgery: Rationale and Proposal for Implementation. Ther. Clin. Risk Manag. 2022, 18, 21–30. [Google Scholar] [CrossRef]
- Briguglio, M.; Cordani, C.; Langella, F.; Perazzo, P.; Pregliasco, F.E.; Banfi, G.; Wainwright, T.W. Why Treat Patients with a Major Orthopaedic Surgery Only to Send Them Back to the Vulnerable Conditions That Made Them Sick in the First Place? A Conceptual Scenario to Improve Patient’s Journey. Int. J. Gen. Med. 2023, 16, 4729–4735. [Google Scholar] [CrossRef]
- Briguglio, M. The Burdens of Orthopedic Patients and the Value of the HEPAS Approach (Healthy Eating, Physical Activity, and Sleep Hygiene). Front. Med. 2021, 8, 650947. [Google Scholar] [CrossRef]
- Sofi, F.; Dinu, M.; Pagliai, G.; Marcucci, R.; Casini, A. Validation of a literature-based adherence score to Mediterranean diet: The MEDI-LITE score. Int. J. Food Sci. Nutr. 2017, 68, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Davis, A.M.; Perruccio, A.V.; Canizares, M.; Tennant, A.; Hawker, G.A.; Conaghan, P.G.; Roos, E.M.; Jordan, J.M.; Maillefert, J.F.; Dougados, M.; et al. The development of a short measure of physical function for hip OA HOOS-Physical Function Shortform (HOOS-PS): An OARSI/OMERACT initiative. Osteoarthr. Cartil. 2008, 16, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Briguglio, M.; Wainwright, T.; Lombardi, G. Definition of malnutrition from routinely-collected data for orthopedic surgery research: The global leadership initiative on malnutrition (GLIM) tool and others. Front. Nutr. 2023, 10, 1200049. [Google Scholar] [CrossRef]
- Holt, P.R. Intestinal malabsorption in the elderly. Dig. Dis. 2007, 25, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Cross, M.L.; Gill, H.S. Immunomodulatory properties of milk. Br. J. Nutr. 2000, 84 (Suppl. S1), S81–S89. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, T.; Hayashi, K.; Kosaka, A.; Kawashima, M.; Igarashi, T.; Tsutsui, H.; Tsuji, N.M.; Nishimura, I.; Hayashi, T.; Obata, A. Lactobacillus plantarum strain YU from fermented foods activates Th1 and protective immune responses. Int. Immunopharmacol. 2011, 11, 2017–2024. [Google Scholar] [CrossRef]
- Singh, N.; Jain, P.; Ujinwal, M.; Langyan, S. Escalate protein plates from legumes for sustainable human nutrition. Front. Nutr. 2022, 9, 977986. [Google Scholar] [CrossRef]
- Purcell, S.; Thornberry, R.; Elliott, S.A.; Panton, L.; Ormsbee, M.J.; Vieira, E.R.; Kim, J.S.; Prado, C.M. Body Composition, Strength, and Dietary Intake of Patients with Hip or Knee Osteoarthritis. Can. J. Diet. Pract. Res. 2016, 77, 98–102. [Google Scholar] [CrossRef]
- Papadopoulou, S.K.; Detopoulou, P.; Voulgaridou, G.; Tsoumana, D.; Spanoudaki, M.; Sadikou, F.; Papadopoulou, V.G.; Zidrou, C.; Chatziprodromidou, I.P.; Giaginis, C.; et al. Mediterranean Diet and Sarcopenia Features in Apparently Healthy Adults over 65 Years: A Systematic Review. Nutrients 2023, 15, 1104. [Google Scholar] [CrossRef] [PubMed]
- Coelho-Júnior, H.J.; Calvani, R.; Tosato, M.; Landi, F.; Picca, A.; Marzetti, E. Protein intake and physical function in older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2022, 81, 101731. [Google Scholar] [CrossRef] [PubMed]
