
Perfectionism or Perfectionisms in Orthorexia Nervosa


Abstract
:1. Introduction
- (a)
- Individuals with high orthorexic characteristics could show more perfectionism than individuals with low orthorexic characteristics. In particular, orthorexic dieters could score higher on perfectionism scales than dieters without orthorexic features.
- (b)
- Dieters with high orthorexic features could score higher on perfectionism scales than non-dieters with orthorexic features.
2. Methods
2.1. Participants
2.2. Measures
- −
- Eating Habits Questionnaire (EHQ-21) [34], Italian version by [35]: a 21-item questionnaire to evaluate orthorexia nervosa on a four-point Likert scale divided into three scales: “Knowledge”, “Problems”, and “Feelings”. Psychometric properties (internal consistency and test–retest reliability) were good in the original and the Italian validation of the instrument. For the current study, Cronbach’s α displayed an excellent internal consistency for the total score (Cronbach’s α = 0.91) and the three scales.
- −
- Multidimensional Perfectionism Scale (MPS) [20,36], Italian version by [37]: a 35-item questionnaire to assess perfectionism on a five-point Likert scale. The authors identified the dimension of positive strivings of perfectionism, with higher levels of planning and lower procrastination (expressed by the “Personal Standards” scale), and negative perfectionism, characterised by maladaptive concerns about actions (“Concern over Mistakes” and “Doubting of Actions” scales). The original and the Italian psychometric properties were good and, in the current study, internal consistency was good both for MPS Striving (Cronbach’s α = 0.86) and MPS Concerns (Cronbach’s α = 0.93).
- −
- Eating Disorder Inventory-3 (EDI-3) [21], Italian version by [22]: a 91-item questionnaire used to assess symptoms and features of eating disorders and scored on a six-point Likert scale. The questionnaire is composed of twelve scales measuring eating disorder symptoms and general psychological features related to the development of EDs (which included “Perfectionism”). In both the original and Italian validation internal consistency and test-retest reliability were good. For the current study, “EDI-Perfectionism” showed good internal consistency (Cronbach’s α = 0.70), as did other subscales.
- −
