
Predictive Value of Malnutrition, Identified via Different Nutritional Screening or Assessment Tools, for Functional Outcomes in Patients with Stroke: A Systematic Review and Meta-Analysis

 ,
,
Abstract
1. Introduction
2. Material and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Data Extraction
2.5. Risk of Bias Assessment
2.6. Data Synthesis
3. Results
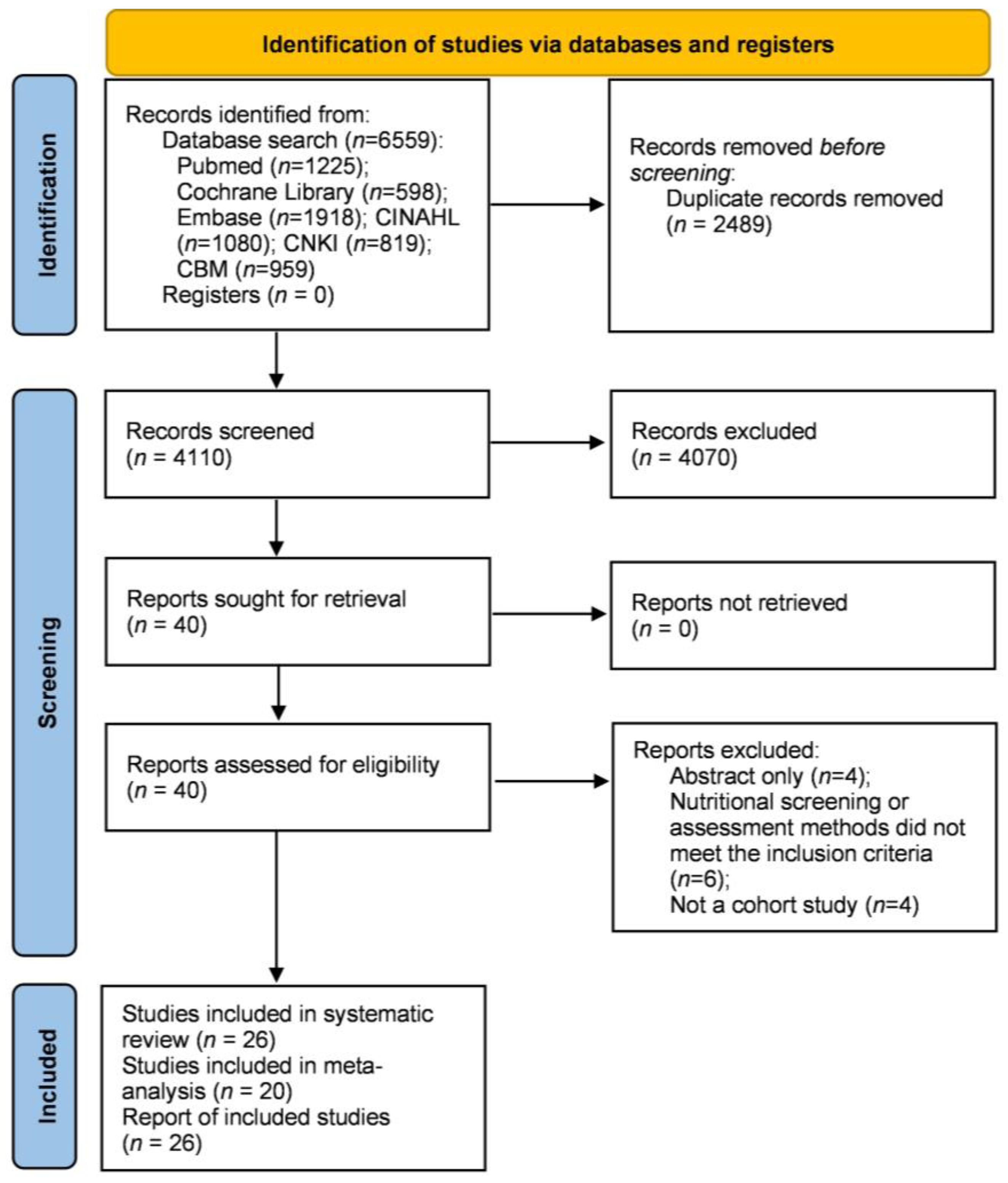
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias
3.4. Nutritional Screening and Assessment Method
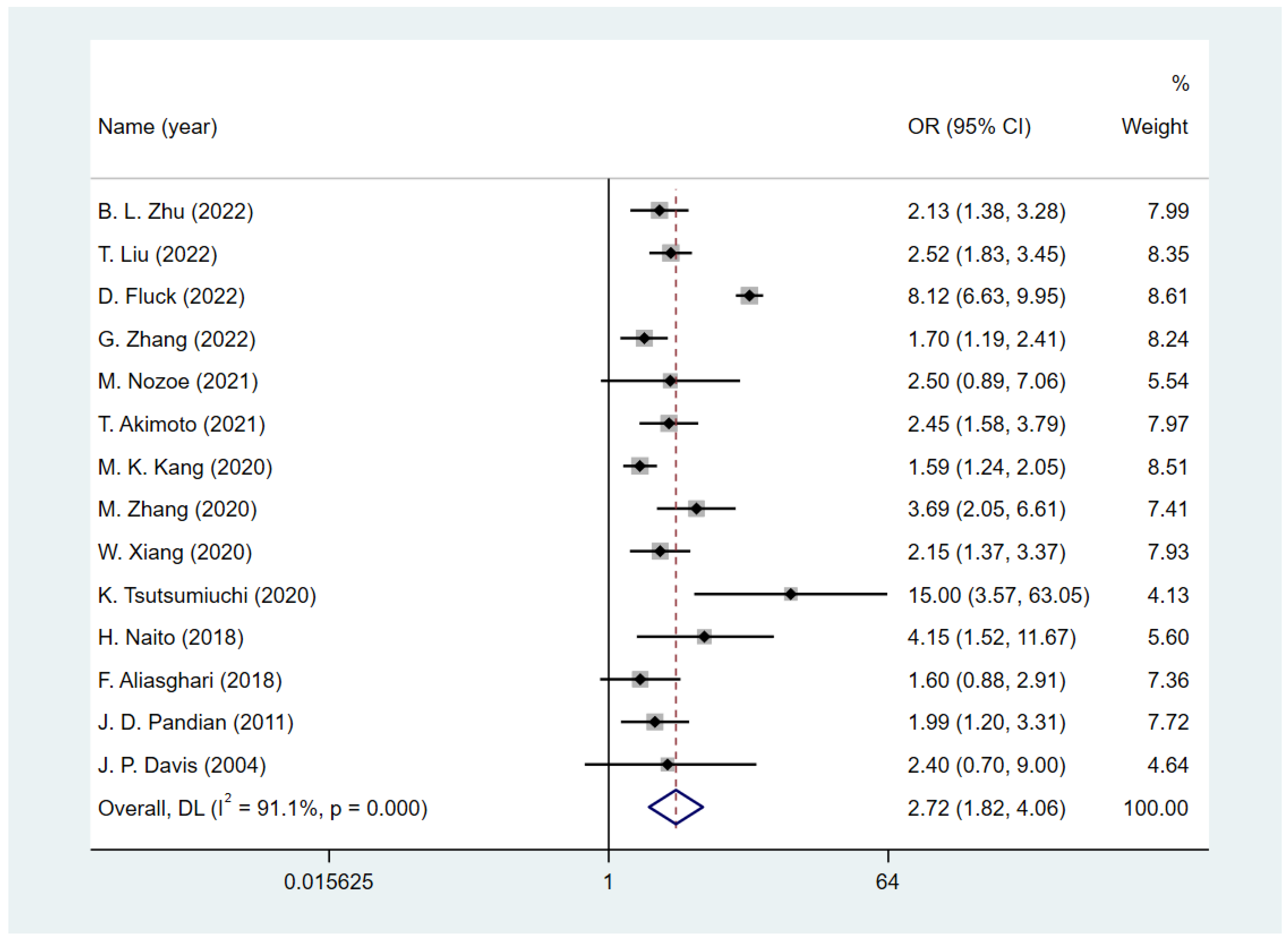
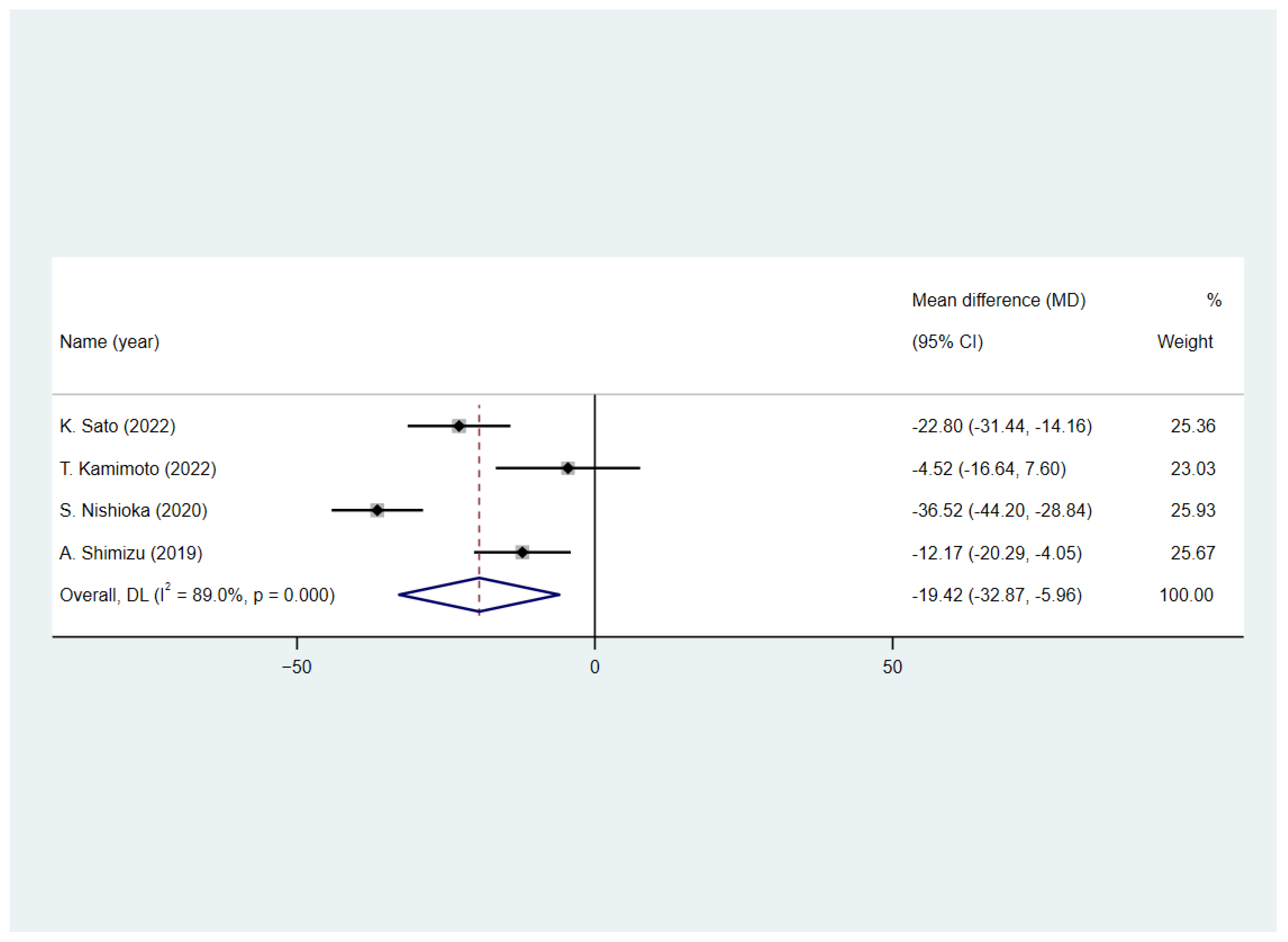
3.5. Predictive Value of Malnutrition on Function Status after Stroke
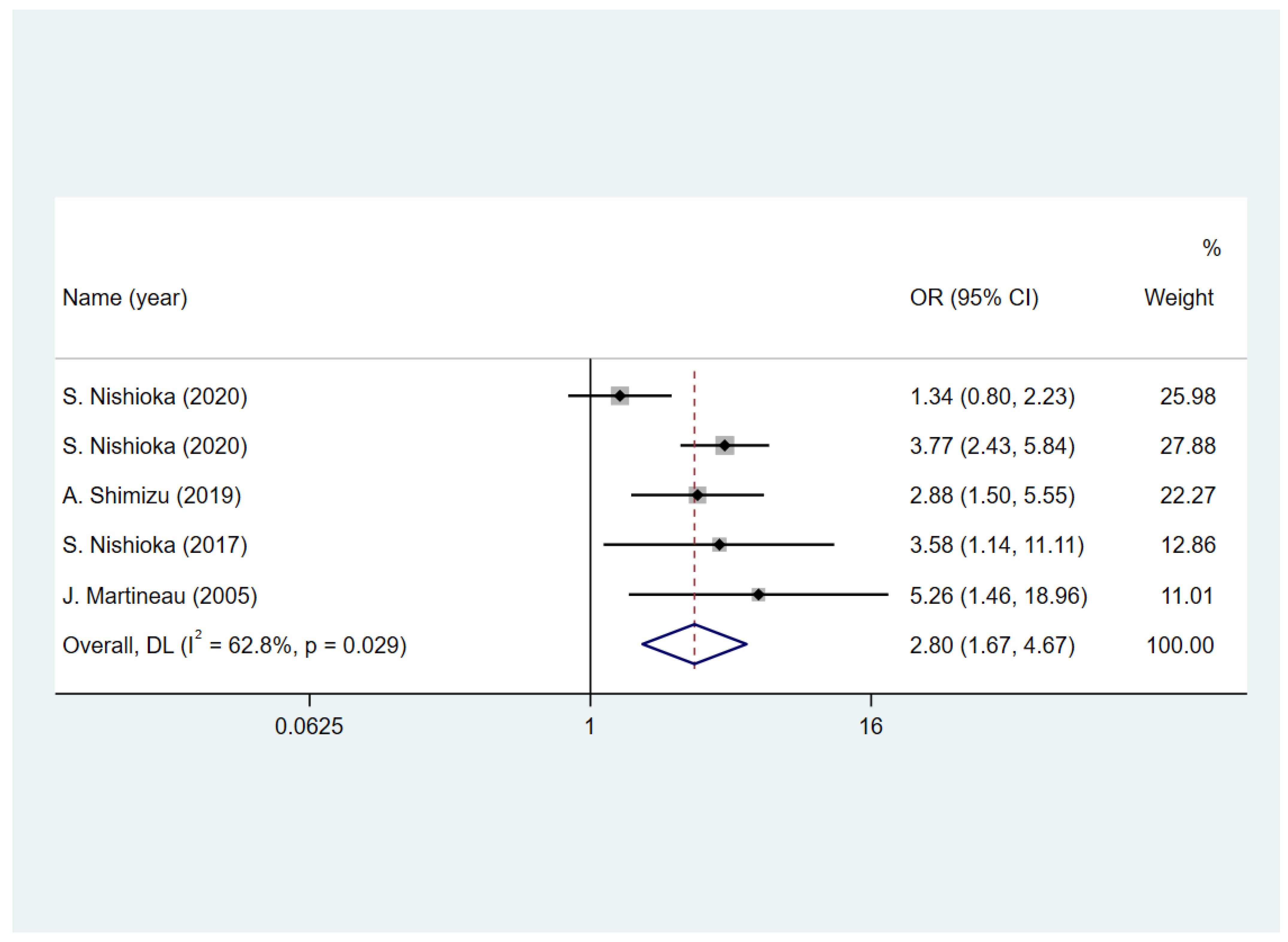
3.6. Predictive Value of Malnutrition on Dysphagia
3.7. Predictive Value of Malnutrition on Quality of Life
3.8. Sensitivity and Subgroup Analyses
3.9. Publication Bias
4. Discussion
4.1. Summary and Interpretation
4.2. Strengths
4.3. Limitations
4.4. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Barker, L.; Gout, B.; Crowe, T. Hospital Malnutrition: Prevalence, Identification and Impact on Patients and the Healthcare System. Int. J. Environ. Res. Public Health 2011, 8, 514–527. [Google Scholar] [CrossRef] [PubMed]
- Huppertz, V.; Guida, S.; Holdoway, A.; Strilciuc, S.; Baijens, L.; Schols, J.M.G.A.; van Helvoort, A.; Lansink, M.; Muresanu, D.F. Impaired Nutritional Condition after Stroke from the Hyperacute to the Chronic Phase: A Systematic Review and Meta-Analysis. Front. Neurol. 2021, 12, 780080. [Google Scholar] [CrossRef]
- Gomes, F.; Emery, P.W.; Weekes, C.E. Risk of Malnutrition Is an Independent Predictor of Mortality, Length of Hospital Stay, and Hospitalization Costs in Stroke Patients. J. Stroke Cerebrovasc. Dis. 2016, 25, 799–806. [Google Scholar] [CrossRef]
- Dávalos, A.; Ricart, W.; Gonzalez-Huix, F.; Soler, S.; Marrugat, J.; Molins, A.; Suñer, R.; Genís, D. Effect of malnutrition after acute stroke on clinical outcome. Stroke 1996, 27, 1028–1032. [Google Scholar] [CrossRef]
- Martineau, J.; Bauer, J.D.; Isenring, E.; Cohen, S. Malnutrition determined by the patient-generated subjective global assessment is associated with poor outcomes in acute stroke patients. Clin. Nutr. 2005, 24, 1073–1077. [Google Scholar] [CrossRef] [PubMed]
- van Wijk, N.; Studer, B.; van den Berg, C.A.; Ripken, D.; Lansink, M.; Siebler, M.; Schmidt-Wilcke, T. Evident lower blood levels of multiple nutritional compounds and highly prevalent malnutrition in sub-acute stroke patients with or without dysphagia. Front. Neurol. 2022, 13, 1028991. [Google Scholar] [CrossRef]
- Cederholm, T.; Jensen, G.L.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.J.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef]
- Mehta, A.; De Paola, L.; A Pana, T.; Carter, B.; Soiza, R.L.; Kafri, M.W.; Potter, J.F.; A Mamas, M.; Myint, P.K. The relationship between nutritional status at the time of stroke on adverse outcomes: A systematic review and meta-analysis of prospective cohort studies. Nutr. Rev. 2022, 80, 2275–2287. [Google Scholar] [CrossRef]
- Haider, M.; Haider, S.Q. Assessment of protein-calorie malnutrition. Clin. Chem. 1984, 30, 1286–1299. [Google Scholar] [CrossRef]
- Ng, W.; Collins, P.; Hickling, D.; Bell, J. Evaluating the concurrent validity of body mass index (BMI) in the identification of malnutrition in older hospital inpatients. Clin. Nutr. 2019, 38, 2417–2422. [Google Scholar] [CrossRef]
