
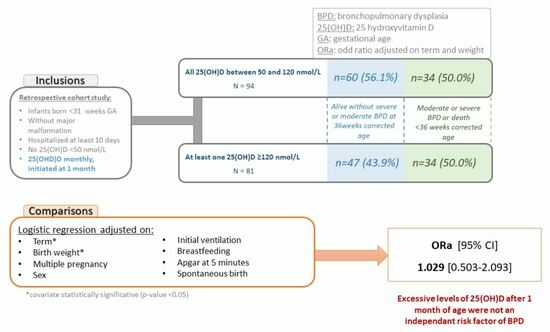
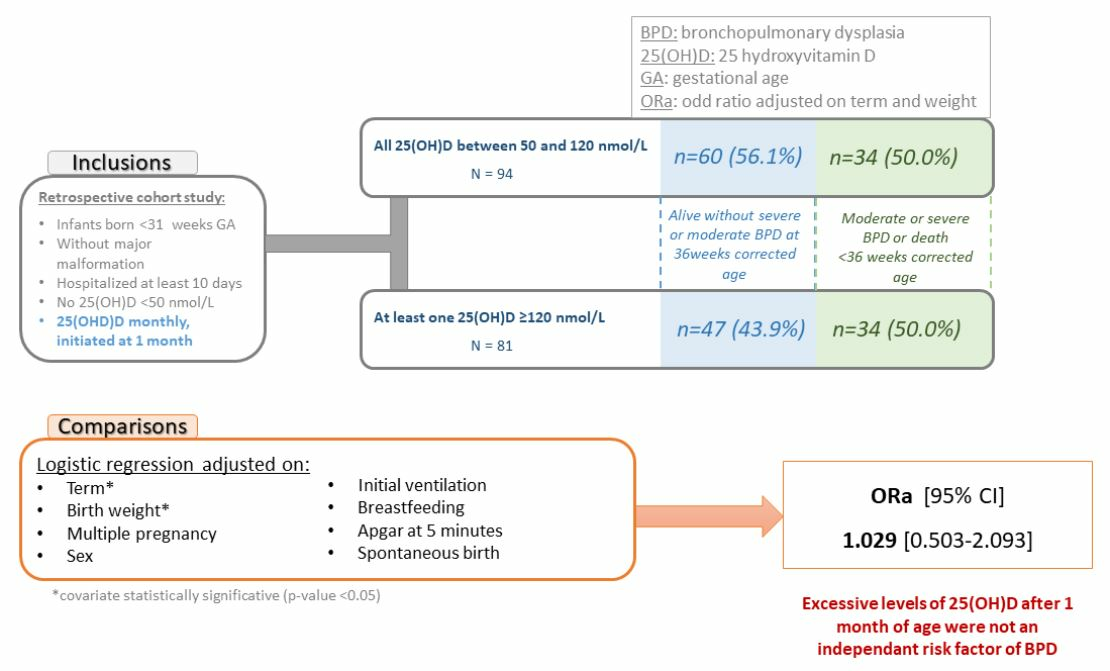
Is 25OH Vitamin D Excess before 36 Weeks Corrected Age an Independent Risk Factor for Bronchopulmonary Dysplasia or Death?

 , , and
, , and
Abstract
1. Introduction
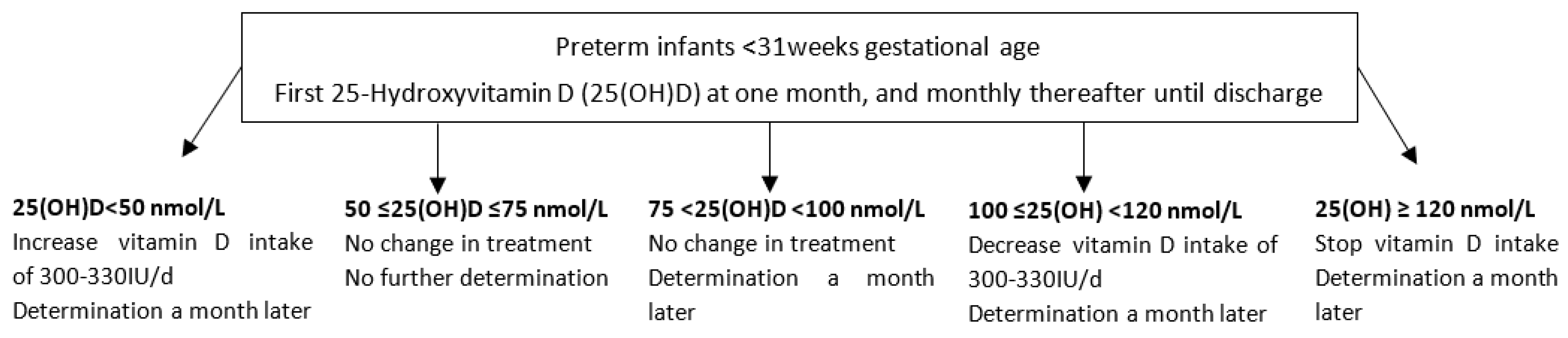
2. Materials and Methods
3. Results
3.1. Population
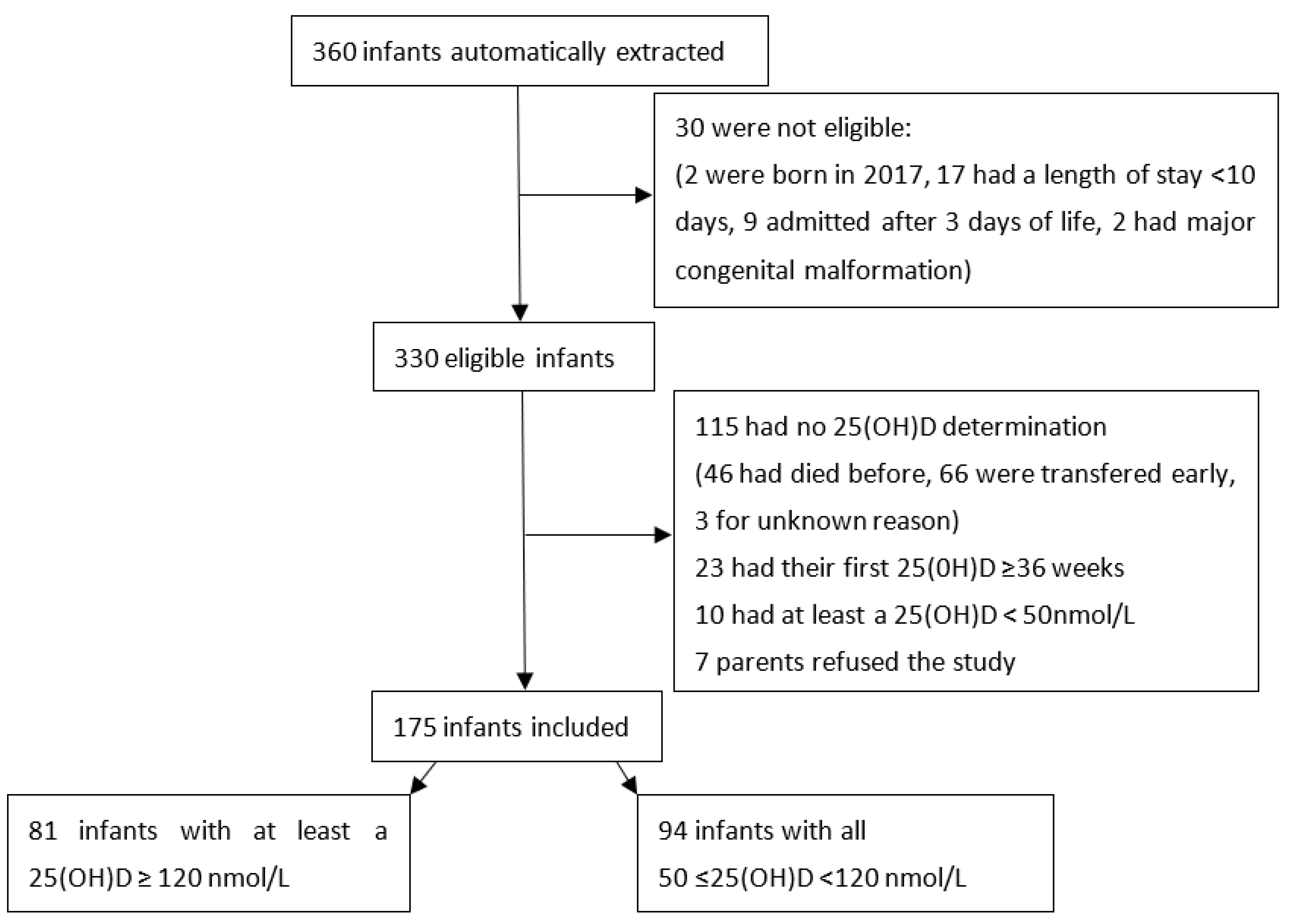
3.1.1. Study Flow-Chart
3.1.2. Description of the Population
3.2. Outcomes
3.3. Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cheong, J.L.Y.; Doyle, L.W. An Update on Pulmonary and Neurodevelopmental Outcomes of Bronchopulmonary Dysplasia. Semin. Perinatol. 2018, 42, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Lykkedegn, S.; Sorensen, G.L.; Beck-Nielsen, S.S.; Christesen, H.T. The Impact of Vitamin D on Fetal and Neonatal Lung Maturation. A Systematic Review. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2015, 308, L587–L602. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Jiang, L. Role of Vitamin D–Vitamin D Receptor Signaling on Hyperoxia-induced Bronchopulmonary Dysplasia in Neonatal Rats. Pediatr. Pulmonol. 2021, 56, 2335–2344. [Google Scholar] [CrossRef] [PubMed]
- Park, H.W.; Lim, G.; Park, Y.-M.; Chang, M.; Son, J.S.; Lee, R. Association between Vitamin D Level and Bronchopulmonary Dysplasia: A Systematic Review and Meta-Analysis. PLoS ONE 2020, 15, e0235332. [Google Scholar] [CrossRef] [PubMed]
- Byun, S.Y.; Bae, M.H.; Lee, N.R.; Han, Y.M.; Park, K.H. Association between Vitamin D Deficiency at One Month of Age and Bronchopulmonary Dysplasia. Medicine 2021, 100, e27966. [Google Scholar] [CrossRef]
- Yu, H.; Fu, J.; Feng, Y. Utility of Umbilical Cord Blood 25-Hydroxyvitamin D Levels for Predicting Bronchopulmonary Dysplasia in Preterm Infants with Very Low and Extremely Low Birth Weight. Front. Pediatr. 2022, 10, 956952. [Google Scholar] [CrossRef]
- Yang, Y.; Li, Z.; Yan, G.; Jie, Q.; Rui, C. Effect of Different Doses of Vitamin D Supplementation on Preterm Infants—An Updated Meta-Analysis. J. Matern. Fetal Neonatal Med. 2018, 31, 3065–3074. [Google Scholar] [CrossRef]
- Aristizabal, N.; Holder, M.P.; Durham, L.; Ashraf, A.P.; Taylor, S.; Salas, A.A. Safety and Efficacy of Early Vitamin D Supplementation in Critically Ill Extremely Preterm Infants: An Ancillary Study of a Randomized Trial. J. Acad. Nutr. Diet. 2023, 123, 87–94. [Google Scholar] [CrossRef]
