
Functional Food in Relation to Gastroesophageal Reflux Disease (GERD)

{kind=link}
{kind=link}
Abstract
1. Introduction
2. GERD Overview
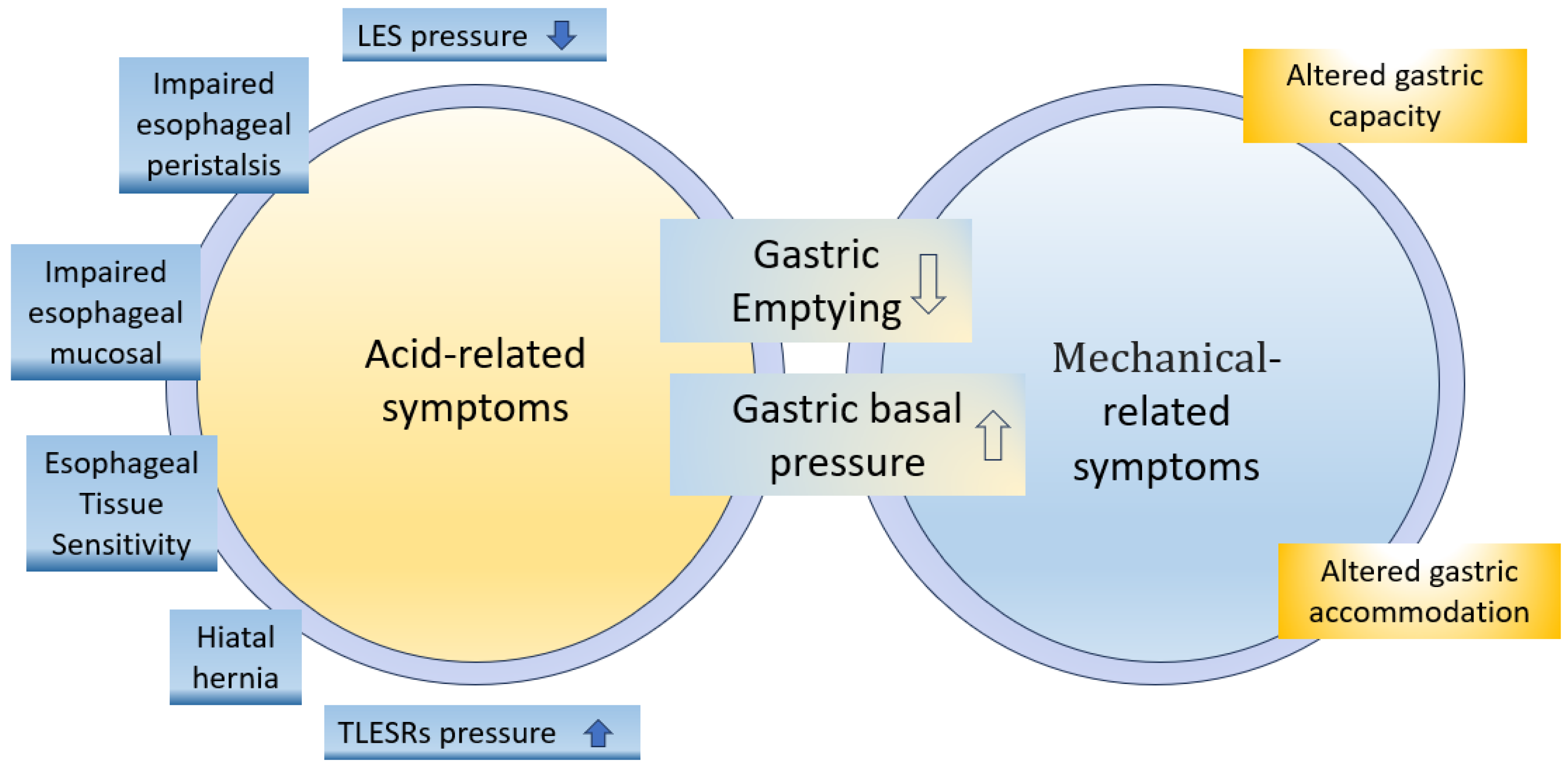
2.1. Pathophysiology of GERD
- Lower esophageal sphincter dysfunction
- 2.
- Enhanced proximal postprandial gastric acid pocket (PPAGP)
- 3.
- Delayed gastric emptying
- 4.
- Impaired esophageal peristalsis
- 5.
- Impaired esophageal mucosal defense against the gastric refluxate
- 6.
- Hiatal hernia
- 7.
- Esophageal Tissue Sensitivity
2.2. Complexity of GERD
2.3. Dietary Factors Pertaining to GERD
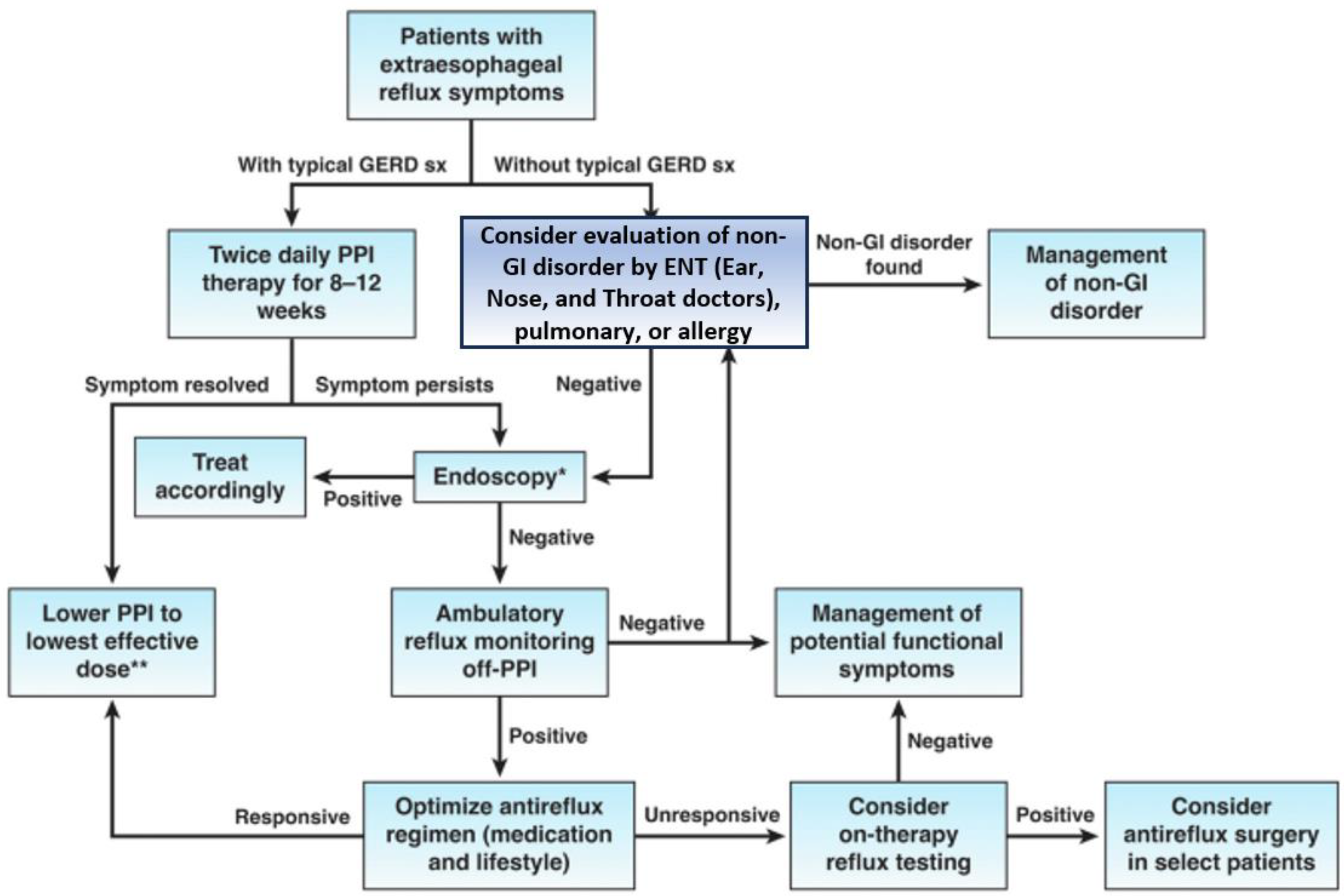
2.4. Management Treatment of GERD
3. Functional Food
3.1. Concept of Functional Food
- Conventional foods containing natural bioactive substances that naturally contain beneficial compounds, such as oat beta-glucan, fruits, and vegetables rich in lycopene and lutein.
