

Health Benefits of Bread Fortification: A Systematic Review of Clinical Trials according to the PRISMA Statement



Abstract
:
1. Introduction
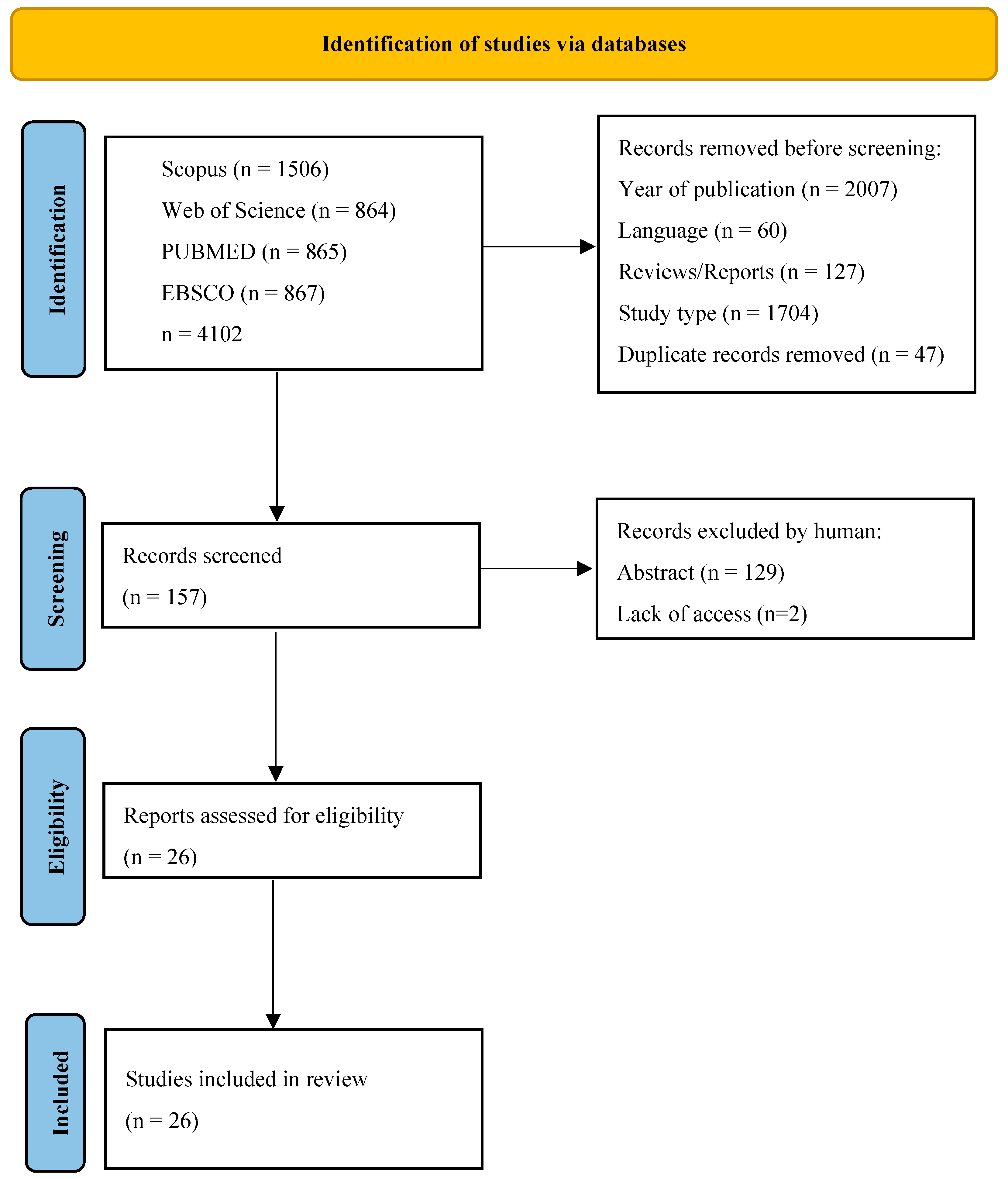
2. Materials and Methods
3. Results
3.1. Influence of Fortified Bread on Human Health
3.1.1. Minerals

{kind=link}
{kind=link}
| Jadad Scale | Participants | Fortificant/Substance/ Dose/Inhibitor | Duration | Methods/Analysis | Results | References/ Country |
|---|---|---|---|---|---|---|
| 1 | Young male adults; N = 11; Age: 18–30 BMI: 23.8–28.6 | Potassium, Magnesium, Phosphorus; 3.6 g of MgCO3 and 12.5 g of KH2PO4/kg of flour; 7.2 g of MgCO3 and 25 g of KH2PO4/kg of flour | 30 days | Venous blood; PG; GR; IR; triacylglycerols; total P, Mg, and K; HOMA-IR | TG and GR after consumption of fortified bread maintained at a lower level compared to control. | [14] Lebanon |
| 3 | Mother–child pairs; N = 22; Age: 18–45, 2.5–5. | Iron; 2/4 mg of 57Fe as FeFum, 2/4 mg of NaFeEDTA (Na58FeEDTA and Na57FeEDTA); 2–4 mg/day (4 times during experiment) | 28 days | Venous blood, FIA, BIS | FIA from NaFeEDTA is 40% higher than from FeFum; combination of both fortificants does not lead to a significant increase in FIA. | [15] Haiti |
| 1 | Women; N = 46; Age: 18–49; Anemic: Hb < 12 g/dL, Non-anemic: Hb ≥ 12 g/dL; BMI: 20.4–25.4 | Iron; 6 mg of 57Fe as NaFeEDTA, 6 mg (3 mg/3 mg) of 58Fe/56Fe as NaFeEDTA; Tea | 17 days | Venous blood, FIA | Fe from NaFeEDTA increases by 17% in the anemia-free group and 33% in the iron-deficient group; tea consumption reduced iron absorption (>85%) in both groups. NaFeEDTA cannot overcome the inhibition of tea polyphenols. | [16] Morocco |
| 1 | Mother–child pairs; N = 17; Age: 18–40, 2–6 BMI: 21.7–22.11. | Iron; 2/4 mg of 58FeSO4, 2/4 mg of 57FeFum; Tea | 30 days | Venous blood, FAFe | Fe absorbed from FeSO4 was 8.85% higher than for FeFum in mothers, and 56.36% in children. Tea reduced FAFe by 44–65%. | [17] Senegal |
| 0 | Women; N = 12; Age: 33–42 BMI: 25.8–30.1 | Iron, Zinc; 58FeSO4, ZnSO4; Tea | 28 days | Venous blood, CI | Fe absorption from the bread fortified with iron was 19.8% (10.5–37.2%); for 30 mg of Zn/kg, it was 18.5% (10.2–33.4%); 17.7% (7.7–38.7%) for 60 mg of Zn/kg; and 11.2% (6.2–20.3%) for 90 mg of Zn/kg. | [18] Chile |
| 3 | Children; N = 82; Age: 2–5. | Iron, Processed amaranth | 6 months | Venous blood, hemoglobin, serum ferritin, CCR | Hemoglobin concentration in the amaranth group increased significantly from 112.1 to 120.3 compared to the control (106.9–113.2 g/L); anemia prevalence: CCR (CI:95%) decrease from 0.57 to 0.37 in amaranth group (μU/mL). | [19] Ethiopia |
