
The Need for Culturally Appropriate Food Allergy Management Strategies: The Indian Milk Ladder
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Formation of Expert Group
2.2. Initial Development of the Indian Milk Ladder
2.3. Testing of the Milk Protein Content of Food Included in the Milk Ladder
3. Results
3.1. Expert Consensus
3.2. Validation of Milk Protein in Selected Foods
3.3. Adaptation of Sugar Content
3.4. Consideration of Food Matrix
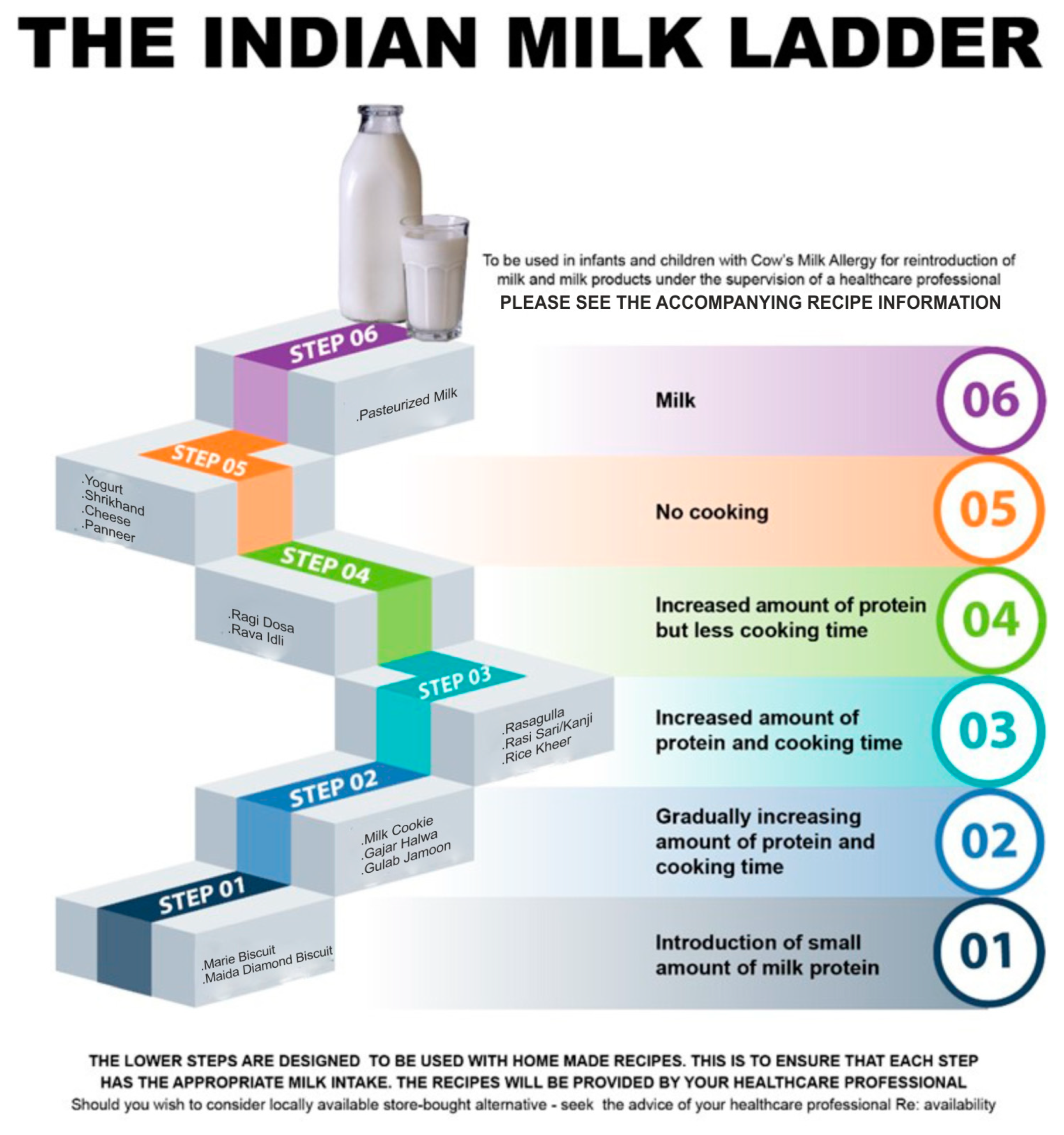
3.5. Finalization of the Indian Milk Ladder
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Muraro, A.; Werfel, T.; Hoffmann-Sommergruber, K.; Roberts, G.; Beyer, K.; Bindslev-Jensen, C.; Cardona, V.; Dubois, A.; Dutoit, G.; Eigenmann, P.; et al. EAACI food allergy and anaphylaxis guidelines: Diagnosis and management of food allergy. Allergy 2014, 69, 1008–1025. [Google Scholar] [CrossRef]
- Fiocchi, A.; Schünemann, H.J.; Brozek, J.; Restani, P.; Beyer, K.; Troncone, R.; Martelli, A.; Terracciano, L.; Bahna, S.L.; Rance, F.; et al. Diagnosis and Rationale for Action Against Cow’s Milk Allergy (DRACMA): A summary report. J. Allergy Clin. Immunol. 2010, 126, 1119–1128.e12. [Google Scholar] [CrossRef]
- Luyt, D.; Ball, H.; Makwana, N.; Green, M.R.; Bravin, K.; Nasser, S.M.; Clark, A.T. BSACI guideline for the diagnosis and management of cow’s milk allergy. Clin. Exp. Allergy 2014, 44, 642–672. [Google Scholar] [CrossRef] [PubMed]
- Fox, A.; Brown, T.; Walsh, J.; Venter, C.; Meyer, R.; Nowak-Wegrzyn, A.; Levin, M.; Spawls, H.; Beatson, J.; Lovis, M.-T.; et al. An update to the Milk Allergy in Primary Care guideline. Clin. Transl. Allergy 2019, 9, 40. [Google Scholar] [CrossRef]
- Flom, J.D.; Sicherer, S.H. Epidemiology of Cow’s Milk Allergy. Nutrients 2019, 11, 1051. [Google Scholar] [CrossRef]
- Vincent, R.; MacNeill, S.J.; Marrs, T.; Craven, J.; Logan, K.; Flohr, C.; Lack, G.; Radulovic, S.; Perkin, M.R.; Ridd, M.J. Frequency of guideline-defined cow’s milk allergy symptoms in infants: Secondary analysis of EAT trial data. Clin. Exp. Allergy 2022, 52, 82–93. [Google Scholar] [CrossRef] [PubMed]
- Yachha, S.K.; Misra, S.; Malik, A.K.; Nagi, B.; Mehta, S. Spectrum of malabsorption syndrome in north Indian children. Indian J. Gastroenterol. 1993, 12, 120–125. [Google Scholar] [PubMed]