- Fort, P.; Salas, A.A.; Nicola, T.; Craig, C.M.; Carlo, W.A.; Ambalavanan, N. A Comparison of 3 Vitamin D Dosing Regimens in Extremely Preterm Infants: A Randomized Controlled Trial. J. Pediatr. 2016, 174, 132–138.e1. [Google Scholar] [CrossRef]
- Natarajan, C.K.; Sankar, M.J.; Agarwal, R.; Pratap, O.T.; Jain, V.; Gupta, N.; Gupta, A.K.; Deorari, A.K.; Paul, V.K.; Sreenivas, V. Trial of Daily Vitamin D Supplementation in Preterm Infants. Pediatrics 2014, 133, e628–e634. [Google Scholar] [CrossRef]
- Vierge, M.; Laborie, S.; Bertholet-Thomas, A.; Carlier, M.-C.; Picaud, J.-C.; Claris, O.; Bacchetta, J. Intoxication néonatale à la vitamine D chez des anciens prématurés: Une série de 16 cas. Arch. Pédiatrie 2017, 24, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, R.; Singh, H.; Wang, Y.; Harb, A.; Gornes, C.; Liu, J.; Rehan, V.K. Effect of Perinatal Vitamin D Deficiency on Lung Mesenchymal Stem Cell Differentiation and Injury Repair Potential. Am. J. Respir. Cell Mol. Biol. 2021, 65, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Yurt, M.; Liu, J.; Sakurai, R.; Gong, M.; Husain, S.M.; Siddiqui, M.A.; Husain, M.; Villarreal, P.; Akcay, F.; Torday, J.S.; et al. Vitamin D Supplementation Blocks Pulmonary Structural and Functional Changes in a Rat Model of Perinatal Vitamin D Deficiency. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2014, 307, L859–L867. [Google Scholar] [CrossRef]
- Chen, C.; Weng, H.; Zhang, X.; Wang, S.; Lu, C.; Jin, H.; Chen, S.; Liu, Y.; Sheng, A.; Sun, Y. Low-Dose Vitamin D Protects Hyperoxia-Induced Bronchopulmonary Dysplasia by Inhibiting Neutrophil Extracellular Traps. Front. Pediatr. 2020, 8, 335. [Google Scholar] [CrossRef]
- Laborie, S.; Denis, A.; Raverot, V.; Claris, O.; Bacchetta, J.; Butin, M. A Third of Premature Neonates Displayed Inadequate 25-hydroxyvitamin D Levels before Being Discharged from a French Neonatal Intensive Care Unit. Acta Paediatr. 2022, 111, 104–106. [Google Scholar] [CrossRef] [PubMed]
- Mathilde, M.; Butin, M.; Pascal, R.; Plaisant, F.; Laborie, S.; Bacchetta, J. Local Protocol Helped to Deliver Vitamin D Levels More Accurately in Preterm Infants. Acta Paediatr. 2022, 111, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Kołodziejczyk-Nowotarska, A.; Bokiniec, R.; Seliga-Siwecka, J. Monitored Supplementation of Vitamin D in Preterm Infants: A Randomized Controlled Trial. Nutrients 2021, 13, 3442. [Google Scholar] [CrossRef] [PubMed]