| 0 | Healthy adults; N= 12; Age: 19.6–27.2 BMI: 19.9–24.7 | Chromium; Cr-enriched yeast 500 μg of Cr/50 g of available carbohydrates | 4 weeks | Venous blood, PG, IR, GR, GI | GR after fortified bread was 101.27 mg/dL and 117.82 mg/dL, compared to control (128.46 mg/dL); GI of enriched breads was 34.22 and 62.35 while the control bread had GI = 100. | [21] Greece |
| 3 | Type 2 diabetes adults; N= 30; Age: 40–65 BMI: 27.9–31.1 | Chromium; Cr-enriched yeast 99.0 μg of Cr/28 g of bread | 12 weeks | Venous blood, BMI, GR, IR | Reduction in BMI from 29.3 to 28.9; decreased fasting plasma glucose from 143.2 to 129.6 (mg/dL); decrease of the mean glycosylated hemoglobin from 6.9 to 6.3 (%); decrease in fasting insulin from 6.8 to 4.4 (μU/mL). | [22] Greece |
| 0 | Healthy young adults; Type 2 diabetes adults; N= 10, 10; Age: 23–26, 43–65 BMI: 20–26.57 | Chromium, Magnesium, Selenium; Wheat varieties; Cr: 14.0–15.2 μg/100 g Mg: 32.9–85.6 mg/100 g Se: 1.6–5.5 μg/100 g Buckwheat; Mg: 172 mg/100 g Se: 3.5 μg/100 g | 2 h | Vein blood, GI, PG | Lower GI of Jizi439 by 19.67% and 10.78% (that of the mixture of white wheat and Chu20); the lowest PG in diabetes patients after Jizi439. | [23] China |
3.1.2. Vitamins
| Jadad Scale | Participants | Fortificant/Substance/ Dose/Inhibitor | Duration | Methods/Analysis | Results | References/ Country |
|---|---|---|---|---|---|---|
| 4 | Adults N = 45 Age: 18–45 BMI: 18.5–30 | Folic acid; Folate, Calcium L-5-methyltetrahydrofolic acid; 452 mg of L-5-MTHF/roll; 400 mg of folic acid/roll | 16 weeks | Venous blood, Plasma folate, Whole-blood folate concentrations | Increase in mean erythrocyte folate by 60% for L-5-MTHF, and by 44% for folic acid. | [24] Canada |
| 3 | Adult women N = 41 Age: 20–40 BMI: 19.9–24.5 | Vitamin D2, UV-treated baker’s yeast; 30.2 μg/100 g | 8 weeks | Venous blood sample, Serum 25-hydroxyvitamin D concentrations | Increase in S-25(OH)D2 concentration by 6.4 nmol/L. | [25] Finland |
| 4 | Adults N = 90 Age: 26–48 BMI: 21.7–31.2 | Vitamin D3, Vitamin premix, 25 μg/50 g | 8 weeks | Venous blood sample, serum 25-hydroxyvitamin D concentrations. | [26] Iran | |
| 0 | Young adults N = 27 Age: 20–29 BMI: 20–24 | Vitamin C; L-ascorbic acid; 5 ppm, 10 ppm, 15 ppm | 120 min (30, 60, 90, and 120 min) | Venous blood, GR, GI, GL | GR was the lowest for 5 ppm ascorbic acid brad: 85, 98, 101, 93, 92 for 72% flour extract, and 91, 90, 95, 91, 86 for 72% flour extract; lowest GI (83–90% flour extract) in variant fortified with 10 ppm ascorbic acid, lowest GL (42–90% flour extract) in variant fortified with 10 ppm ascorbic acid. | [27] Iraq |
3.1.3. Other Nutritional Compounds
Fiber
Protein
| Jadad Scale | Participants | Fortificant/Substance/ Dose/Inhibitor | Duration | Methods/Analysis | Results | References/ Country |
|---|---|---|---|---|---|---|
