
Accuracy in Determining the Glycaemic Impact of Meals by Adding Individual Food Values Is Affected by Food Number, Homeostasis and Glucose Reference Dose


Abstract
:1. Introduction
2. Materials and Methods
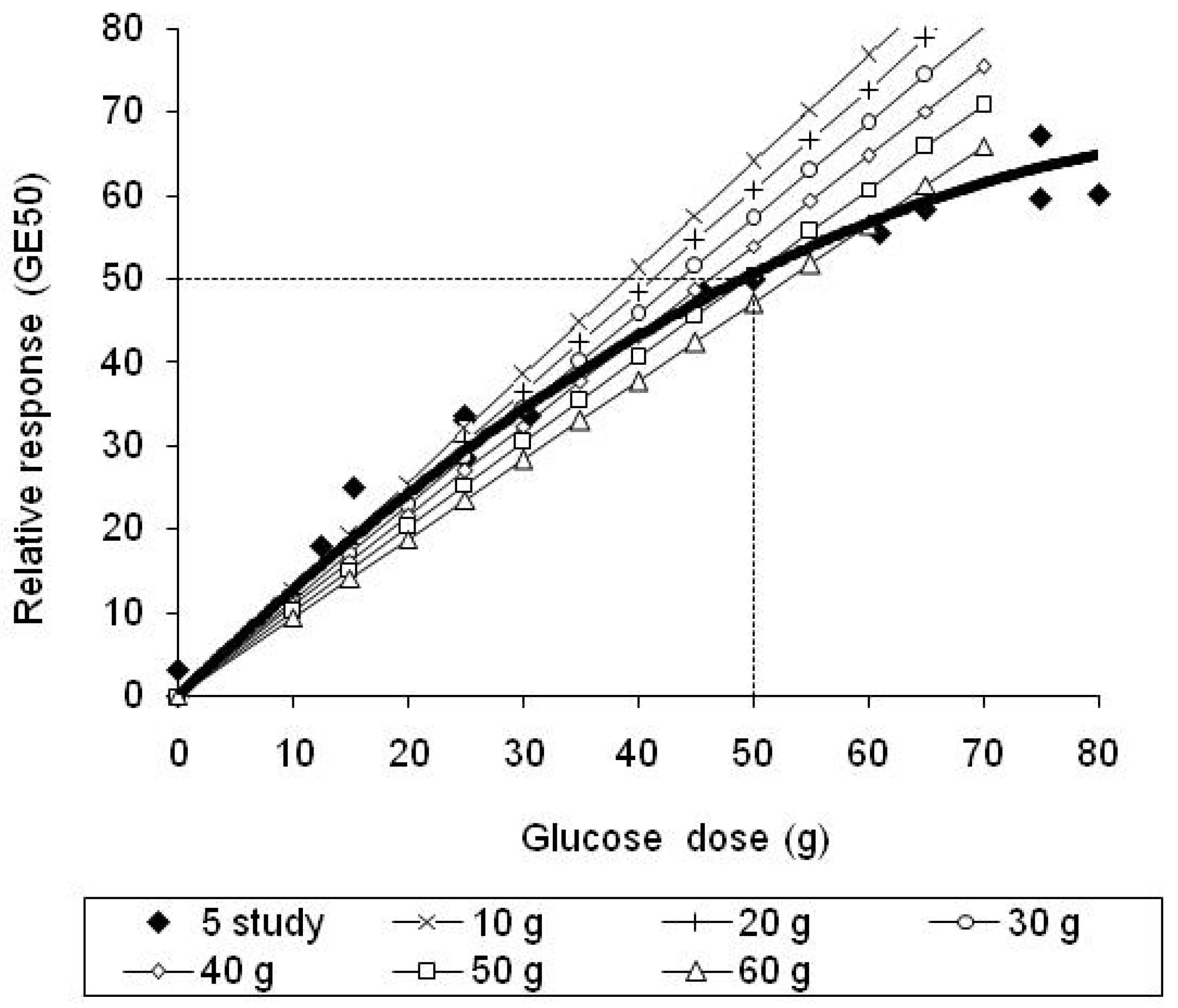
2.1. Establishing a Glucose Dose–Glycaemic Response Curve and a Definition of GE50
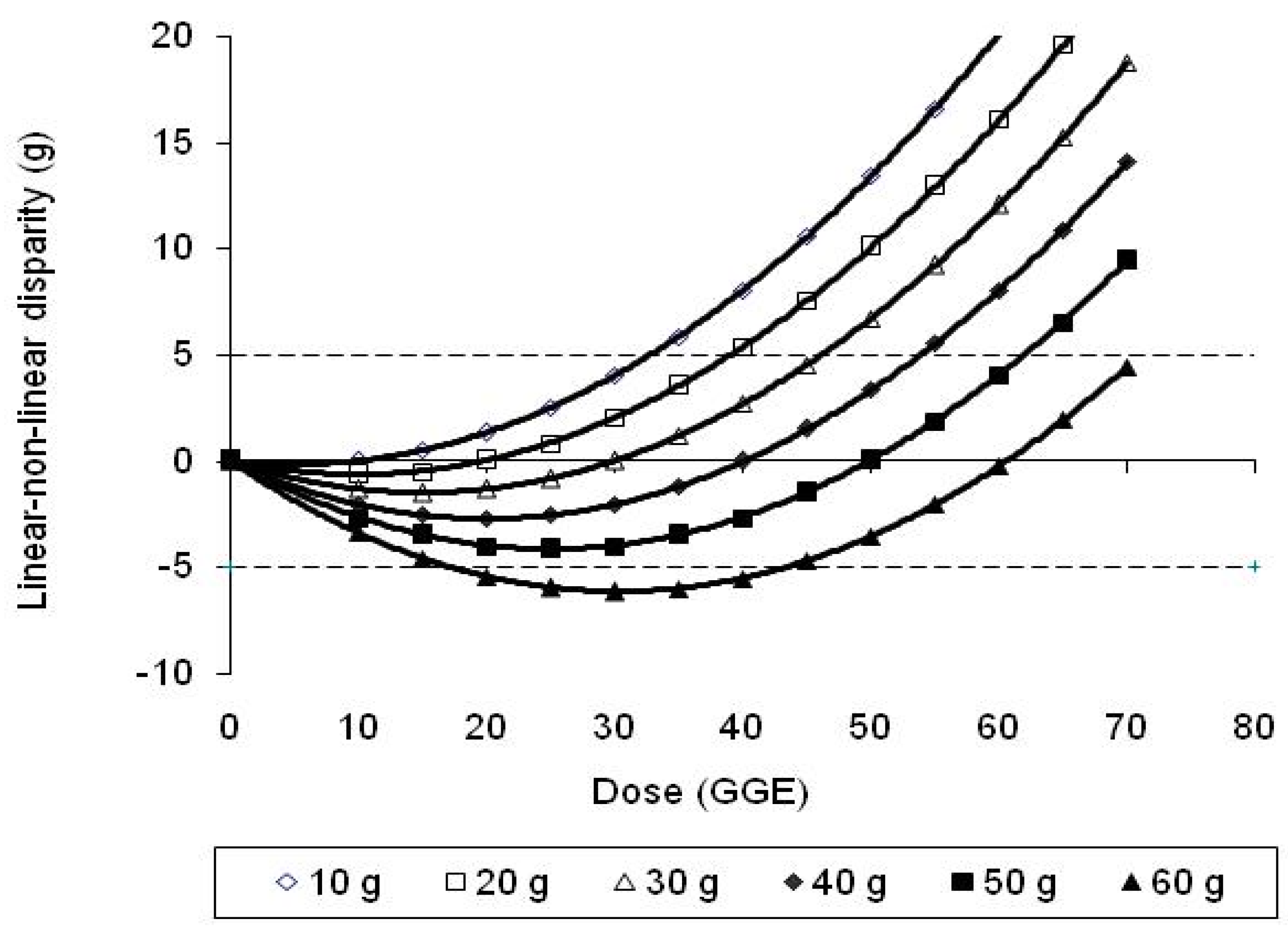
2.2. Linear Extrapolations from Different Reference Responses and Their Difference from Quadratic
2.3. Inaccuracy in Using Food GGEs Determined with a Single Reference to Obtain a Meal GGE
2.4. Validity of Equation (1) Tested against Clinical Data
2.5. A Criterion Tolerable Discrepancy between True GGE and Linear Estimates
2.6. Data Analysis
3. Results



4. Discussion


5. Conclusions
- The difference between the glycaemic impact of the meal and that of the glucose reference used to determine the GGE content of the food.
- The number of carbohydrate foods whose individual inaccuracies contribute to the total meal inaccuracy.