- Poddar, U.; Agarwal, J.; Yachha, S.K.; Srivastava, A. Toddler’s diarrhea: Is it an under-recognized entity in developing countries? J. Trop. Pediatr. 2013, 59, 470–475. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Mandal, J.; Das, M.; Roy, I.; Chatterjee, S.; Barui, N.C.; Gupta-Bhattacharya, S. Immediate hypersensitivity to common food allergens: An investigation on food sensitization in respiratory allergic patients of calcutta, India. World Allergy Organ. J. 2009, 2, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Ball, H.B.; Luyt, D. Home-based cow’s milk reintroduction using a milk ladder in children less than 3 years old with IgE-mediated cow’s milk allergy. Clin. Exp. Allergy 2019, 49, 911–920. [Google Scholar] [CrossRef]
- Venter, C.; Brown, T.; Meyer, R.; Walsh, J.; Shah, N.; Nowak-Węgrzyn, A.; Chen, T.-X.; Gleischer, D.M.; Heine, R.G.; Levin, M.; et al. Better recognition, diagnosis and management of non-IgE-mediated cow’s milk allergy in infancy: iMAP-an international interpretation of the MAP (Milk Allergy in Primary Care) guideline. Clin. Transl. Allergy 2017, 7, 26. [Google Scholar] [CrossRef] [PubMed]
- Venter, C.; Brown, T.; Shah, N.; Walsh, J.; Fox, A.T. Diagnosis and management of non-IgE-mediated cow’s milk allergy in infancy—A UK primary care practical guide. Clin. Transl. Allergy 2013, 3, 23. [Google Scholar] [CrossRef] [PubMed]
- Nowak-Węgrzyn, A.; Chehade, M.; Groetch, M.E.; Spergel, J.M.; Wood, R.A.; Allen, K.; Atkins, D.; Bahna, S.; Barad, A.V.; Berin, C.; et al. International consensus guidelines for the diagnosis and management of food protein-induced enterocolitis syndrome: Executive summary-Workgroup Report of the Adverse Reactions to Foods Committee, American Academy of Allergy, Asthma & Immunology. J. Allergy Clin. Immunol. 2017, 139, 1111–1126.e4. [Google Scholar]
- Cianferoni, A.; Shuker, M.; Brown-Whitehorn, T.; Hunter, H.; Venter, C.; Spergel, J.M. Food avoidance strategies in eosinophilic oesophagitis. Clin. Exp. Allergy 2019, 49, 269–284. [Google Scholar] [CrossRef]
- Nowak-Wegrzyn, A.; Szajewska, H.; Lack, G. Food allergy and the gut. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 241–257. [Google Scholar] [CrossRef] [PubMed]
- Vassilopoulou, E.; McMilin, C.; Venter, C. Mediterranean Milk Ladder: Integrating a Healthy Eating Plan While Reintroducing Cow’s Milk. Children 2023, 10, 234. [Google Scholar] [CrossRef]
