
Adherence to the Mediterranean Diet in Preventing Major Cardiovascular Events in Patients with Ischemic Heart Disease: The EVA Study

 ,
,  , ,
, ,  , , , ,
, , , ,  ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
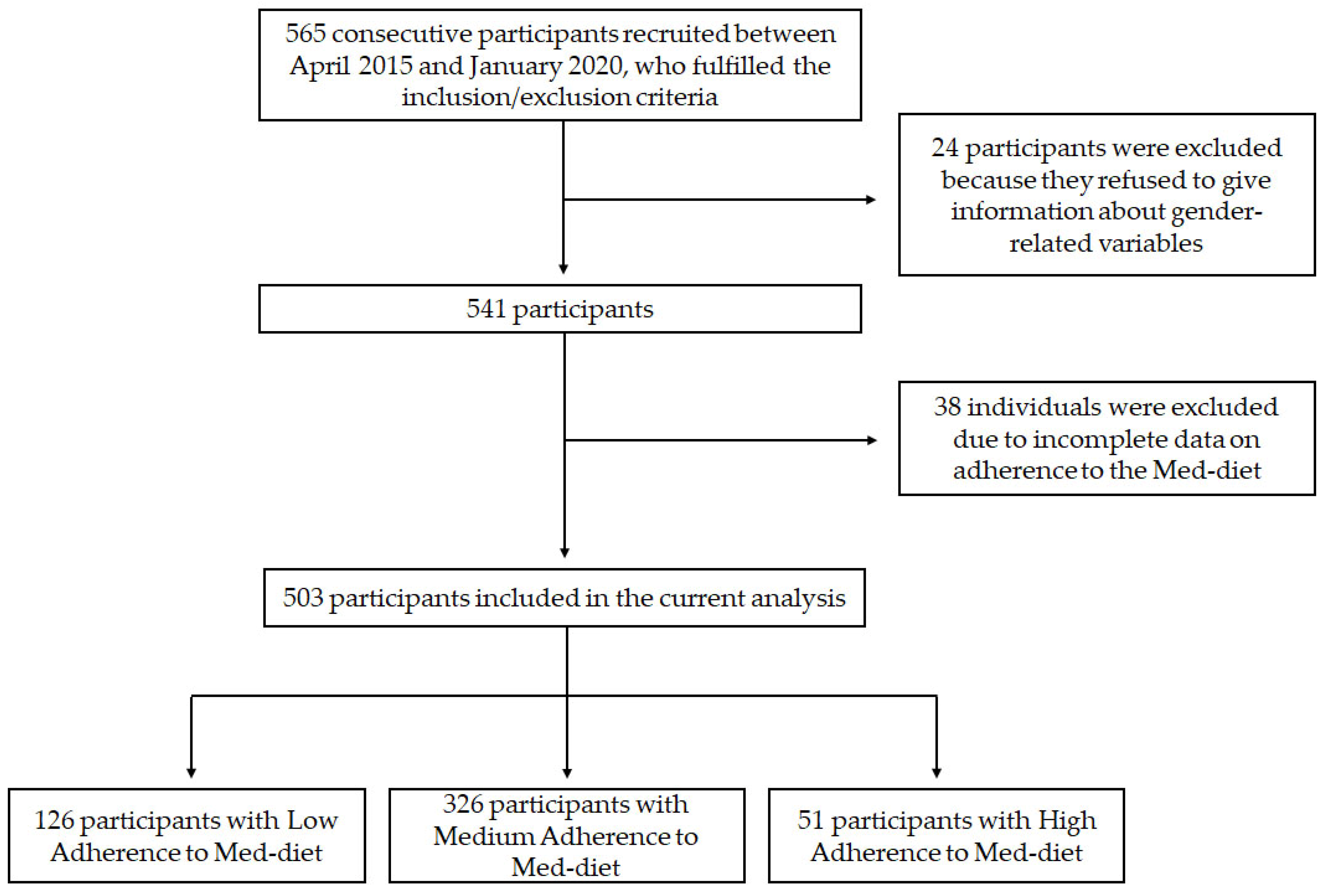
2.1. Study Population
2.2. Assessment of Adherence to Med-Diet
2.3. Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Baseline Participants’ Characteristics and Med-Diet Adherence
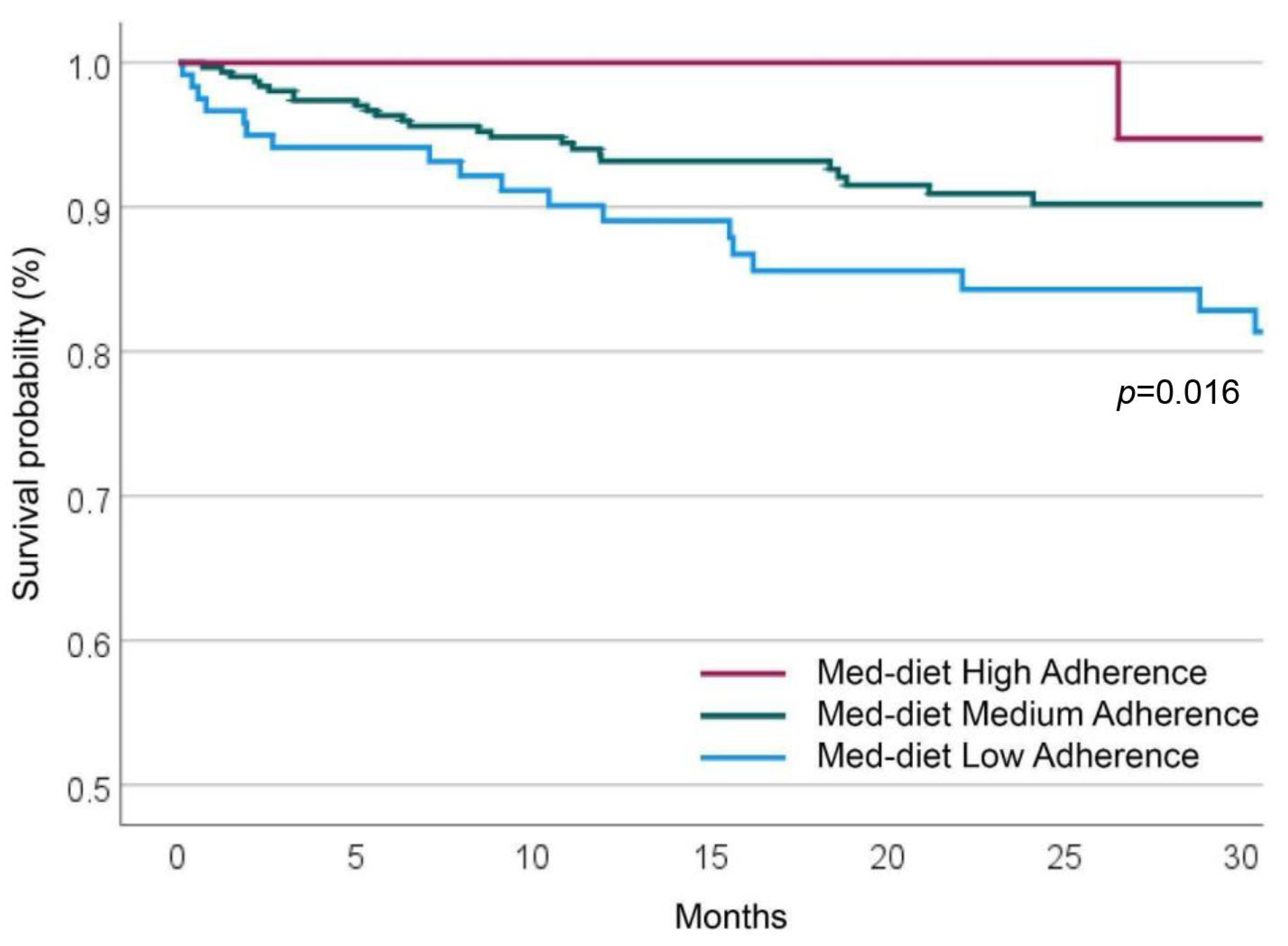
3.2. Adherence to Med-Diet and MACEs at Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lichtenstein, A.H.; Appel, L.J.; Vadiveloo, M.; Hu, F.B.; Kris-Etherton, P.M.; Rebholz, C.M.; Sacks, F.M.; Thorndike, A.N.; van Horn, L.; Wylie-Rosett, J. 2021 Dietary Guidance to Improve Cardiovascular Health: A Scientific Statement from the American Heart Association. Circulation 2021, 144, e472–e487. [Google Scholar] [CrossRef] [PubMed]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Karam, G.; Agarwal, A.; Sadeghirad, B.; Jalink, M.; Hitchcock, C.L.; Ge, L.; Kiflen, R.; Ahmed, W.; Zea, A.M.; Milenkovic, J.; et al. Comparison of Seven Popular Structured Dietary Programmes and Risk of Mortality and Major Cardiovascular Events in Patients at Increased Cardiovascular Risk: Systematic Review and Network Meta-Analysis. BMJ 2023, 380, e072003. [Google Scholar] [CrossRef] [PubMed]
- Mattavelli, E.; Olmastroni, E.; Casula, M.; Grigore, L.; Pellegatta, F.; Baragetti, A.; Magni, P.; Catapano, A.L. Adherence to Mediterranean Diet: A Population-Based Longitudinal Cohort Study. Nutrients 2023, 15, 1844. [Google Scholar] [CrossRef] [PubMed]