- Agostoni, C.; Buonocore, G.; Carnielli, V.; De Curtis, M.; Darmaun, D.; Decsi, T.; Domellöf, M.; Embleton, N.; Fusch, C.; Genzel-Boroviczeny, O.; et al. Enteral Nutrient Supply for Preterm Infants: Commentary From the European Society of Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 85–91. [Google Scholar] [CrossRef]
- Koletzko, B.; Goulet, O.; Hunt, J.; Krohn, K.; Shamir, R.; for the Parenteral Nutrition Guidelines Working Group 8. Vitamins. J. Pediatr. Gastroenterol. Nutr. 2005, 41, S47–S53. [Google Scholar] [CrossRef]
- Higgins, R.D.; Jobe, A.H.; Koso-Thomas, M.; Bancalari, E.; Viscardi, R.M.; Hartert, T.V.; Ryan, R.M.; Kallapur, S.G.; Steinhorn, R.H.; Konduri, G.G.; et al. Bronchopulmonary Dysplasia: Executive Summary of a Workshop. J. Pediatr. 2018, 197, 300–308. [Google Scholar] [CrossRef]
- Jobe, A.H.; Bancalari, E. Bronchopulmonary Dysplasia. Am. J. Respir. Crit. Care Med. 2001, 163, 1723–1729. [Google Scholar] [CrossRef] [PubMed]
- Baud, O.; Laughon, M.; Lehert, P. Survival without Bronchopulmonary Dysplasia of Extremely Preterm Infants: A Predictive Model at Birth. Neonatology 2021, 118, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Laughon, M.M.; Langer, J.C.; Bose, C.L.; Smith, P.B.; Ambalavanan, N.; Kennedy, K.A.; Stoll, B.J.; Buchter, S.; Laptook, A.R.; Ehrenkranz, R.A.; et al. Prediction of Bronchopulmonary Dysplasia by Postnatal Age in Extremely Premature Infants. Am. J. Respir. Crit. Care Med. 2011, 183, 1715–1722. [Google Scholar] [CrossRef]
- Lapcharoensap, W.; Gage, S.C.; Kan, P.; Profit, J.; Shaw, G.M.; Gould, J.B.; Stevenson, D.K.; O’Brodovich, H.; Lee, H.C. Hospital Variation and Risk Factors for Bronchopulmonary Dysplasia in a Population-Based Cohort. JAMA Pediatr. 2015, 169, e143676. [Google Scholar] [CrossRef] [PubMed]
- Spiegler, J.; Preuß, M.; Gebauer, C.; Bendiks, M.; Herting, E.; Göpel, W.; Bendiks, M.; Berghäuser, M.A.; Böckenholt, K.; Bohnhorst, B.; et al. Does Breastmilk Influence the Development of Bronchopulmonary Dysplasia? J. Pediatr. 2016, 169, 76–80.e4. [Google Scholar] [CrossRef]
- Fenton, T.R.; Kim, J.H. A Systematic Review and Meta-Analysis to Revise the Fenton Growth Chart for Preterm Infants. BMC Pediatr. 2013, 13, 59. [Google Scholar] [CrossRef]
- Laborie, S. Les Surdosages en 25 OHD Pendant les Premiers Mois de vie Sont-Ils un Facteur de Risque de Dysplasie Bronchopulmonaire? JFRN: Paris, France, 2022. [Google Scholar]