- Foods modified via enrichment with bioactive substances: These foods are regular foods fortified or enriched with specific bioactive components, such as margarine with added phytosterols, calcium-fortified orange juice, or folic-acid-rich pomegranates.
- Foods intended for medicinal use, which are specialized formulae that resemble foods but are designed to be consumed as medicine via and according to a prescription, such as special formulas for children with medical conditions.
- Special dietary needs foods, which are formulated for specific requirements (gluten-free, lactose-free, and infant food).
- The identification of appropriate active ingredients: This entails a comprehensive investigation into the suitable active ingredients or combinations thereof, particularly when dealing with groups of related substances or the diverse bacteria used in probiotics.
- The determination of optimal concentrations: Rigorous research is essential to ascertain the optimal concentrations for the active ingredients present in functional foods.
- A concrete demonstration of health benefits: The claims should be attributed to functional foods. A rigorous and thorough demonstration of the purported health benefits must be executed through well-designed research.
- Thorough assessment of safety: Before marketing, a meticulous assessment of the safety of functional foods is indispensable in order to ensure consumer well-being and confidence [14].
3.2. Importance and Popularity of Functional Food
3.3. Key Characteristics and Benefits of Functional Food
- Fortified foods: Fortified foods are supplemented with additional nutrients to enhance their nutritional value, thereby addressing nutrient deficiencies and improving overall nutrition [93].
- Enriched foods: Enriched foods are designed to replenish nutrients lost while processing certain foods. An example is refined grains, like white flour, where vitamins and minerals are added to the product to compensate for the nutrients lost during the refining process [94].
- Modified foods: Modified foods undergo specific alterations to provide health benefits beyond basic nutrition. They include products with reduced fat or sugar content, gluten-free products, or low-sodium options [95].
- Naturally functional foods: Naturally functional foods are inherently rich in beneficial compounds and offer health benefits without requiring any modifications. Examples include fruits, vegetables, whole grains, nuts, and seeds. These foods naturally contain vitamins, minerals, antioxidants, fiber, and other bioactive compounds that promote health and well-being.
3.4. Preparation in Functional Food
- Increasing the concentration of beneficial components in foods [99].
4. Mechanism of Functional Food in GERD Mitigation
4.1. Reducing Acid Production
4.2. Soothing and Protecting the Esophagus
4.3. Enhancing Digestive Function
4.4. Alleviating Inflammation
5. Perspective
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ozkahraman Kırık, M.; Uslu Coskun, B. Gastroesophageal Reflux Disease BT—Airway Diseases; Cingi, C., Yorgancıoğlu, A., Bayar Muluk, N., Cruz, A.A., Eds.; Springer International Publishing: Cham, Switzerland, 2023; pp. 1–27. ISBN 978-3-031-22483-6. [Google Scholar]
- Durazzo, M.; Lupi, G.; Cicerchia, F.; Ferro, A.; Barutta, F.; Beccuti, G.; Gruden, G.; Pellicano, R. Extra-Esophageal Presentation of Gastroesophageal Reflux Disease: 2020 Update. J. Clin. Med. 2020, 9, 2559. [Google Scholar] [CrossRef] [PubMed]
- Chhabra, P.; Ingole, N. Gastroesophageal Reflux Disease (GERD): Highlighting Diagnosis, Treatment, and Lifestyle Changes. Cureus 2022, 14, e28563. [Google Scholar] [CrossRef] [PubMed]
- Širić, L.; Rosso, M.; Včev, A. Extraesophageal Manifestations and Symptoms of Esophageal Diseases. In Esophagitis and Gastritis; Neri, V., Ahmed, M., Eds.; IntechOpen: Rijeka, Croatia, 2021. [Google Scholar]
- Baker, M.T.; Lu, P.; Parrella, J.A.; Leggette, H.R. Consumer Acceptance toward Functional Foods: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 1217. [Google Scholar] [CrossRef]
- Newberry, C.; Lynch, K. The role of diet in the development and management of gastroesophageal reflux disease: Why we feel the burn. J. Thorac. Dis. 2019, 11, S1594–S1601. [Google Scholar] [CrossRef]
- Yadlapati, R.; Hubscher, E.; Pelletier, C.; Jacob, R.; Brackley, A.; Shah, S. Induction and maintenance of healing in erosive esophagitis in the United States. Expert Rev. Gastroenterol. Hepatol. 2022, 16, 967–980. [Google Scholar] [CrossRef]
- Meyiz, H.; El Agheb, M.; Lamine, A.; El Yousfi, M.; Aqodad, N.; Benajeh, D.; El Abkari, M.; Ibrahimi, A.; Mellouki, I. The Impact of Gastroesophageal Reflux on the Quality of Life: About a Series of 100 Patients at Fez University Hospital. Open J. Gastroenterol. 2019, 9, 99–108. [Google Scholar] [CrossRef]
- Gorczyca, R.; Pardak, P.; Pękala, A.; Filip, R. Impact of gastroesophageal reflux disease on the quality of life of Polish patients. World J. Clin. Cases 2019, 7, 1421–1429. [Google Scholar] [CrossRef]
- Alshammari, S.A.; Alabdulkareem, A.M.; Aloqeely, K.M.; Alhumud, M.I.; Alghufaily, S.A.; Al-Dossare, Y.I.; Alrashdan, N.O. The Determinants of the Quality of Life of Gastroesophageal Reflux Disease Patients Attending King Saud University Medical City. Cureus 2020, 12, e9505. [Google Scholar] [CrossRef]