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Monro, J.A. Virtual food components: Functional food effects expressed as food components. Eur. J. Clin. Nutr. 2004, 58, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.L.; Murphy, S.P.; Au, D.L.M. Compiling glycemic index and glycemic load values for addition to a food composition database. J. Food Comp. Anal. 2008, 21, 469–473. [Google Scholar] [CrossRef]
- Schakel, S.; Schauer, R.; Himes, J.; Harnack, L.; Van Heel, N. Development of a glycemic index database for dietary assessment. J. Food Comp. Anal. 2008, 21, S50–S55. [Google Scholar] [CrossRef]
- Miller-Jones, J. Glycemic response definitions. Cereal Foods World 2007, 52, 54–55. [Google Scholar]
- Monro, J.A.; Shaw, M. Glycemic impact, glycemic glucose equivalents, glycemic index, and glycemic load: Definitions, distinctions and implications. Am. J. Clin. Nutr. 2008, 87, 237S–243S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallace, A.; Monro, J.; Brown, R.; Frampton, C. A glucose reference curve is the optimum method to determine the Glycemic Glucose Equivalent values of foods in humans. Nutr. Res. 2008, 28, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Venn, B.; Wallace, A.; Monro, J.; Perry, T.; Brown, R.; Frampton, C.; Green, T. Glycemic load estimated from glycaemic index does not differ greatly from glycemic load measured using a standard curve in healthy volunteers. J. Nutr. 2006, 136, 1377–1381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkins, D.; Wolever, T.; Taylor, R.; Barker, H.; Fielden, H.; Baldwin, J.; Bowling, A.; Newman, H.; Jenkins, A. Glycemic index of foods: A physiological basis for carbohydrate exchange. Am. J. Clin. Nutr. 1981, 34, 362–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gannon, M.; Nuttal, F.; Neil, B.; Westphal, S. The insulin and glucose responses to meals of glucose plus various proteins in Type II diabetic subjects. Metabolism 1988, 37, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- Wolever, T.M.S.; Katzmanrelle, L.; Jenkins, A.L.; Vuksan, V.; Josse, R.G.; Jenkins, D.J.A. Glycemic index of 102 complex carbohydrate foods in patients with diabetes. Nutr. Res. 1994, 14, 651–669. [Google Scholar] [CrossRef]
- Wolever, T.; Bolognesi, C. Source and amount of carbohydrate affect postprandial glucose and insulin in normal subjects. J. Nutr. 1996, 126, 2798–2806. [Google Scholar] [PubMed]
- Lee, B.; Wolever, T. Effect of glucose, sucrose and fructose on plasma glucose and insulin responses in normal humans: Comparison with white bread. Eur. J. Clin. Nutr. 1998, 52, 924–928. [Google Scholar] [CrossRef] [PubMed]
- Wallace, A.; Monro, J.; Hedderley, D.; Willis, J.; Scott, R. Determining the glycemic glucose equivalent value of foods in humans. Nutr. Res. 2006, 26, 47–52. [Google Scholar] [CrossRef]
