
Association of Plasma Zinc and Copper with Body Composition, Lipids and Inflammation in a Cross-Sectional General Population Sample from Germany
 , , , and
, , , and
Abstract
:1. Introduction
2. Subjects and Methods
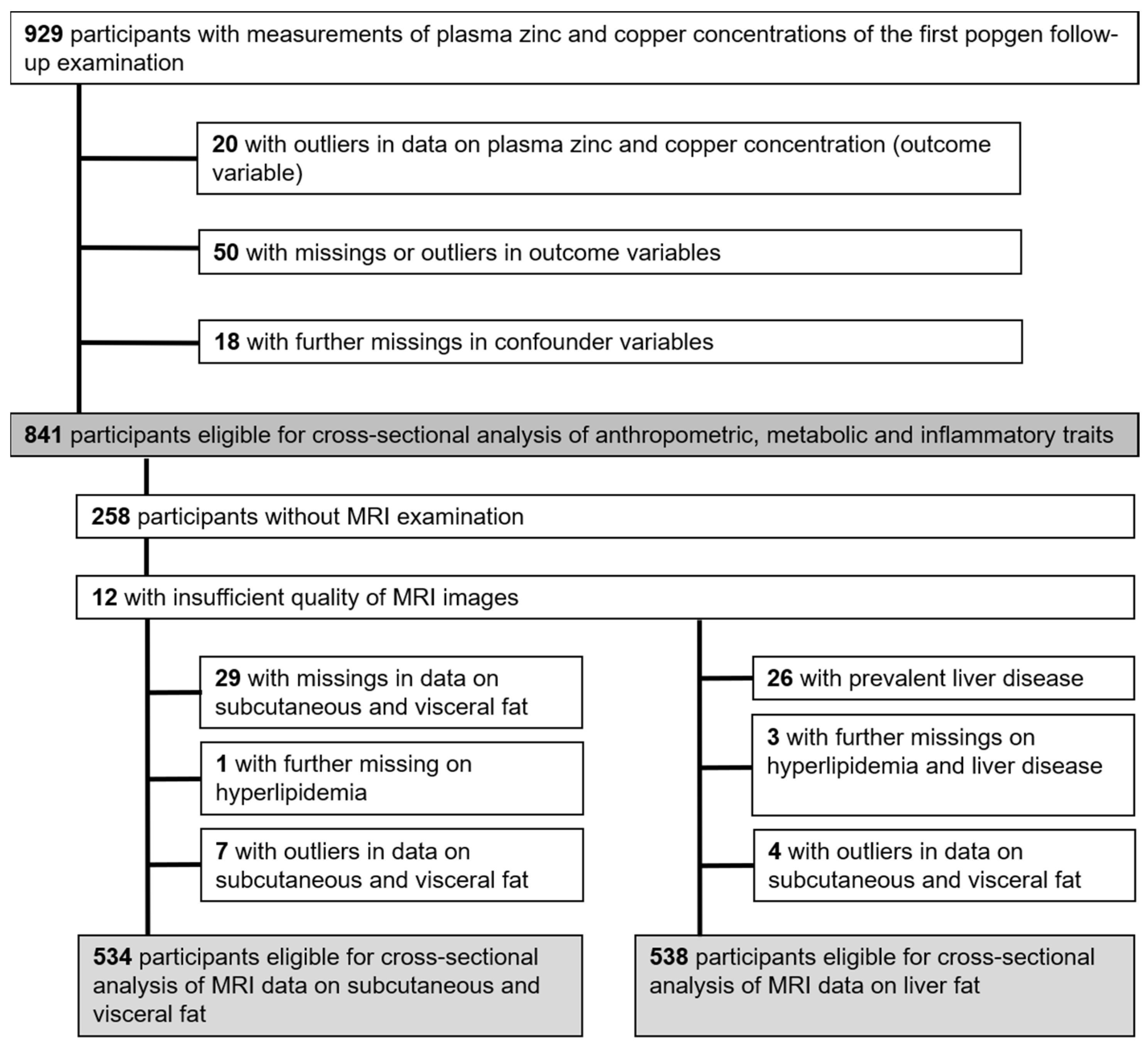
2.1. Study Sample
2.2. Clinical Evaluation and Laboratory Analyses
2.2.1. Assessment of Plasma Zinc and Copper
2.2.2. Assessment of Dietary Intake of Zinc, Total Fat and Saturated Fatty Acids
2.2.3. Assessment of Subcutaneous and Visceral Adipose Tissue and Liver Fat
2.3. Definitions
2.4. Statistical Analyses
2.4.1. Association of Zinc and Copper with Anthropometric, Metabolic and Inflammatory Parameters
2.4.2. Association of Zinc and Copper with MRI Traits of Body Composition
2.4.3. Sensitivity Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Association of Zinc and Copper with Anthropometric, Metabolic and Inflammatory Traits
3.3. Associations of Zinc and Copper with Adipose Tissue and Liver Fat
4. Discussion
4.1. Associations of Zinc and Copper with Anthropometric Traits and MRI Measures of Body Composition
4.2. Association of Zinc and Copper with Blood Lipids
4.3. Diet
4.4. Association of Zinc and Copper with Inflammation
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body mass index |
| CI | Confidence interval |
| CRP | C-reactive protein |
| Cu | Copper |
| DEXA | Dual-energy X-ray absorptiometry |
| FFQ | Food frequency questionnaire |
| HDL | High-density lipoprotein cholesterol |
| LDL | Low-density lipoprotein cholesterol |
| LSI | Liver signal intensity |
| MRI | Magnet resonance imaging |
| NAFLD | Non-alcoholic fatty liver disease |
| NHANES | National Health and Nutrition Examination Survey |
| SAFs | Saturated fatty acids |
| SAT | Subcutaneous adipose tissue |
| TG | Triglycerides |
| SD | Standard deviation |
| VAT | Visceral adipose tissue |
| WC | Waist circumference |
| WHR | Waist-to-hip ratio |
| Zn | Zinc |
References
- Stefanidou, M.; Maravelias, C.; Dona, A.; Spiliopoulou, C. Zinc: A multipurpose trace element. Arch. Toxicol. 2006, 80, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Livingstone, C. Zinc: Physiology, deficiency, and parenteral nutrition. Nutr. Clin. Pract. 2015, 30, 371–382. [Google Scholar] [CrossRef]
- Huang, X.; Jiang, D.; Zhu, Y.; Fang, Z.; Che, L.; Lin, Y.; Xu, S.; Li, J.; Huang, C.; Zou, Y.; et al. Chronic High Dose Zinc Supplementation Induces Visceral Adipose Tissue Hypertrophy without Altering Body Weight in Mice. Nutrients 2017, 9, 1138. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Guan, Y.; Shi, X.; Ding, H.; Song, Y.; Li, C.; Liu, R.; Liu, G. Effects of high zinc levels on the lipid synthesis in rat hepatocytes. Biol. Trace Elem. Res. 2013, 154, 97–102. [Google Scholar] [CrossRef]
- Zhang, H.B.; Wang, M.S.; Wang, Z.S.; Zhou, A.M.; Zhang, X.M.; Dong, X.W.; Peng, Q.H. Supplementation dietary zinc levels on growth performance, carcass traits, and intramuscular fat deposition in weaned piglets. Biol. Trace Elem. Res. 2014, 161, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Andriollo-Sanchez, M.; Hininger-Favier, I.; Meunier, N.; Toti, E.; Zaccaria, M.; Brandolini-Bunlon, M.; Polito, A.; O’Connor, J.M.; Ferry, M.; Coudray, C.; et al. Zinc intake and status in middle-aged and older European subjects: The ZENITH study. Eur. J. Clin. Nutr. 2005, 59 (Suppl. S2), S37–S41. [Google Scholar] [CrossRef] [PubMed]
