
Phosphate Control in Peritoneal Dialysis Patients: Issues, Solutions, and Open Questions
 ,
,  , and
, and 
Abstract
1. Introduction
2. Effects of Phosphate Burden and Pathophysiology of CKD-MBD
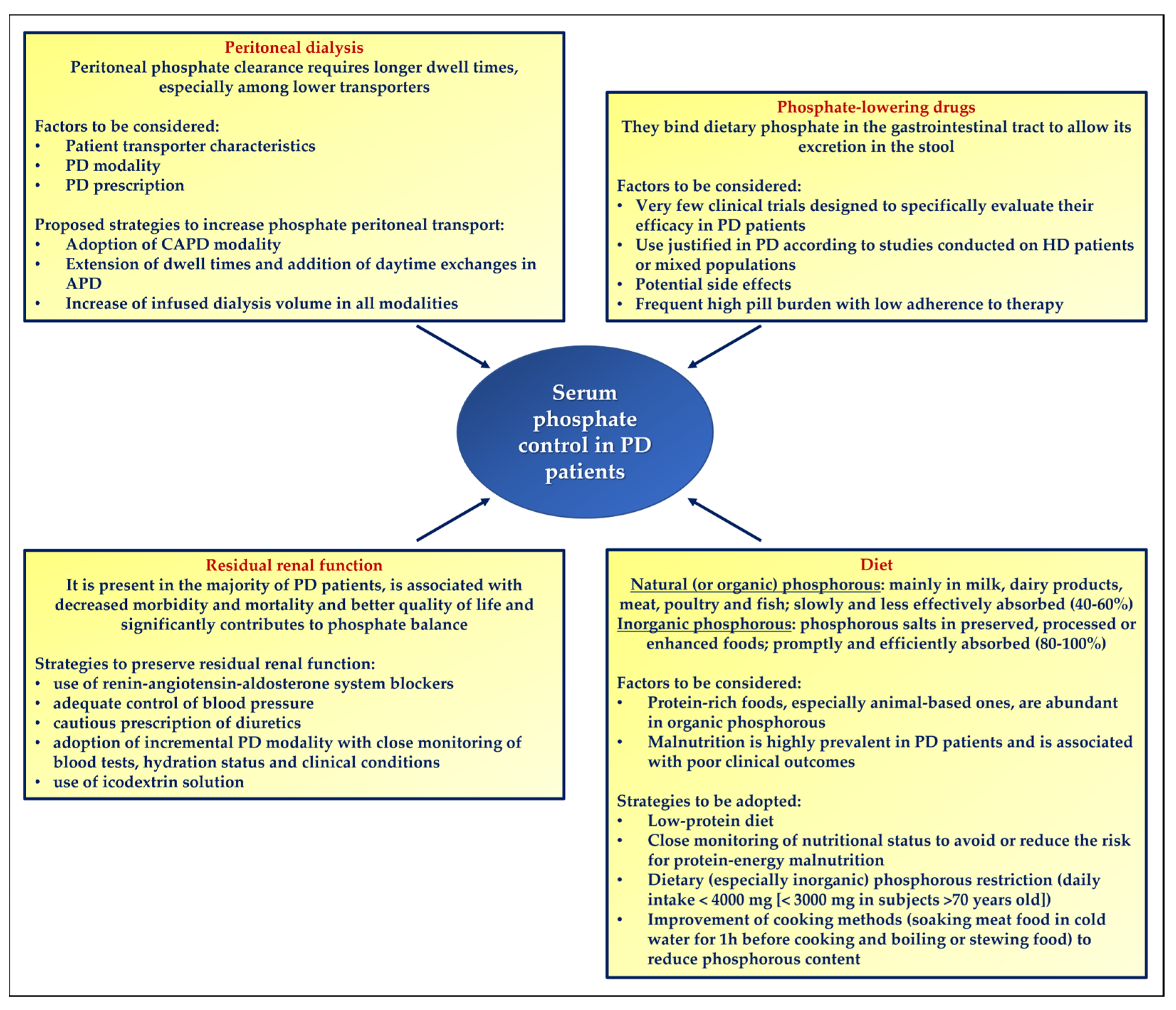
3. Phosphate Removal by Peritoneal Dialysis
4. Phosphate Binders in Peritoneal Dialysis Patients: Results from Clinical Trials
5. Dietary Recommendations to Manage Hyperphosphatemia in Peritoneal Dialysis Patients
6. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.D. Global Prevalence of Chronic Kidney Disease—A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef] [PubMed]
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef]
- Merchant, R.A.; Vathsala, A. Healthy aging and chronic kidney disease. Kidney Res. Clin. Pract. 2022, 41, 644–656. [Google Scholar] [CrossRef] [PubMed]
- Moe, S.; Drüeke, T.; Cunningham, J.; Goodman, W.; Martin, K.; Olgaard, K.; Ott, S.; Sprague, S.; Lameire, N.; Eknoyan, G.; et al. Definition, evaluation, and classification of renal osteodystrophy: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2006, 69, 1945–1953. [Google Scholar] [CrossRef]
- Stevens, K.K.; Denby, L.; Patel, R.K.; Mark, P.B.; Kettlewell, S.; Smith, G.L.; Clancy, M.J.; Delles, C.; Jardine, A.G. Deleterious effects of phosphate on vascular and endothelial function via disruption to the nitric oxide pathway. Nephrol. Dial. Transplant. 2017, 32, 1617–1627. [Google Scholar] [CrossRef]
- Shanahan, C.M.; Crouthamel, M.H.; Kapustin, A.; Giachelli, C.M. Arterial calcification in chronic kidney disease: Key roles for calcium and phosphate. Circ. Res. 2011, 109, 697–711. [Google Scholar] [CrossRef]
- Ix, J.H.; De Boer, I.H.; Peralta, C.A.; Adeney, K.L.; Duprez, D.A.; Jenny, N.S.; Siscovick, D.S.; Kestenbaum, B.R. Serum phosphorus concentrations and arterial stiffness among individuals with normal kidney function to moderate kidney disease in MESA. Clin. J. Am. Soc. Nephrol. 2009, 4, 609–615. [Google Scholar] [CrossRef]
- Petchey, W.G.; Hawley, C.M.; Johnson, D.W.; Haluska, B.A.; Watkins, T.W.; Isbel, N.M. Multimodality vascular imaging in CKD: Divergence of risk between measured parameters. Nephrol. Dial. Transplant. 2012, 27, 1004–1012. [Google Scholar] [CrossRef]
- Ishimura, E.; Okuno, S.; Taniwaki, H.; Kizu, A.; Tsuchida, T.; Shioi, A.; Shoji, T.; Tabata, T.; Inaba, M.; Nishizawa, Y. Different risk factors for vascular calcification in end-stage renal disease between diabetics and nondiabetics: The respective importance of glycemic and phosphate control. Kidney Blood Press. Res. 2008, 31, 10–15. [Google Scholar] [CrossRef]
- Ishimura, E.; Okuno, S.; Kitatani, K.; Kim, M.; Shoji, T.; Nakatani, T.; Inaba, M.; Nishizawa, Y. Different risk factors for peripheral vascular calcification between diabetic and non-diabetic haemodialysis patients—Importance of glycaemic control. Diabetologia 2002, 45, 1446–1448. [Google Scholar]
- Amnuay, K.; Srisawat, N.; Wudhikarn, K.; Assanasen, T.; Polprasert, C. Factors associated with erythropoiesis-stimulating agent hyporesponsiveness anemia in chronic kidney disease patients. Hematol. Rep. 2019, 11, 8183. [Google Scholar] [CrossRef]
