
Amino Acids, B Vitamins, and Choline May Independently and Collaboratively Influence the Incidence and Core Symptoms of Autism Spectrum Disorder


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Choline
3.2. B Vitamins
3.3. Amino Acids
3.4. Nutrient Roles
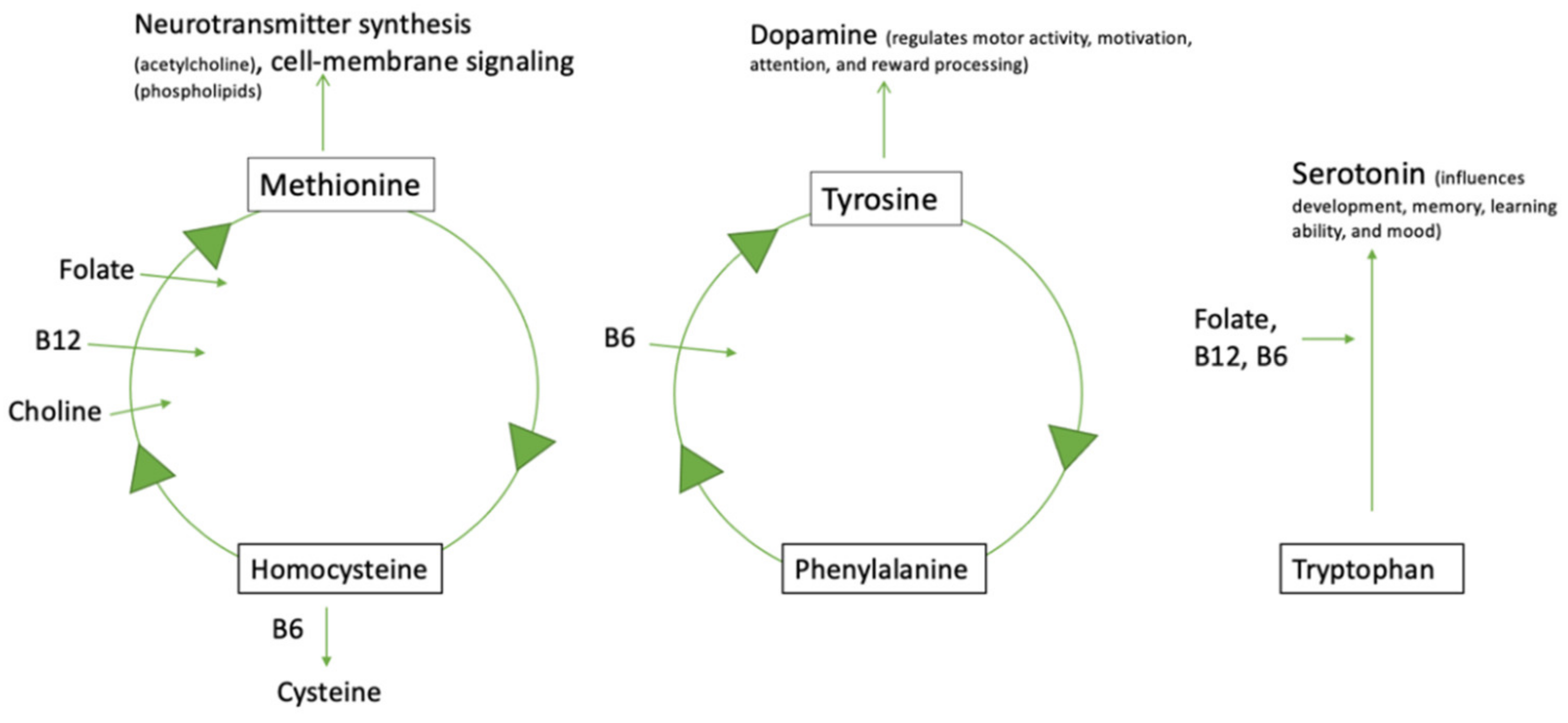
3.5. Interrelationship between B Vitamins, Choline, Amino Acids, and Neurotransmitters
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Data & Statistics on Autism Spectrum Disorder|CDC. Available online: https://www.cdc.gov/ncbddd/autism/data.html (accessed on 31 March 2022).
- Causes. Available online: https://www.autism-society.org/what-is/causes/ (accessed on 5 May 2022).