- Danks, D.M. Copper deficiency in humans. Annu. Rev. Nutr. 1988, 8, 235–257. [Google Scholar] [CrossRef]
- Myint, Z.W.; Oo, T.H.; Thein, K.Z.; Tun, A.M.; Saeed, H. Copper deficiency anemia: Review article. Ann. Hematol. 2018, 97, 1527–1534. [Google Scholar] [CrossRef]
- Chen, C.; Zhou, Q.; Yang, R.; Wu, Z.; Yuan, H.; Zhang, N.; Zhi, M.; Zhang, Y.; Ni, X.; Wang, Z.; et al. Copper exposure association with prevalence of non-alcoholic fatty liver disease and insulin resistance among US adults (NHANES 2011–2014). Ecotoxicol. Environ. Saf. 2021, 218, 112295. [Google Scholar] [CrossRef]
- Cousins, R.J.; Ayaz, M.; Turan, B.; Grosell, M.; McGeer, J.C.; Wood, C.M.; Miller, L.V.; Krebs, N.F.; Hambidge, K.M.; Cappelli-Bigazzi, M.; et al. Absorption, transport, and hepatic metabolism of copper and zinc: Special reference to metallothionein and ceruloplasmin. Physiol. Rev. 1985, 65, 238–309. [Google Scholar] [CrossRef]
- Kim, H.-N.; Song, S.-W.; Choi, W.-S. Association between serum zinc level and body composition: The Korean National Health and Nutrition Examination Survey. Nutrition 2016, 32, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Li, Q.; Zhang, K.; Zhao, J. The association between serum copper and obesity and all-cause mortality: The NHANES 2011–2016. Environ. Sci. Pollut. Res. 2023, 30, 31395–31407. [Google Scholar] [CrossRef]
- Liang, J.; Chen, F.; Fang, G.; Zhang, X.; Li, Y.; Ma, B.; Lin, S.; Pan, J.; Zhang, Z. Relationship Between Plasma Copper Concentration and Body Fat Distribution in Children in China: A Cross-Sectional Study. Biol. Trace Elem. Res. 2020, 198, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Mendoza, H.; Martínez-Navarro, I.; Hernández-Ochoa, E.; Espinoza-Ruiz, M.; Lugo-Trampe, A.; Trujillo-Murillo, K.d.C.; López-García, M.A.; Rios-Lugo, M.J.; Chang-Rueda, C. Serum zinc levels are associated with obesity and low-density lipoprotein cholesterol in Mexican adults. J. Trace Elem. Med. Biol. 2022, 73, 127002. [Google Scholar] [CrossRef]
- Jaksic, M.; Martinovic, M.; Gligorovic-Barhanovic, N.; Vujacic, A.; Djurovic, D.; Nedovic-Vukovic, M. Association between inflammation, oxidative stress, vitamin D, copper and zinc with pre-obesity and obesity in school children from the city of Podgorica, Montenegro. J. Pediatr. Endocrinol. Metab. 2019, 32, 951–957. [Google Scholar] [CrossRef]
- Müller, M.J.; Braun, W.; Pourhassan, M.; Geisler, C.; Bosy-Westphal, A. Application of standards and models in body composition analysis. Proc. Nutr. Soc. 2016, 75, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Nöthlings, U.; Krawczak, M. PopGen. Eine populationsbasierte Biobank mit Langzeitverfolgung der Kontrollkohorte. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2012, 55, 831–835. [Google Scholar] [CrossRef]