- Czaya, B.; Heitman, K.; Campos, I.; Yanucil, C.; Kentrup, D.; Westbrook, D.; Gutierrez, O.; Babitt, J.L.; Jung, G.; Salusky, I.B.; et al. Hyperphosphatemia increases inflammation to exacerbate anemia and skeletal muscle wasting independently of FGF23-FGFR4 signaling. Elife 2022, 11, e74782. [Google Scholar] [CrossRef] [PubMed]
- Beto, J.; Bhatt, N.; Gerbeling, T.; Patel, C.; Drayer, D. Overview of the 2017 KDIGO CKD-MBD Update: Practice Implications for Adult Hemodialysis Patients. J Ren Nutr 2019, 29, 2–15. [Google Scholar] [CrossRef] [PubMed]
- Neyra, J.A.; Hu, M.C.; Moe, O.W. Klotho in Clinical Nephrology: Diagnostic and Therapeutic Implications. Clin. J. Am. Soc. Nephrol. 2020, 16, 162–176. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Napoletano, A.; Provenzano, M.; Garofalo, C.; Bini, C.; Comai, G.; La Manna, G. Mineral Bone Disorders in Kidney Disease Patients: The Ever-Current Topic. Int. J. Mol. Sci. 2022, 23, 12223. [Google Scholar] [CrossRef]
- Tsujikawa, H.; Kurotaki, Y.; Fujimori, T.; Fukuda, K.; Nabeshima, Y. Klotho, a gene related to a syndrome resembling human premature aging, functions in a negative regulatory circuit of vitamin D endocrine system. Mol. Endocrinol. 2003, 17, 2393–2403. [Google Scholar] [CrossRef]
- Galitzer, H.; Ben-Dov, I.Z.; Silver, J.; Naveh-Many, T. Parathyroid cell resistance to fibroblast growth factor 23 in secondary hyperparathyroidism of chronic kidney disease. Kidney Int. 2010, 77, 211–218. [Google Scholar] [CrossRef]
- Yamada, S.; Giachelli, C.M. Vascular calcification in CKD-MBD: Roles for phosphate, FGF23, and Klotho. Bone 2017, 100, 87–93. [Google Scholar] [CrossRef]
- Paloian, N.J.; Giachelli, C.M. A current understanding of vascular calcification in CKD. Am. J. Physiol. Renal Physiol. 2014, 307, F891–F900. [Google Scholar] [CrossRef]
- Li, X.; Yang, H.Y.; Giachelli, C.M. Role of the sodium-dependent phosphate cotransporter, Pit-1, in vascular smooth muscle cell calcification. Circ. Res. 2006, 98, 905–912. [Google Scholar] [CrossRef] [PubMed]
- Crouthamel, M.H.; Lau, W.L.; Leaf, E.M.; Chavkin, N.W.; Wallingford, M.C.; Peterson, D.F.; Li, X.; Liu, Y.; Chin, M.T.; Levi, M.; et al. Sodium-dependent phosphate cotransporters and phosphate-induced calcification of vascular smooth muscle cells: Redundant roles for PiT-1 and PiT-2. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 2625–2632. [Google Scholar] [CrossRef] [PubMed]
- Kendrick, J.; Chonchol, M. The role of phosphorus in the development and progression of vascular calcification. Am. J. Kidney Dis. 2011, 58, 826–834. [Google Scholar] [CrossRef]
- Hu, M.C.; Shi, M.; Zhang, J.; Quiñones, H.; Griffith, C.; Kuro-o, M.; Moe, O.W. Klotho deficiency causes vascular calcification in chronic kidney disease. J. Am. Soc. Nephrol. 2011, 22, 124–136. [Google Scholar] [CrossRef] [PubMed]