- Bonaccio, M.; Costanzo, S.; Di Castelnuovo, A.; Persichillo, M.; De Curtis, A.; Olivieri, M.; Cerletti, C.; Donati, M.B.; de Gaetano, G.; Iacoviello, L. The CASSIOPEA Study (Economic Crisis and Adherence to the Mediterranean Diet: PoSSIble Impact on BiOmarkers of Inflammation and Metabolic PhEnotypes in the Cohort of the Moli-SAni Study): Rationale, Design and Characteristics of Participants. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 1053–1062. [Google Scholar] [CrossRef] [PubMed]
- Herrera-Ramos, E.; Tomaino, L.; Sánchez-Villegas, A.; Ribas-Barba, L.; Gómez, S.F.; Wärnberg, J.; Osés, M.; González-Gross, M.; Gusi, N.; Aznar, S.; et al. Trends in Adherence to the Mediterranean Diet in Spanish Children and Adolescents across Two Decades. Nutrients 2023, 15, 2348. [Google Scholar] [CrossRef]
- Lovell, A.L.; Roy, R.; Klein, A.; Cavadino, A.; Foster, M.; Krebs, J.D.; Braakhuis, A.; Merry, T.L. Habitual Dietary Patterns, Nutrient Intakes, and Adherence to the Mediterranean Diet among New Zealand Adults: The NZ MED Cross-Sectional Study. Nutrients 2023, 15, 2663. [Google Scholar] [CrossRef]
- Grams, L.; Nelius, A.K.; Pastor, G.G.; Sillero-Quintana, M.; Veiga, Ó.L.; Homeyer, D.; Kück, M. Comparison of Adherence to Mediterranean Diet between Spanish and German School-Children and Influence of Gender, Overweight, and Physical Activity. Nutrients 2022, 14, 4697. [Google Scholar] [CrossRef]
- Zeraattalab-Motlagh, S.; Jayedi, A.; Shab-Bidar, S. Mediterranean Dietary Pattern and the Risk of Type 2 Diabetes: A Systematic Review and Dose-Response Meta-Analysis of Prospective Cohort Studies. Eur. J. Nutr. 2022, 61, 1735–1748. [Google Scholar] [CrossRef]
