
SLC6A4 DNA Methylation Levels and Serum Kynurenine/Tryptophan Ratio in Eating Disorders: A Possible Link with Psychopathological Traits?

 , , , ,
, , , ,  , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Healthy Control Recruitment
2.2. Ethical Statement and Inclusion Criteria
2.3. Psychological Traits
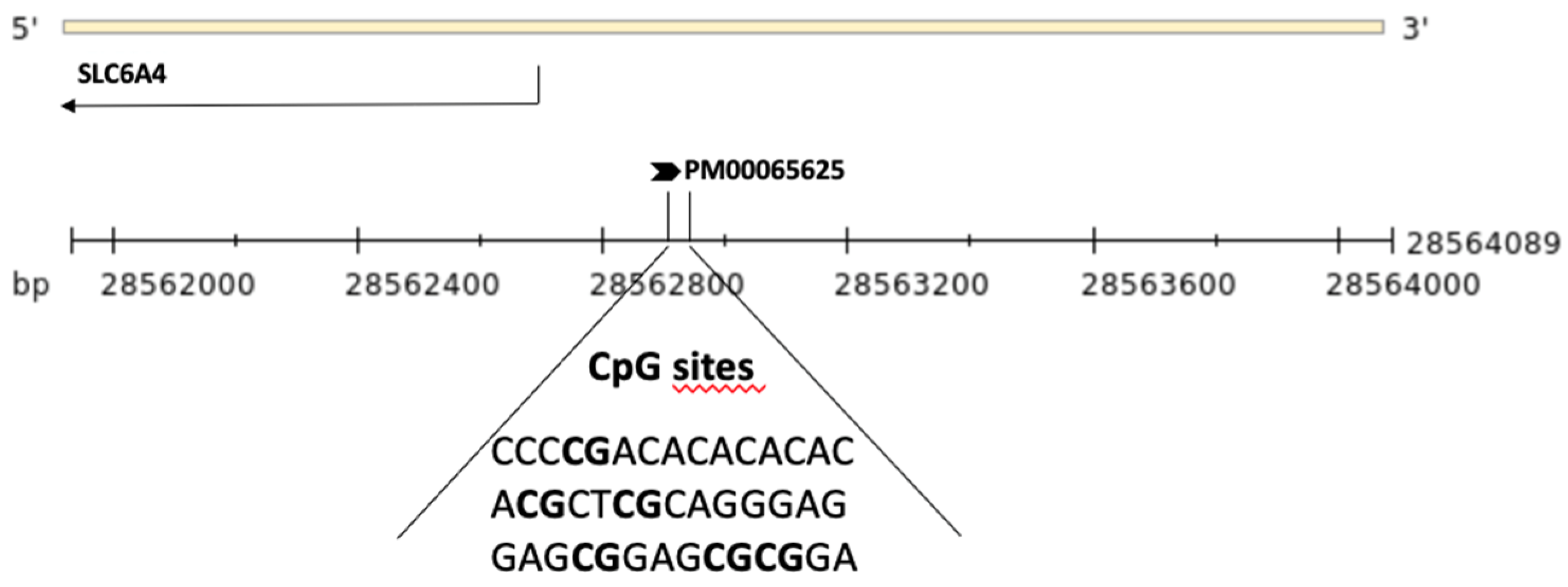
2.4. DNA Methylation Analysis
2.5. HPLC Analysis
2.6. Statistical Analysis
3. Results
3.1. Clinical Data
Hematological Data
3.2. Biochemical Data
3.3. Epigenetic Data
3.4. Psychopathological Data
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Arcelus, J.; Mitchell, A.J.; Wales, J.; Nielsen, S. Mortality rates in patients with anorexia nervosa and other eating disorders: A meta-analysis of 36 studies. Arch. Gen. Psychiatry 2011, 68, 724–731. [Google Scholar] [CrossRef] [PubMed]
- Udo, T.; Grilo, C.M. Prevalence and correlates of DSM-5-defined eating disorders in a nationally representative sample of US adults. Biol. Psychiatry. 2018, 84, 345–354. [Google Scholar] [CrossRef]
- Feltner, C.; Peat, C.; Reddy, S.; Riley, S.; Berkman, N.; Middleton, J.C.; Balio, C.; Coker-Schwimmer, M.; Jonas, D.E. Screening for Eating Disorders in Adolescents and Adults: Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2022, 327, 1068–1082. [Google Scholar] [CrossRef]
- Momen, N.C.; Plana-Ripoll, O.; Bulik, C.M.; McGrath, J.J.; Thornton, L.M.; Yilmaz, Z.; Petersen, L.V. Comorbidity between types of eating disorder and general medical conditions. Br. J. Psychiatry 2021, 23, 1–8. [Google Scholar] [CrossRef]
- Levinson, C.A.; Cusack, C.; Brown, M.L.; Smith, A.R. A network approach can improve eating disorder conceptualization and treatment. Nat. Rev. Psychol. 2022, 1, 419–430. [Google Scholar] [CrossRef]
- Preti, A.; de Girolamo, G.; Vilagut, G.; Alonso, J.; de Graaf, R.; Bruffaerts, R.; Demyttenaere, K.; Pinto-Meza, A.; Haro, J.M.; Morosini, P.; et al. The epidemiology of eating disorders in six European countries: Results of the ESEMeD-WMH project. J. Psychiatr. Res. 2009, 43, 1125–1132. [Google Scholar] [CrossRef]
- Merikangas, K.R.; He, J.P.; Burstein, M.; Swanson, S.A.; Avenevoli, S.; Cui, L.; Benjet, C.; Georgiades, K.; Swendsen, J. Lifetime prevalence of mental disorders in U.S. adolescents: Results from the National Comorbidity Survey Replication-Adolescent Supplement (NCS-A). J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 980–989. [Google Scholar] [CrossRef]
- Paolacci, S.; Kiani, A.K.; Manara, E.; Beccari, T.; Ceccarini, M.R.; Stuppia, L.; Chiurazzi, P.; Dalla Ragione, L.; Bertelli, M. Genetic contributions to the etiology of anorexia nervosa: New perspectives in molecular diagnosis and treatment. Mol. Genet. Genom. Med. 2020, 8, e1244. [Google Scholar] [CrossRef] [PubMed]
- Bulik, C.M.; Coleman, J.R.I.; Hardaway, J.A.; Breithaupt, L.; Watson, H.J.; Bryant, C.D.; Breen, G. Genetics and neurobiology of eating disorders. Nat. Neurosci. 2022, 25, 543–554. [Google Scholar] [CrossRef] [PubMed]
- Ceccarini, M.R.; Precone, V.; Manara, E.; Paolacci, S.; Maltese, P.E.; Benfatti, V.; Dhuli, K.; Donato, K.; Guerri, G.; Marceddu, G.; et al. A next generation sequencing gene panel for use in the diagnosis of anorexia nervosa. Eat Weight Disord. 2022, 27, 1869–1880. [Google Scholar] [CrossRef]
- Trace, S.E.; Baker, J.H.; Peñas-Lledó, E.; Bulik, C.M. The genetics of eating disorders. Annu. Rev. Clin. Psychol. 2013, 9, 589–620. [Google Scholar] [CrossRef]
- Hinney, A.; Volckmar, A.L. Genetics of eating disorders. Curr. Psychiatry Rep. 2013, 15, 423. [Google Scholar] [CrossRef] [PubMed]
- Soubrié, P. Reconciling the role of central serotonin neurons in human and animal behavior. Behav. Brain Sci. 1986, 9, 319–335. [Google Scholar] [CrossRef]
- Walther, D.J.; Peter, J.U.; Bashammakh, S.; Hörtnagl, H.; Voits, M.; Fink, H.; Bader, M. Synthesis of serotonin by a second tryptophan hydroxylase isoform. Science 2003, 299, 76. [Google Scholar] [CrossRef] [PubMed]
