
Vitamin D Status in Bipolar Disorder

 ,
,  , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
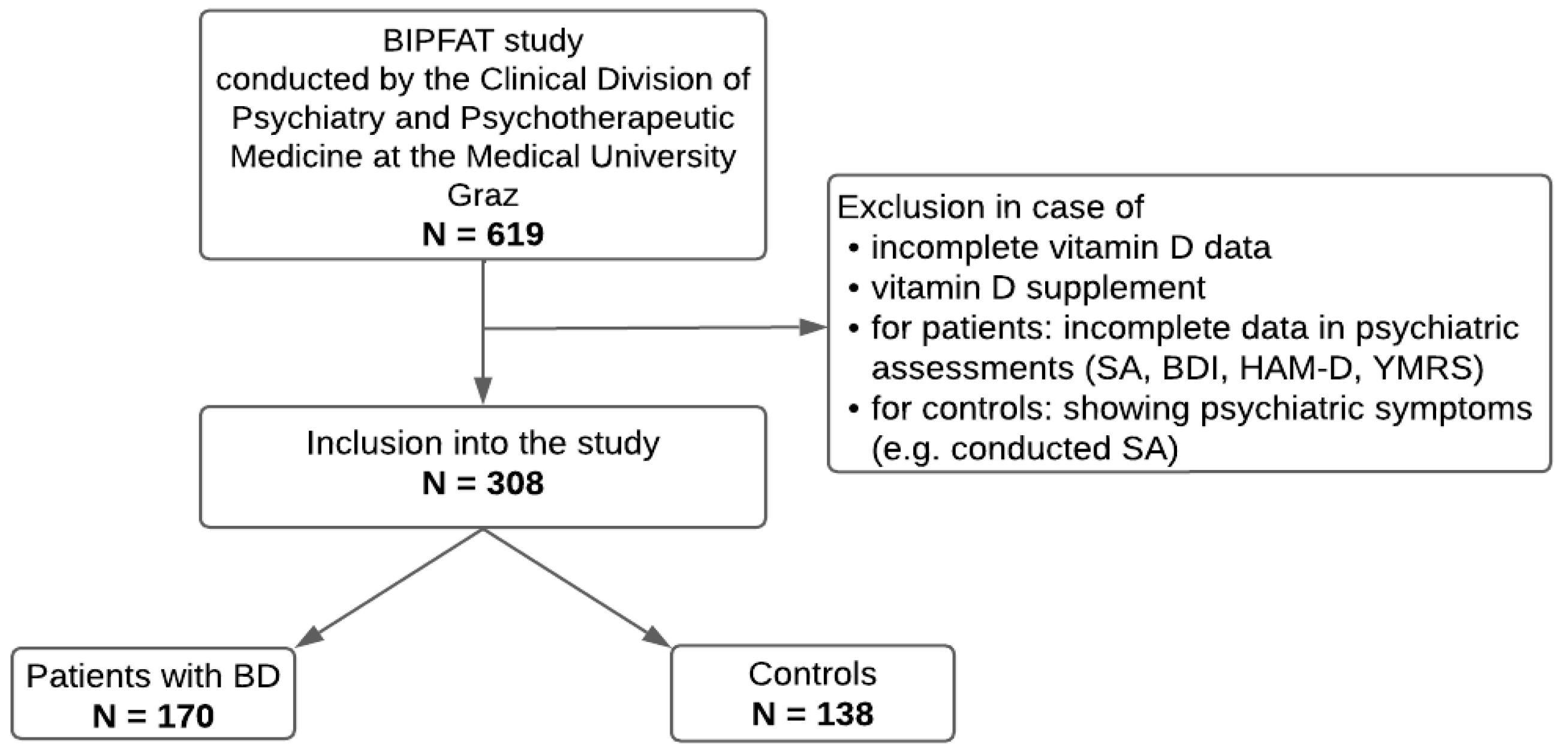
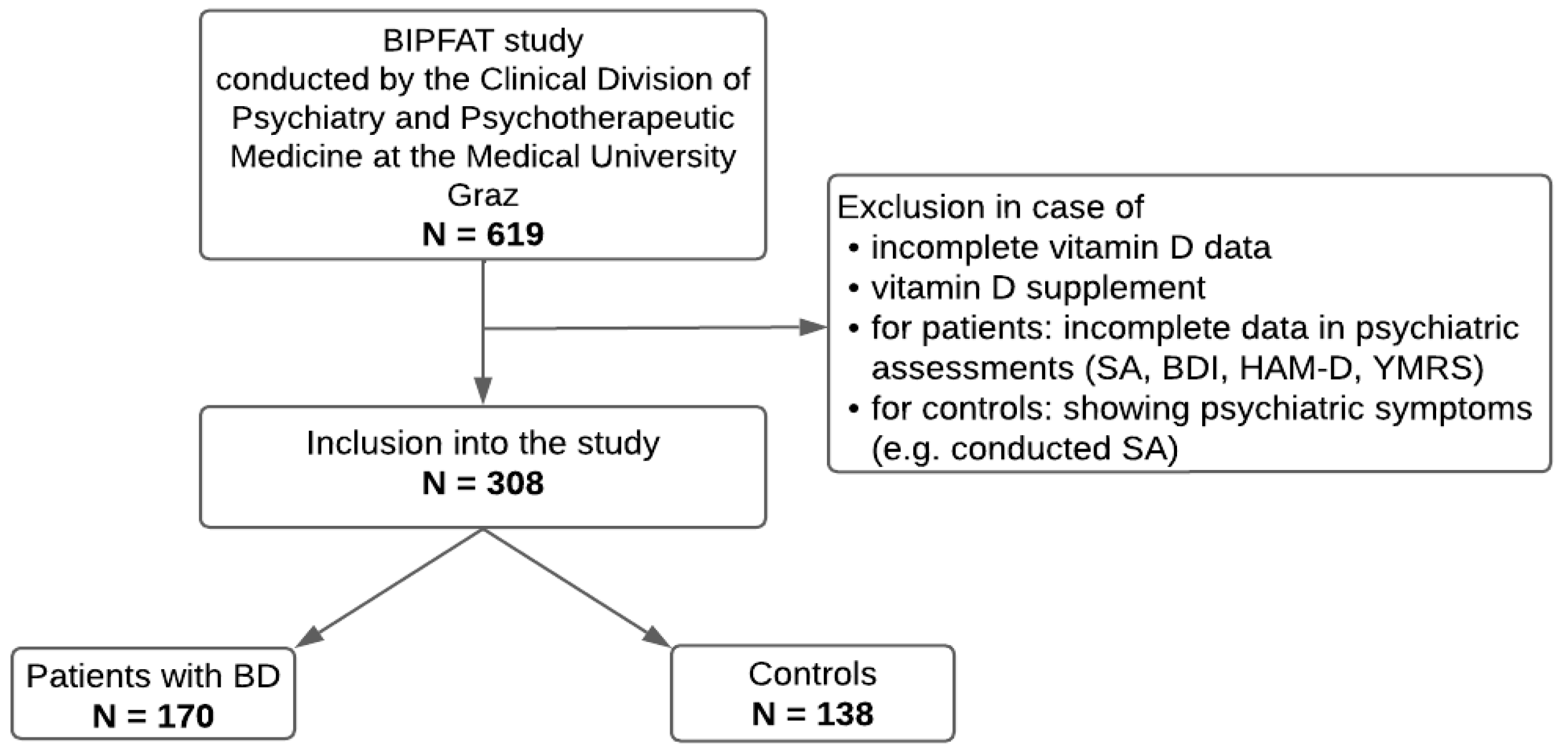
2.1. Participants
2.2. Psychometric Assessment
2.3. Vitamin D
2.4. Statistical Analyses
3. Results
3.1. Descriptive Statistics
3.2. Vitamin D Status and Clinical Parameters
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rowland, T.A.; Marwaha, S. Epidemiology and risk factors for bipolar disorder. Ther. Adv. Psychopharmacol. 2018, 8, 251–269. [Google Scholar] [CrossRef]
- Wittchen, H.U.; Wunderlich, U.; Gruschwitz, S.; Zaudig, M. SKID I. Strukturiertes Klinisches Interview für DSM-IV. Achse I: Psychische Störungen. Interviewheft und Beurteilungsheft. Eine Deutschsprachige, Erweiterte Bearb. d. Amerikanischen Originalversion des SKID I; Hogrefe: Göttingen, Germany, 1997. [Google Scholar]
- Rothenhäusler, H.B.; Täschner, K.L. Kompendium Praktische Psychiatrie, 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Benedetti, F.; Aggio, V.; Pratesi, M.L.; Greco, G.; Furlan, R. Neuroinflammation in Bipolar Depression. Front. Psychiatry 2020, 11, 71. [Google Scholar] [CrossRef]
- Cyrino, L.A.R.; Delwing-de Lima, D.; Ullmann, O.M.; Maia, T.P. Concepts of Neuroinflammation and Their Relationship with Impaired Mitochondrial Functions in Bipolar Disorder. Front. Behav. Neurosci. 2021, 15, 609487. [Google Scholar] [CrossRef] [PubMed]
- Sinha, A.; Shariq, A.; Said, K.; Sharma, A.; Jeffrey Newport, D.; Salloum, I.M. Medical Comorbidities in Bipolar Disorder. Curr. Psychiatry Rep. 2018, 20, 36. [Google Scholar] [CrossRef] [PubMed]
- Reininghaus, B.; Dalkner, N.; Schörkhuber, C.; Fleischmann, E.; Fellendorf, F.T.; Ratzenhofer, M.; Maget, A.; Platzer, M.; Bengesser, S.A.; Tmava-Berisha, A.; et al. Nutrition, Overweight, and Cognition in Euthymic Bipolar Individuals Compared to Healthy Controls. Nutrients 2022, 14, 1176. [Google Scholar] [CrossRef]
- Mangge, H.; Bengesser, S.; Dalkner, N.; Birner, A.; Fellendorf, F.; Platzer, M.; Queissner, R.; Pilz, R.; Maget, A.; Reininghaus, B.; et al. Weight Gain During Treatment of Bipolar Disorder (BD)—Facts and Therapeutic Options. Front. Nutr. 2019, 6, 76. [Google Scholar] [CrossRef]