- Rasool, M.F.; Sarwar, R.; Arshad, M.S.; Imran, I.; Saeed, H.; Majeed, A.; Akbar, M.; Chaudhry, M.O.; Rehman, A.U.; Ashraf, W.; et al. Assessing the frequency and risk factors associated with gastroesophageal reflux disease (GERD) in southern Punjab, Pakistan. Risk Manag. Healthc. Policy 2021, 14, 4619–4625. [Google Scholar] [CrossRef]
- Yuan, S.; Larsson, S.C. Adiposity, diabetes, lifestyle factors and risk of gastroesophageal reflux disease: A Mendelian randomization study. Eur. J. Epidemiol. 2022, 37, 747–754. [Google Scholar] [CrossRef]
- Kariri, A.M.; Darraj, M.A.; Wassly, A.; Arishi, H.A.; Lughbi, M.; Kariri, A.; Madkhali, A.M.; Ezzi, M.I.; Khawaji, B. Prevalence and Risk Factors of Gastroesophageal Reflux Disease in Southwestern Saudi Arabia. Cureus 2020, 12, 1–9. [Google Scholar] [CrossRef]
- Islam, S.M.R.; Siddiqua, T.J. 20—Functional Foods in Cancer Prevention and Therapy: Recent Epidemiological Findings. In Functional Foods in Cancer Prevention and Therapy; Academic Press: Cambridge, MA, USA, 2020; pp. 405–433. ISBN 978-0-12-816151-7. [Google Scholar]
- Fan, W.J.; Hou, Y.T.; Sun, X.H.; Li, X.Q.; Wang, Z.F.; Guo, M.; Zhu, L.M.; Wang, N.; Yu, K.; Li, J.N.; et al. Effect of high-fat, standard, and functional food meals on esophageal and gastric pH in patients with gastroesophageal reflux disease and healthy subjects. J. Dig. Dis. 2018, 19, 664–673. [Google Scholar] [CrossRef]
- Antunes, C.; Aleem, A.; Curtis, S.A. Gastroesophageal Reflux Disease. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Rettura, F.; Bronzini, F.; Campigotto, M.; Lambiase, C.; Pancetti, A.; Berti, G.; Marchi, S.; de Bortoli, N.; Zerbib, F.; Savarino, E.; et al. Refractory Gastroesophageal Reflux Disease: A Management Update. Front. Med. 2021, 8, 765061. [Google Scholar] [CrossRef]
- Zheng, Z.; Shang, Y.; Wang, N.; Liu, X.; Xin, C.; Yan, X.; Zhai, Y.; Yin, J.; Zhang, J.; Zhang, Z. Current Advancement on the Dynamic Mechanism of Gastroesophageal Reflux Disease. Int. J. Biol. Sci. 2021, 17, 4154–4164. [Google Scholar] [CrossRef] [PubMed]
- Carabotti, M.; Severi, C. Chapter 38—Upper Gastrointestinal Diseases before and after Bariatric Surgery. In Metabolism and Pathophysiology of Bariatric Surgery; Academic Press: Boston, MA, USA, 2017; pp. 343–349. ISBN 978-0-12-804011-9. [Google Scholar]
- Rodriguez, L.; Nurko, S. 64—Gastrointestinal Motility Procedures. In Pediatric Gastrointestinal and Liver Disease; Elsevier: Philadelphia, PN, USA, 2021; pp. 679–695.e4. ISBN 978-0-323-67293-1. [Google Scholar]
- Chen, R.R.; Chen, Q.Z.; Feng, B.C.; Wang, M.F.; Lin, L.; Ye, B.X.; Jiang, L.Q. Characteristics of reflux and gastric electrical activity in gastroesophageal reflux disease with ineffective esophageal motility. J. Dig. Dis. 2023, 24, 2–9. [Google Scholar] [CrossRef]
- MacFarlane, B. Management of gastroesophageal reflux disease in adults: A pharmacist’s perspective. Integr. Pharm. Res. Pract. 2018, 7, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Liu, D.; Feng, C.; Luo, Y.; Nian, Y.; Wang, X.; Zhang, J. The Characteristics of Postprandial Proximal Gastric Acid Pocket in Gastroesophageal Reflux Disease. Med. Sci. Monit. 2018, 24, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Sumi, S.; Ishimura, N.; Mikami, H.; Okimoto, E.; Tamagawa, Y.; Mishiro, T.; Kinoshita, Y.; Ishihara, S. Evaluations of Gastric Acid Pocket Using Novel Vertical 8-Channel pH Monitoring System and Effects of Acid Secretion Inhibitors. J. Neurogastroenterol. Motil. 2021, 27, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, S.E.; Zheng, P.; Sarici, I.S.; Shen, X.; Jobe, B.A.; Ayazi, S. The impact of delayed gastric emptying as measured by gastric emptying scintigraphy on the outcome of magnetic sphincter augmentation. Surg. Endosc. 2023. [Google Scholar] [CrossRef]
- Dunn, C.P.; Wu, J.; Gallagher, S.P.; Putnam, L.R.; Bildzukewicz, N.A.; Lipham, J.C. Understanding the GERD Barrier. J. Clin. Gastroenterol. 2021, 55, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Schwinghammer, T.L.; DiPiro, J.T.; Ellingrod, V.L.; DiPiro, C.V. Gastroesophageal Reflux Disease. In Pharmacotherapy Handbook, 11th ed.; McGraw Hill: New York, NY, USA, 2021. [Google Scholar]
- Patel, D.A.; Yadlapati, R.; Vaezi, M.F. Esophageal Motility Disorders: Current Approach to Diagnostics and Therapeutics. Gastroenterology 2022, 162, 1617–1634. [Google Scholar] [CrossRef]
- Abdelghani, A.; Ibrahim, A.; El-Sayed, E.S.; El Sherbiny, M.; Al-Badry, A. Esophageal motility disorders in symptomatic patients and its relation to age. BMC Gastroenterol. 2023, 23, 69. [Google Scholar] [CrossRef]
- Agostinis, C.; Bossi, F.; Mangogna, A.; Balduit, A.; Pacor, M.; Giacomello, E.; Belmonte, B.; Greco, D.; Rodolico, V.; Voinovich, D.; et al. Protective and regenerative effects of a novel medical device against esophageal mucosal damage using in vitro and ex vivo models. Biomed. Pharmacother. 2020, 131, 110752. [Google Scholar] [CrossRef]
- Ustaoglu, A.; Nguyen, A.; Spechler, S.; Sifrim, D.; Souza, R.; Woodland, P. Mucosal pathogenesis in gastro-esophageal reflux disease. Neurogastroenterol. Motil. 2020, 32, e14022. [Google Scholar] [CrossRef] [PubMed]
- Sfara, A.; Dumitrascu, D.L. The management of hiatal hernia: An update on diagnosis and treatment. Med. Pharm. Rep. 2019, 92, 321–325. [Google Scholar] [CrossRef]