- Tai, M.M. A mathematical-model for the determination of total area under glucose-tolerance and other metabolic curves. Diabetes Care 1994, 17, 152–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foster-Powell, K.; Holt, S.H.A.; Brand-Miller, J.C. International table of glycemic index and glycemic load values: 2002. Am. J. Clin. Nutr. 2002, 76, 5–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolever, T.; Yang, M.; Zeng, X.; Atkinson, F.; Brand-Miller, J. Food glycemic index, as given in Glycemic Index tables, is a significant determinant of glycemic response elicited by composite breakfast meals. Am. J. Clin. Nutr. 2006, 83, 1306–1312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guyton, A.; Hall, J. Textbook of Medical Physiology, 10th ed.; W.B. Saunders Company: New York, NY, USA, 2000. [Google Scholar]
- Vega-Lopez, S.; Griffith, J.; Ausman, L.; Lichtenstein, A. Interindividual variability and intraindividual reproducibility of glycemic index values for commercial white bread. Diabetes Care 2007, 30, 1412–1417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venn, B.J.; Green, T.J. Glycemic index and glycemic load: Measurement issues and their effect on diet-disease relationships. Eur. J. Clin. Nutr. 2007, 61, S122–S131. [Google Scholar] [CrossRef] [PubMed]
- Brouns, F.; Bjorck, I.; Frayn, K.; Gibbs, A.; Lang, V.; Slama, G.; Wolever, T. Glycaemic index methodology. Nutr. Res. Rev. 2005, 18, 145–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liljeberg, H.; Björk, I. Delayed gastric emptying rate may explain improved glycemia in healthy subjects to a starchy meal with added vinegar. Eur. J. Clin. Nutr. 1998, 52, 368–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Glucose Reference (g) | Linear Equations Linking Zero to Reference Response |
|---|---|
| 10 | y = 1.279x |
| 20 | y = 1.212x |
| 30 | y = 1.145x |
| 40 | y = 1.078x |
| 50 | y = 1.011x |
| 60 | y = 0.940x |
| Glucose Reference (g) | Equation of Disparity between Linear and True (Homeostasis-Adjusted) GGE |
|---|---|
| 10 | y = −0.0067x2 + 0.067x |
| 20 | y = −0.0067x2 + 0.134x |
| 30 | y = −0.0067x2 + 0.201x |
| 40 | y = −0.0067x2 + 0.268x |
| 50 | y = −0.0067x2 + 0.335x |
| 60 | y = −0.0067x2 + 0.4060x |
| Linear Estimates of GGE Using Equations in Table 1 | ||||||||
|---|---|---|---|---|---|---|---|---|
| Glucose Reference | ||||||||
| Diet | GL 1 | GGE50 2 | 10 | 20 | 30 | 40 | 50 | 60 |
| 1 | ||||||||
| 45 g fibre and fruit cereal | 20.80 | 25.1 | 26.6 | 25.2 | 23.8 | 22.4 | 21.0 | 19.6 |
| 120 mL 1.4%-fat milk | 1.90 | 2.5 | 2.4 | 2.3 | 2.2 | 2.0 | 1.9 | 1.8 |
| 80 g Rockmelon | 2.60 | 3.5 | 3.3 | 3.2 | 3.0 | 2.8 | 2.6 | 2.4 |
| 80 g Pineapple | 4.40 | 5.8 | 5.6 | 5.3 | 5.0 | 4.7 | 4.4 | 4.1 |
| A Sum of food values | 29.70 | 36.9 | 38.0 | 36.0 | 34.0 | 32.0 | 30.0 | 27.9 |
| B 3 Whole meal GGE | 34.07 | |||||||
| A-B (inaccuracy) | 2.8 | 3.9 | 1.9 | −0.1 | −2.1 | −4.0 | −6.2 | |
| 2 | ||||||||
| 45 g High-fibre cereal | 6.70 | 8.7 | 8.6 | 8.1 | 7.7 | 7.2 | 6.8 | 6.3 |
| 120 mL 1.4%-fat milk | 1.90 | 2.5 | 2.4 | 2.3 | 2.2 | 2.0 | 1.9 | 1.8 |
