
Is There More to Olive Oil than Healthy Lipids?


 and
and
Abstract
:1. Introduction
2. Materials and Methods
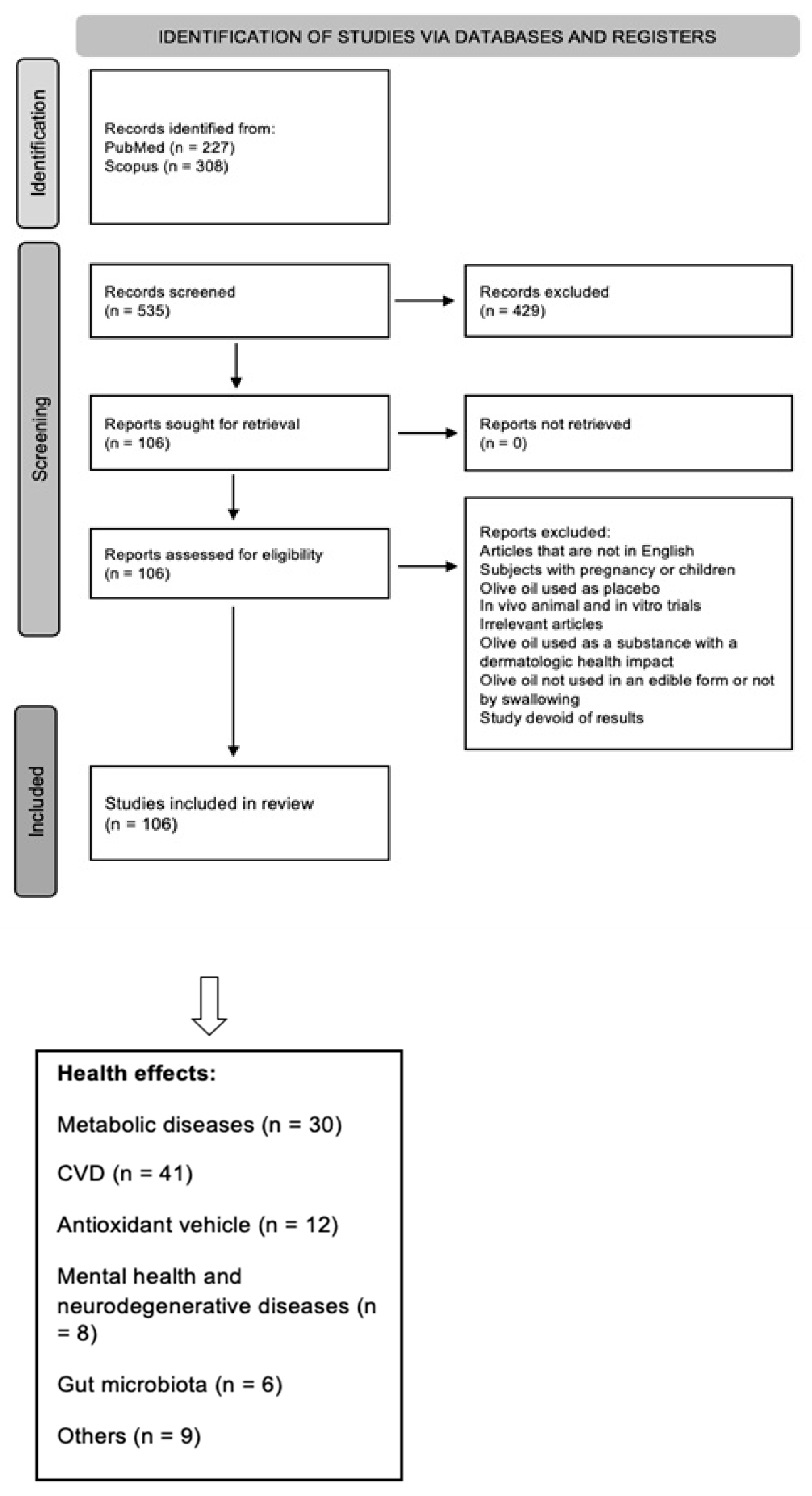
2.1. Bibliographic Search
2.2. Characteristics of the Excluded Studies
3. Results and Discussion
3.1. Olive Oil’s Effects on Metabolic Diseases
3.2. Olive Oil Effects on Cardiovascular Diseases (CVD)
3.3. Olive Oil as an Antioxidant Vehicle
3.4. Olive Oil Effects on Mental Health and Neurodegenerative Diseases
3.5. Olive Oil’s Effects on Gut Microbiota
3.6. Olive Oil’s Effects on Other Health Outcomes
4. Discussion
5. Concluding Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Massaro, M.; Scoditti, E.; Carluccio, M.A.; Calabriso, N.; Santarpino, G.; Verri, T.; De Caterina, R. Effects of Olive Oil on Blood Pressure: Epidemiological, Clinical, and Mechanistic Evidence. Nutrients 2020, 12, 1548. [Google Scholar] [CrossRef] [PubMed]
- Foscolou, A.; Critselis, E.; Panagiotakos, D. Olive Oil Consumption and Human Health: A Narrative Review. Maturitas 2018, 118, 60–66. [Google Scholar] [CrossRef]
- International Olive Council. Designations and Definitions of Olive Oils. Available online: https://www.internationaloliveoil.org/olive-world/olive-oil/ (accessed on 16 June 2023).
- International Olive Council. EU Olive Oil Figures: Consumption. Available online: https://www.internationaloliveoil.org/wp-content/uploads/2021/12/HO-CE901-17-12-2021-C.pdf (accessed on 16 June 2023).
- International Olive Council. EU Olive Oil Figures: Production. Available online: https://www.internationaloliveoil.org/wp-content/uploads/2021/12/HO-CE901-17-12-2021-P.pdf (accessed on 16 June 2023).
- International Olive Council. World Olive Oil Figures: Consumption. Available online: https://www.internationaloliveoil.org/wp-content/uploads/2021/12/HO-W901-17-12-2021-C.pdf (accessed on 16 June 2023).
- International Olive Council. Trade Standard Applying to Olive Oils and Olive Pomace Oils. Reference COI/T.15/NC No 3/Rev. 19. Available online: https://www.internationaloliveoil.org/wp-content/uploads/2022/12/Norme-comerciale-REV-19_ENK.pdf (accessed on 16 June 2023).
- Visioli, F.; Poli, A.; Gall, C. Antioxidant and Other Biological Activities of Phenols from Olives and Olive Oil. Med. Res. Rev. 2002, 22, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Abenavoli, L.; Milanović, M.; Milić, N.; Luzza, F.; Giuffrè, A.M. Olive Oil Antioxidants and Non-Alcoholic Fatty Liver Disease. Expert Rev. Gastroenterol. Hepatol. 2019, 13, 739–749. [Google Scholar] [CrossRef] [PubMed]
- Tomé-Carneiro, J.; Crespo, M.C.; de Las Hazas, M.C.L.; Visioli, F.; Dávalos, A. Olive Oil Consumption and Its Repercussions on Lipid Metabolism. Nutr. Rev. 2020, 78, 952–968. [Google Scholar] [CrossRef]
- Romani, A.; Ieri, F.; Urciuoli, S.; Noce, A.; Marrone, G.; Nediani, C.; Bernini, R. Health Effects of Phenolic Compounds Found in Extra-Virgin Olive Oil, By-Products, and Leaf of Olea Europaea L. Nutrients 2019, 11, 1776. [Google Scholar] [CrossRef]
- Capurso, A.; Crepaldi, G.; Capurso, C. Benefits of the Mediterranean Diet in the Elderly Patient; Springer International Publishing: Cham, Swizerland, 2018. [Google Scholar] [CrossRef]
- Vazquez-Aguilar, A.; Sanchez-Rodriguez, E.; Rodriguez-Perez, C.; Rangel-Huerta, O.D.; Mesa, M.D. Metabolomic-Based Studies of the Intake of Virgin Olive Oil: A Comprehensive Review. Metabolites 2023, 13, 472. [Google Scholar] [CrossRef] [PubMed]
- De Santis, S.; Cariello, M.; Piccinin, E.; Sabbà, C.; Moschetta, A. Extra Virgin Olive Oil: Lesson from Nutrigenomics. Nutrients 2019, 11, 2085. [Google Scholar] [CrossRef]
- Gaforio, J.J.; Visioli, F.; Alarcón-de-la-Lastra, C.; Castañer, O.; Delgado-Rodríguez, M.; Fitó, M.; Hernández, A.F.; Huertas, J.R.; Martínez-González, M.A.; Menendez, J.A.; et al. Virgin Olive Oil and Health: Summary of the III International Conference on Virgin Olive Oil and Health Consensus Report, JAEN (Spain) 2018. Nutrients 2019, 11, 2039. [Google Scholar] [CrossRef]
- Reboredo-Rodríguez, P.; Varela-López, A.; Forbes-Hernández, T.Y.; Gasparrini, M.; Afrin, S.; Cianciosi, D.; Zhang, J.; Manna, P.P.; Bompadre, S.; Quiles, J.L.; et al. Phenolic Compounds Isolated from Olive Oil as Nutraceutical Tools for the Prevention and Management of Cancer and Cardiovascular Diseases. Int. J. Mol. Sci. 2018, 19, 2305. [Google Scholar] [CrossRef]
- Mediterranean Diet inscribed in 2013 on the Representative List of the Intangible Cultural Heritage of Humanity. UNESCO. Available online: https://ich.unesco.org/en/RL/mediterranean-diet-00884 (accessed on 16 June 2023).