- Simjanoski, M.; Patel, S.; De Boni, R.; Balanzá-Martínez, V.; Frey, B.N.; Minuzzi, L.; Kapczinski, F.; Cardoso, T.d.A. Lifestyle interventions for bipolar disorders: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2023, 152, 105257. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.; Glenn, T.; Alda, M.; Andreassen, O.A.; Angelopoulos, E.; Ardau, R.; Baethge, C.; Bauer, R.; Bellivier, F.; Belmaker, R.H.; et al. Relationship between sunlight and the age of onset of bipolar disorder: An international multisite study. J. Affect. Disord. 2014, 167, 104–111. [Google Scholar] [CrossRef]
- Bauer, M.E.; Teixeira, A.L. Inflammation in psychiatric disorders: What comes first? Ann. N. Y. Acad. Sci. 2019, 1437, 57–67. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Barrea, L.; Scannapieco, M.; Di Somma, C.; Scacchi, M.; Aimaretti, G.; Savastano, S.; Colao, A.; Marzullo, P. The lullaby of the sun: The role of vitamin D in sleep disturbance. Sleep. Med. 2019, 54, 262–265. [Google Scholar] [CrossRef]
- Steardo, L.; Luciano, M.; Sampogna, G.; Carbone, E.A.; Caivano, V.; Di Cerbo, A.; Giallonardo, V.; Palummo, C.; Vece, A.; Del Vecchio, V.; et al. Clinical Severity and Calcium Metabolism in Patients with Bipolar Disorder. Brain Sci. 2020, 10, 417. [Google Scholar] [CrossRef]
- Christakos, S.; Ajibade, D.V.; Dhawan, P.; Fechner, A.J.; Mady, L.J. Vitamin D: Metabolism. Endocrinol. Metab. Clin. N. Am. 2010, 39, 243–253. [Google Scholar] [CrossRef] [PubMed]
- Parker, G.B.; Brotchie, H.; Graham, R.K. Vitamin D and depression. J. Affect. Disord. 2017, 208, 56–61. [Google Scholar] [CrossRef]
- Herrmann, M.; Farrell, C.-J.L.; Pusceddu, I.; Fabregat-Cabello, N.; Cavalier, E. Assessment of vitamin D status—A changing landscape. Clin. Chem. Lab. Med. 2017, 55, 3–26. [Google Scholar] [CrossRef] [PubMed]
- Zelzer, S.; Hofer, E.; Meinitzer, A.; Fritz-Petrin, E.; Simstich, S.; Goessler, W.; Schmidt, R.; Herrmann, M. Association of vitamin D metabolites with cognitive function and brain atrophy in elderly individuals—The Austrian stroke prevention study. Aging 2021, 13, 9455–9467. [Google Scholar] [CrossRef] [PubMed]
- Alonso, N.; Zelzer, S.; Eibinger, G.; Herrmann, M. Vitamin D Metabolites: Analytical Challenges and Clinical Relevance. Calcif. Tissue Int. 2022, 112, 158–177. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, M. Assessing vitamin D metabolism—Four decades of experience. Clin. Chem. Lab. Med. 2023, 61, 880–894. [Google Scholar] [CrossRef]
