
Nutritional Ultrasonography, a Method to Evaluate Muscle Mass and Quality in Morphofunctional Assessment of Disease Related Malnutrition

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Subject
2.3. Variables
- -
- Bioelectrical Impedanciometry (BIA): The BIA measure the hydration and cell density of the body by the determination of electric parameters such as resistance, reactance, and phase angle. The use of validated estimative equations allows us to define the compartments of body composition [20]. Bioimpedanciometry (BIA NutriLab; EFG Akern, Akern, Pisa, Italy) was performed between 8:00 and 9:15, after an overnight fast and after a time of 15 min in the supine position. The BIA measured the parameters of impedance (Z), resistance (R) and capacitance (X). The phase angle (PhA) is calculated with: PhA = ((X/R) × 180°/π). It was calculated by estimative equation fat mass (FM), fat-free mass (FFM), fat-free mass index (FFMI) and percentage of skeletal muscle mass (%MM) [20]. We estimated the appendicular skeletal muscle mass (ASMI) by Sergi Formula: −3.964 + (0.227 × RI) + (0.095 × weight) + (1.384 × sex) + (0.064 × Z), where RI resistivity index (sex: Male = 1; Female = 0) [21].
- -
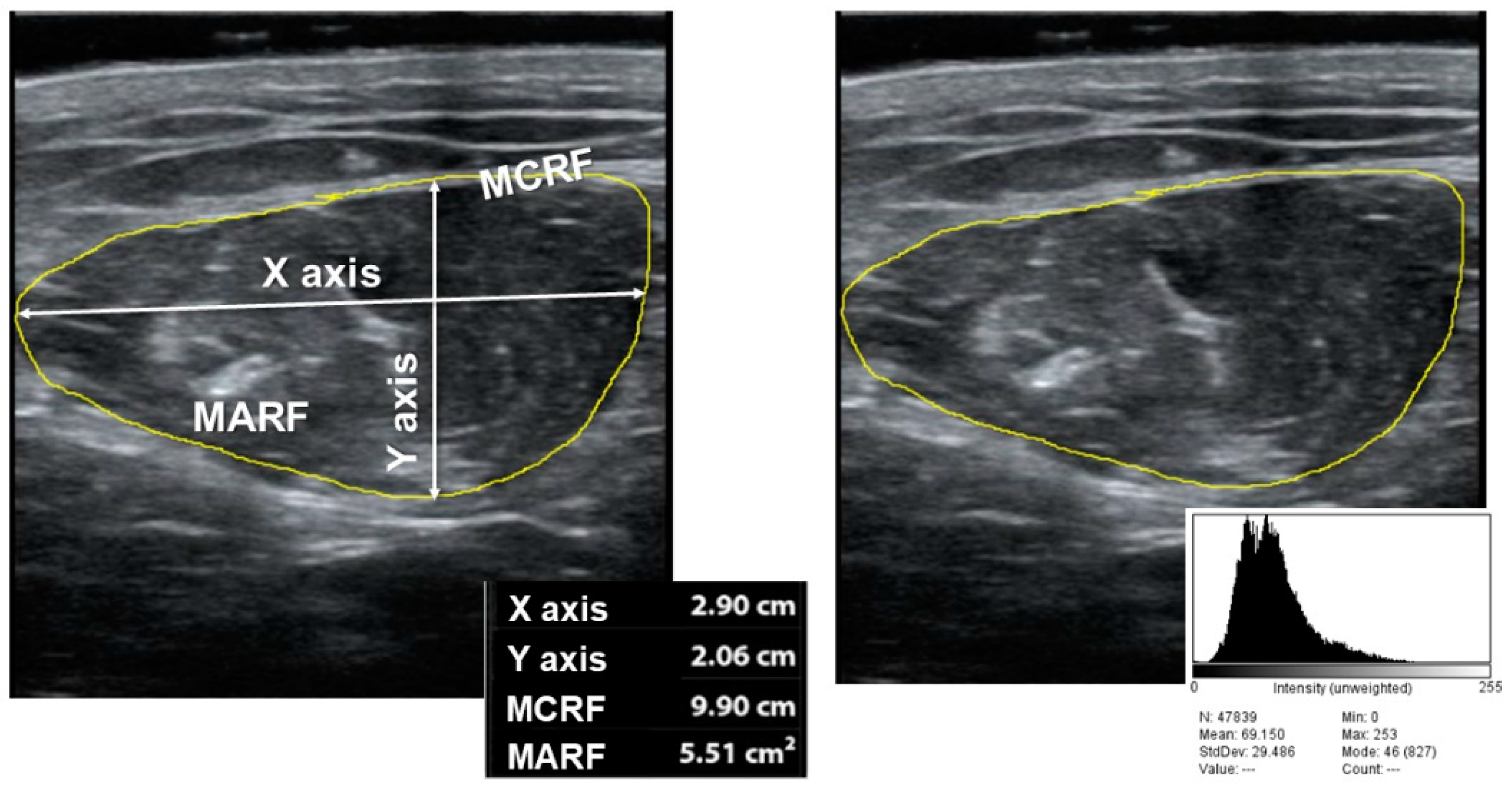
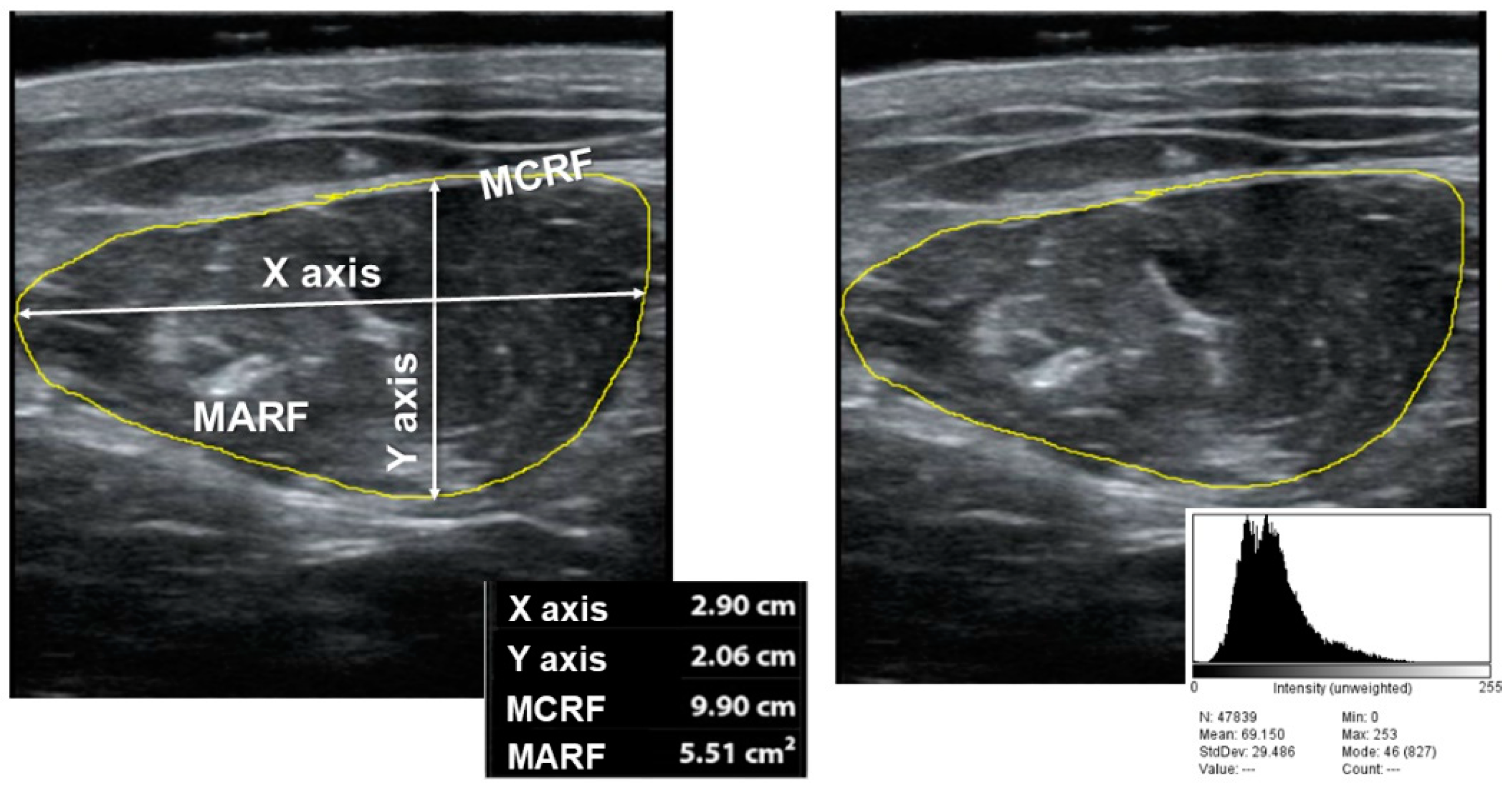
- Nutritional Ultrasonography: We made a muscular ultrasonography of the quadriceps rectus femoris (QRF) of the dominant lower extremity with a 10 to 12 MHz probe and a multifrequency linear matrix (Mindray Z60, Madrid, Spain). The measurement was made with the patient in the supine position. The probe was aligned perpendicular to the longitudinal and transverse axis of QRF. The determination was performed without compression at the level of the lower third from the superior pole of the patella and the anterior superior iliac spine [14].