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, J.; Fialho, M.; Santos, R.; Peixoto-Plácido, C.; Madeira, T.; Sousa-Santos, N.; Virgolino, A.; Santos, O.; Carneiro, A.V. Is olive oil good for you? A systematic review and meta-analysis on anti-inflammatory benefits from regular dietary intake. Nutrition 2019, 69, 110559. [Google Scholar] [CrossRef] [PubMed]
- Pastor, R.; Bouzas, C.; Tur, J.A. Beneficial effects of dietary supplementation with olive oil, oleic acid, or hydroxytyrosol in metabolic syndrome: Systematic review and meta-analysis. Free. Radic. Biol. Med. 2021, 172, 372–385. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Krause, M.; Schmucker, C.; Hoffmann, G.; Rücker, G.; Meerpohl, J.J. Impact of different types of olive oil on cardiovascular risk factors: A systematic review and network meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 1030–1039. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Lampousi, A.-M.; Portillo, M.P.; Romaguera, D.; Hoffmann, G.; Boeing, H. Olive oil in the prevention and management of type 2 diabetes mellitus: A systematic review and meta-analysis of cohort studies and intervention trials. Nutr. Diabetes 2017, 7, e262. [Google Scholar] [CrossRef]
- Yahay, M.; Heidari, Z.; Allameh, Z.; Amani, R. The Effects of Canola and Olive Oils Consumption Compared to Sunflower Oil, on Lipid Profile and Hepatic Steatosis in Women with Polycystic Ovarian Syndrome: A Randomized Controlled Trial. Lipids Health Dis. 2021, 20, 7. [Google Scholar] [CrossRef] [PubMed]
- Patti, A.M.; Carruba, G.; Cicero, A.F.G.; Banach, M.; Nikolic, D.; Giglio, R.V.; Terranova, A.; Soresi, M.; Giannitrapani, L.; Montalto, G.; et al. Daily Use of Extra Virgin Olive Oil with High Oleocanthal Concentration Reduced Body Weight, Waist Circumference, Alanine Transaminase, Inflammatory Cytokines and Hepatic Steatosis in Subjects with the Metabolic Syndrome: A 2-Month Intervention Study. Metabolites 2020, 10, 392. [Google Scholar] [CrossRef]
- Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Fitó, M.; Chiva-Blanch, G.; Fiol, M.; Gómez-Gracia, E.; Arós, F.; Lapetra, J.; et al. Effect of a High-Fat Mediterranean Diet on Bodyweight and Waist Circumference: A Prespecified Secondary Outcomes Analysis of the PREDIMED Randomised Controlled Trial. Lancet Diabetes Endocrinol. 2019, 7, e6–e17. [Google Scholar] [CrossRef]
- AlKhattaf, N.F.; Alraddadi, A.M.; Aljarbou, M.A.; Arnauti, M.A.; Alfaleh, A.M.; Hammouda, S.A. Determining the Correlation between Olive Oil Consumption, BMI, and Waist Circumference in the Adult Saudi Population. J. Taibah Univ. Med. Sci. 2020, 15, 380–386. [Google Scholar] [CrossRef]
- Silveira, E.A.; De Souza, J.D.; Dos Santos Rodrigues, A.P.; Lima, R.M.; de Souza Cardoso, C.K.; De Oliveira, C. Effects of Extra Virgin Olive Oil (EVOO) and the Traditional Brazilian Diet on Sarcopenia in Severe Obesity: A Randomized Clinical Trial. Nutrients 2020, 12, 1498. [Google Scholar] [CrossRef]
- Monfort-Pires, M.; U-Din, M.; Nogueira, G.A.; de Almeida-Faria, J.; Sidarta-Oliveira, D.; Sant’Ana, M.R.; De Lima-Júnior, J.C.; Cintra, D.E.; de Souza, H.P.; Ferreira, S.R.G.; et al. Short Dietary Intervention with Olive Oil Increases Brown Adipose Tissue Activity in Lean but Not Overweight Subjects. J. Clin. Endocrinol. Metab. 2021, 106, 472–484. [Google Scholar] [CrossRef] [PubMed]
- Kabiri, A.; Hosseinzadeh-Attar, M.J.; Haghighatdoost, F.; Eshraghian, M.; Esmaillzadeh, A. Impact of Olive Oil-Rich Diet on Serum Omentin and Adiponectin Levels: A Randomized Cross-over Clinical Trial among Overweight Women. Int. J. Food Sci. Nutr. 2017, 68, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Martinussen, C.; Dirksen, C.; Bojsen-Møller, K.N.; Svane, M.S.; Carlsson, E.R.; Hartmann, B.; Clausen, T.R.; Veedfald, S.; Kristiansen, V.B.; Rehfeld, J.F.; et al. Intestinal Sensing and Handling of Dietary Lipids in Gastric Bypass–Operated Patients and Matched Controls. Am. J. Clin. Nutr. 2020, 111, 28–41. [Google Scholar] [CrossRef]
- Giezenaar, C.; Lange, K.; Hausken, T.; Jones, K.; Horowitz, M.; Chapman, I.; Soenen, S. Acute Effects of Substitution, and Addition, of Carbohydrates and Fat to Protein on Gastric Emptying, Blood Glucose, Gut Hormones, Appetite, and Energy Intake. Nutrients 2018, 10, 1451. [Google Scholar] [CrossRef]
- Pintó, X.; Fanlo-Maresma, M.; Corbella, E.; Corbella, X.; Mitjavila, M.T.; Moreno, J.J.; Casas, R.; Estruch, R.; Corella, D.; Bulló, M.; et al. A Mediterranean Diet Rich in Extra-Virgin Olive Oil Is Associated with a Reduced Prevalence of Nonalcoholic Fatty Liver Disease in Older Individuals at High Cardiovascular Risk. J. Nutr. 2019, 149, 1920–1929. [Google Scholar] [CrossRef]
- Rezaei, S.; Akhlaghi, M.; Sasani, M.R.; Boldaji, R.B. Olive Oil Lessened Fatty Liver Severity Independent of Cardiometabolic Correction in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized Clinical Trial. Nutrition 2019, 57, 154–161. [Google Scholar] [CrossRef]
- Shidfar, F.; Bahrololumi, S.S.; Doaei, S.; Mohammadzadeh, A.; Gholamalizadeh, M.; Mohammadimanesh, A. The Effects of Extra Virgin Olive Oil on Alanine Aminotransferase, Aspartate Aminotransferase, and Ultrasonographic Indices of Hepatic Steatosis in Nonalcoholic Fatty Liver Disease Patients Undergoing Low Calorie Diet. Can. J. Gastroenterol. Hepatol. 2018, 2018, 1053710. [Google Scholar] [CrossRef]
- Carnevale, R.; Loffredo, L.; Del Ben, M.; Angelico, F.; Nocella, C.; Petruccioli, A.; Bartimoccia, S.; Monticolo, R.; Cava, E.; Violi, F. Extra Virgin Olive Oil Improves Post-Prandial Glycemic and Lipid Profile in Patients with Impaired Fasting Glucose. Clin. Nutr. 2017, 36, 782–787. [Google Scholar] [CrossRef]
- Bozzetto, L.; Alderisio, A.; Clemente, G.; Giorgini, M.; Barone, F.; Griffo, E.; Costabile, G.; Vetrani, C.; Cipriano, P.; Giacco, A.; et al. Gastrointestinal Effects of Extra-Virgin Olive Oil Associated with Lower Postprandial Glycemia in Type 1 Diabetes. Clin. Nutr. 2019, 38, 2645–2651. [Google Scholar] [CrossRef] [PubMed]
- Galang, D.G.; Isidro, M.J.; Gonzales, M.C.; Macabuag-Oliva, A. Extra Virgin Olive Oil and Postprandial Blood Glucose in Type 2 Diabetes Mellitus Patients: A Randomized Controlled Cross-over Trial. Philipp. J. Intern. Med. 2020, 58, 24–29. [Google Scholar]
- Silveira, E.A.; de Souza Rosa, L.P.; de Resende, D.P.; Dos Santos Rodrigues, A.P.; da Costa, A.C.; de Oliveira Rezende, A.T.; Noll, M.; de Oliveira, C.; Junqueira-Kipnis, A.P. Positive Effects of Extra-Virgin Olive Oil Supplementation and DietBra on Inflammation and Glycemic Profiles in Adults with Type 2 Diabetes and Class II/III Obesity: A Randomized Clinical Trial. Front. Endocrinol. 2022, 13, 841971. [Google Scholar] [CrossRef] [PubMed]
- Wijayanthie, N.; Gunarti, D.R.; Manikam, N.R. Yulhasri Effects of Extra Virgin Olive Oil Versus Rice Bran Oil on Glycemic Control in Patients with Type-2 Diabetes Mellitus. Int. J. Appl. Pharm. 2019, 11, 56–59. [Google Scholar] [CrossRef]
- Sun, G.; Xia, H.; Yang, Y.; Ma, S.; Zhou, H.; Shu, G.; Wang, S.; Yang, X.; Tang, H.; Wang, F.; et al. Effects of Palm Olein and Olive Oil on Serum Lipids in a Chinese Population: A Randomized, Double-Blind, Cross-over Trial. Asia Pac. J. Clin. Nutr. 2018, 27, 572–580. [Google Scholar] [CrossRef] [PubMed]
- Mandøe, M.J.; Hansen, K.B.; Windeløv, J.A.; Knop, F.K.; Rehfeld, J.F.; Rosenkilde, M.M.; Holst, J.J.; Hansen, H.S. Comparing Olive Oil and C4-Dietary Oil, a Prodrug for the GPR119 Agonist, 2-Oleoyl Glycerol, Less Energy Intake of the Latter Is Needed to Stimulate Incretin Hormone Secretion in Overweight Subjects with Type 2 Diabetes. Nutr. Diabetes 2018, 8, 2. [Google Scholar] [CrossRef] [PubMed]
- Del Ben, M.; Nocella, C.; Loffredo, L.; Bartimoccia, S.; Cammisotto, V.; Mancinella, M.; Angelico, F.; Valenti, V.; Cavarretta, E.; Carnevale, R.; et al. Oleuropein-Enriched Chocolate by Extra Virgin Olive Oil Blunts Hyperglycaemia in Diabetic Patients: Results from a One-Time 2-Hour Post-Prandial Cross over Study. Clin. Nutr. 2020, 39, 2187–2191. [Google Scholar] [CrossRef]
- Tuccinardi, D.; Di Mauro, A.; Lattanzi, G.; Rossini, G.; Monte, L.; Beato, I.; Spiezia, C.; Bravo, M.; Watanabe, M.; Soare, A.; et al. An Extra Virgin Olive Oil-enriched Chocolate Spread Positively Modulates Insulin-resistance Markers Compared with a Palm Oil-enriched One in Healthy Young Adults: A Double-blind, Cross-over, Randomised Controlled Trial. Diabetes Metab. Res. Rev. 2022, 38, e3492. [Google Scholar] [CrossRef]
- Santos-Lozano, J.M.; Rada, M.; Lapetra, J.; Guinda, Á.; Jiménez-Rodríguez, M.C.; Cayuela, J.A.; Ángel-Lugo, A.; Vilches-Arenas, Á.; Gómez-Martín, A.M.; Ortega-Calvo, M.; et al. Prevention of Type 2 Diabetes in Prediabetic Patients by Using Functional Olive Oil Enriched in Oleanolic Acid: The PREDIABOLE Study, a Randomized Controlled Trial. Diabetes Obes. Metab. 2019, 21, 2526–2534. [Google Scholar] [CrossRef]
- Errazuriz, I.; Dube, S.; Slama, M.; Visentin, R.; Nayar, S.; O’Connor, H.; Cobelli, C.; Das, S.K.; Basu, A.; Kremers, W.K.; et al. Randomized Controlled Trial of a MUFA or Fiber-Rich Diet on Hepatic Fat in Prediabetes. J. Clin. Endocrinol. Metab. 2017, 102, 1765–1774. [Google Scholar] [CrossRef]
- Basterra-Gortari, F.J.; Ruiz-Canela, M.; Martínez-González, M.A.; Babio, N.; Sorlí, J.V.; Fito, M.; Ros, E.; Gómez-Gracia, E.; Fiol, M.; Lapetra, J.; et al. Effects of a Mediterranean Eating Plan on the Need for Glucose-Lowering Medications in Participants with Type 2 Diabetes: A Subgroup Analysis of the PREDIMED Trial. Diabetes Care 2019, 42, 1390–1397. [Google Scholar] [CrossRef]
- Ruiz-Canela, M.; Guasch-Ferré, M.; Toledo, E.; Clish, C.B.; Razquin, C.; Liang, L.; Wang, D.D.; Corella, D.; Estruch, R.; Hernáez, Á.; et al. Plasma Branched Chain/Aromatic Amino Acids, Enriched Mediterranean Diet and Risk of Type 2 Diabetes: Case-Cohort Study within the PREDIMED Trial. Diabetologia 2018, 61, 1560–1571. [Google Scholar] [CrossRef]
- D’Amore, S.; Vacca, M.; Cariello, M.; Graziano, G.; D’Orazio, A.; Salvia, R.; Sasso, R.C.; Sabbà, C.; Palasciano, G.; Moschetta, A. Genes and MiRNA Expression Signatures in Peripheral Blood Mononuclear Cells in Healthy Subjects and Patients with Metabolic Syndrome after Acute Intake of Extra Virgin Olive Oil. Biochim. Biophys. Acta (BBA) Mol. Cell Biol. Lipids 2016, 1861, 1671–1680. [Google Scholar] [CrossRef] [PubMed]
- Khaw, K.-T.; Sharp, S.J.; Finikarides, L.; Afzal, I.; Lentjes, M.; Luben, R.; Forouhi, N.G. Randomised Trial of Coconut Oil, Olive Oil or Butter on Blood Lipids and Other Cardiovascular Risk Factors in Healthy Men and Women. BMJ Open 2018, 8, e020167. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.; Wang, D.; Xia, H.; Wang, F.; Yang, X.; Pan, D.; Wang, S.; Yang, L.; Lu, H.; Shu, G.; et al. A Comparative Study of the Effects of Palm Olein, Cocoa Butter and Extra Virgin Olive Oil on Lipid Profile, Including Low-Density Lipoprotein Subfractions in Young Healthy Chinese People. Int. J. Food Sci. Nutr. 2019, 70, 355–366. [Google Scholar] [CrossRef] [PubMed]