- Kim, J.S.; Nowak-Węgrzyn, A.; Sicherer, S.H.; Noone, S.; Moshier, E.L.; Sampson, H.A. Dietary baked milk accelerates the resolution of cow’s milk allergy in children. J. Allergy Clin. Immunol. 2011, 128, 125–131.e2. [Google Scholar] [CrossRef]
- Nowak-Wegrzyn, A.; Bloom, K.A.; Sicherer, S.H.; Shreffler, W.G.; Noone, S.; Wanich, N.; Sampson, H.A. Tolerance to extensively heated milk in children with cow’s milk allergy. J. Allergy Clin. Immunol. 2008, 122, 342–347.e3472. [Google Scholar] [CrossRef]
- Nowak-Węgrzyn, A.; Lawson, K.; Masilamani, M.; Kattan, J.; Bahnson, H.T.; Sampson, H.A. Increased Tolerance to Less Extensively Heat-Denatured (Baked) Milk Products in Milk-Allergic Children. J. Allergy Clin. Immunol. Pract. 2018, 6, 486–495.e5. [Google Scholar] [CrossRef] [PubMed]
- Chomyn, A.; Chan, E.S.; Yeung, J.; Leek, T.K.V.; Williams, B.A.; Soller, L.; Abrams, E.M.; Mak, R.; Wong, T. Canadian food ladders for dietary advancement in children with IgE-mediated allergy to milk and/or egg. Allergy Asthma Clin. Immunol. 2021, 17, 83. [Google Scholar] [CrossRef]
- Athanasopoulou, P.; Deligianni, E.; Dean, T.; Dewey, A.; Venter, C. Use of baked milk challenges and milk ladders in clinical practice: A worldwide survey of healthcare professionals. Clin. Exp. Allergy 2017, 47, 430–434. [Google Scholar] [CrossRef]
- Venter, C.; Meyer, R.; Ebisawa, M.; Athanasopoulou, P.; Mack, D.P. Food allergen ladders: A need for standardization. Pediatr. Allergy Immunol. 2022, 33, e13714. [Google Scholar] [CrossRef]
- Lynch, J.M.; Barbano, D.M. Kjeldahl nitrogen analysis as a reference method for protein determination in dairy products. J. AOAC Int. 1999, 82, 1389–1398. [Google Scholar] [CrossRef]
- Ivens, K.O.; Baumert, J.L.; Taylor, S.L. Commercial Milk Enzyme-Linked Immunosorbent Assay (ELISA) Kit Reactivities to Purified Milk Proteins and Milk-Derived Ingredients. J. Food Sci. 2016, 81, T1871–T1878. [Google Scholar] [CrossRef]
- Moore, J.C.; DeVries, J.W.; Lipp, M.; Griffiths, J.C.; Abernethy, D.R. Total Protein Methods and Their Potential Utility to Reduce the Risk of Food Protein Adulteration. Compr. Rev. Food Sci. Food Saf. 2010, 9, 330–357. [Google Scholar] [CrossRef]
- AOAC International. AOAC Official method 2011.11 Protein (crude) in animal feed, forage (plant tissue), grain and oilseeds. In Official Methods of Analysis of AOAC International, 19th ed.; AOAC International: Gaithersburg, MD, USA; Volume II, Chapter 4; p. 34.
