
Change in Liver Fibrosis Associates with Progress of Diabetic Nephropathy in Patients with Nonalcoholic Fatty Liver Disease


 ,
, (This article belongs to the Section Nutrition and Metabolism)
Abstract
1. Introduction
2. Methods
2.1. Study Design and Patients
2.2. Education Course for Diabetic Nephropathy
2.3. Physical Examination and Biochemical Measurements
2.4. Definitions of Diabetes and Diabetic Nephropathy
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Patients at Baseline According to Baseline DN Category and FIB-4 Index
3.2. Characteristics of the Patients at Baseline According to DN Outcome
3.3. Characteristics of the Patients at 5 Years and Changes in the Parameters of the Groups
3.4. Changes in the Parameters of the Groups
3.5. Changes in ALT Concentrations and the FIB-4 Index
3.6. Factors Associated with the ΔFIB-4 Index
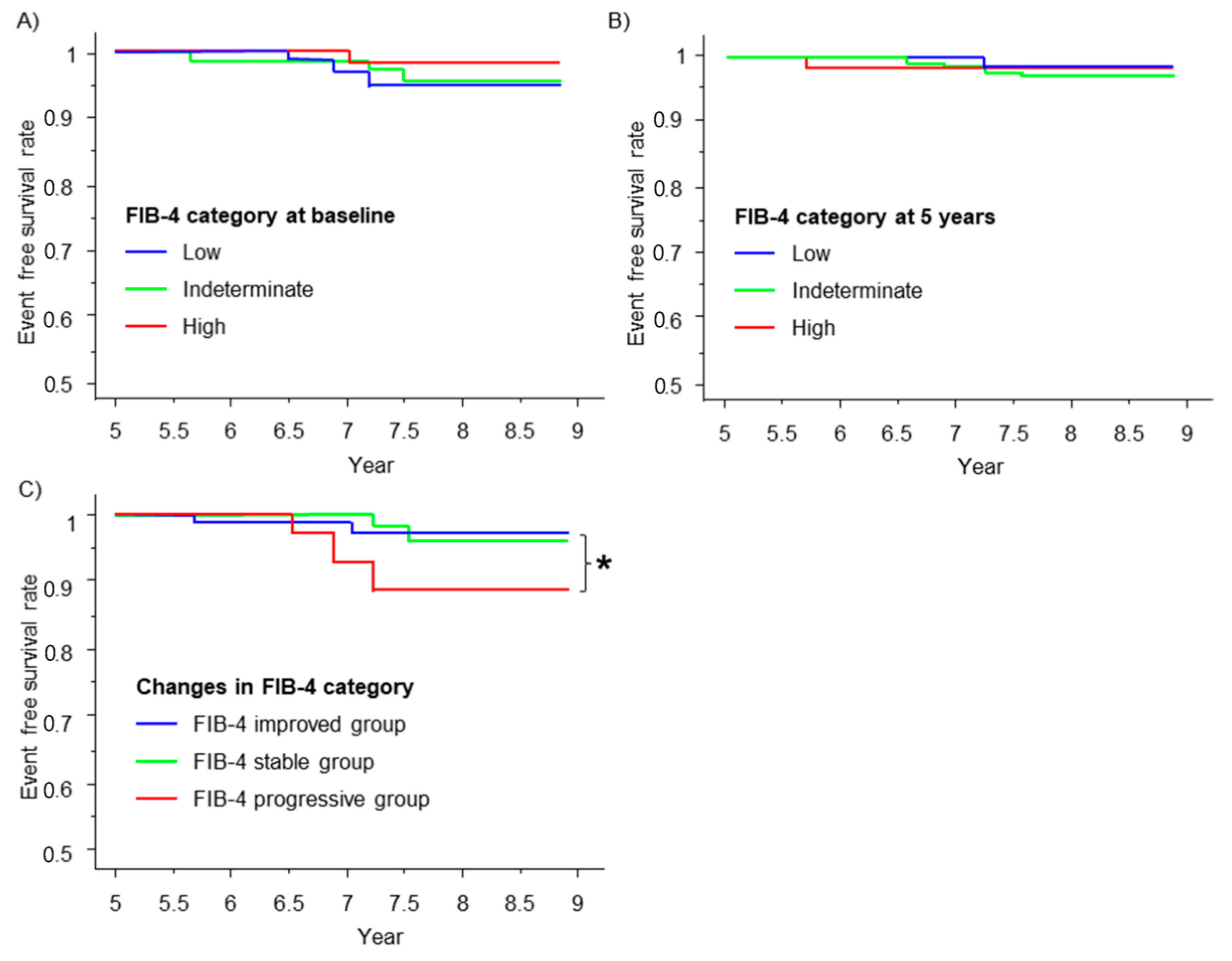
3.7. Renal Outcome and the FIB-4 Index
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- de Boer, I.H.; Khunti, K.; Sadusky, T.; Tuttle, K.R.; Neumiller, J.J.; Rhee, C.M.; Rosas, S.E.; Rossing, P.; Bakris, G. Diabetes Management in Chronic Kidney Disease: A Consensus Report by the American Diabetes Association (ADA) and Kidney Disease: Improving Global Outcomes (KDIGO). Diabetes Care 2022, 45, 3075–3090. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving Global Outcomes Diabetes Work Group. KDIGO 2020 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney Int. 2020, 98, S1–S115. [Google Scholar] [CrossRef] [PubMed]
- Rossing, P.; Caramori, M.L.; Chan, J.C.N.; Heerspink, H.J.L.; Hurst, C.; Khunti, K.; Liew, A.; Michos, E.D.; Navaneethan, S.D.; Olowu, W.A.; et al. Executive summary of the KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease: An update based on rapidly emerging new evidence. Kidney Int. 2022, 102, 990–999. [Google Scholar] [CrossRef] [PubMed]
- Rao Kondapally Seshasai, S.; Kaptoge, S.; Thompson, A.; Di Angelantonio, E.; Gao, P.; Sarwar, N.; Whincup, P.H.; Mukamal, K.J.; Gillum, R.F.; Holme, I.; et al. Diabetes mellitus, fasting glucose, and risk of cause-specific death. N. Engl. J. Med. 2011, 364, 829–841. [Google Scholar] [CrossRef] [PubMed]
- Gregg, E.W.; Li, Y.; Wang, J.; Burrows, N.R.; Ali, M.K.; Rolka, D.; Williams, D.E.; Geiss, L. Changes in diabetes-related complications in the United States, 1990–2010. N. Engl. J. Med. 2014, 370, 1514–1523. [Google Scholar] [CrossRef]
- Wu, B.; Zhang, S.; Lin, H.; Mou, S. Prevention of renal failure in Chinese patients with newly diagnosed type 2 diabetes: A cost-effectiveness analysis. J. Diabetes Investig. 2018, 9, 152–161. [Google Scholar] [CrossRef]