- Obsessive Beliefs Questionnaire (OBQ-46) [23,24], Italian version by [38,39]: a 46-item questionnaire that uses a seven-point Likert scale used to evaluate cognitive domains related to the development and maintenance of obsessive–compulsive disorder. It is composed of five subscales in which is included “Perfectionism”, a measure of the need to do things perfectly, and the perceived sense of failure when certain personal standards are not met. Psychometric properties (internal consistency, test-retest reliability, and convergent/discriminant validity) were good both in the original and Italian validation. This study showed excellent internal consistency for the “OBQ-Perfectionism” scale (Cronbach’s α = 0.92) and other dimensions.
2.3. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics
3.2. Perfectionism and Orthorexia Nervosa
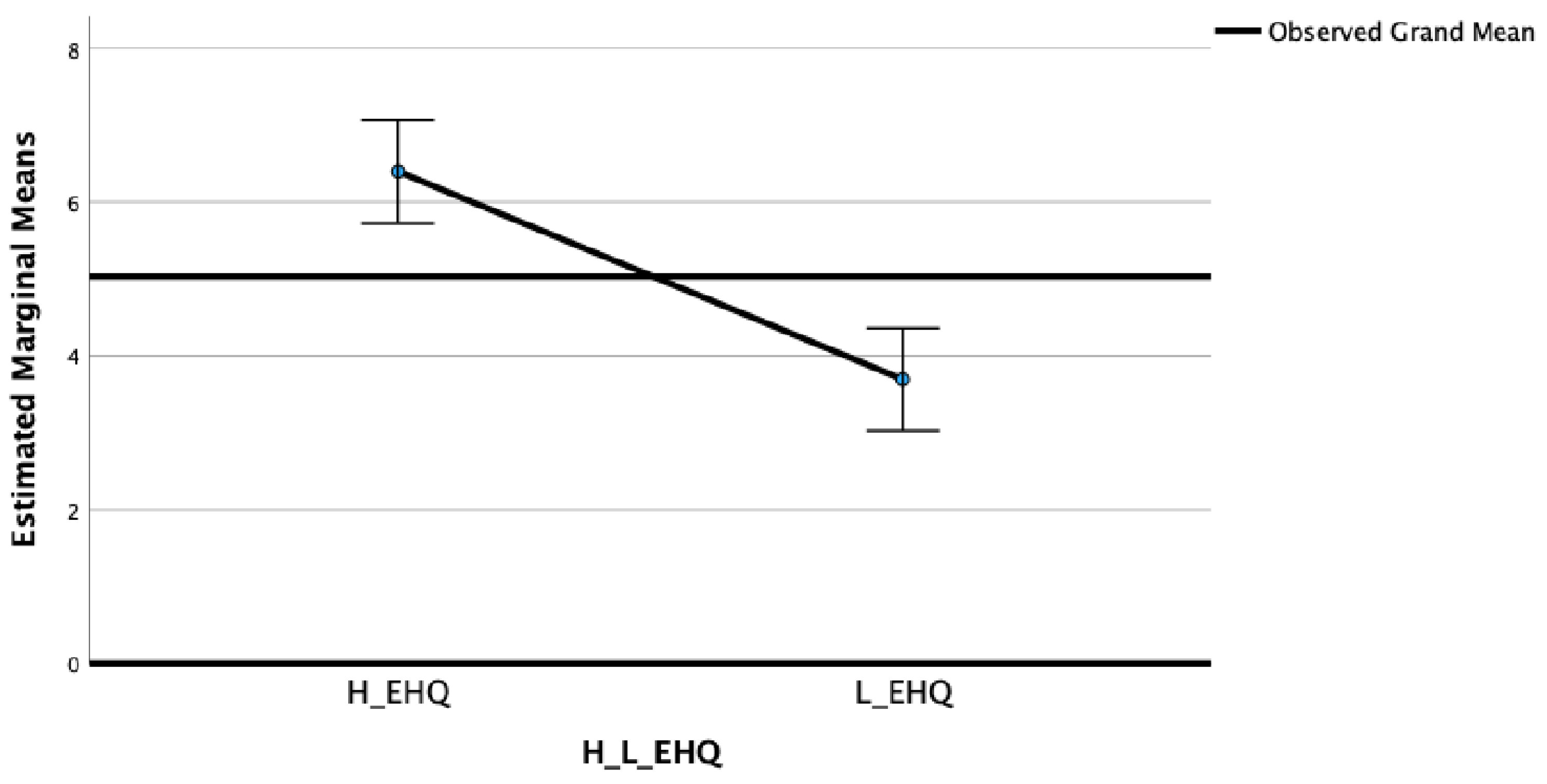
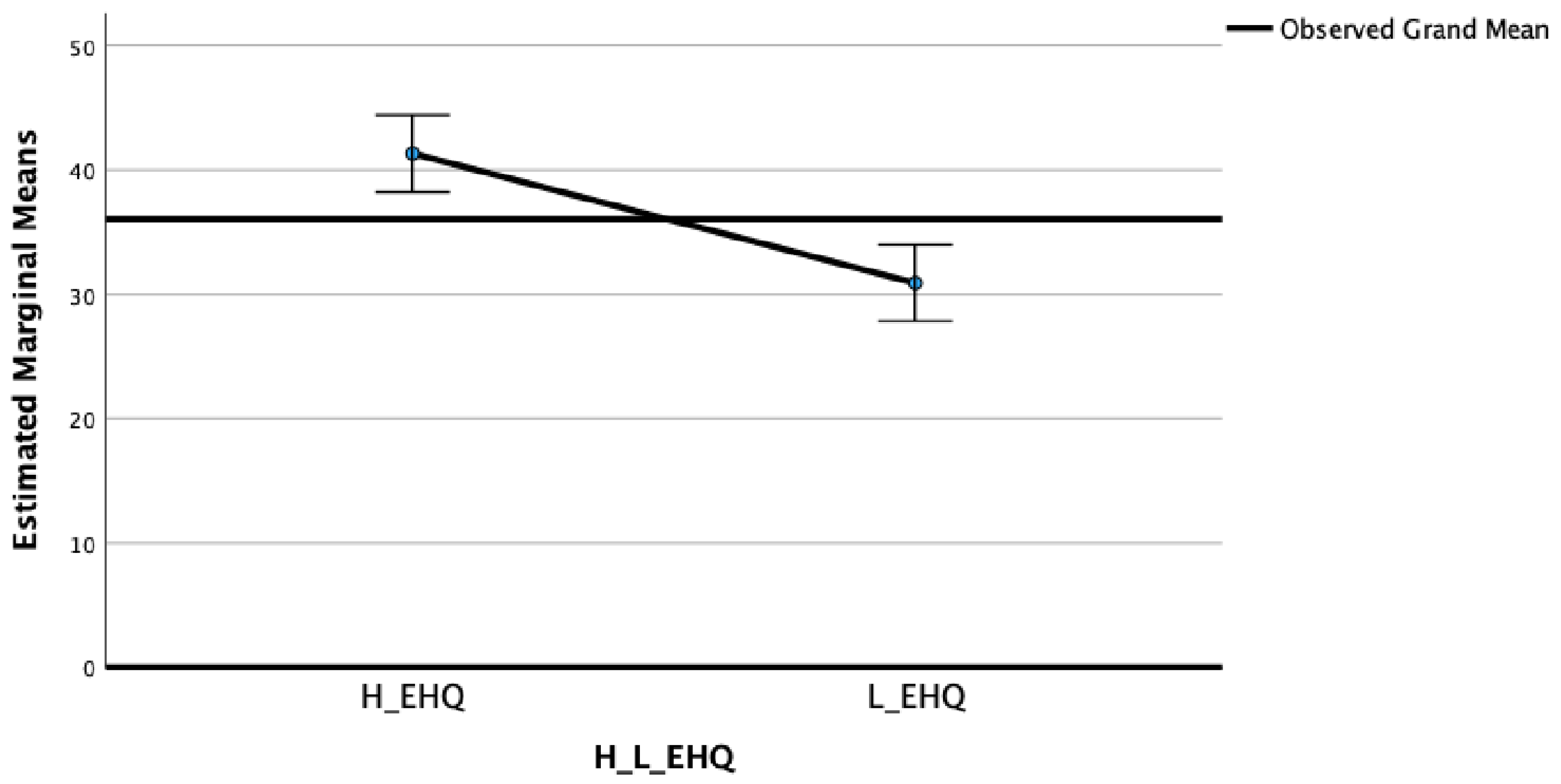
3.3. Differences between High and Low EHQ in Perfectionist Traits
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bratman, S.; Knight, D. Orthorexia Nervosa: Overcoming the Obsession with Healthful Eating. Health Food Junkies; Broadway Books: New York, NY, USA, 2000. [Google Scholar]
- Varga, M.; Dukay-Szabó, S.; Túry, F.; van Furth Eric, F. Evidence and gaps in the literature on orthorexia nervosa. Eat. Weight Disord.—Stud. Anorex. Bulim. Obes. 2013, 18, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Moroze, R.M.; Dunn, T.M.; Holland, J.C.; Yager, J.; Weintraub, P. Microthinking About Micronutrients: A Case of Transition From Obsessions about Healthy Eating to Near-Fatal “Orthorexia Nervosa” and Proposed Diagnostic Criteria. Psychosomatics 2015, 56, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Segura-Garcia, C.; Ramacciotti, C.; Rania, M.; Aloi, M.; Caroleo, M.; Bruni, A.; Gazzarrini, D.; Sinopoli, F.; De Fazio, P. The prevalence of orthorexia nervosa among eating disorder patients after treatment. Eat. Weight. Disord.—Stud. Anorex. Bulim. Obes. 2015, 20, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Gramaglia, C.; Brytek-Matera, A.; Rogoza, R.; Zeppegno, P. Orthorexia and anorexia nervosa: Two distinct phenomena? A cross-cultural comparison of orthorexic behaviours in clinical and non-clinical samples. BMC Psychiatry 2017, 17, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parra-Fernández, M.-L.; Rodríguez-Cano, T.; Onieva-Zafra, M.-D.; Perez-Haro, M.J.; Casero-Alonso, V.; Martínez, E.F.; Notario-Pacheco, B. Prevalence of orthorexia nervosa in university students and its relationship with psychopathological aspects of eating behaviour disorders. BMC Psychiatry 2018, 18, 364. [Google Scholar] [CrossRef]