- de la Guía-Galipienso, F.; Martínez-Ferran, M.; Vallecillo, N.; Lavie, C.J.; Sanchis-Gomar, F.; Pareja-Galeano, H. Vitamin D and cardiovascular health. Clin. Nutr. 2021, 40, 2946–2957. [Google Scholar] [CrossRef]
- Wong, B.; Ravani, P.; Oliver, M.J.; Holroyd-Leduc, J.; Venturato, L.; Garg, A.X.; Quinn, R.R. Comparison of Patient Survival Between Hemodialysis and Peritoneal Dialysis Among Patients Eligible for Both Modalities. Am. J. Kidney Dis. 2018, 71, 344–351. [Google Scholar] [CrossRef]
- Himmelfarb, J.; Vanholder, R.; Mehrotra, R.; Tonelli, M. The current and future landscape of dialysis. Nat. Rev. Nephrol. 2020, 16, 573–585. [Google Scholar] [CrossRef]
- Jansen, M.A.; Hart, A.A.; Korevaar, J.C.; Dekker, F.W.; Boeschoten, E.W.; Krediet, R.T.; NECOSAD Study Group. Predictors of the rate of decline of residual renal function in incident dialysis patients. Kidney Int. 2002, 62, 1046–1053. [Google Scholar] [CrossRef]
- Tanriover, C.; Ucku, D.; Basile, C.; Tuttle, K.R.; Kanbay, M. On the importance of the interplay of residual renal function with clinical outcomes in end-stage kidney disease. J. Nephrol. 2022, 35, 2191–2204. [Google Scholar] [CrossRef]
- Rippe, B.; Venturoli, D.; Simonsen, O.; de Arteaga, J. Fluid and electrolyte transport across the peritoneal membrane during CAPD according to the three-pore model. Perit. Dial. Int. 2004, 24, 10–27. [Google Scholar] [CrossRef]
- Bammens, B. Urea and uremic solutes: How does peritoneal dialysis work? Semin. Nephrol. 2011, 31, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Khanna, R. Solute and Water Transport in Peritoneal Dialysis: A Case-Based Primer. Am. J. Kidney Dis. 2017, 69, 461–472. [Google Scholar] [CrossRef] [PubMed]
- Devuyst, O.; Rippe, B. Water transport across the peritoneal membrane. Kidney Int. 2014, 85, 750–758. [Google Scholar] [CrossRef]
- Perl, J.; Bargman, J.M. Peritoneal dialysis: From bench to bedside and bedside to bench. Am. J. Physiol. Renal Physiol. 2016, 311, F999–F1004. [Google Scholar] [CrossRef] [PubMed]
- Courivaud, C.; Davenport, A. Phosphate Removal by Peritoneal Dialysis: The Effect of Transporter Status and Peritoneal Dialysis Prescription. Perit. Dial. Int. 2016, 36, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Bammens, B.; Evenepoel, P.; Verbeke, K.; Vanrenterghem, Y. Time profiles of peritoneal and renal clearances of different uremic solutes in incident peritoneal dialysis patients. Am. J. Kidney Dis. 2005, 46, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Bammens, B.; Evenepoel, P.; Verbeke, K.; Vanrenterghem, Y. Removal of middle molecules and protein-bound solutes by peritoneal dialysis and relation with uremic symptoms. Kidney Int. 2003, 64, 2238–2243. [Google Scholar] [CrossRef]
- Kuhlmann, M.K. Phosphate elimination in modalities of hemodialysis and peritoneal dialysis. Blood Purif. 2010, 29, 137–144. [Google Scholar] [CrossRef]
- Noordzij, M.; Korevaar, J.C.; Boeschoten, E.W.; Dekker, F.W.; Bos, W.J.; Krediet, R.T. Hyperphosphataemia and related mortality. Nephrol. Dial. Transplant. 2006, 21, 2676–2677. [Google Scholar] [CrossRef]