- Gaede, P.; Vedel, P.; Larsen, N.; Jensen, G.V.; Parving, H.H.; Pedersen, O. Multifactorial intervention and cardiovascular disease in patients with type 2 diabetes. N. Engl. J. Med. 2003, 348, 383–393. [Google Scholar] [CrossRef]
- Ueki, K.; Sasako, T.; Okazaki, Y.; Miyake, K.; Nangaku, M.; Ohashi, Y.; Noda, M.; Kadowaki, T.; Group, J.D.S. Multifactorial intervention has a significant effect on diabetic kidney disease in patients with type 2 diabetes. Kidney Int. 2021, 99, 256–266. [Google Scholar] [CrossRef]
- Buades, J.M.; Craver, L.; Del Pino, M.D.; Prieto-Velasco, M.; Ruiz, J.C.; Salgueira, M.; de Sequera, P.; Vega, N. Management of Kidney Failure in Patients with Diabetes Mellitus: What Are the Best Options? J. Clin. Med. 2021, 10, 2943. [Google Scholar] [CrossRef]
- Chen, Y.R.; Yang, Y.; Wang, S.C.; Chiu, P.F.; Chou, W.Y.; Lin, C.Y.; Chang, J.M.; Chen, T.W.; Ferng, S.H.; Lin, C.L. Effectiveness of multidisciplinary care for chronic kidney disease in Taiwan: A 3-year prospective cohort study. Nephrol. Dial. Transpl. 2013, 28, 671–682. [Google Scholar] [CrossRef]
- Imamura, Y.; Takahashi, Y.; Uchida, S.; Iwamoto, M.; Nakamura, R.; Yamauchi, M.; Ogawara, Y.; Goto, M.; Takeba, K.; Yaguchi, N.; et al. Effect of multidisciplinary care of dialysis initiation for outpatients with chronic kidney disease. Int. Urol. Nephrol. 2021, 53, 1435–1444. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.; Tacke, F.; Arrese, M.; Chander Sharma, B.; Mostafa, I.; Bugianesi, E.; Wai-Sun Wong, V.; Yilmaz, Y.; George, J.; Fan, J.; et al. Global Perspectives on Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis. Hepatology 2019, 69, 2672–2682. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Golabi, P.; de Avila, L.; Paik, J.M.; Srishord, M.; Fukui, N.; Qiu, Y.; Burns, L.; Afendy, A.; Nader, F. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis. J. Hepatol. 2019, 71, 793–801. [Google Scholar] [CrossRef] [PubMed]
- Alexopoulos, A.S.; Crowley, M.J.; Wang, Y.; Moylan, C.A.; Guy, C.D.; Henao, R.; Piercy, D.L.; Seymour, K.A.; Sudan, R.; Portenier, D.D.; et al. Glycemic Control Predicts Severity of Hepatocyte Ballooning and Hepatic Fibrosis in Nonalcoholic Fatty Liver Disease. Hepatology 2021, 74, 1220–1233. [Google Scholar] [CrossRef] [PubMed]
- Kramer, J.R.; Natarajan, Y.; Dai, J.; Yu, X.; Li, L.; El-Serag, H.B.; Kanwal, F. Effect of diabetes medications and glycemic control on risk of hepatocellular cancer in patients with nonalcoholic fatty liver disease. Hepatology 2022, 75, 1420–1428. [Google Scholar] [CrossRef]