- Poyraz, C.; Tufekcioglu, E.; Ozdemir, A.; Bas, A.; Kani, A.; Erginoz, E.; Duran, A. Relationship between orthorexia and obsessive-compulsive symptoms in patients with generalised anxiety disorder, panic disorder and obsessive compulsive disorder. Yeni Symp. 2015, 53, 22. [Google Scholar] [CrossRef] [Green Version]
- Vaccari, G.; Cutino, A.; Luisi, F.; Giambalvo, N.; Daneshmand, S.N.; Pinelli, M.; Maina, G.; Galeazzi, G.M.; Kaleci, S.; Albert, U.; et al. Is orthorexia nervosa a feature of obsessive–compulsive disorder? A multicentric, controlled study. Eat. Weight. Disord.—Stud. Anorex. Bulim. Obes. 2021, 26, 2531–2544. [Google Scholar] [CrossRef]
- Novara, C.; Pardini, S.; Maggio, E.; Mattioli, S.; Piasentin, S. Orthorexia Nervosa: Over concern or obsession about healthy food? Eat. Weight. Disord.—Stud. Anorex. Bulim. Obes. 2021, 26, 2577–2588. [Google Scholar] [CrossRef]
- Ma, A.Z.; Vacca, M.; Cerolini, S.; Ballesio, A.; Lombardo, C. Associations between orthorexia, disordered eating, and obsessive–compulsive symptoms: A systematic review and meta-analysis. Int. J. Eat. Disord. 2022, 55, 295–312. [Google Scholar] [CrossRef]
- Novara, C.; Mattioli, S.; Piasentin, S.; Pardini, S.; Maggio, E. The role of dieting, psychopathological characteristics and maladaptive personality traits in Orthorexia Nervosa. BMC Psychiatry 2022, 22, 290. [Google Scholar] [CrossRef]
- Koven, N.; Abry, A. The clinical basis of orthorexia nervosa: Emerging perspectives. Neuropsychiatr. Dis. Treat. 2015, 11, 385–394. [Google Scholar] [CrossRef] [Green Version]
- Barnes, M.A.; Caltabiano, M.L. The interrelationship between orthorexia nervosa, perfectionism, body image and attachment style. Eat. Weight. Disord.—Stud. Anorex. Bulim. Obes. 2017, 22, 177–184. [Google Scholar] [CrossRef]
- Oberle, C.D.; Samaghabadi, R.O.; Hughes, E.M. Orthorexia nervosa: Assessment and correlates with gender, BMI, and personality. Appetite 2017, 108, 303–310. [Google Scholar] [CrossRef]
- Novara, C.; Maggio, E.; Piasentin, S.; Pardini, S.; Mattioli, S. Orthorexia Nervosa: Differences between clinical and non-clinical samples. BMC Psychiatry 2021, 21, 341. [Google Scholar] [CrossRef]
- Fairburn, C.G.; Cooper, Z.; Shafran, R. Cognitive behaviour therapy for eating disorders: A “transdiagnostic” theory and treatment. Behav. Res. Ther. 2003, 41, 509–528. [Google Scholar] [CrossRef]