| 0 | Young adults N = 10 Age: 16–30 BMI: 27.6–36.6 | Fiber; pumpkin powder at 75 g/450 g of flour, corn powder at 20 g/450 g of flour | 3 days | Vein blood, SG, IR, SAS | SG after 120 min: enriched bread at 56.8 L vs. 75.9 mmol*min/L for control bread; MI after 120 min: 20,476 vs. 32,892 mmol*min/L; lower SAS | [28] New Zealand |
| 2 | Young adults N = 19 Age: 22–24 BMI: 22.2 | Fiber; arabinoxylan oligosaccharides: 8.9 g/portion, 18.4 g/portion; resistant starch: 6.6 g/portion, 15 g/portion | 3 h | Vein blood, GR, IR, ISI | GR decrease from 183.3 mmol min/L to 168.3 to 154.4 mmol min/L at 0–120 min; IR decreased from 0.050 nmol/l to 0.042 and 0.038 nmol/l; ISI increase from 478 to 512 and 551 | [29] Sweden |
| 5 | Adults N = 35 Age: 17–74 BMI: 18.5–29.99 | Fiber; VERSAFIBE™2470 at 16.5 g/portion | 3 weeks | Vein blood, GR, IR, PS, gastrointestinal tolerance | GR reduced by 43–45%, IR by 35–40%, reduced hunger | [30] USA |
| 4 | Adults N = 24 Age: 34–61 BMI: 22.1 | Fiber; arabinoxylan at 3.2 g/100 g | 7 days | Vein blood, PPG | PPG reduced by 20% | [31] Italy |
| 3 | Overweight or obese women with type 2 diabetes N = 48 Age: 25–55 BMI: 25–40 | Protein, whey protein at 20 g/portion | 12 weeks | Vein blood, GS, FGL, IL, LP, BP | FGL elevated from 154.50 to 178.50 mg/dL; IL increased from 22.45 to 44.30 μIU/mL and from 16.30 to 38.30 μIU/mL in experimental and placebo group, respectively | [32] Iran |
| 3 | Diabetes patients, women N = 30 Age: 30–50 BMI: 29.5 | Protein, soy flour | 8 weeks | Vein blood, metabolic profile (n > 30) | No statistically significant changes | [33] Iran |
| 3 | Overweight/obese women N = 30 Age: 19–35 BMI: 25–30 | Protein, soy flour | 15 weeks | Vein blood, LP, BP, anthropometric parameters, CVD factors, BMI, weight | Weight reduction by 4.8 kg; BMI reduction by 0.6 | [34] Iran |
3.1.4. Physiological Compounds
| Jadad Scale | Participants | Fortificant/Substance/ Dose/Inhibitor | Duration | Methods/Analysis | Results | References/ Country |
|---|---|---|---|---|---|---|
| 3 | Diabetes patients N = 122 Age: 19–50+ BMI: 22.7–38.3 | Phytochemicals/polyphenols; Borassus powder: (wheat flour: BRP; m:m) 2:1; 5:1; 10:1; 20:1 | 3 months | Venous blood, Physical parameters Visceral fat, Metabolic age SBP, DBP, TC | waste reduction from 98.3 ± 14.6 cm to 95.9 ± 15.8 cm; BMI reduction by 3.4; visceral fat reduction from 10.4 ± 3.2 to 9.9 ± 3.0; metabolic age reduced from 61:6 ± 13:4 to 59:3 ± 13:0; SBP reduced from 161.2 ± 25.5 to 137.6 ± 22.9; DBP reduced from 99.2 ± 13.6 to 85.1 ± 10.8; TC reduced from 5.9 to 4.9; LDL reduced from 3.4 to 2.8; HDL reduced from 2.2 to 1.5 | [35] Ghana |
