
What Is the Role of Nutraceutical Products in Cancer Patients? A Systematic Review of Randomized Clinical Trials
 , ,
, , 
Abstract

1. Introduction
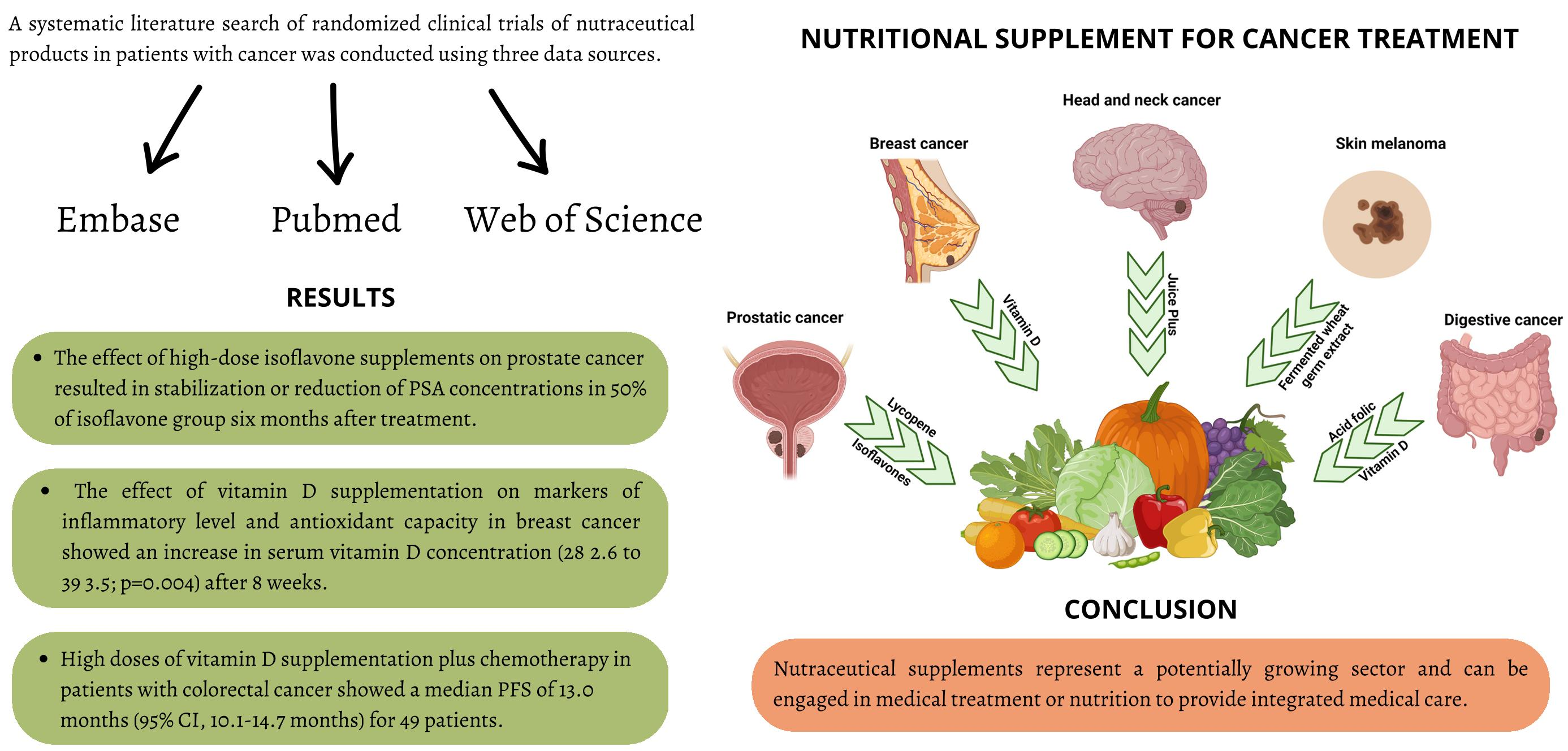
2. Methods of the Systematic Review
2.1. Protocol Registration and Reporting Format
2.2. Search Strategy and Selection Criteria
2.3. PICO Question
2.4. Eligibility Criteria
2.5. Study Evaluation
3. Results of the Systematic Review
3.1. Randomized Clinical Trials Focused on Prostatic Cancer
3.2. Randomized Clinical Trials Focused on Digestive Cancer
3.3. Randomized Clinical Trials Focused on Other Cancer
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kamal, N.; Ilowefah, M.A.; Hilles, A.R.; Anua, N.A.; Awin, T.; Alshwyeh, H.A.; Aldosary, S.K.; Jambocus, N.G.S.; Alosaimi, A.A.; Rahman, A.; et al. Genesis and Mechanism of Some Cancer Types and an Overview on the Role of Diet and Nutrition in Cancer Prevention. Molecules 2022, 27, 1794. [Google Scholar] [CrossRef]
- Maiuolo, J.; Gliozzi, M.; Carresi, C.; Musolino, V.; Oppedisano, F.; Scarano, F.; Nucera, S.; Scicchitano, M.; Bosco, F.; Macri, R.; et al. Nutraceuticals and Cancer: Potential for Natural Polyphenols. Nutrients 2021, 13, 3834. [Google Scholar] [CrossRef] [PubMed]
- Chaffer, C.L.; Weinberg, R.A. A Perspective on Cancer Cell Metastasis. Science 2011, 331, 1559–1564. [Google Scholar] [CrossRef]
- Tripathi, C.; Girme, A.; Champaneri, S.; Patel, R.J.; Hingorani, L. Nutraceutical Regulations: An Opportunity in ASEAN Countries. Nutrition 2020, 74, 110729. [Google Scholar] [CrossRef] [PubMed]
- D’Angelo, S.; La Porta, R.; Napolitano, M.; Galletti, P.; Quagliuolo, L.; Boccellino, M. Effect of Annurca Apple Polyphenols on Human HaCaT Keratinocytes Proliferation. J. Med. Food 2012, 15, 1024–1031. [Google Scholar] [CrossRef] [PubMed]
- Akutsu, T.; Kitamura, H.; Himeiwa, S.; Kitada, S.; Akasu, T.; Urashima, M. Vitamin D and Cancer Survival: Does Vitamin D Supplementation Improve the Survival of Patients with Cancer? Curr. Oncol. Rep. 2020, 22, 62. [Google Scholar] [CrossRef]
- Wang, L.; Sesso, H.D.; Glynn, R.J.; Christen, W.G.; Bubes, V.; Manson, J.A.E.; Buring, J.E.; Gaziano, J.M. Vitamin E and C Supplementation and Risk of Cancer in Men: Posttrial Follow-up in the Physicians’ Health Study II Randomized Trial. Am. J. Clin. Nutr. 2014, 100, 915–923. [Google Scholar] [CrossRef]
- Hanson, M.G.V.; Özenci, V.; Carlsten, M.C.V.; Glimelius, B.L.; Frödin, J.-E.A.; Masucci, G.; Malmberg, K.-J.; Kiessling, R.V.R. A Short-Term Dietary Supplementation with High Doses of Vitamin E Increases NK Cell Cytolytic Activity in Advanced Colorectal Cancer Patients. Cancer Immunol. Immunother. 2007, 56, 973–984. [Google Scholar] [CrossRef]