- Głąbska, D.; Kołota, A.; Lachowicz, K.; Skolmowska, D.; Stachoń, M.; Guzek, D. The Influence of Vitamin D Intake and Status on Mental Health in Children: A Systematic Review. Nutrients 2021, 13, 952. [Google Scholar] [CrossRef]
- Cereda, G.; Enrico, P.; Ciappolino, V.; Delvecchio, G.; Brambilla, P. The role of vitamin D in bipolar disorder: Epidemiology and influence on disease activity. J. Affect. Disord. 2021, 278, 209–217. [Google Scholar] [CrossRef]
- Rihal, V.; Khan, H.; Kaur, A.; Singh, T.G.; Abdel-Daim, M.M. Therapeutic and mechanistic intervention of vitamin D in neuropsychiatric disorders. Psychiatry Res. 2022, 317, 114782. [Google Scholar] [CrossRef]
- Christakos, S.; Dhawan, P.; Verstuyf, A.; Verlinden, L.; Carmeliet, G. Vitamin D: Metabolism, Molecular Mechanism of Action, and Pleiotropic Effects. Physiol. Rev. 2016, 96, 365–408. [Google Scholar] [CrossRef] [PubMed]
- Cui, X.; Eyles, D.W. Vitamin D and the Central Nervous System: Causative and Preventative Mechanisms in Brain Disorders. Nutrients 2022, 14, 4353. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.R.M.; Barros, W.M.A.; da Silva, M.L.; da Silva, J.M.L.; Souza, A.P.S.; da Silva, A.B.J.; de Sousa Fernandes, M.S.; de Souza, S.L.; de Oliveira Nogueira Souza, V. Relationship between vitamin d deficiency and psychophysiological variables: A systematic review of the literature. Clinics 2021, 76, e3155. [Google Scholar] [CrossRef] [PubMed]
- Humble, M.B.; Gustafsson, S.; Bejerot, S. Low serum levels of 25-hydroxyvitamin D (25-OHD) among psychiatric out-patients in Sweden: Relations with season, age, ethnic origin and psychiatric diagnosis. J. Steroid Biochem. Mol. Biol. 2010, 121, 467–470. [Google Scholar] [CrossRef] [PubMed]
- Menkes, D.B.; Lancaster, K.; Grant, M.; Marsh, R.W.; Dean, P.; du Toit, S.A. Vitamin D status of psychiatric inpatients in New Zealand’s Waikato region. BMC Psychiatry 2012, 12, 68. [Google Scholar] [CrossRef]
- Grønli, O.; Kvamme, J.M.; Jorde, R.; Wynn, R. Vitamin D deficiency is common in psychogeriatric patients, independent of diagnosis. BMC Psychiatry 2014, 14, 134. [Google Scholar] [CrossRef]
- Jorde, R.; Kubiak, J. No improvement in depressive symptoms by vitamin D supplementation: Results from a randomised controlled trial. J. Nutr. Sci. 2018, 7, e30. [Google Scholar] [CrossRef] [PubMed]