2.4. Statistical Analysis
3. Results
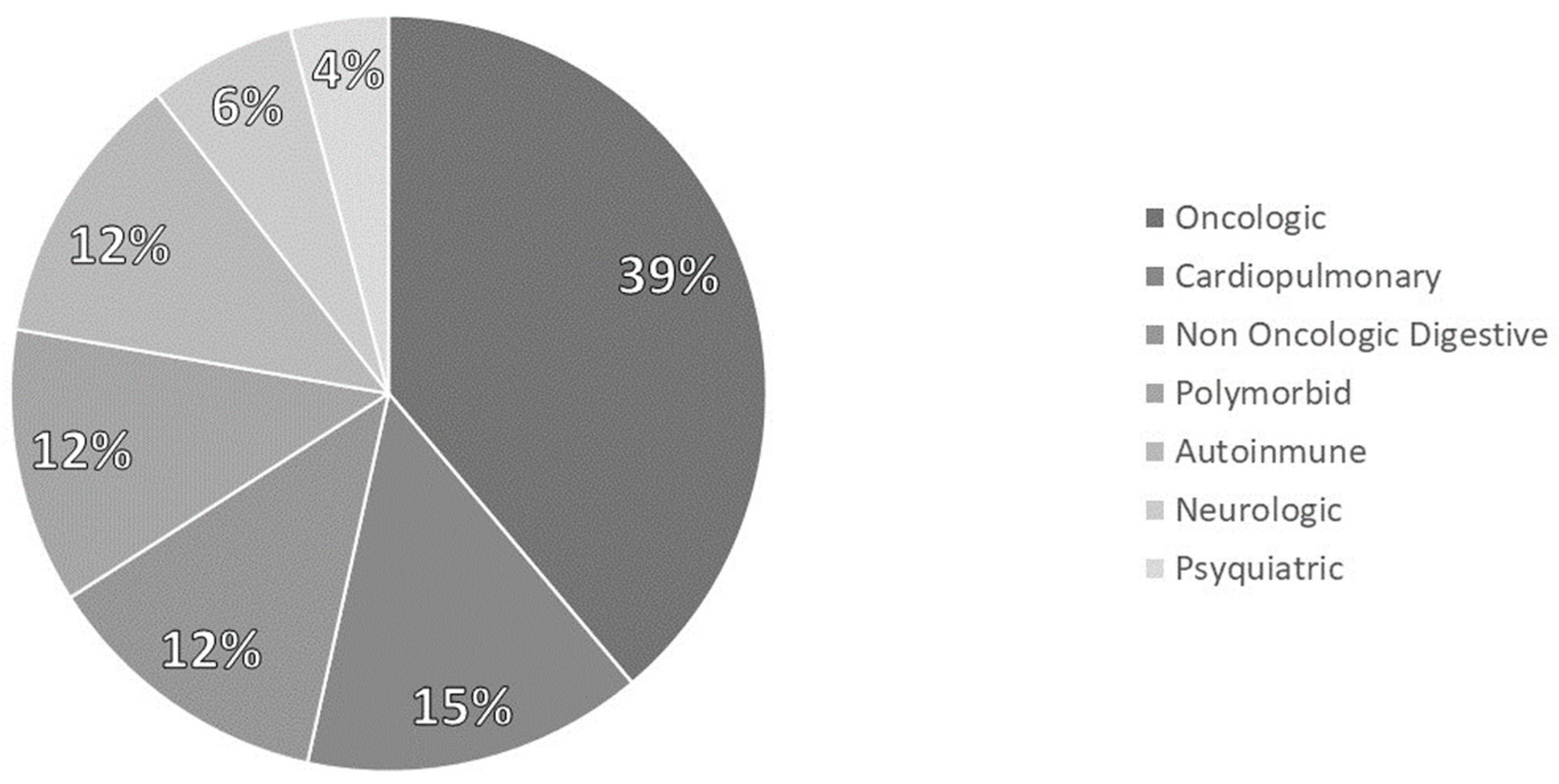
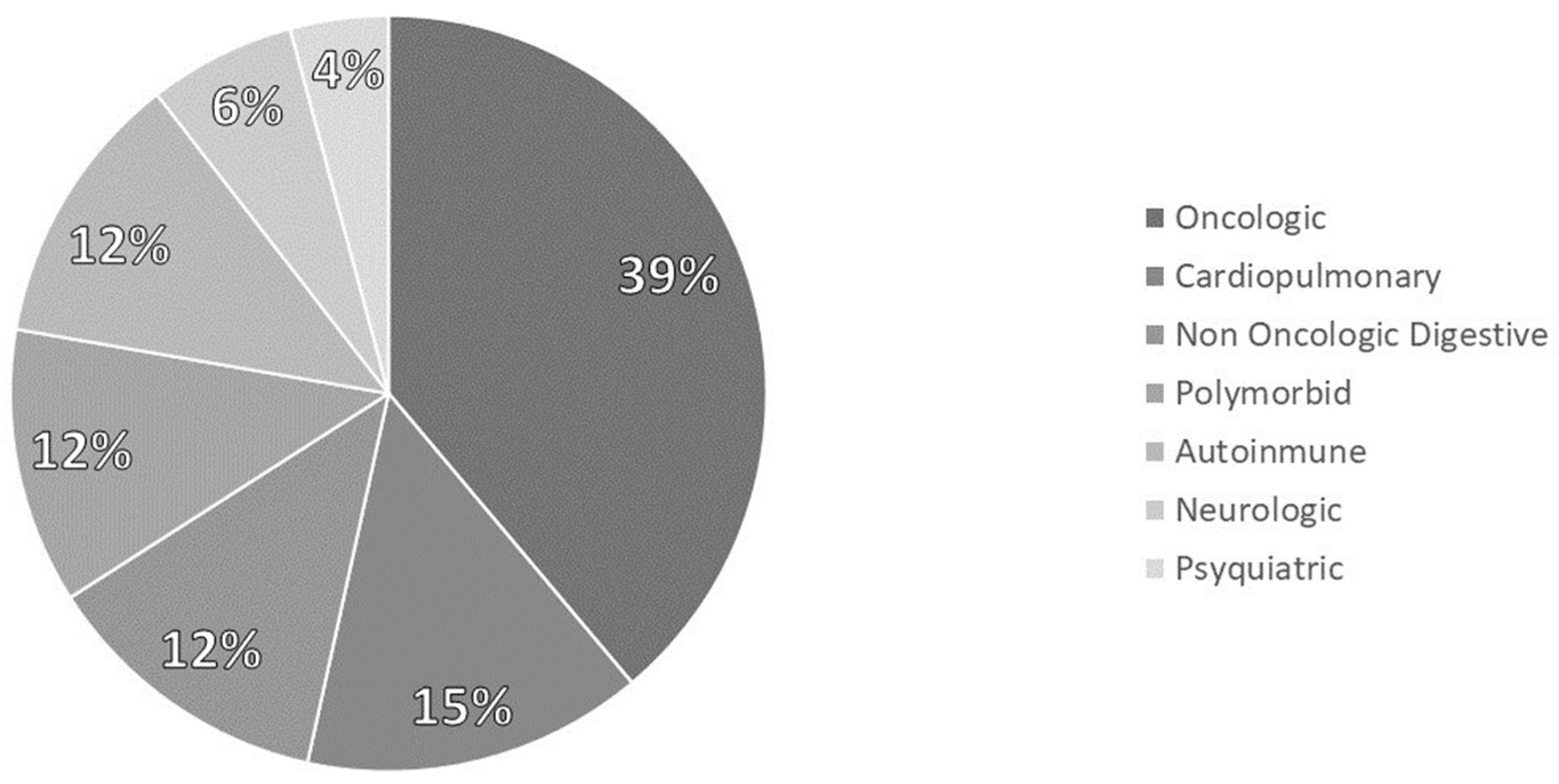
3.1. Sample Description
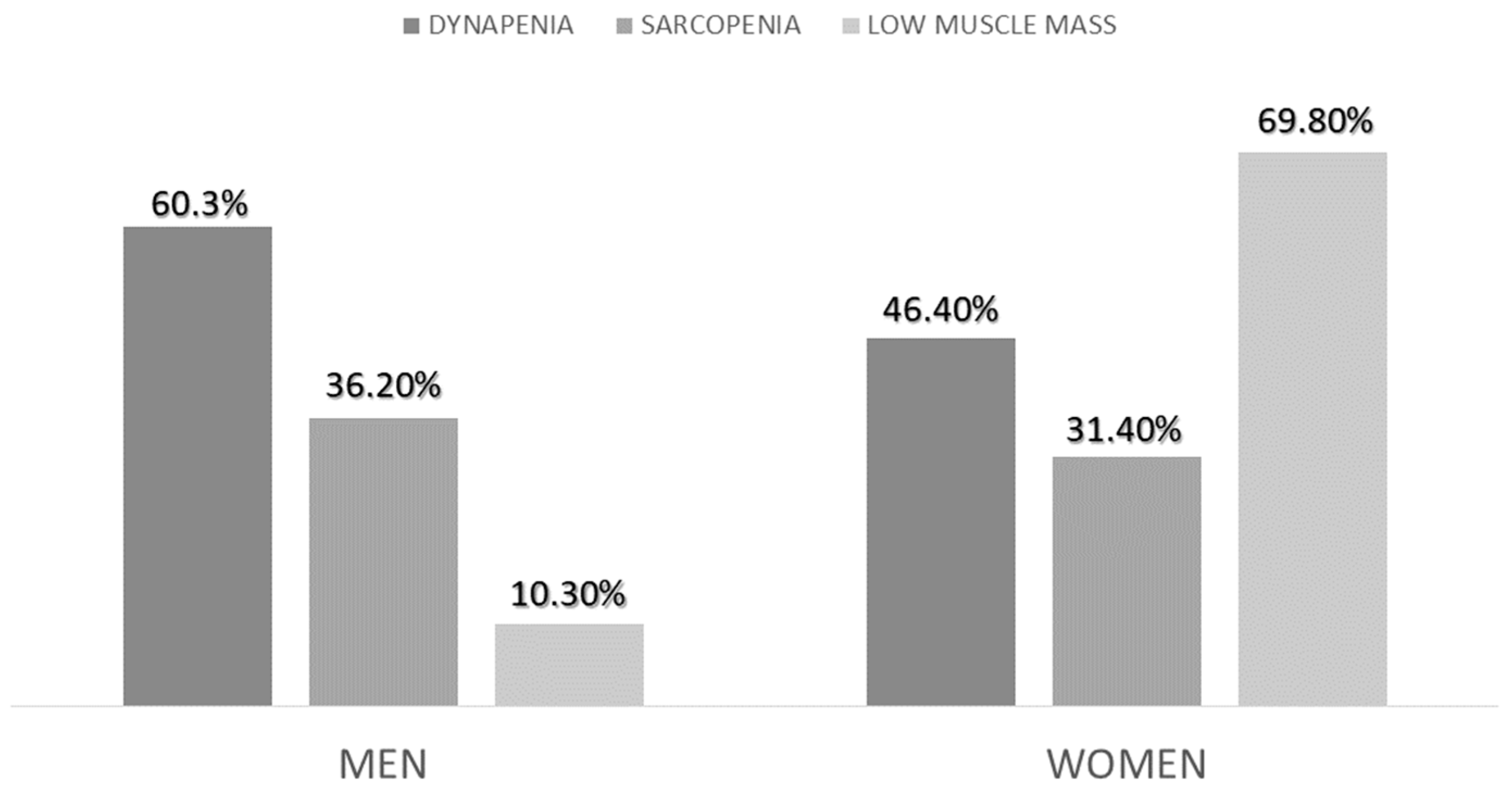
3.2. Morphofunctional Assessment and Diagnosis of Sarcopenia
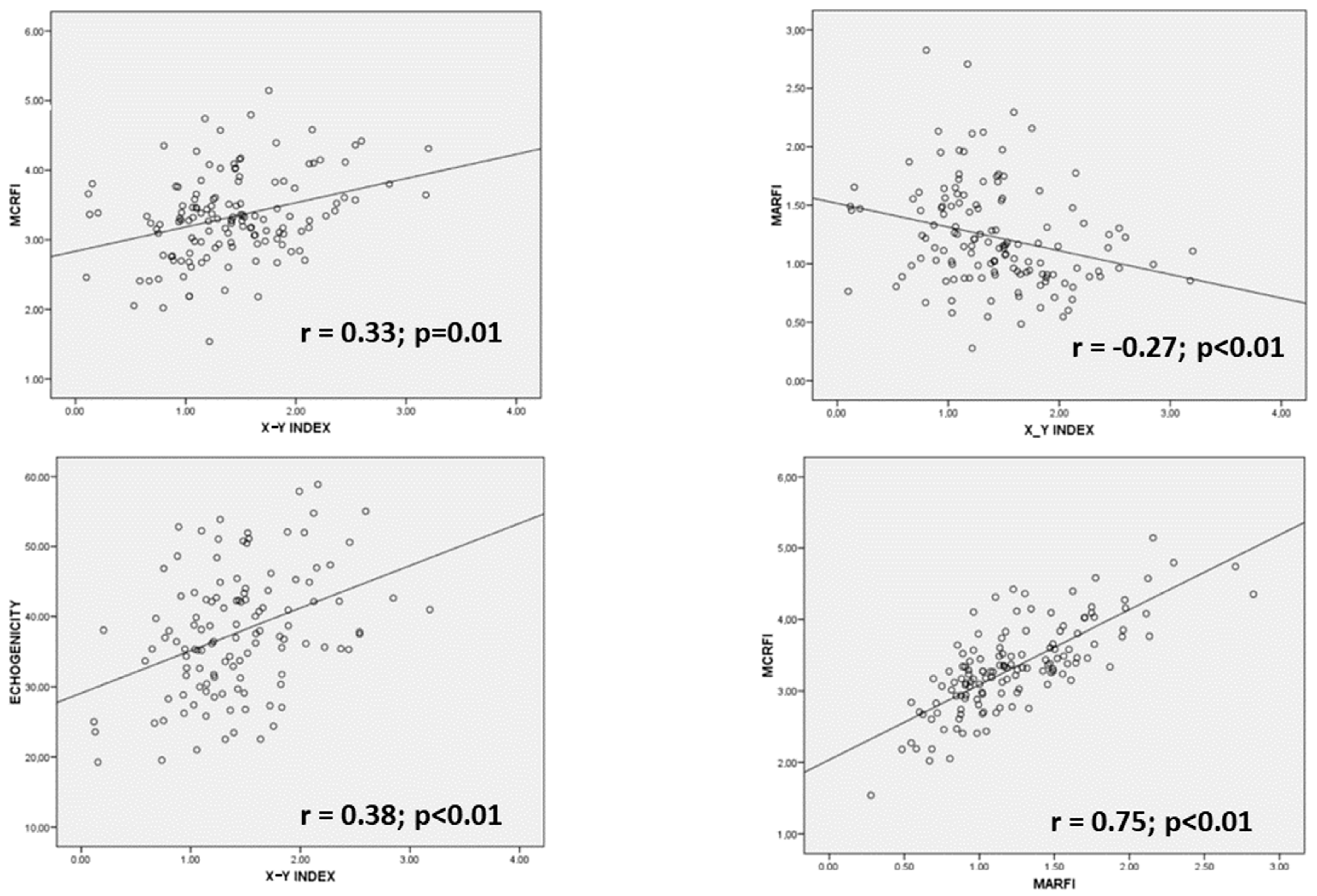
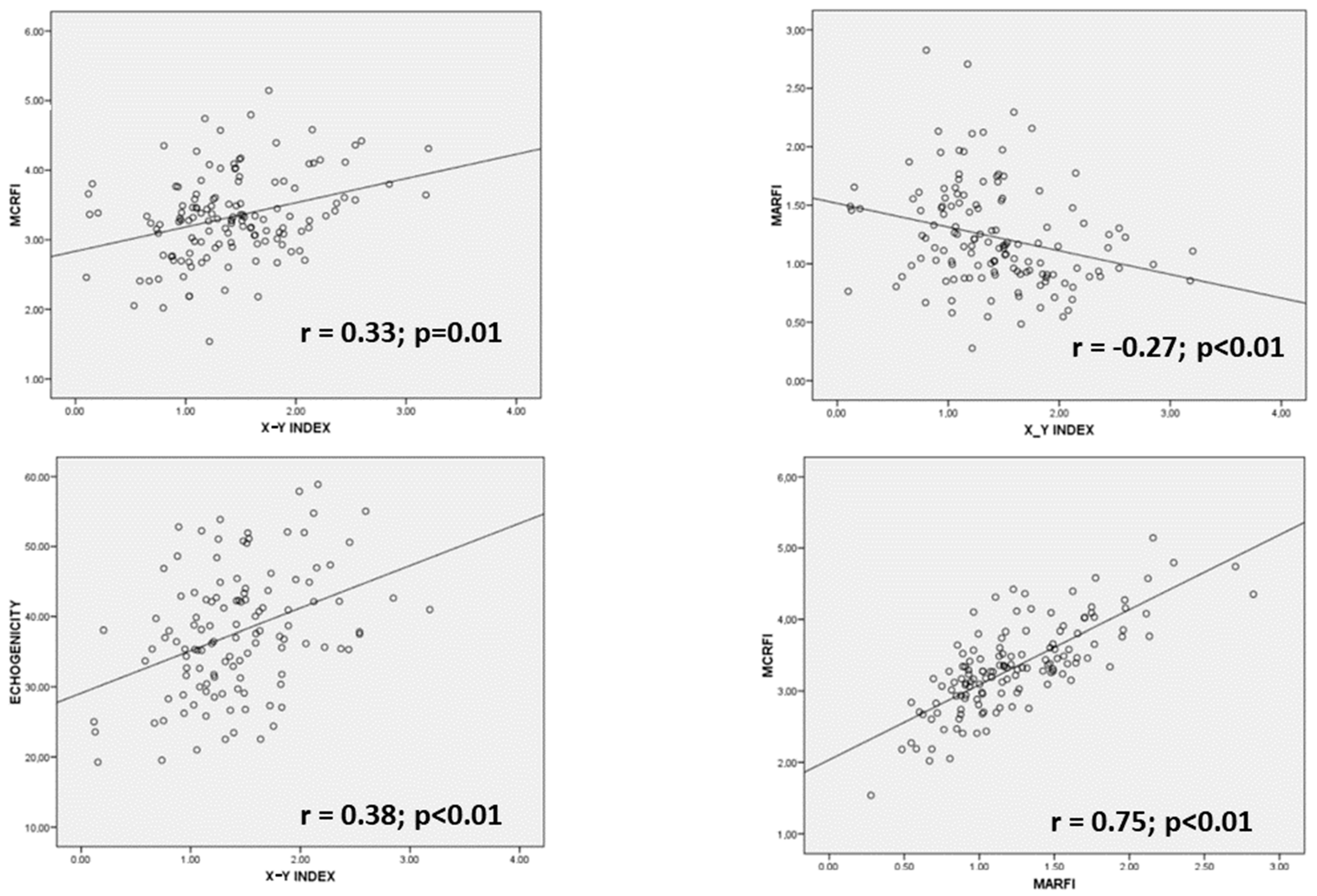
3.3. Comparison of Parameters of Muscle Mass and Quality of Nutritional Ultrasonography
3.4. Comparison of Parameters of Muscle Mass and Quality of Nutritional Ultrasonog-Raphy
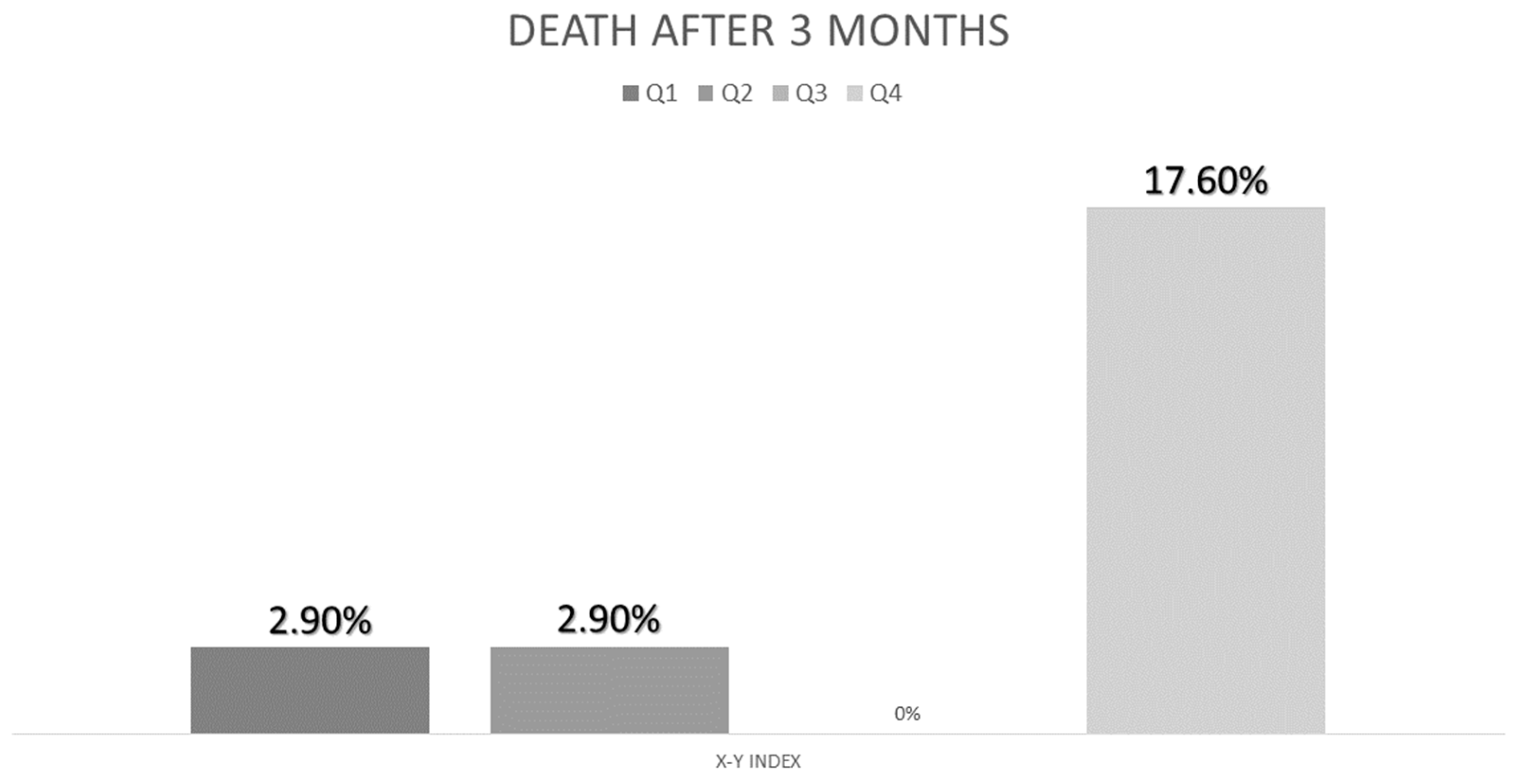
3.5. Relationship of Nutritional Ultrasonography with Morbidity
4. Discussion
4.1. Use of Nutritional Ultrasonography in Disease-Related Malnutrition
4.2. Nutritional Ultrasonography and Diagnosis of Sarcopenia
4.3. Nutritional Ultrasonography in Morphofunctional Assessment
4.4. Nutritional Ultrasonography and Complications in DRE
4.5. Strengths and Limitations
4.6. Future Lines of Investigation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Álvarez Hernández, J.; Planas Vila, M.; León-Sanz, M.; García de Lorenzo, A.; Celaya-Pérez, S.; García-Lorda, P.; Araujo, K.; Sarto Guerri, B.; on behalf of the PREDyCES® Researches. Prevalencia y costes de la malnutrición en pacientes hospitalizados; estudio predyces. Nutr. Hosp. 2012, 27, 1049–1059. [Google Scholar] [CrossRef] [PubMed]
- Merker, M.; Felder, M.; Gueissaz, L.; Bolliger, R.; Tribolet, P.; Kägi-Braun, N.; Gomes, F.; Hoess, C.; Pavlicek, V.; Bilz, S.; et al. Association of Baseline Inflammation with Effectiveness of Nutritional Support Among Patients with Disease-Related Malnutrition: A Secondary Analysis of a Randomized Clinical Trial. JAMA Netw. Open 2020, 3, e200663. [Google Scholar] [CrossRef] [PubMed]
- Kaegi-Braun, N.; Boesiger, F.; Tribolet, P.; Gomes, F.; Kutz, A.; Hoess, C.; Pavlicek, V.; Bilz, S.; Sigrist, S.; Brändle, M.; et al. Validation of modified GLIM criteria to predict adverse clinical outcome and response to nutritional treatment: A secondary analysis of a randomized clinical trial. Clin. Nutr. 2022, 41, 795–804. [Google Scholar] [CrossRef] [PubMed]
- León-Sanz, M.; Brosa, M.; Planas, M.; García-de-Lorenzo, A.; Celaya-Pérez, S.; Hernández, J.Á. PREDyCES study: The cost of hospital malnutrition in Spain. Nutrition 2015, 31, 1096–1102. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Gingrich, A.; Volkert, D.; Kiesswetter, E.; Thomanek, M.; Bach, S.; Sieber, C.C.; Zopf, Y. Prevalence and overlap of sarcopenia, frailty, cachexia and malnutrition in older medical inpatients. BMC Geriatr. 2019, 19, 120. [Google Scholar] [CrossRef]