- Crocetto, F.; Boccellino, M.; Barone, B.; Di Zazzo, E.; Sciarra, A.; Galasso, G.; Settembre, G.; Quagliuolo, L.; Imbimbo, C.; Boffo, S.; et al. The Crosstalk between Prostate Cancer and Microbiota Inflammation: Nutraceutical Products Are Useful to Balance This Interplay? Nutrients 2020, 12, 2648. [Google Scholar] [CrossRef]
- Marino, M.M.; Nastri, B.M.; D’Agostino, M.; Risolo, R.; De Angelis, A.; Settembre, G.; Rienzo, M.; D’Esposito, V.; Abbondanza, C.; Formisano, P.; et al. Does Gut-Breast Microbiota Axis Orchestrates Cancer Progression? Endocr. Metab. Immune Disord. Drug Targets 2022, 22, 1111–1122. [Google Scholar] [CrossRef]
- Zovi, A.; Ferrara, F.; Pasquinucci, R.; Nava, L.; Vitiello, A.; Arrigoni, R.; Ballini, A.; Cantore, S.; Palmirotta, R.; Di Domenico, M.; et al. Effects of Vitamin D on the Renin-Angiotensin System and Acute Childhood Pneumonia. Antibiotics 2022, 11, 1545. [Google Scholar] [CrossRef]
- Calvani, M.; Pasha, A.; Favre, C. Nutraceutical Boom in Cancer: Inside the Labyrinth of Reactive Oxygen Species. Int. J. Mol. Sci. 2020, 21, 1936. [Google Scholar] [CrossRef]
- Vrânceanu, M.; Galimberti, D.; Banc, R.; Dragoş, O.; Cozma-Petruţ, A.; Hegheş, S.C.; Voştinaru, O.; Cuciureanu, M.; Stroia, C.M.; Miere, D.; et al. The Anticancer Potential of Plant-Derived Nutraceuticals via the Modulation of Gene Expression. Plants 2022, 11, 2524. [Google Scholar] [CrossRef] [PubMed]
- Arrigoni, R.; Ballini, A.; Santacroce, L.; Cantore, S.; Inchingolo, A.; Inchingolo, F.; Di Domenico, M.; Quagliuolo, L.; Boccellino, M. Another Look at Dietary Polyphenols: Challenges in Cancer Prevention and Treatment. Curr. Med. Chem. 2021, 29, 1061–1082. [Google Scholar] [CrossRef]
- Boccellino, M.; Donniacuo, M.; Bruno, F.; Rinaldi, B.; Quagliuolo, L.; Ambruosi, M.; Pace, S.; De Rosa, M.; Olgaç, A.; Banoglu, E.; et al. Protective Effect of Piceatannol and Bioactive Stilbene Derivatives against Hypoxia-Induced Toxicity in H9c2 Cardiomyocytes and Structural Elucidation as 5-LOX Inhibitors. Eur. J. Med. Chem. 2019, 180, 637–647. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.M.; Weinberg, V.; Magbanua, M.J.; Sosa, E.; Simko, J.; Shinohara, K.; Federman, S.; Mattie, M.; Hughes-Fulford, M.; Haqq, C.; et al. Nutritional Supplements, COX-2 and IGF-1 Expression in Men on Active Surveillance for Prostate Cancer. Cancer Causes Control 2011, 22, 141–150. [Google Scholar] [CrossRef]
- DeVere White, R.W.; Tsodikov, A.; Stapp, E.C.; Soares, S.E.; Fujii, H.; Hackman, R.M. Effects of a High Dose, Aglycone-Rich Soy Extract on Prostate-Specific Antigen and Serum Isoflavone Concentrations in Men with Localized Prostate Cancer. Nutr. Cancer 2010, 62, 1036–1043. [Google Scholar] [CrossRef]
- Gontero, P.; Marra, G.; Soria, F.; Oderda, M.; Zitella, A.; Baratta, F.; Chiorino, G.; Gregnanin, I.; Daniele, L.; Cattel, L.; et al. A Randomized Double-Blind Placebo Controlled Phase I-II Study on Clinical and Molecular Effects of Dietary Supplements in Men With Precancerous Prostatic Lesions. Chemoprevention or “Chemopromotion”? Prostate 2015, 75, 1177–1186. [Google Scholar] [CrossRef] [PubMed]