- Waniek, S.; Di Giuseppe, R.; Esatbeyoglu, T.; Plachta-Danielzik, S.; Ratjen, I.; Jacobs, G.; Nöthlings, U.; Koch, M.; Schlesinger, S.; Rimbach, G.; et al. Vitamin E (α- and γ-Tocopherol) Levels in the Community: Distribution, Clinical and Biochemical Correlates, and Association with Dietary Patterns. Nutrients 2017, 10, 3. [Google Scholar] [CrossRef]
- Barbaresko, J.; Siegert, S.; Koch, M.; Aits, I.; Lieb, W.; Nikolaus, S.; Laudes, M.; Jacobs, G.; Nöthlings, U. Comparison of two exploratory dietary patterns in association with the metabolic syndrome in a Northern German population. Br. J. Nutr. 2014, 112, 1364–1372. [Google Scholar] [CrossRef]
- Koch, M.; Borggrefe, J.; Barbaresko, J.; Groth, G.; Jacobs, G.; Siegert, S.; Lieb, W.; Müller, M.J.; Bosy-Westphal, A.; Heller, M.; et al. Dietary patterns associated with magnetic resonance imaging–determined liver fat content in a general population study. Am. J. Clin. Nutr. 2014, 99, 369–377. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef]
- DIN EN ISO 17294-2: 2017-01; Water quality—Application of Inductively Coupled Plasma Mass Spectrometry (ICP-MS)—Part 2: Determination of Selected Elements Including Uranium Isotopes (ISO 17294-2:2016). ISO: Geneva, Switzerland, 2017.
- Weber, K.S.; Ratjen, I.; Enderle, J.; Seidel, U.; Rimbach, G.; Lieb, W. Plasma boron concentrations in the general population: A cross-sectional analysis of cardio-metabolic and dietary correlates. Eur. J. Nutr. 2022, 61, 1363–1375. [Google Scholar] [CrossRef] [PubMed]
- Nöthlings, U.; Hoffmann, K.; Bergmann, M.M.; Boeing, H. Fitting portion sizes in a self-administered food frequency questionnaire. J. Nutr. 2007, 137, 2781–2786. [Google Scholar] [CrossRef] [PubMed]
- Dehne, L.I.; Klemm, C.; Henseler, G.; Hermann-Kunz, E. The German Food Code and Nutrient Data Base (BLS II.2). Eur. J. Epidemiol. 1999, 15, 355–358. [Google Scholar] [CrossRef] [PubMed]
- Waniek, S.; Di Giuseppe, R.; Plachta-Danielzik, S.; Ratjen, I.; Jacobs, G.; Koch, M.; Borggrefe, J.; Both, M.; Müller, H.-P.; Kassubek, J.; et al. Association of Vitamin E Levels with Metabolic Syndrome, and MRI-Derived Body Fat Volumes and Liver Fat Content. Nutrients 2017, 9, 1143. [Google Scholar] [CrossRef]
- Fischer, K.; Moewes, D.; Koch, M.; Müller, H.-P.; Jacobs, G.; Kassubek, J.; Lieb, W.; Nöthlings, U. MRI-determined total volumes of visceral and subcutaneous abdominal and trunk adipose tissue are differentially and sex-dependently associated with patterns of estimated usual nutrient intake in a northern German population. Am. J. Clin. Nutr. 2015, 101, 794–807. [Google Scholar] [CrossRef]
- Müller, H.-P.; Raudies, F.; Unrath, A.; Neumann, H.; Ludolph, A.C.; Kassubek, J. Quantification of human body fat tissue percentage by MRI. NMR Biomed. 2011, 24, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Heil, W.; Ehrhardt, V. Referenzbereiche für Kinder und Erwachsene: Präanalytik; Boehringer: Mannheim, Germany, 2007. [Google Scholar]
- Jiang, S.; Ma, X.; Li, M.; Yan, S.; Zhao, H.; Pan, Y.; Wang, C.; Yao, Y.; Jin, L.; Li, B. Association between dietary mineral nutrient intake, body mass index, and waist circumference in U.S. adults using quantile regression analysis NHANES 2007–2014. PeerJ 2020, 8, e9127. [Google Scholar] [CrossRef]