- Park, B.; Bhat, S.; Xia, W.; Barazanchi, A.W.; Frampton, C.; Hill, A.G.; MacCormick, A.D. Consensus-defined sarcopenia predicts adverse outcomes after elective abdominal surgery: Meta-analysis. BJS Open 2023, 7, zrad065. [Google Scholar] [CrossRef]
- Jensen, S.; Bloch, Z.; Quist, M.; Hansen, T.T.D.; Johansen, C.; Pappot, H.; Suetta, C.; Skjødt Rafn, B. Sarcopenia and loss of muscle mass in patients with lung cancer undergoing chemotherapy treatment: A systematic review and meta-analysis. Acta Oncol. 2023, 62, 318–328. [Google Scholar] [CrossRef]
- Mazeaud, S.; Zupo, R.; Couret, A.; Panza, F.; Sardone, R.; Castellana, F. Prevalence of Sarcopenia in Liver Cirrhosis: A Systematic Review and Meta-Analysis. Clin. Transl. Gastroenterol. 2023, 14, e00584. [Google Scholar] [CrossRef]
- Chan, H.C.N.; Fei, X.; Leung, E.L.Y.; Langston, K.; Marshall, S.; van der Meij, B.S. Post-discharge consequences of protein-energy malnutrition, sarcopenia, and frailty in older adults admitted to rehabilitation: A systematic review. Clin. Nutr. ESPEN 2023, 54, 382–397. [Google Scholar] [CrossRef]
- Schuetz, P.; Fehr, R.; Baechli, V.; Geiser, M.; Deiss, M.; Gomes, F.; Kutz, A.; Tribolet, P.; Bregenzer, T.; Braun, N.; et al. Individualised nutritional support in medical inpatients at nutritional risk: A randomised clinical trial. Lancet 2019, 393, 2312–2321. [Google Scholar] [CrossRef]
- García-Almeida, J.M.; García-García, C.; Ballesteros-Pomar, M.D.; Olveira, G.; Lopez-Gomez, J.J.; Bellido, V.; Bretón Lesmes, I.; Burgos, R.; Sanz-Paris, A.; Matia-Martin, P.; et al. Expert Consensus on Morphofunctional Assessment in Disease-Related Malnutrition. Grade Review and Delphi Study. Nutrients 2023, 15, 612. [Google Scholar] [CrossRef] [PubMed]
- Barazzoni, R.; Jensen, G.L.; Correia, M.I.T.; Gonzalez, M.C.; Higashiguchi, T.; Shi, H.P.; Bischoff, S.C.; Boirie, Y.; Carrasco, F.; Cruz-Jentoft, A.; et al. Guidance for assessment of the muscle mass phenotypic criterion for the Global Leadership Initiative on Malnutrition (GLIM) diagnosis of malnutrition. Clin. Nutr. 2022, 41, 1425–1433. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Socorro, C.R.; Saavedra, P.; López-Fernández, J.C.; Ruiz-Santana, S. Assessment of Muscle Wasting in Long-Stay ICU Patients Using a New Ultrasound Protocol. Nutrients 2018, 10, 1849. [Google Scholar] [CrossRef] [PubMed]
- García-Almeida, J.M.; García-García, C.; Vegas-Aguilar, I.M.; Pomar, M.D.B.; Cornejo-Pareja, I.M.; Medina, B.F.; de Luis Román, D.A.; Guerrero, D.B.; Lesmes, I.B.; Madueño, F.J.T. Nutritional ultrasound®: Conceptualisation, technical considerations and standardisation. Endocrinol. Diabetes Nutr. 2022, 70, 74–84. [Google Scholar] [CrossRef]