- Cakir, J.; Frye, R.E.; Walker, S.J. The Lifetime Social Cost of Autism: 1990–2029. Res. Autism Spectr. Disord. 2020, 72, 101502. [Google Scholar] [CrossRef]
- Nierengarten, M.B. Managing Autism Symptoms through Nutrition. Contemp. Pediatrics 2014, 31, 23–27. [Google Scholar]
- Martínez García, R.M.; Jiménez Ortega, A.I.; López Sobaler, A.M.; Ortega, R.M. Nutrition strategies that improve cognitive function. Nutr. Hosp. 2018, 35, 16–19. [Google Scholar] [CrossRef]
- Gabis, L.V.; Ben-Hur, R.; Shefer, S.; Jokel, A.; Shalom, D.B. Improvement of Language in Children with Autism with Combined Donepezil and Choline Treatment. J. Mol. Neurosci. 2019, 69, 224–234. [Google Scholar] [CrossRef] [PubMed]
- Zeisel, S.H.; da Costa, K.-A. Choline: An Essential Nutrient for Public Health. Nutr. Rev. 2009, 67, 615–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olson, A.; Zhang, F.; Cao, H.; Baranova, A.; Slavin, M. In Silico Cholinergic Pathway Analysis Indicates Possible Role for Exogenous Choline in Modulating Sensory Processing in Autism Spectrum Disorder. 2020. Available online: https://figshare.com/articles/poster/In_silico_cholinergic_pathway_analysis_indicates_possible_role_for_exogenous_choline_in_modulating_sensory_processing_in_autism_spectrum_disorder/12150414 (accessed on 5 May 2022). [CrossRef]
- Langley, E.A.; Krykbaeva, M.; Blusztajn, J.K.; Mellott, T.J. High Maternal Choline Consumption during Pregnancy and Nursing Alleviates Deficits in Social Interaction and Improves Anxiety-like Behaviors in the BTBR T+Itpr3tf/J Mouse Model of Autism. Behav. Brain Res. 2015, 278, 210–220. [Google Scholar] [CrossRef]
- Agam, G.; Taylor, Z.; Vainer, E.; Golan, H.M. The Influence of Choline Treatment on Behavioral and Neurochemical Autistic-like Phenotype in Mthfr-Deficient Mice. Transl. Psychiatry 2020, 10, 316. [Google Scholar] [CrossRef] [PubMed]
- Hamlin, J.C.; Pauly, M.; Melnyk, S.; Pavliv, O.; Starrett, W.; Crook, T.A.; James, S.J. Dietary Intake and Plasma Levels of Choline and Betaine in Children with Autism Spectrum Disorders. Autism Res. Treat. 2013, 2013, 578429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kałużna-Czaplińska, J.; Jóźwik-Pruska, J.; Chirumbolo, S.; Bjørklund, G. Tryptophan Status in Autism Spectrum Disorder and the Influence of Supplementation on Its Level. Metab. Brain Dis. 2017, 32, 1585–1593. [Google Scholar] [CrossRef] [Green Version]
- Tardy, A.-L.; Pouteau, E.; Marquez, D.; Yilmaz, C.; Scholey, A. Vitamins and Minerals for Energy, Fatigue and Cognition: A Narrative Review of the Biochemical and Clinical Evidence. Nutrients 2020, 12, 228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dean, L. Methylenetetrahydrofolate Reductase Deficiency. In Medical Genetics Summaries; Pratt, V.M., Scott, S.A., Pirmohamed, M., Esquivel, B., Kane, M.S., Kattman, B.L., Malheiro, A.J., Eds.; National Center for Biotechnology Information (US): Bethesda, MD, USA, 2012. [Google Scholar]
