
A Systematic Review and Meta-Analysis Exploring Variations in Copper Levels between Individuals with Malaria and Uninfected Controls

 , ,
, ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. International Prospective Register of Systematic Review (PROSPERO) Registration
2.2. Outcomes
2.3. Search Strategy
2.4. Inclusion and Exclusion Criteria
2.5. Study Selection and Data Extraction
2.6. Quality Assessment
2.7. Data Synthesis and Analysis
2.8. Sensitivity Analysis
3. Results
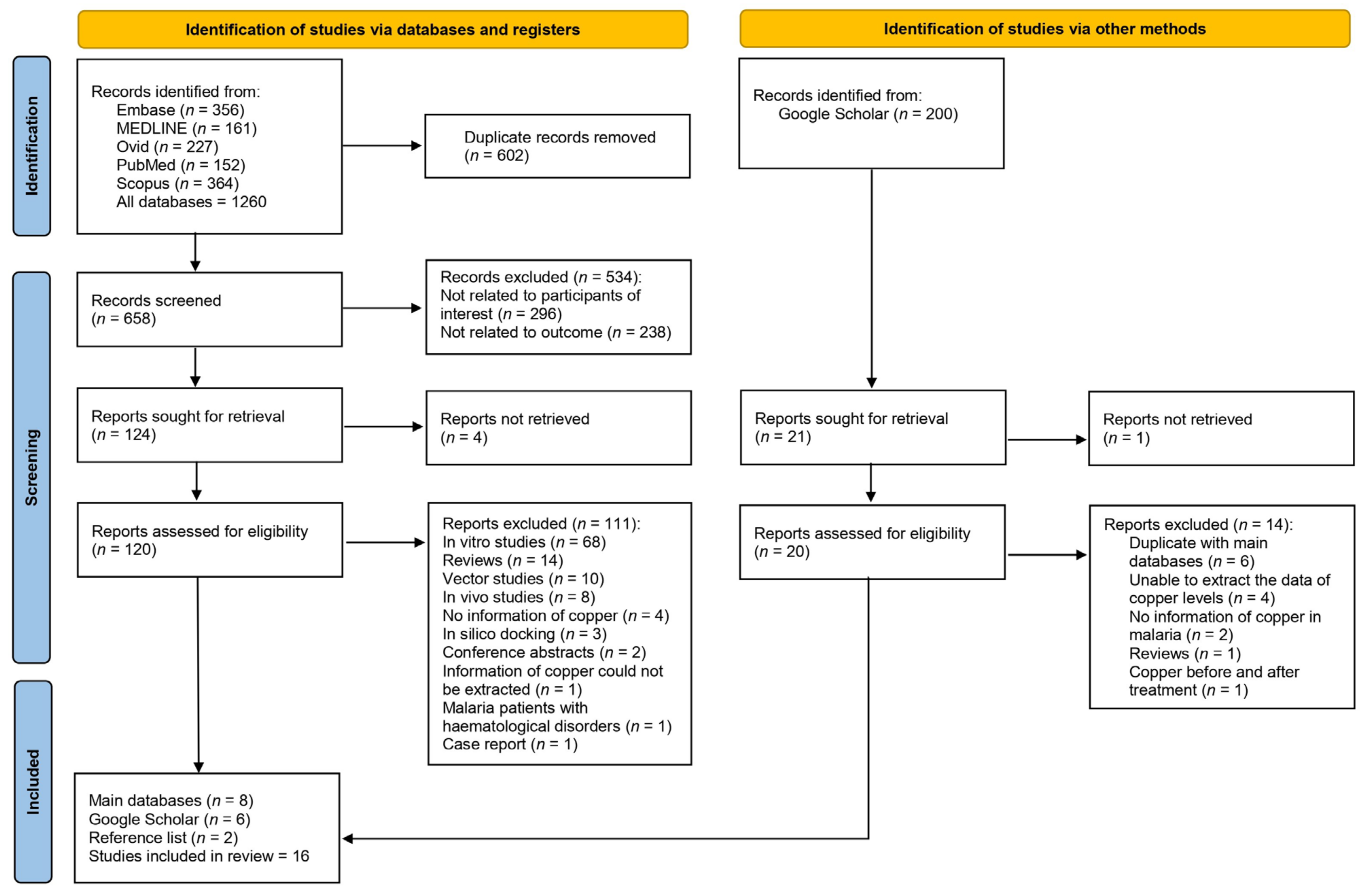
3.1. Search Results
3.2. Studies’ Characteristics
3.3. Quality of the Studies