- Grainger, E.M.; Schwartz, S.J.; Wang, S.; Unlu, N.Z.; Boileau, T.W.M.; Ferketich, A.K.; Monk, J.P.; Gong, M.C.; Bahnson, R.R.; DeGroff, V.L.; et al. A Combination of Tomato and Soy Products for Men with Recurring Prostate Cancer and Rising Prostate Specific Antigen. Nutr. Cancer 2008, 60, 145–154. [Google Scholar] [CrossRef]
- Kumar, N.B.; Cantor, A.; Allen, K.; Riccardi, D.; Besterman-Dahan, K.; Seigne, J.; Helal, M.; Salup, R.; Pow-Sang, J. The Specific Role of Isoflavones in Reducing Prostate Cancer Risk. Prostate 2004, 59, 141–147. [Google Scholar] [CrossRef]
- Kumar, N.B.; Krischer, J.P.; Allen, K.; Riccardi, D.; Besterman-Dahan, K.; Salup, R.; Kang, L.; Xu, P.; Pow-Sang, J. A Phase II Randomized, Placebo-Controlled Clinical Trial of Purified Isoflavones in Modulating Steroid Hormones in Men Diagnosed With Localized Prostate Cancer. Nutr. Cancer 2007, 59, 163. [Google Scholar] [CrossRef]
- Schröder, F.H.; Roobol, M.J.; Boevé, E.R.; De Mutsert, R.; Zuijdgeest-Van Leeuwen, S.D.; Kersten, I.; Wildhagen, M.F.; Van Helvoort, A. Randomized, Double-Blind, Placebo-Controlled Crossover Study in Men with Prostate Cancer and Rising PSA: Effectiveness of a Dietary Supplement. Eur. Urol. 2005, 48, 922–931. [Google Scholar] [CrossRef]
- Farsad-Naeimi, A.; Alizadeh, M.; Esfahani, A.; Darvish Aminabad, E. Effect of Fisetin Supplementation on Inflammatory Factors and Matrix Metalloproteinase Enzymes in Colorectal Cancer Patients. Food Funct. 2018, 9, 2025–2031. [Google Scholar] [CrossRef]
- Ng, K.; Nimeiri, H.S.; McCleary, N.J.; Abrams, T.A.; Yurgelun, M.B.; Cleary, J.M.; Rubinson, D.A.; Schrag, D.; Miksad, R.; Bullock, A.J.; et al. Effect of High-Dose vs Standard-Dose Vitamin D3 Supplementation on Progression-Free Survival Among Patients With Advanced or Metastatic Colorectal Cancer: The SUNSHINE Randomized Clinical Trial. JAMA 2019, 321, 1370. [Google Scholar] [CrossRef]
- Tsai, H.L.; Tai, C.J.; Huang, C.W.; Chang, F.R.; Wang, J.Y. Efficacy of Low-Molecular-Weight Fucoidan as a Supplemental Therapy in Metastatic Colorectal Cancer Patients: A Double-Blind Randomized Controlled Trial. Mar. Drugs 2017, 15, 122. [Google Scholar] [CrossRef] [PubMed]
- Urashima, M.; Ohdaira, H.; Akutsu, T.; Okada, S.; Yoshida, M.; Kitajima, M.; Suzuki, Y. Effect of Vitamin D Supplementation on Relapse-Free Survival Among Patients With Digestive Tract Cancers: The AMATERASU Randomized Clinical Trial. JAMA 2019, 321, 1361. [Google Scholar] [CrossRef] [PubMed]