| 50 g Strawberries | 0.50 | 0.7 | 0.6 | 0.6 | 0.6 | 0.5 | 0.5 | 0.5 |
| 100 g Grapefruit | 2.30 | 3.1 | 2.9 | 2.8 | 2.6 | 2.5 | 2.3 | 2.2 |
| A Sum of food values | 11.40 | 15.0 | 14.6 | 13.8 | 13.1 | 12.3 | 11.5 | 10.7 |
| B Whole meal GGE | 14.47 | |||||||
| A-B (inaccuracy) | 0.5 | 0.1 | −0.7 | −1.4 | −2.2 | −2.9 | −3.8 | |
| 3 | ||||||||
| 80 g Egg omelette | 0.00 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| 40 g Wholemeal bread | 13.30 | 16.7 | 17.0 | 16.1 | 15.2 | 14.3 | 13.4 | 12.5 |
| 80 g Spinach | 0.20 | 0.3 | 0.3 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 |
| 20 g Red capsicum | 0.50 | 0.7 | 0.6 | 0.6 | 0.6 | 0.5 | 0.5 | 0.5 |
| 80 g Grilled tomato | 0.80 | 1.1 | 1.0 | 1.0 | 0.9 | 0.9 | 0.8 | 0.8 |
| A Sum of food values | 14.80 | 18.7 | 18.9 | 17.9 | 16.9 | 16.0 | 15.0 | 13.9 |
| B Whole meal GGE | 18.45 | |||||||
| A-B (inaccuracy) | 0.3 | 0.5 | −0.5 | −1.5 | −2.5 | −3.5 | −4.5 | |
| 4 | ||||||||
| 80 g Egg omelette | 0.00 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| 38 g Honey and oat-bran bread | 11.20 | 14.2 | 14.3 | 13.6 | 12.8 | 12.1 | 11.3 | 10.5 |
| 80 g Spinach | 0.20 | 0.3 | 0.3 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 |
| 20 g Red capsicum | 0.50 | 0.7 | 0.6 | 0.6 | 0.6 | 0.5 | 0.5 | 0.5 |
| 80 Grilled tomato | 0.80 | 1.1 | 1.0 | 1.0 | 0.9 | 0.9 | 0.8 | 0.8 |
| A Sum of food values | 12.70 | 16.2 | 16.2 | 15.4 | 14.5 | 13.7 | 12.8 | 11.9 |
| B Whole meal GGE | 16.01 | |||||||
| A-B (inaccuracy) | 0.2 | 0.2 | −0.6 | −1.5 | −2.3 | −3.2 | −4.1 | |
| 5 | ||||||||
| 15 g Whole-wheat cereal | 6.60 | 8.6 | 8.4 | 8.0 | 7.6 | 7.1 | 6.7 | 6.2 |
| 120 mL 1.4%-fat milk | 1.90 | 2.5 | 2.4 | 2.3 | 2.2 | 2.0 | 1.9 | 1.8 |
| 4 g Brown sugar | 1.90 | 2.5 | 2.4 | 2.3 | 2.2 | 2.0 | 1.9 | 1.8 |
| 90 g Banana | 9.40 | 12.1 | 12.0 | 11.4 | 10.8 | 10.1 | 9.5 | 8.8 |
| 100 mL Orange juice | 4.90 | 6.4 | 6.3 | 5.9 | 5.6 | 5.3 | 5.0 | 4.6 |
| A Sum of food values | 24.70 | 32.2 | 31.6 | 29.9 | 28.3 | 26.6 | 25.0 | 23.2 |
| B Whole meal GGE | 29.16 | |||||||
| A-B (inaccuracy) | 3.0 | 2.4 | 0.8 | −0.9 | −2.5 | −4.2 | −5.9 | |
| 6 | ||||||||
| 64 g Muffin | 19.60 | 23.8 | 25.1 | 23.8 | 22.4 | 21.1 | 19.8 | 18.4 |
| 14 g Peanut butter | 0.00 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| A Sum of food values | 19.60 | 23.8 | 25.1 | 23.8 | 22.4 | 21.1 | 19.8 | 18.4 |
| B Whole meal GGE | 23.81 | |||||||
| A-B (inaccuracy) | 0.0 | 1.3 | −0.1 | −1.4 | −2.7 | −4.0 | −5.4 | |
| 7 | ||||||||
| 30 g Corn flakes | 21.10 | 25.4 | 27.0 | 25.6 | 24.2 | 22.7 | 21.3 | 19.8 |
| 125 mL 2%-fat milk | 2.10 | 2.8 | 2.7 | 2.5 | 2.4 | 2.3 | 2.1 | 2.0 |
| 10 g Brown sugar | 4.80 | 6.3 | 6.1 | 5.8 | 5.5 | 5.2 | 4.9 | 4.5 |
| 50 g Whole-wheat bread | 15.40 | 19.1 | 19.7 | 18.7 | 17.6 | 16.6 | 15.6 | 14.5 |
| 10 g Margarine | 0.00 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| 125 mL Orange juice | 6.00 | 7.8 | 7.7 | 7.3 | 6.9 | 6.5 | 6.1 | 5.6 |
| A Sum of food values | 49.40 | 61.5 | 63.2 | 59.9 | 56.6 | 53.3 | 49.9 | 46.4 |