3.4. Qualitative Synthesis of Copper Levels in Malaria
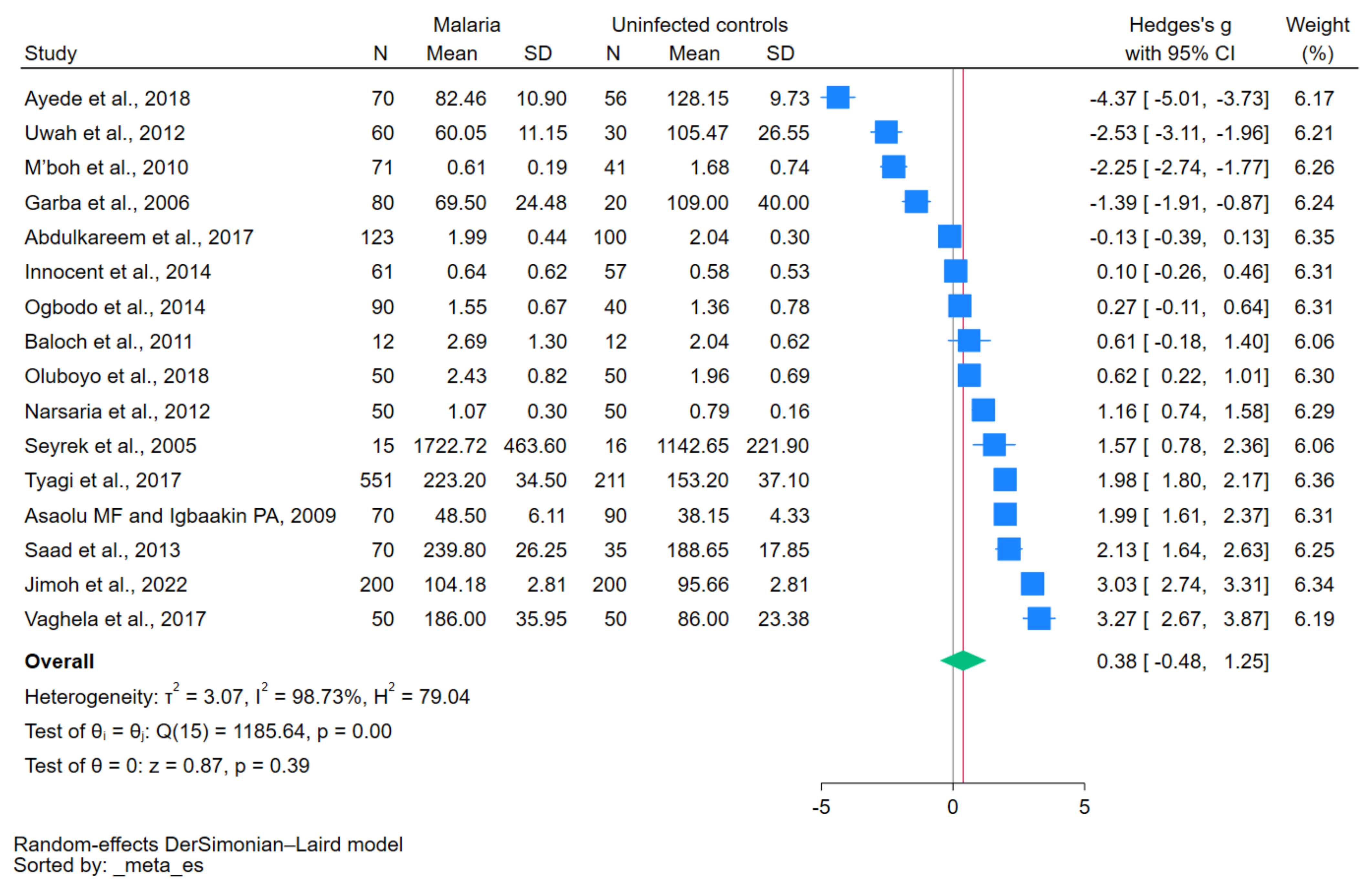
3.5. Difference in Copper Levels between Patients with Malaria and Uninfected Controls
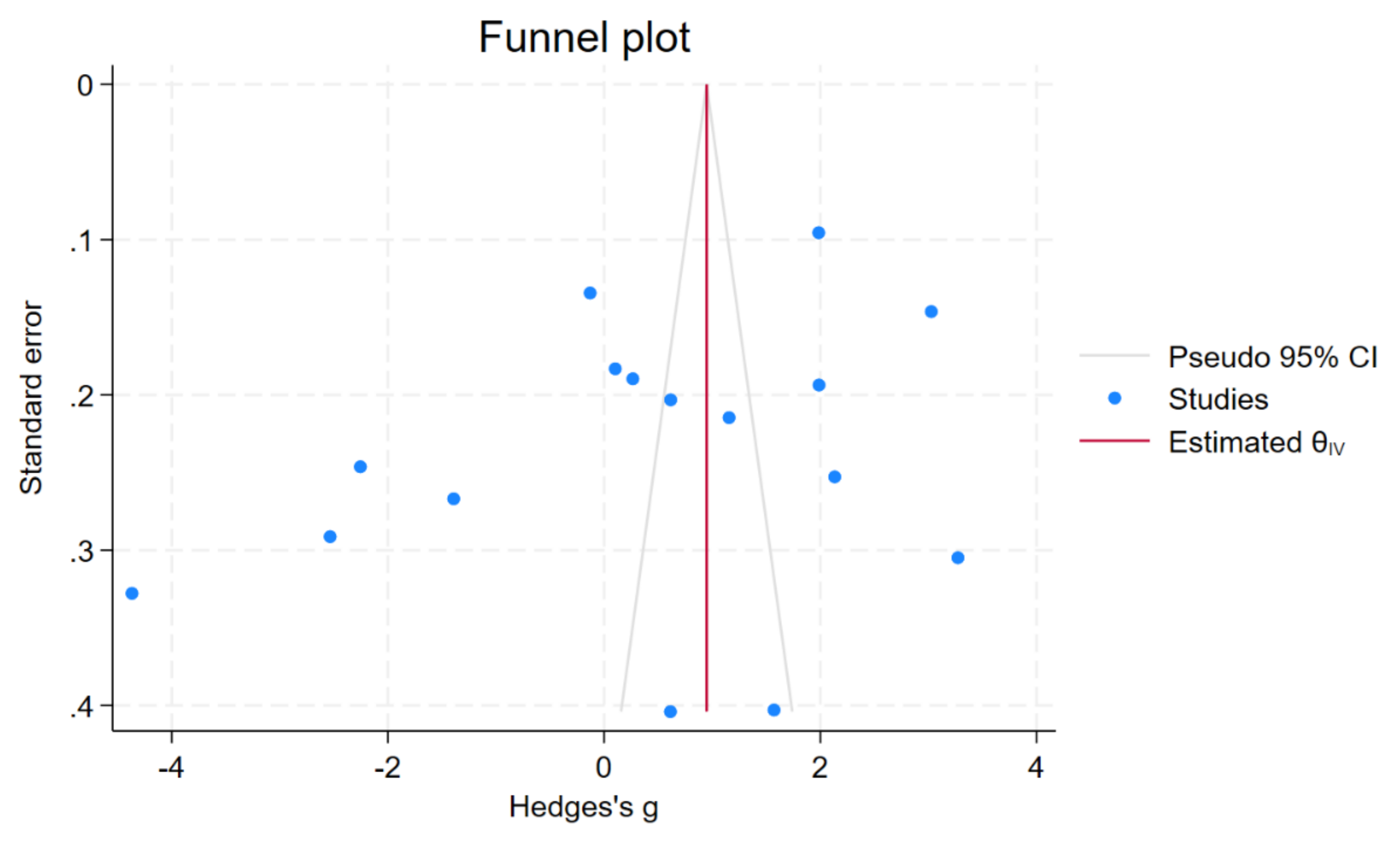
3.6. Publication Bias
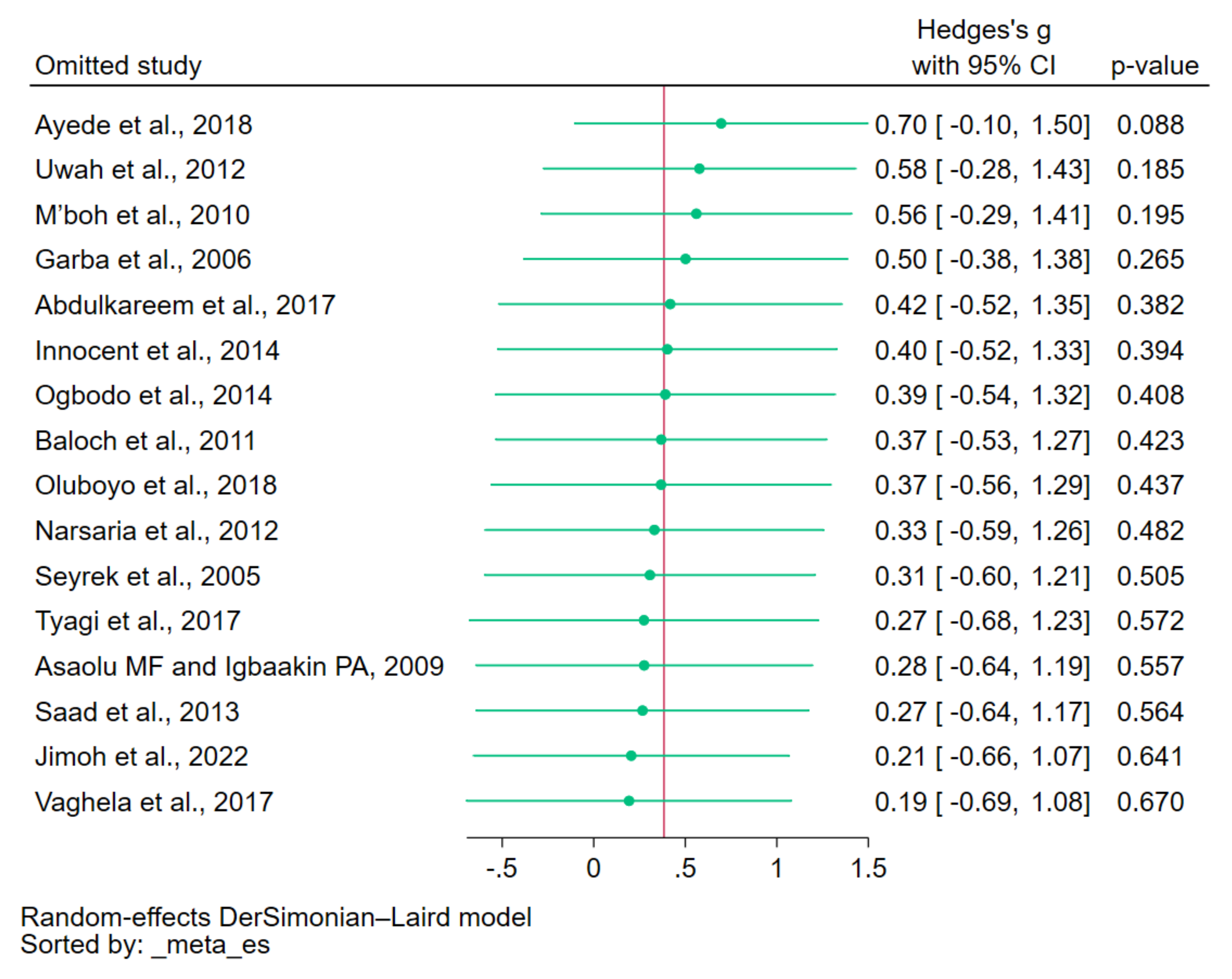
3.7. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. World Malaria Report 2022. 2022. Available online: https://www.who.int/publications/i/item/9789240064898 (accessed on 8 July 2023).
- WHO. WHO Guidelines for Malaria. 2022. Available online: https://www.who.int/publications/i/item/guidelines-for-malaria (accessed on 8 July 2023).