- Schuetz, P.; Seres, D.; Lobo, D.N.; Gomes, F.; Kaegi-Braun, N.; Stanga, Z. Management of disease-related malnutrition for patients being treated in hospital. Lancet 2021, 398, 1927–1938. [Google Scholar] [CrossRef]
- Burgos, R.; Bretón, I.; Cereda, E.; Desport, J.C.; Dziewas, R.; Genton, L.; Gomes, F.; Jésus, P.; Leischker, A.; Muscaritoli, M.; et al. ESPEN guideline clinical nutrition in neurology. Clin. Nutr. 2018, 37, 354–396. [Google Scholar] [CrossRef]
- Foley, N.C.; Salter, K.L.; Robertson, J.; Teasell, R.W.; Woodbury, M.G.; Martino, R.; Bhogal, S.; Diamant, N.; Speechley, M.; Dávalos, A.; et al. Which reported estimate of the prevalence of malnutrition after stroke is valid? Stroke 2009, 40, e66–e74. [Google Scholar] [CrossRef]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef]
- Hu, J.; Chen, T.; Wang, Z.; Chen, X.; Lin, K.; Zhang, G.; Wu, J. Geriatric Nutritional Risk Index and the Prognosis of Patients with Stroke: A Meta-Analysis. Horm. Metab. Res. 2022, 54, 736–746. [Google Scholar] [CrossRef]
- Sato, Y.; Yoshimura, Y.; Abe, T.; Nagano, F.; Matsumoto, A.; Kokura, Y.; Momosaki, R. Combination of High Energy Intake and Intensive Rehabilitation Is Associated with the Most Favorable Func-tional Recovery in Acute Stroke Patients with Sarcopenia. Nutrients 2022, 14, 4740. [Google Scholar] [CrossRef]
- Rabadi, M.H.; Coar, P.L.; Lukin, M.; Lesser, M.; Blass, J.P. Intensive nutritional supplements can improve outcomes in stroke rehabilitation. Neurology 2008, 71, 1856–1861. [Google Scholar] [CrossRef]
- Liu, J.; Dong, J.; Guo, J. The effects of nutrition supplement on rehabilitation for patients with stroke: Analysis based on 16 randomized controlled trials. Medicine 2022, 101, e29651. [Google Scholar] [CrossRef]
- Eto, F.; Nezu, T.; Aoki, S.; Kamimura, T.; Naito, H.; Shiga, Y.; Hosomi, N.; Maruyama, H. The association between nutritional intake one week after admission and outcome in acute ischemic stroke patients. J. Stroke Cerebrovasc. Dis. 2022, 31, 106812. [Google Scholar] [CrossRef]
- Shimizu, A.; Maeda, K.; Koyanagi, Y.; Kayashita, J.; Fujishima, I.; Mori, N. The Global Leadership Initiative on Malnutrition–Defined Malnutrition Predicts Prognosis in Persons with Stroke-Related Dysphagia. J. Am. Med Dir. Assoc. 2019, 20, 1628–1633. [Google Scholar] [CrossRef]
- Nishioka, S.; Yamasaki, K.; Ogawa, K.; Oishi, K.; Yano, Y.; Okazaki, Y.; Nakashima, R.; Kurihara, M. Impact of nutritional status, muscle mass and oral status on recovery of full oral intake among stroke patients receiving enteral nutrition: A retrospective cohort study. Nutr. Diet. 2020, 77, 456–466. [Google Scholar] [CrossRef]
- Nishioka, S.; Okamoto, T.; Takayama, M.; Urushihara, M.; Watanabe, M.; Kiriya, Y.; Shintani, K.; Nakagomi, H.; Kageyama, N. Malnutrition risk predicts recovery of full oral intake among older adult stroke patients undergoing enteral nutrition: Secondary analysis of a multicentre survey (the APPLE study). Clin. Nutr. 2017, 36, 1089–1096. [Google Scholar] [CrossRef]
- Zhu, B.L.; Wu, Y.Z.; Cai, Z.M.; Liao, C.-W.; Sun, L.Q.; Liu, Z.P.; Chen, H.M.; Huang, X.R.; Feng, R.Q.; Ye, S.L.; et al. A prospective epidemiological analysis of controlling nutritional status score with the poor functional outcomes in Chinese patients with haemorrhagic stroke. Br. J. Nutr. 2022, 128, 192–199. [Google Scholar] [CrossRef]
- Scrutinio, D.; Lanzillo, B.; Guida, P.; Passantino, A.; Spaccavento, S.; Battista, P. Association Between Malnutrition and Outcomes in Patients with Severe Ischemic Stroke Undergoing Rehabilitation. Arch. Phys. Med. Rehabil. 2020, 101, 852–860. [Google Scholar] [CrossRef]