- Shroff, R.; Wan, M.; Nagler, E.V.; Bakkaloğlu, S.; Fischer, D.-C.; Bishop, N.; Cozzolino, M.; Bacchetta, J.; Edefonti, A.; Stefanidis, C.J.; et al. Clinical Practice Recommendations for Native Vitamin D Therapy in Children with Chronic Kidney Disease Stages 2–5 and on Dialysis. Nephrol. Dial. Transplant. 2017, 32, 1098–1113. [Google Scholar] [CrossRef]
- Embleton, N.D.; Moltu, S.J.; Lapillonne, A.; van den Akker, C.H.P.; Carnielli, V.; Fusch, C.; Gerasimidis, K.; van Goudoever, J.B.; Haiden, N.; Iacobelli, S.; et al. Enteral Nutrition in Preterm Infants (2022): A Position Paper from the ESPGHAN Committee on Nutrition and Invited Experts. J. Pediatr. Gastroenterol. Nutr. 2022. ahead of print. [Google Scholar] [CrossRef]
- Bronsky, J.; Campoy, C.; Braegger, C.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Carnielli, V.; Darmaun, D.; Decsi, T.; et al. ESPGHAN/ESPEN/ESPR/CSPEN Guidelines on Pediatric Parenteral Nutrition: Vitamins. Clin. Nutr. 2018, 37, 2366–2378. [Google Scholar] [CrossRef]
- Burris, H.H.; Van Marter, L.J.; McElrath, T.F.; Tabatabai, P.; Litonjua, A.A.; Weiss, S.T.; Christou, H. Vitamin D Status among Preterm and Full-Term Infants at Birth. Pediatr. Res. 2014, 75, 75–80. [Google Scholar] [CrossRef]
- Kassai, M.S.; Cafeo, F.R.; Affonso-Kaufman, F.A.; Suano-Souza, F.I.; Sarni, R.O.S. Vitamin D Plasma Concentrations in Pregnant Women and Their Preterm Newborns. BMC Pregnancy Childbirth 2018, 18, 412. [Google Scholar] [CrossRef] [PubMed]
- Onwuneme, C.; Martin, F.; McCarthy, R.; Carroll, A.; Segurado, R.; Murphy, J.; Twomey, A.; Murphy, N.; Kilbane, M.; McKenna, M.; et al. The Association of Vitamin D Status with Acute Respiratory Morbidity in Preterm Infants. J. Pediatr. 2015, 166, 1175–1180.e1. [Google Scholar] [CrossRef] [PubMed]
- Courbebaisse, M.; Souberbielle, J.-C.; Baptiste, A.; Taieb, J.; Tsatsaris, V.; Guibourdenche, J.; Senat, M.-V.; Haidar, H.; Jani, J.; Guizani, M.; et al. Vitamin D Status during Pregnancy and in Cord Blood in a Large Prospective French Cohort. Clin. Nutr. 2019, 38, 2136–2144. [Google Scholar] [CrossRef]
- Papalia, H.; Samonini, A.; Buffat, C.; Gras, E.; des Robert, C.; Landrier, J.-F.; Pauly, V.; Boubred, F. Low Vitamin D Levels at Birth and Early Respiratory Outcome in Infants With Gestational Age Less Than 29 Weeks. Front. Pediatr. 2022, 9, 790839. [Google Scholar] [CrossRef] [PubMed]
- Bacchetta, J.; Schmitt, C.P.; Bakkaloglu, S.A.; Cleghorn, S.; Leifheit-Nestler, M.; Prytula, A.; Ranchin, B.; Schön, A.; Stabouli, S.; Van de Walle, J.; et al. Diagnosis and Management of Mineral and Bone Disorders in Infants with CKD: Clinical Practice Points from the ESPN CKD-MBD and Dialysis Working Groups and the Pediatric Renal Nutrition Taskforce. Pediatr. Nephrol. 2023, 38, 3163–3181. [Google Scholar] [CrossRef] [PubMed]