- Battle, K.E.; Baird, J.K. The global burden of Plasmodium vivax malaria is obscure and insidious. PLoS Med. 2021, 18, e1003799. [Google Scholar] [CrossRef]
- Wångdahl, A.; Sondén, K.; Wyss, K.; Stenström, C.; Björklund, D.; Zhang, J.; Askling, H.H.; Carlander, C.; Hellgren, U.; Färnert, A. Relapse of Plasmodium vivax and Plasmodium ovale malaria with and without primaquine treatment in a nonendemic area. Clin. Infect. Dis. 2021, 74, 1199–1207. [Google Scholar] [CrossRef]
- Oriero, E.C.; Amenga-Etego, L.; Ishengoma, D.S.; Amambua-Ngwa, A. Plasmodium malariae, current knowledge and future research opportunities on a neglected malaria parasite species. Crit. Rev. Microbiol. 2021, 47, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Jeyaprakasam, N.K.; Liew, J.W.K.; Low, V.L.; Wan-Sulaiman, W.-Y.; Vythilingam, I. Plasmodium knowlesi infecting humans in Southeast Asia: What’s next? PLoS Neglected Trop. Dis. 2020, 14, e0008900. [Google Scholar] [CrossRef] [PubMed]
- Mbanefo, A.; Kumar, N. Evaluation of malaria diagnostic methods as a key for successful control and elimination programs. Trop. Med. Infect. Dis. 2020, 5, 102. [Google Scholar] [CrossRef]
- Fitri, L.E.; Widaningrum, T.; Endharti, A.T.; Prabowo, M.H.; Winaris, N.; Nugraha, R.Y.B. Malaria diagnostic update: From conventional to advanced method. J. Clin. Lab. Anal. 2022, 36, e24314. [Google Scholar] [CrossRef]
- Takeki, Y.; Muneaki, H.; Kenji, N.; Takahiro, N.; Yasuyuki, S.; Takuya, H.; Ido, Y.; Yatsushiro, S.; Abe, K.; Kajimoto, K.; et al. Field evaluation of a quantitative, and rapid malaria diagnostic system using a fluorescent Blue-ray optical device. bioRxiv 2019, bioRxiv:721076. [Google Scholar] [CrossRef]
- Arndt, L.; Koleala, T.; Orbán, A.; Ibam, C.; Lufele, E.; Timinao, L.; Lorry, L.; Butykai, A.; Kaman, P.; Molnár, A.P.; et al. Magneto-optical diagnosis of symptomatic malaria in Papua New Guinea. Nat. Commun. 2021, 12, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Peng, W.K.; Kong, T.F.; Ng, C.S.; Chen, L.; Huang, Y.; Bhagat, A.A.S.; Nguyen, N.-T.; Preiser, P.R.; Han, J. Micromagnetic resonance relaxometry for rapid label-free malaria diagnosis. Nat. Med. 2014, 20, 1069–1073. [Google Scholar] [CrossRef]
- Abdulkareem, B.O.; Adam, A.O.; Ahmed, A.O.; Mariam, A.A.; Samuel, U.U. Malaria-induced anaemia and serum micronutrients in asymptomatic Plasmodium falciparum infected patients. J. Parasit. Dis. 2017, 41, 1093–1097. [Google Scholar] [CrossRef]
- Alexandre, M.A.A.; Benzecry, S.G.; Siqueira, A.M.; Vitor-Silva, S.; Melo, G.C.; Monteiro, W.M.; Leite, H.P.; Lacerda, M.V.G.; Alecrim, M.d.G.C. The association between nutritional status and malaria in children from a rural community in the Amazonian region: A longitudinal study. PLoS Neglected Trop. Dis. 2015, 9, e0003743. [Google Scholar] [CrossRef] [PubMed]
- Frosch, A.E.P.; Ondigo, B.; Ayodo, G.A.; Vulule, J.M.; John, C.C.; Cusick, S.E. Decline in childhood iron deficiency after interruption of malaria transmission in highland Kenya. Am. J. Clin. Nutr. 2014, 100, 968–973. [Google Scholar] [CrossRef] [PubMed]
- Shankar, A.H.; Genton, B.; Semba, R.D.; Baisor, M.; Paino, J.; Tamja, S.; Adiguma, T.; Wu, L.; Rare, L.; Tielsch, J.M.; et al. Effect of vitamin A supplementation on morbidity due to Plasmodium falciparum in young children in Papua New Guinea: A randomised trial. Lancet 1999, 354, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Shankar, A.H.; West, K.P.; Rare, L.; Bannon, D.; Adiguma, T.; Tielsch, J.M.; Wu, L.; Baisor, M.; Tamja, S.; Paino, J.; et al. The influence of zinc supplementation on morbidity due to Plasmodium falciparum: A randomized trial in preschool children in Papua New Guinea. Am. J. Trop. Med. Hyg. 2000, 62, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Neuberger, A.; Okebe, J.; Yahav, D.; Paul, M. Oral iron supplements for children in malaria-endemic areas. Cochrane Database Syst. Rev. 2016, 2, CD006589. [Google Scholar] [CrossRef] [PubMed]
- Barceloux, D.G. Copper. J. Toxicol. Clin. Toxicol. 1999, 37, 217–230. [Google Scholar] [CrossRef]
- Hordyjewska, A.; Popiołek, Ł.; Kocot, J. The many “faces” of copper in medicine and treatment. BioMetals 2014, 27, 611–621. [Google Scholar] [CrossRef]
- Cheng, F.; Peng, G.; Lu, Y.; Wang, K.; Ju, Q.; Ju, Y.; Ouyang, M. Relationship between copper and immunity: The potential role of copper in tumor immunity. Front. Oncol. 2022, 12, 1019153. [Google Scholar] [CrossRef] [PubMed]
- Percival, S.S. Copper and immunity. Am. J. Clin. Nutr. 1998, 67, 1064S–1068S. [Google Scholar] [CrossRef]
- Husain, N.; Mahmood, R. Copper(II) generates ROS and RNS, impairs antioxidant system and damages membrane and DNA in human blood cells. Environ. Sci. Pollut. Res. Int. 2019, 26, 20654–20668. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Moola, S.M.Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; Mu, P.-F. Chapter 7: Systematic Reviews of Etiology and Risk: JBI. 2020. Available online: https://synthesismanual.jbi.global (accessed on 5 September 2023).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; Updated March 2011; The Cochrane Collaboration: London, UK, 2011; Available online: https://www.handbook.cochrane.org (accessed on 5 September 2023).