- AOAC International. AOAC 939.02 (1939), Protein (milk) in milk chocolate. Kjeldahl method. In Official Methods of Analysis of AOAC International, 19th ed.; AOAC International: Gaithersburg, MD, USA; Volume II, Chapter 31; p. 12.
- Bloom, K.A.; Huang, F.R.; Bencharitiwong, R.; Bardina, L.; Ross, A.; Sampson, H.A.; Nowak-Węgrzyn, A. Effect of heat treatment on milk and egg proteins allergenicity. Pediatr. Allergy Immunol. 2014, 25, 740–746. (In English) [Google Scholar] [CrossRef]
- Nowak-Wegrzyn, A.; Fiocchi, A. Rare, medium, or well done? The effect of heating and food matrix on food protein allergenicity. Curr. Opin. Allergy Clin. Immunol. 2009, 9, 234–237. (In English) [Google Scholar] [CrossRef] [PubMed]
- Heppell, L.M.; Cant, A.J.; Kilshaw, P.J. Reduction in the antigenicity of whey proteins by heat treatment: A possible strategy for producing a hypoallergenic infant milk formula. Br. J. Nutr. 1984, 51, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Upton, J.; Nowak-Wegrzyn, A. The Impact of Baked Egg and Baked Milk Diets on IgE- and Non-IgE-Mediated Allergy. Clin. Rev. Allergy Immunol. 2018, 55, 118–138. [Google Scholar] [CrossRef]
- Vandenplas, Y.; Brueton, M.; Dupont, C.; Hill, D.; Isolauri, E.; Koletzko, S.; Oranje, A.P.; Staiano, A. Guidelines for the diagnosis and management of cow’s milk protein allergy in infants. Arch. Dis. Child. 2007, 92, 902–908. [Google Scholar] [CrossRef] [PubMed]
- Vandenplas, Y.; Brueton, M.; Dupont, C.; Hill, D.; Isolauri, E.; Koletzko, S.; Oranje, A.P.; Staiano, A. Predicting food challenge outcomes for baked milk: Role of specific IgE and skin prick testing. Ann. Allergy Asthma Immunol. 2012, 109, 309–313.e1. [Google Scholar]
- Lack, G. Epidemiologic risks for food allergy. J. Allergy Clin. Immunol. 2008, 121, 1331–1336. [Google Scholar] [CrossRef]
- Staden, U.; Rolinck-Werninghaus, C.; Brewe, F.; Wahn, U.; Niggemann, B.; Beyer, K. Specific oral tolerance induction in food allergy in children: Efficacy and clinical patterns of reaction. Allergy 2007, 62, 1261–1269. [Google Scholar] [CrossRef]
- Sackesen, C.; Altintas, D.U.; Bingol, A.; Bingol, G.; Buyuktiryaki, B.; Demir, E.; Kansu, A.; Kuloglu, Z.; Tamay, Z.; Sekerel, B.E. Current Trends in Tolerance Induction in Cow’s Milk Allergy: From Passive to Proactive Strategies. Front. Pediatr. 2019, 7, 372. [Google Scholar] [CrossRef] [PubMed]
- Lambert, R.; Grimshaw, K.E.C.; Ellis, B.; Jaitly, J.; Roberts, G. Evidence that eating baked egg or milk influences egg or milk allergy resolution: A systematic review. Clin. Exp. Allergy 2017, 47, 829–837. [Google Scholar] [CrossRef] [PubMed]
- Nowak-Wegrzyn, A.; Strong, B.D.; Ananos, D.; Sampson, H.A. Long term follow up of children who incorporated extensively heated (baked milk) in the diet. J. Allergy Clin. Immunol. 2014, 133, AB107. [Google Scholar] [CrossRef]
- Nowak-Wegrzyn, A.; Strong, B.D.; Fernandez, K.; Bahnson, T.; Sampson, H.A. Increasing tolerance to less extensively heat-denatured (baked) milk products in milk-allergic children. J. Allergy Clin. Immunol. 2015, 135, AB234. [Google Scholar] [CrossRef]