- Bacchetta, J.; Edouard, T.; Laverny, G.; Bernardor, J.; Bertholet-Thomas, A.; Castanet, M.; Garnier, C.; Gennero, I.; Harambat, J.; Lapillonne, A.; et al. Vitamin D and Calcium Intakes in General Pediatric Populations: A French Expert Consensus Paper. Arch. Pédiatrie 2022, 29, 312–325. [Google Scholar] [CrossRef] [PubMed]
- Durup, D.; Jørgensen, H.L.; Christensen, J.; Schwarz, P.; Heegaard, A.M.; Lind, B. A Reverse J-Shaped Association of All-Cause Mortality with Serum 25-Hydroxyvitamin D in General Practice: The CopD Study. J. Clin. Endocrinol. Metab. 2012, 97, 2644–2652. [Google Scholar] [CrossRef]
- Sempos, C.T.; Durazo-Arvizu, R.A.; Dawson-Hughes, B.; Yetley, E.A.; Looker, A.C.; Schleicher, R.L.; Cao, G.; Burt, V.; Kramer, H.; Bailey, R.L.; et al. Is There a Reverse J-Shaped Association Between 25-Hydroxyvitamin D and All-Cause Mortality? Results from the U.S. Nationally Representative NHANES. J. Clin. Endocrinol. Metab. 2013, 98, 3001–3009. [Google Scholar] [CrossRef]
- Salle, B.L.; Delvin, E.E.; Lapillonne, A.; Bishop, N.J.; Glorieux, F.H. Perinatal Metabolism of Vitamin D. Am. J. Clin. Nutr. 2000, 71, 1317S–1324S. [Google Scholar] [CrossRef]
- Matejek, T.; Zapletalova, B.; Stepan, M.; Malakova, J.; Palicka, V. Dynamics of the Vitamin D C3-Epimer Levels in Preterm Infants. Clin. Chem. Lab. Med. CCLM 2023, 61, 1084–1094. [Google Scholar] [CrossRef]
- Bailey, D.; Veljkovic, K.; Yazdanpanah, M.; Adeli, K. Analytical Measurement and Clinical Relevance of Vitamin D3 C3-Epimer. Clin. Biochem. 2013, 46, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Mandell, E.W.; Ryan, S.; Seedorf, G.J.; Gonzalez, T.; Smith, B.J.; Fleet, J.C.; Abman, S.H. Maternal Vitamin D Deficiency Causes Sustained Impairment of Lung Structure and Function and Increases Susceptibility to Hyperoxia-Induced Lung Injury in Infant Rats. Am. J. Respir. Cell Mol. Biol. 2020, 63, 79–91. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M.; Feng, R.; Bazacliu, C.; Ferkol, T.W.; Ren, C.L.; Mariani, T.J.; Poindexter, B.B.; Wang, F.; Moore, P.E.; Chougnet, C.; et al. Black Race Is Associated with a Lower Risk of Bronchopulmonary Dysplasia. J. Pediatr. 2019, 207, 130–135.e2. [Google Scholar] [CrossRef]
- Dhandai, R.; Jajoo, M.; Singh, A.; Mandal, A.; Jain, R. Association of Vitamin D Deficiency with an Increased Risk of Late-Onset Neonatal Sepsis. Paediatr. Int. Child Health 2018, 38, 193–197. [Google Scholar] [CrossRef]