- Sato, K.; Inoue, T.; Maeda, K.; Shimizu, A.; Ueshima, J.; Ishida, Y.; Ogawa, T.; Suenaga, M. Undernutrition at Admission Suppresses Post-Stroke Recovery of Trunk Function. J. Stroke Cerebrovasc. Dis. 2022, 31, 06354. [Google Scholar] [CrossRef]
- Nozoe, M.; Kubo, H.; Kanai, M.; Yamamoto, M. Relationships between Pre-Stroke SARC-F Scores, Disability, and Risk of Malnutrition and Functional Out-comes after Stroke—A Prospective Cohort Study. Nutrients 2021, 13, 3586. [Google Scholar] [CrossRef]
- Nishioka, S.; Omagari, K.; Nishioka, E.; Mori, N.; Taketani, Y.; Kayashita, J. Concurrent and predictive validity of the Mini Nutritional Assessment Short-Form and the Geriatric Nutri-tional Risk Index in older stroke rehabilitation patients. J. Hum. Nutr. Diet. 2020, 33, 12–22. [Google Scholar] [CrossRef]
- Naito, H.; Nezu, T.; Hosomi, N.; Aoki, S.; Kinoshita, N.; Kuga, J.; Shimomura, R.; Araki, M.; Ueno, H.; Ochi, K.; et al. Controlling nutritional status score for predicting 3-mo functional outcome in acute ischemic stroke. Nutrition 2018, 55–56, 1–6. [Google Scholar] [CrossRef]
- Liu, T.; Wu, L.Y.; Yang, X.M.; Chen, Y.; Du, X.J.; Luo, X.D.; Zhou, J.; Sui, Y.; Zhu, W.T. Influence of Nutritional Status on Prognosis of Stroke Patients with Dysphagia. Altern. Ther. Health Med. 2022, 28, 26–33. [Google Scholar]
- Lee, E.C.; Jeong, Y.G.; Jung, J.H.; Moon, H.I. Validity of the Controlling Nutritional Status score as a Nutritional Assessment Tool early after stroke. Int. J. Rehabil. Res. 2022, 45, 58–64. [Google Scholar] [CrossRef]
- Kokura, Y.; Maeda, K.; Wakabayashi, H.; Nishioka, S.; Higashi, S. High Nutritional-Related Risk on Admission Predicts Less Improvement of Functional Independence Measure in Geriatric Stroke Patients: A Retrospective Cohort Study. J. Stroke Cerebrovasc. Dis. 2016, 25, 1335–1341. [Google Scholar] [CrossRef]
- Kokura, Y.; Kimoto, K.; Okada, Y.; Kawakita, S. The Controlling Nutritional Status score as a functional prognostic marker in patients with acute stroke: A multicenter retrospective cohort study. Nutrition 2020, 79–80, 110889. [Google Scholar] [CrossRef]
- Kamimoto, T.; Shindo, K.; Shimomura, T.; Akimoto, T.; Yamada, T.; Mori, N.; Nakao, K.; Tsujikawa, M.; Honaga, K.; Kutsuna, T.; et al. Relationship between initial nutritional status and functional independence measures at discharge in subacute stroke. J. Stroke Cerebrovasc. Dis. 2022, 31, 106754. [Google Scholar] [CrossRef]
- Irisawa, H.; Mizushima, T. Correlation of Body Composition and Nutritional Status with Functional Recovery in Stroke Rehabilitation Patients. Nutrients 2020, 12, 1923. [Google Scholar] [CrossRef]
- Fluck, D.; Dsc, C.H.F.; Gulli, G.; Affley, B.; Robin, J.; Kakar, P.; Sharma, P.; Han, T.S. Association of risk of malnutrition with adverse outcomes and early support on discharge in acute stroke patients without prestroke disability: A multicenter, registry-based cohort study. Nutr. Clin. Pr. 2022, 37, 1233–1241. [Google Scholar] [CrossRef]
- Davis, J.P.; Wong, A.A.; Schluter, P.J.; Henderson, R.D.; O’sullivan, J.D.; Read, S.J. Impact of premorbid undernutrition on outcome in stroke patients. Stroke 2004, 35, 1930–1934. [Google Scholar] [CrossRef]
- Zhang, M.; Ye, S.; Huang, X.; Sun, L.; Liu, Z.; Liao, C.; Feng, R.; Chen, H.; Wu, Y.; Cai, Z.; et al. Comparing the prognostic significance of nutritional screening tools and ESPEN-DCM on 3-month and 12-month outcomes in stroke patients. Clin. Nutr. 2021, 40, 3346–3353. [Google Scholar] [CrossRef]
