
Exploring the Interrelationships between Diabetes, Nutrition, Anxiety, and Depression: Implications for Treatment and Prevention Strategies


Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Investigating the Effects of Diabetes on Depression Risk
3.2. Examining the Impact of Depression on Diabetes Risk
3.3. The Effects of Diabetes on Anxiety Risk
3.4. The Effects of Anxiety on Diabetes Risk
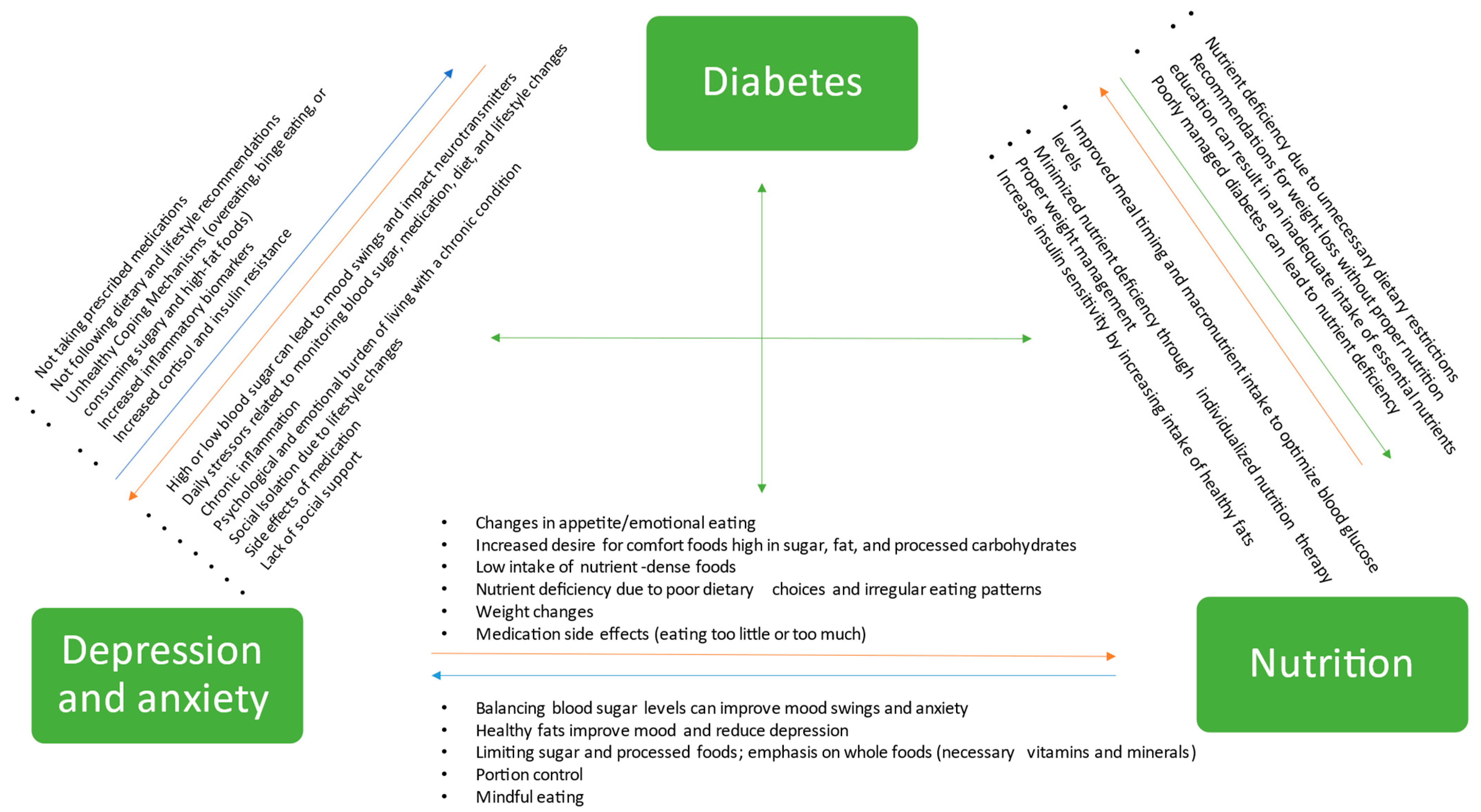
3.5. Exploring the Role of Nutrition in Preventing and Managing Diabetes, Depression, and Anxiety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Diabetes Federation—Home. Available online: https://www.idf.org/ (accessed on 9 October 2022).
- CDC Prediabetes: You Could Be That 1 in 3. Available online: https://www.cdc.gov/diabetes/library/features/prediabetes-1-in-3.html (accessed on 9 October 2022).
- Saeedi:, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and Regional Diabetes Prevalence Estimates for 2019 and Projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th Edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed]
- Mental Disorders. Available online: https://www.who.int/news-room/fact-sheets/detail/mental-disorders (accessed on 11 November 2022).