- Simon, T.G.; Roelstraete, B.; Khalili, H.; Hagstrom, H.; Ludvigsson, J.F. Mortality in biopsy-confirmed nonalcoholic fatty liver disease: Results from a nationwide cohort. Gut 2021, 70, 1375–1382. [Google Scholar] [CrossRef]
- Fujii, H.; Iwaki, M.; Hayashi, H.; Toyoda, H.; Oeda, S.; Hyogo, H.; Kawanaka, M.; Morishita, A.; Munekage, K.; Kawata, K.; et al. Clinical Outcomes in Biopsy-Proven Nonalcoholic Fatty Liver Disease Patients: A Multicenter Registry-based Cohort Study. Clin. Gastroenterol. Hepatol. 2023, 21, 370–379. [Google Scholar] [CrossRef]
- Taylor, R.S.; Taylor, R.J.; Bayliss, S.; Hagstrom, H.; Nasr, P.; Schattenberg, J.M.; Ishigami, M.; Toyoda, H.; Wai-Sun Wong, V.; Peleg, N.; et al. Association between Fibrosis Stage and Outcomes of Patients with Nonalcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. Gastroenterology 2020, 158, 1611–1625.e12. [Google Scholar] [CrossRef]
- Rinella, M.E.; Neuschwander-Tetri, B.A.; Siddiqui, M.S.; Abdelmalek, M.F.; Caldwell, S.; Barb, D.; Kleiner, D.E.; Loomba, R. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology 2023, 77, 1797–1835. [Google Scholar] [CrossRef]
- Byrne, C.D.; Targher, G. NAFLD: A multisystem disease. J. Hepatol. 2015, 62, S47–S64. [Google Scholar] [CrossRef]
- Wang, T.Y.; Wang, R.F.; Bu, Z.Y.; Targher, G.; Byrne, C.D.; Sun, D.Q.; Zheng, M.H. Association of metabolic dysfunction-associated fatty liver disease with kidney disease. Nat. Rev. Nephrol. 2022, 18, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Petracca, G.; Beatrice, G.; Csermely, A.; Lonardo, A.; Schattenberg, J.M.; Tilg, H.; Byrne, C.D.; Targher, G. Non-alcoholic fatty liver disease and risk of incident chronic kidney disease: An updated meta-analysis. Gut 2022, 71, 156–162. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, D.; Kim, H.J.; Lee, C.H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Cho, S.H.; Sung, M.W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef]
- Horio, M.; Imai, E.; Yasuda, Y.; Watanabe, T.; Matsuo, S. Performance of GFR equations in Japanese subjects. Clin. Exp. Nephrol. 2013, 17, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Okamura, T.; Miura, K.; Kadowaki, T.; Ueshima, H.; Nakagawa, H.; Hashimoto, T. A simple method to estimate populational 24-h urinary sodium and potassium excretion using a casual urine specimen. J. Hum. Hypertens. 2002, 16, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD fibrosis score: A noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Definition and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycemia: Report of a WHO/IDF Consultation. Available online: https://www.who.int/publications/i/item/who-ucn-ncd-20.1 (accessed on 17 May 2023).