- Zhang, G.; Pan, Y.; Zhang, R.; Wang, M.; Meng, X.; Li, Z.; Li, H.; Wang, Y.; Zhao, X.; Liu, G.; et al. Prevalence and Prognostic Significance of Malnutrition Risk in Patients with Acute Ischemic Stroke: Results From the Third China National Stroke Registry. Stroke 2022, 53, 111–119. [Google Scholar] [CrossRef]
- Xiang, W.; Chen, X.; Ye, W.; Li, J.; Zhang, X.; Xie, D. Prognostic Nutritional Index for Predicting 3-Month Outcomes in Ischemic Stroke Patients Undergoing Thrombolysis. Front. Neurol. 2020, 11, 599. [Google Scholar] [CrossRef]
- Tsutsumiuchi, K.; Wakabayashi, H.; Maeda, K.; Shamoto, H. Impact of malnutrition on post-stroke cognitive impairment in convalescent rehabilitation ward inpa-tients. Eur. Geriatr. Med. 2021, 12, 167–174. [Google Scholar] [CrossRef]
- Pandian, J.D.; Jyotsna, R.; Singh, R.; Sylaja, P.N.; Vijaya, P.; Padma, M.V.; Venkateswaralu, K.; Sukumaran, S.; Radhakrishnan, K.; Sarma, P.S.; et al. Premorbid nutrition and short term outcome of stroke: A multicentre study from India. J. Neurol. Neurosurg. Psychiatry 2011, 82, 1087–1092. [Google Scholar] [CrossRef]
- Kang, M.K.; Kim, T.J.; Kim, Y.; Nam, K.-W.; Jeong, H.-Y.; Kim, S.K.; Lee, J.S.; Ko, S.-B.; Yoon, B.-W. Geriatric nutritional risk index predicts poor outcomes in patients with acute ischemic stroke—Automated undernutrition screen tool. PLoS ONE 2020, 15, e0228738. [Google Scholar] [CrossRef]
- Aliasghari, F.; Izadi, A.; Khalili, M.; Farhoudi, M.; Ahmadiyan, S.; Deljavan, R. Impact of Premorbid Malnutrition and Dysphagia on Ischemic Stroke Outcome in Elderly Patients: A Community-Based Study. J. Am. Coll. Nutr. 2019, 38, 318–326. [Google Scholar] [CrossRef]
- Akimoto, T.; Hara, M.; Morita, A.; Uehara, S.; Nakajima, H. Relationship between Nutritional Scales and Prognosis in Elderly Patients after Acute Ischemic Stroke: Comparison of Controlling Nutritional Status Score and Geriatric Nutritional Risk Index. Ann. Nutr. Metab. 2021, 77, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Zielińska-Nowak, E.; Cichon, N.; Saluk-Bijak, J.; Bijak, M.; Miller, E. Nutritional Supplements and Neuroprotective Diets and Their Potential Clinical Significance in Post-Stroke Rehabilitation. Nutrients 2021, 13, 2704. [Google Scholar] [CrossRef]
- Yang, J.-S.; Wang, S.-S.; Zhou, X.-Y.; Chen, Z.-L.; Liu, C.-F.; Shen, Y.-P.; Hao, J.-J. The risk factors for malnutrition in post-stroke patients. Zhonghua Nei Ke Za Zhi 2009, 48, 1016–1018. [Google Scholar]
- Poels, B.J.J.; Brinkman-Zijlker, H.G.; Dijkstra, P.U.; Postema, K. Malnutrition, eating difficulties and feeding dependence in a stroke rehabilitation centre. Disabil. Rehabilitation 2006, 28, 637–643. [Google Scholar]
- Finestone, H.M.; Greene-Finestone, L.S.; Wilson, E.S.; Teasell, R.W. Malnutrition in stroke patients on the rehabilitation service and at follow-up—Prevalence and predictors. Arch. Phys. Med. Rehabil. 1995, 76, 310–316. [Google Scholar] [CrossRef]
- Chen, N.; Li, Y.; Fang, J.; Lu, Q.; He, L. Risk factors for malnutrition in stroke patients: A meta-analysis. Clin. Nutr. 2019, 38, 127–135. [Google Scholar] [CrossRef]
- Liu, C.H.; Huo, M.; Qin, H.H.; Zhao, B.L. Critical prognostic factors for poststroke dysphagia: A meta-analysis. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 610–622. [Google Scholar]