- Gu, K.; Xiang, W.; Zhang, Y.; Sun, K.; Jiang, X. The association between serum zinc level and overweight/obesity: A meta-analysis. Eur. J. Nutr. 2019, 58, 2971–2982. [Google Scholar] [CrossRef]
- Tungtrongchitr, R.; Pongpaew, P.; Phonrat, B.; Tungtrongchitr, A.; Viroonudomphol, D.; Vudhivai, N.; Schelp, F.P. Serum copper, zinc, ceruloplasmin and superoxide dismutase in Thai overweight and obese. J. Med. Assoc. Thai 2003, 86, 543–551. [Google Scholar]
- Kerkadi, A.; Alkudsi, D.S.; Hamad, S.; Alkeldi, H.M.; Salih, R.; Agouni, A. The Association between Zinc and Copper Circulating Levels and Cardiometabolic Risk Factors in Adults: A Study of Qatar Biobank Data. Nutrients 2021, 13, 2729. [Google Scholar] [CrossRef]
- Gu, K.; Li, X.; Xiang, W.; Jiang, X. The Relationship Between Serum Copper and Overweight/Obesity: A Meta-analysis. Biol. Trace Elem. Res. 2020, 194, 336–347. [Google Scholar] [CrossRef] [PubMed]
- Fukasawa, H.; Niwa, H.; Ishibuchi, K.; Kaneko, M.; Iwakura, T.; Yasuda, H.; Furuya, R. The Impact of Serum Zinc Levels on Abdominal Fat Mass in Hemodialysis Patients. Nutrients 2020, 12, 656. [Google Scholar] [CrossRef] [PubMed]
- García, O.P.; Ronquillo, D.; Caamaño, M.d.C.; Camacho, M.; Long, K.Z.; Rosado, J.L. Zinc, vitamin A, and vitamin C status are associated with leptin concentrations and obesity in Mexican women: Results from a cross-sectional study. Nutr. Metab. 2012, 9, 59. [Google Scholar] [CrossRef]
- Ghosh, C.; Yang, S.H.; Kim, J.G.; Jeon, T.-I.; Yoon, B.H.; Lee, J.Y.; Lee, E.Y.; Choi, S.G.; Hwang, S.G. Zinc-chelated Vitamin C Stimulates Adipogenesis of 3T3-L1 Cells. Asian-Australas. J. Anim. Sci. 2013, 26, 1189–1196. [Google Scholar] [CrossRef]
- Chen, M.-D.; Lin, P.-Y.; Cheng, V.; Lin, W.-H. Zinc supplementation aggravates body fat accumulation in genetically obese mice and dietary-obese mice. Biol. Trace Elem. Res. 1996, 52, 125–132. [Google Scholar] [CrossRef]
- Santoro, A.; McGraw, T.E.; Kahn, B.B. Insulin action in adipocytes, adipose remodeling, and systemic effects. Cell Metab. 2021, 33, 748–757. [Google Scholar] [CrossRef]
- Smidt, K.; Pedersen, S.B.; Brock, B.; Schmitz, O.; Fisker, S.; Bendix, J.; Wogensen, L.; Rungby, J. Zinc-transporter genes in human visceral and subcutaneous adipocytes: Lean versus obese. Mol. Cell. Endocrinol. 2007, 264, 68–73. [Google Scholar] [CrossRef]
- Yazihan, N.; Akdas, S. Serum zinc level and dietary zinc intake status in non-alcoholic fatty liver disease: A meta-analysis and systematic review. Hepatol. Forum 2020, 1, 59–67. [Google Scholar] [CrossRef]
- Antonucci, L.; Porcu, C.; Iannucci, G.; Balsano, C.; Barbaro, B. Non-Alcoholic Fatty Liver Disease and Nutritional Implications: Special Focus on Copper. Nutrients 2017, 9, 1137. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Jia, X.-F.; Zhang, B.; Wang, Z.-H.; Zhang, J.-G.; Huang, F.-F.; Su, C.; Ouyang, Y.-F.; Zhao, J.; Du, W.-W.; et al. Dietary Zinc Intake and Its Association with Metabolic Syndrome Indicators among Chinese Adults: An Analysis of the China Nutritional Transition Cohort Survey 2015. Nutrients 2018, 10, 572. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.-H.; Choi, M.