- van Zweeden, A.A.; van Groeningen, C.J.; Honeywell, R.J.; Giovannetti, E.; Ruijter, R.; Smorenburg, C.H.; Giaccone, G.; Verheul, H.M.W.; Peters, G.J.; van der Vliet, H.J. Randomized Phase 2 Study of Gemcitabine and Cisplatin with or without Vitamin Supplementation in Patients with Advanced Esophagogastric Cancer. Cancer Chemother. Pharmacol. 2018, 82, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Datta, M.; Shaw, E.G.; Lesser, G.J.; Case, L.D.; Vitolins, M.Z.; Schneider, C.; Frizzell, B.; Sullivan, C.; Lively, M.; Franzmann, E.; et al. A Randomized Double-Blind Placebo-Controlled Trial of Fruit and Vegetable Concentrates on Intermediate Biomarkers in Head and Neck. Integr. Cancer Ther. 2018, 17, 115. [Google Scholar] [CrossRef]
- Demidov, L.V.; Manziuk, L.V.; Kharkevitch, G.Y.; Pirogova, N.A.; Artamonova, E.V. Adjuvant Fermented Wheat Germ Extract (AvemarTM) Nutraceutical Improves Survival of High-Risk Skin Melanoma Patients: A Randomized, Pilot, Phase II Clinical Study with a 7-Year Follow-Up. Cancer Biother. Radiopharm. 2008, 23, 477–482. [Google Scholar] [CrossRef]
- Mohseni, H.; Amani, R.; Hosseini, S.A.; Ekrami, A.; Ahmadzadeh, A.; Latifi, S.M. Genetic Variations in VDR Could Modulate the Efficacy of Vitamin D3 Supplementation on Inflammatory Markers and Total Antioxidant Capacity among Breast Cancer Women: A Randomized Double Blind Controlled Trial. Asian Pac J Cancer Prev 2019, 20, 2065. [Google Scholar] [CrossRef] [PubMed]
- Shahvegharasl, Z.; Pirouzpanah, S.; Mahboob, S.A.; Montazeri, V.; Adili, A.; Asvadi, I.; Sanaat, Z.; Esfehani, A.; Pirouzpanah, S.S.; Mesgari, M. Effects of Cholecalciferol Supplementation on Serum Angiogenic Biomarkers in Breast Cancer Patients Treated with Tamoxifen: A Controlled Randomized Clinical Trial. Nutrition 2020, 72, 110656. [Google Scholar] [CrossRef]
- Bhosale, P.B.; Ha, S.E.; Vetrivel, P.; Kim, H.H.; Kim, S.M.; Kim, G.S. Functions of Polyphenols and Its Anticancer Properties in Biomedical Research: A Narrative Review. Transl. Cancer Res. 2020, 9, 7619. [Google Scholar] [CrossRef]
- Niranjana, R.; Gayathri, R.; Nimish Mol, S.; Sugawara, T.; Hirata, T.; Miyashita, K.; Ganesan, P. Carotenoids Modulate the Hallmarks of Cancer Cells. J. Funct. Foods 2015, 18, 968–985. [Google Scholar] [CrossRef]
- Jóźwiak, M.; Filipowska, A.; Fiorino, F.; Struga, M. Anticancer Activities of Fatty Acids and Their Heterocyclic Derivatives. Eur. J. Pharmacol. 2020, 871, 172937. [Google Scholar] [CrossRef]
- Skrajnowska, D.; Bobrowska-Korczak, B. Potential Molecular Mechanisms of the Anti-Cancer Activity of Vitamin D. Anticancer Res. 2019, 39, 3353–3363. [Google Scholar] [CrossRef]
- Liang, Z.; Xie, H.; Shen, W.; Shao, L.; Zeng, L.; Huang, X.; Zhu, Q.; Zhai, X.; Li, K.; Qiu, Z.; et al. The Synergism of Natural Compounds and Conventional Therapeutics against Colorectal Cancer Progression and Metastasis. Front. Biosci. 2022, 27, 263. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.Y.; Cui, J.; Zhang, Y.; Wang, Z.L.; Chong, T.; Wang, Z.M. Isoflavones and Prostate Cancer: A Review of Some Critical Issues. Chin. Med. J. 2016, 129, 341. [Google Scholar] [CrossRef]