- Fischer, A.; Hertwig, A.; Hahn, R.; Anwar, M.; Siebenrock, T.; Pesta, M.; Liebau, K.; Timmermann, I.; Brugger, J.; Posch, M.; et al. Validation of bedside ultrasound to predict lumbar muscle area in the computed tomography in 200 non-critically ill patients: The USVALID prospective study. Clin. Nutr. 2022, 41, 829–837. [Google Scholar] [CrossRef]
- LóLópez-Gómez, J.J.; Benito-Sendín Plaar, K.; Izaola-Jauregui, O.; Primo-Martín, D.; Gómez-Hoyos, E.; Torres-Torres, B.; De Luis-Román, D.A. Muscular Ultrasonography in Morphofunctional Assessment of Patients with Oncological Pathology at Risk of Malnutrition. Nutrients 2022, 14, 1573. [Google Scholar] [CrossRef]
- Cederholm, T.; Jensen, G.L.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.J.S.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. Clin. Nutr. 2019, 38, 207–217. [Google Scholar] [CrossRef]
- Canda, A.S. Variables Antropométricas de la Población Deportista Española; Consejo Superior de Deportes, Servicio de Documentación y Publicaciones: Madrid, Spain, 2012. [Google Scholar]
- Bellido, D.; García-García, C.; Talluri, A.; Lukaski, H.C.; García-Almeida, J.M. Future lines of research on phase angle: Strengths and limitations. Rev. Endocr. Metab. Disord. 2023, 24, 563–583. [Google Scholar] [CrossRef]
- Sergi, G.; De Rui, M.; Veronese, N.; Bolzetta, F.; Berton, L.; Carraro, S.; Bano, G.; Coin, A.; Manzato, E.; Perissinotto, E. Assessing appendicular skeletal muscle mass with bioelectrical impedance analysis in free-living Caucasian older adults. Clin. Nutr. 2015, 34, 667–673. [Google Scholar] [CrossRef]
- Schneider, C.A.; Rasband, W.S.; Eliceiri, K.W. NIH Image to ImageJ: 25 years of image analysis. Nat. Methods 2012, 9, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Ballesteros-Pomar, M.D.; Gajete-Martín, L.M.; Pintor-De-La-Maza, B.; González-Arnáiz, E.; González-Roza, L.; García-Pérez, M.P.; González-Alonso, V.; García-González, M.A.; de Prado-Espinosa, R.; Cuevas, M.J.; et al. Disease-Related Malnutrition and Sarcopenia Predict Worse Outcome in Medical Inpatients: A Cohort Study. Nutrients 2021, 13, 2937. [Google Scholar] [CrossRef] [PubMed]
- Riesgo, H.; Castro, A.; Del Amo, S.; San Ceferino, M.J.; Izaola, O.; Primo, D.; Gomez Hoyos, E.; Lopez Gomez, J.J.; de Luis, D.A. Prevalence of Risk of Malnutrition and Risk of Sarcopenia in a Reference Hospital for COVID-19, Relationship with Mortality. Ann. Nutr. Metab. 2021, 77, 324–329. [Google Scholar] [CrossRef]
- Campa, F.; Coratella, G.; Cerullo, G.; Stagi, S.; Paoli, S.; Marini, S.; Grigoletto, A.; Moroni, A.; Petri, C.; Andreoli, A.; et al. New bioelectrical impedance vector references and phase angle centile curves in 4367 adults: The need for an urgent update after 30 years. Clin. Nutr. 2023, 42, 1749–1758. [Google Scholar] [CrossRef]