- Stevanovic, D.; Habtewold, T.; Niksić, A.; Avicena, M.; Mehta, G.; Popović, L.; Erić, A.; Ristic, S.; Ćurković, K.; Bježančević, M.; et al. Anxiety and Depressive Disorders in Diabetes. In Sadikot’s International Textbook of Diabetes; JAYPEE: Noida, India, 2019; pp. 823–828. ISBN 978-93-5270-032-5. [Google Scholar]
- Doctors with Africa CUAMM. redazione_adm Diabetes in Low Income Countries: Drugs or Education? Doctors with Africa CUAMM: Padova, Italy, 2017. [Google Scholar]
- Bădescu, S.; Tătaru, C.; Kobylinska, L.; Georgescu, E.; Zahiu, D.; Zăgrean, A.; Zăgrean, L. The Association between Diabetes Mellitus and Depression. J. Med. Life 2016, 9, 120–125. [Google Scholar] [PubMed]
- Geiker, N.R.W.; Astrup, A.; Hjorth, M.F.; Sjödin, A.; Pijls, L.; Markus, C.R. Does Stress Influence Sleep Patterns, Food Intake, Weight Gain, Abdominal Obesity and Weight Loss Interventions and Vice Versa? Obes. Rev. 2018, 19, 81–97. [Google Scholar] [CrossRef] [PubMed]
- Gangwisch, J.E.; Hale, L.; Garcia, L.; Malaspina, D.; Opler, M.G.; Payne, M.E.; Rossom, R.C.; Lane, D. High Glycemic Index Diet as a Risk Factor for Depression: Analyses from the Women’s Health Initiative. Am. J. Clin. Nutr. 2015, 102, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.; He, H.; Zhang, Q.; Wu, H.; Du, H.; Liu, L.; Wang, C.; Shi, H.; Xia, Y.; Guo, X.; et al. Soft Drink Consumption Is Associated with Depressive Symptoms among Adults in China. J. Affect. Disord. 2015, 172, 422–427. [Google Scholar] [CrossRef]
- Jeffery, R.W.; Linde, J.A.; Simon, G.E.; Ludman, E.J.; Rohde, P.; Ichikawa, L.E.; Finch, E.A. Reported Food Choices in Older Women in Relation to Body Mass Index and Depressive Symptoms. Appetite 2009, 52, 238–240. [Google Scholar] [CrossRef]
- Macht, M. How Emotions Affect Eating: A Five-Way Model. Appetite 2008, 50, 1–11. [Google Scholar] [CrossRef]
- Calder, P.C.; Ahluwalia, N.; Brouns, F.; Buetler, T.; Clement, K.; Cunningham, K.; Esposito, K.; Jönsson, L.S.; Kolb, H.; Lansink, M.; et al. Dietary Factors and Low-Grade Inflammation in Relation to Overweight and Obesity. Br. J. Nutr. 2011, 106, S1–S78. [Google Scholar] [CrossRef]
- Kivimäki, M.; Shipley, M.J.; Batty, G.D.; Hamer, M.; Akbaraly, T.N.; Kumari, M.; Jokela, M.; Virtanen, M.; Lowe, G.D.; Ebmeier, K.P.; et al. Long-Term Inflammation Increases Risk of Common Mental Disorder: A Cohort Study. Mol. Psychiatry 2014, 19, 149–150. [Google Scholar] [CrossRef]
- Paans, N.P.G.; Gibson-Smith, D.; Bot, M.; van Strien, T.; Brouwer, I.A.; Visser, M.; Penninx, B.W.J.H. Depression and Eating Styles Are Independently Associated with Dietary Intake. Appetite 2019, 134, 103–110. [Google Scholar] [CrossRef]
- Sarlio-Lähteenkorva, S.; Lahelma, E.; Roos, E. Mental Health and Food Habits among Employed Women and Men. Appetite 2004, 42, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Coleman, J. Anxiety and Diabetes. Available online: https://www.thediabetescouncil.com/anxiety-and-diabetes/ (accessed on 10 October 2022).
- Illinois Science Council. Diabetes in Low-Income Communities: Its Causes and Its Solutions; Illinois Science Council: Chicago, IL, USA, 2018. [Google Scholar]
- Stress: Cortisol and Insulin Resistance in El Segundo CA & Marietta GA. Available online: https://holtorfmed.com/articles/hormonal-health/stress-cortisol-and-insulin-resistance (accessed on 10 October 2022).