- Chen, P.; Zhang, W.; Wang, X.; Zhao, K.; Negi, D.S.; Zhuo, L.; Qi, M.; Wang, X.; Zhang, X. Lycopene and Risk of Prostate Cancer: A Systematic Review and Meta-Analysis. Medicine 2015, 94, e1260. [Google Scholar] [CrossRef]
- Engelhardt, P.F.; Riedl, C.R. Effects of One-Year Treatment with Isoflavone Extract from Red Clover on Prostate, Liver Function, Sexual Function, and Quality of Life in Men with Elevated PSA Levels and Negative Prostate Biopsy Findings. Urology 2008, 71, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Haseen, F.; Cantwell, M.M.; O’Sullivan, J.M.; Murray, L.J. Is There a Benefit from Lycopene Supplementation in Men with Prostate Cancer? A Systematic Review. Prostate Cancer Prostatic Dis. 2009, 12, 325–332. [Google Scholar] [CrossRef] [PubMed]
- de La Puente-Yagüe, M.; Cuadrado-Cenzual, M.A.; Ciudad-Cabañas, M.J.; Hernández-Cabria, M.; Collado-Yurrita, L. Vitamin D: And Its Role in Breast Cancer. Kaohsiung J. Med. Sci. 2018, 34, 423–427. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.Z.; Long, H.; Wu, T.D.; Zhou, Y.; Lu, H.B. The Effect of Estrogen-Related Receptor α on the Regulation of Angiogenesis after Spinal Cord Injury. Neuroscience 2015, 290, 570–580. [Google Scholar] [CrossRef]
- Vaughan-Shaw, P.G.; O’Sullivan, F.; Farrington, S.M.; Theodoratou, E.; Campbell, H.; Dunlop, M.G.; Zgaga, L. The Impact of Vitamin D Pathway Genetic Variation and Circulating 25-Hydroxyvitamin D on Cancer Outcome: Systematic Review and Meta-Analysis. Br. J. Cancer 2017, 116, 1095–1110. [Google Scholar] [CrossRef]
- Saiko, P.; Ozsvar-Kozma, M.; Madlener, S.; Bernhaus, A.; Lackner, A.; Grusch, M.; Horvath, Z.; Krupitza, G.; Jaeger, W.; Ammer, K.; et al. Avemar, a Nontoxic Fermented Wheat Germ Extract, Induces Apoptosis and Inhibits Ribonucleotide Reductase in Human HL-60 Promyelocytic Leukemia Cells. Cancer Lett. 2007, 250, 323–328. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Author (Year) | Number of Patient | Stage/Grade Prostatic Tumor | Nutraceutic Arm (Type; N) | Control Arm (Type; N) | Age Nutraceutic Arm Mean ± SD | Age Control Arm Mean ± SD | Nutraceutic Dosage | Outcome Included | Results |
|---|---|---|---|---|---|---|---|---|---|
| Chan JM, et al., 2010 [17] | 97 |
| First arm: lycopen; n = 22 Second arm: oil fish; n = 21 | Placebo; n = 26 | First arm: 61 ± 7 Second arm: 62 ± 8 | 59 ± 8 | First arm: two 15 mg lycopene soft gel capsules daily Second arm: three 1 g fish oil capsules daily (including 1098 mg EPA and 549 mg DHA |
|
|
| deVere White RW, et al., 2014 [18] | 53 | - | GCP; n = 28 | Placebo; n = 25 | 70.5 ± 9.3 | 68.6 ± 7.3 | 5 g/day of GCP, which contained 450 mg genistein and 300 mg daidzein and other isoflavones |