- Leser, B.; Dalkner, N.; Tmava-Berisha, A.; Fellendorf, F.T.; Unterrainer, H.-F.; Stross, T.; Maget, A.; Platzer, M.; Bengesser, S.A.; Häussl, A.; et al. The Influence of Vitamin D Status on Cognitive Ability in Patients with Bipolar Disorder and Healthy Controls. Nutrients 2023, 15, 4111. [Google Scholar] [CrossRef]
- Dalkner, N.; Bengesser, S.A.; Birner, A.; Fellendorf, F.T.; Fleischmann, E.; Großschädl, K.; Lenger, M.; Maget, A.; Platzer, M.; Queissner, R.; et al. Metabolic Syndrome Impairs Executive Function in Bipolar Disorder. Front. Neurosci. 2021, 15, 717824. [Google Scholar] [CrossRef]
- Fellendorf, F.T.; Gostner, J.M.; Lenger, M.; Platzer, M.; Birner, A.; Maget, A.; Queissner, R.; Tmava-Berisha, A.; Pater, C.A.; Ratzenhofer, M.; et al. Tryptophan Metabolism in Bipolar Disorder in a Longitudinal Setting. Antioxidants 2021, 10, 1795. [Google Scholar] [CrossRef]
- Platzer, M.; Dalkner, N.; Fellendorf, F.T.; Birner, A.; Bengesser, S.A.; Queissner, R.; Kainzbauer, N.; Pilz, R.; Herzog-Eberhard, S.; Hamm, C.; et al. Tryptophan breakdown and cognition in bipolar disorder. Psychoneuroendocrinology 2017, 81, 144–150. [Google Scholar] [CrossRef]
- Reininghaus, E.Z.; McIntyre, R.S.; Reininghaus, B.; Geisler, S.; Bengesser, S.A.; Lackner, N.; Hecht, K.; Birner, A.; Kattnig, F.; Unterweger, R.; et al. Tryptophan breakdown is increased in euthymic overweight individuals with bipolar disorder: A preliminary report. Bipolar Disord. 2014, 16, 432–440. [Google Scholar] [CrossRef] [PubMed]
- BECK, A.T. An Inventory for Measuring Depression. Arch. Gen. Psychiatry 1961, 4, 561. [Google Scholar] [CrossRef]
- Hamilton, M. Development of a rating scale for primary depressive illness. Br. J. Soc. Clin. Psychol. 1967, 6, 278–296. [Google Scholar] [CrossRef]
- Young, R.C.; Biggs, J.T.; Ziegler, V.E.; Meyer, D.A. A Rating Scale for Mania: Reliability, Validity and Sensitivity. Br. J. Psychiatry 1978, 133, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Schorre, B.E.H.; Vandvik, I.H. Global assessment of psychosocial functioning in child and adolescent psychiatry. Eur. Child. Adolesc. Psychiatry 2004, 13, 273–286. [Google Scholar] [CrossRef]