| B Whole meal GGE | 50.14 | |||||||
| A-B (inaccuracy) | 11.4 | 13.0 | 9.7 | 6.4 | 3.1 | −0.2 | −3.7 | |
| 8 | ||||||||
| 110 g Twelve-grain bagel | 39.60 | 42.8 | 50.6 | 48.0 | 45.3 | 42.7 | 40.0 | 37.2 |
| 30 g Cream cheese | 0.50 | 0.7 | 0.6 | 0.6 | 0.6 | 0.5 | 0.5 | 0.5 |
| 125 mL Orange juice | 6.00 | 7.8 | 7.7 | 7.3 | 6.9 | 6.5 | 6.1 | 5.6 |
| A Sum of food values | 46.10 | 51.3 | 59.0 | 55.9 | 52.8 | 49.7 | 46.6 | 43.3 |
| B Whole meal GGE | 47.81 | 51.42 | ||||||
| A-B (inaccuracy) | 3.5 | 11.2 | 8.1 | 5.0 | 1.9 | −1.2 | −4.5 | |
| 9 | ||||||||
| 50 g Whole-rye pumpernickel | 10.00 | 12.8 | 12.8 | 12.1 | 11.5 | 10.8 | 10.1 | 9.4 |
| 10 g Margarine | 0.00 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| 45 g Cracked wheat cereal | 16.20 | 20.0 | 20.7 | 19.6 | 18.5 | 17.5 | 16.4 | 15.2 |
| 10 g Brown sugar | 6.80 | 8.8 | 8.7 | 8.2 | 7.8 | 7.3 | 6.9 | 6.4 |
| 125 mL 2%-fat milk | 2.10 | 2.8 | 2.7 | 2.5 | 2.4 | 2.3 | 2.1 | 2.0 |
| 125 mL Orange juice | 6.00 | 7.8 | 7.7 | 7.3 | 6.9 | 6.5 | 6.1 | 5.6 |
| A Sum of food values | 41.10 | 52.3 | 52.6 | 49.8 | 47.1 | 44.3 | 41.6 | 38.6 |
| B Whole meal GGE | 44.00 | |||||||
| A-B (inaccuracy) | 8.3 | 8.6 | 5.8 | 3.1 | 0.3 | −2.4 | −5.4 | |
| 10 | ||||||||
| 30 g Whole-rye pumpernickel | 6.00 | 7.8 | 7.7 | 7.3 | 6.9 | 6.5 | 6.1 | 5.6 |
| 5 g Margarine | 0.00 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| 175 mL Strawberry yoghurt | 7.80 | 10.1 | 10.0 | 9.5 | 8.9 | 8.4 | 7.9 | 7.3 |
| 142 g Canned fruit | 10.40 | 13.3 | 13.3 | 12.6 | 11.9 | 11.2 | 10.5 | 9.8 |
| 125 mL Orange juice | 6.00 | 7.8 | 7.7 | 7.3 | 6.9 | 6.5 | 6.1 | 5.6 |
| A Sum of food values | 30.20 | 39.0 | 38.6 | 36.6 | 34.6 | 32.6 | 30.5 | 28.4 |
| B Whole meal GGE | 34.54 | |||||||
| A-B (inaccuracy) | 4.5 | 4.1 | 2.1 | 0.0 | −2.0 | −4.0 | −6.2 | |
| 11 | ||||||||
| 100 g Egg | 0.00 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| 75 g French fries | 10.90 | 13.9 | 13.9 | 13.2 | 12.5 | 11.8 | 11.0 | 10.2 |
| 25 g While-wheat bread | 7.70 | 10.0 | 9.8 | 9.3 | 8.8 | 8.3 | 7.8 | 7.2 |
| 5 g Margarine | 0.00 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| 125 mL Orange juice | 6.00 | 7.8 | 7.7 | 7.3 | 6.9 | 6.5 | 6.1 | 5.6 |
| A Sum of food values | 24.60 | 31.7 | 31.5 | 29.8 | 28.2 | 26.5 | 24.9 | 23.1 |
| B Whole meal GGE | 29.06 | |||||||
| A-B (inaccuracy) | 2.6 | 2.4 | 0.8 | −0.9 | −2.5 | −4.2 | −5.9 | |
| 12 | ||||||||
| 60 g Bran muffin | 15.20 | 18.9 | 19.4 | 18.4 | 17.4 | 16.4 | 15.4 | 14.3 |
| 10 g Margarine | 0.00 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| 125 mL Orange juice | 6.00 | 7.8 | 7.7 | 7.3 | 6.9 | 6.5 | 6.1 | 5.6 |
| A Sum of food values | 21.20 | 26.7 | 27.1 | 25.7 | 24.3 | 22.9 | 21.4 | 19.9 |
| B Whole meal GGE | 25.52 | |||||||
| A-B (inaccuracy) | 1.2 | 1.6 | 0.2 | −1.2 | −2.7 | −4.1 | −5.6 | |
| 13 | ||||||||
| 175 mL Strawberry yoghurt | 7.80 | 10.1 | 10.0 | 9.5 | 8.9 | 8.4 | 7.9 | 7.3 |