-K. Seven dietary minerals (Ca, P, Mg, Fe, Zn, Cu, and Mn) and their relationship with blood pressure and blood lipids in healthy adults with self-selected diet. Biol. Trace Elem. Res. 2013, 153, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Neggers, Y.H.; Bindon, J.R.; Dressler, W.W. The relationship between zinc and copper status and lipid levels in African-Americans. Biol. Trace Elem. Res. 2001, 79, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Xie, Y.; Zhou, Y.; Wang, D.; Cao, L.; Zhou, M.; Wang, X.; Wang, B.; Chen, W. Urinary copper, systemic inflammation, and blood lipid profiles: Wuhan-Zhuhai cohort study. Environ. Pollut. 2020, 267, 115647. [Google Scholar] [CrossRef] [PubMed]
- Tiber, A.M.; Sakhaii, M.; Joffe, C.D.; Ratnaparkhi, M.V. Relative value of plasma copper, zinc, lipids and lipoproteins as markers for coronary artery disease. Atherosclerosis 1986, 62, 105–110. [Google Scholar] [CrossRef]
- Hininger-Favier, I.; Andriollo-Sanchez, M.; Arnaud, J.; Meunier, N.; Bord, S.; Graham, C.; Polito, A.; Maiani, G.; O’Connor, J.M.; Coudray, C.; et al. Age- and sex-dependent effects of long-term zinc supplementation on essential trace element status and lipid metabolism in European subjects: The Zenith Study. Br. J. Nutr. 2007, 97, 569–578. [Google Scholar] [CrossRef]
- Nazem, M.R.; Asadi, M.; Jabbari, N.; Allameh, A. Effects of zinc supplementation on superoxide dismutase activity and gene expression, and metabolic parameters in overweight type 2 diabetes patients: A randomized, double-blind, controlled trial. Clin. Biochem. 2019, 69, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Ranasinghe, P.; Wathurapatha, W.S.; Galappatthy, P.; Katulanda, P.; Jayawardena, R.; Constantine, G.R. Zinc supplementation in prediabetes: A randomized double-blind placebo-controlled clinical trial. J. Diabetes 2018, 10, 386–397. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Wang, N.; Pan, D.; Zhang, H.; Sun, G. Effects of Copper Supplementation on Blood Lipid Level: A Systematic Review and a Meta-Analysis on Randomized Clinical Trials. Biol. Trace Elem. Res. 2021, 199, 2851–2857. [Google Scholar] [CrossRef]
- Deutsche Gesellschaft für Ernährung. Referenzwerte für die Nährstoffzufuhr, 2nd ed.; Deutsche Gesellschaft für Ernährung: Bonn, Germany, 2015. [Google Scholar]
- Biesalski, H.-K. (Ed.) Ernährungsmedizin: Nach dem Curriculum Ernährungsmedizin der Bundesärztekammer, 281 Tabellen, 2nd ed.; Thieme: Stuttgart, Germany, 1999. [Google Scholar]
- Bawadi, H.; Akasheh, R.T.; Kerkadi, A.; Haydar, S.; Tayyem, R.; Shi, Z. Validity and Reproducibility of a Food Frequency Questionnaire to Assess Macro and Micro-Nutrient Intake among a Convenience Cohort of Healthy Adult Qataris. Nutrients 2021, 13, 2002. [Google Scholar] [CrossRef]
- Saravia, L.; Miguel-Berges, M.L.; Iglesia, I.; Nascimento-Ferreira, M.V.; Perdomo, G.; Bove, I.; Slater, B.; Moreno, L.A. Relative validity of FFQ to assess food items, energy, macronutrient and micronutrient intake in children and adolescents: A systematic review with meta-analysis. Br. J. Nutr. 2020, 125, 792–818. [Google Scholar] [CrossRef] [PubMed]