- Ignacio de Ulíbarri, J.; González-Madroño, A.; de Villar, N.G.P.; González, P.; González, B.; Mancha, A.; Rodríguez, F.; Fernández, G. CONUT: A tool for controlling nutritional status. First validation in a hospital population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.-P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef] [PubMed]
- Bharadwaj, S.; Ginoya, S.; Tandon, P.; Gohel, T.D.; Guirguis, J.; Vallabh, H.; Jevenn, A.; Hanouneh, I. Malnutrition: Laboratory markers vs. nutritional assessment. Gastroenterol. Rep. 2016, 4, 272–280. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, X. Controlling nutritional status score, a promising prognostic marker in patients with gastrointestinal cancers after surgery: A systematic review and meta-analysis. Int. J. Surg. 2018, 55, 39–45. [Google Scholar] [CrossRef]
- Xie, H.; Tang, S.; Wei, L.; Gan, J. Geriatric nutritional risk index as a predictor of complications and long-term outcomes in patients with gas-trointestinal malignancy: A systematic review and meta-analysis. Cancer Cell Int. 2020, 20, 530. [Google Scholar] [CrossRef]
- Hu, Y.; Yang, H.; Zhou, Y.; Liu, X.; Zou, C.; Ji, S.; Liang, T. Prediction of all-cause mortality with malnutrition assessed by nutritional screening and assessment tools in patients with heart failure: A systematic review. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 1361–1374. [Google Scholar] [CrossRef]
- Lin, H.; Zhang, H.; Lin, Z.; Li, X.; Kong, X.; Sun, G. Review of nutritional screening and assessment tools and clinical outcomes in heart failure. Hear. Fail. Rev. 2016, 21, 549–565. [Google Scholar] [CrossRef]
- Power, L.; Mullally, D.; Gibney, E.R.; Clarke, M.; Visser, M.; Volkert, D.; Bardon, L.; de van der Schueren, M.A.; Corish, C.A. A review of the validity of malnutrition screening tools used in older adults in community and healthcare settings—A MaNuEL study. Clin. Nutr. Espen 2018, 24, 1–13. [Google Scholar] [CrossRef]
- de Ulíbarri Pérez, J.I.; Fernández, G.; Salvanés, F.R.; López, A.M.D. Nutritional screening; control of clinical undernutrition with analytical parameters. Nutr. Hosp. 2014, 29, 797–811. [Google Scholar]
- Cengiz, O.; Kocer, B.; Sürmeli, S.; Santicky, M.J.; Soran, A. Are pretreatment serum albumin and cholesterol levels prognostic tools in patients with colorectal carcinoma? Med. Sci. Monit. 2006, 12, Cr240-7. [Google Scholar]
- Kondrup, J.; Rasmussen, H.H.; Hamberg, O.; Stanga, Z. Nutritional risk screening (NRS 2002): A new method based on an analysis of controlled clinical trials. Clin. Nutr. 2003, 22, 321–336. [Google Scholar] [CrossRef]
- Poulia, K.-A.; Klek, S.; Doundoulakis, I.; Bouras, E.; Karayiannis, D.; Baschali, A.; Passakiotou, M.; Chourdakis, M. The two most popular malnutrition screening tools in the light of the new ESPEN consensus definition of the diagnostic criteria for malnutrition. Clin. Nutr. 2017, 36, 1130–1135. [Google Scholar] [CrossRef] [PubMed]
- Thibault, R.; Abbasoglu, O.; Ioannou, E.; Meija, L.; Ottens-Oussoren, K.; Pichard, C.; Rothenberg, E.; Rubin, D.; Siljamäki-Ojansuu, U.; Vaillant, M.-F.; et al. ESPEN guideline on hospital nutrition. Clin. Nutr. 2021, 40, 5684–5709. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Li, D.; Liu, Y.; Zhu, L.; Jia, Y.; Gao, Y. Nutritional risk screening 2002 scale and subsequent risk of stroke-associated infection in ischemic stroke: The REMISE study. Front. Nutr. 2022, 9, 895803. [Google Scholar] [CrossRef] [PubMed]