- Brewerton, T.D. Toward a unified theory of serotonin dysregulation in eating and related disorders. Psychoneuroendocrinology 1995, 20, 561–590. [Google Scholar] [CrossRef]
- Boehm, I.; Walton, E.; Alexander, N.; Batury, V.L.; Seidel, M.; Geisler, D.; King, J.A.; Weidner, K.; Roessner, V.; Ehrlich, S. Peripheral serotonin transporter DNA methylation is linked to increased salience network connectivity in females with anorexia nervosa. J. Psychiatry Neurosci. 2020, 45, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Kaye, W.H.; Gwirtsman, H.E.; Brewerton, T.D.; George, D.T.; Wurtman, R.J. Bingeing behavior and plasma amino acids: A possible involvement of brain serotonin in bulimia nervosa. Psychiatry Res. 1988, 23, 31–43. [Google Scholar] [CrossRef]
- Favaro, A.; Caregaro, L.; Burlina, A.B.; Santonastaso, P. Tryptophan levels, excessive exercise, and nutritional status in anorexia nervosa. Psychosom. Med. 2000, 62, 535–538. [Google Scholar] [CrossRef]
- Lischka, J.; Schanzer, A.; Baumgartner, M.; de Gier, C.; Greber-Platzer, S.; Zeyda, M. Tryptophan Metabolism Is Associated with BMI and Adipose Tissue Mass and Linked to Metabolic Disease in Pediatric Obesity. Nutrients 2022, 14, 286. [Google Scholar] [CrossRef]
- Sundaramurthy, D.; Pieri, L.F.; Gape, H.; Markham, A.F.; Campbell, D.A. Analysis of the serotonin transporter gene linked polymorphism (5-HTTLPR) in anorexia nervosa. Am. J. Med. Genet. 2000, 96, 53–55. [Google Scholar] [CrossRef]
- Gelernter, J.; Pakstis, A.J.; Kidd, K.K. Linkage mapping of serotonin transporter protein gene SLC6A4 on chromosome 17. Hum. Genet. 1995, 95, 677–680. [Google Scholar] [CrossRef]
- Murphy, D.L.; Moya, P.R. Human serotonin transporter gene (SLC6A4) variants: Their contributions to understanding pharmacogenomic and other functional G x G and G x E differences in health and disease. Curr. Opin. Pharmacol. 2011, 11, 3–10. [Google Scholar] [CrossRef]
- Rozenblat, V.; Ong, D.; Fuller-Tyszkiewicz, M.; Akkermann, K.; Collier, D.; Engels, R.R.C.M.E.; Fernandez-Aranda, F.; Harro, J.; Homberg, J.R.; Karwautz, A.; et al. A systematic review and secondary data analysis of the interactions between the serotonin transporter 5-HTTLPR polymorphism and environmental and psychological factors in eating disorders. J. Psychiatr. Res. 2017, 84, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Jang, Y.J.; Lim, S.W.; Moon, Y.K.; Kim, S.Y.; Lee, H.; Kim, S.; Kim, D.K. 5-HTTLPR-rs25531 and Antidepressant Treatment Outcomes in Korean Patients with Major Depression. Pharmacopsychiatry 2021, 54, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Tanahashi, S.; Tanii, H.; Konishi, Y.; Otowa, T.; Sasaki, T.; Tochigi, M.; Okazaki, Y.; Kaiya, H.; Okada, M. Association of Serotonin Transporter Gene (5-HTTLPR/rs25531) Polymorphism with Comorbidities of Panic Disorder. Neuropsychobiology 2021, 80, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Wang, L.; Cao, C.; Fang, R.; Hall, B.J.; Elhai, J.D.; Liberzon, I. Post-traumatic stress symptoms of children and adolescents exposed to the 2008 Wenchuan Earthquake: A longitudinal study of 5-HTTLPR genotype main effects and gene-environment interactions. Int. J. Psychol. 2021, 56, 22–29. [Google Scholar] [CrossRef]
- Pringle, A.; Jennings, K.A.; Line, S.; Bannerman, D.M.; Higgs, S.; Sharp, T. Mice overexpressing the 5-hydroxytryptamine transporter show no alterations in feeding behaviour and increased non-feeding responses to fenfluramine. Psychopharmacology 2008, 200, 291–300. [Google Scholar] [CrossRef]
- Murphy, D.L.; Lesch, K.P. Targeting the murine serotonin transporter: Insights into human neurobiology. Nat. Rev. Neurosci. 2008, 9, 85–96. [Google Scholar] [CrossRef]
- Steiger, H.; Booij, L. Eating Disorders, Heredity and Environmental Activation: Getting Epigenetic Concepts into Practice. J. Clin. Med. 2020, 9, 1332. [Google Scholar] [CrossRef]
- Franzago, M.; La Rovere, M.; Guanciali Franchi, P.; Vitacolonna, E.; Stuppia, L. Epigenetics and human reproduction: The primary prevention of the noncommunicable diseases. Epigenomics 2019, 11, 1441–1460. [Google Scholar] [CrossRef]