- Mantilla-Escalante, D.C.; Hazas, M.-C.L.d.l.; Crespo, M.C.; Martín-Hernández, R.; Tomé-Carneiro, J.; del Pozo-Acebo, L.; Salas-Salvadó, J.; Bulló, M.; Dávalos, A. Mediterranean Diet Enriched in Extra-Virgin Olive Oil or Nuts Modulates Circulating Exosomal Non-Coding RNAs. Eur. J. Nutr. 2021, 60, 4279–4293. [Google Scholar] [CrossRef]
- Kouli, G.-M.; Panagiotakos, D.B.; Kyrou, I.; Magriplis, E.; Georgousopoulou, E.N.; Chrysohoou, C.; Tsigos, C.; Tousoulis, D.; Pitsavos, C. Olive Oil Consumption and 10-Year (2002–2012) Cardiovascular Disease Incidence: The ATTICA Study. Eur. J. Nutr. 2019, 58, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Guasch-Ferré, M.; Liu, G.; Li, Y.; Sampson, L.; Manson, J.E.; Salas-Salvadó, J.; Martínez-González, M.A.; Stampfer, M.J.; Willett, W.C.; Sun, Q.; et al. Olive Oil Consumption and Cardiovascular Risk in U.S. Adults. J. Am. Coll. Cardiol. 2020, 75, 1729–1739. [Google Scholar] [CrossRef] [PubMed]
- Khandouzi, N.; Zahedmehr, A.; Nasrollahzadeh, J. Effects of Canola or Olive Oil on Plasma Lipids, Lipoprotein-Associated Phospholipase A2 and Inflammatory Cytokines in Patients Referred for Coronary Angiography. Lipids Health Dis. 2020, 19, 183. [Google Scholar] [CrossRef]
- Memon, A.R.; Ghanghro, A.B.; Shaikh, I.A.; Qazi, N.; Ghanghro, I.H.; Shaikh, U. Effects of Olive Oil and Garlic on Serum Cholesterol and Triglycerides Levels in the Patients of Type–II Diabetes Mellitus. J. Liaquat Univ. Med. Health Sci. 2018, 17, 101–105. [Google Scholar] [CrossRef]
- Otrante, A.; Trigui, A.; Walha, R.; Berrougui, H.; Fulop, T.; Khalil, A. Extra Virgin Olive Oil Prevents the Age-Related Shifts of the Distribution of HDL Subclasses and Improves Their Functionality. Nutrients 2021, 13, 2235. [Google Scholar] [CrossRef]
- Campos, V.P.; Portal, V.L.; Markoski, M.M.; Quadros, A.S.; Bersch-Ferreira, Â.C.; Garavaglia, J.; Marcadenti, A. Effects of a Healthy Diet Enriched or Not with Pecan Nuts or Extra-virgin Olive Oil on the Lipid Profile of Patients with Stable Coronary Artery Disease: A Randomised Clinical Trial. J. Hum. Nutr. Diet. 2020, 33, 439–450. [Google Scholar] [CrossRef]
- de Araújo, A.R.; Sampaio, G.R.; da Silva, L.R.; Portal, V.L.; Markoski, M.M.; de Quadros, A.S.; Rogero, M.M.; da Silva Torres, E.A.F.; Marcadenti, A. Effects of Extra Virgin Olive Oil and Pecans on Plasma Fatty Acids in Patients with Stable Coronary Artery Disease. Nutrition 2021, 91–92, 111411. [Google Scholar] [CrossRef] [PubMed]
- Martín-Peláez, S.; Castañer, O.; Konstantinidou, V.; Subirana, I.; Muñoz-Aguayo, D.; Blanchart, G.; Gaixas, S.; de la Torre, R.; Farré, M.; Sáez, G.T.; et al. Effect of Olive Oil Phenolic Compounds on the Expression of Blood Pressure-Related Genes in Healthy Individuals. Eur. J. Nutr. 2017, 56, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Cândido, F.G.; Valente, F.X.; da Silva, L.E.; Coelho, O.G.L.; Peluzio, M.D.C.G.; Alfenas, R.D.C.G. Consumption of Extra Virgin Olive Oil Improves Body Composition and Blood Pressure in Women with Excess Body Fat: A Randomized, Double-Blinded, Placebo-Controlled Clinical Trial. Eur. J. Nutr. 2018, 57, 2445–2455. [Google Scholar] [CrossRef]
- Lee, J.B.; Notay, K.; Klingel, S.L.; Chabowski, A.; Mutch, D.M.; Millar, P.J. Docosahexaenoic Acid Reduces Resting Blood Pressure but Increases Muscle Sympathetic Outflow Compared with Eicosapentaenoic Acid in Healthy Men and Women. Am. J. Physiol. Heart Circ. Physiol. 2019, 316, H873–H881. [Google Scholar] [CrossRef]
- Storniolo, C.E.; Casillas, R.; Bulló, M.; Castañer, O.; Ros, E.; Sáez, G.T.; Toledo, E.; Estruch, R.; Ruiz-Gutiérrez, V.; Fitó, M.; et al. A Mediterranean Diet Supplemented with Extra Virgin Olive Oil or Nuts Improves Endothelial Markers Involved in Blood Pressure Control in Hypertensive Women. Eur. J. Nutr. 2017, 56, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Rodriguez, E.; Lima-Cabello, E.; Biel-Glesson, S.; Fernandez-Navarro, J.; Calleja, M.; Roca, M.; Espejo-Calvo, J.; Gil-Extremera, B.; Soria-Florido, M.; de la Torre, R.; et al. Effects of Virgin Olive Oils Differing in Their Bioactive Compound Contents on Metabolic Syndrome and Endothelial Functional Risk Biomarkers in Healthy Adults: A Randomized Double-Blind Controlled Trial. Nutrients 2018, 10, 626. [Google Scholar] [CrossRef] [PubMed]
- Njike, V.Y.; Ayettey, R.; Treu, J.A.; Doughty, K.N.; Katz, D.L. Post-Prandial Effects of High-Polyphenolic Extra Virgin Olive Oil on Endothelial Function in Adults at Risk for Type 2 Diabetes: A Randomized Controlled Crossover Trial. Int. J. Cardiol. 2021, 330, 171–176. [Google Scholar] [CrossRef]
- Loffredo, L.; Del Ben, M.; Bartimoccia, S.; Castellani, V.; Mancinella, M.; Ciacci, P.; Orlando, F.; Paraninfi, A.; Angelico, F.; Ferro, D.; et al. Chocolate Enriched by Extra Virgin Olive Oil Improves Endothelial Function and Oxidative Stress in Patients with Diabetes. Nutrition 2021, 90, 111270. [Google Scholar] [CrossRef]
- Cutruzzolà, A.; Parise, M.; Vallelunga, R.; Lamanna, F.; Gnasso, A.; Irace, C. Effect of Extra Virgin Olive Oil and Butter on Endothelial Function in Type 1 Diabetes. Nutrients 2021, 13, 2436. [Google Scholar] [CrossRef]
- Rus, A.; Molina, F.; Martínez-Ramírez, M.J.; Aguilar-Ferrándiz, M.E.; Carmona, R.; del Moral, M.L. Effects of Olive Oil Consumption on Cardiovascular Risk Factors in Patients with Fibromyalgia. Nutrients 2020, 12, 918. [Google Scholar] [CrossRef]
- Vignini, A.; Nanetti, L.; Raffaelli, F.; Sabbatinelli, J.; Salvolini, E.; Quagliarini, V.; Cester, N.; Mazzanti, L. Effect of 1-y Oral Supplementation with Vitaminized Olive Oil on Platelets from Healthy Postmenopausal Women. Nutrition 2017, 42, 92–98. [Google Scholar] [CrossRef]
- Zhang, R.; Moscona, A.; Myndzar, K.; Luttrell-Williams, E.; Vanegas, S.; Jay, M.R.; Calderon, K.; Berger, J.S.; Heffron, S.P. More Frequent Olive Oil Intake Is Associated with Reduced Platelet Activation in Obesity. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 3322–3325. [Google Scholar] [CrossRef] [PubMed]
- Daimiel, L.; Micó, V.; Valls, R.M.; Pedret, A.; Motilva, M.J.; Rubió, L.; Fitó, M.; Farrás, M.; Covas, M.I.; Solá, R.; et al. Impact of Phenol-Enriched Virgin Olive Oils on the Postprandial Levels of Circulating MicroRNAs Related to Cardiovascular Disease. Mol. Nutr. Food Res. 2020, 64, 2000049. [Google Scholar] [CrossRef] [PubMed]
- Esquius, L.; Garcia-Retortillo, S.; Balagué, N.; Hristovski, R.; Javierre, C. Physiological- and Performance-Related Effects of Acute Olive Oil Supplementation at Moderate Exercise Intensity. J. Int. Soc. Sports Nutr. 2019, 16, 12. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Papadaki, A.; Martínez-González, M.Á.; Alonso-Gómez, A.; Rekondo, J.; Salas-Salvadó, J.; Corella, D.; Ros, E.; Fitó, M.; Estruch, R.; Lapetra, J.; et al. Mediterranean Diet and Risk of Heart Failure: Results from the PREDIMED Randomized Controlled Trial. Eur. J. Heart Fail. 2017, 19, 1179–1185. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.D.; Hruby, A.; Rosner, B.A.; Willett, W.C.; Sun, Q.; Razquin, C.; Zheng, Y.; Ruiz-Canela, M.; Guasch-Ferré, M.; Corella, D.; et al. Plasma Ceramides, Mediterranean Diet, and Incident Cardiovascular Disease in the PREDIMED Trial (Prevención Con Dieta Mediterránea). Circulation 2017, 135, 2028–2040. [Google Scholar] [CrossRef] [PubMed]
- Hernáez, Á.; Castañer, O.; Elosua, R.; Pintó, X.; Estruch, R.; Salas-Salvadó, J.; Corella, D.; Arós, F.; Serra-Majem, L.; Fiol, M.; et al. Mediterranean Diet Improves High-Density Lipoprotein Function in High-Cardiovascular-Risk Individuals. Circulation 2017, 135, 633–643. [Google Scholar] [CrossRef] [PubMed]
- Hernáez, Á.; Castañer, O.; Goday, A.; Ros, E.; Pintó, X.; Estruch, R.; Salas-Salvadó, J.; Corella, D.; Arós, F.; Serra-Majem, L.; et al. The Mediterranean Diet Decreases LDL Atherogenicity in High Cardiovascular Risk Individuals: A Randomized Controlled Trial. Mol. Nutr. Food Res. 2017, 61, 1601015. [Google Scholar] [CrossRef]
- Toledo, E.; Wang, D.D.; Ruiz-Canela, M.; Clish, C.B.; Razquin, C.; Zheng, Y.; Guasch-Ferré, M.; Hruby, A.; Corella, D.; Gómez-Gracia, E.; et al. Plasma Lipidomic Profiles and Cardiovascular Events in a Randomized Intervention Trial with the Mediterranean Diet. Am. J. Clin. Nutr. 2017, 106, 973–983. [Google Scholar] [CrossRef]
- Sánchez-Quesada, C.; Toledo, E.; González-Mata, G.; Ramos-Ballesta, M.I.; Peis, J.I.; Martínez-González, M.Á.; Salas-Salvadó, J.; Corella, D.; Fitó, M.; Romaguera, D.; et al. Relationship between Olive Oil Consumption and Ankle-Brachial Pressure Index in a Population at High Cardiovascular Risk. Atherosclerosis 2020, 314, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Razquin, C.; Ruiz-Canela, M.; Toledo, E.; Clish, C.B.; Guasch-Ferré, M.; García-Gavilán, J.F.; Wittenbecher, C.; Alonso-Gómez, A.; Fitó, M.; Liang, L.; et al. Circulating Amino Acids and Risk of Peripheral Artery Disease in the PREDIMED Trial. Int. J. Mol. Sci. 2022, 24, 270. [Google Scholar] [CrossRef]
- Fernández-Castillejo, S.; Rubió, L.; Hernáez, Á.; Catalán, Ú.; Pedret, A.; Valls, R.; Mosele, J.I.; Covas, M.; Remaley, A.T.; Castañer, O.; et al. Determinants of HDL Cholesterol Efflux Capacity after Virgin Olive Oil Ingestion: Interrelationships with Fluidity of HDL Monolayer. Mol. Nutr. Food Res. 2017, 61, 1700445. [Google Scholar] [CrossRef] [PubMed]
- Martín-Peláez, S.; Mosele, J.I.; Pizarro, N.; Farràs, M.; de la Torre, R.; Subirana, I.; Pérez-Cano, F.J.; Castañer, O.; Solà, R.; Fernandez-Castillejo, S.; et al. Effect of Virgin Olive Oil and Thyme Phenolic Compounds on Blood Lipid Profile: Implications of Human Gut Microbiota. Eur. J. Nutr. 2017, 56, 119–131. [Google Scholar] [CrossRef] [PubMed]
- Farràs, M.; Fernández-Castillejo, S.; Rubió, L.; Arranz, S.; Catalán, Ú.; Subirana, I.; Romero, M.-P.; Castañer, O.; Pedret, A.; Blanchart, G.; et al. Phenol-Enriched Olive Oils Improve HDL Antioxidant Content in Hypercholesterolemic Subjects. A Randomized, Double-Blind, Cross-over, Controlled Trial. J. Nutr. Biochem. 2018, 51, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Hernáez, Á.; Sanllorente, A.; Castañer, O.; Martínez-González, M.Á.; Ros, E.; Pintó, X.; Estruch, R.; Salas-Salvadó, J.; Corella, D.; Alonso-Gómez, Á.M.; et al. Increased Consumption of Virgin Olive Oil, Nuts, Legumes, Whole Grains, and Fish Promotes HDL Functions in Humans. Mol. Nutr. Food Res. 2019, 63, e1800847. [Google Scholar] [CrossRef]
- Jimenez-Torres, J.; Alcalá-Diaz, J.F.; Torres-Peña, J.D.; Gutierrez-Mariscal, F.M.; Leon-Acuña, A.; Gómez-Luna, P.; Fernández-Gandara, C.; Quintana-Navarro, G.M.; Fernandez-Garcia, J.C.; Perez-Martinez, P.; et al. Mediterranean Diet Reduces Atherosclerosis Progression in Coronary Heart Disease: An Analysis of the CORDIOPREV Randomized Controlled Trial. Stroke 2021, 52, 3440–3449. [Google Scholar] [CrossRef]