- Dana, H.; Bayramov, K.K.; Delibaşı, N.; Tahtasakal, R.; Bayramov, R.; Hamurcu, Z.; Sener, E.F. Disregulation of Autophagy in the Transgenerational Cc2d1a Mouse Model of Autism. Neuromolecular Med. 2020, 22, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Tang, G.; Gudsnuk, K.; Kuo, S.-H.; Cotrina, M.L.; Rosoklija, G.; Sosunov, A.; Sonders, M.S.; Kanter, E.; Castagna, C.; Yamamoto, A.; et al. Loss of MTOR-Dependent Macroautophagy Causes Autistic-like Synaptic Pruning Deficits. Neuron 2014, 83, 1131–1143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutsler, J.J.; Zhang, H. Increased Dendritic Spine Densities on Cortical Projection Neurons in Autism Spectrum Disorders. Brain Res. 2010, 1309, 83–94. [Google Scholar] [CrossRef] [PubMed]
- Nicolini, C.; Fahnestock, M. The Valproic Acid-Induced Rodent Model of Autism. Exp. Neurol. 2018, 299, 217–227. [Google Scholar] [CrossRef] [PubMed]
- Kwak, J.-H.; Lee, Y.; Jun, M.-H.; Roh, M.; Seo, H.; Lee, J.; Lee, K.; Lee, J.-A. Autophagy Activity Contributes to the Impairment of Social Recognition in Epac2−/− Mice. Mol. Brain 2021, 14, 100. [Google Scholar] [CrossRef] [PubMed]
- Deacon, R.M.J. Digging and Marble Burying in Mice: Simple Methods for in Vivo Identification of Biological Impacts. Nat. Protoc. 2006, 1, 122–124. [Google Scholar] [CrossRef] [PubMed]
- Hunt, A.; Harrington, D.; Robinson, S. Vitamin B12 Deficiency. BMJ 2014, 349, g5226. [Google Scholar] [CrossRef] [PubMed]
- Robea, M.-A.; Luca, A.-C.; Ciobica, A. Relationship between Vitamin Deficiencies and Co-Occurring Symptoms in Autism Spectrum Disorder. Medicina 2020, 56, 245. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.B. Summary of Dietary, Nutritional, and Medical Treatments for Autism–Based on over 150 Published Research Studies. ARI Publ. 2013, 40, 1–53. [Google Scholar]
- Rimland, B. Controversies in the Treatment of Autistic Children: Vitamin and Drug Therapy. J. Child Neurol. 1988, 3, S68–S72. [Google Scholar] [CrossRef]
- Mousain-Bosc, M.; Roche, M.; Polge, A.; Pradal-Prat, D.; Rapin, J.; Bali, J.P. Improvement of Neurobehavioral Disorders in Children Supplemented with Magnesium-Vitamin B6. II. Pervasive Developmental Disorder-Autism. Magnes Res. 2006, 19, 53–62. [Google Scholar] [PubMed]
- Martineau, J.; Barthelemy, C.; Garreau, B.; Lelord, G. Vitamin B6, Magnesium, and Combined B6-Mg: Therapeutic Effects in Childhood Autism. Biol. Psychiatry 1985, 20, 467–478. [Google Scholar] [CrossRef]
- Kennedy, D.O. B Vitamins and the Brain: Mechanisms, Dose and Efficacy-A Review. Nutrients 2016, 8, 68. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, R.J.; Hansen, R.L.; Hartiala, J.; Allayee, H.; Schmidt, L.C.; Tancredi, D.J.; Tassone, F.; Hertz-Picciotto, I. Prenatal Vitamins, One-Carbon Metabolism Gene Variants, and Risk for Autism. Epidemiology 2011, 22, 476. [Google Scholar] [CrossRef] [Green Version]
- Raghavan, R.; Riley, A.W.; Volk, H.; Caruso, D.; Hironaka, L.; Sices, L.; Hong, X.; Wang, G.; Ji, Y.; Brucato, M.; et al. Maternal Multivitamin Intake, Plasma Folate and Vitamin B(12) Levels and Autism Spectrum Disorder Risk in Offspring. Paediatr. Perinat. Epidemiol. 2018, 32, 100–111. [Google Scholar] [CrossRef]
- Steenweg-de Graaff, J.; Ghassabian, A.; Jaddoe, V.W.V.; Tiemeier, H.; Roza, S.J. Folate Concentrations during Pregnancy and Autistic Traits in the Offspring. The Generation R Study. Eur. J. Public Health 2015, 25, 431–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Surén, P.; Roth, C.; Bresnahan, M.; Haugen, M.; Hornig, M.; Hirtz, D.; Lie, K.K.; Lipkin, W.I.; Magnus, P.; Reichborn-Kjennerud, T.; et al. Association between Maternal Use of Folic Acid Supplements and Risk of Autism in Children. JAMA 2013, 309, 570–577. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3908544/ (accessed on 23 March 2022). [CrossRef] [Green Version]