- Kang, H.J.; Kim, J.M.; Stewart, R.; Kim, S.Y.; Bae, K.Y.; Kim, S.W.; Shin, I.S.; Shin, M.G.; Yoon, J.S. Association of SLC6A4 methylation with early adversity, characteristics and outcomes in depression. Prog. Neuropsychopharmacol. Biol. Psychiatry 2013, 44, 23–28. [Google Scholar] [CrossRef]
- Booij, L.; Szyf, M.; Carballedo, A.; Frey, E.M.; Morris, D.; Dymov, S.; Vaisheva, F.; Ly, V.; Fahey, C.; Meaney, J.; et al. DNA methylation of the serotonin transporter gene in peripheral cells and stress-related changes in hippocampal volume: A study in depressed patients and healthy controls. PLoS ONE 2015, 10, e0119061. [Google Scholar] [CrossRef] [PubMed]
- Alasaari, J.S.; Lagus, M.; Ollila, H.M.; Toivola, A.; Kivimäki, M.; Vahtera, J.; Kronholm, E.; Härmä, M.; Puttonen, S.; Paunio, T. Environmental stress affects DNA methylation of a CpG rich promoter region of serotonin transporter gene in a nurse cohort. PLoS ONE 2012, 7, e45813. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Goldberg, J.; Vaccarino, V. Promoter methylation of serotonin transporter gene is associated with obesity measures: A monozygotic twin study. Int. J. Obes. 2013, 37, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Ruddick, J.P.; Evans, A.K.; Nutt, D.J.; Lightman, S.L.; Rook, G.A.; Lowry, C.A. Tryptophan metabolism in the central nervous system: Medical implications. Expert Rev. Mol. Med. 2006, 8, 1–27. [Google Scholar] [CrossRef]
- Floc’h, L.; Otten, W.; Merlot, E. Tryptophan metabolism, from nutrition to potential therapeutic applications. Amino Acids 2011, 41, 1195–1205. [Google Scholar] [CrossRef]
- Bender, D.A.; Olufunwa, R. Utilization of tryptophan, nicotinamide and nicotinic acid as precursors for nicotinamide nucleotide synthesis in isolated rat liver cells. Br. J. Nutr. 1988, 59, 279–287. [Google Scholar] [CrossRef]
- Mondanelli, G.; Coletti, A.; Greco, F.A.; Pallotta, M.T.; Orabona, C.; Iacono, A.; Belladonna, M.L.; Albini, E.; Panfili, E.; Fallarino, F.; et al. Positive allosteric modulation of indoleamine 2,3-dioxygenase 1 restrains neuroinflammation. Proc. Natl. Acad. Sci. USA 2020, 117, 3848–3857. [Google Scholar] [CrossRef]
- Chen, Y.; Guillemin, G.J. Kynurenine pathway metabolites in humans: Disease and healthy States. Int. J. Tryptophan Res. 2009, 2, 1–19. [Google Scholar] [CrossRef]
- Ceccarini, M.R.; Fittipaldi, S.; Ciccacci, C.; Granese, E.; Centofanti, F.; Dalla Ragione, L.; Bertelli, M.; Beccari, T.; Botta, A. Association Between DRD2 and DRD4 Polymorphisms and Eating Disorders in an Italian Population. Front. Nutr. 2022, 9, 838177. [Google Scholar] [CrossRef]
- Garner, D.M. The Eating Disorder Inventory-3: Professional Manual; Psychological Assessment Resources Inc.: Odessa, FL, USA, 2004. [Google Scholar]
- Ceccarini, M.R.; Tasegian, A.; Franzago, M.; Patria, F.F.; Albi, E.; Codini, M.; Conte, C.; Bertelli, M.; Dalla Ragione, L.; Stuppia, L. 5-HT2AR and BDNF gene variants in eating disorders susceptibility. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2020, 183, 155–163. [Google Scholar] [CrossRef]
- Franzago, M.; Porreca, A.; D’Ardes, M.; Di Nicola, M.; Di Tizio, L.; Liberati, M.; Stuppia, L.; Vitacolonna, E. The Obesogenic Environment: Epigenetic Modifications in Placental Melanocortin 4 Receptor Gene Connected to Gestational Diabetes and Smoking. Front. Nutr. 2022, 9, 879526. [Google Scholar] [CrossRef] [PubMed]
- Brandacher, G.; Hoeller, E.; Fuchs, D.; Weiss, H.G. Chronic Immune Activation Underlies Morbid Obesity: Is IDO a Key Player? Curr. Drug Metab. 2007, 8, 289–295. [Google Scholar] [CrossRef]
- Breum, L.; Rasmussen, M.H.; Hilsted, J.; Fernstrom, J.D. Twenty-four-hour plasma tryptophan concentrations and ratios are below normal in obese subjects and are not normalized by substantial weight reduction. Am. J. Clin. Nutr. 2003, 77, 1112–1118. [Google Scholar] [CrossRef] [PubMed]