- Noordzij, M.; Korevaar, J.C.; Boeschoten, E.W.; Dekker, F.W.; Bos, W.J.; Krediet, R.T.; Netherlands Cooperative Study on the Adequacy of Dialysis (NECOSAD) Study Group. The Kidney Disease Outcomes Quality Initiative (K/DOQI) Guideline for Bone Metabolism and Disease in CKD: Association with mortality in dialysis patients. Am. J. Kidney Dis. 2005, 46, 925–932. [Google Scholar] [CrossRef]
- Debowska, M.; Gomez, R.; Pinto, J.; Waniewski, J.; Lindholm, B. Phosphate clearance in peritoneal dialysis. Sci. Rep. 2020, 10, 17504. [Google Scholar] [CrossRef]
- Peruzzo, D.; Guedes, M.; Larkin, J.W.; Yokoyama, G.; Dos Santos, T.L.; Pecoits-Filho, R.; Ribeiro, S.C.; Ramos, A.; Barretti, P.; de Moraes, T.P.; et al. Peritoneal dialysis modality transition and impact on phosphate and potassium serum levels. PLoS ONE 2021, 16, e0257140. [Google Scholar] [CrossRef] [PubMed]
- Domenici, A.; Giuliani, A.; Sivo, F.; Falcone, C.; Punzo, G.; Menè, P. Cross-Over Efficiency Comparison of Different Tidal Automated Peritoneal Dialysis Schedules. Blood Purif. 2016, 42, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Badve, S.V.; Zimmerman, D.L.; Knoll, G.A.; Burns, K.D.; McCormick, B.B. Peritoneal phosphate clearance is influenced by peritoneal dialysis modality, independent of peritoneal transport characteristics. Clin. J. Am. Soc. Nephrol. 2008, 3, 1711–1717. [Google Scholar] [CrossRef] [PubMed]
- Tsuchiya, K.; Akihisa, T. The Importance of Phosphate Control in Chronic Kidney Disease. Nutrients 2021, 13, 1670. [Google Scholar] [CrossRef]
- Pergola, P.E. Phosphate Frustration: Treatment Options to Complement Current Therapies. Int. J. Nephrol. 2022, 2022, 9457440. [Google Scholar] [CrossRef]
- Cernaro, V.; Santoro, D.; Lucisano, S.; Nicocia, G.; Lacquaniti, A.; Buemi, M. The future of phosphate binders: A perspective on novel therapeutics. Expert. Opin. Investig. Drugs 2014, 23, 1459–1463. [Google Scholar] [CrossRef]
- Locatelli, F.; Del Vecchio, L.; Violo, L.; Pontoriero, G. Phosphate binders for the treatment of hyperphosphatemia in chronic kidney disease patients on dialysis: A comparison of safety profiles. Expert. Opin. Drug Saf. 2014, 13, 551–561. [Google Scholar] [CrossRef]
- Russo, D.; Bellasi, A.; Pota, A.; Russo, L.; Di Iorio, B. Effects of phosphorus-restricted diet and phosphate-binding therapy on outcomes in patients with chronic kidney disease. J. Nephrol. 2015, 28, 73–80. [Google Scholar] [CrossRef]
- Di Iorio, B.; Bellasi, A.; Russo, D.; Independent Study Investigators. Mortality in kidney disease patients treated with phosphate binders: A randomized study. Clin. J. Am. Soc. Nephrol. 2012, 7, 487–493. [Google Scholar] [CrossRef]
- Bellinghieri, G.; Santoro, D.; Savica, V. Emerging drugs for hyperphosphatemia. Expert. Opin. Emerg. Drugs 2007, 12, 355–365. [Google Scholar] [CrossRef]
- Cernaro, V.; Santoro, D.; Lacquaniti, A.; Costantino, G.; Visconti, L.; Buemi, A.; Buemi, M. Phosphate binders for the treatment of chronic kidney disease: Role of iron oxyhydroxide. Int. J. Nephrol. Renovasc. Dis. 2016, 9, 11–19. [Google Scholar] [CrossRef]