- Wu, M.-Y.; Du, M.-H.; Wen, H.; Wang, W.-Q.; Tang, J.; Shen, L.-R. Effects of N-6 PUFA-Rich Soybean Oil, MUFA-Rich Olive Oil and Camellia Seed Oil on Weight and Cardiometabolic Profiles among Chinese Women: A 3-Month Double-Blind Randomized Controlled-Feeding Trial. Food Funct. 2022, 13, 4375–4383. [Google Scholar] [CrossRef]
- Podadera-Herreros, A.; Alcala-Diaz, J.F.; Gutierrez-Mariscal, F.M.; Jimenez-Torres, J.; de la Cruz-Ares, S.; Larriva, A.P.A.-D.; Cardelo, M.P.; Torres-Peña, J.D.; Luque, R.M.; Ordovas, J.M.; et al. Long-Term Consumption of a Mediterranean Diet or a Low-Fat Diet on Kidney Function in Coronary Heart Disease Patients: The CORDIOPREV Randomized Controlled Trial. Clin. Nutr. 2022, 41, 552–559. [Google Scholar] [CrossRef]
- Hosseinabadi, S.M.; Nasrollahzadeh, J. Effects of Diets Rich in Ghee or Olive Oil on Cardiometabolic Risk Factors in Healthy Adults: A Two-Period, Crossover, Randomised Trial. Br. J. Nutr. 2022, 128, 1720–1729. [Google Scholar] [CrossRef]
- Prater, M.C.; Scheurell, A.R.; Paton, C.M.; Cooper, J.A. Blood Lipid Responses to Diets Enriched with Cottonseed Oil Compared with Olive Oil in Adults with High Cholesterol in a Randomized Trial. J. Nutr. 2022, 152, 2060–2071. [Google Scholar] [CrossRef]
- Marrone, G.; Urciuoli, S.; Di Lauro, M.; Ruzzolini, J.; Ieri, F.; Vignolini, P.; Di Daniele, F.; Guerriero, C.; Nediani, C.; Di Daniele, N.; et al. Extra Virgin Olive Oil and Cardiovascular Protection in Chronic Kidney Disease. Nutrients 2022, 14, 4265. [Google Scholar] [CrossRef] [PubMed]
- Hernáez, Á.; Soria-Florido, M.T.; Schröder, H.; Ros, E.; Pintó, X.; Estruch, R.; Salas-Salvadó, J.; Corella, D.; Arós, F.; Serra-Majem, L.; et al. Role of HDL function and LDL atherogenicity on cardiovascular risk: A comprehensive examination. PLoS ONE 2019, 14, e0218533. [Google Scholar] [CrossRef] [PubMed]
- Santangelo, C.; Filesi, C.; Varì, R.; Scazzocchio, B.; Filardi, T.; Fogliano, V.; D’Archivio, M.; Giovannini, C.; Lenzi, A.; Morano, S.; et al. Consumption of Extra-Virgin Olive Oil Rich in Phenolic Compounds Improves Metabolic Control in Patients with Type 2 Diabetes Mellitus: A Possible Involvement of Reduced Levels of Circulating Visfatin. J. Endocrinol. Investig. 2016, 39, 1295–1301. [Google Scholar] [CrossRef]
- Atefi, M.; Pishdad, G.R.; Faghih, S. The Effects of Canola and Olive Oils on Insulin Resistance, Inflammation and Oxidative Stress in Women with Type 2 Diabetes: A Randomized and Controlled Trial. J. Diabetes Metab. Disord. 2018, 17, 85–91. [Google Scholar] [CrossRef]
- Sureda, A.; del Mar Bibiloni, M.; Martorell, M.; Buil-Cosiales, P.; Marti, A.; Pons, A.; Tur, J.A.; Martinez-Gonzalez, M.Á. Mediterranean Diets Supplemented with Virgin Olive Oil and Nuts Enhance Plasmatic Antioxidant Capabilities and Decrease Xanthine Oxidase Activity in People with Metabolic Syndrome: The PREDIMED Study. Mol. Nutr. Food Res. 2016, 60, 2654–2664. [Google Scholar] [CrossRef]
- Sarapis, K.; George, E.S.; Marx, W.; Mayr, H.L.; Willcox, J.; Esmaili, T.; Powell, K.L.; Folasire, O.S.; Lohning, A.E.; Garg, M.; et al. Extra Virgin Olive Oil High in Polyphenols Improves Antioxidant Status in Adults: A Double-Blind, Randomized, Controlled, Cross-over Study (OLIVAUS). Eur. J. Nutr. 2022, 61, 1073–1086. [Google Scholar] [CrossRef]
- Luisi, M.L.E.; Lucarini, L.; Biffi, B.; Rafanelli, E.; Pietramellara, G.; Durante, M.; Vidali, S.; Provensi, G.; Madiai, S.; Gheri, C.F.; et al. Effect of Mediterranean Diet Enriched in High Quality Extra Virgin Olive Oil on Oxidative Stress, Inflammation and Gut Microbiota in Obese and Normal Weight Adult Subjects. Front. Pharmacol. 2019, 10, 1366. [Google Scholar] [CrossRef] [PubMed]
- Longhi, R.; de Carvalho Santos, A.S.E.A.; López-Yerena, A.; Rodrigues, A.P.S.; de Oliveira, C.; Silveira, E.A. The Effectiveness of Extra Virgin Olive Oil and the Traditional Brazilian Diet in Reducing the Inflammatory Profile of Individuals with Severe Obesity: A Randomized Clinical Trial. Nutrients 2021, 13, 4139. [Google Scholar] [CrossRef]
- Sanchez-Rodriguez, E.; Biel-Glesson, S.; Fernandez-Navarro, J.; Calleja, M.; Espejo-Calvo, J.; Gil-Extremera, B.; de la Torre, R.; Fito, M.; Covas, M.-I.; Vilchez, P.; et al. Effects of Virgin Olive Oils Differing in Their Bioactive Compound Contents on Biomarkers of Oxidative Stress and Inflammation in Healthy Adults: A Randomized Double-Blind Controlled Trial. Nutrients 2019, 11, 561. [Google Scholar] [CrossRef]
- Carnevale, R.; Pastori, D.; Nocella, C.; Cammisotto, V.; Bartimoccia, S.; Novo, M.; Del Ben, M.; Farcomeni, A.; Angelico, F.; Violi, F. Gut-Derived Lipopolysaccharides Increase Post-Prandial Oxidative Stress via Nox2 Activation in Patients with Impaired Fasting Glucose Tolerance: Effect of Extra-Virgin Olive Oil. Eur. J. Nutr. 2019, 58, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Hunter, D.J.; James, L.; Hussey, B.; Wadley, A.J.; Lindley, M.R.; Mastana, S.S. Impact of Aerobic Exercise and Fatty Acid Supplementation on Global and Gene-Specific DNA Methylation. Epigenetics 2019, 14, 294–309. [Google Scholar] [CrossRef] [PubMed]
- Foshati, S.; Ghanizadeh, A.; Akhlaghi, M. The Effect of Extra Virgin Olive Oil on Anthropometric Indices, Lipid Profile, and Markers of Oxidative Stress and Inflammation in Patients with Depression, a Double-blind Randomised Controlled Trial. Int. J. Clin. Pract. 2021, 75, e14254. [Google Scholar] [CrossRef] [PubMed]
- Lopresti, A.L.; Hood, S.D.; Drummond, P.D. A Review of Lifestyle Factors That Contribute to Important Pathways Associated with Major Depression: Diet, Sleep and Exercise. J. Affect. Disord. 2013, 148, 12–27. [Google Scholar] [CrossRef]
- Lourida, I.; Soni, M.; Thompson-Coon, J.; Purandare, N.; Lang, I.A.; Ukoumunne, O.C.; Llewellyn, D.J. Mediterranean Diet, Cognitive Function, and Dementia. Epidemiology 2013, 24, 479–489. [Google Scholar] [CrossRef]
- Mazza, E.; Fava, A.; Ferro, Y.; Rotundo, S.; Romeo, S.; Bosco, D.; Pujia, A.; Montalcini, T. Effect of the Replacement of Dietary Vegetable Oils with a Low Dose of Extravirgin Olive Oil in the Mediterranean Diet on Cognitive Functions in the Elderly. J. Transl. Med. 2018, 16, 10. [Google Scholar] [CrossRef]
- de Sousa Canheta, A.B.; de Carvalho Santos, A.S.E.A.; de Souza, J.D.; Silveira, E.A. Traditional Brazilian Diet and Extra Virgin Olive Oil Reduce Symptoms of Anxiety and Depression in Individuals with Severe Obesity: Randomized Clinical Trial. Clin. Nutr. 2021, 40, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Warrior, L.; Weber, K.M.; Daubert, E.; Morris, M.C.; Agarwal, P.; Koralnik, I.J.; French, A.L. Olive Oil Intake Associated with Increased Attention Scores in Women Living with HIV: Findings from the Chicago Women’s Interagency HIV Study. Nutrients 2019, 11, 1759. [Google Scholar] [CrossRef]
- Tsolaki, M.; Lazarou, E.; Kozori, M.; Petridou, N.; Tabakis, I.; Lazarou, I.; Karakota, M.; Saoulidis, I.; Melliou, E.; Magiatis, P. A Randomized Clinical Trial of Greek High Phenolic Early Harvest Extra Virgin Olive Oil in Mild Cognitive Impairment: The MICOIL Pilot Study. J. Alzheimer’s Dis. 2020, 78, 801–817. [Google Scholar] [CrossRef]
- Dimitriadis, S.I.; Lyssoudis, C.; Tsolaki, A.C.; Lazarou, E.; Kozori, M.; Tsolaki, M. Greek High Phenolic Early Harvest Extra Virgin Olive Oil Reduces the Over-Excitation of Information-Flow Based on Dominant Coupling Mode (DoCM) Model in Patients with Mild Cognitive Impairment: An EEG Resting-State Validation Approach. J. Alzheimer’s Dis. 2021, 83, 191–207. [Google Scholar] [CrossRef]
- Tzekaki, E.E.; Papaspyropoulos, A.; Tsolaki, M.; Lazarou, E.; Kozori, M.; Pantazaki, A.A. Restoration of BMI1 Levels after the Administration of Early Harvest Extra Virgin Olive Oil as a Therapeutic Strategy against Alzheimer’s Disease. Exp. Gerontol. 2021, 144, 111178. [Google Scholar] [CrossRef] [PubMed]
- Tzekaki, E.E.; Tsolaki, M.; Pantazaki, A.A.; Geromichalos, G.; Lazarou, E.; Kozori, M.; Sinakos, Z. The Pleiotropic Beneficial Intervention of Olive Oil Intake on the Alzheimer’s Disease Onset via Fibrinolytic System. Exp. Gerontol. 2021, 150, 111344. [Google Scholar] [CrossRef] [PubMed]
- Kaddoumi, A.; Denney, T.S.; Deshpande, G.; Robinson, J.L.; Beyers, R.J.; Redden, D.T.; Praticò, D.; Kyriakides, T.C.; Lu, B.; Kirby, A.N.; et al. Extra-Virgin Olive Oil Enhances the Blood–Brain Barrier Function in Mild Cognitive Impairment: A Randomized Controlled Trial. Nutrients 2022, 14, 5102. [Google Scholar] [CrossRef]
- Boulangé, C.L.; Neves, A.L.; Chilloux, J.; Nicholson, J.K.; Dumas, M.-E. Impact of the Gut Microbiota on Inflammation, Obesity, and Metabolic Disease. Genome Med. 2016, 8, 42. [Google Scholar] [CrossRef]
- Murphy, E.A.; Velazquez, K.T.; Herbert, K.M. Influence of High-Fat Diet on Gut Microbiota. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 515–520. [Google Scholar] [CrossRef]
- Deiana, M.; Serra, G.; Corona, G. Modulation of Intestinal Epithelium Homeostasis by Extra Virgin Olive Oil Phenolic Compounds. Food Funct. 2018, 9, 4085–4099. [Google Scholar] [CrossRef] [PubMed]
- Olalla, J.; de Lomas, J.M.G.; Chueca, N.; Pérez-Stachowski, X.; De Salazar, A.; Del Arco, A.; Plaza-Díaz, J.; De la Torre, J.; Prada, J.L.; García-Alegría, J.; et al. Effect of Daily Consumption of Extra Virgin Olive Oil on the Lipid Profile and Microbiota of HIV-Infected Patients over 50 Years of Age. Medicine 2019, 98, e17528. [Google Scholar] [CrossRef]
- Morvaridi, M.; Jafarirad, S.; Seyedian, S.S.; Alavinejad, P.; Cheraghian, B. The Effects of Extra Virgin Olive Oil and Canola Oil on Inflammatory Markers and Gastrointestinal Symptoms in Patients with Ulcerative Colitis. Eur. J. Clin. Nutr. 2020, 74, 891–899. [Google Scholar] [CrossRef]
- Cândido, T.L.N.; da Silva, L.E.; Cândido, F.G.; Valente, F.X.; da Silva, J.S.; Lopes, D.R.G.; Peluzio, M.D.C.G.; Mantovani, H.C.; Alfenas, R.D.C.G. Effect of the Ingestion of Vegetable Oils Associated with Energy-Restricted Normofat Diet on Intestinal Microbiota and Permeability in Overweight Women. Food Res. Int. 2021, 139, 109951. [Google Scholar] [CrossRef]
- Lim, R.R.X.; Park, M.A.; Wong, L.H.; Haldar, S.; Lim, K.J.; Nagarajan, N.; Henry, C.J.; Jiang, Y.R.; Moskvin, O.V. Gut Microbiome Responses to Dietary Intervention with Hypocholesterolemic Vegetable Oils. NPJ Biofilms Microbiomes 2022, 8, 24. [Google Scholar] [CrossRef]
- Roncero-Martín, R.; Aliaga Vera, I.; Moreno-Corral, L.; Moran, J.; Lavado-Garcia, J.; Pedrera-Zamorano, J.; Pedrera-Canal, M. Olive Oil Consumption and Bone Microarchitecture in Spanish Women. Nutrients 2018, 10, 968. [Google Scholar] [CrossRef] [PubMed]
- García-Gavilán, J.F.; Bulló, M.; Canudas, S.; Martínez-González, M.A.; Estruch, R.; Giardina, S.; Fitó, M.; Corella, D.; Ros, E.; Salas-Salvadó, J. Extra Virgin Olive Oil Consumption Reduces the Risk of Osteoporotic Fractures in the PREDIMED Trial. Clin. Nutr. 2018, 37, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Cazzoletti, L.; Zanolin, M.E.; Spelta, F.; Bono, R.; Chamitava, L.; Cerveri, I.; Garcia-Larsen, V.; Grosso, A.; Mattioli, V.; Pirina, P.; et al. Dietary Fats, Olive Oil and Respiratory Diseases in Italian Adults: A Population-based Study. Clin. Exp. Allergy 2019, 49, 799–807. [Google Scholar] [CrossRef] [PubMed]