- Caballero, B.; Finer, N.; Wurtman, R.J. Plasma amino acids and insulin levels in obesity: Response to carbohydrate intake and tryptophan supplements. Metabolism 1988, 37, 672–676. [Google Scholar] [CrossRef]
- Ashley, D.V.; Fleury, M.O.; Golay, A.; Maeder, E.; Leathwood, P.D. Evidence for diminished brain 5-hydroxytryptamine biosynthesis in obese diabetic and non-diabetic humans. Am. J. Clin. Nutr. 1985, 42, 1240–1245. [Google Scholar] [CrossRef] [PubMed]
- Chaves Filho, A.J.M.; Lima, C.N.C.; Vasconcelos, S.M.M.; de Lucena, D.F.; Maes, M.; Macedo, D. IDO chronic immune activation and tryptophan metabolic pathway: A potential pathophysiological link between depression and obesity. Prog. Neuropsychopharmacol. Biol. Psychiatry 2018, 80, 234–249. [Google Scholar] [CrossRef]
- Cussotto, S.; Delgado, I.; Anesi, A.; Dexpert, S.; Aubert, A.; Beau, C.; Forestier, D.; Ledaguenel, P.; Magne, E.; Mattivi, F.; et al. Tryptophan Metabolic Pathways Are Altered in Obesity and Are Associated with Systemic Inflammation. Front. Immunol. 2020, 11, 557. [Google Scholar] [CrossRef] [PubMed]
- Badawy, A.A. Kynurenine Pathway of Tryptophan Metabolism: Regulatory and Functional Aspects. Int. J. Tryptophan Res. 2017, 10, 1178646917691938. [Google Scholar] [CrossRef]
- Jamshed, L.; Debnath, A.; Jamshed, S.; Wish, J.V.; Raine, J.C.; Tomy, G.T.; Thomas, P.J.; Holloway, A.C. An Emerging Cross-Species Marker for Organismal Health: Tryptophan-Kynurenine Pathway. Int. J. Mol. Sci. 2022, 23, 6300. [Google Scholar] [CrossRef]
- Strasser, B.; Berger, K.; Fuchs, D. Effects of a caloric restriction weight loss diet on tryptophan metabolism and inflammatory biomarkers in overweight adults. Eur. J. Nutr. 2015, 54, 101–107. [Google Scholar] [CrossRef]
- Gauthier, C.; Hassler, C.; Mattar, L.; Launay, J.M.; Callebert, J.; Steiger, H.; Melchior, J.C.; Falissard, B.; Berthoz, S.; Mourier-Soleillant, V.; et al. Symptoms of depression and anxiety in anorexia nervosa: Links with plasma tryptophan and serotonin metabolism. Psychoneuroendocrinology 2014, 39, 170–178. [Google Scholar] [CrossRef]
- Attia, E.; Wolk, S.; Cooper, T.; Glasofer, D.; Walsh, B.T. Plasma tryptophan during weight restoration in patients with anorexia nervosa. Biol. Psychiatry 2005, 57, 674–678. [Google Scholar] [CrossRef] [PubMed]
- Dudzińska, E.; Szymona, K.; Kloc, R.; Kocki, T.; Gil-Kulik, P.; Bogucki, J.; Kocki, J.; Paduch, R.; Urbańska, E.M. Fractalkine, sICAM-1 and Kynurenine Pathway in Restrictive Anorexia Nervosa-Exploratory Study. Nutrients 2021, 13, 339. [Google Scholar] [CrossRef]
- Haleem, D.J. Improving therapeutics in anorexia nervosa with tryptophan. Life Sci. 2017, 178, 87–93. [Google Scholar] [CrossRef]
- Goodwin, G.M.; Shapiro, C.M.; Bennie, J.; Dick, H.; Carroll, S.; Fink, G. The neuroendocrine responses and psychological effects of infusion of L-tryptophan in anorexia nervosa. Psychol. Med. 1989, 19, 857–864. [Google Scholar] [CrossRef]
- Kaye, W.H.; Barbarich, N.C.; Putnam, K.; Gendall, K.A.; Fernstrom, J.; Fernstrom, M.; McConaha, C.W.; Kishore, A. Anxiolytic effects of acute tryptophan depletion in anorexia nervosa. Int. J. Eat Disord. 2003, 33, 257–267. [Google Scholar] [CrossRef] [PubMed]
- van Galen, K.A.; Booij, J.; Schrantee, A.; Adriaanse, S.M.; Unmehopa, U.A.; Fliers, E.; Schwartz, G.J.; DiLeone, R.J.; Ter Horst, K.W.; la Fleur, S.E.; et al. The response to prolonged fasting in hypothalamic serotonin transporter availability is blunted in obesity. Metabolism 2021, 123, 154839. [Google Scholar] [CrossRef]
- Hübel, C.; Marzi, S.J.; Breen, G.; Bulik, C.M. Epigenetics in eating disorders: A systematic review. Mol. Psychiatry 2019, 24, 901–915. [Google Scholar] [CrossRef] [PubMed]
- Campbell, I.C.; Mill, J.; Uher, R.; Schmidt, U. Eating disorders, gene–environment interactions and epigenetics. Neurosci. Biobehav. Rev. 2011, 35, 784–793. [Google Scholar] [CrossRef]
- Pjetri, E.; Schmidt, U.; Kas, M.; Campbell, I. Epigenetics and eating disorders. Curr. Opin. Clin. Nutr. Metab. Care 2012, 15, 330–335. [Google Scholar] [CrossRef]