- Milanino, R.; Marrella, M.; Gasperini, R.; Pasqualicchio, M.; Velo, G. Copper and zinc body levels in inflammation: An overview of the data obtained from animal and human studies. Agents Actions 1993, 39, 195–209. [Google Scholar] [CrossRef] [PubMed]
- Malavolta, M.; Piacenza, F.; Basso, A.; Giacconi, R.; Costarelli, L.; Mocchegiani, E. Serum copper to zinc ratio: Relationship with aging and health status. Mech. Ageing Dev. 2015, 151, 93–100. [Google Scholar] [CrossRef]
- Chasapis, C.T.; Ntoupa, P.-S.A.; Spiliopoulou, C.A.; Stefanidou, M.E. Recent aspects of the effects of zinc on human health. Arch. Toxicol. 2020, 94, 1443–1460. [Google Scholar] [CrossRef]
- Cousins, R.J.; Leinart, A.S. Tissue-specific regulation of zinc metabolism and metallothionein genes by interleukin 1. FASEB J. 1988, 2, 2884–2890. [Google Scholar] [CrossRef]
- Lowe, N.M.; Fekete, K.; Decsi, T. Methods of assessment of zinc status in humans: A systematic review. Am. J. Clin. Nutr. 2009, 89, 2040S–2051S. [Google Scholar] [CrossRef] [PubMed]
- Harvey, L.J.; Ashton, K.; Hooper, L.; Casgrain, A.; Fairweather-Tait, S.J. Methods of assessment of copper status in humans: A systematic review. Am. J. Clin. Nutr. 2009, 89, 2009S–2024S. [Google Scholar] [CrossRef]
- Ouchi, N.; Parker, J.L.; Lugus, J.J.; Walsh, K. Adipokines in inflammation and metabolic disease. Nat. Rev. Immunol. 2011, 11, 85–97. [Google Scholar] [CrossRef]


{kind=link}
| Total | T1 | T2 | T3 | p Values d | |
|---|---|---|---|---|---|
| 434.9–958.7 µg/L | 434.9–658.2 µg/L | 658.3–724.9 µg/L | 725.0–958.7 µg/L | ||
| n (% female) a | 841 (42) | 280 (41) | 281 (44) | 280 (40) | 0.501 |
| Age (years) b | 61 ± 12 | 60 ± 13 | 62 ± 12 | 61 ± 12 | 0.103 |
| Plasma zinc (µg/L) b | 695.0 ± 83.1 | 607.7 ± 40.7 | 690.9 ± 18.9 | 786.3 ± 52.4 | <0.001 |
| Plasma copper (µg/L) b | 1037.9 ± 192.5 | 1035.9 ± 197.1 | 1043.9 ± 183.5 | 1034.0 ± 197.2 | 0.813 |
| Zinc intake (mg/day) c | 11.1 (9.4; 13.2) | 11.2 (9.3; 13.4) | 11.1 (9.7; 13.0) | 11.0 (9.3; 13.2) | 0.865 |
| Intake of zinc supplements (yes, (%)) a | 57 (7) | 15 (5) | 20 (7) | 22 (8) | 0.481 |
| Copper intake (mg/day) c | 2.5 (2.1; 2.9) | 2.5 (2.1; 3.0) | 2.4 (2.1; 2.9) | 2.4 (2.1; 2.8) | 0.370 |
| Intake of total fat (g/day) c | 94.1 (78.5; 115.9) | 95.6 (77.7; 119.7) | 94.1 (78.2; 112.8) | 93.2 (79.1; 112.5) | 0.783 |
| Intake of saturated fatty acids (g/day) c | 38.0 (30.8; 46.9) | 38.4 (29.8; 48.7) | 38.1 (31.6; 45.5) | 37.6 (30.6; 46.4) | 0.838 |
| Subcutaneous adipose tissue (dm3) (n = 534) c | 6.0 (4.7; 8.2) | 5.9 (4.8; 8.1) | 6.1 (4.5; 8.3) | 6.1 (4.8; 8.2) | 0.732 |
| Visceral adipose tissue (dm3) (n = 538) c | 3.8 (2.4; 5.2) | 3.5 (2.2; 5.1) | 3.8 (2.5; 5.0) | 4.1 (2.7; 5.2) | 0.179 |
| Liver signal intensity c | 18.5 (14.9; 23.5) | 17.5 (14.5; 22.1) | 19.0 (14.9; 23.8) | 18.8 (15.3; 24.4) | 0.067 |
| Body mass index (kg/m2) b | 27.2 ± 4.2 | 27.0 ± 4.3 | 27.3 ± 4.2 | 27.4 ± 4.2 | 0.484 |
| Waist circumference (cm) b | |||||
| Females | 90.3 ± 12.8 | 88.5 ± 12.4 | 91.5 ± 12.8 | 90.8 ± 13.2 | 0.172 |
| Males | 100.4 ± 10.8 | 100.6 ± 11.0 | 100.3 ± 10.9 | 100.4 ± 10.7 | 0.998 |
| Waist-to-hip ratio b | |||||
| Females | 0.87 ± 0.07 | 0.86 ± 0.07 | 0.88 ± 0.06 | 0.88 ± 0.07 | 0.151 |
| Males | 0.98 ± 0.06 | 0.98 ± 0.06 | 0.99 ± 0.06 | 0.98 ± 0.07 | 0.661 |