- Willis, B.H.; Riley, R.D. Measuring the statistical validity of summary meta-analysis and meta-regression results for use in clinical practice. Stat. Med. 2017, 36, 3283–3301. [Google Scholar] [CrossRef]
- Ayede, A.I.; Amoo, B.L.; Anetor, J.I.; Adeola, A.S. Status of Some Basic Antioxidants in pre- and postmalaria treatment in children. J. Child Sci. 2018, 8, e31–e35. [Google Scholar] [CrossRef]
- Baloch, S.; Memon, S.; Gachal, G.; Baloch, M. determination of trace metals abnormalities in patients with vivax malaria. Iran J. Parasitol. 2011, 6, 54–59. [Google Scholar] [PubMed]
- Garba, I.H.; Ubom, G.A.; Ejiogu, N.B. Serum copper concentration in adults with acute, uncomplicated falciparum malaria infection. Biol. Trace Elem. Res. 2006, 113, 125–130. [Google Scholar] [CrossRef]
- Narsaria, N.; Mohanty, C.; Das, B.K.; Mishra, S.P.; Prasad, R. Oxidative stress in children with severe malaria. J. Trop. Pediatr. 2012, 58, 147–150. [Google Scholar] [CrossRef]
- Saad, A.A.; Doka, Y.A.; Osman, S.M.; Magzoub, M.; Ali, N.I.; Adam, I. Zinc, copper and C-reactive protein in children with severe Plasmodium falciparum malaria in an area of unstable malaria transmission in eastern Sudan. J. Trop. Pediatr. 2013, 59, 150–153. [Google Scholar] [CrossRef]
- Seyrek, A.; Kocyigit, A.; Erel, O. Essential trace elements selenium, zinc, copper, and iron concentrations and their related acute-phase proteins in patients with vivax malaria. Biol. Trace Elem. Res. 2005, 106, 107–116. [Google Scholar] [CrossRef]
- Tyagi, R.A.; Tyagi, A.G.; Ram Choudhary, P.; Shekhawat, J.S. Study of cation imbalance in patients of malaria. Physiol. Pharmacol. 2017, 21, 175–184. [Google Scholar]
- Asaolu, M.F.; Igbaakin, P.A. Serum levels of micronutrients and antioxidants during malaria in pregnant women in Ado-Ekiti, Ekiti State, Nigeria. Int. J. Med. Med. Sci. 2009, 1, 523–526. [Google Scholar]
- Doka, Y.A. Zinc and Copper Levels in Children with Severe Plasmodium falciparum malaria in an Area of Unstable Malaria Transmission in Eastern Sudan; University of Khartoum: Khartoum, Sudan, 2003. [Google Scholar]
- Innocent, K.K.; Melaine, M.G.; Issa, B.; Joseph, D.A. Assessment of serum iron, manganese and Cu/Zn ratio in the course of falciparum malaria among Ivorian patients (Côte d’Ivoire). Int. J. Biochem. Res. Rev. 2014, 4, 527–535. [Google Scholar] [CrossRef]
- Jimoh, B.O.; Fadipe, M.T.; Emokpae, M.A. Serum copper, zinc, and copper−zinc ratio in children with malaria. Saudi J. Health Sci. 2022, 11, 119–124. [Google Scholar]
- M’boh, M.G.; Yapi, F.H.; Ahiboh, H.T.; Yapo, A.; Bla, B.K.; Djaman, J.A. The effect of falciparum malaria infection on the quantity of trace elements (iron, copper, zinc) in the blood in children of Côte d’Ivoire. Agric. Biol. J. N. Am. 2010, 1, 565–570. [Google Scholar]
- Ogbodo, S.O.; Okaka, A.N.C.; Nwagha, U.I.; Ejezie, F.E.; Okafor, C.S. Oxidative stress in symptomatic malaria parasitemic pregnant women from malaria endemic area of Nigeria. Am. J. Med. Sci. 2014, 4, 168–174. [Google Scholar]