- Cizmeci, M.N.; Kanburoglu, M.K.; Akelma, A.Z.; Ayyildiz, A.; Kutukoglu, I.; Malli, D.D.; Tatli, M.M. Cord-Blood 25-Hydroxyvitamin D Levels and Risk of Early-Onset Neonatal Sepsis: A Case–Control Study from a Tertiary Care Center in Turkey. Eur. J. Pediatr. 2015, 174, 809–815. [Google Scholar] [CrossRef]
- Say, B.; Uras, N.; Sahin, S.; Degirmencioglu, H.; Oguz, S.S.; Canpolat, F.E. Effects of Cord Blood Vitamin D Levels on the Risk of Neonatal Sepsis in Premature Infants. Korean J. Pediatr. 2017, 60, 248. [Google Scholar] [CrossRef][Green Version]
- Cetinkaya, M.; Cekmez, F.; Buyukkale, G.; Erener-Ercan, T.; Demir, F.; Tunc, T.; Aydın, F.N.; Aydemir, G. Lower Vitamin D Levels Are Associated with Increased Risk of Early-Onset Neonatal Sepsis in Term Infants. J. Perinatol. 2015, 35, 39–45. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Pregnancy Characteristics * | Excessive 25(OH)D N = 81 | Normal 25(OH)D N = 94 | Total N = 175 | |
|---|---|---|---|---|
| Parity | 1 | 29 (35.8%) | 40 (42.6%) | 69 (39.4%) |
| 2 | 25 (30.9%) | 31 (33.0%) | 56 (32.0%) | |
| 3 | 19 (23.5%) | 14 (14.9%) | 33 (18.9%) | |
| ≥4 | 8 (9.9%) | 8 (8.5%) | 16 (9.1%) | |
| Unknown | 0 (0.0%) | 1 (1.1%) | 1 (0.6%) | |
| Multiple pregnancy | 30 (37.5%) | 25 (26.6%) | 56 (32.0%) | |
| Any hypertension during pregnancy | 19 (23.5%) | 21 (22.3%) | 40 (22.9%) | |
| Preterm premature rupture of membranes | 26 (32.1%) | 27 (28.7%) | 53 (30.3%) | |
| Any diabetes during pregnancy | 8 (9.9%) | 13 (13.8%) | 21 (12.0%) | |
| Histological chorioamnionitis | 21 (25.9%) | 13 (13.8%) | 34 (19.4%) | |
| Unavailable | 0 (0%) | 3 (3.2%) | 3 (1.7%) | |
| Clinical chorioamnionitis | 11 (13.6%) | 7 (7.4%) | 18 (10.3%) | |
| Unknown | 1/1.2%) | 3 (3.2%) | 4 (2.3%) | |
| Any antenatal corticosteroids | 76 (93.8%) | 83 (88.3%) | 159 (90.9%) |
| Neonatal Characteristics * | N (%), Except if Specified | Excessive 25(OH)D N = 81 | Normal 25(OH)D N = 94 | Total N = 175 | |
|---|---|---|---|---|---|
| Birth season | Summer | 19 (23.5%) | 32 (34.0%) | 51 (29.1%) | |
| Fall | 20 (24.7%) | 26 (27.7%) | 46 (26.3%) | ||
| Winter | 21 (25.9%) | 18 (19.1%) | 39 (22.3%) | ||
| Spring | 21 (25.9%) | 18 (19.1%) | 39 (22.3%) | ||
| Sex | Male | 39 (48.1%) | 51 (54.3%) | 90 (51.4%) | |
| Term (weeks) | Mean (SD) | 27.58 (1.84) | 27.88 (1.56) | 27.74 (1.70) | |
| Weight (g) | Mean (SD) | 938 (272) | 998 (305) | 970 (291) | |