- Arts, I.M.P.; Pillen, S.; Schelhaas, H.J.; Overeem, S.; Zwarts, M.J. Normal values for quantitative muscle ultrasonography in adults. Muscle Nerve 2010, 41, 32–41. [Google Scholar] [CrossRef]
- Cannataro, R.; Carbone, L.; Petro, J.L.; Cione, E.; Vargas, S.; Angulo, H.; Forero, D.A.; Odriozola-Martínez, A.; Kreider, R.B.; Bonilla, D.A. Sarcopenia: Etiology, Nutritional Approaches, and miRNAs. Int. J. Mol. Sci. 2021, 22, 9724. [Google Scholar] [CrossRef] [PubMed]
- Li, C.-W.; Yu, K.; Shyh-Chang, N.; Li, G.-X.; Jiang, L.-J.; Yu, S.-L.; Xu, L.-Y.; Liu, R.-J.; Guo, Z.-J.; Xie, H.-Y.; et al. Circulating factors associated with sarcopenia during ageing and after intensive lifestyle intervention. J. Cachexia Sarcopenia Muscle 2019, 10, 586–600. [Google Scholar] [CrossRef]
- Sáez Moreno, M.Á.; Jiménez Lorenzo, R.; Lueso Moreno, M.; López-Torres Hidalgo, J. Prevalence of dynapenia in patients over 65 years. Aten Primaria 2018, 50, 567–568. [Google Scholar] [CrossRef]
- Nijholt, W.; Scafoglieri, A.; Jager-Wittenaar, H.; Hobbelen, J.S.M.; van der Schans, C.P. The reliability and validity of ultrasound to quantify muscles in older adults: A systematic review. J. Cachexia Sarcopenia Muscle 2017, 8, 702–712. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Torralvo, F.J.; Porras, N.; Ruiz-García, I.; Maldonado-Araque, C.; García-Olivares, M.; Girón, M.V.; Gonzalo-Marín, M.; Olveira, C.; Olveira, G. Usefulness of Muscle Ultrasonography in the Nutritional Assessment of Adult Patients with Cystic Fibrosis. Nutrients 2022, 14, 3377. [Google Scholar] [CrossRef]
- Rustani, K.; Kundisova, L.; Capecchi, P.L.; Nante, N.; Bicchi, M. Ultrasound measurement of rectus femoris muscle thickness as a quick screening test for sarcopenia assessment. Arch. Gerontol. Geriatr. 2019, 83, 151–154. [Google Scholar] [CrossRef] [PubMed]
- BBot, D.; Lucassen, C.; Werkman, M.; van Dijk, S.; Feshtali, S.S.; Tushuizen, M.E.; van Hoek, B. Skeletal muscle mass in patients with end-stage liver disease: Not only muscle size but especially muscle quality matters in relation to physical fitness. Clin. Nutr. ESPEN 2023, 55, 407–413. [Google Scholar] [CrossRef]
- Bunout, D.; Gonzalez, S.; Canales, M.; Barrera, G.; Hirsch, S. Ultrasound assessment of rectus femoris pennation angle and echogenicity. Their association with muscle functional measures and fat infiltration measured by CT scan. Clin. Nutr. ESPEN 2023, 55, 420–424. [Google Scholar] [CrossRef] [PubMed]