- Chun, O.K.; Chung, S.J.; Claycombe, K.J.; Song, W.O. Serum C-reactive protein concentrations are inversely associated with dietary flavonoid intake in U.S. adults. J. Nutr. 2008, 138, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Hruby, A.; Jacques, P.F. Dietary Protein and Changes in Biomarkers of Inflammation and Oxidative Stress in the Framingham Heart Study Offspring Cohort. Curr. Dev. Nutr. 2019, 3, nzz019. [Google Scholar] [CrossRef] [PubMed]
- Formica, M.B.; Gianoudis, J.; Nowson, C.A.; O’Connell, S.L.; Milte, C.; Ellis, K.A.; Daly, R.M. Effect of lean red meat combined with a multicomponent exercise program on muscle and cognitive function in older adults: A 6-month randomized controlled trial. Am. J. Clin. Nutr. 2020, 112, 113–128. [Google Scholar] [CrossRef] [PubMed]
- Daly, R.M.; O’Connell, S.L.; Mundell, N.L.; Grimes, C.A.; Dunstan, D.W.; Nowson, C.A. Protein-enriched diet, with the use of lean red meat, combined with progressive resistance training enhances lean tissue mass and muscle strength and reduces circulating IL-6 concentrations in elderly women: A cluster randomized controlled trial. Am. J. Clin. Nutr. 2014, 99, 899–910. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.; Oguma, Y.; Asakura, K.; Abe, Y.; Arai, Y. Relationship between dietary patterns and physical performance in the very old population: A cross-sectional study from the Kawasaki Aging and Wellbeing Project. Public. Health Nutr. 2023, 26, 1163–1171. [Google Scholar] [CrossRef] [PubMed]
- Rondanelli, M.; Perna, S.; Faliva, M.A.; Peroni, G.; Infantino, V.; Pozzi, R. Novel insights on intake of meat and prevention of sarcopenia: All reasons for an adequate consumption. Nutr. Hosp. 2015, 32, 2136–2143. [Google Scholar] [CrossRef]
- Musumeci, G.; Trovato, F.M.; Pichler, K.; Weinberg, A.M.; Loreto, C.; Castrogiovanni, P. Extra-virgin olive oil diet and mild physical activity prevent cartilage degeneration in an osteoarthritis model: An in vivo and in vitro study on lubricin expression. J. Nutr. Biochem. 2013, 24, 2064–2075. [Google Scholar] [CrossRef]
- Chin, K.Y.; Pang, K.L. Therapeutic Effects of Olive and Its Derivatives on Osteoarthritis: From Bench to Bedside. Nutrients 2017, 9, 1060. [Google Scholar] [CrossRef]
- Hébert, J.R.; Hurley, T.G.; Steck, S.E.; Miller, D.R.; Tabung, F.K.; Peterson, K.E.; Kushi, L.H.; Frongillo, E.A. Considering the value of dietary assessment data in informing nutrition-related health policy. Adv. Nutr. 2014, 5, 447–455. [Google Scholar] [CrossRef]
- Paddon-Jones, D.; Rasmussen, B.B. Dietary protein recommendations and the prevention of sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 86–90. [Google Scholar] [CrossRef]
- Struijk, E.A.; Banegas, J.R.; Rodríguez-Artalejo, F.; Lopez-Garcia, E. Consumption of meat in relation to physical functioning in the Seniors-ENRICA cohort. BMC Med. 2018, 16, 50. [Google Scholar] [CrossRef]
- Pelchat, M.L.; Schaefer, S. Dietary monotony and food cravings in young and elderly adults. Physiol. Behav. 2000, 68, 353–359. [Google Scholar] [CrossRef]


{kind=link}
| Descriptors | Cohort |
|---|---|
| Sex, male; female | 30; 27 |
| Age, years | 71.48 (6.54) [60.89–84.14] |
| BMI, kg·m−2 | 27.00 (4.72) [19.57–40.49] |
| CCI | 3.44 (1.20) [2.00–7.00] |