- Stratton, R.J.; Hackston, A.; Longmore, D.; Dixon, R.; Price, S.; Stroud, M.; King, C.; Elia, M. Malnutrition in hospital outpatients and inpatients: Prevalence, concurrent validity and ease of use of the ‘malnutrition universal screening tool’ (‘MUST’) for adults. Br. J. Nutr. 2007, 92, 799–808. [Google Scholar] [CrossRef]
- Di Vincenzo, O.; Luisi, M.L.E.; Alicante, P.; Ballarin, G.; Biffi, B.; Gheri, C.F.; Scalfi, L. The Assessment of the Risk of Malnutrition (Undernutrition) in Stroke Patients. Nutrients 2023, 15, 683. [Google Scholar] [CrossRef] [PubMed]
- Ukleja, A.; Gilbert, K.; Mogensen, K.M.; Walker, R.; Ward, C.T.; Ybarra, J.; Holcombe, B. Standards for Nutrition Support: Adult Hospitalized Patients. Nutr. Clin. Pract. 2018, 33, 906–920. [Google Scholar] [CrossRef]
- Detsky, A.S.; McLaughlin, J.R.; Baker, J.P.; Johnston, N.A.N.C.Y.; Whittaker, S.; Mendelson, R.A.; Jeejeebhoy, K.N. What is subjective global assessment of nutritional status? JPEN J. Parenter. Enter. Nutr. 1987, 11, 8–13. [Google Scholar] [CrossRef]
- FD, O. Patient-Generated Subjective Global Assessment. In The Clinical Guide to Oncology Nutrition; Polisena, P.M.C., Ed.; The American Dietetic Association: Chicago, IL, USA, 2000; pp. 11–23. [Google Scholar]
- Guigoz, Y.; Vellas, B.; Garry, P.J. Assessing the nutritional status of the elderly: The mini nutritional assessment as part of the geriatric evaluation. Nutr. Rev. 1996, 54, S59–S65. [Google Scholar] [CrossRef]
- Cederholm, T.; Bosaeus, I.; Barazzoni, R.; Bauer, J.; Van Gossum, A.; Klek, S.; Muscaritoli, M.; Nyulasi, I.; Ockenga, J.; Schneider, S.; et al. Diagnostic criteria for malnutrition—An ESPEN Consensus Statement. Clin. Nutr. 2015, 34, 335–340. [Google Scholar] [CrossRef]
- van Bokhorst-de van der Schueren, M.A.; Guaitoli, P.R.; Jansma, E.P.; de Vet, H.C. Nutrition screening tools: Does one size fit all? A systematic review of screening tools for the hospital setting. Clin. Nutr. 2014, 33, 39–58. [Google Scholar] [CrossRef] [PubMed]
- Correia, M. Nutrition Screening vs. Nutrition Assessment: What’s the Difference? Nutr. Clin. Pract. 2018, 33, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Barbosa-Silva, M.C.G.; Barros, A.J.D. Indications and limitations of the use of subjective global assessment in clinical practice: An update. Curr. Opin. Clin. Nutr. Metab. Care 2006, 9, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, C.; Paur, I.; Pedersen, A.; Kværner, A.S.; Ræder, H.; Henriksen, H.B.; Bøhn, S.K.; Wiedswang, G.; Blomhoff, R. Agreement between GLIM and PG-SGA for diagnosis of malnutrition depends ons the screening tool used in GLIM. Clin. Nutr. 2022, 41, 329–336. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year Published | Country | Study Design | Study Population | Sample Size (n) | Age (Mean ± SD, Years) | Gender (n, Female/Male) | Screening or Assessment Tools | Follow-Up Time | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| B. L. Zhu, 2022 [23] | China | prospectively | patients with hemorrhagic stroke | 328 | 60.38 ± 12.38 | 109/219 | NRS2002, COUNT | after 3 months | physical functional status |
| K. Sato, 2022 [25] | Japan | retrospective | elderly patients with subacute stroke | 183 | 79.7 ± 7.5 | 80/103 | GLIM criteria | at hospital discharge | physical functional status |
| T. Liu, 2022 [29] | China | retrospective | patients with dysphagia after acute stroke | 789 | Not mentioned | 261/528 | NRS2002, SGA | after 3 months | physical functional status |