- Morante, A.N.; Wolff, A.; Mendoza, G.R.B.; López-Jornet, P. Natural Products for the Management of Xerostomia: A Randomized, Double-Blinded, Placebo-Controlled Clinical Trial. J. Oral Pathol. Med. 2017, 46, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Mendonça, C.R.; Noll, M.; de Souza Cardoso, C.K.; de Carvalho Santos, A.S.A.; dos Santos Rodrigues, A.P.; Silveira, E.A. Reduction in Pain and Pain Intensity with Nonpharmacological Treatment in Severely Obese Patients: A Randomized Clinical Trial. Int. J. Environ. Res. Public. Health 2021, 18, 11112. [Google Scholar] [CrossRef]
- Violi, F.; Loffredo, L.; Pignatelli, P.; Angelico, F.; Bartimoccia, S.; Nocella, C.; Cangemi, R.; Petruccioli, A.; Monticolo, R.; Pastori, D.; et al. Extra virgin olive oil use is associated with improved post-prandial blood glucose and LDL cholesterol in healthy subjects. Nutr. Diabetes 2015, 5, e172. [Google Scholar] [CrossRef]
- Stark, A.H.; Madar, Z. Olive Oil as a Functional Food: Epidemiology and Nutritional Approaches. Nutr. Rev. 2002, 60, 170–176. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on the Substantiation of Health Claims Related to Polyphenols in Olive and Protection of LDL Particles from Oxidative Damage (ID 1333, 1638, 1639, 1696, 2865), Maintenance of Normal Blood HDL Cholesterol Concentrations (ID 1639), maintenance of normal blood pressure (ID 3781),“anti-inflammatory properties” (ID 1882), “contributes to the upper respiratory tract health” (ID 3468), “can help to maintain a normal function of gastrointestinal tract” (3779), and “contributes to body defences against external agents” (ID 3467) pursuant to Article 13(1) of Regulation (EC) No 1924/2006. EFSA J. 2011, 9, 2033. [Google Scholar] [CrossRef]
- Sánchez, R.; Arroyo, L.; Luaces, P.; Sanz, C.; Pérez, A.G. Olive Polyphenol Oxidase Gene Family. Int. J. Mol. Sci. 2023, 24, 3233. [Google Scholar] [CrossRef]

{kind=link}
| Study Design | Compound | Intervention | Outcomes/ Biomarkers | Results | Reference |
|---|---|---|---|---|---|
| Clinical trial on 12 healthy subjects (age: 27–31 years old) and 12 patients with metabolic syndrome (age: 32–38 years old), 12 men and 12 women | High-Polyphenol Extra-Virgin Olive Oil (HP-EVOO) Low-Polyphenol Extra-Virgin Olive Oil (LP-EVOO) | Acute ingestion of 50 mL of HP-EVOO or LP-EVOO, after 1-week washout period and overnight fasting | Gene and miR expression analysis | In healthy subjects, HP-EVOO improved glycaemia and insulin sensitivity, and modulated the transcription of genes and miR involved in metabolism, inflammation, and cancer, modifying to a less deleterious inflammatory phenotype; In healthy subjects and in patients with metabolic syndrome, LP-EVOO showed weaker effects | [48] |
| RCT, crossover on 17 overweight women, age: 20–50 years old, BMI: 25–29.9 kg/m2 | OO | Two 6-week periods, separated by a 2-week washout period, to consume either a usual diet or an OO-rich diet | Omentin and adiponectin | OO-rich diet tended to increase omentin and adiponectin | [29] |
| Randomized, blind, parallel on 43 subjects with prediabetes, 25 men and 18 women | EVOO | 12 weeks of isocaloric weight-maintaining diet containing MUFA (OO) or extra fiber or habitual food (control diet) | Hepatic fat, glucose tolerance, insulin action and secretion | Diet rich in MUFA from OO significantly decreased hepatic fat and improved both hepatic and total insulin sensitivity | [45] |
| Randomized, crossover on 30 patients with impaired fasting glucose, 17 men and 13 women, age: 45–70 years old | EVOO | Patients were randomized to receive a meal including or not 10 g of EVOO in a crossover design; there was an interval of at least 7 days between the two phases of the study | Post-prandial glucose, lipid profile, glucose, insulin, GLP-1, DPP4, TG, total cholesterol, HDL, Apo B-48 | EVOO reduced glucose and DPP4, significantly increased insulin and GLP-1, and significantly decreased TG and Apo B-48; total cholesterol and HDL levels did not significantly change; EVOO improved post-prandial glucose and lipid profile with a mechanism probably related to incretin up-regulation | [35] |
| Randomized double blind, crossover on 13 healthy young men, BMI: 23–25 kg/m2 age: 22–24 years old | OO | On 4 occasions, each separated by 3–14 days, ingestion of a control drink (450 mL) or iso-volumetric drinks containing protein/carbohydrate/fat: (1) 14 g/28 g/12.4 g, (2) 70 g/28 g/12.4 g, (3) 70 g/0 g/0 g | Gastric emptying, glucose, insulin, ghrelin, CCK, GLP-1, total energy intake | The substitution of whey protein with carbohydrate (dextrose) and fat (OO) resulted in faster gastric emptying, reduced suppression of ghrelin, and less stimulation of CCK and GLP-1; meanwhile, the addition of carbohydrate and fat to whey protein did not further slow gastric emptying, suppress ghrelin, or increase CCK and GLP-1 responses | [31] |
| Unstratified case-cohort study within the PREDIMED study on 251 patients with T2D and 641 without T2D, age: 60–73 years old | EVOO | 1 year of intervention, 3 groups: MedDiet + EVOO (4 tablespoons/day/person), MedDiet + nuts (30 g mixed nuts—walnuts, hazelnuts, and almonds), low-fat diet | Plasma levels of amino acids | MedDiet + EVOO significantly lowered the levels of branched-chain amino acids (BCAAs) | [47] |
| RCT, single blind on 43 patients with NAFLD, 26 men and 17 women, BMI: 29.7 ± 0.58 kg/m2 age: 36–56 years old | VOO | 12 weeks, 2 groups consuming a hypocaloric diet: (1) enriched with OO, or (2) with normal fat | ALT, AST, liver steatosis severity | Diet containing OO significantly decreased weight and ALT and AST levels, but the severity of liver steatosis did not change significantly during the study. | [34] |
| Randomized, double blind, crossover on 100 healthy adults, 47 men and 53 women, mean age: 40 years old, BMI: 18.5–24.9 kg/m2 | OO | After 2-week run-in period, ingestion of 48 g/day of palm olein or OO during two phases of 5-week intervention period with a 2-week washout period between them | Anthropometric data and lipid profile | Palm olein and OO had no significantly different effect on body fatness or blood lipids | [40] |
| Randomized, single blind, crossover on 13 overweight patients with T2D, 8 men and 5 women, BMI: 30 ± 4.3 kg/m2 age: 47–75 years old | EVOO | On 3 different days, separated by 2–10 days, in random order, acute intake of either: (a) 200 g carrot, (b) 19 g EVOO + 200 g carrot, or (c) 10.7 g C4 dietary oil + 200 g carrot | Secretion of gut and pancreatic hormones | Both EVOO and C4-dietary oil resulted in greater secretion of GLP-1 and GIP | [41] |
| RCT, parallel, not blind on 94 healthy subjects, 31 men and 63 women, age: 50–75 years old | EVOO | 4 weeks consumption of 50 g/day of one of 3 different dietary fats: EVOO, coconut oil or butter | Blood lipid profile, weight, fat distribution, and metabolic markers | Butter significantly increased LDL, TC/HDL ratio and non-HDL; coconut oil significantly increased HDL; there were no significant differences on weight, fat distribution and metabolic markers among any of the three dietary fats | [49] |
| RCT, parallel, multicenter, from the PREDIMED study on 7447 high CVD risk patients, >90% overweight or obese, 4282 women and 3165 men, age: 55–80 years old | EVOO | 5 years of intervention, 3 groups: MedDiet + EVOO (50 mL/day), MedDiet + nuts (30 g/day), low-fat diet | Bodyweight and waist circumference | MedDiet enriched with EVOO or nuts showed small reductions in weight and lesser increases in waist circumference | [25] |
| Randomized, crossover on 67 healthy adults, 33 men and 34 women, BMI: 19.2–22.6 kg/m2 age: 21–25 years old | EVOO | 18-weeks: first phase was a 2-week run-in period, followed by 3 phases of 4-week experimental period with a 2-week washout period between them; 3 groups of subjects consumed alternately a Chinese diet containing one of the 3 fats: EVOO, palm olein or cocoa butter | Lipid profile and LDL subfractions | Palm olein significantly lowered serum TG concentrations than EVOO; All the other lipid indices and LDL subfractions showed no significant differences amongst the three test fats | [50] |
| RCT, multicenter, parallel-group, subgroup analysis of PREDIMED trial on 100 men and women at high CVD risk, age: 55–80 years old | EVOO | 3-year follow up, 3 groups: Med Diet + EVOO 60 mL/day, Med Diet + 30 g/day nuts, Low-fat diet (control group) | Hepatic steatosis | Med Diet + EVOO is associated with a lower prevalence of hepatic steatosis | [32] |
| RCT, crossover on 11 patients with T1D, 5 men and 6 women, age: 32–50 years old | EVOO | Consumption, alternating at 1-week intervals of one of 3 experimental meals, with different amount and quality of fat: 37 g EVOO (high-MU fat), 43 g butter (high-saturated fat), and 8 g (low fat) | Glucose, gastric emptying rate, GLP-1, GIP, glucagon, lipids | EVOO reduced glucose and significantly increased gastric emptying rate, GLP-1 and TG; GIP and glucagon were not significantly different between EVOO and butter | [36] |
| RCT, parallel, double-blind on 66 adults with NAFLD, BMI: 25 kg/m2 | OO | 12 weeks, 2 groups consuming: 20 g/day OO or 20 g/day SFO, both combined with a hypocaloric diet | Fatty liver grade, liver enzymes, anthropometric data, blood pressure, serum lipid profile, glucose, insulin, malondialdehyde (MDA), TAC, IL-6 | OO intake lessened fatty liver grade and reduced body-fat percentage but did not affect liver enzymes and cardiometabolic risk factors; OO and SFO reduced weight, waist circumference, blood pressure, and serum aminotransferases | [33] |
| Randomized, single blind, crossover on 10 patients with T2D, 9 women and 1 man, BMI: 20–30 kg/m2 age: 30–60 years old | EVOO | EVOO or rice bran oil (15 mL/day) was administered for 4 weeks, followed by a 2-week washout period and a crossover for another 4 weeks | Glycemic control and lipid profiles | EVOO or rice bran oil significantly decreased only the HDL levels | [39] |
| RCT, parallel, double-blind, multicentre, PREDIABOLE study on 176 prediabetic subjects (with IFG and impaired glucose tolerance (IGT)), BMI: 25–39.9 kg/m2 age: 30–80 years old | OA-enriched OO non-enriched OO | 55 mL/day of OA-enriched OO or non-enriched OO during 25–30 months | New-onset T2D incidence | The intake of OA-enriched OO substantially reduced the risk of developing T2D | [44] |
| RCT, parallel, multicenter, subgroup of PREDIMED study on 3230 patients with T2D, without treatment, 1552 men and 1678 women, age: 61–74 years old | EVOO | 5 years of intervention, 3 groups: MedDiet + EVOO (1 L/week), MedDiet + nuts (30 g/day), low-fat diet | Need for glucose-lowering medications and for insulin treatment | MedDiet + EVOO significantly decreased the need for glucose-lowering medications; MedDiet, with EVOO or nuts, did not result in a lower need for insulin treatment | [46] |