- Zheng, Z.; Liu, X.; Xin, C.; Zhang, W.; Gao, Y.; Zeng, N.; Li, M.; Cai, J.; Meng, F.; Liu, D.; et al. A new technique for treating hiatal hernia with gastroesophageal reflux disease: The laparoscopic total left-side surgical approach. BMC Surg. 2021, 21, 361. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Yadlapati, R. Pathophysiology and treatment options for gastroesophageal reflux disease: Looking beyond acid. Ann. N. Y. Acad. Sci. 2021, 1486, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Marabotto, E.; Savarino, V.; Ghisa, M.; Frazzoni, M.; Ribolsi, M.; Barberio, B.; Savarino, E. Advancements in the use of 24-hour impedance-pH monitoring for GERD diagnosis. Curr. Opin. Pharmacol. 2022, 65, 102264. [Google Scholar] [CrossRef]
- Czarniak, P.; Ahmadizar, F.; Hughes, J.; Parsons, R.; Kavousi, M.; Ikram, M.; Stricker, B.H. Proton pump inhibitors are associated with incident type 2 diabetes mellitus in a prospective population-based cohort study. Br. J. Clin. Pharmacol. 2022, 88, 2718–2726. [Google Scholar] [CrossRef]
- Robinson, B.J. Regular use of PPIs linked with increased risk of type 2 diabetes, study suggests. Pharm. J. 2020, 2–4. [Google Scholar] [CrossRef]
- Rajput, M.A.; Ali, F.; Zehra, T.; Zafar, S.; Kumar, G. The effect of proton pump inhibitors on glycaemic control in diabetic patients. J. Taibah Univ. Med. Sci. 2020, 15, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.-M.; Tan, J.-C.; Zhu, Y.; Lin, L. Association between diabetes mellitus and gastroesophageal reflux disease: A meta-analysis. World J. Gastroenterol. 2015, 21, 3085–3092. [Google Scholar] [CrossRef] [PubMed]
- Althoff, M.D.; Sharma, S. Gastroesophageal Reflux, Atopic Dermatitis, and Asthma: Finally Evidence for Causal Links? Am. J. Respir. Crit. Care Med. 2023, 207, 117–118. [Google Scholar] [CrossRef] [PubMed]
- Grandes, X.A.; Talanki Manjunatha, R.; Habib, S.; Sangaraju, S.L.; Yepez, D. Gastroesophageal Reflux Disease and Asthma: A Narrative Review. Cureus 2022, 14, e24917. [Google Scholar] [CrossRef]
- Lin, H.-C.; Xirasagar, S.; Chung, S.-D.; Huang, C.-C.; Tsai, M.-C.; Chen, C.-H. Fewer acute respiratory infection episodes among patients receiving treatment for gastroesophageal reflux disease. PLoS ONE 2017, 12, e0172436. [Google Scholar] [CrossRef]
- Sharma, P. Barrett Esophagus: A Review. JAMA 2022, 328, 663–671. [Google Scholar] [CrossRef]
- Souza, R.F.; Spechler, S.J. Mechanisms and pathophysiology of Barrett oesophagus. Nat. Rev. Gastroenterol. Hepatol. 2022, 19, 605–620. [Google Scholar] [CrossRef]
- Mahajan, R.; Kulkarni, R.; Stoopler, E.T. Gastroesophageal reflux disease and oral health: A narrative review. Spec. Care Dent. Off. Publ. Am. Assoc. Hosp. Dent. Acad. Dent. Handicap. Am. Soc. Geriatr. Dent. 2022, 42, 555–564. [Google Scholar] [CrossRef]
- Shah, S. COVID-19 and paediatric dentistry- traversing the challenges. A narrative review. Ann. Med. Surg. 2020, 58, 22–33. [Google Scholar] [CrossRef]
- Chakraborty, A.; Anjankar, A.P. Association of Gastroesophageal Reflux Disease with Dental Erosion. Cureus 2022, 14, e30381. [Google Scholar] [CrossRef]
- Howard, J.P.; Howard, L.J.; Geraghty, J.; Leven, A.J.; Ashley, M. Gastrointestinal conditions related to tooth wear. Br. Dent. J. 2023, 234, 451–454. [Google Scholar] [CrossRef] [PubMed]
- Grossi, L.; Ciccaglione, A.F.; Marzio, L. World Journal of Gastroenterology. World J. Gastroenterol. 2017, 7, 3011–3016. [Google Scholar] [CrossRef] [PubMed]
- Heidarzadeh-Esfahani, N.; Soleimani, D.; Hajiahmadi, S.; Moradi, S.; Heidarzadeh, N.; Nachvak, S.M. Dietary Intake in Relation to the Risk of Reflux Disease: A Systematic Review. Prev. Nutr. Food Sci. 2021, 26, 367–379. [Google Scholar] [CrossRef] [PubMed]
- Chamorro, R.; Kannenberg, S.; Wilms, B.; Kleinerüschkamp, C.; Meyhöfer, S.; Park, S.Q.; Lehnert, H.; Oster, H.; Meyhöfer, S.M. Meal Timing and Macronutrient Composition Modulate Human Metabolism and Reward-Related Drive to Eat. Nutrients 2022, 14, 562. [Google Scholar] [CrossRef]
- Fox, M.; Gyawali, C.P. Dietary factors involved in GERD management. Best Pract. Res. Clin. Gastroenterol. 2023, 62–63, 101826. [Google Scholar] [CrossRef]
- Wildi, S.M.; Tutuian, R.; Castell, D.O. The Influence of Rapid Food Intake on Postprandial Reflux: Studies in Healthy Volunteers. Off. J. Am. Coll. Gastroenterol. | ACG 2004, 99, 1645–1651. [Google Scholar] [CrossRef]
- Mangano, M.; Colombo, P.; Bianchi, P.A.; Penagini, R. Fat and Esophageal Sensitivity to Acid. Dig. Dis. Sci. 2002, 47, 657–660. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Su, Z.; Li, P.; Li, Y.; Johnson, N.; Zhang, Q.; Du, S.; Zhao, H.; Li, K.; Zhang, C.; et al. Association of Symptoms with Eating Habits and Food Preferences in Chronic Gastritis Patients: A Cross-Sectional Study. Evid.-Based Complement. Altern. Med. 2020, 2020, 5197201. [Google Scholar] [CrossRef]
- Fox, M.; Barr, C.; Nolan, S.; Lomer, M.; Anggiansah, A.; Wong, T. The effects of dietary fat and calorie density on esophageal acid exposure and reflux symptoms. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2007, 5, 439–444. [Google Scholar] [CrossRef]
- Zhang, M.; Hou, Z.-K.; Huang, Z.-B.; Chen, X.-L.; Liu, F.-B. Dietary and Lifestyle Factors Related to Gastroesophageal Reflux Disease: A Systematic Review. Ther. Clin. Risk Manag. 2021, 17, 305–323. [Google Scholar] [CrossRef]