- Hendren, R.L.; James, S.J.; Widjaja, F.; Lawton, B.; Rosenblatt, A.; Bent, S. Randomized, Placebo-Controlled Trial of Methyl B12 for Children with Autism. J. Child Adolesc. Psychopharmacol. 2016, 26, 774–783. [Google Scholar] [CrossRef]
- Wang, T.; Zhang, T.; Sun, L.; Li, W.; Zhang, C.; Yu, L.; Guan, Y. Gestational B-Vitamin Supplementation Alleviates PM2.5-Induced Autism-like Behavior and Hippocampal Neurodevelopmental Impairment in Mice Offspring. Ecotoxicol. Environ. Saf. 2019, 185, 109686. [Google Scholar] [CrossRef]
- Gariballa, S.; Afandi, B.; Abuhaltem, M.; Yasin, J.; Habib, H.; Ibrahim, W. Oxidative Damage and Inflammation in Obese Diabetic Emirati Subjects Supplemented with Antioxidants and B-Vitamins: A Randomized Placebo-Controlled Trail. Nutr. Metab. 2013, 10, 21. [Google Scholar] [CrossRef] [Green Version]
- Calderón-Ospina, C.A.; Nava-Mesa, M.O. B Vitamins in the Nervous System: Current Knowledge of the Biochemical Modes of Action and Synergies of Thiamine, Pyridoxine, and Cobalamin. CNS Neurosci. Ther. 2019, 26, 5–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- 8.14: Vitamins Important for Metabolism. Available online: https://med.libretexts.org/Courses/American_Public_University/APU%3A_Basic_Foundation_of_Nutrition_for_Sports_Performance_(Byerley)/08%3A_Vitaminand_Mineral_Basics%3A_Metabolic_Regulators/8.14%3A_Vitamins_Important_for_Metabolism (accessed on 4 May 2022).
- Saad, K.; Hammad, E.; Abdel-rahman, A.A.; Sobhy, K.M. Autistic Symptoms in Late Diagnosed Phenylketonuric Children in Upper Egypt. J. Neurol. Res. 2013, 3, 122–129. [Google Scholar] [CrossRef]
- Arum, P.; Amareta, D.I.; Zannah, F. Phenylalanine and Tryptophan Intake of Hyperactive Children with Autism. J. Biomed. Transl. Res. 2017, 3, 34–36. [Google Scholar] [CrossRef]
- Neuro-Cognitive Effects of Acute Tyrosine Administration on Reactive and Proactive Response Inhibition in Healthy Older Adults-PMC. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6084775/ (accessed on 13 May 2022).
- Young, S.N. How to Increase Serotonin in the Human Brain without Drugs. J. Psychiatry Neurosci. 2007, 32, 394–399. [Google Scholar] [PubMed]
- Gaspar, P.; Cases, O.; Maroteaux, L. The Developmental Role of Serotonin: News from Mouse Molecular Genetics. Nat. Rev. Neurosci. 2003, 4, 1002–1012. [Google Scholar] [CrossRef]
- Celada, P.; Puig, M.V.; Artigas, F. Serotonin Modulation of Cortical Neurons and Networks. Front. Integr. Neurosci. 2013, 7, 25. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, T.A.; Nguyen, J.C.D.; Polglaze, K.E.; Bertrand, P.P. Influence of Tryptophan and Serotonin on Mood and Cognition with a Possible Role of the Gut-Brain Axis. Nutrients 2016, 8, 56. [Google Scholar] [CrossRef]
- Rose’meyer, R. A Review of the Serotonin Transporter and Prenatal Cortisol in the Development of Autism Spectrum Disorders. Mol. Autism 2013, 4, 37. [Google Scholar] [CrossRef] [Green Version]
- Schultz, W. Dopamine Neurons and Their Role in Reward Mechanisms. Curr. Opin. Neurobiol. 1997, 7, 191–197. [Google Scholar] [CrossRef]