- Adam, T.C.; Epel, E.S. Stress, Eating and the Reward System. Physiol. Behav. 2007, 91, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Penckofer, S.; Quinn, L.; Byrn, M.; Ferrans, C.; Miller, M.; Strange, P. Does Glycemic Variability Impact Mood and Quality of Life? Diabetes Technol. Ther. 2012, 14, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Oğuz, N. Anxiety and Depression in Diabetic Patients. EJMI 2018, 2, 174–177. [Google Scholar] [CrossRef]
- Tuligenga, R.H.; Dugravot, A.; Tabák, A.G.; Elbaz, A.; Brunner, E.J.; Kivimäki, M.; Singh-Manoux, A. Midlife Type 2 Diabetes and Poor Glycaemic Control as Risk Factors for Cognitive Decline in Early Old Age: A Post-Hoc Analysis of the Whitehall II Cohort Study. Lancet Diabetes Endocrinol. 2014, 2, 228–235. [Google Scholar] [CrossRef]
- Meurs, M.; Roest, A.M.; Wolffenbuttel, B.H.R.; Stolk, R.P.; de Jonge, P.; Rosmalen, J.G.M. Association of Depressive and Anxiety Disorders With Diagnosed Versus Undiagnosed Diabetes: An Epidemiological Study of 90,686 Participants. Psychosom. Med. 2016, 78, 233–241. [Google Scholar] [CrossRef]
- Rajput, R.; Gehlawat, P.; Gehlan, D.; Gupta, R.; Rajput, M. Prevalence and Predictors of Depression and Anxiety in Patients of Diabetes Mellitus in a Tertiary Care Center. Indian J. Endocrinol. Metab. 2016, 20, 746. [Google Scholar] [CrossRef]
- Lindekilde, N.; Rutters, F.; Erik Henriksen, J.; Lasgaard, M.; Schram, M.T.; Rubin, K.H.; Kivimäki, M.; Nefs, G.; Pouwer, F. Psychiatric Disorders as Risk Factors for Type 2 Diabetes: An Umbrella Review of Systematic Reviews with and without Meta-Analyses. Diabetes Res. Clin. Pract. 2021, 176, 108855. [Google Scholar] [CrossRef]
- Bergmans, R.S.; Rapp, A.; Kelly, K.M.; Weiss, D.; Mezuk, B. Understanding the Relationship between Type 2 Diabetes and Depression: Lessons from Genetically Informative Study Designs. Diabet. Med. 2021, 38, e14399. [Google Scholar] [CrossRef]
- Roy, T.; Lloyd, C.E. Epidemiology of Depression and Diabetes: A Systematic Review. J. Affect. Disord. 2012, 142, S8–S21. [Google Scholar] [CrossRef]
- CDC Diabetes and Mental Health. Available online: https://www.cdc.gov/diabetes/managing/mental-health.html (accessed on 27 March 2023).
- Pozzo, M.J.; Mociulsky, J.; Martinez, E.T.; Senatore, G.; Farias, J.M.; Sapetti, A.; Sanzana, M.G.; Gonzalez, P.; Cafferata, A.; Peloche, A.; et al. Diabetes and Quality of Life: Initial Approach to Depression, Physical Activity, and Sexual Dysfunction. Am. J. Ther. 2016, 23, e159–e171. [Google Scholar] [CrossRef] [PubMed]
- Hasan, S.S.; Clavarino, A.M.; Dingle, K.; Mamun, A.A.; Kairuz, T. Diabetes Mellitus and the Risk of Depressive and Anxiety Disorders in Australian Women: A Longitudinal Study. J. Womens Health 2015, 24, 889–898. [Google Scholar] [CrossRef] [PubMed]
- Arshad, A.R.; Alvi, K.Y. Frequency of Depression in Type 2 Diabetes Mellitus and an Analysis of Predictive Factors. J. Pak. Med. Assoc. 2016, 66, 425–429. [Google Scholar]
- Dunlavey, C.J. Introduction to the Hypothalamic-Pituitary-Adrenal Axis: Healthy and Dysregulated Stress Responses, Developmental Stress and Neurodegeneration. J. Undergrad. Neurosci. Educ. 2018, 16, R59–R60. [Google Scholar]
- Chan, O.; Inouye, K.; Riddell, M.C.; Vranic, M.; Matthews, S.G. Diabetes and the Hypothalamo-Pituitary-Adrenal (HPA) Axis. Minerva Endocrinol. 2003, 28, 87–102. [Google Scholar]
- Holt, R.I.G.; de Groot, M.; Golden, S.H. Diabetes and Depression. Curr. Diab. Rep. 2014, 14, 491. [Google Scholar] [CrossRef]
- Gonzalez, J.S.; Peyrot, M.; McCarl, L.A.; Collins, E.M.; Serpa, L.; Mimiaga, M.J.; Safren, S.A. Depression and Diabetes Treatment Nonadherence: A Meta-Analysis. Diabetes Care 2008, 31, 2398–2403. [Google Scholar] [CrossRef] [PubMed]