| 0 | Diabetes patients Women N = 72 Age: 46–51 BMI: 35–37 | Polyphenols; Turmeric powder: 10/100 g Ginger powder: 10/100 g | 8 weeks | Vein blood, Physical parameters (>10), CVD risk factors | BMI reduction from 37 to 36, 35 to 34; BF reduction of 1–1.5%; TG reduction from 139.28 to 118 mg/dL, 135 to 102 mg/dL; TC from 234 to 205, 218 to 183; CVDrf decreased from 5.17 to 3.99, 4.73–3.63 | [36] Egypt |
| 0 | Healthy adults N = 15 Age: 35–65 BMI: 21–32 | Phenolic acids, Native ray bran: Ferulic acid—134 mg/portion; Sinapic acid—31 mg/portion; 4-Coumaric acid—4.7 mg/portion; Bioprocessed rye bran: Ferulic acid—117 mg/portion; Sinapic acid—28 mg/portion; 4-Coumaric acid—5 mg/portion | 24 h | Vein blood, Urine samples; Postprandial phenolic acid excretions, GR | Bioprocessing of rye bran increased FA absorption by 14% vs. native rye bran | [37] Finland |
| 5 | Healthy adults N = 36, 39 Age: 18–70 BMI: <40 kg | Phytosterols; Vegapure® 67WDP (BASF): 2.3g/2 slices; Curcumin: 228 mg/2 slices | 4 weeks | Venous blood, TC, LDL, CVD risk | TC decrease of 0.52 mmol/L; LDL decrease of 0.49 mmol/L–124.33 nmol/L; CVD risk decreased from 1.1 to 12.7% | [38] Australia |
| 1 | Healthy adults N = 13 Age: 20–46 BMI: 19.4–29.7 | Polyphenols; Green tea extract powder: 0.4% of loaf weight in g; Baobab fruit extract powder: 1.88% of loaf weight in g | 6 days | Vein blood, GR, IR, Satiety | No statistically significant changes | [39] Australia |
| 5 | CVD risk patients N = 30 Age: 18–65 BMI: 23–31 | Neurotransmitters, Enzyme inhibitors, γ-Aminobutyric acid: 22.8 mg/100 g; Angiotensin-converting enzyme inhibitor: 7.23 mg/g (LSBþG) | 112 days | Vein blood, Urine samples, BP, GM, Endothelial function | BP decreased for 2.12 mmHg for LSBþG | [40] Spain |
3.2. Health Benefits of Consumption of Fortified Bread
4. Discussion
5. Strength
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dwyer, J.T.; Wiemer, K.L.; Dary, O.; Keen, C.L.; King, J.C.; Miller, K.B.; Philbert, M.A.; Tarasuk, V.; Taylor, C.L.; Gaine, P.C.; et al. Forti Fi Cation and Health: Challenges and Opportunities 1–4. Adv. Nutr. 2015, 15, 124–131. [Google Scholar] [CrossRef] [PubMed]
- John, R.; Singla, A. Functional Foods: Components, Health Benefits, Challenges, and Major Projects. DRC Sustain. Future J. Environ. Agric. Energy 2021, 2, 61–72. [Google Scholar] [CrossRef]
- Ahmad, S.; Al-Shabib, N.A. Functional Food Products and Sustainable Health, 1st ed.; Springer Nature Singapore Pte Ltd.: Singapore, 2020; ISBN 9789811547157. [Google Scholar]
- Dary, O.; Hurrell, R. Guidelines on Food Fortification with Micronutrients; World Health Organization, Food and Agricultural Organization of the United Nations: Geneva, Switzerland, 2006; pp. 1–376.
- Bishai, D.; Nalubola, R. The History of Food Fortification in the United States: Its Relevance for Current Fortification Efforts in Developing Countries. Econ. Dev. Cult. Chang. 2002, 51, 37–53. [Google Scholar] [CrossRef]