- Uwah, A.F.; Otitoju, O.; Ndem, J.I.; Akpanabiatu, M.I.; Akpanyung, E.O. Effect of malaria infection on serum copper, iron and beta-carotene levels in Nigerian children. Eur. J. Sci. Res. 2012, 86, 573–579. [Google Scholar]
- Oluboyo, A.O.; Fakologbon, O.D.; Oluboyo, B.O.; Odewusi, O.O.; Ajayi, F.O. Variations in levels of selected micronutrients during malaria infection: A study from Ado-Ekiti, Ekiti, Nigeria. J. Biomed. Sci. 2018, 5, 4–9. [Google Scholar] [CrossRef][Green Version]
- Vaghela, V.K.; Vaghela, B.K.; Vaghela, J.K. Study of serum zinc and copper level in children with malarial infection in Civil Hospital, Ahmedabad. Int. J. Clin. Biochem. Res. 2018, 5, 26–30. [Google Scholar]
- Cheung, K.-S.; Seto, W.-K.; Fung, J.; Mak, L.-Y.; Lai, C.-L.; Yuen, M.-F. Epidemiology and natural history of Wilson’s disease in the Chinese: A territory-based study in Hong Kong between 2000 and 2016. World J. Gastroenterol. 2017, 23, 7716–7726. [Google Scholar] [CrossRef]
- Cheng, N.; Wang, K.; Hu, W.; Sun, D.; Wang, X.; Hu, J.; Yang, R.; Han, Y. Wilson disease in the South Chinese Han population. Can. J. Neurol. Sci. 2014, 41, 363–367. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Luan, J.; Zhou, X.; Cui, Y.; Han, J. Epidemiology, diagnosis, and treatment of Wilson’s disease. Intractable Rare Dis. Res. 2017, 6, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Doolan, D.L.; Dobaño, C.; Baird, J.K. Acquired immunity to malaria. Clin. Microbiol. Rev. 2009, 22, 13–36. [Google Scholar] [CrossRef]
- Lian, S.; Zhang, T.; Yu, Y.; Zhang, B. Relationship of circulating copper level with gestational diabetes mellitus: A meta-analysis and systemic review. Biol. Trace Elem. Res. 2021, 199, 4396–4409. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Li, B.; Li, Z.; Wang, J.; Zhang, D. High serum copper level is associated with an increased risk of preeclampsia in Asians: A meta-analysis. Nutr. Res. 2017, 39, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Shen, R.; Huang, L.; Yu, J.; Rong, H. Association between serum copper and heart failure: A meta-analysis. Asia Pac. J. Clin Nutr. 2019, 28, 761–769. [Google Scholar] [CrossRef]
- Quinn, J.F.; Harris, C.; Kaye, J.A.; Lind, B.; Carter, R.; Anekonda, T.; Ralle, M. Gender effects on plasma and brain copper. Int. J. Alzheimers Dis. 2011, 2011, 150916. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | N (16 Studies) | % |
|---|---|---|
| Publication year | ||
| 2010–2023 | 13 | 81.2 |
| 2000–2009 | 3 | 18.8 |
| Study designs | ||
| Cross-sectional studies | 12 | 75.0 |
| Case–control studies | 4 | 25.0 |
| Study areas | ||
| Africa | 11 | 68.8 |
| Nigeria | 8 | 50.0 |
| Cote d’Ivoire | 2 | 12.5 |
| Sudan | 1 | 6.25 |
| Asia | 5 | 31.2 |
| India | 3 | 18.8 |
| Pakistan | 1 | 6.25 |
| Turkey | 1 | 6.25 |
| Plasmodium species | ||
| P. falciparum | 10 | 62.5 |
| P. falciparum and P. vivax | 1 | 6.25 |
| P. vivax | 1 | 6.25 |
| Not specified | 4 | 25.0 |
| Age group | ||
| Children | 7 | 43.8 |
| Adults | 4 | 25.0 |
| All age groups | 4 | 25.0 |
| Not specified | 1 | 6.25 |
| Methods for malaria detection | ||
| Microscopy | 15 | 93.8 |
| Microscopy/RDT | 1 | 6.25 |
| Methods for copper measurement | ||