- Nieoullon, A. Dopamine and the Regulation of Cognition and Attention. Prog. Neurobiol. 2002, 67, 53–83. [Google Scholar] [CrossRef]
- Doya, K. Complementary Roles of Basal Ganglia and Cerebellum in Learning and Motor Control. Curr. Opin. Neurobiol. 2000, 10, 732–739. [Google Scholar] [CrossRef]
- Nakamura, K.; Sekine, Y.; Ouchi, Y.; Tsujii, M.; Yoshikawa, E.; Futatsubashi, M.; Tsuchiya, K.J.; Sugihara, G.; Iwata, Y.; Suzuki, K.; et al. Brain Serotonin and Dopamine Transporter Bindings in Adults with High-Functioning Autism. Arch. Gen. Psychiatry 2010, 67, 59–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makkonen, I.; Riikonen, R.; Kokki, H.; Airaksinen, M.M.; Kuikka, J.T. Serotonin and Dopamine Transporter Binding in Children with Autism Determined by SPECT. Dev. Med. Child Neurol. 2008, 50, 593–597. [Google Scholar] [CrossRef]
- Kurniawan, L.B. Patogenesis, Skrining, Diagnosis, Dan Penatalaksanaan Phenylketonuria Screening, Diagnosis, and Management of Phenylketonuria. Cermin Dunia Kedokt. 2015, 42, 668–673. [Google Scholar]
- Petersen, S.E.; Posner, M.I. The Attention System of the Human Brain: 20 Years After. Annu. Rev. Neurosci. 2012, 35, 73–89. [Google Scholar] [CrossRef] [Green Version]
- Tu, W.-J.; Chen, H.; He, J. Application of LC-MS/MS Analysis of Plasma Amino Acids Profiles in Children with Autism. J. Clin. Biochem. Nutr. 2012, 51, 248–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tirouvanziam, R.; Obukhanych, T.V.; Laval, J.; Aronov, P.A.; Libove, R.; Banerjee, A.G.; Parker, K.J.; O’Hara, R.; Herzenberg, L.A.; Herzenberg, L.A.; et al. Distinct Plasma Profile of Polar Neutral Amino Acids, Leucine, and Glutamate in Children with Autism Spectrum Disorders. J. Autism Dev. Disord. 2012, 42, 827–836. [Google Scholar] [CrossRef]
- Arnold, G.L.; Hyman, S.L.; Mooney, R.A.; Kirby, R.S. Plasma Amino Acids Profiles in Children with Autism: Potential Risk of Nutritional Deficiencies. J. Autism Dev. Disord. 2003, 33, 449–454. [Google Scholar] [CrossRef]
- Aldred, S.; Moore, K.M.; Fitzgerald, M.; Waring, R.H. Plasma Amino Acid Levels in Children with Autism and Their Families. J. Autism. Dev. Disord. 2003, 33, 93–97. [Google Scholar] [CrossRef]
- Xu, X.-J.; Cai, X.-E.; Meng, F.-C.; Song, T.-J.; Wang, X.-X.; Wei, Y.-Z.; Zhai, F.-J.; Long, B.; Wang, J.; You, X.; et al. Comparison of the Metabolic Profiles in the Plasma and Urine Samples Between Autistic and Typically Developing Boys: A Preliminary Study. Front. Psychiatry 2021, 12, 657105. [Google Scholar] [CrossRef]
- Ali, A.; Waly, M.I.; Al-Farsi, Y.M.; Essa, M.M.; Al-Sharbati, M.M.; Deth, R.C. Hyperhomocysteinemia among Omani Autistic Children: A Case-Control Study. Acta Biochim. Pol. 2011, 58, 547–551. [Google Scholar] [CrossRef] [PubMed]
- Paşca, S.P.; Nemeş, B.; Vlase, L.; Gagyi, C.E.; Dronca, E.; Miu, A.C.; Dronca, M. High Levels of Homocysteine and Low Serum Paraoxonase 1 Arylesterase Activity in Children with Autism. Life Sci. 2006, 78, 2244–2248. [Google Scholar] [CrossRef] [PubMed]
- Hyperlysinemia: MedlinePlus Genetics. Available online: https://medlineplus.gov/genetics/condition/hyperlysinemia/ (accessed on 15 June 2022).
- Lysine Information|Mount Sinai-New York. Available online: https://www.mountsinai.org/health-library/supplement/lysine (accessed on 30 March 2022).