| Plasma triglyceride concentration (mg/dL) c | 105.0 (76.0; 138.0) | 101.5 (77.5; 134.5) | 103.0 (76.0; 131.0) | 110.0 (73.0; 149.5) | 0.301 |
| Plasma high-density lipoprotein cholesterol (mg/dL) b | 65.1 ± 17.2 | 66.2 ± 17.7 | 64.2 ± 17.2 | 64.8 ± 16.8 | 0.397 |
| Plasma low-density lipoprotein cholesterol (mg/dL) b | 131.6 ± 33.0 | 125.6 ± 34.2 | 133.8 ± 30.7 | 135.6 ± 33.4 | <0.001 |
| Lipid-lowering medication (yes, (%)) a | 114 (14) | 30 (11) | 36 (13) | 48 (17) | 0.077 |
| C-reactive protein (mg/L) c | 1.2 (0.5; 2.4) | 1.3 (0.5; 2.8) | 1.2 (0.5; 2.4) | 1.1 (0.5; 2.1) | 0.203 |
| Current smokers (yes, (%)) a | 108 (13) | 44 (16) | 32 (11) | 32 (11) | 0.263 |
| Alcohol intake (g/day) c | 9.0 (3.2; 18.5) | 10.7 (3.9; 21.9) | 8.5 (3.0; 17.6) | 8.4 (2.8; 16.4) | 0.022 |
| Physical activity (MET-hours/week) c | 90.5 (59.0; 131.5) | 90.5 (59.7; 132.3) | 88.3 (56.9; 126.3) | 93.8 (59.1; 135.6) | 0.694 |
| Education level (low [<10 years], medium [10 years], high [≥11 years]) a | 292 (35); 271 (32); 278 (33) | 87 (31); 93 (33); 100 (36) | 106 (38); 90 (32); 85 (30) | 99 (35); 88 (31); 93 (33) | 0.517 |
| Anthropometric, Metabolic and Inflammatory Outcome Variables | Zinc | Copper | ||
|---|---|---|---|---|
| Estimates (95% CI) a | p Values | Estimates (95% CI) a | p Values | |
| Body mass index (kg/m2) | ||||
| Model A1 | 1.35 (0.30; 2.40) | 0.011 | 0.38 (−0.66; 1.42) | 0.475 |
| Model A2 | 1.19 (0.16; 2.23) | 0.024 | 1.60 (0.38; 2.84) | 0.010 |
| Model A3 | 1.18 (0.17; 2.21) | 0.023 | 1.65 (0.43; 2.89) | 0.008 |
| Model A4 | 1.17 (0.15; 2.20) | 0.024 | 1.64 (0.41; 2.88) | 0.009 |
| Waist circumference (cm) | ||||
| Model A1 | 1.15 (0.23; 2.07) | 0.014 | −1.79 (−2.67; −0.89) | <0.001 |
| Model A2 | 0.83 (0.02; 1.65) | 0.046 | 1.26 (0.30; 2.24) | 0.011 |
| Model A3 | 0.84 (0.03; 1.66) | 0.041 | 1.20 (0.23; 2.18) | 0.015 |
| Model A4 | 0.85 (0.04; 1.67) | 0.040 | 1.22 (0.25; 2.20) | 0.014 |
| Waist-to-hip ratio | ||||
| Model A1 | 0.88 (0.25; 1.51) | 0.006 | −2.45 (−3.03; −1.85) | <0.001 |
| Model A2 | 0.58 (0.12; 1.04) | 0.014 | 0.67 (0.13; 1.22) | 0.016 |
| Model A3 | 0.63 (0.18; 1.09) | 0.007 | 0.47 (−0.07; 1.02) | 0.090 |
| Model A4 | 0.64 (0.18; 1.09) | 0.006 | 0.48 (−0.06; 1.03) | 0.084 |
| Plasma triglyceride concentration (mg/dL) | ||||
| Model A1 | 2.79 (−0.33; 6.00) | 0.080 | −0.89 (−3.90; 2.21) | 0.569 |
| Model A2 | 2.16 (−0.87; 5.29) | 0.164 | 2.24 (−1.34; 5.97) | 0.223 |
| Model A3 | 1.58 (−1.33; 4.57) | 0.290 | −0.08 (−3.41; 3.36) | 0.963 |
| Model A4 | 1.52 (−1.39; 4.51) | 0.310 | −0.18 (−3.51; 3.26) | 0.917 |
| Plasma HDL concentration (mg/dL) | ||||
| Model A1 | −1.58 (−3.33; 0.20) | 0.082 | 7.49 (5.64; 9.37) | <0.001 |
| Model A2 | −1.26 (−2.85; 0.35) | 0.124 | 1.40 (−0.53; 3.37) | 0.156 |
| Model A3 | −0.50 (−1.99; 1.02) | 0.517 | 2.85 (1.06; 4.67) | 0.002 |
| Model A4 | −0.50 (−1.99; 1.03) | 0.520 | 2.87 (1.07; 4.69) | 0.002 |
| Plasma LDL concentration (mg/dL) | ||||
| Model A1 | 3.32 (1.48; 5.18) | <0.001 | 3.17 (1.33; 5.03) | <0.001 |
| Model A2 | 3.16 (1.34; 5.02) | <0.001 | 3.62 (1.46; 5.84) | 0.001 |
| Model A3 | 3.77 (1.99; 5.59) | <0.001 | 2.73 (0.66; 4.84) | 0.010 |