| Experimental in 23 subjects with metabolic syndrome and hepatic steatosis, 15 men and 8 women, age: 49–71 years old | EVOO | EVOO with high oleocanthal concentration was given (32 g/day) for 2 months | Anthropometric data, metabolic parameters, hepatic steatosis, abdominal fat distribution, and pro- and anti-inflammatory cytokines | Oleocanthal-enriched EVOO significantly reduced body weight, waist circumference, body mass index, alanine transaminase, hepatic steatosis, pro-inflammatory cytokines (IL-6, IL-17A, TNF-α, IL-1B), while significantly increased anti-inflammatory cytokine (IL-10) | [24] |
| Cross-sectional observational study on 200 healthy adults, age: 20–30 years old | OO | Participants were divided in 2 groups regarding their OO consumption: low < 12.5 g/day, and high ≥ 12.5 g/day | BMI and waist circumference | OO consumption was not associated with increasing body mass index and waist circumference | [26] |
| RCT, parallel, blind on 111 adults with severe obesity, BMI ≥ 35 kg/m2 age: 18–64 years old | EVOO | 12 weeks of intervention, 3 groups: DieTBra, EVOO (52 mL/day) and DieTBra + EVOO (52 mL/day) | Body composition and sarcopenia indicators | DieTBra + EVOO significantly reduced body weight and reduced total body fat; DieTBra significantly reduced body weight, and total body fat, and significantly improved walking speed and handgrip strength (sarcopenia indicators); EVOO alone did not improve any of the outcomes | [27] |
| Exploratory randomized crossover on 20 10 RYGB-operated patients and 10 controls | EVOO | Ingestion during 3 days, on separated occasions and in randomized order, of different triacylglycerol formulations: (1) 20 mL EVOO, (2) 13.8 mL C8-dietary oil, and (3) 10.7 mL tricaprylin | Enteroendocrine secretions, glucose, lipid, and bile acid metabolism | EVOO was significantly more effective in stimulating enteroendocrine secretion in RYGB-operated patients and controls, and gut hormone release was greater in RYGB-operated patients | [30] |
| RCT, crossover on 13 patients with T2D, 6 men and 7 women, age: 53–63 years old, BMI under the overweight or obese class | EVOO | Participants received a meal with or without EVOO followed by a 1-week washout period, after which they were given the other intervention | Postprandial blood glucose | Meals with EVOO increased the postprandial blood glucose, providing no additional benefit | [37] |
| RCT single blind, crossover on 25 patients with T2D and 20 healthy subjects, 22 men and 23 women, age: 27–77 year old | EVOO | One single intake of 40 g of oleuropein-enriched chocolate (addition of EVOO to enable final concentration of 4 mg% oleuropein) or 40 g of control chocolate spread. After 10 days washout phase, participants crossed over to take the opposite chocolate | Glucose, insulin | EVOO, as a source of oleuropein, is associated with a modest increase or no change of glycemia in T2D and healthy subjects, respectively | [42] |
| RCT, double blind in 72 women with polycystic ovarian syndrome, age: 18–45 years old | OO | 3 groups receiving 25 g/day of OO, CO or SFO for 10 weeks | Lipid profile and fatty liver severity | OO consumption resulted in no significant reduction in lipid profile; OO and CO significantly decreased fatty liver grade and HOMA-IR | [23] |
| Short-term, open clinical trial, proof-of-concept study on 41 adults, lean (BMI 18.5–24.9 kg/m2) and obese/overweight (BMI 25–35 kg/m2), age: 25–40 years old | EVOO | Participants were encouraged to increase their usual OO consumption by replacing their habitual vegetable oil for OO during 4 weeks | Brown adipose tissue | EVOO ingestion leads to increased brown adipose tissue activity by significant increase in leptin, secretin, FGF21 and 12, 13 di-HOME in lean but not in overweight/obese volunteers | [28] |
| RCT, double blind, crossover on 20 healthy normal-weight subjects, 10 men and 10 women, age: 23–25 years old | EVOO | 2-weeks consumption of 100 g/day chocolate spread enriched with either EVOO or palm oil, followed by 1 week of washout period and another 2 weeks of the opposite treatment | Ceramides concentration, glucose and lipid metabolism, inflammatory markers, appetite regulation | EVOO-enriched chocolate spread consumption led to decreased circulating harmful sphingolipids, HOMA-IR and plasma insulin; no major significant changes in TC, TG, HDL, inflammatory markers, and appetite regulation were observed between the groups | [43] |
| RCT, parallel, within the PREDIMED study on 150 subjects free of T2D, BMI: 27–35 kg/m2 | EVOO | 1 year of intervention, 3 groups: MedDiet + EVOO, MedDiet + nuts, low-fat diet | Exosomal non-coding RNAs (Ribonucleic acid) (Long Non-Coding RNAs (lncRNAs), messenger RNA (mRNA) and miRs) modulation | MedDiet + nuts and MedDiet + EVOO modulated exosomal RNA content, with the former affecting a higher number of miR | [51] |
| RCT in 40 adults aged 18–64 years with T2D and class II/III obesity | EVOO | 2 groups receiving EVOO or EVOO+DieTBra for 12 weeks | Glycemic parameters, inflammatory markers, BMI, and weight | DieTBra significantly reduced fasting insulin levels and decreased BMI, weight, serum levels of inflammatory cytokines, IL-1α and adiponectin and increased TNF-α showing its role in ameliorating inflammatory profiles and fasting insulin levels. | [38] |
| Study Design | Compound | Intervention | Outcomes/ Biomarkers | Results | Reference |
|---|---|---|---|---|---|
| RCT, double-blind, crossover, subsample from EUROLIVE study on 18 healthy men, age: 20–60 years old | EVOO ROO | Ingestion of 25 mL/day f OO (366 mg/kg phenolic compounds) for 3 weeks, preceded by 2-week washout periods | Anthropometric and blood pressure measurements, TC, LDL, HDL, TG, glucose, blood pressure-related gene expression analysis | EVOO decreased systolic blood pressure, maintained diastolic blood pressure, and decreased ACE, NR1H2 and IL8RA gene expression | [59] |
| RCT, double blind, parallel on 41 women overweight and obese age: 26–28 years old | EVOO | 9 weeks, 25 mL/day intake of one of the tested oils, EVOO or soybean oil, associated with energy-restricted normofat diets | Anthropometric, body composition and blood pressure measurements; metabolic biomarkers | EVOO consumption reduced body fat, diastolic blood pressure, alkaline phosphatase; increased serum creatinine; and tended to reduce IL-1β concentrations | [60] |
| RCT, parallel, multicenter, PREDIMED study on 7403 high CVD risk patients, age: 55–80 years old | EVOO | 5 years of intervention, 3 groups: MedDiet + EVOO (1 L/week), MedDiet + nuts (210 g/week), low-fat diet | Heart failure incidence | MedDiet with EVOO and MedDiet with nuts showed no significant effect on lowering heart failure incidence | [73] |
| Prospective, case-cohort, nested in the PREDIMED study on 980 high CVD risk patients | EVOO | 5 years of intervention, 3 groups: MedDiet + EVOO, MedDiet + nuts, low-fat diet | Plasma ceramides concentration | MedDiet enriched with EVOO or nuts showed the potential to mitigate the deleterious effects of elevated plasma ceramide concentration on CVD risk | [74] |
| RCT, parallel, multicenter, substudy of PREDIMED on 90 high CVD risk women, age: 60–80 years old | EVOO | 1 year of intervention, 3 groups: MedDiet + EVOO (52 g/day), MedDiet + nuts (30 g/day), low-fat diet | Endothelial markers involved in blood pressure control | MedDiet with EVOO or nuts reduced blood pressure values | [62] |
| RCT, parallel, multicenter, subsample of PREDIMED study on 210 high CVD risk patients, age: 58–73 years old | VOO | 1 year of intervention, 3 groups: MedDiet + VOO (1 L/week), MedDiet + nuts (210 g/week), low-fat diet | LDL atherogenic traits: resistance against oxidation, particle size, composition, cytotoxicity | MedDiet + VOO decreased LDL atherogenicity by increasing LDL resistance against oxidation, LDL particle size and composition (cholesterol-rich), and decreasing LDL oxidative modifications and particles cytotoxicity | [75] |
| RCT, parallel, multicenter, subsample of PREDIMED study on 296 high CVD risk patients, age: 59–72 years old | VOO | 1 year of intervention, 3 groups: MedDiet + VOO (1 L/week), MedDiet + nuts (210 g/week), low-fat diet | HDL functionality | MedDiet, especially when enriched with VOO, improved HDL atheroprotective functions; both MedDiet increased cholesterol efflux capacity; MedDiet + VOO decreased cholesteryl ester transfer protein activity and increased HDL ability to esterify cholesterol, paraoxonase-1 arylesterase activity, and HDL vasodilatory capacity; the 3 diets increased the percentage of large HDL particles | [76] |
| RCT, single-center, placebo study on 60 postmenopausal women, age: 50–61 years old | EVOO | 1 year of oral supplementation with placebo or EVOO enriched with vitamins D3, K1 and B6 20 mL/day | Platelet membrane fluidity, Na+/K+-ATPase activity, serum nitric oxide (NO), and peroxynitrite | EVOO enriched with vitamins decreased platelet membrane anisotropy, NO and peroxynitrite, and increased Na+/K+-ATPase activity | [68] |
| RCT, double-blind, crossover, post hoc analyses from VOHF study on 33 hypercholesterolemics adults, 19 men and 14 women, TC > 200 mg/dL, age: 35–80 years old | VOO FVOO FVOOT | The different OO will be sequentially ingested (30 mL/day) during three periods of 3 weeks, preceded by 2-week washout periods | HDL composition, fluidity, oxidation, size and cholesterol efflux capacity | VOO ingestion increased HDL fluidity and apolipoprotein A-I concentration in HDL, and decreased HDL oxidative status, which are main determinants for cholesterol efflux capacity enhancement | [80] |
| Case-cohort design, subcohort of PREDIMED study on 983 high CVD risk patients, age: 61–76 years old | EVOO | 1 year of intervention, 3 groups: MedDiet + EVOO (50 g/day), MedDiet + nuts (30 g/day), low-fat diet | Lipid species | Although the MedDiet interventions, supplemented with EVOO or nuts, induced some significant changes in the lipidome, they were not significantly associated with subsequent CVD risk | [77] |
| RCT, double-blind, crossover, subsample from VOHF study on 12 hypercholesterolemic adults, 7 men and 5 women, TC > 200 mg/dL, age: 46–67 years old | VOO FVOO FVOOT | The different OO will be sequentially ingested (30 mL/day) during three periods of 3 weeks, preceded by 2-week washout periods | Blood lipids, faecal quantitative changes in microbial populations, short chain fatty acids, cholesterol microbial metabolites, bile acids, and phenolic metabolites | FVOOT decreased ox-LDL, increased bifidobacteria numbers, and increased protocatechuic acid levels | [81] |
| RCT, double-blind, crossover, VOHF study on 33 hypercholesterolemics adults, 19 men and 14 women, TC > 200 mg/dL, age: 35–80 years old | VOO FVOO FVOOT | The different OO were sequentially ingested (25 mL/day) during three periods of 3 weeks, preceded by 2-week washout periods | HDL fatty acids, HDL antioxidant content, HDL monolayer fluidity, HDL cholesterol efflux capacity | The FVOO and FVOOT increased HDL antioxidant content, but α-tocopherol was only augmented after FVOOT | [82] |