| 142 g Canned fruit | 10.40 | 13.3 | 13.3 | 12.6 | 11.9 | 11.2 | 10.5 | 9.8 |
| A Sum of food values | 18.20 | 23.4 | 23.3 | 22.1 | 20.8 | 19.6 | 18.4 | 17.1 |
| B Whole meal GE50 | 22.28 | |||||||
| A-B (inaccuracy) | 1.1 | 1.0 | −0.2 | −1.4 | −2.7 | −3.9 | −5.2 | |
| Linear Estimates of GGE Using Equations in Table 1 | ||||||||
|---|---|---|---|---|---|---|---|---|
| Glucose Reference | ||||||||
| Meal | GL 1 | GGE50 2 | 10 | 20 | 30 | 40 | 50 | 60 |
| 14 | ||||||||
| 2 slices white bread (54 g) | 20.00 | 24.2 | 25.6 | 24.2 | 22.9 | 21.6 | 20.2 | 18.8 |
| 2 tsp margarine (10 g) | 0.00 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| 1 tablesp honey (21 g) | 9.00 | 11.6 | 11.5 | 10.9 | 10.3 | 9.7 | 9.1 | 8.5 |
| 250 mL fruit drink (256 g) | 8.00 | 10.3 | 10.2 | 9.7 | 9.2 | 8.6 | 8.1 | 7.5 |
| A Sum of food values | 37.00 | 46.2 | 47.3 | 44.8 | 42.4 | 39.9 | 37.4 | 34.8 |
| B 3 Whole meal GGE | 40.63 | |||||||
| A-B (inaccuracy) | 5.5 | 6.7 | 4.2 | 1.7 | −0.7 | −3.2 | −5.9 | |
| 15 | ||||||||
| 1 cup instant noodles (180 g) | 14.00 | 17.5 | 17.9 | 17.0 | 16.0 | 15.1 | 14.2 | 13.2 |
| 1 apple (120 g) | 5.00 | 6.6 | 6.4 | 6.1 | 5.7 | 5.4 | 5.1 | 4.7 |
| 1 soft cereal bar (340 g) | 19.00 | 23.2 | 24.3 | 23.0 | 21.8 | 20.5 | 19.2 | 17.9 |
| A Sum of food values | 38.00 | 47.2 | 48.6 | 46.1 | 43.5 | 41.0 | 38.4 | 35.7 |
| B Whole meal GGE | 41.47 | |||||||
| A-B (inaccuracy) | 5.8 | 7.1 | 4.6 | 2.0 | −0.5 | −3.1 | −5.8 | |
| 16 | ||||||||
| 1 roast chicken thigh (119 g) | 0.00 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| 1 baked potato (90 g) | 14.00 | 17.5 | 17.9 | 17.0 | 16.0 | 15.1 | 14.2 | 13.2 |
| Portion roast pumpkin (150 g) | 6.00 | 7.8 | 7.7 | 7.3 | 6.9 | 6.5 | 6.1 | 5.6 |
| 1 med. portion sweet potato (70 g) | 6.00 | 7.8 | 7.7 | 7.3 | 6.9 | 6.5 | 6.1 | 5.6 |
| 1 corn on cob (100 g) | 14.00 | 17.5 | 17.9 | 17.0 | 16.0 | 15.1 | 14.2 | 13.2 |
| A Sum of food values | 40.00 | 50.7 | 51.2 | 48.5 | 45.8 | 43.1 | 40.4 | 37.6 |
| B Whole meal GGE | 43.12 | |||||||
| A-B (inaccuracy) | 7.6 | 8.0 | 5.4 | 2.7 | 0.0 | −2.7 | −5.5 | |
| 17 | ||||||||
| 2 sausages (142 g) | 2.00 | 2.7 | 2.6 | 2.4 | 2.3 | 2.2 | 2.0 | 1.9 |
| 1 cup mashed potato (180 g) | 22.00 | 26.4 | 28.1 | 26.7 | 25.2 | 23.7 | 22.2 | 20.7 |
| 1 cup green salad (105 g) | 0.00 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| 2 slices canned beetroot (80 g) | 4.00 | 5.3 | 5.1 | 4.8 | 4.6 | 4.3 | 4.0 | 3.8 |
| 1 cup canned peaches (208 g) | 9.00 | 11.6 | 11.5 | 10.9 | 10.3 | 9.7 | 9.1 | 8.5 |
| 0.5 cup custard (120 g) | 7.00 | 9.1 | 9.0 | 8.5 | 8.0 | 7.5 | 7.1 | 6.6 |
| A Sum of food values | 44.00 | 54.98 | 56.28 | 53.33 | 50.38 | 47.43 | 44.48 | 41.36 |
| B Whole meal GGE | 46.25 | |||||||
| A-B (inaccuracy) | 8.7 | 10.0 | 7.1 | 4.1 | 1.2 | −1.8 | −4.9 | |
| 18 | ||||||||
| 1 individual steak pie (172 g) | 12.00 | 15.2 | 15.3 | 14.5 | 13.7 | 12.9 | 12.1 | 11.3 |
| 1 cup fried potatoes (80 g) | 13.00 | 16.4 | 16.6 | 15.8 | 14.9 | 14.0 | 13.1 | 12.2 |