- Arai, Y.; Nakanishi, N.; Ono, Y.; Inoue, S.; Kotani, J.; Harada, M.; Oto, J. Ultrasound assessment of muscle mass has potential to identify patients with low muscularity at intensive care unit admission: A retrospective study. Clin. Nutr. ESPEN 2021, 45, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Primo, D.; Izaola, O.; Gómez, J.J.L.; de Luis, D. Correlation of the Phase Angle with Muscle Ultrasound and Quality of Life in Obese Females. Dis. Markers 2022, 2022, 7165126. [Google Scholar] [CrossRef]
- García-García, C.; Vegas-Aguilar, I.M.; Rioja-Vázquez, R.; Cornejo-Pareja, I.; Tinahones, F.J.; García-Almeida, J.M. Rectus Femoris Muscle and Phase Angle as Prognostic Factor for 12-Month Mortality in a Longitudinal Cohort of Patients with Cancer (AnyVida Trial). Nutrients 2023, 15, 522. [Google Scholar] [CrossRef]
- Geng, J.; Wei, Y.; Xue, Q.; Deng, L.; Wang, J. Phase angle is a useful bioelectrical marker for skeletal muscle quantity and quality in hospitalized elderly patients. Medicine 2022, 101, e31646. [Google Scholar] [CrossRef]
- Bourgeois, B.; Fan, B.; Johannsen, N.; Gonzalez, M.C.; Ng, B.K.; Sommer, M.J.; Shepherd, J.A.; Heymsfield, S.B. Improved strength prediction combining clinically available measures of skeletal muscle mass and quality. J. Cachexia Sarcopenia Muscle 2019, 10, 84–94. [Google Scholar] [CrossRef]
- Casey, P.; Alasmar, M.; McLaughlin, J.; Ang, Y.; McPhee, J.; Heire, P.; Sultan, J. The current use of ultrasound to measure skeletal muscle and its ability to predict clinical outcomes: A systematic review. J. Cachexia Sarcopenia Muscle 2022, 13, 2298–2309. [Google Scholar] [CrossRef]
- Stock, M.S.; Thompson, B.J. Echo intensity as an indicator of skeletal muscle quality: Applications, methodology, and future directions. Eur. J. Appl. Physiol. 2021, 121, 369–380. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Men | Women | p-Value | |
|---|---|---|---|---|
| Anthropometry | ||||
| BMI (kg/m2) | 21.79 (4.61) | 23.99 (4.62) | 20.31 (4.01) | <0.01 |
| Age (years) | 61.4 (17.34) | 64.91 (14.70) | 60.71 (18.80) | 0.15 |
| %weight loss | 11.84 (9.44) | 10.42 (7.38) | 12.88 (10.63) | 0.15 |
| Arm Circumference (cm) | 23.07 (2.98) | 24.73 (2.92) | 21.97 (2.47) | <0.01 |
| Calf circumference (cm) | 31.03 (3.42) | 32.47 (3.69) | 30.06 (2.86) | <0.01 |
| Bioelectrical Impedanciometry | ||||
| Resistance (ohm) | 595.81 (110.42) | 531.03 (98.38) | 638.73 (96.51) | <0.01 |
| Reactance (ohm) | 50.58 (11.76) | 46.46 (12.17) | 53.32 (10.69) | <0.01 |
| Phase Angle (°) | 4.86 (0.83) | 4.99 (0.88) | 4.78 (0.79) | 0.15 |
| ASMI (kg/m2) | 5.88 (1.09) | 6.77 (0.96) | 5.30 (0.71) | <0.01 |
| MMI (kg/m2) | 9.69 (1.78) | 10.75 (1.73) | 9.02 (1.47) | <0.01 |
| Nutritional Ultrasonography | ||||
| MCRFI (cm/m2) | 3.33 (0.61) | 3.19 (0.63) | 3.41 (0.59) | 0.03 |
| MARFI (cm2/m2) | 1.21 (0.43) | 1.22 (0.51) | 1.21 (0.38) | 0.81 |
| X-Y index | 3.56 (1.35) | 3.46 (1.37) | 3.61 (1.35) | 0.54 |