- Ehrlich, S.; Weiss, D.; Burghardt, R.; Infante-Duarte, C.; Brockhaus, S.; Muschler, M.A.; Bleich, S.; Lehmkuhl, U.; Frieling, H. Promoter specific DNA methylation and gene expression of POMC in acutely underweight and recovered patients with anorexia nervosa. J. Psychiatr. Res. 2010, 44, 827–833. [Google Scholar] [CrossRef]
- Wyler, S.C.; Lord, C.C.; Lee, S.; Elmquist, J.K.; Liu, C. Serotonergic Control of Metabolic Homeostasis. Front. Cell Neurosci. 2017, 11, 277. [Google Scholar] [CrossRef] [PubMed]
- Silverstein-Metzler, M.G.; Shively, C.A.; Clarkson, T.B.; Appt, S.E.; Carr, J.J.; Kritchevsky, S.B.; Jones, S.R.; Register, T.C. Sertraline inhibits increases in body fat and carbohydrate dysregulation in adult female cynomolgus monkeys. Psychoneuroendocrinology 2016, 68, 29–38. [Google Scholar] [CrossRef]
- Palma-Gudiel, H.; Fañanás, L. An integrative review of methylation at the serotonin transporter gene and its dialogue with environmental risk factors, psychopathology and 5-HTTLPR. Neurosci. Biobehav. Rev. 2017, 72, 190–209. [Google Scholar] [CrossRef]
- Steiger, H.; Booij, L.; Kahan, E.; McGregor, K.; Thaler, L.; Fletcher, E.; Labbe, A.; Joober, R.; Israël, M.; Szyf, M.; et al. A longitudinal, epigenome-wide study of DNA methylation in anorexia nervosa: Results in actively ill, partially weight-restored, long-term remitted and non-eating-disordered women. J. Psychiatry Neurosci. 2019, 44, 205–213. [Google Scholar] [CrossRef]
- Pjetri, E.; Dempster, E.; Collier, D.A.; Treasure, J.; Kas, M.J.; Mill, J.; Campbell, I.C.; Schmidt, U. Quantitative promoter DNA methylation analysis of four candidate genes in anorexia nervosa: A pilot study. J. Psychiatr. Res. 2013, 47, 280–282. [Google Scholar] [CrossRef]
- Frieling, H.; Römer, K.D.; Wilhelm, J.; Hillemacher, T.; Kornhuber, J.; de Zwaan, M.; Jacoby, G.E.; Bleich, S. Association of catecholamine-O-methyltransferase and 5-HTTLPR genotype with eating disorder-related behavior and attitudes in females with eating disorders. Psychiatr. Genet. 2006, 16, 205–208. [Google Scholar] [CrossRef] [PubMed]
- Ando, T.; Ichimaru, Y.; Konjiki, F.; Shoji, M.; Komaki, G. Variations in the preproghrelin gene correlate with higher body mass index, fat mass, and body dissatisfaction in young Japanese women. Am. J. Clin. Nutr. 2007, 86, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Nisoli, E.; Brunani, A.; Borgomainerio, E.; Tonello, C.; Dioni, L.; Briscini, L.; Redaelli, G.; Molinari, E.; Cavagnini, F.; Carruba, M.O. D2 dopamine receptor (DRD2) gene Taq1A polymorphism and the eating-related psychological traits in eating disorders (anorexia nervosa and bulimia) and obesity. Eat Weight Disord. 2007, 12, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Castellini, G.; Franzago, M.; Bagnoli, S.; Lelli, L.; Balsamo, M.; Mancini, M.; Nacmias, B.; Ricca, V.; Sorbi, S.; Antonucci, I.; et al. Fat mass and obesity-associated gene (FTO) is associated to eating disorders susceptibility and moderates the expression of psychopathological traits. PLoS ONE 2017, 12, e0173560. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.K.; Wexler, T.L.; Zha, A.M.; Lawson, E.A.; Meenaghan, E.M.; Misra, M.; Binstock, A.B.; Herzog, D.B.; Klibanski, A. Androgen deficiency: Association with increased anxiety and depression symptom severity in anorexia nervosa. J. Clin. Psychiatry 2007, 68, 959–965. [Google Scholar] [CrossRef]
- Monteleone, P.; Santonastaso, P.; Pannuto, M.; Favaro, A.; Caregaro, L.; Castaldo, E.; Zanetti, T.; Maj, M. Enhanced serum cholesterol and triglyceride levels in bulimia nervosa: Relationships to psychiatric comorbidity, psychopathology and hormonal variables. Psychiatry Res. 2005, 134, 267–273. [Google Scholar] [CrossRef]
- Domschke, K.; Tidow, N.; Schwarte, K.; Deckert, J.; Lesch, K.P.; Arolt, V.; Zwanzger, P.; Baune, B.T. Serotonin transporter gene hypomethylation predicts impaired antidepressant treatment response. Int. J. Neuropsychopharmacol. 2014, 17, 1167–1176. [Google Scholar] [CrossRef] [PubMed]