- Khambaty, T.; Callahan, C.M.; Perkins, A.J.; Stewart, J.C. Depression and Anxiety Screens as Simultaneous Predictors of 10-Year Incidence of Diabetes Mellitus in Older Adults in Primary Care. J. Am. Geriatr. Soc. 2017, 65, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Lustman, P.; Clouse, R. Depression in Diabetic patientsThe Relationship between Mood and Glycemic Control. J. Diabetes Its Complicat. 2005, 19, 113–122. [Google Scholar] [CrossRef]
- Kessler, R.C. The Costs of Depression. Psychiatr. Clin. N. Am. 2012, 35, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Campayo, A.; de Jonge, P.; Roy, J.F.; Saz, P.; de la Cámara, C.; Quintanilla, M.A.; Marcos, G.; Santabárbara, J.; Lobo, A. Depressive Disorder and Incident Diabetes Mellitus: The Effect of Characteristics of Depression. AJP 2010, 167, 580–588. [Google Scholar] [CrossRef]
- Renn, B.N.; Feliciano, L.; Segal, D.L. The Bidirectional Relationship of Depression and Diabetes: A Systematic Review. Clin. Psychol. Rev. 2011, 31, 1239–1246. [Google Scholar] [CrossRef]
- Mezuk, B.; Eaton, W.W.; Albrecht, S.; Golden, S.H. Depression and Type 2 Diabetes Over the Lifespan. Diabetes Care 2008, 31, 2383–2390. [Google Scholar] [CrossRef] [PubMed]
- Katon, W.J.; Russo, J.E.; Heckbert, S.R.; Lin, E.H.B.; Ciechanowski, P.; Ludman, E.; Young, B.; Von Korff, M. The Relationship between Changes in Depression Symptoms and Changes in Health Risk Behaviors in Patients with Diabetes. Int. J. Geriat. Psychiatry 2010, 25, 466–475. [Google Scholar] [CrossRef] [PubMed]
- Golden, S.H.; Lazo, M.; Carnethon, M.; Bertoni, A.G.; Schreiner, P.J.; Roux, A.V.D.; Lee, H.B.; Lyketsos, C. Examining a Bidirectional Association Between Depressive Symptoms and Diabetes. JAMA 2008, 299, 2751–2759. [Google Scholar] [CrossRef]
- Steffensen, C.; Dekkers, O.M.; Lyhne, J.; Pedersen, B.G.; Rasmussen, F.; Rungby, J.; Poulsen, P.L.; Jørgensen, J.O.L. Hypercortisolism in Newly Diagnosed Type 2 Diabetes: A Prospective Study of 384 Newly Diagnosed Patients. Horm. Metab. Res. 2019, 51, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Bao, W.; Liu, J.; OuYang, Y.-Y.; Wang, D.; Rong, S.; Xiao, X.; Shan, Z.-L.; Zhang, Y.; Yao, P.; et al. Inflammatory Markers and Risk of Type 2 Diabetes. Diabetes Care 2013, 36, 166–175. [Google Scholar] [CrossRef]
- Basiri, R.; Spicer, M.; Levenson, C.; Ledermann, T.; Akhavan, N.; Arjmandi, B. Improving Dietary Intake of Essential Nutrients Can Ameliorate Inflammation in Patients with Diabetic Foot Ulcers. Nutrients 2022, 14, 2393. [Google Scholar] [CrossRef]
- Polonsky, W.; Henry, R. Poor Medication Adherence in Type 2 Diabetes: Recognizing the Scope of the Problem and Its Key Contributors. PPA 2016, 10, 1299–1307. [Google Scholar] [CrossRef]
- Rubin, R.R.; Peyrot, M. Psychological Issues and Treatments for People with Diabetes. J. Clin. Psychol. 2001, 57, 457–478. [Google Scholar] [CrossRef]
- Force, I.C.G.T. Global Guideline for Type 2 Diabetes: Recommendations for Standard, Comprehensive, and Minimal Care. Diabet. Med. 2006, 23, 579–593. [Google Scholar] [CrossRef]
- Kaur, G.; Tee, G.H.; Ariaratnam, S.; Krishnapillai, A.S.; China, K. Depression, Anxiety and Stress Symptoms among Diabetics in Malaysia: A Cross Sectional Study in an Urban Primary Care Setting. BMC Fam. Pract. 2013, 14, 69. [Google Scholar] [CrossRef] [PubMed]
- Beckerle, C.M.; Lavin, M.A. Association of Self-Efficacy and Self-Care with Glycemic Control in Diabetes. Diabetes Spectr. 2013, 26, 172–178. [Google Scholar] [CrossRef][Green Version]
- McSharry, J.; Byrne, M.; Casey, B.; Dinneen, S.F.; Fredrix, M.; Hynes, L.; Lake, A.J.; Morrissey, E. Behaviour Change in Diabetes: Behavioural Science Advancements to Support the Use of Theory. Diabet. Med. 2020, 37, 455–463. [Google Scholar] [CrossRef]
- The ACE/ADA Task Force on Inpatient Diabetes. American College of Endocrinology and American Diabetes Association Consensus Statement on Inpatient Diabetes and Glycemic Control. Diabetes Care 2006, 29, 1955–1962. [Google Scholar] [CrossRef]
- Pouwer, F. Should We Screen for Emotional Distress in Type 2 Diabetes Mellitus? Nat. Rev. Endocrinol. 2009, 5, 665–671. [Google Scholar] [CrossRef]