| 1 apple (120 g) | 5.00 | 6.6 | 6.4 | 6.1 | 5.7 | 5.4 | 5.1 | 4.7 |
| A Sum of food values | 30.00 | 38.12 | 38.37 | 36.36 | 34.35 | 32.34 | 30.33 | 28.20 |
| B Whole meal GGE | 34.35 | |||||||
| A-B (inaccuracy) | 3.77 | 4.02 | 2.01 | 0.00 | −2.01 | −4.02 | −6.15 | |
| 19 | ||||||||
| 1 filled bread roll (77 g) | 29.00 | 33.4 | 37.1 | 35.1 | 33.2 | 31.3 | 29.3 | 27.3 |
| 1 banana (120 g) | 16.00 | 19.8 | 20.5 | 19.4 | 18.3 | 17.2 | 16.2 | 15.0 |
| 1 can “Coca-cola” (365 g) | 23.00 | 27.4 | 29.4 | 27.9 | 26.3 | 24.8 | 23.3 | 21.6 |
| A Sum of food values | 68.00 | 80.6 | 87.0 | 82.4 | 77.9 | 73.3 | 68.7 | 63.9 |
| B Whole meal GGE | 60.55 | |||||||
| A-B (inaccuracy) | 20.1 | 26.4 | 21.9 | 17.3 | 12.8 | 8.2 | 3.4 | |
| 20 | ||||||||
| 2 medium potatoes (180 g) | 30.00 | 34.4 | 38.4 | 36.4 | 34.4 | 32.3 | 30.3 | 28.2 |
| 1 medium steak (145 g) | 0.00 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| 0.5 cups broccoli (82 g) | 1.00 | 1.3 | 1.3 | 1.2 | 1.1 | 1.1 | 1.0 | 0.9 |
| 0.5 cups pumpkin (110 g) | 4.00 | 5.3 | 5.1 | 4.8 | 4.6 | 4.3 | 4.0 | 3.8 |
| 0.5 cups carrot (800 g) | 2.00 | 2.7 | 2.6 | 2.4 | 2.3 | 2.2 | 2.0 | 1.9 |
| 1 cup ice cream (143 g) | 12.00 | 15.2 | 15.3 | 14.5 | 13.7 | 12.9 | 12.1 | 11.3 |
| 0.5 cups fruit salad (120 g) | 8.00 | 10.3 | 10.2 | 9.7 | 9.2 | 8.6 | 8.1 | 7.5 |
| A Sum of food values | 57.00 | 69.16 | 72.90 | 69.08 | 65.27 | 61.45 | 57.63 | 53.58 |
| B Whole meal GGE | 54.95 | |||||||
| A-B (inaccuracy) | 14.21 | 17.95 | 14.13 | 10.32 | 6.50 | 2.68 | −1.37 | |
| Total GGE Content of Meal | ||||||||
|---|---|---|---|---|---|---|---|---|
| Number of Foods | 20 g | 30 g | 40 g | 50 g | ||||
| GGE/Food | CI * | GGE/Food | CI | GGE/Food | CI | GGE/Food | CI | |
| 1 | 20 | 0.00 | 30 | 0.00 | 40 | 0.00 | 50 | 0.00 |
| 2 | 10 | −1.34 | 15 | −3.02 | 20 | −5.36 | 25 | −8.38 |
| 3 | 6.66 | −1.78 | 10 | −4.02 | 13.33 | −7.13 | 16.67 | −11.14 |
| 4 | 5.0 | −2.01 | 7.5 | −4.52 | 10 | −8.04 | 12.5 | −12.56 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monro, J. Accuracy in Determining the Glycaemic Impact of Meals by Adding Individual Food Values Is Affected by Food Number, Homeostasis and Glucose Reference Dose. Nutrients 2023, 15, 3296. https://doi.org/10.3390/nu15153296
Monro J. Accuracy in Determining the Glycaemic Impact of Meals by Adding Individual Food Values Is Affected by Food Number, Homeostasis and Glucose Reference Dose. Nutrients. 2023; 15(15):3296. https://doi.org/10.3390/nu15153296
Chicago/Turabian StyleMonro, John. 2023. "Accuracy in Determining the Glycaemic Impact of Meals by Adding Individual Food Values Is Affected by Food Number, Homeostasis and Glucose Reference Dose" Nutrients 15, no. 15: 3296. https://doi.org/10.3390/nu15153296
APA StyleMonro, J. (2023). Accuracy in Determining the Glycaemic Impact of Meals by Adding Individual Food Values Is Affected by Food Number, Homeostasis and Glucose Reference Dose. Nutrients, 15(15), 3296. https://doi.org/10.3390/nu15153296