| Model A4 | 3.75 (1.97; 5.57) | <0.001 | 2.70 (0.63; 4.81) | 0.010 |
| C-reactive protein (mg/L) | ||||
| Model A1 | −6.12 (−12.05; 0.20) | 0.058 | 38.98 (30.70; 47.78) | <0.001 |
| Model A2 | −6.59 (−12.42; −0.36) | 0.039 | 47.09 (36.86; 58.08) | <0.001 |
| Model A3 | −7.75 (−13.02; −2.17) | 0.007 | 37.34 (28.41; 46.90) | <0.001 |
| Model A4 | −7.81 (−13.08; −2.22) | 0.007 | 37.33 (28.38; 46.91) | <0.001 |
| MRI Traits as Outcome Variables | Zinc | Copper | ||
|---|---|---|---|---|
| Estimates (95% CI) a | p Values | Estimates (95% CI) a | p Values | |
| Subcutaneous adipose tissue (dm3) | ||||
| Model B1 | 3.17 (−0.54; 7.03) | 0.095 | 9.89 (6.02; 13.91) | <0.001 |
| Model B2 | 3.77 (0.18; 7.48) | 0.039 | 3.65 (−0.63; 8.11) | 0.096 |
| Model B3 | 3.60 (0.01; 7.31) | 0.049 | 4.77 (0.44; 9.29) | 0.031 |
| Model B4 | 3.38 (−0.21; 7.10) | 0.065 | 4.64 (0.31; 9.15) | 0.036 |
| Model B5 | −0.37 (−2.22; 1.51) | 0.697 | 0.46 (−1.77; 2.74) | 0.688 |
| Visceral adipose tissue (dm3) | ||||
| Model B1 | 7.60 (3.01; 12.40) | 0.001 | −12.07 (−15.74; −8.23) | <0.001 |
| Model B2 | 5.78 (2.02; 9.68) | 0.002 | 2.31 (−2.06; 6.88) | 0.305 |
| Model B3 | 5.69 (2.02; 9.50) | 0.002 | 3.56 (−0.78; 8.08) | 0.109 |
| Model B4 | 5.73 (2.04; 9.56) | 0.002 | 3.57 (−0.78; 8.10) | 0.109 |
| Model B5 | 2.40 (−0.07; 4.93) | 0.057 | −0.06 (−2.96; 2.91) | 0.966 |
| Liver signal intensity | ||||
| Model B1 | 6.32 (2.73; 10.04) | <0.001 | −2.17 (−5.50; 1.29) | 0.216 |
| Model B2 | 5.83 (2.32; 9.45) | 0.001 | −3.70 (−7.53; 0.29) | 0.069 |
| Model B3 | 3.92 (1.57; 6.32) | 0.001 | −1.48 (−4.16; 1.29) | 0.291 |
| Model B4 | 3.84 (1.49; 6.25) | 0.001 | −1.49 (−4.18; 1.27) | 0.287 |
| Model B5 | 3.20 (0.90; 5.54) | 0.006 | −2.11 (−4.72; 0.56) | 0.121 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Övermöhle, C.; Rimbach, G.; Waniek, S.; Strathmann, E.A.; Liedtke, T.; Stürmer, P.; Both, M.; Weber, K.S.; Lieb, W. Association of Plasma Zinc and Copper with Body Composition, Lipids and Inflammation in a Cross-Sectional General Population Sample from Germany. Nutrients 2023, 15, 4460. https://doi.org/10.3390/nu15204460
Övermöhle C, Rimbach G, Waniek S, Strathmann EA, Liedtke T, Stürmer P, Both M, Weber KS, Lieb W. Association of Plasma Zinc and Copper with Body Composition, Lipids and Inflammation in a Cross-Sectional General Population Sample from Germany. Nutrients. 2023; 15(20):4460. https://doi.org/10.3390/nu15204460
Chicago/Turabian StyleÖvermöhle, Cara, Gerald Rimbach, Sabina Waniek, Eike A. Strathmann, Tatjana Liedtke, Paula Stürmer, Marcus Both, Katharina S. Weber, and Wolfgang Lieb. 2023. "Association of Plasma Zinc and Copper with Body Composition, Lipids and Inflammation in a Cross-Sectional General Population Sample from Germany" Nutrients 15, no. 20: 4460. https://doi.org/10.3390/nu15204460
APA StyleÖvermöhle, C., Rimbach, G., Waniek, S., Strathmann, E. A., Liedtke, T., Stürmer, P., Both, M., Weber, K. S., & Lieb, W. (2023). Association of Plasma Zinc and Copper with Body Composition, Lipids and Inflammation in a Cross-Sectional General Population Sample from Germany. Nutrients, 15(20), 4460. https://doi.org/10.3390/nu15204460