- Olson, R.; Gavin-Smith, B.; Ferraboschi, C.; Kraemer, K. Food Fortification: The Advantages, Disadvantages and Lessons from Sight and Life Programs. Nutrients 2021, 13, 1118. [Google Scholar] [CrossRef] [PubMed]
- Sajdakowska, M.; Gębski, J.; Jeżewska-Zychowicz, M.; Królak, M. Consumer Choices in the Bread Market: The Importance of Fiber in Consumer Decisions. Nutrients 2021, 13, 132. [Google Scholar] [CrossRef] [PubMed]
- Bredariol, P.; Vanin, F.M. Bread Baking Review: Insight into Technological Aspects in Order to Preserve Nutrition. Food Rev. Int. 2022, 38, 651–668. [Google Scholar] [CrossRef]
- Żakowska-Biemans, S.; Kostyra, E. Sensory Profile, Consumers’ Perception and Liking of Wheat–Rye Bread Fortified with Dietary Fibre. Appl. Sci. 2023, 13, 694. [Google Scholar] [CrossRef]
- Bangar, S.P.; Siroha, A.K. Functional Cereals and Cereal Foods: Properties, Functionality and Applications; Springer: Cham, Switzerland, 2022; ISBN 9783031056116. [Google Scholar]
- Rosell, C.M.; Bajerska, J.; El Sheikha, A.F. Bread and Its Fortification, 1st ed.; CRC Press: Boca Raton, FL, USA, 2015. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 88, 105906. [Google Scholar]
- Clark, H.D.; Wells, G.A.; Huët, C.; McAlister, F.A.; Salmi, L.R.; Fergusson, D.; Laupacis, A. Assessing the Quality of Randomized Trials: Reliability of the Jadad Scale. Control. Clin. Trials 1999, 20, 448–452. [Google Scholar] [CrossRef]
- El Khoury, R.; El Solh, N.; Olabi, A.; Toufeili, I.; Hlais, S.; Obeid, O. Macromineral Enrichment of White Bread Reduces Postprandial Glycaemia without Altering Sensory Properties: A Crossover Study. East Mediterr. Health J. 2020, 26, 1388–1395. [Google Scholar] [CrossRef]
- Herter-Aeberli, I.; Eliancy, K.; Rathon, Y.; Loechl, C.U.; Marhône Pierre, J.; Zimmermann, M.B. In Haitian Women and Preschool Children, Iron Absorption from Wheat Flour-Based Meals Fortified with Sodium Iron EDTA Is Higher than That from Meals Fortified with Ferrous Fumarate, and Is Not Affected by Helicobacter Pylori Infection in Children. Br. J. Nutr. 2017, 118, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Lazrak, M.; El Kari, K.; Stoffel, N.U.; Elammari, L.; Al-Jawaldeh, A.; Loechl, C.U.; Yahyane, A.; Barkat, A.; Zimmermann, M.B.; Aguenaou, H. Tea Consumption Reduces Iron Bioavailability from NaFeEDTA in Nonanemic Women and Women with Iron Deficiency Anemia: Stable Iron Isotope Studies in Morocco. J. Nutr. 2021, 151, 2714–2720. [Google Scholar] [CrossRef]
- Ndiaye, N.F.; Idohou-Dossou, N.; Bürkli, S.; Diouf, A.; Loucoubar, C.; Guiro, A.T.; Zimmermann, M.B.; Wade, S.; Moretti, D. Polyphenol-Rich Tea Decreases Iron Absorption from Fortified Wheat Bread in Senegalese Mother–Child Pairs and Bioavailability of Ferrous Fumarate Is Sharply Lower in Children. Eur. J. Clin. Nutr. 2020, 74, 1221–1228. [Google Scholar] [CrossRef] [PubMed]