- Hochwallner, H.; Schulmeister, U.; Swoboda, I.; Spitzauer, S.; Valenta, R. Cow’s milk allergy: From allergens to new forms of diagnosis, therapy and prevention. Methods 2014, 66, 22–33. [Google Scholar] [CrossRef]
- Bartuzi, Z.; Cocco, R.R.; Muraro, A.; Nowak-Węgrzyn, A. Contribution of Molecular Allergen Analysis in Diagnosis of Milk Allergy. Curr. Allergy Asthma Rep. 2017, 17, 46. [Google Scholar] [CrossRef]
- Lifschitz, C.; Szajewska, H. Cow’s milk allergy: Evidence-based diagnosis and management for the practitioner. Eur. J. Pediatr. 2015, 174, 141–150. [Google Scholar] [CrossRef]
- BBavaro, S.L.; De Angelis, E.; Barni, S.; Pilolli, R.; Mori, F.; Novembre, E.M.; Monaci, L. Modulation of Milk Allergenicity by Baking Milk in Foods: A Proteomic Investigation. Nutrients 2019, 11, 1536. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Step | Food | Milk/Serving | Milk Protein/ Serving | Cooking Temperature (°C) | Cooking Time |
|---|---|---|---|---|---|
| Step 1 and 2: Gradually increasing amount of protein with increasing cooking time | |||||
| Step 1 | Marie Biscuit | 0.050 g | 180 | 15 min | |
| Maida Diamond Biscuits | 1.25 mL | 0.040 g | 180 | 15 min | |
| Step 2 | Milk Cookie | 1.8 g milk powder | 0.37 g | 180 | 10 min |
| Halwa | 25 mL | 0.75 g | Boiled | 25 min | |
| Ragi Sari/Kanji (with milk) | 25 mL | 0.75 g | Boiled | 30 min | |
| Step 3: Slightly lower amount of protein and lower heating time | |||||
| Step 3 | Ragi Dosa | 21 mL | 0.74 g | Fry | 2–4 min |
| Rava Idli | 20 mL | 0.70 g | Steam | 15 min | |
| Step 4: Increased Protein and Increased Cooking time too | |||||
| Step 4 | Gulab Jamun (dry) | 8.3 g milk powder | 2.15 g | Boiled + Fried | 20 min |
| Rasagullah | 100 mL | 3.5 g | Boiled | 30 min | |
| Rice Kheer | 100 mL | 3.5 g | Boiled | 30 min | |
| Step 5: No Cooking | |||||
| Step 5 | Paneer | 3.7 g | No cooking But through cheese-making process | ||
| Shrikand or Yoghurt | 180 mL | 6.0 | No cooking | ||
| Step 6: Pasteurized Milk | |||||
| Step 6 | Milk | ¼ cup | 2.17 g | ||
| ½ cup | 4.34 g | ||||
| 1 cup | 8.68 g | ||||
| Sample Name | Method | Reading 1 | Reading 2 | Reading 3 | Mean | SD |
|---|---|---|---|---|---|---|
| Biscuit | ELISA | 0.005 | 0.005 | 0.005 | 0.005 | 0 |
| Maida Biscuits | ELISA | 0.006 | 0.005 | 0.006 | 0.005 | 0.0005 |
| Shrikhand | AOAC 939.02 | 0.28 | 0.28 | 0.28 | 0.28 | 0 |
| Cookie | ELISA | 0.32 | 0.38 | 0.38 | 0.36 | 0.0346 |
| Pan Cake | ELISA | 0.34 | 0.35 | 0.37 | 0.353 | 0.0152 |
| Gajar Halwa | AOAC 939.02 | 0.41 | 0.41 | 0.41 | 0.41 | 0 |
| GulabJamun | AOAC 939.02 | 1.23 | 1.23 | 1.23 | 1.23 | 0 |
| Rasagulla | AOAC 2001.11 | 2.49 | 2.67 | 2.49 | 2.55 | 0.1039 |
| Ragi Sari | AOAC 939.02 | 2.73 | 2.59 | 2.73 | 2.68 | 0.0808 |
| Rice Kheer | AOAC 939.02 | 2.87 | 2.87 | 2.73 | 2.82 | 0.0808 |
| Ragi Dosa | ELISA | 2.92 | 2.997 | 2.87 | 2.92 | 0.0639 |
| Rava Idli | ELISA | 3.12 | 3.08 | 3.2 | 3.13 | 0.0611 |
| Muffin | ELISA | 4.63 | 4.08 | 4.36 | 4.35 | 0.2750 |
| Yogurt | AOAC 2001.11 | 7.33 | 7.21 | 7.16 | 7.23 | 0.0873 |
| Cheese | AOAC 2001.11 | 21.15 | 21.28 | 21.1 | 21.17 | 0.0929 |
| Paneer | AOAC 2001.11 | 21.37 | 21.49 | 21.49 | 21.45 | 0.0692 |