- Ross, A.C.; Taylor, C.L.; Yaktine, A.L.; Del Valle, H.B. Dietary Reference Intakes for Calcium and Vitamin, D; National Academies Press: Washington, DC, USA, 2011. [Google Scholar] [CrossRef]
- Zelzer, S.; Meinitzer, A.; Enko, D.; Simstich, S.; Le Goff, C.; Cavalier, E.; Herrmann, M.; Goessler, W. Simultaneous determination of 24,25- and 25,26-dihydroxyvitamin D3 in serum samples with liquid-chromatography mass spectrometry—A useful tool for the assessment of vitamin D metabolism. J. Chromatogr. B 2020, 1158, 122394. [Google Scholar] [CrossRef] [PubMed]
- Pape, K.; Tamouza, R.; Leboyer, M.; Zipp, F. Immunoneuropsychiatry—Novel perspectives on brain disorders. Nat. Rev. Neurol. 2019, 15, 317–328. [Google Scholar] [CrossRef]
- Berking, M.; Wirtz, C.M.; Svaldi, J.; Hofmann, S.G. Emotion regulation predicts symptoms of depression over five years. Behav. Res. Ther. 2014, 57, 13–20. [Google Scholar] [CrossRef]
- Boerman, R.; Cohen, D.; Schulte, P.F.J.; Nugter, A. Prevalence of Vitamin D Deficiency in Adult Outpatients with Bipolar Disorder or Schizophrenia. J. Clin. Psychopharmacol. 2016, 36, 588–592. [Google Scholar] [CrossRef] [PubMed]
- Petrov, B.; Aldoori, A.; James, C.; Yang, K.; Algorta, G.P.; Lee, A.; Zhang, L.; Lin, T.; Al Awadhi, R.; Parquette, J.R.; et al. Bipolar disorder in youth is associated with increased levels of vitamin D-binding protein. Transl. Psychiatry 2018, 8, 61. [Google Scholar] [CrossRef]
- Sikoglu, E.M.; Navarro, A.A.L.; Starr, D.; Dvir, Y.; Nwosu, B.U.; Czerniak, S.M.; Rogan, R.C.; Castro, M.C.; Edden, R.A.E.; Frazier, J.A.; et al. Vitamin D 3 Supplemental Treatment for Mania in Youth with Bipolar Spectrum Disorders. J. Child. Adolesc. Psychopharmacol. 2015, 25, 415–424. [Google Scholar] [CrossRef]
- Belzeaux, R.; Boyer, L.; Ibrahim, E.C.; Féron, F.; Leboyer, M.; Fond, G. Mood disorders are associated with a more severe hypovitaminosis D than schizophrenia. Psychiatry Res. 2015, 229, 613–616. [Google Scholar] [CrossRef]
- Moghaddam, B.; Bolinao, M.L.; Stein-Behrens, B.; Sapolsky, R. Glucocortcoids mediate the stress-induced extracellular accumulation of glutamate. Brain Res. 1994, 655, 251–254. [Google Scholar] [CrossRef]