- Van Buren, P.N.; Lewis, J.B.; Dwyer, J.P.; Greene, T.; Middleton, J.; Sika, M.; Umanath, K.; Abraham, J.D.; Arfeen, S.S.; Bowline, I.G.; et al. The Phosphate Binder Ferric Citrate and Mineral Metabolism and Inflammatory Markers in Maintenance Dialysis Patients: Results From Prespecified Analyses of a Randomized Clinical Trial. Am. J. Kidney Dis. 2015, 66, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.B.; Sika, M.; Koury, M.J.; Chuang, P.; Schulman, G.; Smith, M.T.; Whittier, F.C.; Linfert, D.R.; Galphin, C.M.; Athreya, B.P.; et al. Ferric citrate controls phosphorus and delivers iron in patients on dialysis. J. Am. Soc. Nephrol. 2015, 26, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Floege, J.; Covic, A.C.; Ketteler, M.; Rastogi, A.; Chong, E.M.; Gaillard, S.; Lisk, L.J.; Sprague, S.M.; PA21 Study Group. A phase III study of the efficacy and safety of a novel iron-based phosphate binder in dialysis patients. Kidney Int. 2014, 86, 638–647. [Google Scholar] [CrossRef] [PubMed]
- Shima, H.; Miya, K.; Okada, K.; Minakuchi, J.; Kawashima, S. Sucroferric oxyhydroxide decreases serum phosphorus level and fibroblast growth factor 23 and improves renal anemia in hemodialysis patients. BMC Res. Notes 2018, 11, 363. [Google Scholar] [CrossRef] [PubMed]
- Lioulios, G.; Stangou, M.; Sarafidis, P.A.; Tsouchnikas, I.; Minasidis, I.; Vainas, A.; Faitatzidou, D.; Sampani, E.; Papagianni, A. Chronic Therapy with Sucroferric Oxyhydroxide Does Not Affect Iron and Anemia Markers in Dialysis Patients. Blood Purif. 2020, 49, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Di Iorio, B.; Molony, D.; Bell, C.; Cucciniello, E.; Bellizzi, V.; Russo, D.; Bellasi, A.; Independent Study Investigators. Sevelamer versus calcium carbonate in incident hemodialysis patients: Results of an open-label 24-month randomized clinical trial. Am. J. Kidney Dis. 2013, 62, 771–778. [Google Scholar] [CrossRef]
- Xu, J.P.; Zeng, R.X.; Liao, P.D.; Zhang, M.Z. Effect of lanthanum carbonate on the progression of coronary artery calcification in hemodialysis patients: A meta-analysis of randomized controlled trials. Hemodial. Int. 2022, 26, 223–233. [Google Scholar] [CrossRef]
- Yokoyama, K.; Hashimoto, T.; Okuda, Y.; Matsumoto, Y.; Ito, K.; Yamada, R.; Susai, H.; Nishino, N. Safety and effectiveness of ferric citrate hydrate in serum phosphorus management of patients with chronic kidney disease: A long-term, real-world, observational, post-marketing surveillance study. Clin. Exp. Nephrol. 2022, 26, 688–699. [Google Scholar] [CrossRef]
- Katopodis, K.P.; Andrikos, E.K.; Gouva, C.D.; Bairaktari, E.T.; Nikolopoulos, P.M.; Takouli, L.K.; Tzallas, C.S.; Elisaf, M.S.; Pappas, M.V.; Siamopoulos, K.C. Sevelamer hydrochloride versus aluminum hydroxide: Effect on serum phosphorus and lipids in CAPD patients. Perit. Dial. Int. 2006, 26, 320–327. [Google Scholar] [CrossRef]