| Milk Ladder Foods | Sugar per Portion in Original Recipes | Sugar Content in Adapted Recipes | Reduction in Sugar per Portion |
|---|---|---|---|
| Maida Diamond Biscuit | 1.5 g | 0.75 g | 0.75 g |
| Milk Cookie | 11.25 g | 1.9 g | 9.6 g |
| Gajar Halwa | 25 g | 6 g | 19 g |
| Gulab Jamun | 20 g | 5 g | 15 g |
| Rasagulla | 33 g | 13 g | 20 g |
| Ragi Sair/Kanji | 5 g | 5 g | Nil |
| Rice Kheer | 31.25 g | 12.5 g | 18.75 g |
| Srikhand | 30 g | 7.5 g | 22.5 g |
| Step | Food | Cooked Milk Protein Content (g/100 g) | Recommended Portion per Serving | Cooking Temperature (°C) | Cooking Time |
|---|---|---|---|---|---|
| Step 1: Introduction of small amount of milk protein | |||||
| Step 1 | Marie Biscuit | 0.005 | ½ Biscuit to start with & build up gradually | Commercial Preparation | |
| Maida Dimond Biscuit | 0.006 | 180 | 15 min | ||
| Step 2: Gradually increasing amount of protein and cooking time | |||||
| Step 2 | Milk Cookie | 0.35 | Start with ¼ portion & increase gradually | 180 | 12 min |
| Gajar Halwa | 0.410 | Boil | 25 min | ||
| Gulab Jamun (dry) | 1.230 | Boil + Fry | 20 + 5 min | ||
| Step 3: Increasing amount of protein and cooking time | |||||
| Step 3 | Rasgulla | 2.550 | Start with ¼ portion increase gradually | Boil | 30 min |
| Ragi Sari/Kanji | 2.686 | Boil | 30 min | ||
| Rice Kheer | 2.823 | Boil | 30 min | ||
| Step 4: Increasing amount of protein but less cooking time | |||||
| Step 4 | Ragi Dosa | 2.929 | Start with ¼ portion increase gradually | Fry | 2–4 min |
| Rava Idli | 3.120 | Steam | 15 min | ||
| Step 5: No cooking | |||||
| Step 5 | Yoghurt | 7.330 | Start with ¼ portion and increase gradually | No Cooking | Through Cheese making |
| Srikhand | 8.680 | No Cooking | |||
| Cheese | 21.28 | – | – | ||
| Paneer | 21.49 | ||||
| Step 6: Milk | |||||
| Step 6 | Pasteurized Milk | Start with ¼ cup and increase gradually | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hosaagrahara Ramakrishna, S.; Shah, N.; Acharyya, B.C.; Durairaj, E.; Verma, L.; Sankaranarayanan, S.; Wadhwa, N.; Venter, C. The Need for Culturally Appropriate Food Allergy Management Strategies: The Indian Milk Ladder. Nutrients 2023, 15, 3921. https://doi.org/10.3390/nu15183921
Hosaagrahara Ramakrishna S, Shah N, Acharyya BC, Durairaj E, Verma L, Sankaranarayanan S, Wadhwa N, Venter C. The Need for Culturally Appropriate Food Allergy Management Strategies: The Indian Milk Ladder. Nutrients. 2023; 15(18):3921. https://doi.org/10.3390/nu15183921
Chicago/Turabian StyleHosaagrahara Ramakrishna, Somashekara, Neil Shah, Bhaswati C. Acharyya, Emmany Durairaj, Lalit Verma, Srinivas Sankaranarayanan, Nishant Wadhwa, and Carina Venter. 2023. "The Need for Culturally Appropriate Food Allergy Management Strategies: The Indian Milk Ladder" Nutrients 15, no. 18: 3921. https://doi.org/10.3390/nu15183921
APA StyleHosaagrahara Ramakrishna, S., Shah, N., Acharyya, B. C., Durairaj, E., Verma, L., Sankaranarayanan, S., Wadhwa, N., & Venter, C. (2023). The Need for Culturally Appropriate Food Allergy Management Strategies: The Indian Milk Ladder. Nutrients, 15(18), 3921. https://doi.org/10.3390/nu15183921