- Papes, F.; Surpili, M.J.; Langone, F.; Trigo, J.R.; Arruda, P. The Essential Amino Acid Lysine Acts as Precursor of Glutamate in the Mammalian Central Nervous System. FEBS Lett. 2001, 488, 34–38. [Google Scholar] [CrossRef] [Green Version]
- Petty, F. GABA and Mood Disorders: A Brief Review and Hypothesis. J. Affect. Disord. 1995, 34, 275–281. [Google Scholar] [CrossRef]
- Liu, A.; Zhou, W.; Qu, L.; He, F.; Wang, H.; Wang, Y.; Cai, C.; Li, X.; Zhou, W.; Wang, M. Altered Urinary Amino Acids in Children with Autism Spectrum Disorders. Front. Cell. Neurosci. 2019, 13, 7. [Google Scholar] [CrossRef] [PubMed]
- Demirci, E. Autism Spectrum Disorder and Phenylketonuria: Dyzygotic Twins with Double Syndrome. Noro Psikiyatr. Ars. 2017, 54, 92–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brumm, V.L.; Bilder, D.; Waisbren, S.E. Psychiatric Symptoms and Disorders in Phenylketonuria. Mol. Genet. Metab. 2010, 99 (Suppl. 1), S59–S63. [Google Scholar] [CrossRef]
- Yektaş, Ç.; Alpay, M.; Tufan, A.E. Comparison of Serum B12, Folate and Homocysteine Concentrations in Children with Autism Spectrum Disorder or Attention Deficit Hyperactivity Disorder and Healthy Controls. Neuropsychiatr. Dis. Treat. 2019, 15, 2213–2219. [Google Scholar] [CrossRef] [Green Version]
- Soni, R.M.; Tiwari, S.C.; Mahdi, A.A.; Kohli, N. Serum Homocysteine and Behavioral and Psychological Symptoms of Dementia: Is There Any Correlation in Alzheimer’s Disease? Ann. Neurosci. 2019, 25, 152–159. [Google Scholar] [CrossRef]
- Al-Farsi, Y.M.; Waly, M.I.; Deth, R.C.; Al-Sharbati, M.M.; Al-Shafaee, M.; Al-Farsi, O.; Al-Khaduri, M.M.; Gupta, I.; Ali, A.; Al-Khalili, M.; et al. Low Folate and Vitamin B12 Nourishment Is Common in Omani Children with Newly Diagnosed Autism. Nutrition 2013, 29, 537–541. [Google Scholar] [CrossRef]
- Carmel, R.; Green, R.; Rosenblatt, D.S.; Watkins, D. Update on Cobalamin, Folate, and Homocysteine. Hematol. Am. Soc. Hematol. Educ. Program 2003, 2003, 62–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brumm, V.L.; Azen, C.; Moats, R.A.; Stern, A.M.; Broomand, C.; Nelson, M.D.; Koch, R. Neuropsychological Outcome of Subjects Participating in the PKU Adult Collaborative Study: A Preliminary Review. J. Inherit. Metab. Dis. 2004, 27, 549–566. [Google Scholar] [CrossRef] [PubMed]
- Allen, M.J.; Sabir, S.; Sharma, S. GABA Receptor. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Garcia, A.; Zanibbi, K. Homocysteine and Cognitive Function in Elderly People. CMAJ 2004, 171, 897–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Amino Acid | ASD |
|---|---|
| Tryptophan | High [38] Low [52,53,54] |
| Tyrosine | Low [52,53,54] |
| Phenylalanine | High [38,55,56] |
| Homocysteine | High [52,57,58] |
| Lysine | High [52,55] Low [54] |
| Nutrient | Confirmed Roles | Evidence-Based Findings Relevant to ASD |
|---|---|---|
| Choline | Converts into acetylcholine in the body [6] | Lower dietary intake and plasma levels of choline in children with ASD [11] Supplementation (36 mmol/kg) improved anxiety levels, deficits in social interaction, and reduced marble-burying behavior in mice with ASD-like behavior [9] |
| Aids in the production of methionine [10] | Supplementation (350mg) resulted in improved language skills in children ≤10 years old [6] | |
| Contributes to brain development [9] | Supplementation (350mg) increased acetylcholine which improved ion transport resulting in ameliorated ASD symptoms [6] Supplementation decreased repetitive behavior and anxiety among ASD-induced mice [10] Supplementation improved social behavior and cortical protein levels of autophagy markers (p62 and beclin-1) among ASD-induced mice [10] Improves sensory processing, cognitive functioning, memory, and learning [32] | |
| Tryptophan | Involves in the synthesis of serotonin [40] | Elevated dietary intake increased hyperactivity among individuals with ASD [38] |
| Tyrosine | Involves in the synthesis of dopamine [39] | Low blood levels of tyrosine can decrease dopamine, leading to a decrease in focus and an increase in hyperactivity in ASD [38] |
| Phenylalanine | Converts into tyrosine [38] Toxic levels of phenylalanine have a neurotoxic effect [65] Elevated levels of phenylalanine could lead to behavioral problems and intellectual disabilities [70] | High dietary intake of phenylalanine was reported in children with ASD [38] 25% of late-diagnosed PKU children had autism [37] Well-established relationship between toxic levels and ASD [64] Phenylalanine free diet showed improvements in symptoms for children diagnosed with PKU/ASD [64] |