- Khuwaja, A.K.; Lalani, S.; Dhanani, R.; Azam, I.S.; Rafique, G.; White, F. Anxiety and Depression among Outpatients with Type 2 Diabetes: A Multi-Centre Study of Prevalence and Associated Factors. Diabetol. Metab. Syndr. 2010, 2, 72. [Google Scholar] [CrossRef]
- Huang, C.-J.; Wang, S.-Y.; Lee, M.-H.; Chiu, H.-C. Prevalence and Incidence of Mental Illness in Diabetes: A National Population-Based Cohort Study. Diabetes Res. Clin. Pract. 2011, 93, 106–114. [Google Scholar] [CrossRef]
- Svenningsson, I.; Björkelund, C.; Marklund, B.; Gedda, B. Anxiety and Depression in Obese and Normal-Weight Individuals with Diabetes Type 2: A Gender Perspective. Scand. J. Caring Sci. 2012, 26, 349–354. [Google Scholar] [CrossRef]
- AlBekairy, A.; AbuRuz, S.; Alsabani, B.; Alshehri, A.; Aldebasi, T.; Alkatheri, A.; Almodaimegh, H. Exploring Factors Associated with Depression and Anxiety among Hospitalized Patients with Type 2 Diabetes Mellitus. MPP 2017, 26, 547–553. [Google Scholar] [CrossRef]
- Al-Hayek, A.A.; Robert, A.A.; Alzaid, A.A.; Nusair, H.M.; Zbaidi, N.S.; Al-Eithan, M.H.; Sam, A.E. Association between Diabetes Self-Care, Medication Adherence, Anxiety, Depression, and Glycemic Control in Type 2 Diabetes. Saudi Med. J. 2012, 33, 681–683. [Google Scholar] [PubMed]
- Khowaja, L.A.; Khuwaja, A.K.; Cosgrove, P. Cost of Diabetes Care in Out-Patient Clinics of Karachi, Pakistan. BMC Health Serv. Res. 2007, 7, 189. [Google Scholar] [CrossRef]
- Lin, E.H.B.; Rutter, C.M.; Katon, W.; Heckbert, S.R.; Ciechanowski, P.; Oliver, M.M.; Ludman, E.J.; Young, B.A.; Williams, L.H.; McCulloch, D.K.; et al. Depression and Advanced Complications of Diabetes. Diabetes Care 2010, 33, 264–269. [Google Scholar] [CrossRef]
- Smith, K.J.; Béland, M.; Clyde, M.; Gariépy, G.; Pagé, V.; Badawi, G.; Rabasa-Lhoret, R.; Schmitz, N. Association of Diabetes with Anxiety: A Systematic Review and Meta-Analysis. J. Psychosom. Res. 2013, 74, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Wiltink, J.; Beutel, M.E.; Till, Y.; Ojeda, F.M.; Wild, P.S.; Münzel, T.; Blankenberg, S.; Michal, M. Prevalence of Distress, Comorbid Conditions and Well Being in the General Population. J. Affect. Disord. 2011, 130, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Chien, I.-C.; Lin, C.-H. Increased Risk of Diabetes in Patients with Anxiety Disorders: A Population-Based Study. J. Psychosom. Res. 2016, 86, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Kautzky-Willer, A.; Harreiter, J.; Pacini, G. Sex and Gender Differences in Risk, Pathophysiology and Complications of Type 2 Diabetes Mellitus. Endocr. Rev. 2016, 37, 278–316. [Google Scholar] [CrossRef]
- Demmer, R.T.; Gelb, S.; Suglia, S.F.; Keyes, K.M.; Aiello, A.E.; Colombo, P.C.; Galea, S.; Uddin, M.; Koenen, K.C.; Kubzansky, L.D. Sex Differences in the Association between Depression, Anxiety, and Type 2 Diabetes Mellitus. Psychosom. Med. 2015, 77, 467–477. [Google Scholar] [CrossRef]
- Altemus, M.; Sarvaiya, N.; Neill Epperson, C. Sex Differences in Anxiety and Depression Clinical Perspectives. Front. Neuroendocrinol. 2014, 35, 320–330. [Google Scholar] [CrossRef]
- Engum, A. The Role of Depression and Anxiety in Onset of Diabetes in a Large Population-Based Study. J. Psychosom. Res. 2007, 62, 31–38. [Google Scholar] [CrossRef]
- Randler, C.; Desch, I.H.; Otte im Kampe, V.; Wüst-Ackermann, P.; Wilde, M.; Prokop, P. Anxiety, Disgust and Negative Emotions Influence Food Intake in Humans. Int. J. Gastron. Food Sci. 2017, 7, 11–15. [Google Scholar] [CrossRef][Green Version]