| E. C. Lee, 2022 [30] | South Korea | retrospective | patients with stroke | 117 | 67.77 ± 15.15 | 54/63 | COUNT | after 1 month | physical functional status |
| T. Kamimoto, 2022 [33] | Japan | retrospective | elderly patients with subacute stroke | 205 | 77.8 ± 7.1 | 107/98 | COUNT | at hospital discharge | physical functional status |
| D. Fluck, 2022 [35] | UK. | prospectively | patients with stroke | 2962 | 73.5 ± 13.1 | 1447/1515 | MUST | at hospital discharge | physical functional status |
| G. Zhang, 2022 [38] | China | prospectively | patients with acute ischemic stroke | 8698 | 62.26 ± 11.25 | 2706/5992 | GNRI, COUNT, PNI | after 12 months | physical functional status |
| M. Nozoe, 2021 [26] | Japan | prospectively | elderly patients with acute stroke | 324 | 76 ± 11 | 137/187 | GNRI | after 3 months | physical functional status |
| T. Akimoto, 2021 [44] | Japan | retrospective | elderly patients with acute ischemic stroke | 218 | 80.51 ± 25.37 | 81/137 | COUNT, GNRI | at hospital discharge | physical functional status |
| D. Scrutinio, 2020 [24] | Italy | retrospective | patients with subacute ischemic stroke | 668 | 75 (67–81) | 325/363 | PNI | at hospital discharge | physical functional status |
| S. Nishioka, 2020 [21] | Japan | retrospective | patients over 50 years old with dysphagia after acute stroke | 113 | 77 (66–83) | 58/55 | ESPEN-DCM | after 6 months | dysphagia |
| S. Nishioka, 2020 [27] | Japan | retrospective | elderly patients with subacute stroke | 420 | 78.1 ± 7.9 | 171/249 | MNA-SF, GNRI, ESPEN-DCM | at hospital discharge | physical functional status, dysphagia, quality of life |
| Y. Kokura, 2020 [32] | Japan | retrospective | elderly patients with stroke | 702 | 76.3 ± 12 | 334/368 | COUNT | at hospital discharge | physical functional status |
| H. Irisawa, 2020 [34] | Japan | prospectively | patients with subacute stroke | 179 | 79.5 ± 11.5 | 90/89 | GNRI | after 1 month | physical functional status |
| M. K. Kang, 2020 [42] | South Korea | prospectively | patients with stroke | 1906 | 67.77 ± 12.30 | 738/1168 | GNRI | after 3 months | physical functional status |
| M. Zhang, 2020 [37] | China | prospectively | patients with stroke | 593 | 67.3 ± 12.0 | 237/356 | COUNT, GNRI, MUST, NRS-2002, ESPEN-DCM | after 3 months | physical functional status |
| W. Xiang, 2020 [39] | China | retrospective | patients after thrombolytic therapy | 405 | 66 ± 16 | 210/195 | COUNT, PNI | after 3 months | physical functional status |
| K. Tsutsumiuchi, 2020 [40] | Japan | retrospective | patients with subacute stroke and functional impairment | 90 | 75 ± 8.7 | 43/47 | MNA-SF | at hospital discharge | physical functional status |
| A. Shimizu, 2019 [20] | Japan | retrospective | elderly patients with dysphagia after acute stroke | 188 | 78.9 ± 7.7 | 68/120 | GLIM criteria | at hospital discharge | physical functional status, dysphagia |
| H. Naito, 2018 [28] | Japan | retrospective | patients with acute ischemic stroke | 264 | 70.9 ± 12.2 | 93/171 | COUNT | after 3 months | physical functional status |
| F. Aliasghari, 2018 [43] | Iran | prospectively | patients with ischemic stroke | 253 | 74.42 ± 7.8 | 120/133 | MNA | after 3 months | physical functional status |
| S. Nishioka, 2017 [22] | Japan | retrospective | patients with dysphagia after stroke | 264 | 78.5 ± 7.5 | 109/155 | GNRI | at hospital discharge | dysphagia |
| Y. Kokura, 2016 [31] | Japan | retrospective | patients with subacute stroke | 540 | 80 (75–85) | 269/271 | GNRI | at hospital discharge | physical functional status |