- Altunsoy, N.; Yüksel, R.N.; Cingi Yirun, M.; Kılıçarslan, A.; Aydemir, Ç. Exploring the relationship between vitamin D and mania: Correlations between serum vitamin D levels and disease activity. Nord. J. Psychiatry 2018, 72, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Marsh, W.K.; Penny, J.L.; Rothschild, A.J. Vitamin D supplementation in bipolar depression: A double blind placebo controlled trial. J. Psychiatr. Res. 2017, 95, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Wakeman, M. A Literature Review of the Potential Impact of Medication on Vitamin D Status. Risk Manag. Healthc. Policy 2021, Volume 14, 3357–3381. [Google Scholar] [CrossRef]
- Gupta, A.; Chadda, R.K. Adverse psychiatric effects of non-psychotropic medications. BJPsych Adv. 2016, 22, 325–334. [Google Scholar] [CrossRef]
- Wacker, M.; Holick, M.F. Sunlight and Vitamin, D. Dermatoendocrinol 2013, 5, 51–108. [Google Scholar] [CrossRef]
- Kinuta, K.; Tanaka, H.; Moriwake, T.; Aya, K.; Kato, S.; Seino, Y. Vitamin D Is an Important Factor in Estrogen Biosynthesis of Both Female and Male Gonads*. Endocrinology 2000, 141, 1317–1324. [Google Scholar] [CrossRef] [PubMed]
- Arnold, L.M. Gender differences in bipolar disorder. Psychiatr. Clin. N. Am. 2003, 26, 595–620. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Functional vitamin D deficiency | Both criteria fulfilled | VMR ≤ 4% and 24,25(OH)D2 ≤ 3 nmol/L |
| Suboptimal vitamin D metabolism | One criterium fulfilled | or |
| Functional vitamin D sufficiency | No criterium fulfilled | VMR ≥ 4% and 24,25(OH)2D ≥ 3 nmol/L |
| Patients (n = 170) | Controls (n = 138) | Statistics | |
|---|---|---|---|
| Sex | χ2 (1) = 9.260, p = 0.002 * | ||
| Female | 84 (49.4%) | 92 (66.7%) | |
| Male | 86 (50.6%) | 46 (33.3%) | |
| Age, Mean ± SD (IQR) | |||
| 43.9 ± 12.8 (32.9–52.8) | 36.5 ± 14.8 (24.2–50.9) | U = 7845.000, Z = −4.999, p < 0.001 * | |
| BMI (kg/m2), Mean ± SD (IQR) | |||
| 27.8 ± 5.9 (23.8–30.2) | 24.1 ± 4.5 (21.1–26.6) | U = 4441.000, Z = −5.716, p < 0.001 * | |
| 25(OH)D (nmol/L), Mean ± SD (IQR) | |||
| 57.8 ± 24.3 (39.5–72.9) | 61.5 ± 29.3 (42–72.2) | U = 10,956.000, Z =–.996, p = 0.319 | |
| < 30 | 20 (11.8%) | 13 (9.4%) | U = 129.000, Z = −0.037, p = 0.971 |
| 30–50 | 44 (25.9%) | 32 (23.2%) | t (74) = 0.054, p = 0.957 |
| > 50 | 106 (62.4%) | 93 (67.4%) | U = 4778.500, Z = −0.371, p = 0.710 |
| 24,25(OH)2D (nmol/L), Mean ± SD (IQR) | |||
| 3.8 ± 2.4 (2–5.2) | 4.2 ± 2.7 (2.4–5.5) | U = 10,573.000, Z = −1.489, p = 0.137 | |
| <3 | 67 (39.4%) | 43 (31.2%) | U = 1396.500, Z = −0.270, p = 0.788 |