- Evenepoel, P.; Selgas, R.; Caputo, F.; Foggensteiner, L.; Heaf, J.G.; Ortiz, A.; Kelly, A.; Chasan-Taber, S.; Duggal, A.; Fan, S. Efficacy and safety of sevelamer hydrochloride and calcium acetate in patients on peritoneal dialysis. Nephrol. Dial. Transplant. 2009, 24, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Floege, J.; Covic, A.C.; Ketteler, M.; Mann, J.; Rastogi, A.; Spinowitz, B.; Rakov, V.; Lisk, L.J.; Sprague, S.M. One-year efficacy and safety of the iron-based phosphate binder sucroferric oxyhydroxide in patients on peritoneal dialysis. Nephrol. Dial. Transplant. 2017, 32, 1918–1926. [Google Scholar] [CrossRef] [PubMed]
- Floege, J.; Covic, A.C.; Ketteler, M.; Mann, J.F.; Rastogi, A.; Spinowitz, B.; Chong, E.M.; Gaillard, S.; Lisk, L.J.; Sprague, S.M.; et al. Long-term effects of the iron-based phosphate binder, sucroferric oxyhydroxide, in dialysis patients. Nephrol. Dial. Transplant. 2015, 30, 1037–1046. [Google Scholar] [CrossRef] [PubMed]
- Narasaki, Y.; Rhee, C.M. Dietary Therapy for Managing Hyperphosphatemia. Clin. J. Am. Soc. Nephrol. 2020, 16, 9–11. [Google Scholar] [CrossRef]
- Ruospo, M.; Palmer, S.C.; Natale, P.; Craig, J.C.; Vecchio, M.; Elder, G.J.; Strippoli, G.F. Phosphate binders for preventing and treating chronic kidney disease-mineral and bone disorder (CKD-MBD). Cochrane Database Syst. Rev. 2018, 8, CD006023. [Google Scholar] [CrossRef]
- Brunner-Ziegler, S.; Fröschl, B.; Hiebinger, C.; Zsifkovits, J. Effectiveness and cost-efficacy of phosphate binders in hemodialysis. Ann. Nutr. Metab. 2011, 58, 315–319. [Google Scholar] [CrossRef]
- St Peter, W.L.; Wazny, L.D.; Weinhandl, E.D. Phosphate-Binder Use in US Dialysis Patients: Prevalence, Costs, Evidence, and Policies. Am. J. Kidney Dis. 2018, 71, 246–253. [Google Scholar] [CrossRef]
- Calvo, M.S.; Moshfegh, A.J.; Tucker, K.L. Assessing the health impact of phosphorus in the food supply: Issues and considerations. Adv. Nutr. 2014, 5, 104–113. [Google Scholar] [CrossRef]
- Calvo, M.S.; Lamberg-Allardt, C.J. Phosphorus. Adv. Nutr. 2015, 6, 860–862. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Gutekunst, L.; Mehrotra, R.; Kovesdy, C.P.; Bross, R.; Shinaberger, C.S.; Noori, N.; Hirschberg, R.; Benner, D.; Nissenson, A.R.; et al. Understanding sources of dietary phosphorus in the treatment of patients with chronic kidney disease. Clin. J. Am. Soc. Nephrol. 2010, 5, 519–530. [Google Scholar] [CrossRef] [PubMed]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am. J. Kidney Dis. 2020, 76 (Suppl. S1), S1–S107, Erratum in Am. J. Kidney Dis. 2021, 77, 308. [Google Scholar]
- Bi, S.H.; Wang, X.; Tang, W.; Wang, T.; Li, B.; Su, C. Longitudinal association between dietary protein intake and survival in peritoneal dialysis patients. Ren. Fail. 2023, 45, 2182605. [Google Scholar] [CrossRef] [PubMed]
- Canada-USA (CANUSA) Peritoneal Dialysis Study Group. Adequacy of dialysis and nutrition in continuous peritoneal dialysis: Association with clinical outcomes. J. Am. Soc. Nephrol. 1996, 7, 198–207. [Google Scholar] [CrossRef]
- Garibotto, G.; Saffioti, S.; Russo, R.; Verzola, D.; Cappelli, V.; Aloisi, F.; Sofia, A. Malnutrition in peritoneal dialysis patients: Causes and diagnosis. Contrib. Nephrol. 2003, 140, 112–121. [Google Scholar]