- Beigrezaei, S.; Sasanfar, B.; Nafei, Z.; Behniafard, N.; Aflatoonian, M.; Salehi-Abargouei, A. Dietary approaches to stop hypertension (DASH)-style diet in association with gastroesophageal reflux disease in adolescents. BMC Public Health 2023, 23, 358. [Google Scholar] [CrossRef]
- Keshteli, A.H.; Shaabani, P.; Tabibian, S.-R.; Saneei, P.; Esmaillzadeh, A.; Adibi, P. The relationship between fruit and vegetable intake with gastroesophageal reflux disease in Iranian adults. J. Res. Med. Sci. Off. J. Isfahan Univ. Med. Sci. 2017, 22, 125. [Google Scholar] [CrossRef]
- Yuan, L.Z.; Yi, P.; Wang, G.S.; Tan, S.Y.; Huang, G.M.; Qi, L.Z.; Jia, Y.; Wang, F. Lifestyle intervention for gastroesophageal reflux disease: A national multicenter survey of lifestyle factor effects on gastroesophageal reflux disease in China. Therap. Adv. Gastroenterol. 2019, 12, 1756284819877788. [Google Scholar] [CrossRef]
- Myung, S.-K.; Kim, H.-B.; Lee, Y.-J.; Choi, Y.-J.; Oh, S.-W. Calcium Supplements and Risk of Cardiovascular Disease: A Meta-Analysis of Clinical Trials. Nutrients 2021, 13, 368. [Google Scholar] [CrossRef]
- Morelli, M.B.; Santulli, G.; Gambardella, J. Calcium supplements: Good for the bone, bad for the heart? A systematic updated appraisal. Atherosclerosis 2020, 296, 68–73. [Google Scholar] [CrossRef]
- Özenoğlu, A.; Anul, N.; Özçelikçi, B. The relationship of gastroesophageal reflux with nutritional habits and mental disorders. Hum. Nutr. Metab. 2023, 33, 200203. [Google Scholar] [CrossRef]
- Basharat, S.; Binté, F.; Amir, S.; Zubair, M. Association of Dietary Practices and Lifestyle Modifications in Gastroesophageal Reflux Disease in Pakistani Women. Am. Sci. Res. J. Eng. Technol. Sci. 2020, 64, 43–52. [Google Scholar]
- Chen, J.W.; Vela, M.F.; Peterson, K.A.; Carlson, D.A. AGA Clinical Practice Update on the Diagnosis and Management of Extraesophageal Gastroesophageal Reflux Disease: Expert Review. Clin. Gastroenterol. Hepatol. 2023, 21, 1414–1421.e3. [Google Scholar] [CrossRef]
- Lee, D.P.; Chang, K.J. Endoscopic Management of GERD. Dig. Dis. Sci. 2022, 67, 1455–1468. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.H.; Vasas, D.; Hassan, A.; Molnár, J. The impact of functional food in prevention of malnutrition. PharmaNutrition 2022, 19, 100288. [Google Scholar] [CrossRef]
- Guadagnoli, L.; Simons, M.; McGarva, J.; Taft, T.H.; van Tilburg, M.A.L. Improving Patient Adherence to Lifestyle Changes for the Management of Gastroesophageal Reflux. Patient Prefer. Adherence 2022, 16, 897–909. [Google Scholar] [CrossRef] [PubMed]
- Wilks, A.; Panahi, L.; Udeani, G.; Surani, S. Review of Gastroesophageal Reflux Pharmacotherapy Management. In Gastroesophageal Reflux Disease; Chai, J., Ed.; IntechOpen: Rijeka, Croatia, 2022; Chapter 4; ISBN 978-1-80355-958-2. [Google Scholar]
- Kröner, P.T.; Cortés, P.; Lukens, F.J. The Medical Management of Gastroesophageal Reflux Disease: A Narrative Review. J. Prim. Care Community Health 2021, 12, 21501327211046736. [Google Scholar] [CrossRef] [PubMed]
- Turaga, A.H.; Salem, Y.H. Transoral incisionless fundoplication and open hiatal hernia repair: A case report. Front. Gastroenterol. 2023, 2, 1207659. [Google Scholar] [CrossRef]
- Bell, R.C.W. Beyond Proton Pump Inhibitors and Nissen Fundoplication: Minimally Invasive Alternatives for Gastroesophageal Reflux Disease. Gastroenterol. Hepatol. 2021, 17, 553–555. [Google Scholar]
- Dumitru, V.; Hoara, P.; Dumitru, D.; Birla, R.; Gindea, C.; Constantinoiu, S. Invasive Treatment Options for Gastro-Esophageal Reflux Disease. J. Med. Life 2020, 13, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Hoffsten, J.; Forsell, Y. Laparoscopic Nissen fundoplication versus 90° and 180° fundoplication for gastroesophageal reflux disease: Systematic review and meta-analysis of 5-year outcomes. Eur. Surg.—Acta Chir. Austriaca 2022, 54, 66–73. [Google Scholar] [CrossRef]
- Loo, G.H.; Rajan, R.; Deva Tata, M.; Ritza Kosai, N. Changes in the disease-specific quality of life following Dor fundoplication. A multicentre cross-sectional study. Ann. Med. Surg. 2020, 55, 252–255. [Google Scholar] [CrossRef]
- Tjeerdsma, M.; Quinn, K.R.; Helmer, S.D.; Vincent, K.B. Comparing Outcomes of Robotic-Assisted versus Conventional Laparoscopic Hiatal Hernia Repair. Kansas J. Med. 2022, 15, 365–368. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Rahut, D.B. Healthy Foods as Proxy for Functional Foods: Consumers’ Awareness, Perception, and Demand for Natural Functional Foods in Pakistan. Int. J. Food Sci. 2019, 2019, 6390650. [Google Scholar] [CrossRef]
- Vettorazzi, A.; López de Cerain, A.; Sanz-Serrano, J.; Gil, A.G.; Azqueta, A. European Regulatory Framework and Safety Assessment of Food-Related Bioactive Compounds. Nutrients 2020, 12, 613. [Google Scholar] [CrossRef]
- Arnold, M.; Rajagukguk, Y.V.; Gramza-Michałowska, A. Functional food for elderly high in antioxidant and chicken eggshell calcium to reduce the risk of osteoporosis—A narrative review. Foods 2021, 10, 656. [Google Scholar] [CrossRef]
- González-Díaz, C.; Vilaplana-Aparicio, M.J.; Iglesias-García, M. How Is Functional Food Advertising Understood? An Approximation in University Students. Nutrients 2020, 12, 3312. [Google Scholar] [CrossRef]