- Webb, L.M.; Phillips, K.E.; Ho, M.C.; Veldic, M.; Blacker, C.J. The Relationship between DNA Methylation and Antidepressant Medications: A Systematic Review. Int. J. Mol. Sci. 2020, 21, 826. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | AN0 | AN1 | BN | BED | UFED | OSFED | CTR | p-Value * |
|---|---|---|---|---|---|---|---|---|
| Gender: | 0.001 | |||||||
| Female | 45 (100.0) | 21 (100.0) | 20 (95.2) | 23 (74.2) | 19 (82.6) | 12 (85.7) | 29 (85.3) | |
| Male | 0 (0.0) | 0 (0.0) | 1 (4.76) | 8 (25.8) | 4 (17.4) | 2 (14.3) | 5 (14.7) | |
| Relatives with EDs: | 0.309 | |||||||
| No | 27 (61.4) | 17 (81.0) | 12 (66.7) | 17 (58.6) | 13 (56.5) | 6 (42.9) | 34 (100.0) | |
| Yes | 17 (38.6) | 4 (19.0) | 6 (33.3) | 12 (41.4) | 10 (43.5) | 8 (57.1) | 0 (0.0) | |
| Age at time of admission, years | 16.0 [14.0;18.0] | 18.0 [17.0;19.0] | 19.0 [17.0;26.0] | 39.0 [20.2;52.8] | 54.0 [18.5;64.5] | 54.5 [35.2;58.5] | 25.0 [24.0;33.0] | <0.001 |
| Heigh, m | 1.62 [1.57;1.65] | 1.62 [1.58;1.65] | 1.67 [1.60;1.71] | 1.65 [1.60;1.70] | 1.60 [1.58;1.69] | 1.67 [1.60;1.73] | 1.70 [1.62;1.75] | 0.124 |
| Minimum Weight, kg | 38.0 [34.0;40.0] | 41.4 [37.6;48.0] | 48.0 [45.0;55.0] | 70.0 [62.2;85.5] | 67.0 [58.0;85.0] | 65.0 [48.0;75.0] | 56.0 [53.0;60.0] | <0.001 |
| Maximum Weight, kg | 54.5 [50.0;58.5] | 57.0 [53.0;63.0] | 68.0 [60.0;75.2] | 111 [106;126] | 106 [96.0;128] | 113 [98.5;130] | 63.0 [58.5;70.5] | <0.001 |
| BMI, kg/m2 | 14.4 [13.6;15.4] | 15.8 [14.7;17.2] | 17.7 [16.1;19.0] | 26.2 [23.6;30.9] | 25.4 [21.9;31.5] | 22.3 [18.9;26.9] | 20.5 [19.0;21.7] | <0.001 |
| Maximum BMI, kg/m2 | 21.3 [19.8;23.3] | 22.9 [19.7;24.6] | 24.3 [23.1;25.9] | 45.7 [38.3;49.3] | 42.3 [37.3;46.9] | 38.9 [37.1;45.9] | 22.8 [21.5;23.6] | <0.001 |
| Variables | AN0 | AN1 | BN | BED | UFED | OSFED | p-Value |
|---|---|---|---|---|---|---|---|
| Secondary Amenorrhea: | <0.001 | ||||||
| No | 10.5 | 36.8 | 37.5 | 47.4 | 37.5 | 50.0 | |
| Yes | 89.5 | 63.2 | 62.5 | 10.5 | 18.8 | 30.0 | |
| Menopause | 0.00 | 0.00 | 0.00 | 42.1 | 43.8 | 20.0 | |
| Food restriction: | <0.001 | ||||||
| No | 0.00 | 0.00 | 5.56 | 36.0 | 40.0 | 33.3 | |
| Yes | 100 | 100 | 94.4 | 64.0 | 60.0 | 66.7 | |
| Water restriction: | <0.001 | ||||||
| No | 45.5 | 47.6 | 66.7 | 84.0 | 90.0 | 91.7 | |
| Yes | 54.5 | 52.4 | 33.3 | 16.0 | 10.0 | 8.33 | |
| Fasting: | <0.001 | ||||||
| No | 22.7 | 20.0 | 16.7 | 73.1 | 80.0 | 83.3 | |
| Yes | 77.3 | 80.0 | 83.3 | 26.9 | 20.0 | 16.7 | |
| Diets pills: | 0.002 | ||||||
| No | 100 | 78.9 | 94.4 | 73.1 | 85.0 | 83.3 | |
| Yes | 0.00 | 21.1 | 5.56 | 26.9 | 15.0 | 16.7 | |
| Binge eating: | <0.001 | ||||||
| No | 84.1 | 45.0 | 11.1 | 0.00 | 40.0 | 16.7 | |
| Yes | 15.9 | 55.0 | 88.9 | 100 | 60.0 | 83.3 | |
| Vomit: | <0.001 | ||||||
| No | 86.4 | 15.0 | 11.1 | 92.3 | 84.2 | 91.7 | |
| Yes | 13.6 | 85.0 | 88.9 | 7.69 | 15.8 | 8.33 | |
| Alcohol abuse: | 0.112 | ||||||
| No | 95.3 | 88.9 | 75.0 | 92.3 | 100 | 90.9 | |
| Yes | 4.65 | 11.1 | 25.0 | 7.69 | 0.00 | 9.09 | |
| Laxatives abuse: | 0.008 | ||||||
| No | 93.2 | 65.0 | 66.7 | 92.3 | 94.7 | 83.3 | |
| Yes | 6.82 | 35.0 | 33.3 | 7.69 | 5.26 | 16.7 | |
| Diuretics abuse: | 0.027 | ||||||
| No | 100 | 84.2 | 88.2 | 96.2 | 100 | 91.7 | |
| Yes | 0.00 | 15.8 | 11.8 | 3.85 | 0.00 | 8.33 | |
| Drugs abuse: | 0.303 | ||||||
| No | 95.5 | 100 | 94.4 | 92.3 | 100 | 83.3 | |
| Yes | 4.55 | 0.00 | 5.56 | 7.69 | 0.00 | 16.7 | |
| Excessive physical activity: | <0.001 | ||||||
| No | 20.5 | 10.0 | 33.3 | 92.3 | 90.0 | 83.3 | |
| Yes | 79.5 | 90.0 | 66.7 | 7.7 | 10.0 | 16.7 | |
| Sleep disorder: | 0.116 | ||||||
| No | 20.0 | 18.2 | 54.5 | 50.0 | 42.9 | 16.7 | |
| Yes | 80.0 | 81.8 | 45.5 | 50.0 | 57.1 | 83.3 | |
| CPAP ventilator: | 0.002 | ||||||
| No | 100.0 | 100.0 | 100.0 | 69.2 | 71.4 | 100.0 | |
| Yes | 0.0 | 0.0 | 0.0 | 30.8 | 28.6 | 0.0 |