| Atomic absorption spectrophotometry | 13 | 81.3 |
| Spectrophotometry | 3 | 18.7 |
| Blood used for copper measurement | ||
| Serum | 12 | 75.0 |
| Plasma | 4 | 25.0 |
| Subgroup Analyses | p Value | Hedges’ g (95% CI) | I2 (%) | Number of Studies |
|---|---|---|---|---|
| Publication years | ||||
| 2010–2023 | 0.54 | 0.31 (−0.68 to 1.29) | 98.89 | 13 |
| 2000–2009 | 0.54 | 0.72 (−1.56 to 3.00) | 98.15 | 3 |
| Study design | ||||
| Cross–sectional study | 0.79 | −0.14 (−1.13 to 0.85) | 98.36 | 12 |
| Case–control study | <0.01 | 1.96 (1.19 to 2.74) | 95.19 | 4 |
| Continent | ||||
| Africa | 0.71 | −0.22 (−1.37 to 0.93) | 98.93 | 11 |
| Asia | <0.01 | 1.74 (1.04 to 2.44) | 90.88 | 5 |
| Age group | ||||
| Children | 0.95 | 0.07 (−2.04 to 2.18) | 99.30 | 7 |
| Adults | 0.55 | 0.38 (−0.87 to 1.62) | 97.28 | 4 |
| All age groups | 0.18 | 0.87 (−0.40 to 2.14) | 98.50 | 4 |
| Age not specified | N/A | 0.61 (−0.18 to 1.40) | N/A | 1 |
| Plasmodium species | ||||
| P. falciparum | 0.74 | −0.22 (−1.52 to 1.08) | 99.04 | 10 |
| P. vivax | N/A | 1.57 (0.78 to 2.36) | N/A | 1 |
| P. falciparum, P. vivax | N/A | 3.27 (2.67 to 3.87) | N/A | 1 |
| Not specified | 0.09 | 0.88 (0.13 to 1.90) | 96.72 | 4 |
| Diagnostic method for malaria | ||||
| Microscopy | 0.48 | 0.33 (−0.59 to 1.26) | 98.82 | 15 |
| Microscopy/RDT | N/A | 1.16 (0.74 to 1.58) | N/A | 1 |
| Types of blood samples | ||||
| Serum | 0.91 | 0.07 (−1.10 to 1.24) | 98.92 | 12 |
| Plasma | <0.01 | 1.33 (0.60 to 2.07) | 93.11 | 4 |
| Methods for copper measurement | ||||
| Atomic absorption spectrophotometry | 0.59 | 0.26 (−0.70 to 1.22) | 98.56 | 13 |
| Spectrophotometry | 0.53 | 0.91 (−1.93 to 3.75) | 99.19 | 3 |
| Databases | ||||
| Main databases | 0.75 | 0.20 (−1.05 to 1.45) | 98.72 | 8 |
| Other sources (Google Scholar and reference list) | 0.42 | 0.56 (−0.80 to 1.93) | 98.90 | 8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kotepui, K.U.; Mahittikorn, A.; Wilairatana, P.; Masangkay, F.R.; Kotepui, M. A Systematic Review and Meta-Analysis Exploring Variations in Copper Levels between Individuals with Malaria and Uninfected Controls. Nutrients 2023, 15, 4749. https://doi.org/10.3390/nu15224749
Kotepui KU, Mahittikorn A, Wilairatana P, Masangkay FR, Kotepui M. A Systematic Review and Meta-Analysis Exploring Variations in Copper Levels between Individuals with Malaria and Uninfected Controls. Nutrients. 2023; 15(22):4749. https://doi.org/10.3390/nu15224749
Chicago/Turabian StyleKotepui, Kwuntida Uthaisar, Aongart Mahittikorn, Polrat Wilairatana, Frederick Ramirez Masangkay, and Manas Kotepui. 2023. "A Systematic Review and Meta-Analysis Exploring Variations in Copper Levels between Individuals with Malaria and Uninfected Controls" Nutrients 15, no. 22: 4749. https://doi.org/10.3390/nu15224749
APA StyleKotepui, K. U., Mahittikorn, A., Wilairatana, P., Masangkay, F. R., & Kotepui, M. (2023). A Systematic Review and Meta-Analysis Exploring Variations in Copper Levels between Individuals with Malaria and Uninfected Controls. Nutrients, 15(22), 4749. https://doi.org/10.3390/nu15224749