| RCT, prospective on 160 patients with T2D, 118 men and 42 women, age: 40–60 years old | OO | Diet without or with 1.1 mL of OO + 500 mg of garlic powder for 3 months | Serum cholesterol and serum TG | Combination of OO with garlic powder significantly normalized the cholesterol and TG levels | [55] |
| RCT double-blind, crossover, NUTRAOLEOUM Study on 51 healthy adults | VOO OVOO Functional Olive Oil (FOO) | VOO (124 ppm PC, 86 ppm triterpenes), OVOO (490 ppm PC, 86 ppm triterpenes) and FOO (487 ppm PC and 389 ppm triterpenes) all at (30 mL/day) were sequentially administered over three periods of 3 weeks preceded by 2-week washout periods | Metabolic syndrome and endothelial function biomarkers | VOO, OVOO, and FOO reduced the plasma endothelin-1 levels; no effect of triterpenes was observed. | [63] |
| RCT, parallel, multicenter, subsample of PREDIMED study on 7447 high CVD risk patients, 4282 women and 3165 men, age: 55–80 years old | EVOO | 5 years of intervention, 3 groups: MedDiet + EVOO (50 mL/day), MedDiet + nuts (30 g/day), low-fat diet | CVD incidence | MedDiet supplemented with EVOO or nuts decreased the incidence of major cardiovascular events, including acute myocardial infarction, stroke and death for CVD | [72] |
| RCT, parallel, multicenter, subsample of PREDIMED study on 296 high CVD risk patients | VOO | 1-year increases in the consumption of VOO (10 g/day), nuts (30 g/day), legumes (25 g/day), whole grains (25 g/day), and fish (25 g/day) | HDL functionality | Increases in the consumption of VOO, nuts, legumes, whole grains, and fish improved HDL functions; VOO increased cholesterol efflux capacity | [83] |
| Prospective, population-based study, ATTICA study on 2020 CVD-free adults, age: 18–89 years old | OO | 10-year follow up; participants were classified into 3 groups: no use, mixed use, and exclusive use of OO | Fatal/non-fatal CVD incidence | Exclusive OO use decreased the risk of developing CVD | [52] |
| RCT, double-blind, multiarm parallel study on 86 healthy young adults, 43 men and 43 women, age: 18–30 years old | OO | 12 weeks of 3 g/day supplementation of OO, eicosapentaenoic acid or docosahexaenoic acid | Resting hemodynamics and muscle sympathetic nerve activity | OO supplementation reduced resting systolic and diastolic blood pressure and reduced muscle sympathetic nerve activity | [61] |
| RCT, crossover, double-blind study on 7 healthy males, active runners engaged in endurance activities (10–14 h/week), age: 28–36 years old, BMI: 23.1 ± 1.7 Kg/m2 | EVOO | Three separate effort test sessions were carried out separated by 7-day interval. During each session, participants repeated the same test, but under different acute dietary supplementation in a randomized order: EVOO (25 mL), palm oil (25 mL), and placebo | Cardiorespiratory coordination and performance | Supplementation with EVOO increased cardiorespiratory coordination during a progressive walking test at moderate intensity, although it did not change performance | [71] |
| Follow-up study on 92,978 adults: 61,181 women and 31,797 men, Free of cancer, heart disease, and stroke | OO | 24-year follow up; OO intake was categorized into 4 categories: (1) never or <1/month; (2) >0 to ≤4.5 g/day; (3) >4.5 to ≤7 g/day; and (4) >7g/day | CVD, coronary heart disease and stroke risk; inflammatory and lipid biomarkers | Higher OO intake was associated with lower risk of coronary heart disease and CVD; in a subset of participants, higher OO intake was associated with lower levels of circulating inflammatory biomarkers and a better lipid profile | [53] |
| RCT, parallel-arm, open label study on 48 patients with at least one classic CVD risk factor (hypertension, dyslipidemia, or diabetes), 44 men and 4 women, age: 51–64 years old | ROO | Ingestion of 25 mL/day of ROO or CO for 6 weeks | Plasma lipids, some selected inflammatory markers, lipoprotein-associated phospholipase A2 (Lp-PLA2) levels | OO consumption significantly decreased IL-6 concentration | [54] |
| RCT, parallel, single-center study on 204 patients with stable coronary artery disease, age: 40–80 years old | EVOO | 12 weeks, 3 groups: healthy diet, healthy diet + 30 mL/day EVOO, healthy diet + 30 g/day pecans | TG, TC, LDL, HDL, non-HDL, TC/HDL ratio, LDL/HDL ratio, HDL/TG ratio, atherogenic index | There were no significant differences in LDL levels after the consumption of a healthy diet supplemented with EVOO or pecans; supplementing the healthy diet with pecan nuts may improve other lipid profile markers | [57] |
| RCT, double-blind, preliminary study on 30 women with fibromyalgia, age: 44–60 years old | EVOO ROO | Ingestion of 50 mL/day of EVOO or ROO for 3 weeks | Thrombosis-related parameters, ESR, inflammatory markers, NO levels, lipid profile and cortisol levels | Consumption of EVOO decreased significantly red blood cell count, ESR and cortisol levels. Consumption of ROO significantly increased mean platelet volume and cortisol levels, and reduced platelet distribution width, neutrophil-to-lymphocyte ratio, ESR, and fibrinogen. No significant changes in the lipid profile, inflammatory markers and NO levels | [67] |
| RCT, postprandial, parallel, double-blind, subsample from VOHF study on 20 healthy participants, age: 22–60 years old | EVOO | Acute intake of 30 mL of the EVOO after 12 h of fasting | Plasma miR related to CVD | All EVOO, regardless of polyphenol content, decreased the levels of let-7e-5p; Low Phenolic Content Extra-Virgin Olive Oil (L-EVOO) and Medium Phenolic Content Extra-Virgin Olive Oil (M-EVOO) increased miR-17-92 cluster | [70] |
| Cross-sectional analysis of the PREDIMED study on 4330 high CVD risk patients, with an ankle-brachial pressure index (ABI) <1.4 and total energy intakes: 800–4000 Kcal/day for men, 500–3500 Kcal/day for women | EVOO VOO ROO VOO mixture Olive-pomace oil | Consumption of any category of OO and olive-pomace oil was assessed through a validated food-frequency questionnaire | ABI | VOO (EVOO and VOO) consumption was associated with a higher mean ABI | [78] |
| Quasi-experimental on 84 healthy men and women, age: 23–85 years old, divided into 2 groups: 28 young (23–45 years) and 56 elderly (65–85 years) | EVOO | Consumption of 25 mL/day of raw EVOO for 12 weeks | Blood pressure, TC, LDL, HDL, TG, glucose, CEC of HDL, HDL subclasses distribution | EVOO significantly decreased the CEC of the HDL of elderly healthy subjects (to a level comparable to that of young healthy subjects), and improved distribution of HDL subclasses (increasing large HDL and decreasing small HDL particles) | [56] |
| RCT, parallel and unicentricstudy in 149 patients with stable coronary artery disease, age: 40–80 years old | EVOO | 12 weeks, 3 groups: healthy diet, healthy diet + 30 mL/day EVOO, healthy diet + 30 g/day pecans | Plasma fatty acids | There were no significant differences in plasma fatty acids after the consumption of a healthy diet supplemented with EVOO or pecans | [58] |
| RCT, double-blind, crossover study on 20 adults at risk of T2D, 10 men and 10 women, age: 25–75 years old | EVOO ROO | 50 mL single dose administration of each of 2 treatments (EVOO—189 ppm phenolic compounds or ROO ≤ 20 ppm PC) in random sequence, with a 1-week washout between treatment assignments | Endothelial function and blood pressure | EVOO acutely improved endothelial function; no significant effects on systolic or diastolic blood pressure were observed | [64] |
| RCT single-blind, crossover study on 25 T2D patients, 12 men + 13 women, age: 61–77 years-old | EVOO | One single intake of 40 g of EVOO-enriched chocolate or 40 g of control chocolate spread. After a 10-day washout phase, participants crossed over to take the opposite chocolate | Endothelial function and oxidative stress | EVOO-enriched chocolate is associated with increased endothelial function (increasing the arterial brachial flow-mediated dilation) and reduction of oxidative stress | [65] |
| Exploratory crossover study on 10 patients with T1D and 6 healthy subjects, 13 men and 3 women, age: 20–36 year old | EVOO | Each participant received 2 types of high glycemic index meal: one enriched with EVOO and one with butter | Endothelial function, glucose and lipids measurements, and gastric emptying assessment | EVOO, added to a single high glycemic index meal, significantly increased the endothelial function by increasing the arterial brachial flow-mediated dilation | [66] |
| Prospective study on 63 patients with severe obesity, age: 24–40 years old, BMI: 44.1 ± 8.5 kg/m2 | OO | OO intake was stratified into <1 time/week, 1–3 times/week, ≥4 times/week | Platelet activation with and without thrombin exposure | More frequent OO intake reduced thrombin-induced platelet activation | [69] |
| Prospective, randomized, single-blind, controlled trial in 1002 coronary heart disease patients analysis | EVOO | 2 groups following a MedDiet or low-fat diet monitored at baseline and after 5 and 7 years. | IMT-CC, carotid plaque number and height | EVOO-rich MedDiet was linked to reduced atherosclerosis progression and lower carotid plaquemax height and IMT-CC while no changes were observed with the low-fat diet group, evidencing the MedDiet’s advantages as secondary CVD prevention. | [84] |
| Three-arm, randomized, controlled-feeding trial in 90 middle-aged and elderly Chinese women at high cardiovascular risk | OO | 3 groups using n-6 PUFA-rich soybean oil, MUFA-rich olive oil, or MUFA-rich camellia seed oil as cooking oils within traditional Chinese eating habits for 3 months | Body weight, cardiovascular profiles, HDL, and AST | MUFA-rich OO and camellia seed oil were shown to be more beneficial on the cardiometabolic profiles as they had a role in increasing HDL-C and decreasing AST, respectively. | [85] |
| CORDIOPREV randomized controlled trial in 1002 coronary heart disease patients | EVOO | 2 groups followed a MedDiet or a low-fat diet monitored at baseline and after 5 years | Kidney function by determination of serum creatinine-based estimated glomerular filtration rate | The advantages of the MedDiet rich in EVOO as a secondary CVD prevention was supported as it may have a preservation role for kidney function and a reduction in estimated glomerular filtration rate decrease in coronary heart disease patients with T2D. HDL-C had a minimal increase in the OO group and AST was decreased more in camellia seed oil in comparison to the soybean oil. | [86] |
| A crossover, randomized trial in 30 healthy participants | OO | 2 groups consuming isoenergetic ghee or OO for 4 weeks | Fasting plasma apo-B, non-HDL-cholesterol, LDL-cholesterol, total cholesterol:HDL-cholesterol ratio | The diet that included ghee increased the fasting plasma Apo-B and non-HDL cholesterol. Despite the non-significant differences between the two groups on LDL-C, this study emphasizes the recommendation of replacing SFA with unsaturated fats to decrease the risk of CVD. | [87] |