| Echogenicity (%) | 36.68 (9.70) | 32.79 (9.42) | 39.16 (9.09) | <0.01 |
| Muscle Strength | ||||
| Handgrip strength (kg) | 20.28 (7.57) | 24.82 (7.93) | 17.15 (0.59) | <0.01 |
| Sarcopenia | No Sarcopenia | p-Value | |
|---|---|---|---|
| SEX (%M/%W) | 36.2%/32.1% | 63.8%/67.9% | 0.72 |
| Anthropometry | |||
| BMI (kg/m2) | 20.07 (3.49) | 22.73 (4.89) | <0.01 |
| Age (years) | 67.92 (13.56) | 59.62 (18.59) | <0.01 |
| %weight loss | 13.83 (11.14) | 10.76 (8.35) | 0.09 |
| Arm Circumference (cm) | 22.31 (2.08) | 23.49 (3.28) | 0.03 |
| Calf circumference (cm) | 29.57 (2.69) | 31.83 (3.53) | <0.01 |
| Bioelectrical Impedanciometry | |||
| Resistance (ohm) | 641 (0.49) | 569.53 (110.39) | <0.01 |
| Reactance (ohm) | 50.06 (9.07) | 50.94 (13.02) | 0.68 |
| Phase Angle (°) | 4.47 (0.79) | 5.09 (0.84) | <0.01 |
| ASMI (kg/m2) | 5.40 (0.76) | 6.16 (1.13) | <0.01 |
| MMI (kg/m2) | 8.69 (1.29) | 10.26 (1.75) | <0.01 |
| Nutritional Ultrasonography | |||
| MCRFI (cm/m2) | 3.31 (0.55) | 3.34 (0.64) | 0.82 |
| MARFI (cm2/m2) | 1.09 (0.39) | 1.27 (0.45) | 0.02 |
| X-Y index | 4.12 (1.28) | 3.29 (1.32) | <0.01 |
| Echogenicity (%) | 38.13 (10.72) | 36.07 (9.12) | 0.27 |
| Muscle Strength | |||
| Handgrip strength (kg) | 15.07 (5.85) | 22.94 (6.96) | <0.01 |
| Dynapenia | No Dynapenia | p-Value | Low Muscle Mass | No Low Muscle Mass | p-Value | |
|---|---|---|---|---|---|---|
| Anthropometry | ||||||
| BMI (kg/m2) | 22.29 (4.69) | 21.34 (4.55) | 0.22 | 19.76 (3.68) | 25.61 (3.69) | <0.01 |
| Age (years) | 68.19 (14.27) | 56.15 (18.52) | <0.01 | 59.66 (18.33) | 67.56 (14.08) | <0.01 |
| %weight loss | 11.93 (10.01) | 11.52 (8.78) | 0.81 | 13.23 (9.68) | 9.55 (8.64) | 0.03 |
| Arm Circumference (cm) | 23.53 (3.01) | 22.64 (2.89) | 0.08 | 21.94 (2.39) | 25.16 (2.83) | <0.01 |
| Calf circumference (cm) | 30.91 (3.58) | 31.23 (3.28) | 0.57 | 29.87 (2.99) | 33.22 (3.12) | <0.01 |
| Bioelectrical Impedanciometry | ||||||
| Resistance (ohm) | 589.58 (110.45) | 597.81 (108.62) | 0.64 | 647.66 (89.31) | 499.36 (75.92) | <0.01 |
| Reactance (ohm) | 47.37 (10.16) | 54.17 (12.53) | <0.01 | 53.51 (11.21) | 45.14 (10.88) | <0.01 |
| Phase Angle (°) | 4.61 (0.74) | 5.17 (0.81) | <0.01 | 4,71 (0.77) | 5.14 (0.88) | <0.01 |
| ASMI (kg/m2) | 5.94 (1.13) | 5.87 (1.03) | 0.68 | 5.35 (0.71) | 6.88 (0.98) | <0.01 |
| MMI (kg/m2) | 9.63 (1.84) | 9.85 (1.69) | 0.47 | 8.77 (1.21) | 11.40 (1.36) | <0.01 |
| Nutritional Ultrasonography | ||||||
| MCRFI (cm/m2) | 3.31 (0.61) | 3.36 (0.62) | 0.62 | 3.27 (0.61) | 3.43 (0.61) | 0.13 |
| MARFI (cm2/m2) | 1.15 (0.45) | 1.29 (0.41) | 0.04 | 1.17 (0.42) | 1.30 (0.45) | 0.08 |
| X-Y index | 3.76 (1.41) | 3.35 (1.28) | 0.08 | 3.69 (1.30) | 3.31 (1.43) | 0.12 |