| Height (cm) | Mean (SD) | 35.05 (3.11) | 35.15 (3.98) | 35.11 (3.60) | |
| Head circumference (cm) | Mean (SD) | 24.83 (2.19) | 25.44 (2.72) | 25.16 (2,50) | |
| Small for gestational age ** | 14 (17.3%) | 17 (18.1%) | 31 (17.7%) | ||
| Apgar at 5 min | 8–10 | 55 (67.9%) | 52 (55.3%) | 107 (61.1%) | |
| 4–7 | 21 (25.9%) | 37 (39.4%) | 58 (33.1%) | ||
| 0–3 | 4 (4.9%) | 4 (4.3%) | 8 (4.6%) | ||
| Not available | 1 (1.2%) | 1 (1.1%) | 2 (1.1%) | ||
| Maximum ventilation during the first 24 h | FiO2 < 30% and noninvasive ventilation | 7 (8.6%) | 6 (6.4%) | 13 (7.4%) | |
| Assisted ventilation and FiO2 < 30% | 0 (0.0%) | 1 (1.1%) | 1 (0.6%) | ||
| Assisted ventilation or FiO2≥ 30% | 74 (91.4%) | 87 (92.6%) | 161 (92.0%) | ||
| Parenteral nutrition (days) | Median | 14 | 13 | 14 | |
| Interquartile range | 7–23 | 7–20 | 7–21 | ||
| Enteral feeding | Maternal or donor milk | 17 (21.0%) | 19 (20.2%) | 36 (20.6%) | |
| Mixed | 50 (61.7%) | 49 (52.1%) | 99 (56.6%) | ||
| Formula or donor milk | 14 (17.3%) | 26 (27.7%) | 40 (22.9%) | ||
| Any mother’s milk given | 66 (81.5%) | 68 (72.3%) | 134 (76.6%) | ||
| First determination of 25(OH)D (nmol/L) | Mean (SD) | 139.4 (43.1) | 86.1 (19.6) | 110.8 (42.1) | |
| Corrected age at first 25(OH)D determination | Mean (SD) | 32.4 (1.9) | 32.5 (1.5) | 32.4 (1.7) | |
| Second determination of 25(OH)D (nmol/L) | 25 (30.9%) | 20 (21.3%) | 45 (25.7%) | ||
| Mean (SD) | 144.40 (29.58) | 85.20 (17.76) | 118.1 (38.7) | ||
| Corrected age at second determination of 25(OH)D | Mean (SD) | 34.2 (1.2) | 34.2 (1.5) | 34.2 (1.3) | |
| Outcomes * | N (%), Except if Specified | Excessive 25(OH)D N = 81 | Normal 25(OH)D N = 94 | Total N = 175 |
|---|---|---|---|---|
| Intraventricular hemorrhage | 1 | 6 (7.4%) | 11 (11.7%) | 17 (9.7%) |
| 2 | 2 (2.5%) | 4 (4.3%) | 6 (3.4%) | |
| 3 | 1 (1.2%) | 1 (1.1%) 4 (4.3%) | 2 (1.1%) | |
| 4 | 3 (3.7%) | 4 (4.3%) | 7 (4.0%) | |
| Cystic periventricular leukomalacia | 0 (0.0%) | 5 (5.3%) | 5 (2.9%) | |
| Retinopathy of prematurity | 1 | 9 (11.1%) | 15 (16.0%) | 24 (13.7%) |
| 2 | 18 (22.2%) | 14 (14.9%) | 32 (18.3%) | |
| 3 | 7 (8.6%) | 5 (5.3%) | 12 (6.9%) | |
| Unknown | 9 (11.1%) | 13 (13.8%) | 22 (12.6%) | |
| PDA requiring treatment | 22 (27.2%) | 30 (31.9%) | 52 (29.7%) | |
| Enterocolitis grade ≥2 | 2 | 0 (0.0%) | 1 (1.1%) | 1 (0.6%) |
| 3 | 0 (0.0%) | 2 (2.1%) | 2 (1.1%) | |
| Number of sepsis events | 1 | 23 (28.4%) | 19 (20.2%) | 42 (24.0%) |