| A randomized trial in 43 hypercholesterolemic adults | OO | 2 groups consuming cottonseed oil or OO diets for 8 weeks | blood lipid responses | The partial outpatient feeding intervention concluded that cottonseed oil was more effective in improving the fasting and postprandial blood lipids and postprandial glycemia in hypercholesterolemic adults. | [88] |
| A case-control study nested in the PREDIMED study; 167 peripheral artery disease cases matched with 250 controls | EVOO | 3 groups: MedDiet with supplementation of tree nuts, MedDiet with EVOO supplementation, or control (low-fat diet) | Plasma amino acids and risk of peripheral artery disease | MedDiet+EVOO group was protected against peripheral artery disease regardless of baseline threonine which can be an early biomarker of future disease incidences in high-risk CVD individuals. | [79] |
| Study performed on 40 chronic kidney disease patients under conservative therapy for the in vivo clinical testing | EVOO rich in phenolic compounds | Participants consumed 40 mL/day of raw EVOO for 9 weeks | Inflammatory parameters, oxidative stress biomarkers, lipid and purine metabolism, atherogenic indices | Inflammatory parameters, carotid intima-media thickness (CIMT), and oxidative stress biomarkers decreased while the lipid and purine metabolism, atherogenic indices, and body compositions were enhanced. | [89] |
| Study Design | Compound | Intervention | Outcomes/ Biomarkers | Results | Reference |
|---|---|---|---|---|---|
| RCT, parallel-group, multicenter, from the PREDIMED study on 75 metabolic syndrome patients, age: 55–80 years old | EVOO | 5 years of intervention, 3 groups: MedDiet + EVOO (50 g/day), MedDiet + nuts (30 g/day), low-fat diet | Antioxidant capabilities and xanthine oxidase activity | MedDiet + EVOO and MedDiet + nuts decreased xanthine oxidase activity and increased superoxide dismutase and catalase levels and antioxidant activities | [93] |
| Experimental on 11 overweight and non-insulin treated T2D Caucasian patients, 7 men and 4 women, mean age: 64.63 ± 8.52 years old, diabetes duration ≤10 years | ROO HP-EVOO | 8 weeks: intake of ROO (25 mL/day) for the first 4 weeks (wash-out period) followed by intake of HP-EVOO (25 mL/day) for the rest of 4 weeks | Anthropometric parameters, fasting plasma glycaemia, HbA1c, CRP, plasma lipid profile, liver function, and serum levels of TNF-α, adiponectin, IL-6, visfatin, apelin | HP-EVOO consumption reduced fasting glucose, HbA1c, BMI, body weight, AST, ALT, and visfatin | [91] |
| RCT, parallel group, single-center study on 77 T2D women, age: >50 years old; mean BMI 28 kg/m2 | OO | 8 weeks, 3 groups: balanced diet + 30 g/day of OO or CO or SFO | Height, weight, waist circumference, fasting blood sugar, serum insulin, CRP, MDA | CRP level was reduced significantly in OO and CO groups | [92] |
| Two-arm study on 18 overweight/obese subjects (BMI ≥ 25 kg/m2) + 18 normal weight controls (BMI 18.5–24.9 kg/m2) | HQ-EVOO | MedDiet enriched with 40 g/day of HQ-EVOO for 3 months | Lactic acid bacteria composition, oxidative stress, metabolic and inflammation parameters | MedDiet rich in HQ-EVOO increased lactic acid bacteria numbers, decreased oxidative stress and inflammation parameters, and increased adiponectin and IL-10 concentrations | [95] |
| RCT double-blind, crossover, NUTRAOLEOUM study on 51 healthy adults | VOO OVOO FOO | VOO, OVOO and FOO (30 mL/day) were sequentially administered over three periods of 3 weeks preceded by 2-week washout periods | Oxidative and inflammatory biomarkers. | Urinary 8-hidroxy-2′-deoxyguanosine, plasma IL-8 and TNF-α were lower after the intervention with the FOO than after the OVOO. IL-8 was lower after the intervention with FOO than after VOO intervention. | [97] |
| RCT, crossover on 30 patients with IFG, 17 men + 13 women, mean age: 58 years-old | EVOO | Taking a meal with or without 10 g of EVOO | LPS, Apo-B48, ox-LDL, sNox2-dp, plasma polyphenols | EVOO significantly decreased LPS, ox-LDL, sNox2-dp and plasma polyphenols | [98] |
| RCT, double-blind, crossover study on 8 male trained cyclists, age: 34–45 years-old | EVOO | Four-week supplementation of n-3 PUFA (5.7 g/day) or EVOO (6 g/day), followed by a four-week washout and crossover to the other supplement | Global and gene-specific (PPARGC1A, IL6 and TNF) DNA methylation, and DNMT1 mRNA expression | EVOO decreased the methylation of the gene encoding IL-6 and the expression of DNMT1 | [99] |
| RCT double-blind, crossover, OLIVAUS study on 43 healthy Australian adults, age: 38.5 ± 13.9 years old, 66% females | High Polyphenol Extra-Virgin Olive Oil (HPOO—320 mg/kg PC) Low Polyphenol Extra-Virgin Olive Oil (LPOO—86 mg/kg PC) | Consumption of 60 mL/day of HPOO or LPOO for 3 weeks. Following a 2-week wash-out period, participants crossed-over to the alternate treatment | Anthropometric parameters, TAC, plasma oxLDL, CRP | After HPOO consumption it was observed a reduction in ox-LDL and CRP and an increase in TAC, although there were no significant differences between treatments | [94] |
| RCT single-blind, crossover study on 25 T2D patients, 12 men + 13 women, age: 61–77 years-old | EVOO | One single intake of 40 g of EVOO-enriched chocolate or 40 g of control chocolate spread. After a 10 days washout phase, participants crossed over to take the opposite chocolate | Endothelial function and oxidative stress | EVOO-enriched chocolate is associated with increased endothelial function and reduction of oxidative stress (decreasing sNox2-dp) | [65] |
| RCT double-blind study on 62 patients with major depression, age: 18–65 years-old | EVOO | 52 days, during which participants consumed 25 mL/day of EVOO or SFO | Weight, BMI, waist circumference. TG, TC, LDL, HDL, Very Low-Density Lipoprotein Cholesterol (VLDL), MDA, CRP | EVOO significantly decreased waist circumference and significantly increased HDL | [100] |
| RCT in 149 severely obese individuals aged 18–65 years | EVOO | 2 groups: nutritional EVOO and DieTBra+EVOO followed for 12 weeks | Inflammation profiles, neutrophil-to-lymphocyte ratio, LMR, leukocytes, and CRP | DieTBra+EVOO was able to significantly decrease the total leukocytes and LMR. DieTBra showed a minimal decrease in neutrophil-to-lymphocyte ratio. EVOO and DieTBra interventions decreased CRP. It was also noted that the total leukocytes and LMR were similarly reduced in all groups. | [96] |
| Study Design | Compound | Intervention | Outcomes/ Biomarkers | Results | Reference |
|---|---|---|---|---|---|
| RCT on 180 elderly individuals, aged ≥ 65 years | EVOO | 1 year, 2 groups: MedDiet + EVOO (20–30 g/day) and control MedDiet | Cognitive functions | MedDiet + EVOO resulted in a higher improvement of cognitive functions, compared with MedDiet alone | [103] |
| RCT, parallel on 129 adults with severe obesity, age: 18–65 years old, BMI ≥ 35 kg/m2 | EVOO | 12 weeks of intervention, 3 groups: DieTBra, EVOO (52 mL/day) and DieTBra + EVOO (52 mL/day) | Anxiety and depression | DieTBra and EVOO, alone or in combination, resulted in a significant reduction of anxiety and depression symptoms | [104] |
| Cross-sectional analysis of 166 women aging with HIV | OO | Evaluation within 18 months, women were divided into those who reported using OO and those who did not | Cognitive performance | OO increased their attention/concentration scores | [105] |
| RCT, prospective, longitudinal, double-blind, MICOIL study on 60 patients with mild cognitive impairment, age: 60–80 years old | High-Phenolic Early Harvest Extra-Virgin Olive Oil (HP-EH-EVOO) Moderate-Phenolic Extra-Virgin Olive Oil (MP-EVOO) | 1 year of intervention, 3 groups: HP-EH-EVOO (50 mL/day), MP-EVOO (50 mL/day) and MedDiet | Cognitive functions, Apolipoprotein E (APOE-4) (risk gene for AD) | HP-EH-EVOO or MP-EVOO was associated with significant improvement in cognitive function compared to MedDiet, independent of the presence of APOE-4 | [106] |
| RCT, prospective, longitudinal, double-blind, MICOIL study on 43 patients with Mild Cognitive Impairment, age: 60–80 years old | HP-EH-EVOO MP-EVOO | 1 year of intervention, 3 groups: HP-EH-EVOO (50 mL/day), MP-EVOO (50 mL/day) and MedDiet | Spontaneous Electroencephalography (EEG) dynamic connectivity | Reduced the over excitation of information flow in spontaneous brain activity and increased brain flexibility | [107] |
| RCT, prospective, longitudinal, double-blind, MICOIL study on 80 patients with Mild Cognitive Impairment, age: 64–80 years old | EVOO | 1 year of intervention, 2 groups: with EVOO (50 mL/day) and without EVOO | BMI1, p53, AD biomarkers (tau, p-tau, Aβ1–40, Aβ1–42 and Aβ1–42/Aβ-40 ratio) | The administration of EVOO resulted in an increase of BMI1 and a decrease of p53 and AD biomarkers | [108] |
| RCT, prospective, longitudinal, double-blind MICOIL study on 84 patients with Mild Cognitive Impairment, age: 65–80 years old | EVOO | 1 year of intervention, 2 groups: with EVOO (50 mL/day) and without EVOO | Fibrinolytic system factors (PAI-1, α2AP and tPA), MDA | The administration of EVOO resulted in a reduction of PAI-1, α2AP, tPA, and MDA | [109] |
| RCT on 25 mild cognitive impaired participants | EVOO ROO | 6 months of intervention with a daily intake of 30 mL/day of EVOO (1200 mg/kg total PC; 13 participants) or ROO (no PC; 12 participants) | Clinical dementia rating, behavioral scores, functional connectivity, blood brain barrier connectivity and permeability, brain function, cognitive function, and Alzheimer’s disease blood biomarkers | Daily consumption of EVOO significantly ameliorated the clinical dementia rating and behavioral scores, enhanced the functional connectivity, and decreased the blood–brain barrier permeability. It was concluded that both ROO and EVOO are beneficial with the latter having additional effects due to its bioactive phenolic content. | [110] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Isaakidis, A.; Maghariki, J.E.; Carvalho-Barros, S.; Gomes, A.M.; Correia, M. Is There More to Olive Oil than Healthy Lipids? Nutrients 2023, 15, 3625. https://doi.org/10.3390/nu15163625
Isaakidis A, Maghariki JE, Carvalho-Barros S, Gomes AM, Correia M. Is There More to Olive Oil than Healthy Lipids? Nutrients. 2023; 15(16):3625. https://doi.org/10.3390/nu15163625
Chicago/Turabian StyleIsaakidis, Akritas, Jane El Maghariki, Sérgio Carvalho-Barros, Ana Maria Gomes, and Marta Correia. 2023. "Is There More to Olive Oil than Healthy Lipids?" Nutrients 15, no. 16: 3625. https://doi.org/10.3390/nu15163625
APA StyleIsaakidis, A., Maghariki, J. E., Carvalho-Barros, S., Gomes, A. M., & Correia, M. (2023). Is There More to Olive Oil than Healthy Lipids? Nutrients, 15(16), 3625. https://doi.org/10.3390/nu15163625