|
|
| Gontero P, et al., 2015 [19] | 53 |
| Selenium, lycopene, green tea catechins; n = 27 | Placebo; n = 26 | 64.1 ± 5.7 | 62.6 ± 8.2 | 55 μg selenium; 35 mg lycopene; 600 mg green tea catechins |
|
|
| Grainger EM, et al., 2008 [20] | 41 | - | Group A: First period tomato only, Second period Tomato +soy; n = 20 | Group B: First period Soy only, Second period Tomato +soy; n = 21 | - | - | Group A First period tomato only (Lycopene mg/day ± SD 43 ± 15) Second period Tomato +soy (Lycopene mg/day ± SD 40 ± 17; Soy protein g/day ± SD) Group B First period Soy only (protein g/day ± SD 39 ±1) Second period Tomato +soy (Lycopene mg/day 36 ± 11 Soy protein g/day ± SD 39 ± 2) |
|
|
| Kumar NB, et al., 2004 [21] | 76 |
| Isoflavone; n = 39 | Placebo; n = 37 | 72.5 ± 5.0 | 70.9 ± 5.3 | 60 mg/day of genistein |
|
|
| Kumar NB, et al., 2007 [22] | 53 |
| Isoflavones; n = 25 | Placebo; n = 28 | 71.75 ± 6.39 | 71.92 ± 5.59 | 80 mg daily |
|
|
| Schröder FH, et al., 2005 [23] | 42 | - | Soy, isoflavones, lycopene, silymarin and antioxidant; n = 20 | Placebo; n = 22 | - | - | Two tablets of the dietary supplement per day |
|
|
| Author (Year) | Number of Patient | Stage Tumor | Nutraceutic Arm (Type; N) | Control Arm (Type; N) | Male/Female Nutraceutic (N) | Male/Female Control (N) | Age Nutraceutic Arm Median (Range) | Age Control Arm Median (range) | Cancer Type | Nutraceutic Dosage | Outcome Included | Results |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Farsad-Naeimi A, et al., 2018 [24] | 37 | Stages II or III | Fisetin; n = 18 | Placebo; n = 19 | 13/5 | 10/9 | 53.87 ± 17.23 * | 57.12 ± 14.09 * | Colorectal cancer | 100 mg/day |
|
|
| Ng K, et al., 2019 [25] | 139 | - | High-Dose Vitamin D; n = 69 | Standard-Dose Vitamin D; n = 70 | 41/28 | 38/32 | 54 (47–65) | 56 (50–64) | Advanced or Metastatic Colorectal Cancer | 8000 IU/day (two 4000 IU capsules) for cycle 1 followed by 4000 IU/day for subsequent cycles |
|
|
| Tsai HL, et al., 2017 [26] | 54 | Stage IV | Low-Molecular-Weight Fucoidan; n = 28 | Placebo; n = 26 | 16/12 | 15/11 | 57.46 (30–79) | 62.38 (43–83) | Metastatic Colorectal Cancer | 4 g twice a day |
|
|
| Urashima M, et al., 2019 [27] | 417 | Stages I to III | Vitamin D; n = 251 | Placebo; n = 166 | 173/78 | 103/63 | 67 (61–75) | 64 (58–71) | Digestive Tract Cancer (esophagus, stomach, small intestine, colon, and rectum) | 2000 IU/day |
|
|
| van Zweeden AA, et al., 2018 [28] | 82 | - | Chemotherapy + Folic acid and vitamin B12; n = 41 | Chemotherapy; n = 41 | 33/8 | 33/8 | 61 (50–78) ** | 61 (35–82) ** | Advanced esophagogastric cancer | Folic acid 450 µg/day; vitamin B12 1000 µg every 9 weeks |
|
|