- Haneda, M.; Utsunomiya, K.; Koya, D.; Babazono, T.; Moriya, T.; Makino, H.; Kimura, K.; Suzuki, Y.; Wada, T.; Ogawa, S.; et al. A new Classification of Diabetic Nephropathy 2014: A report from Joint Committee on Diabetic Nephropathy. J. Diabetes Investig. 2015, 6, 242–246. [Google Scholar] [CrossRef]
- Oshima, M.; Shimizu, M.; Yamanouchi, M.; Toyama, T.; Hara, A.; Furuichi, K.; Wada, T. Trajectories of kidney function in diabetes: A clinicopathological update. Nat. Rev. Nephrol. 2021, 17, 740–750. [Google Scholar] [CrossRef]
- Cusi, K.; Isaacs, S.; Barb, D.; Basu, R.; Caprio, S.; Garvey, W.T.; Kashyap, S.; Mechanick, J.I.; Mouzaki, M.; Nadolsky, K.; et al. American Association of Clinical Endocrinology Clinical Practice Guideline for the Diagnosis and Management of Nonalcoholic Fatty Liver Disease in Primary Care and Endocrinology Clinical Settings: Co-Sponsored by the American Association for the Study of Liver Diseases (AASLD). Endocr. Pract. 2022, 28, 528–562. [Google Scholar] [CrossRef]
- Tokushige, K.; Ikejima, K.; Ono, M.; Eguchi, Y.; Kamada, Y.; Itoh, Y.; Akuta, N.; Yoneda, M.; Iwasa, M.; Yoneda, M.; et al. Evidence-based clinical practice guidelines for nonalcoholic fatty liver disease/nonalcoholic steatohepatitis 2020. J. Gastroenterol. 2021, 56, 951–963. [Google Scholar] [CrossRef]
- Simon, T.G.; Roelstraete, B.; Hagstrom, H.; Sundstrom, J.; Ludvigsson, J.F. Non-alcoholic fatty liver disease and incident major adverse cardiovascular events: Results from a nationwide histology cohort. Gut 2022, 71, 1867–1875. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Nascimbeni, F.; Mantovani, A.; Targher, G. Hypertension, diabetes, atherosclerosis and NASH: Cause or consequence? J. Hepatol. 2018, 68, 335–352. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Bertolini, L.; Rodella, S.; Zoppini, G.; Lippi, G.; Day, C.; Muggeo, M. Non-alcoholic fatty liver disease is independently associated with an increased prevalence of chronic kidney disease and proliferative/laser-treated retinopathy in type 2 diabetic patients. Diabetologia 2008, 51, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.T.; Cho, Y.K.; Yun, J.W.; Park, J.H.; Kim, H.J.; Park, D.I.; Sohn, C.I.; Jeon, W.K.; Kim, B.I.; Rhee, E.J.; et al. Impact of non-alcoholic fatty liver disease on microalbuminuria in patients with prediabetes and diabetes. Intern. Med. J. 2010, 40, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.Y.; Jung, C.H.; Mok, J.O.; Kang, S.K.; Kim, C.H. Prevalences of diabetic retinopathy and nephropathy are lower in Korean type 2 diabetic patients with non-alcoholic fatty liver disease. J. Diabetes Investig. 2014, 5, 170–175. [Google Scholar] [CrossRef]