- Frost, R.O.; Steketee, G. Perfectionism in Obsessive-Compulsive Disorder patients. Behav. Res. Ther. 1997, 35, 291–296. [Google Scholar] [CrossRef]
- Pinto, A.; Dargani, N.; Wheaton, M.G.; Cervoni, C.; Rees, C.S.; Egan, S.J. Perfectionism in obsessive-compulsive disorder and related disorders: What should treating clinicians know? J. Obs.-Compuls. Relat. Disord. 2017, 12, 102–108. [Google Scholar] [CrossRef]
- Dunn, T.M.; Bratman, S. On orthorexia nervosa: A review of the literature and proposed diagnostic criteria. Eat. Behav. 2016, 21, 11–17. [Google Scholar] [CrossRef]
- Frost, R.O.; Marten, P.; Lahart, C.; Rosenblate, R. The dimensions of perfectionism. Cogn. Ther. Res. 1990, 14, 449–468. [Google Scholar] [CrossRef]
- Garner, D.M. Eating Disorder Inventory-3 (EDI-3): Professional Manual; Psychological Assessment Resourches: Odessa, Ukraine, 2004. [Google Scholar]
- Giannini, M.; Pannocchia, L.; Dalle Grave, R.; Muratori, F.; Viglione, V. Eating Disorder Inventory-3; Giunti OS: Firenze, Italy, 2008. [Google Scholar]
- Steketee, G.; Frost, R.O.; Bhar, S.S.; Bouvard, M.; Calamari, J.E.; Carmin, C.N.; Clark, D.A.; Cottraux, J.; Emmelkamp, P.M.G.; Forrester, E.; et al. Psychometric validation of the Obsessive Beliefs Questionnaire and the Interpretation of Intrusions Inventory: Part I. Behav. Res. Ther. 2003, 41, 863–878. [Google Scholar] [CrossRef]
- Obsessive Compulsive Cognitions Working Group. Psychometric validation of the obsessive belief questionnaire and interpretation of intrusions inventory—Part 2: Factor analyses and testing of a brief version. Behav. Res. Ther. 2005, 43, 1527–1542. [Google Scholar] [CrossRef] [PubMed]
- Stoeber, J.; Otto, K. Positive Conceptions of Perfectionism: Approaches, Evidence, Challenges. Pers. Soc. Psychol. Rev. 2006, 10, 295–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoeber, J.; Madigan, D.J.; Gonidis, L. Perfectionism is adaptive and maladaptive, but what's the combined effect? Pers. Individ. Differ. 2020, 161, 109846. [Google Scholar] [CrossRef]
- Bills, E.; Greene, D.; Stackpole, R.; Egan, S.J. Perfectionism and eating disorders in children and adolescents: A systematic review and meta-analysis. Appetite 2023, 187, 106586. [Google Scholar] [CrossRef]
- Limburg, K.; Watson, H.J.; Hagger, M.S.; Egan, S.J. The Relationship Between Perfectionism and Psychopathology: A Meta-Analysis. J. Clin. Psychol. 2017, 73, 1301–1326. [Google Scholar] [CrossRef] [Green Version]