- Siró, I.; Kápolna, E.; Kápolna, B.; Lugasi, A. Functional food. Product development, marketing and consumer acceptance—A review. Appetite 2008, 51, 456–467. [Google Scholar] [CrossRef]
- Budreviciute, A.; Damiati, S.; Sabir, D.K.; Onder, K.; Schuller-Goetzburg, P.; Plakys, G.; Katileviciute, A.; Khoja, S.; Kodzius, R. Management and Prevention Strategies for Non-communicable Diseases (NCDs) and Their Risk Factors. Front. Public Health 2020, 8, 574111. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Zhang, B.; Tian, W.; Wei, Y.; Wang, F.; Yin, X.; Wei, X.; Liu, J.; Tang, X. Trends in gastroesophageal reflux disease research: A bibliometric and visualized study. Front. Med. 2022, 9, 994534. [Google Scholar] [CrossRef] [PubMed]
- Aman, F.; Masood, S. How Nutrition can help to fight against COVID-19 Pandemic. Pakistan J. Med. Sci. 2020, 36, S121–S123. [Google Scholar] [CrossRef] [PubMed]
- Topolska, K.; Florkiewicz, A.; Filipiak-Florkiewicz, A. Functional Food-Consumer Motivations and Expectations. Int. J. Environ. Res. Public Health 2021, 18, 5327. [Google Scholar] [CrossRef] [PubMed]
- Gu, S.; Ślusarczyk, B.; Hajizada, S.; Kovalyova, I.; Sakhbieva, A. Impact of the COVID-19 pandemic on online consumer purchasing behavior. J. Theor. Appl. Electron. Commer. Res. 2021, 16, 2263–2281. [Google Scholar] [CrossRef]
- Schifferstein, H.N.J.; de Boer, A.; Lemke, M. Conveying information through food packaging: A literature review comparing legislation with consumer perception. J. Funct. Foods 2021, 86, 104734. [Google Scholar] [CrossRef]
- Wang, H.; Ab Gani, M.A.A.; Liu, C. Impact of Snack Food Packaging Design Characteristics on Consumer Purchase Decisions. SAGE Open 2023, 13, 21582440231167109. [Google Scholar] [CrossRef]
- Nguyen, N.; Nguyen, H.V.; Nguyen, P.T.; Tran, V.T.; Nguyen, H.N.; Nguyen, T.M.N.; Cao, T.K.; Nguyen, T.H. Some Key Factors Affecting Consumers’ Intentions to Purchase Functional Foods: A Case Study of Functional Yogurts in Vietnam. Foods 2019, 9, 24. [Google Scholar] [CrossRef] [PubMed]
- FDA. Label Claim for Food & Dietary Supplements; FDA: Washington, DC, USA, 2004; pp. 1–14. [Google Scholar]
- Fernández-Ríos, A.; Laso, J.; Hoehn, D.; Amo-Setién, F.J.; Abajas-Bustillo, R.; Ortego, C.; Fullana-i-Palmer, P.; Bala, A.; Batlle-Bayer, L.; Balcells, M.; et al. A critical review of superfoods from a holistic nutritional and environmental approach. J. Clean. Prod. 2022, 379, 134491. [Google Scholar] [CrossRef]
- Jagdale, Y.D.; Mahale, S.V.; Zohra, B.; Nayik, G.A.; Dar, A.H.; Ali Khan, K.; Abdi, G.; Karabagias, I.K. Nutritional profile and potential health benefits of super foods: A review. Sustainability 2021, 13, 9240. [Google Scholar] [CrossRef]
- Santillán-Urquiza, E.; Ruiz-Espinosa, H.; Angulo-Molina, A.; Vélez Ruiz, J.F.; Méndez-Rojas, M.A. 8—Applications of nanomaterials in functional fortified dairy products: Benefits and implications for human health. In Nutrient Delivery; Nanotechnology in the Agri-Food Industry; Academic Press: Cambridge, MA, USA, 2017; pp. 293–328. ISBN 978-0-12-804304-2. [Google Scholar]
- Sadler, C.R.; Grassby, T.; Hart, K.; Raats, M.; Sokolović, M.; Timotijevic, L. Processed food classification: Conceptualisation and challenges. Trends Food Sci. Technol. 2021, 112, 149–162. [Google Scholar] [CrossRef]
- Smyth, S.J. The human health benefits from GM crops. Plant Biotechnol. J. 2020, 18, 887–888. [Google Scholar] [CrossRef] [PubMed]
- Martirosyan, D.; Lampert, T.; Lee, M. A comprehensive review on the role of food bioactive compounds in functional food science. Funct. Food Sci. 2022, 2, 64. [Google Scholar] [CrossRef]
- Muncke, J.; Andersson, A.M.; Backhaus, T.; Boucher, J.M.; Carney Almroth, B.; Castillo Castillo, A.; Chevrier, J.; Demeneix, B.A.; Emmanuel, J.A.; Fini, J.B.; et al. Impacts of food contact chemicals on human health: A consensus statement. Environ. Health A Glob. Access Sci. Source 2020, 19, 25. [Google Scholar] [CrossRef]
- Yuan, S.; Li, C.; Zhang, Y.; Yu, H.; Xie, Y.; Guo, Y.; Yao, W. Ultrasound as an emerging technology for the elimination of chemical contaminants in food: A review. Trends Food Sci. Technol. 2021, 109, 374–385. [Google Scholar] [CrossRef]
- Liu, R.H. Health-promoting components of fruits and vegetables in the diet. Adv. Nutr. 2013, 4, 384S–392S. [Google Scholar] [CrossRef]
- Martínez, E.; Pardo, J.E.; Rabadán, A.; Álvarez-Ortí, M. Effects of Animal Fat Replacement by Emulsified Melon and Pumpkin Seed Oils in Deer Burgers. Foods 2023, 12, 1279. [Google Scholar] [CrossRef]
- Astrup, A.; Magkos, F.; Bier, D.M.; Brenna, J.T.; de Oliveira Otto, M.C.; Hill, J.O.; King, J.C.; Mente, A.; Ordovas, J.M.; Volek, J.S.; et al. Saturated Fats and Health: A Reassessment and Proposal for Food-Based Recommendations: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 76, 844–857. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Mhaske, P.; Farahnaky, A.; Kasapis, S.; Majzoobi, M. Cassava starch: Chemical modification and its impact on functional properties and digestibility, a review. Food Hydrocoll. 2022, 129, 107542. [Google Scholar] [CrossRef]
- Arshad, R.; Gulshad, L.; Haq, I.U.; Farooq, M.A.; Al-Farga, A.; Siddique, R.; Manzoor, M.F.; Karrar, E. Nanotechnology: A novel tool to enhance the bioavailability of micronutrients. Food Sci. Nutr. 2021, 9, 3354–3361. [Google Scholar] [CrossRef] [PubMed]