| Echogenicity (%) | 38.70 (10.35) | 34.59 (8.49) | 0.02 | 34.94 (9.58) | 39.83 (9.21) | <0.01 |
| Muscle Strength | ||||||
| Handgrip strength (kg) | 16.02 (6.02) | 24.91 (6.29) | <0.01 | 19.78 (7.72) | 21.19 (7.28) | 0.29 |
| Echogenicity | Marfi | X-Y Index | |
|---|---|---|---|
| Arm Circumference (cm) | r = 0.05; p = 0.55 | r = 0.05; p = 0.55 | r = −0.03; p = 0.75 |
| Calf Circumference (cm) | r = 0.07; p = 0.41 | r = 0.13; p = 0.12 | r = −0.04; p = 0.62 |
| ASMI (kg/m2) | r = −0.05; p = 0.56 | r = 0.17; p = 0.04 * | r = −0.11; p = 0.19 |
| MMI (kg/m2) | r = −0.03; p = 0.76 | r = 0.25; p < 0.01 * | r = −0.23; p < 0.01 * |
| Resistance (ohm) | r = −0.03; p = 0.71 | r = −0.17; p = 0.04 * | r = −0.03; p = 0.74 |
| Reactance (ohm) | r = −0.21; p = 0.02 * | r = 0.12; p = 0.15 | r = −0.31; p < 0.01 * |
| Phase Angle (°) | r = −0.23; p = 0.01 * | r = 0.35; p < 0.01 * | r = −0.42; p < 0.01 * |
| Handgrip Strength (kg) | r = −0.36; p < 0.01 * | r = 0.13; p = 0.13 | r = −0.18; p = 0.04 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Gómez, J.J.; García-Beneitez, D.; Jiménez-Sahagún, R.; Izaola-Jauregui, O.; Primo-Martín, D.; Ramos-Bachiller, B.; Gómez-Hoyos, E.; Delgado-García, E.; Pérez-López, P.; De Luis-Román, D.A. Nutritional Ultrasonography, a Method to Evaluate Muscle Mass and Quality in Morphofunctional Assessment of Disease Related Malnutrition. Nutrients 2023, 15, 3923. https://doi.org/10.3390/nu15183923
López-Gómez JJ, García-Beneitez D, Jiménez-Sahagún R, Izaola-Jauregui O, Primo-Martín D, Ramos-Bachiller B, Gómez-Hoyos E, Delgado-García E, Pérez-López P, De Luis-Román DA. Nutritional Ultrasonography, a Method to Evaluate Muscle Mass and Quality in Morphofunctional Assessment of Disease Related Malnutrition. Nutrients. 2023; 15(18):3923. https://doi.org/10.3390/nu15183923
Chicago/Turabian StyleLópez-Gómez, Juan José, David García-Beneitez, Rebeca Jiménez-Sahagún, Olatz Izaola-Jauregui, David Primo-Martín, Beatriz Ramos-Bachiller, Emilia Gómez-Hoyos, Esther Delgado-García, Paloma Pérez-López, and Daniel A. De Luis-Román. 2023. "Nutritional Ultrasonography, a Method to Evaluate Muscle Mass and Quality in Morphofunctional Assessment of Disease Related Malnutrition" Nutrients 15, no. 18: 3923. https://doi.org/10.3390/nu15183923
APA StyleLópez-Gómez, J. J., García-Beneitez, D., Jiménez-Sahagún, R., Izaola-Jauregui, O., Primo-Martín, D., Ramos-Bachiller, B., Gómez-Hoyos, E., Delgado-García, E., Pérez-López, P., & De Luis-Román, D. A. (2023). Nutritional Ultrasonography, a Method to Evaluate Muscle Mass and Quality in Morphofunctional Assessment of Disease Related Malnutrition. Nutrients, 15(18), 3923. https://doi.org/10.3390/nu15183923