| Author (Year) | Number of Patient | Stage Tumor | Nutraceutic Arm (Type; N) | Control Arm (Type; N) | Male/Female Nutraceutic (N) | Male/Female Control (N) | Age Nutraceutic Arm Mean ± SD | Age Control Arm Mean ± SD | Cancer Type | Nutraceutic Dosage | Outcome Included | Results |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Datta M, et al., 2018 [29] | 134 | Stage I, II, III, or IV | Juice PLUS+; n = 72 | Placebo; n = 62 | 61/11 | 52/10 | 58 (30–82) * | 59 (41–82) * | Head and Neck Cancer | 2 capsules in the morning and 2 in the afternoon/evening |
|
|
| Demidov LV, et al., 2008 [30] | 52 | Stage III | FWGE + DTIC-based adjuvant chemotherapy; n = 26 | DTIC; n = 26 | 15/11 | 15/11 | 50.4 ± 12.6 | 47.7 ± 13.9 | Skin melanoma | 8.5 g of FWGE granulate to dissolve in 150 mmL of water, orally once-daily |
|
|
| Mohseni H, et al., 2019 [31] | 52 | Stage I to III | Vitamin D; n = 26 | Edible paraffin; n = 26 | - | - | 46.3 ± 9.5 | 47.7 ± 8.0 | Breast cancer | Vitamin D3: 50,000 IU/week |
|
|
| Shahvegharasl Z, et al., 2020 [32] | 44 | Stage I to III | Cholecalciferol; n = 22 | Placebo; n = 22 | - | - | 44.1 ± 6.8 | 41.8 ± 7.5 | Breast cancer | 50,000 IU weekly of cholecalciferol |
|
|
| Nutraceuticals Classes | Active ingredients of Nutraceuticals | Mechanism of Action | References |
|---|---|---|---|
| Polyphenolic Compounds | Flavones, Isoflavones, Flavonones, Flavonols, Phenolic Acids, Resveratrol, Curcumin |
| [33] |
| Carotenoids | Lycopene, α- and β-carotene, α-cryptoxanthin, Zeaxanthin, Fucoxanthin |
| [34] |
| Lipids and polyunsaturated fatty acids | Alpha-linolenic acid, Docosahexaenoic acid, Eicosapentaenoic acid |
| [35] |
| Vitamins | Vitamin D, Vitamin B12 |
| [36] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Napoli, R.; Balzano, N.; Mascolo, A.; Cimmino, C.; Vitiello, A.; Zovi, A.; Capuano, A.; Boccellino, M. What Is the Role of Nutraceutical Products in Cancer Patients? A Systematic Review of Randomized Clinical Trials. Nutrients 2023, 15, 3249. https://doi.org/10.3390/nu15143249
Di Napoli R, Balzano N, Mascolo A, Cimmino C, Vitiello A, Zovi A, Capuano A, Boccellino M. What Is the Role of Nutraceutical Products in Cancer Patients? A Systematic Review of Randomized Clinical Trials. Nutrients. 2023; 15(14):3249. https://doi.org/10.3390/nu15143249
Chicago/Turabian StyleDi Napoli, Raffaella, Nunzia Balzano, Annamaria Mascolo, Carla Cimmino, Antonio Vitiello, Andrea Zovi, Annalisa Capuano, and Mariarosaria Boccellino. 2023. "What Is the Role of Nutraceutical Products in Cancer Patients? A Systematic Review of Randomized Clinical Trials" Nutrients 15, no. 14: 3249. https://doi.org/10.3390/nu15143249
APA StyleDi Napoli, R., Balzano, N., Mascolo, A., Cimmino, C., Vitiello, A., Zovi, A., Capuano, A., & Boccellino, M. (2023). What Is the Role of Nutraceutical Products in Cancer Patients? A Systematic Review of Randomized Clinical Trials. Nutrients, 15(14), 3249. https://doi.org/10.3390/nu15143249