- Xiong, K.; Zhou, L.; Wang, J.; Ma, A.; Fang, D.; Xiong, L.; Sun, Q. Construction of food-grade pH-sensitive nanoparticles for delivering functional food ingredients. Trends Food Sci. Technol. 2020, 96, 102–113. [Google Scholar] [CrossRef]
- Putnik, P.; Kovačević, D.B. Sustainable functional food processing. Foods 2021, 10, 1438. [Google Scholar] [CrossRef]
- Knorr, D.; Augustin, M.A.; Tiwari, B. Advancing the Role of Food Processing for Improved Integration in Sustainable Food Chains. Front. Nutr. 2020, 7, 34. [Google Scholar] [CrossRef]
- Kasote, D.; Tiozon, R.N.; Sartagoda, K.J.D.; Itagi, H.; Roy, P.; Kohli, A.; Regina, A.; Sreenivasulu, N. Food Processing Technologies to Develop Functional Foods with Enriched Bioactive Phenolic Compounds in Cereals. Front. Plant Sci. 2021, 12, 771276. [Google Scholar] [CrossRef]
- Morozov, S.; Isakov, V.; Konovalova, M. Fiber-enriched diet helps to control symptoms and improves esophageal motility in patients with non-erosive gastroesophageal reflux disease. World J. Gastroenterol. 2018, 24, 2291–2299. [Google Scholar] [CrossRef]
- Hong, S.W.; Chun, J.; Park, S.; Lee, H.J.; Im, J.P.; Kim, J.S. Aloe vera Is Effective and Safe in Short-term Treatment of Irritable Bowel Syndrome: A Systematic Review and Meta-analysis. J. Neurogastroenterol. Motil. 2018, 24, 528–535. [Google Scholar] [CrossRef]
- Kontareva, V.Y.; Belik, S.N.; Morgul, E.V.; Gorlov, I.F.; Slozhenkina, M.I. Yogurt enriched to correct intestinal microflora in dysbiosis. IOP Conf. Ser. Earth Environ. Sci. 2020, 548, 082051. [Google Scholar] [CrossRef]
- Zhai, Z.; Wang, J.; Huang, B.; Yin, S. Low-fat yogurt alleviates the pro-inflammatory cytokine IL-1β-induced intestinal epithelial barrier dysfunction. J. Dairy Sci. 2019, 102, 976–984. [Google Scholar] [CrossRef] [PubMed]
- Ioniță-Mîndrican, C.-B.; Ziani, K.; Mititelu, M.; Oprea, E.; Neacșu, S.M.; Moroșan, E.; Dumitrescu, D.-E.; Roșca, A.C.; Drăgănescu, D.; Negrei, C. Therapeutic Benefits and Dietary Restrictions of Fiber Intake: A State of the Art Review. Nutrients 2022, 14, 2641. [Google Scholar] [CrossRef] [PubMed]
- Muliawati, E.; Carolin, B.T.; Lail, N.H. Comparison Between the Provision of White Ambon Banana Fruit and Red Dragon Fruit on Hemoglobin Levels. Nurs. Health Sci. J. 2022, 2, 87–93. [Google Scholar] [CrossRef]
- Zou, F.; Tan, C.; Zhang, B.; Wu, W.; Shang, N. The Valorization of Banana By-Products: Nutritional Composition, Bioactivities, Applications, and Future Development. Foods 2022, 11, 3170. [Google Scholar] [CrossRef]
- Nikkhah Bodagh, M.; Maleki, I.; Hekmatdoost, A. Ginger in gastrointestinal disorders: A systematic review of clinical trials. Food Sci. Nutr. 2019, 7, 96–108. [Google Scholar] [CrossRef]
- Schulz, R.M.; Ahuja, N.K.; Slavin, J.L. Effectiveness of Nutritional Ingredients on Upper Gastrointestinal Conditions and Symptoms: A Narrative Review. Nutrients 2022, 14, 672. [Google Scholar] [CrossRef]
- Valussi, M. Functional foods with digestion-enhancing properties. Int. J. Food Sci. Nutr. 2012, 63, 82–89. [Google Scholar] [CrossRef]
- Fiorini, G.; Saracino, I.M.; Pavoni, M.; Saccomanno, L.; Vaira, D. Efficacy of a new nutraceutical formulation (CHETOGERD(®)) in patients with nonerosive reflux disease (NERD): A prospective observational study. Intern. Emerg. Med. 2020, 15, 1265–1269. [Google Scholar] [CrossRef]
- Valdes, A.M.; Walter, J.; Segal, E.; Spector, T.D. Role of the gut microbiota in nutrition and health. BMJ 2018, 361, k2179. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, P.; Zhang, X. Probiotics Regulate Gut Microbiota: An Effective Method to Improve Immunity. Molecules 2021, 26, 6076. [Google Scholar] [CrossRef]
- Dahiya, D.; Nigam, P.S. The Gut Microbiota Influenced by the Intake of Probiotics and Functional Foods with Prebiotics Can Sustain Wellness and Alleviate Certain Ailments like Gut-Inflammation and Colon-Cancer. Microorganisms 2022, 10, 665. [Google Scholar] [CrossRef]
- Das, T.K.; Pradhan, S.; Chakrabarti, S.; Mondal, K.C.; Ghosh, K. Current status of probiotic and related health bene-fits. Appl. Food Res. 2022, 2, 100185. [Google Scholar] [CrossRef]
- Cheng, J.; Ouwehand, A.C. Gastroesophageal Reflux Disease and Probiotics: A Systematic Review. Nutrients 2020, 12, 132. [Google Scholar] [CrossRef] [PubMed]
- Rollet, M.; Bohn, T.; Vahid, F.; ORISCAV Working Group. Association between Dietary Factors and Constipation in Adults Living in Luxembourg and Taking Part in the ORISCAV-LUX 2 Survey. Nutrients 2021, 14, 122. [Google Scholar] [CrossRef]
- Heidelbaugh, J.J.; Nostrant, T.T.; Kim, C.; Van Harrison, R. Management of gastroesophageal reflux disease. Am. Fam. Physician 2003, 68, 1311–1318+1321. [Google Scholar]
- Hamid, N.K.A.; Somdare, P.O.; Md Harashid, K.A.; Othman, N.A.; Kari, Z.A.; Wei, L.S.; Dawood, M.A.O. Effect of papaya (Carica papaya) leaf extract as dietary growth promoter supplement in red hybrid tilapia (Oreochromis mossambicus × Oreochromis niloticus) diet. Saudi J. Biol. Sci. 2022, 29, 3911–3917. [Google Scholar] [CrossRef] [PubMed]