- Jenks, S.J.; Conway, B.R.; Hor, T.J.; Williamson, R.M.; McLachlan, S.; Robertson, C.; Morling, J.R.; Strachan, M.W.; Price, J.F. Hepatic steatosis and non-alcoholic fatty liver disease are not associated with decline in renal function in people with Type 2 diabetes. Diabet. Med. 2014, 31, 1039–1046. [Google Scholar] [CrossRef]
- Yeung, M.W.; Wong, G.L.; Choi, K.C.; Luk, A.O.; Kwok, R.; Shu, S.S.; Chan, A.W.; Lau, E.S.H.; Ma, R.C.W.; Chan, H.L.; et al. Advanced liver fibrosis but not steatosis is independently associated with albuminuria in Chinese patients with type 2 diabetes. J. Hepatol. 2017, 68, 147–156. [Google Scholar] [CrossRef]
- Saito, H.; Tanabe, H.; Kudo, A.; Machii, N.; Higa, M.; Yamaguchi, S.; Maimaituxun, G.; Abe, K.; Takahashi, A.; Tanaka, K.; et al. High FIB4 index is an independent risk factor of diabetic kidney disease in type 2 diabetes. Sci. Rep. 2021, 11, 11753. [Google Scholar] [CrossRef]
- Goh, G.B.; Pagadala, M.R.; Dasarathy, J.; Unalp-Arida, A.; Sargent, R.; Hawkins, C.; Sourianarayanane, A.; Khiyami, A.; Yerian, L.; Pai, R.; et al. Renin-angiotensin system and fibrosis in non-alcoholic fatty liver disease. Liver Int. 2015, 35, 979–985. [Google Scholar] [CrossRef]
- Armstrong, M.J.; Adams, L.A.; Canbay, A.; Syn, W.K. Extrahepatic complications of nonalcoholic fatty liver disease. Hepatology 2014, 59, 1174–1197. [Google Scholar] [CrossRef]
- Zhou, S.; Su, L.; Xu, R.; Li, Y.; Chen, R.; Cao, Y.; Gao, P.; Zhang, X.; Luo, F.; Gao, Q.; et al. Statin initiation and risk of incident kidney disease in patients with diabetes. CMAJ 2023, 195, E729–E738. [Google Scholar] [CrossRef] [PubMed]
- Kuwashiro, T.; Takahashi, H.; Hyogo, H.; Ogawa, Y.; Imajo, K.; Yoneda, M.; Nakahara, T.; Oeda, S.; Tanaka, K.; Amano, Y.; et al. Discordant pathological diagnosis of non-alcoholic fatty liver disease: A prospective multicenter study. JGH Open 2020, 4, 497–502. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| DN Category | ||
|---|---|---|
| Category 2 n = 127 | Category 3 n = 62 | |
| Age, years | 64 (52–76) | 63 (53–73) |
| Female, n (%) | 40 (31.5) | 20 (32.3) |
| Body weight, kg | 65.7 (51.4–80) | 68.9 (56.1–81.7) |
| BMI, kg/m2 | 25.7 (21.8–29.6) | 26 (21.1–30.9) |
| Systolic blood pressure, mmHg | 133 (113–153) | 137 (123–150) |
| Diastolic blood pressure, mmHg | 78 (66–90) | 77 (57–97) |
| Hypertension, n (%) | 68 (53.5) * | 46 (74.2) |
| Dyslipidemia, n (%) | 43 (33.9) | 17 (27.4) |
| HbA1c, % | 7 (5.6–8.4) * | 7.5 (6.3–8.8) |
| Creatinine, mg/dL | 0.84 (0.53–1.15) ** | 1.03 (0.59–1.47) |
| eGFR, mL/min/1.73 m2 | 67.1 (43.1–91.1) ** | 52 (30.5–73.5) |
| CKD stage G1/G2/G3a/G3b, n (%) | 15/67/37/8 (11.8/52.8/29.1/6.3) ** | 4/21/13/24 (6.5/33.9/21/38.7) |
| U-Alb/U-Cre, mg/g | 79.4 (42.0–116.8) | - |
| U-Pro/U-Cre, mg/g | - | 1.3 (0.7–0.9) |
| Estimated salt intake, g/day | 10.6 (7.3–13.9) | 10.9 (8.2–13.6) |