- Olivares, M.; Castro, C.; Pizarro, F.; López De Romaña, D. Effect of Increasing Levels of Zinc Fortificant on the Iron Absorption of Bread Co-Fortified with Iron and Zinc Consumed with a Black Tea. Biol. Trace Elem. Res. 2013, 154, 321–325. [Google Scholar] [CrossRef] [PubMed]
- Orsango, A.Z.; Loha, E.; Lindtjørn, B.; Engebretsen, I.M.S. Efficacy of Processed Amaranth-Containing Bread Compared to Maize Bread on Hemoglobin, Anemia and Iron Deficiency Anemia Prevalence among Two-to-Five Year-Old Anemic Children in Southern Ethiopia: A Cluster Randomized Controlled Trial. PLoS ONE 2020, 15, e0239192. [Google Scholar] [CrossRef]
- Hurrell, R.F. Ensuring the Efficacious Iron Fortification of Foods: A Tale of Two Barriers. Nutrients 2022, 14, 1609. [Google Scholar] [CrossRef] [PubMed]
- Yanni, A.E.; Stamataki, N.; Stoupaki, M.; Konstantopoulos, P.; Pateras, I.; Tentolouris, N.; Perrea, D.T.; Karathanos, V. Cr-Enriched Yeast: Beyond Fibers for the Management of Postprandial Glycemic Response to Bread. Eur. J. Nutr. 2017, 56, 1445–1453. [Google Scholar] [CrossRef]
- Yanni, A.E.; Stamataki, N.S.; Konstantopoulos, P.; Stoupaki, M.; Abeliatis, A.; Nikolakea, I.; Perrea, D.; Karathanos, V.T.; Tentolouris, N. Controlling Type-2 Diabetes by Inclusion of Cr-Enriched Yeast Bread in the Daily Dietary Pattern: A Randomized Clinical Trial. Eur. J. Nutr. 2018, 57, 259–267. [Google Scholar] [CrossRef]
- Su-Que, L.; Ya-Ning, M.; Xing-Pu, L.; Ye-Lun, Z.; Guang-Yao, S.; Hui-Juan, M. Effect of Consumption of Micronutrient Enriched Wheat Steamed Bread on Postprandial Plasma Glucose in Healthy and Type 2 Diabetic Subjects. Nutr. J. 2013, 12, 64. [Google Scholar] [CrossRef]
- Green, T.J.; Liu, Y.; Dadgar, S.; Li, W.; Böhni, R.; Kitts, D.D. Wheat Rolls Fortified with Microencapsulated L-5-Methyltetrahydrofolic Acid or Equimolar Folic Acid Increase Blood Folate Concentrations to a Similar Extent in Healthymen and Women. J. Nutr. 2013, 143, 867–871. [Google Scholar] [CrossRef]
- Itkonen, S.T.; Skaffari, E.; Saaristo, P.; Saarnio, E.M.; Erkkola, M.; Jakobsen, J.; Cashman, K.D.; Lamberg-Allardt, C. Effects of Vitamin D2-Fortified Bread v. Supplementation with Vitamin D2 or D3 on Serum 25-HydroxyVitamin D Metabolites: An 8-Week Randomised-Controlled Trial in Young Adult Finnish Women. Br. J. Nutr. 2016, 115, 1232–1239. [Google Scholar] [CrossRef] [PubMed]
- Nikooyeh, B.; Neyestani, T.R.; Zahedirad, M.; Mohammadi, M.; Hosseini, S.H.; Abdollahi, Z.; Salehi, F.; Razaz, J.M.; Shariatzadeh, N.; Kalayi, A.; et al. Vitamin D-Fortified Bread Is as Effective as Supplement in Improving Vitamin D Status: A Randomized Clinical Trial. J. Clin. Endocrinol. Metab. 2016, 101, 2511–2519. [Google Scholar] [CrossRef] [PubMed]