| Variables | AN0 | AN1 | BN | BED | UFED | OSFED | p-Value |
|---|---|---|---|---|---|---|---|
| Glycemia, mg/dL | 76.0 [67.8;80.8] | 80.0 [72.2;85.0] | 80.5 [69.8;84.5] | 90.0 [85.0;101] | 96.5 [85.5;104] | 96.0 [87.0;104] | <0.001 |
| Azotemia, mg/dL | 31.8 [25.0;42.0] | 25.5 [20.8;38.2] | 28.4 [23.5;31.8] | 32.0 [29.2;37.5] | 30.0 [27.0;34.5] | 34.0 [27.2;37.0] | 0.690 |
| Creatinine, mg/dL | 0.74 [0.62;0.86] | 0.71 [0.67;0.82] | 0.78 [0.66;0.83] | 0.74 [0.62;0.79] | 0.77 [0.68;0.90] | 0.78 [0.68;0.83] | 0.756 |
| TSH, mU/L | 2.07 [1.42;2.71] | 2.00 [1.55;3.04] | 1.77 [1.34;2.34] | 2.57 [2.05;3.19] | 2.71 [1.81;3.26] | 2.59 [1.94;4.00] | 0.203 |
| Amylasi, U/L | 68.0 [51.5;101] | 84.0 [64.0;104] | 69.5 [55.0;79.2] | 47.0 [33.0;59.0] | 52.0 [37.2;65.2] | 65.0 [65.0;65.0] | 0.126 |
| WBCs, ×03/uL | 5.19 [3.90;6.10] | 5.14 [4.72;6.88] | 6.19 [5.00;7.10] | 8.22 [7.12;9.00] | 7.18 [6.16;8.34] | 6.97 [6.17;8.18] | <0.001 |
| RBCs, ×06/uL | 4.20 [3.90;4.72] | 4.43 [4.14;4.47] | 4.42 [4.30;4.78] | 4.90 [4.73;5.12] | 4.82 [4.62;5.24] | 4.73 [4.64;5.08] | <0.001 |
| PLT, ×03/uL | 214 [181;238] | 221 [200;292] | 245 [212;302] | 273 [249;312] | 260 [221;287] | 254 [226;296] | <0.001 |
| Hb, g/dL | 13.2 [12.4;14.1] | 13.3 [12.7;13.7] | 13.4 [12.1;13.8] | 14.1 [13.0;14.7] | 13.3 [12.4;14.8] | 13.7 [13.2;14.1] | 0.270 |
| Ht, vol% | 38.7 [37.1;41.6] | 39.6 [37.5;40.9] | 39.5 [38.1;41.2] | 43.2 [40.8;44.4] | 40.5 [37.8;43.8] | 40.5 [39.8;42.9] | 0.001 |
| MCV, fL | 90.8 [87.2;94.8] | 89.4 [88.4;91.6] | 87.6 [85.3;91.7] | 87.0 [83.8;89.1] | 84.6 [80.6;88.0] | 85.8 [82.8;89.9] | 0.002 |
| Serum protein electrophoresis, g/dL | 7.30 [6.85;7.75] | 7.30 [7.20;7.60] | 7.40 [7.00;7.65] | 7.00 [6.82;7.58] | 7.05 [6.95;7.15] | 7.30 [7.30;7.30] | 0.814 |
| Variables | AN0 (a) | AN1 (b) | BN (c) | BED (d) | UFED (e) | OSFED (f) | CTR (*) | p-Value |
|---|---|---|---|---|---|---|---|---|
| Kyn, µmol/L | 1.35 [1.07;1.57] (d) (e) (f) | 1.25 [1.09;1.46] (d) (e) (f) | 1.40 [1.06;1.72] (d) (e) (f) | 1.97 [1.60;2.35] (*) | 1.64 [1.45;2.21] (*) | 2.22 [1.90;2.34] (*) | 1.37 [1.11;1.58] | <0.001 |
| Trp, µmol/L | 50.2 [42.4;53.9] (d) (e) (f) | 50.7 [45.8;58.0] (*) (d) (e) (f) | 50.6 [46.2;58.4] (*) (d) (e) (f) | 41.0 [35.2;47.0] (*) | 43.7 [36.0;46.5] | 40.6 [36.3;46.1] | 45.8 [42.2;49.5] | <0.001 |
| Kyn/Trp, * 1000 | 25.5 [20.3;31.6] (d) (e) (f) | 25.6 [20.8;28.4] (*) (d) (e) (f) | 26.1 [23.6;30.1] (d) (e) (f) | 42.6 [36.8;54.3] (*) | 42.5 [33.8;50.5] (*) | 51.8 [42.6;60.6] (*) | 28.7 [25.4;34.2] | <0.001 |
| SLC6A4 CpG1% | 2.03 [1.69;2.91] | 2.24 [1.83;2.69] | 3.18 [2.02;4.26] | 2.37 [1.89;3.46] | 2.44 [1.95;3.59] | 2.10 [1.58;2.27] | 2.32 [1.83;4.16] | 0.230 |
| SLC6A4 CpG2% | 6.04 [5.09;7.40] | 7.17 [4.32;9.65] | 6.33 [4.99;7.82] | 6.10 [4.83;7.94] | 5.36 [4.46;7.18] | 5.00 [3.66;7.07] | 7.31 [5.70;9.22] | 0.270 |
| SLC6A4 CpG3%, | 2.40 [1.81;2.77] | 2.68 [1.71;3.47] | 2.17 [1.86;2.94] | 2.42 [2.07;3.14] | 2.75 [1.68;3.58] | 1.70 [0.00;2.58] | 2.91 [2.15;3.66] | 0.121 |
| SLC6A4 CpG4% | 3.51 [2.71;4.53] | 4.81 [3.63;5.56] | 3.97 [3.34;4.59] | 4.63 [3.20;5.82] | 4.34 [3.61;5.05] | 4.33 [3.29;5.13] | 4.89 [3.84;5.58] | 0.127 |
| SLC6A4 CpG5% | 0.00 [0.00;2.42] (d) | 1.75 [0.00;2.28] | 0.00 [0.00;2.51] | 2.70 [0.91;3.47] | 2.18 [1.68;3.05] | 0.91 [0.00;2.56] | 2.21 [1.58;2.66] | 0.021 |
| SLC6A4 CpG6% | 0.00 [0.00;2.50] (*) | 1.38 [0.00;3.05] | 2.21 [0.00;3.55] | 2.81 [0.00;3.41] | 2.08 [0.00;3.09] | 0.00 [0.00;3.13] | 2.93 [2.00;3.82] | 0.025 |
| Mean Methylation% | 2.56 [2.20;3.22] (*) | 3.35 [2.37;4.27] | 3.25 [2.41;4.03] | 3.55 [2.60;4.46] | 3.09 [2.17;4.14] | 2.78 [2.01;3.05] | 3.87 [3.17;4.60] | 0.008 |
| EDI Variables | AN0 | AN1 | BN | BED | UFED | OSFED | p-Value |
|---|---|---|---|---|---|---|---|
| DT | 26.0 [22.0;28.0] | 28.0 [25.5;28.0] | 28.0 [21.0;28.0] | 15.0 [10.0;21.0] | 17.0 [11.0;21.0] | 16.0 [6.00;20.0] | <0.001 |
| B | 4.00 [1.00;5.00] | 7.00 [4.00;14.0] | 21.0 [7.00;22.0] | 16.0 [9.00;20.0] | 8.00 [4.00;11.0] | 10.0 [5.00;15.0] | <0.001 |