| 2 | 4 (4.9%) | 5 (5.3%) | 9 (5.1%) | |
| 3 | 1 (1.2%) | 1 (1.1%) | 2 (1.1%) | |
| BPD grade | No BPD | 18 (22.8%) | 22 (23.9%) | 40 (23.4%) |
| Mild | 29 (36.7%) | 38 (41.3%) | 67 (39.2%) | |
| Moderate | 24 (30.4%) | 31 (33.7%) | 55 (32.2%) | |
| Severe | 8 (10.1%) | 1 (1.1%) | 9 (5.3%) | |
| Moderate or severe BPD or death | 34 (42.0%) | 34 (36.2%) | 68 (38.9%) | |
| Moderate or severe BPD | 32 (39.5%) | 32 (34.0%) | 64 (36.6%) | |
| Death before 36 weeks corrected age | 2 (2.5%) | 2 (2.1%) | 4 (2.3%) |
| Variables | OR | 95%CI * | p-Value | |
|---|---|---|---|---|
| Full model | ||||
| Any 25(OH)D determination ≥ 120 nmol/L | 1.011 | 0.475–2.145 | 0.977 | |
| Weight (g) | 0.997 | 0.994–0.999 | 0.019 | |
| Term (weeks) | 0.661 | 0.436–0.989 | 0.046 | |
| Multiple pregnancy | 1.881 | 0.855–4.248 | 0.120 | |
| Sex, female | 0.530 | 0.242–1.134 | 0.106 | |
| Maximal ventilation during the first 24 h | 0.838 | 0.210–3.743 | 0.806 | |
| Any mother’s milk administrated | 1.237 | 0.520–3.011 | 0.634 | |
| Apgar at 5 min | 8–10 | 1.000 | ||
| 4–7 | 0.912 | 0.402–2.041 | 0.823 | |
| 0–3 | 0.795 | 0.147–4.108 | 0.782 | |
| Spontaneous birth | 0.631 | 0.223–1.770 | 0.381 | |
| Final model | ||||
| Any 25(OH)D determination ≥ 120 nmol/L | 1.029 | 0.503–2.093 | 0.936 | |
| Weight (g) | 0.997 | 0.995–0.998 | 0.001 | |
| Term (weeks) | 0.737 | 0.551–0.975 | 0.035 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laborie, S.; Bonjour, M.; Bacchetta, J.; Mauras, M.; Butin, M. Is 25OH Vitamin D Excess before 36 Weeks Corrected Age an Independent Risk Factor for Bronchopulmonary Dysplasia or Death? Nutrients 2023, 15, 4423. https://doi.org/10.3390/nu15204423
Laborie S, Bonjour M, Bacchetta J, Mauras M, Butin M. Is 25OH Vitamin D Excess before 36 Weeks Corrected Age an Independent Risk Factor for Bronchopulmonary Dysplasia or Death? Nutrients. 2023; 15(20):4423. https://doi.org/10.3390/nu15204423
Chicago/Turabian StyleLaborie, Sophie, Maxime Bonjour, Justine Bacchetta, Mathilde Mauras, and Marine Butin. 2023. "Is 25OH Vitamin D Excess before 36 Weeks Corrected Age an Independent Risk Factor for Bronchopulmonary Dysplasia or Death?" Nutrients 15, no. 20: 4423. https://doi.org/10.3390/nu15204423
APA StyleLaborie, S., Bonjour, M., Bacchetta, J., Mauras, M., & Butin, M. (2023). Is 25OH Vitamin D Excess before 36 Weeks Corrected Age an Independent Risk Factor for Bronchopulmonary Dysplasia or Death? Nutrients, 15(20), 4423. https://doi.org/10.3390/nu15204423