- Thannoun, A.M.; Al-Arajy, R.F.L. Effect of Addition of L-Ascorbic Acid to Wheat Bread Dough on Blood Glucose Response, Glycemic Index and Glycemic Load in Normal Subject. J. Pharm. Negat. Results 2022, 13, 570–584. [Google Scholar] [CrossRef]
- Amoah, I.; Cairncross, C.; Merien, F.; Rush, E. Glycaemic and Appetite Suppression Effect of a Vegetable-Enriched Bread. Nutrients 2021, 13, 4277. [Google Scholar] [CrossRef] [PubMed]
- Boll, E.V.J.; Ekström, L.M.N.K.; Courtin, C.M.; Delcour, J.A.; Nilsson, A.C.; Björck, I.M.E.; Östman, E.M. Effects of Wheat Bran Extract Rich in Arabinoxylan Oligosaccharides and Resistant Starch on Overnight Glucose Tolerance and Markers of Gut Fermentation in Healthy Young Adults. Eur. J. Nutr. 2016, 55, 1661–1670. [Google Scholar] [CrossRef] [PubMed]
- Stewart, M.L.; Wilcox, M.L.; Bell, M.; Buggia, M.A.; Maki, K.C. Type-4 Resistant Starch in Substitution for Available Carbohydrate Reduces Postprandial Glycemic Response and Hunger in Acute, Randomized, Double-Blind, Controlled Study. Nutrients 2018, 10, 129. [Google Scholar] [CrossRef]
- Giulia Falchi, A.; Grecchi, I.; Muggia, C.; Palladini, G.; Perlini, S. Effects of a Bioavailable Arabinoxylan-Enriched White Bread Flour on Postprandial Glucose Response in Normoglycemic Subjects. J. Diet. Suppl. 2016, 13, 626–633. [Google Scholar] [CrossRef]
- Nouri, M.; Tarighat-Esfanjani, A.; Sadra, V.; Ghasempour, Z.; Jafarabadi, M.A.; Tajfar, P.; Gargari, B.P. Effects of Whey Protein Concentrate on Glycemic Status, Lipid Profile, and Blood Pressure in Overweight/Obese Women with Type 2 Diabetes Mellitus: A Randomized Placebo-Controlled Clinical Trial. Turk. J. Endocrinol. Metab. 2022, 26, 148–155. [Google Scholar] [CrossRef]
- Salari Moghaddam, A.; Hassan Entezari, M.; Iraj, B.; Reza Askari, G.; Reza Maracy, M. The Effects of Consumption of Bread Fortified With Soy Bean Flour on Metabolic Profile in Type 2 Diabetic Women: A Cross-over Randomized Controlled Clinical Trial. Int. J. Prev. Med. 2014, 5, 1529. [Google Scholar]
- Sharifi-Zahabi, E.; Entezari, M.H.; Maracy, M.R. Effects of Soy Flour Fortified Bread Consumption on Cardiovascular Risk Factors According to APOE Genotypes in Overweight and Obese Adult Women: A Cross-over Randomized Controlled Clinical Trial. Clin. Nutr. Res. 2015, 4, 225. [Google Scholar] [CrossRef]
- Apprey, C.; Peprah, M.; Annan, R.A.; Tandoh, M.A.; Asamoah-Boakye, O. Borassus Aethiopum -Fortified Bread Reduces Metabolic Risk Factors among Cardiovascular Disease Outpatients at 37 Military Hospital, Accra: A Pilot Study. Int. J. Food Sci. 2020, 2020, 2379061. [Google Scholar] [CrossRef]
- Fouad, S.; El Shebini, S.M.; Moaty, M.I.A.; Ahmed, N.H.; Tapozada, S.T. Effect of Soya Beans Bread Fortified with Turmeric or Ginger on Diabesity. Der. Pharma. Chem. 2016, 8, 398–405. [Google Scholar]