- Dombros, N.; Dratwa, M.; Feriani, M.; Gokal, R.; Heimbürger, O.; Krediet, R.; Plum, J.; Rodrigues, A.; Selgas, R.; Struijk, D.; et al. European best practice guidelines for peritoneal dialysis. 8 Nutrition in peritoneal dialysis. Nephrol. Dial. Transplant. 2005, 20 (Suppl. S9), ix28–ix33. [Google Scholar] [PubMed]
- Kiebalo, T.; Holotka, J.; Habura, I.; Pawlaczyk, K. Nutritional Status in Peritoneal Dialysis: Nutritional Guidelines, Adequacy and the Management of Malnutrition. Nutrients 2020, 12, 1715. [Google Scholar] [CrossRef]
- Jiang, N.; Fang, W.; Gu, A.P.; Yuan, J.Z.; Yang, X.X.; Lin, A.W.; Ni, Z.H.; Qian, J.Q. Improving diet recipe and cooking methods attenuates hyperphosphatemia in patients undergoing peritoneal dialysis. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 846–852. [Google Scholar] [CrossRef]
- Cupisti, A.; Comar, F.; Benini, O.; Lupetti, S.; D’Alessandro, C.; Barsotti, G.; Gianfaldoni, D. Effect of boiling on dietary phosphate and nitrogen intake. J. Ren. Nutr. 2006, 16, 36–40. [Google Scholar] [CrossRef]
- Vrdoljak, I.; Panjkota Krbavčić, I.; Bituh, M.; Vrdoljak, T.; Dujmić, Z. Analysis of different thermal processing methods of foodstuffs to optimize protein, calcium, and phosphorus content for dialysis patients. J. Ren. Nutr. 2015, 25, 308–315. [Google Scholar] [CrossRef]
- Cozzolino, M.; Stucchi, A.; Rizzo, M.A.; Brenna, I.; Elli, F.; Ciceri, P.; Bover, J.; Cusi, D.; Gallieni, M. Phosphate control in peritoneal dialysis. Contrib. Nephrol. 2012, 178, 116–123. [Google Scholar]
- Chiu, Y.W.; Teitelbaum, I.; Misra, M.; de Leon, E.M.; Adzize, T.; Mehrotra, R. Pill burden, adherence, hyperphosphatemia, and quality of life in maintenance dialysis patients. Clin. J. Am. Soc. Nephrol. 2009, 4, 1089–1096. [Google Scholar] [CrossRef]
- Sherrard, D.J.; Hercz, G.; Pei, Y.; Maloney, N.A.; Greenwood, C.; Manuel, A.; Saiphoo, C.; Fenton, S.S.; Segre, G.V. The spectrum of bone disease in end-stage renal failure—An evolving disorder. Kidney Int. 1993, 43, 436–442. [Google Scholar] [CrossRef]
- Carmen Sánchez, M.; Auxiliadora Bajo, M.; Selgas, R.; Mate, A.; Millán, I.; Eugenia Martínez, M.; López-Barea, F. Parathormone secretion in peritoneal dialysis patients with adynamic bone disease. Am. J. Kidney Dis. 2000, 36, 953–961. [Google Scholar] [CrossRef] [PubMed]
- Moe, S.M. Management of renal osteodystrophy in peritoneal dialysis patients. Perit. Dial. Int. 2004, 24, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Sherman, R.A. Dietary phosphate restriction and protein intake in dialysis patients: A misdirected focus. Semin. Dial. 2007, 20, 16–18. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, A.; Bhatt, N.; Rossetti, S.; Beto, J. Management of Hyperphosphatemia in End-Stage Renal Disease: A New Paradigm. J. Ren. Nutr. 2021, 31, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Gasmi, A.; Bjørklund, G.; Peana, M.; Mujawdiya, P.K.; Pivina, L.; Ongenae, A.; Piscopo, S.; Severin, B. Phosphocalcic metabolism and the role of vitamin D, vitamin K2, and nattokinase supplementation. Crit. Rev. Food Sci. Nutr. 2022, 62, 7062–7071. [Google Scholar] [CrossRef] [PubMed]