| Dietary assessment | |
| Proteins·kg−1 | 0.75 (0.28) [0.31–1.57] |
| Kcalories·kg−1 | 19.63 (6.01) [9.79–36.47] |
| Medi-Lite index | 10.37 (2.03) [6.00–15.00] |
| Laboratory parameters | |
| RBCs, 106·μL−1 | 4.72 (0.48) [3.48–5.87] |
| Haematocrit, % | 42.78 (3.78) [31.80–52.60] |
| Haemoglobin, g·dL−1 | 14.30 (1.24) [10.70–17.50] |
| MCV, fL | 90.81 (4.75) [76.60–102.40] |
| MCH, pg | 30.38 (1.77) [24.10–34.10] |
| MCHC, g·dL−1 | 33.45 (1.04) [30.40–35.60] |
| Iron, μg·dL−1 | 95.08 (28.41) [45.00–168.00] |
| Transferrin, mg·dL−1 | 240.86 (26.25) [181.00–307.00] |
| Ferritin, ng·mL−1 | 150.56 (129.82) [13.00–743.00] |
| WBCs, 103·μL−1 | 7.21 (1.99) [3.64–12.94] |
| Lymphocytes, 103·μL−1 | 1.89 (0.62) [0.59–4.18] |
| Lymphocytes, % | 26.86 (7.20) [5.00–40.80] |
| Transthyretin, mg·dL−1 | 25.35 (4.59) [17.80–37.10] |
| Albumin, g·dL−1 | 4.42 (0.35) [3.60–5.20] |
| Total proteins, g·dL−1 | 6.86 (0.48) [5.90–7.80] |
| C-reactive protein, mg·L−1 | 0.37 (0.51) [0.04–2.76] |
| Functional status | |
| Barthel index | 98.94 (1.94) [89.00–100.00] |
| Timed up and go, s | 12.45 (3.78) [7.15–23.74] |
| HOOS-PS | 47.36 (19.43) [8.80–100.00] |
| SF-12 PCS | 34.96 (7.58) [24.00–53.60] |
| Dependent Variables | Independent Variables of the Regression Models Adjusted for Sex, Age, BMI, and CCI | ||||
|---|---|---|---|---|---|
| Legumes Score | Cereals Score | Meat Score 1 | Dairy Score 1 | Olive Oil Score | |
| Laboratory parameters | |||||
| Haemoglobin, g·dL−1 | +0.498 * | - | - | - | - |
| Total proteins, g·dL−1 | - | −0.356 ** | - | +0.276 ** | - |
| Functional scores | |||||
| Timed up and go, s | - | - | +1.898 ** | - | −2.783 ** |
| HOOS-PS | - | - | +11.352 ** | - | −13.618 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Briguglio, M.; Sirtori, P.; Mangiavini, L.; Buzzi, S.; Cordani, C.; Zerni, M.F.; Wainwright, T.W.; Ursino, N.; Peretti, G.M.; Banfi, G. How Do Older Patients with End-Stage Osteoarthritis of the Hip Eat Prior to Hip Replacement? A Preliminary Snapshot That Highlights a Poor Diet. Nutrients 2023, 15, 4868. https://doi.org/10.3390/nu15234868
Briguglio M, Sirtori P, Mangiavini L, Buzzi S, Cordani C, Zerni MF, Wainwright TW, Ursino N, Peretti GM, Banfi G. How Do Older Patients with End-Stage Osteoarthritis of the Hip Eat Prior to Hip Replacement? A Preliminary Snapshot That Highlights a Poor Diet. Nutrients. 2023; 15(23):4868. https://doi.org/10.3390/nu15234868
Chicago/Turabian StyleBriguglio, Matteo, Paolo Sirtori, Laura Mangiavini, Sara Buzzi, Claudio Cordani, Maria Francesca Zerni, Thomas W. Wainwright, Nicola Ursino, Giuseppe M. Peretti, and Giuseppe Banfi. 2023. "How Do Older Patients with End-Stage Osteoarthritis of the Hip Eat Prior to Hip Replacement? A Preliminary Snapshot That Highlights a Poor Diet" Nutrients 15, no. 23: 4868. https://doi.org/10.3390/nu15234868
APA StyleBriguglio, M., Sirtori, P., Mangiavini, L., Buzzi, S., Cordani, C., Zerni, M. F., Wainwright, T. W., Ursino, N., Peretti, G. M., & Banfi, G. (2023). How Do Older Patients with End-Stage Osteoarthritis of the Hip Eat Prior to Hip Replacement? A Preliminary Snapshot That Highlights a Poor Diet. Nutrients, 15(23), 4868. https://doi.org/10.3390/nu15234868