| >3 | 103 (60.6%) | 95 (68.8%) | U = 4659.500, Z = −0.578, p = 0.563 |
| VMR (%), Mean ± SD (IQR) | |||
| 6.4 ± 2.2 (4.9–8.2) | 6.8 ± 2.4 (5.3–8.4) | t (306) = −1.601, p = 0.110 | |
| <4 | 23 (13.5%) | 17 (12.3%) | U = 165.500, Z = −0.821, p = 0.412 |
| >4 | 147 (86.5%) | 121 (87.7%) | U = 7910.500, Z = −1.557, p = 0.120 |
| Patients (n = 170) | Controls (n = 138) | ||
|---|---|---|---|
| Deficient | 23 (13.5%) | 17 (12.3%) | χ2 (2) = 2.555, p =.279 |
| Suboptimal | 44 (25.9%) | 26 (18.8%) | |
| Sufficient | 103 (60.6%) | 95 (68.8%) |
| Mean ±SD (IQR) | 25(OH)D | 24,25(OH)2D | VMR | |
|---|---|---|---|---|
| SA | 0.4 ± 0.69 (0–1) | r = 0.023, p = 0.819 | r = −0.004, p = 0.968 | r = −0.042, p = 0.671 |
| BDI | 18.4 ± 12 (8–29) | r = 0.073, p = 0.462 | r = 0.034, p = 0.730 | r = −0.098, p = 0.322 |
| HAM-D | 7.1 ± 5.8 (3–10.8) | r = 0.040, p = 0.684 | r = 0.030, p = 0.765 | r = −0.005, p = 0.957 |
| YMRS | 1.7 ± 3.6 (0–1) | r = −0.127, p = 0.197 | r = −0.220, p = 0.025 ** | r = −0.238, p = 0.015 ** |
| GAF | 65.9 ± 13.1 (56.5–70) | r = −0.011, p = 0.915 | r = 0.031, p = 0.772 | r = 0.114, p = 0.287 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Späth, Z.; Tmava-Berisha, A.; Fellendorf, F.T.; Stross, T.; Maget, A.; Platzer, M.; Bengesser, S.A.; Häussl, A.; Zwigl, I.; Birner, A.; et al. Vitamin D Status in Bipolar Disorder. Nutrients 2023, 15, 4752. https://doi.org/10.3390/nu15224752
Späth Z, Tmava-Berisha A, Fellendorf FT, Stross T, Maget A, Platzer M, Bengesser SA, Häussl A, Zwigl I, Birner A, et al. Vitamin D Status in Bipolar Disorder. Nutrients. 2023; 15(22):4752. https://doi.org/10.3390/nu15224752
Chicago/Turabian StyleSpäth, Zita, Adelina Tmava-Berisha, Frederike T. Fellendorf, Tatjana Stross, Alexander Maget, Martina Platzer, Susanne A. Bengesser, Alfred Häussl, Ina Zwigl, Armin Birner, and et al. 2023. "Vitamin D Status in Bipolar Disorder" Nutrients 15, no. 22: 4752. https://doi.org/10.3390/nu15224752
APA StyleSpäth, Z., Tmava-Berisha, A., Fellendorf, F. T., Stross, T., Maget, A., Platzer, M., Bengesser, S. A., Häussl, A., Zwigl, I., Birner, A., Queissner, R., Stix, K., Wels, L., Lenger, M., Dalkner, N., Zelzer, S., Herrmann, M., & Reininghaus, E. Z. (2023). Vitamin D Status in Bipolar Disorder. Nutrients, 15(22), 4752. https://doi.org/10.3390/nu15224752