- Verma, S.; Hussain, M.E. Obesity and Diabetes: An Update. Diabetes Metab. Syndr. Clin. Res. Rev. 2017, 11, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Pandit, A.U.; Bailey, S.C.; Curtis, L.M.; Seligman, H.K.; Davis, T.C.; Parker, R.M.; Schillinger, D.; DeWalt, D.; Fleming, D.; Mohr, D.C.; et al. Disease-Related Distress, Self-Care and Clinical Outcomes among Low-Income Patients with Diabetes. J. Epidemiol. Community Health 2014, 68, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Tovilla-Zárate, C.; Juárez-Rojop, I.; Jimenez, Y.P.; Jiménez, M.A.; Vázquez, S.; Bermúdez-Ocaña, D.; Ramón-Frías, T.; Mendoza, A.D.G.; García, S.P.; Narváez, L.L. Prevalence of Anxiety and Depression among Outpatients with Type 2 Diabetes in the Mexican Population. PLoS ONE 2012, 7, e36887. [Google Scholar] [CrossRef] [PubMed]
- Collins, M.M.; Corcoran, P.; Perry, I.J. Anxiety and Depression Symptoms in Patients with Diabetes. Diabet. Med. 2009, 26, 153–161. [Google Scholar] [CrossRef]
- Shaban, M.C.; Fosbury, J.; Kerr, D.; Cavan, D.A. The Prevalence of Depression and Anxiety in Adults with Type 1 Diabetes. Diabet. Med. 2006, 23, 1381–1384. [Google Scholar] [CrossRef]
- Iversen, M.M.; Tell, G.S.; Espehaug, B.; Midthjell, K.; Graue, M.; Rokne, B.; Berge, L.I.; Østbye, T. Is Depression a Risk Factor for Diabetic Foot Ulcers? 11-Years Follow-up of the Nord-Trøndelag Health Study (HUNT). J. Diabetes Its Complicat. 2015, 29, 20–25. [Google Scholar] [CrossRef]
- Smith, K.J.; Deschênes, S.S.; Schmitz, N. Investigating the Longitudinal Association between Diabetes and Anxiety: A Systematic Review and Meta-Analysis. Diabet. Med. 2018, 35, 677–693. [Google Scholar] [CrossRef] [PubMed]
- Grajek, M.; Krupa-Kotara, K.; Białek-Dratwa, A.; Sobczyk, K.; Grot, M.; Kowalski, O.; Staśkiewicz, W. Nutrition and Mental Health: A Review of Current Knowledge about the Impact of Diet on Mental Health. Front. Nutr. 2022, 9, 943998. [Google Scholar] [CrossRef]
- Solomou, S.; Logue, J.; Reilly, S.; Perez-Algorta, G. A Systematic Review of the Association of Diet Quality with the Mental Health of University Students: Implications in Health Education Practice. Health Educ. Res. 2023, 38, 28–68. [Google Scholar] [CrossRef]
- O’Neil, A.; Quirk, S.E.; Housden, S.; Brennan, S.L.; Williams, L.J.; Pasco, J.A.; Berk, M.; Jacka, F.N. Relationship Between Diet and Mental Health in Children and Adolescents: A Systematic Review. Am. J. Public Health 2014, 104, e31–e42. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B.; van Dam, R.M.; Liu, S. Diet and Risk of Type II Diabetes: The Role of Types of Fat and Carbohydrate. Diabetologia 2001, 44, 805–817. [Google Scholar] [CrossRef] [PubMed]
- Tseng, T.-S.; Lin, W.-T.; Gonzalez, G.V.; Kao, Y.-H.; Chen, L.-S.; Lin, H.-Y. Sugar Intake from Sweetened Beverages and Diabetes: A Narrative Review. World J. Diabetes 2021, 12, 1530–1538. [Google Scholar] [CrossRef]
- Basiri, R.; Spicer, M.T.; Levenson, C.W.; Ormsbee, M.J.; Ledermann, T.; Arjmandi, B.H. Nutritional Supplementation Concurrent with Nutrition Education Accelerates the Wound Healing Process in Patients with Diabetic Foot Ulcers. Biomedicines 2020, 8, 263. Available online: https://pubmed.ncbi.nlm.nih.gov/32756299/ (accessed on 1 November 2020). [CrossRef] [PubMed]
- Akhavan, N.S.; Pourafshar, S.; Johnson, S.A.; Foley, E.M.; George, K.S.; Munoz, J.; Siebert, S.; Clark, E.A.; Basiri, R.; Hickner, R.C.; et al. The Relationship between Protein Intake and Source on Factors Associated with Glycemic Control in Individuals with Prediabetes and Type 2 Diabetes. Nutrients 2020, 12, 2031. Available online: https://pubmed.ncbi.nlm.nih.gov/32650580/ (accessed on 3 August 2020). [CrossRef]
- Basiri, R.; Spicer, M.; Munoz, J.; Arjmandi, B. Nutritional Intervention Improves the Dietary Intake of Essential Micronutrients in Patients with Diabetic Foot Ulcers. Curr. Dev. Nutr. 2020, 4, 8. [Google Scholar] [CrossRef]
- Nutrition Supplementation and Education May Increase the Healing Rate in Diabetic Patients with Foot Ulcers (P19-005-19)|Current Developments in Nutrition|Oxford Academic. Available online: https://academic.oup.com/cdn/article/3/Supplement_1/nzz049.P19-005-19/5518126 (accessed on 26 April 2023).