| AST, U/L | 22 (13–31) | 20 (11–29) |
| ALT, U/L | 24 (7–41) * | 20 (8–32) |
| Platelet count, ×103/µL | 221 (157–285) | 224 (139–309) |
| FIB-4 index | 1.27 (0.52–2.01) | 1.24 (0.42–2.06) |
| SGLT2 inhibitor, n (%) | 0 | 0 |
| GLP-1 agonist, n (%) | 11 (8.7) | 5 (8.1) |
| DPP-4 inhibitor, n (%) | 61 (48) | 35 (56.5) |
| Pioglitazone, n (%) | 10 (7.9) | 2 (3.2) |
| Insulin injection, n (%) | 47 (37) * | 34 (54.8) |
| DN Outcome | |||
|---|---|---|---|
| Improved Group n = 37 | Stable Group n = 95 | Progressive Group n = 57 | |
| Age, years | 65 (53—78) | 64 (51–77) | 64 (54–75) |
| Female, n (%) | 14 (37.8) | 31 (32.6) | 16 (28.1) |
| Body weight, kg | 66.7 (49.2–84.2) | 66.2 (51.7–80.7) | 67 (53.2–80.8) |
| BMI, kg/m2 | 26.9 (22.9–30.9) | 25.7 (22.1–29.3) | 25.5 (21.0–29.9) |
| Systolic blood pressure, mmHg | 136 (114–158) | 132 (116–148) | 136 (118–154) |
| Diastolic blood pressure, mmHg | 79 (65–93) | 75 (60–90) | 76 (64–88) |
| Hypertension, n (%) | 23 (62.2) | 56 (58.9) | 43 (75.4) |
| Dyslipidemia, n (%) | 17 (45.9) * | 31 (32.6) | 12 (21.1) |
| HbA1c, % | 7.3 (6.0–8.6) | 7.2 (5.9–8.6) | 7.1 (5.7–8.5) |
| Creatinine, mg/dL (AA) | 0.78 (0.49–1.07) ** | 0.85 (0.56–1.14) ** | 1.04 (0.62–1.46) |
| eGFR, mL/min/1.73m2 (AA) | 73 (52.8–93.3) ** | 64 (40.8–87.3) ** | 51.5 (26.5–76.5) |
| U-Alb/U-Cre, mg/g | 66.4 (40.9–91.9) ** | 78.1 (33.8–122.4) * | 112.7 (43.0–182.4) |
| U-Pro/U-Cre, mg/g (AA) | 0.7 (0.3–1.1) * | 1.2 (0.68–1.73) ** | 2.4 (0.88–3.93) |
| DN category, category 2/category 3, (%) | 29/8 (78.4/21.6) | 62/33 (65.3/34.7) | 36/21 (64.2/36.8) |
| Estimated salt intake, g/day | 11.6 (8.6–14.6) | 10.5 (7.6–13.4) | 10.7 (7.3–14.1) |
| AST, U/L | 21 (12–31) | 22 (14–30) | 19 (10–28) |
| ALT, U/L | 18 (13–41) | 24 (11–38) | 21 (8–34) |
| Platelet count, ×103/µL | 229 (150–310) | 221 (159–284) | 223 (151–295) |
| FIB-4 index | 1.23 (0.58–1.89) | 1.27 (0.41–2.12) | 1.24 (0.54–1.93) |
| SGLT2 inhibitor, n (%) | 0 (0) | 0 (0) | 0 (0) |
| GLP-1 agonist, n (%) | 2 (5.4) | 7 (7.4) | 7 (12.3) |
| DPP-4 inhibitor, n (%) | 17 (45.9) | 54 (56.8) | 25 (43.9) |
| Pioglitazone, n (%) | 4 (10.8) | 4 (4.2) | 4 (7.0) |
| Insulin injection, n (%) | 10 (27.0) * | 39 (41.1) | 32 (56.1) |
| DN Outcome | |||
|---|---|---|---|
| Improved Group n = 37 | Stable Group n = 95 | Progressive Group n = 57 | |
| Body weight, kg | 65.9 (51.3–80.6) § | 66.8 (51.5–82.1) | 69.1 (54.4–83.8) § |
| BMI, kg/m2 | 25.4 (20.8–30.0) § | 25.5 (20.7–30.2) | 25.225 (20.2–30.2) |
| Systolic blood pressure, mmHg | 131 (107–155) * | 135 (113–157) | 139 (117–162) |
| Diastolic blood pressure, mmHg | 72 (59–85) § | 75 (58–92) | 77 (61–94) |
| HbA1c, % | 6.9 (6.0–7.9) § | 7.1 (6.1–8.2) | 7.2 (6.2–8.3) |