- Vicent, M.; Gonzálvez, C.; Quiles, M.J.; Sánchez-Meca, J. Perfectionism and binge eating association: A systematic review and meta-analysis. J. Eat. Disord. 2023, 11, 101. [Google Scholar] [CrossRef]
- Barrada, J.R.; Roncero, M. Bidimensional Structure of the Orthorexia: Development and Initial Validation of a New Instrument. An. Psicol. 2018, 34, 283–291. [Google Scholar] [CrossRef]
- Yung, J.J.; Tabri, N. The association of perfectionism, health-focused self-concept, and erroneous beliefs with orthorexia nervosa symptoms: A moderated mediation model. Int. J. Eat. Disord. 2022, 55, 892–901. [Google Scholar] [CrossRef]
- Czepiel, D.; Koopman, H.M. Does physical appearance perfectionism predict disordered dieting? Curr. Psychol. A J. Divers. Perspect. Divers. Psychol. Issues 2021, 42, 24–34. [Google Scholar] [CrossRef]
- Stoeber, J.; Yang, H. Physical appearance perfectionism explains variance in eating disorder symptoms above general perfectionism. Pers. Individ. Differ. 2015, 86, 303–307. [Google Scholar] [CrossRef]
- Gleaves, D.H.; Graham, E.C.; Ambwani, S. Measuring «orthorexia»: Development of the Eating Habits Questionnaire. Int. J. Educ. Psychol. Assess. 2013, 12, 1–18. [Google Scholar]
- Novara, C.; Pardini, S.; Pastore, M.; Mulatti, C. Ortoressia Nervosa: Un’indagine del costrutto e delle caratteristiche psicometriche della versione italiana dell’Eating Habits Questionnaire-21 (EHQ-21). Psicoter. Cogn. E Comport. 2017, 23, 291–316. [Google Scholar]
- Stöber, J. The Frost Multidimensional Perfectionism Scale revisited: More perfect with four (instead of six) dimensions. Pers. Individ. Differ. 1998, 24, 481–491. [Google Scholar] [CrossRef] [Green Version]
- Lombardo, C. Adattamento italiano della multidimensional perfectionism scale (MPS). Psicoter. Cogn. E Comport. 2008, 14, 31–46. [Google Scholar]
- Dorz, S.; Novara, C.; Pastore, M.; Sica, C.; Sanavio, E. Presentazione della versione italiana dell’Obsessive Beliefs Questionnaire (OBQ): Struttura fattoriale e analisi di attendibilità (parte I). Psicoter. Cogn. E Comport. 2009, 15, 139–170. [Google Scholar]
- Novara, C.; Dorz, S.; Pastore, M.; Sica, C.; Sanavio, E. Presentazione della versione italiana dell’Obsessive Beliefs Questionnaire (parte II). Validità convergente e specificità dei costrutti in un campione clinico. Psicoter. Cogn. E Comport. 2011, 17, 157–172. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows, Version 29.0.; Released 2022; IBM Corp: Armonk, NY, USA, 2022. [Google Scholar]