- Basiri, R.; Spicer, M.T.; Ledermann, T.; Arjmandi, B.H. Effects of Nutrition Intervention on Blood Glucose, Body Composition, and Phase Angle in Obese and Overweight Patients with Diabetic Foot Ulcers. Nutrients 2022, 14, 3564. [Google Scholar] [CrossRef]
- Martín-Peláez, S.; Fito, M.; Castaner, O. Mediterranean Diet Effects on Type 2 Diabetes Prevention, Disease Progression, and Related Mechanisms. A Review. Nutrients 2020, 12, 2236. [Google Scholar] [CrossRef]
- Sluik, D.; Brouwer-Brolsma, E.M.; Berendsen, A.A.M.; Mikkilä, V.; Poppitt, S.D.; Silvestre, M.P.; Tremblay, A.; Pérusse, L.; Bouchard, C.; Raben, A.; et al. Protein Intake and the Incidence of Pre-Diabetes and Diabetes in 4 Population-Based Studies: The PREVIEW Project. Am. J. Clin. Nutr. 2019, 109, 1310–1318. [Google Scholar] [CrossRef]
- Ke, Q.; Chen, C.; He, F.; Ye, Y.; Bai, X.; Cai, L.; Xia, M. Association between Dietary Protein Intake and Type 2 Diabetes Varies by Dietary Pattern. Diabetol. Metab. Syndr. 2018, 10, 48. [Google Scholar] [CrossRef]
- Han, Y.; Cheng, B.; Guo, Y.; Wang, Q.; Yang, N.; Lin, P. A Low-Carbohydrate Diet Realizes Medication Withdrawal: A Possible Opportunity for Effective Glycemic Control. Front. Endocrinol. Lausanne 2021, 12, 779636. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, J.Z.; Day, A.; Brinkworth, G.D.; Sato, J.; Yamada, S.; Jönsson, T.; Beardsley, J.; Johnson, J.A.; Thabane, L.; Johnston, B.C. Efficacy and Safety of Low and Very Low Carbohydrate Diets for Type 2 Diabetes Remission: Systematic Review and Meta-Analysis of Published and Unpublished Randomized Trial Data. BMJ 2021, 372, m4743. [Google Scholar] [CrossRef] [PubMed]
- Jennings, L.; Basiri, R. Amino Acids, B Vitamins, and Choline May Independently and Collaboratively Influence the Incidence and Core Symptoms of Autism Spectrum Disorder. Nutrients 2022, 14, 2896. Available online: https://www.mdpi.com/2072-6643/14/14/2896 (accessed on 26 April 2023). [CrossRef]
- Sadeghi, O.; Keshteli, A.H.; Afshar, H.; Esmaillzadeh, A.; Adibi, P. Adherence to Mediterranean Dietary Pattern Is Inversely Associated with Depression, Anxiety and Psychological Distress. Nutr. Neurosci. 2021, 24, 248–259. [Google Scholar] [CrossRef]
- Chen, L.; Liu, B.; Ren, L.; Du, H.; Fei, C.; Qian, C.; Li, B.; Zhang, R.; Liu, H.; Li, Z.; et al. High-Fiber Diet Ameliorates Gut Microbiota, Serum Metabolism and Emotional Mood in Type 2 Diabetes Patients. Front. Cell. Infect. Microbiol. 2023, 13, 1069954. [Google Scholar] [CrossRef]
- Sheikhi, A.; Siassi, F.; Djazayery, A.; Guilani, B.; Azadbakht, L. Plant and Animal Protein Intake and Its Association with Depression, Anxiety, and Stress among Iranian Women. BMC Public Health 2023, 23, 161. [Google Scholar] [CrossRef]
- Mazaherioun, M.; Saedisomeolia, A.; Javanbakht, M.H.; Koohdani, F.; Zarei, M.; Ansari, S.; Khoshkhoo Bazargani, F.; Djalali, M. Long Chain N-3 Fatty Acids Improve Depression Syndrome in Type 2 Diabetes Mellitus. Iran J. Public Health 2018, 47, 575–583. [Google Scholar]
- Zheng, L.; Sun, J.; Yu, X.; Zhang, D. Ultra-Processed Food Is Positively Associated with Depressive Symptoms Among United States Adults. Front. Nutr. 2020, 7, 600449. [Google Scholar] [CrossRef]
- Silva, S.A.; do Carmo, A.S.; Carvalho, K.M.B. Lifestyle Patterns Associated with Common Mental Disorders in Brazilian Adolescents: Results of the Study of Cardiovascular Risks in Adolescents (ERICA). PLoS ONE 2021, 16, e0261261. [Google Scholar] [CrossRef] [PubMed]
- Lane, M.M.; Gamage, E.; Travica, N.; Dissanayaka, T.; Ashtree, D.N.; Gauci, S.; Lotfaliany, M.; O’Neil, A.; Jacka, F.N.; Marx, W. Ultra-Processed Food Consumption and Mental Health: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2022, 14, 2568. [Google Scholar] [CrossRef]
- Basiri, R.; Seidu, B.; Cheskin, L.J. Key Nutrients for Optimal Blood Glucose Control and Mental Health in Individuals with Diabetes: A Review of the Evidence. Nutrients 2023, 15, 3929. [Google Scholar] [CrossRef] [PubMed]
- Parletta, N.; Zarnowiecki, D.; Cho, J.; Wilson, A.; Bogomolova, S.; Villani, A.; Itsiopoulos, C.; Niyonsenga, T.; Blunden, S.; Meyer, B.; et al. A Mediterranean-Style Dietary Intervention Supplemented with Fish Oil Improves Diet Quality and Mental Health in People with Depression: A Randomized Controlled Trial (HELFIMED). Nutr. Neurosci. 2019, 22, 474–487. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Villegas, A.; Cabrera-Suárez, B.; Molero, P.; González-Pinto, A.; Chiclana-Actis, C.; Cabrera, C.; Lahortiga-Ramos, F.; Florido-Rodríguez, M.; Vega-Pérez, P.; Vega-Pérez, R.; et al. Preventing the Recurrence of Depression with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil. The PREDI-DEP Trial: Study Protocol. BMC Psychiatry 2019, 19, 63. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Study Design | Population | Results |