| Lysine | Deficiency leads to disruption of glutamate synthesis, which interferes with gamma-aminobutyric acid (GABA), an important neurotransmitter in CNS synthesis that reduces neuronal excitability by inhibiting nerve transmission [61,71] | Lower urinary levels among individuals with ASD [63] A lack of lysine causes agitation in children with ASD/ADHD [38,60] |
| Homocysteine | Elevated levels may indicate low vitamin B12, B6, and folate [66] Increased homocysteine levels are associated with decreasing cognitive function and dementia [72] | Lower urinary levels among children > 14 years with ASD and no coexisting illnesses [63] Higher serum concentrations among 81% male population of children with a median age of eight years with ASD [66] |
| Vitamin B6 | Contributes to the production of neurotransmitters (serotonin and dopamine), glutathione, and hemoglobin [23] Aids in the synthesis and conversion of amino acids and neurotransmitters [22] Deficiency can cause irritability [27] | Reduced risk for birthing a child with autism when supplementation is paired with iron, B12, and folic acid [28] Supplementation contributed to more stable tryptophan levels [12] When supplemented with folate and B12, reduced neurobehavioral impairment (social communication disorder, stereotyped repetitive behavior, learning and spatial memory impairment) in mice [33] |
| Vitamin B12 | Deficiency has features of neurological impairments such as motor disturbances, cognitive impairments, irritability, and brain cell loss [21,27] Blood cell production [21] | Lower dietary intake and serum concentrations were observed among children with ASD [66,68] Reduced risk for birthing a child with autism when supplementation is paired with iron, B6, and folic acid [28] High plasma levels (>19.5 μg per deciliter) during pregnancy were associated with increased risk for ASD [29] Supplementation (75 μg) correlated with improvements in transmethylation metabolism of AA methionine and improvements in ASD symptoms [32] Supplementation contributed to more stable tryptophan levels, which aids in normal production of neurotransmitters [12] Combined supplementation with folate and B6 reduced neurobehavioral impairment (social communication disorder, stereotyped repetitive behavior, learning, and spatial memory impairment) in mice [33] |
| Folate | Aids in converting AA homocysteine to methionine [10] | Low dietary intake was observed among children with ASD [68] No significant variations between ASD and non-ASD were measured by serum and plasma [30,66] |
| Deficiency can cause behavior changes and cognitive impairment [27] | High plasma levels (>2.2 μg) during pregnancy were associated with an increased risk of birthing a child with ASD [29] A higher risk for autism was found when mothers did not supplement with folic acid before pregnancy [31] Reduced risk for birthing a child with autism when supplemented along with iron, B12, and B6 [28] Supplementation contributed to more stable tryptophan levels, which aids in normal production of neurotransmitters [12] Combined supplementation with folate and B12 reduced neurobehavioral impairment (social communication disorder, stereotyped repetitive behavior, learning, and spatial memory impairment) in mice [33] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jennings, L.; Basiri, R. Amino Acids, B Vitamins, and Choline May Independently and Collaboratively Influence the Incidence and Core Symptoms of Autism Spectrum Disorder. Nutrients 2022, 14, 2896. https://doi.org/10.3390/nu14142896
Jennings L, Basiri R. Amino Acids, B Vitamins, and Choline May Independently and Collaboratively Influence the Incidence and Core Symptoms of Autism Spectrum Disorder. Nutrients. 2022; 14(14):2896. https://doi.org/10.3390/nu14142896
Chicago/Turabian StyleJennings, Laurel, and Raedeh Basiri. 2022. "Amino Acids, B Vitamins, and Choline May Independently and Collaboratively Influence the Incidence and Core Symptoms of Autism Spectrum Disorder" Nutrients 14, no. 14: 2896. https://doi.org/10.3390/nu14142896
APA StyleJennings, L., & Basiri, R. (2022). Amino Acids, B Vitamins, and Choline May Independently and Collaboratively Influence the Incidence and Core Symptoms of Autism Spectrum Disorder. Nutrients, 14(14), 2896. https://doi.org/10.3390/nu14142896