- Kostiuchenko, O.; Kravchenko, N.; Markus, J.; Burleigh, S.; Fedkiv, O.; Cao, L.; Letasiova, S.; Skibo, G.; Fåk Hållenius, F.; Prykhodko, O. Effects of Proteases from Pineapple and Papaya on Protein Digestive Capacity and Gut Microbiota in Healthy C57BL/6 Mice and Dose-Manner Response on Mucosal Permeability in Human Reconstructed Intestinal 3D Tissue Model. Metabolites 2022, 12, 1027. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Ao, M.; Dong, B.; Jiang, Y.; Yu, L.; Chen, Z.; Hu, C.; Xu, R. Anti-Inflammatory Effects of Curcumin in the Inflammatory Diseases: Status, Limitations and Countermeasures. Drug Des. Devel. Ther. 2021, 15, 4503–4525. [Google Scholar] [CrossRef] [PubMed]
- Sharifi-Rad, J.; Rayess, Y.E.; Rizk, A.A.; Sadaka, C.; Zgheib, R.; Zam, W.; Sestito, S.; Rapposelli, S.; Neffe-Skocińska, K.; Zielińska, D.; et al. Turmeric and Its Major Compound Curcumin on Health: Bioactive Effects and Safety Profiles for Food, Pharmaceutical, Biotechnological and Medicinal Applications. Front. Pharmacol. 2020, 11, 1021. [Google Scholar] [CrossRef]
- Kwiecien, S.; Magierowski, M.; Majka, J.; Ptak-Belowska, A.; Wójcik-Grzybek, D.; Sliwowski, Z.; Magierowska, K.; Brzozowski, T. Curcumin: A Potent Protectant against Esophageal and Gastric Disorders. Int. J. Mol. Sci. 2019, 20, 1477. [Google Scholar] [CrossRef]
- Santos, H.O.; May, T.L.; Bueno, A.A. Eating more sardines instead of fish oil supplementation: Beyond omega-3 polyunsaturated fatty acids, a matrix of nutrients with cardiovascular benefits. Front. Nutr. 2023, 10, 1107475. [Google Scholar] [CrossRef] [PubMed]
- Oh, D.Y.; Walenta, E. Omega-3 Fatty Acids and FFAR4. Front. Endocrinol. 2014, 5, 115. [Google Scholar] [CrossRef] [PubMed]
- Fabisiak, A.; Bartoszek, A.; Talar, M.; Binienda, A.; Dziedziczak, K.; Krajewska, J.B.; Mosińska, P.; Niewinna, K.; Tarasiuk, A.; Mokrowiecka, A.; et al. Expression of FFAR3 and FFAR4 Is Increased in Gastroesophageal Reflux Disease. J. Clin. Med. 2020, 9, 4111. [Google Scholar] [CrossRef]
- Ozkur, M.; Benlier, N.; Takan, I.; Vasileiou, C.; Georgakilas, A.G.; Pavlopoulou, A.; Cetin, Z.; Saygili, E.I. Ginger for Healthy Ageing: A Systematic Review on Current Evidence of Its Antioxidant, Anti-Inflammatory, and Anticancer Properties. Oxid. Med. Cell. Longev. 2022, 2022, 4748447. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Shukla, M.K.; Sharma, K.C.; Tirath; Kumar, L.; Anal, J.M.H.; Upadhyay, S.K.; Bhattacharyya, S.; Kumar, D. Revisiting the therapeutic potential of gingerols against different pharmacological activities. Naunyn. Schmiedebergs. Arch. Pharmacol. 2023, 396, 633–647. [Google Scholar] [CrossRef]
- Kim, K.J.; Kim, S.H.; Shin, M.-R.; Kim, Y.J.; Park, H.-J.; Roh, S.-S. Protective effect of S-allyl cysteine-enriched black garlic on reflux esophagitis in rats via NF-κB signaling pathway. J. Funct. Foods 2019, 58, 199–206. [Google Scholar] [CrossRef]
- Granato, D.; Barba, F.J.; Bursać Kovačević, D.; Lorenzo, J.M.; Cruz, A.G.; Putnik, P. Functional Foods: Product Development, Technological Trends, Efficacy Testing, and Safety. Annu. Rev. Food Sci. Technol. 2020, 11, 93–118. [Google Scholar] [CrossRef]
- Huang, L.; Bai, L.; Gong, S. The effects of carrier, benefit, and perceived trust in information channel on functional food purchase intention among Chinese consumers. Food Qual. Prefer. 2020, 81, 103854. [Google Scholar] [CrossRef]
- Konstantinidi, M.; Koutelidakis, A.E. Functional Foods and Bioactive Compounds: A Review of Its Possible Role on Weight Management and Obesity’s Metabolic Consequences. Medicines 2019, 6, 94. [Google Scholar] [CrossRef]
- Sumaedi, S.; Sumardjo; Saleh, A.; Syukri, A.F. Factors influencing males’ loyalty toward functional foods during the COVID-19 pandemic. Int. J. Public Health Sci. 2022, 11, 121–128. [Google Scholar] [CrossRef]
- Thalheimer, A.; Bueter, M. Excess Body Weight and Gastroesophageal Reflux Disease. Visc. Med. 2021, 37, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Seki, Y.; Kasama, K.; Amiki, M.; Baba, S.; Ito, M.; Tanaka, T.; Kanehira, E. Prevalence of reflux esophagitis in obese Japanese undergoing bariatric surgery. JGH Open 2020, 4, 519–524. [Google Scholar] [CrossRef]
- Green, M.; Arora, K.; Prakash, S. Microbial Medicine: Prebiotic and Probiotic Functional Foods to Target Obesity and Metabolic Syndrome. Int. J. Mol. Sci. 2020, 21, 2890. [Google Scholar] [CrossRef] [PubMed]
- Sandner, G.; König, A.; Wallner, M.; Weghuber, J. Functional foods—Dietary or herbal products on obesity: Application of selected bioactive compounds to target lipid metabolism. Curr. Opin. Food Sci. 2020, 34, 9–20. [Google Scholar] [CrossRef]
- Gupta, E.; Mishra, P. Functional Food with Some Health Benefits, So Called Superfood: A Review. Curr. Nutr. Food Sci. 2021, 17, 144–166. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herdiana, Y. Functional Food in Relation to Gastroesophageal Reflux Disease (GERD). Nutrients 2023, 15, 3583. https://doi.org/10.3390/nu15163583
Herdiana Y. Functional Food in Relation to Gastroesophageal Reflux Disease (GERD). Nutrients. 2023; 15(16):3583. https://doi.org/10.3390/nu15163583
Chicago/Turabian StyleHerdiana, Yedi. 2023. "Functional Food in Relation to Gastroesophageal Reflux Disease (GERD)" Nutrients 15, no. 16: 3583. https://doi.org/10.3390/nu15163583
APA StyleHerdiana, Y. (2023). Functional Food in Relation to Gastroesophageal Reflux Disease (GERD). Nutrients, 15(16), 3583. https://doi.org/10.3390/nu15163583