| eGFR, mL/min/1.73m2 (AA) | 63 (30.8–95.3) §§ | 60 (34–86) §§ | 41 (9–73) §§ |
| U-Alb/U-Cre, mg/g (AA) | 18.5 (7.8–29.2) **§§ | 119 (8.2–229.8) ** | 475.9 (197.8–754) §§ |
| U-Pro/U-Cre, mg/g (A) | 0.4 (0.275–0.525) *§ | 3.45 (1.25–8.15) §§ | 2.45 (1.35–8.25) § |
| DN category, 1/2/3/4/5 | 29/8/0/0/0 | 0/62/33/0/0 | 0/0/32/21/4 |
| Estimated salt intake, g/day | 10 (7.4–12.6) § | 10.7 (7.0–14.4) | 9.5 (5.4–13.6) |
| AST, U/L (A) | 19 (12–26) § | 21.5 (13–31) | 20 (13–27) |
| ALT, U/L (A) | 19 (10–28) †§ | 21 (6–36) | 17 (4–30) § |
| Platelet count, ×103/µL | 221 (140–302) | 209 (137–281) | 219 (151–287) |
| FIB-4 index | 1.30 (0.45–2.14) | 1.48 (0.63–2.32) § | 1.57 (0.73–2.42) § |
| Explanatory Variable | Partial Regression Coefficient (×10−3) | t Value | p Value | 95% C.I | |
|---|---|---|---|---|---|
| Univariate | |||||
| % change in albuminuria and proteinuria | 0.35 | 2.84 | 0.005 | 0.0001–0.001 | |
| Δ-eGFR | −1.0 | −0.45 | 0.656 | −0.007–0.004 | |
| Δ-HbA1c | 54.0 | 1.43 | 0.154 | −0.021–0.129 | |
| Δ-Salt intake | −7.0 | −0.72 | 0.47 | −0.027–0.013 | |
| Δ-BMI | 1.0 | 0.05 | 0.958 | −0.047–0.05 | |
| Δ-Systolic blood pressure | 4.0 | 2.08 | 0.039 | 0.0002–0.008 | |
| Δ-Diastolic blood pressure | 4.0 | 1.43 | 0.15 | −0.002–0.011 | |
| Multivariate | |||||
| % change in albuminuria and proteinuria | 0.31 | 2.409 | 0.017 | 0.0001–0.001 | |
| Δ-Systolic blood pressure | 2.0 | 1.167 | 0.245 | −0.002–0.007 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terasaka, Y.; Takahashi, H.; Amano, K.; Fujisaki, K.; Kita, S.; Kato, K.; Nakayama, K.; Yamashita, Y.; Nakamura, S.; Anzai, K. Change in Liver Fibrosis Associates with Progress of Diabetic Nephropathy in Patients with Nonalcoholic Fatty Liver Disease. Nutrients 2023, 15, 3248. https://doi.org/10.3390/nu15143248
Terasaka Y, Takahashi H, Amano K, Fujisaki K, Kita S, Kato K, Nakayama K, Yamashita Y, Nakamura S, Anzai K. Change in Liver Fibrosis Associates with Progress of Diabetic Nephropathy in Patients with Nonalcoholic Fatty Liver Disease. Nutrients. 2023; 15(14):3248. https://doi.org/10.3390/nu15143248
Chicago/Turabian StyleTerasaka, Yoshiko, Hirokazu Takahashi, Kazushi Amano, Koshiro Fujisaki, Shotaro Kita, Kaori Kato, Koujin Nakayama, Yuko Yamashita, Shuji Nakamura, and Keizo Anzai. 2023. "Change in Liver Fibrosis Associates with Progress of Diabetic Nephropathy in Patients with Nonalcoholic Fatty Liver Disease" Nutrients 15, no. 14: 3248. https://doi.org/10.3390/nu15143248
APA StyleTerasaka, Y., Takahashi, H., Amano, K., Fujisaki, K., Kita, S., Kato, K., Nakayama, K., Yamashita, Y., Nakamura, S., & Anzai, K. (2023). Change in Liver Fibrosis Associates with Progress of Diabetic Nephropathy in Patients with Nonalcoholic Fatty Liver Disease. Nutrients, 15(14), 3248. https://doi.org/10.3390/nu15143248