|---|---|---|---|
| Rajput et al., 2016 [25] | Cross-sectional, case–control study design. | Diabetes, n = 410 Healthy control, n = 410 | There were twice as many cases of depression and anxiety in those with T2DM compared with healthy controls (26.3% vs. 11.2%). |
| Tovilla-Zarete et al., 2012 [73] | Cross-sectional, multi-center study | Diabetes, n = 820 | 48.27% were positive for depression while 55.10% showed symptoms of anxiety. Occupation and complications were associated with anxiety while glucose level and complications were correlated with depression. |
| Collins et al., 2009 [74] | Cross-sectional study | Diabetes, n = 1456 | Patients with diabetes had significant levels of anxiety (32.0%) and depressive symptoms (22.4%). Poor glycaemic control and female gender were risk factors for higher anxiety scores. Older age and a higher socioeconomic status demonstrated a protective effect, resulting in lower scores of anxiety and depression. |
| Shaban et al., 2006 [75] | Cohort | Diabetes, n = 273 | Compared to men, women reported considerably greater mean anxiety levels. HbA1c was positively associated with anxiety and depression. |
| Campayo A. et al., 2010 [40] | longitudinal design | Subjects with depression, n = 379 | Severe, moderate, and untreated depression are all linked to an increased risk of developing type 2 diabetes. Although persistent depression had a greater risk than the rest. |
| Golden S.H. et al., 2008 [44] | Longitudinal cohort study | Analysis 1. participants without type 2 diabetes at baseline with and without depressive symptoms, n = 5201 Analysis 2. participants without depression at baseline with and without type 2 diabetes, n = 4847 | The incidence of diabetes was correlated with baseline depressed symptoms. Impaired fasting glucose and untreated type 2 diabetes were negatively correlated with incident depressive symptoms, while treated type 2 diabetes exhibited a positive association. |
| Iversen et al., 2015 [76] | Cohort | Depression, n = 36,031 | Depression was positively associated with diabetes. |
| Chien I. C & Lin C. H, 2016 [65] | Prospective cohort | subjects had primary and secondary diagnoses of anxiety disorder, n = 766,427 | The prevalence of diabetes among individuals with anxiety disorders was greater than that of the general population. |
| Smith et al., 2018 [77] | Meta-analysis | anxiety, 14 studies (n= 1,760,800) | Substantial positive correlation was shown between baseline anxiety and the incidence of diabetes |
| Khambaty T., 2017 [37] | Cohort | anxiety, n = 2156 | Out of 2156 patients, 558 developed diabetes over a 10-year period. |
| Engum A., 2007 [69] | Prospective population-based study | depression and anxiety, n = 8311 | Individuals with reported baseline symptoms of depression and anxiety were more likely to develop diabetes ten years later. |
| Meurs et al., 2016 [24] | Cohort study | Depression n = 3002 Anxiety n = 9018 Diabetes n = 1781 Undiagnosed diabetes n = 786 | Diabetes was independently linked to depression in both identified and undiagnosed cases. Diabetes diagnosis was independently linked to anxiety but this association was not observed for undiagnosed cases. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Basiri, R.; Seidu, B.; Rudich, M. Exploring the Interrelationships between Diabetes, Nutrition, Anxiety, and Depression: Implications for Treatment and Prevention Strategies. Nutrients 2023, 15, 4226. https://doi.org/10.3390/nu15194226
Basiri R, Seidu B, Rudich M. Exploring the Interrelationships between Diabetes, Nutrition, Anxiety, and Depression: Implications for Treatment and Prevention Strategies. Nutrients. 2023; 15(19):4226. https://doi.org/10.3390/nu15194226
Chicago/Turabian StyleBasiri, Raedeh, Blessing Seidu, and Mark Rudich. 2023. "Exploring the Interrelationships between Diabetes, Nutrition, Anxiety, and Depression: Implications for Treatment and Prevention Strategies" Nutrients 15, no. 19: 4226. https://doi.org/10.3390/nu15194226
APA StyleBasiri, R., Seidu, B., & Rudich, M. (2023). Exploring the Interrelationships between Diabetes, Nutrition, Anxiety, and Depression: Implications for Treatment and Prevention Strategies. Nutrients, 15(19), 4226. https://doi.org/10.3390/nu15194226