- Korinth, A.; Schiess, S.; Westenhoefer, J. Eating behaviour and eating disorders in students of nutrition sciences. Public Health Nutr. 2009, 13, 32–37. [Google Scholar] [CrossRef] [Green Version]
- Fidan, T.; Ertekin, V.; Işikay, S.; Kırpınar, I. Prevalence of orthorexia among medical students in Erzurum, Turkey. Compr. Psychiatry 2010, 51, 49–54. [Google Scholar] [CrossRef]
- Agopyan, A.; Kenger, E.B.; Kermen, S.; Ulker, M.T.; Uzsoy, M.A.; Yetgin, M.K. The relationship between orthorexia nervosa and body composition in female students of the nutrition and dietetics department. Eat. Weight. Disord.—Stud. Anorex. Bulim. Obes. 2019, 24, 257–266. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group Type | N (%) or M (SD) | Pearson Chi-Square or F | p | Partial η2 | |
|---|---|---|---|---|---|
| BMI | Diet | 24.65 (5.42) | 18.49 | <0.001 | 0.10 |
| No Diet | 21.84 (3.38) | ||||
| Gender (% female) | Diet | 50 (53.8%) | 4.67 | <0.01 | 0.16 |
| No Diet | 65 (69.1%) | ||||
| Marital status (% single or fiancé) | Diet | 24 (25.8%) | 92.95 | <0.001 | 0.71 |
| No Diet | 89 (94.7%) | ||||
| Employment (% full time) | Diet | 48 (51.6%) | 149.89 | <0.001 | 0.90 |
| No Diet | 2 (2.1%) | ||||
| Employment (% student) | Diet | 7 (7.5%) | |||
| No Diet | 91 (96.8%) | ||||
| Age | Diet | 45.56 (12.85) | 297.82 | <0.001 | 0.30 |
| No Diet | 22.60 (3.27) | ||||
| Years of school attendance | Diet | 14.34 (3.35) | 19.86 | <0.001 | 0.07 |
| No Diet | 16.09 (1.55) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Novara, C.; Piasentin, S.; Mattioli, S.; Pardini, S.; Maggio, E. Perfectionism or Perfectionisms in Orthorexia Nervosa. Nutrients 2023, 15, 3289. https://doi.org/10.3390/nu15153289
Novara C, Piasentin S, Mattioli S, Pardini S, Maggio E. Perfectionism or Perfectionisms in Orthorexia Nervosa. Nutrients. 2023; 15(15):3289. https://doi.org/10.3390/nu15153289
Chicago/Turabian StyleNovara, Caterina, Sara Piasentin, Sofia Mattioli, Susanna Pardini, and Eleonora Maggio. 2023. "Perfectionism or Perfectionisms in Orthorexia Nervosa" Nutrients 15, no. 15: 3289. https://doi.org/10.3390/nu15153289
APA StyleNovara, C., Piasentin, S., Mattioli, S., Pardini, S., & Maggio, E. (2023). Perfectionism or Perfectionisms in Orthorexia Nervosa. Nutrients, 15(15), 3289. https://doi.org/10.3390/nu15153289