| BD | 32.0 [24.0;36.0] | 36.0 [33.5;38.0] | 34.0 [29.0;38.0] | 28.0 [22.0;33.0] | 28.0 [20.0;32.0] | 26.0 [16.0;31.0] | 0.006 |
| EDCR | 60.0 [44.0;69.0] | 70.0 [65.0;75.0] | 85.0 [60.0;88.0] | 57.0 [47.0;71.0] | 54.0 [38.0;60.0] | 56.0 [44.0;65.0] | 0.001 |
| LSE | 19.0 [17.0;21.0] | 17.0 [13.0;19.5] | 18.0 [16.0;23.0] | 10.0 [8.00;16.0] | 8.00 [4.00;17.5] | 9.00 [6.00;15.0] | <0.001 |
| PA | 17.0 [14.0;21.0] | 18.0 [10.0;21.5] | 21.0 [14.0;24.0] | 9.00 [7.00;13.0] | 8.00 [4.50;15.0] | 9.00 [6.00;14.0] | <0.001 |
| II | 17.0 [10.0;19.0] | 16.0 [14.5;21.5] | 16.0 [12.0;19.0] | 11.0 [6.00;16.0] | 10.0 [4.50;16.0] | 11.0 [6.00;13.0] | 0.001 |
| IA | 13.0 [11.0;18.0] | 12.0 [10.0;17.0] | 15.0 [14.0;20.0] | 9.00 [7.00;12.0] | 9.00 [6.50;11.5] | 10.0 [6.00;13.0] | 0.001 |
| ID | 22.0 [18.0;30.0] | 24.0 [18.0;29.5] | 23.0 [17.0;25.0] | 14.0 [7.00;18.0] | 10.0 [6.00;17.0] | 14.0 [4.00;18.0] | <0.001 |
| ED | 13.0 [10.0;17.0] | 15.0 [11.0;16.0] | 16.0 [11.2;20.2] | 6.00 [3.00;12.0] | 6.00 [2.50;10.0] | 3.00 [1.00;4.00] | <0.001 |
| P | 11.0 [7.00;14.0] | 11.0 [8.00;14.5] | 11.0 [8.00;19.0] | 10.0 [5.00;11.0] | 4.00 [2.00;9.50] | 5.00 [4.00;12.0] | 0.006 |
| A | 15.0 [11.0;20.0] | 16.0 [12.0;18.5] | 14.0 [12.0;21.0] | 9.00 [5.00;14.0] | 6.50 [4.00;10.0] | 9.00 [6.00;13.0] | <0.001 |
| MF | 16.0 [14.0;25.0] | 16.0 [11.2;21.5] | 11.0 [7.00;19.0] | 9.00 [7.00;15.0] | 13.0 [10.5;16.0] | 12.0 [7.00;21.0] | 0.022 |
| IC | 37.0 [29.0;41.0] | 34.0 [27.0;40.5] | 40.0 [28.0;46.0] | 21.0 [15.0;31.0] | 15.0 [9.50;35.5] | 19.0 [11.0;28.0] | <0.001 |
| IPC | 28.0 [23.0;37.0] | 27.0 [25.5;38.5] | 31.0 [27.0;36.0] | 22.0 [13.0;25.0] | 20.0 [12.0;25.5] | 23.0 [13.0;25.0] | <0.001 |
| APC | 33.0 [25.0;46.5] | 39.0 [30.0;45.0] | 38.5 [31.5;46.2] | 17.0 [12.0;33.0] | 14.0 [10.5;27.0] | 14.0 [7.00;19.0] | <0.001 |
| OC | 27.0 [19.0;33.0] | 26.0 [22.0;32.0] | 26.0 [22.0;40.0] | 16.0 [14.0;26.0] | 12.0 [7.50;16.0] | 16.0 [11.0;22.0] | <0.001 |
| GPM | 148 [114;166] | 153 [121;171] | 161 [133;166] | 96.0 [66.2;114] | 73.0 [50.0;115] | 62.5 [54.8;112] | <0.001 |
| IN | 10.5 [7.75;14.0] | 10.5 [8.25;11.8] | 5.00 [3.00;10.0] | 12.0 [8.00;15.0] | 9.00 [8.00;14.5] | 8.00 [7.00;12.5] | 0.113 |
| IF | 1.00 [1.00;3.00] | 1.00 [0.00;2.00] | 1.00 [1.00;3.00] | 0.00 [0.00;1.00] | 1.00 [0.00;1.00] | 0.00 [0.00;1.00] | 0.045 |
| NI | 28.0 [13.5;41.5] | 25.0 [16.5;37.8] | 46.0 [30.0;49.0] | 13.0 [8.00;22.0] | 11.0 [6.50;25.0] | 12.0 [8.00;18.0] | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franzago, M.; Orecchini, E.; Porreca, A.; Mondanelli, G.; Orabona, C.; Dalla Ragione, L.; Di Nicola, M.; Stuppia, L.; Vitacolonna, E.; Beccari, T.; et al. SLC6A4 DNA Methylation Levels and Serum Kynurenine/Tryptophan Ratio in Eating Disorders: A Possible Link with Psychopathological Traits? Nutrients 2023, 15, 406. https://doi.org/10.3390/nu15020406
Franzago M, Orecchini E, Porreca A, Mondanelli G, Orabona C, Dalla Ragione L, Di Nicola M, Stuppia L, Vitacolonna E, Beccari T, et al. SLC6A4 DNA Methylation Levels and Serum Kynurenine/Tryptophan Ratio in Eating Disorders: A Possible Link with Psychopathological Traits? Nutrients. 2023; 15(2):406. https://doi.org/10.3390/nu15020406
Chicago/Turabian StyleFranzago, Marica, Elena Orecchini, Annamaria Porreca, Giada Mondanelli, Ciriana Orabona, Laura Dalla Ragione, Marta Di Nicola, Liborio Stuppia, Ester Vitacolonna, Tommaso Beccari, and et al. 2023. "SLC6A4 DNA Methylation Levels and Serum Kynurenine/Tryptophan Ratio in Eating Disorders: A Possible Link with Psychopathological Traits?" Nutrients 15, no. 2: 406. https://doi.org/10.3390/nu15020406
APA StyleFranzago, M., Orecchini, E., Porreca, A., Mondanelli, G., Orabona, C., Dalla Ragione, L., Di Nicola, M., Stuppia, L., Vitacolonna, E., Beccari, T., & Ceccarini, M. R. (2023). SLC6A4 DNA Methylation Levels and Serum Kynurenine/Tryptophan Ratio in Eating Disorders: A Possible Link with Psychopathological Traits? Nutrients, 15(2), 406. https://doi.org/10.3390/nu15020406