- Lappi, J.; Aura, A.M.; Katina, K.; Nordlund, E.; Kolehmainen, M.; Mykkänen, H.; Poutanen, K. Comparison of Postprandial Phenolic Acid Excretions and Glucose Responses after Ingestion of Breads with Bioprocessed or Native Rye Bran. Food Funct 2013, 4, 972–981. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, J.J.A.; Wolska, A.; Remaley, A.T.; Stojanovski, E.; MacDonald-Wicks, L.; Garg, M.L. Bread Enriched with Phytosterols with or without Curcumin Modulates Lipoprotein Profiles in Hypercholesterolaemic Individuals. A Randomised Controlled Trial. Food Funct 2019, 10, 2515–2527. [Google Scholar] [CrossRef]
- Coe, S.; Ryan, L. White Bread Enriched with Polyphenol Extracts Shows No Effect on Glycemic Response or Satiety, yet May Increase Postprandial Insulin Economy in Healthy Participants. Nutr. Res. 2016, 36, 193–200. [Google Scholar] [CrossRef]
- Becerra-Tomas, N.; Guasch-Ferre, M.; Quilez, J.; Merino, J.; Ferre, R.; Diaz-López, A.; Bulló, M.; Hernández-Alonso, P.; Palau-Galindo, A.; Salas-Salvadó, J. Effect of Functional Bread Rich in Potassium, g-Aminobutyric Acid and Angiotensin-Converting Enzyme Inhibitors on Blood Pressure, Glucose Metabolism and Endothelial Function a Double-Blind Randomized Crossover Clinical Trial. Medicine 2015, 94, e1807. [Google Scholar] [CrossRef] [PubMed]
- Poole, N.; Donovan, J.; Erenstein, O. Viewpoint: Agri-Nutrition Research: Revisiting the Contribution of Maize and Wheat to Human Nutrition and Health. Food Policy 2021, 100, 101976. [Google Scholar] [CrossRef]
- Teleanu, R.I.; Niculescu, A.G.; Roza, E.; Vladâcenco, O.; Grumezescu, A.M.; Teleanu, D.M. Neurotransmitters—Key Factors in Neurological and Neurodegenerative Disorders of the Central Nervous System. Int. J. Mol. Sci. 2022, 23, 5954. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaim, U.; Goluch, Z.S. Health Benefits of Bread Fortification: A Systematic Review of Clinical Trials according to the PRISMA Statement. Nutrients 2023, 15, 4459. https://doi.org/10.3390/nu15204459
Kaim U, Goluch ZS. Health Benefits of Bread Fortification: A Systematic Review of Clinical Trials according to the PRISMA Statement. Nutrients. 2023; 15(20):4459. https://doi.org/10.3390/nu15204459
Chicago/Turabian StyleKaim, Urszula, and Zuzanna Sabina Goluch. 2023. "Health Benefits of Bread Fortification: A Systematic Review of Clinical Trials according to the PRISMA Statement" Nutrients 15, no. 20: 4459. https://doi.org/10.3390/nu15204459
APA StyleKaim, U., & Goluch, Z. S. (2023). Health Benefits of Bread Fortification: A Systematic Review of Clinical Trials according to the PRISMA Statement. Nutrients, 15(20), 4459. https://doi.org/10.3390/nu15204459