| J. D. Pandian, 2011 [41] | India | prospectively | patients with stroke | 448 | 58.66 ± 13.7 | 110/216 | SGA | after 1 month | physical functional status |
| J. Martineau, 2005 [5] | Australia | retrospective | patients with stroke | 73 | 72.78 ± 12.98 | - | PG-SGA | at hospital discharge | dysphagia, quality of life |
| J. P. Davis, 2004 [36] | Australia | prospectively | patients with stroke | 185 | Not mentioned | 87/98 | SGA | after 1 month | physical functional status |
| Number of Studies (n) | Poor Functional Outcome (OR with 95% CI) | I2 | Number of Studies (n) | FIM Scores (WMD with 95% CI) | I2 | Number of Studies (n) | Dysphagia (OR with 95% CI) | I2 | |
|---|---|---|---|---|---|---|---|---|---|
| Nutritional screening tools | 10 | 2.29 (1.81 to 2.89) | 51.2% | 2 | −22.90 (−58.16 to 12.36) | 96.3% | 1 | 3.58 (1.15 to 11.17) | 0% |
| Nutritional assessment tools | 5 | 2.34 (1.84 to 2.99) | 0% | 3 | −21.52 (−31.62 to −11.42) | 78.3% | 4 | 2.72 (1.50 to 4.92) | 71.40% |
| Tools | Number of Studies (n) | Poor Functional Outcome (OR with 95% CI) | I2 | Number of Studies (n) | FIM Scores (WMD with 95% CI) | I2 | Number of Studies (n) | Dysphagia (OR with 95% CI) | I2 |
|---|---|---|---|---|---|---|---|---|---|
| COUNT | 6 | 2.04 (1.44 to 2.88) | 72.1% | 1 | −4.52 (−16.64 to 7.60) | 0% | - | - | - |
| GNRI | 5 | 1.67 (1.31 to 2.13) | 52.4% | 1 | −41.73 (−50.48 to −32.97) | 0% | 1 | 3.58 (1.15 to 11.17) | 0% |
| SGA | 3 | 2.32 (1.69 to 3.19) | 0% | - | - | - | - | - | - |
| NRS2002 | 3 | 2.69 (1.74 to 4.15) | 40.8% | - | - | - | - | - | - |
| MUST | 2 | 8.33 (6.88 to 10.08) | 0.0% | - | - | - | - | - | - |
| PNI | 2 | 3.00 (2.11 to 4.27) | 13.0% | - | - | - | - | - | - |
| MNA | 1 | 1.60 (0.88 to 2.91) | 0% | - | - | - | - | - | - |
| MNA-SF | 1 | 15.00 (3.57 to 63.04) | 0% | 1 | −39.21 (−48.22 to −30.21) | 0% | - | - | - |
| ESPEN-DCM | 1 | 3.05 (1.64 to 5.65) | 0% | 1 | −29.43(−37.13 to −21.74) | 0% | 2 | 2.27 (0.82 to 6.25) | 89.0% |
| GLIM criteria | - | - | - | 2 | –17.38 (−27.79 to−6.97) | 67.6% | 1 | 2.88 (1.50 to 5.55) | 0% |
| PG-SGA | - | - | - | - | - | - | 1 | 5.26 (1.46 to 18.96) | 0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, P.; Tian, H.; Ji, T.; Zhong, T.; Gao, L.; Chen, L. Predictive Value of Malnutrition, Identified via Different Nutritional Screening or Assessment Tools, for Functional Outcomes in Patients with Stroke: A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 3280. https://doi.org/10.3390/nu15143280
Liu P, Tian H, Ji T, Zhong T, Gao L, Chen L. Predictive Value of Malnutrition, Identified via Different Nutritional Screening or Assessment Tools, for Functional Outcomes in Patients with Stroke: A Systematic Review and Meta-Analysis. Nutrients. 2023; 15(14):3280. https://doi.org/10.3390/nu15143280
Chicago/Turabian StyleLiu, Peiqi, Huimin Tian, Tianliang Ji, Tangsheng Zhong, Lan Gao, and Li Chen. 2023. "Predictive Value of Malnutrition, Identified via Different Nutritional Screening or Assessment Tools, for Functional Outcomes in Patients with Stroke: A Systematic Review and Meta-Analysis" Nutrients 15, no. 14: 3280. https://doi.org/10.3390/nu15143280
APA StyleLiu, P., Tian, H., Ji, T., Zhong, T., Gao, L., & Chen, L. (2023). Predictive Value of Malnutrition, Identified via Different Nutritional Screening or Assessment Tools, for Functional Outcomes in Patients with Stroke: A Systematic Review and Meta-Analysis. Nutrients, 15(14), 3280. https://doi.org/10.3390/nu15143280