- Stremke, E.R.; Hill Gallant, K.M. Intestinal Phosphorus Absorption in Chronic Kidney Disease. Nutrients 2018, 10, 1364. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Liang, W.; Ye, T.; Chen, Z.; Zuo, X.; Du, X.; Qian, K.; Zhang, C.; Hu, X.; Li, J.; et al. The Association between Nutritional Markers and Biochemical Parameters and Residual Renal Function in Peritoneal Dialysis Patients. PLoS ONE 2016, 11, e0156423. [Google Scholar] [CrossRef]
- Tiong, M.K.; Ullah, S.; McDonald, S.P.; Tan, S.J.; Lioufas, N.M.; Roberts, M.A.; Toussaint, N.D. Serum phosphate and mortality in incident dialysis patients in Australia and New Zealand. Nephrology 2021, 26, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Wu, H.; Huang, X.; Ye, H.; Huang, F.; Yu, X.; Yang, X. Associations between serum mineral metabolism parameters and mortality in patients on peritoneal dialysis. Nephrology 2019, 24, 1148–1156. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Ref. | Study Design | Population | Study Drug | Control | Follow-Up Duration | Main Results |
|---|---|---|---|---|---|---|
| [61] | Open label, randomized crossover trial | 30 adult patients on CAPD | Sevelamer hydrochloride | Aluminum hydroxide |
|
|
| [62] | Multicenter open-label randomized parallel-group trial | 143 adult patients on PD (CAPD/APD 43%/57% in both groups) with serum phosphorus >5.5 mg/dL | Sevelamer hydrochloride (n. 97 patients) | Calcium acetate (n. 46 patients) | 12 wks |
|
| [63] | Subanalysis of a previous initial phase 3 randomized trial [55] followed by an extension study [64] | 84 adult patients on PD | Sucroferric oxyhydroxide (n. 56 patients) | Sevelamer carbonate (n. 28 patients) | 52 wks |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cernaro, V.; Calderone, M.; Gembillo, G.; Calabrese, V.; Casuscelli, C.; Lo Re, C.; Longhitano, E.; Santoro, D. Phosphate Control in Peritoneal Dialysis Patients: Issues, Solutions, and Open Questions. Nutrients 2023, 15, 3161. https://doi.org/10.3390/nu15143161
Cernaro V, Calderone M, Gembillo G, Calabrese V, Casuscelli C, Lo Re C, Longhitano E, Santoro D. Phosphate Control in Peritoneal Dialysis Patients: Issues, Solutions, and Open Questions. Nutrients. 2023; 15(14):3161. https://doi.org/10.3390/nu15143161
Chicago/Turabian StyleCernaro, Valeria, Michela Calderone, Guido Gembillo, Vincenzo Calabrese, Chiara Casuscelli, Claudia Lo Re, Elisa Longhitano, and Domenico Santoro. 2023. "Phosphate Control in Peritoneal Dialysis Patients: Issues, Solutions, and Open Questions" Nutrients 15, no. 14: 3161. https://doi.org/10.3390/nu15143161
APA StyleCernaro, V., Calderone, M., Gembillo, G., Calabrese, V., Casuscelli, C., Lo Re, C., Longhitano, E., & Santoro, D. (2023). Phosphate Control in Peritoneal Dialysis Patients: Issues, Solutions, and Open Questions. Nutrients, 15(14), 3161. https://doi.org/10.3390/nu15143161