- Mendonça, N.; Gregório, M.J.; Salvador, C.; Henriques, A.R.; Canhão, H.; Rodrigues, A.M. Low Adherence to the Mediterranean Diet Is Associated with Poor Socioeconomic Status and Younger Age: A Cross-Sectional Analysis of the EpiDoC Cohort. Nutrients 2022, 14, 1239. [Google Scholar] [CrossRef]
- Cangemi, R.; Romiti, G.F.; Campolongo, G.; Ruscio, E.; Sciomer, S.; Gianfrilli, D.; Raparelli, V. Gender Related Differences in Treatment and Response to Statins in Primary and Secondary Cardiovascular Prevention: The Never-Ending Debate. Pharmacol. Res. 2017, 117, 148–155. [Google Scholar] [CrossRef]
- Clayton, J.A.; Tannenbaum, C. Reporting Sex, Gender, or Both in Clinical Research? JAMA—J. Am. Med. Assoc. 2016, 316, 1863–1864. [Google Scholar] [CrossRef]
- O’Neil, A.; Scovelle, A.J.; Milner, A.J.; Kavanagh, A. Gender/Sex as a Social Determinant of Cardiovascular Risk. Circulation 2018, 137, 854–864. [Google Scholar] [CrossRef]
- Raparelli, V.; Romiti, G.F.; Spugnardi, V.; Borgi, M.; Cangemi, R.; Basili, S.; Proietti, M.; Lenzi, A.; Tiberti, C.; Panimolle, F.; et al. Gender-Related Determinants of Adherence to the Mediterranean Diet in Adults with Ischemic Heart Disease. Nutrients 2020, 12, 759. [Google Scholar] [CrossRef]
- Rees, K.; Takeda, A.; Martin, N.; Ellis, L.; Wijesekara, D.; Vepa, A.; Das, A.; Hartley, L.; Stranges, S. Mediterranean-Style Diet for the Primary and Secondary Prevention of Cardiovascular Disease. Cochrane Database Syst. Rev. 2019, 3, CD009825. [Google Scholar] [CrossRef]
- Kwaśny, A.; Łokieć, K.; Uchmanowicz, B.; Młynarska, A.; Smereka, J.; Czapla, M. Sex-Related Differences in the Impact of Nutritional Status on In-Hospital Mortality in Acute Coronary Syndrome: A Retrospective Cohort Study. Nutr. Metab. Cardiovasc. Dis. 2023. [Google Scholar] [CrossRef]
- Kwaśny, A.; Uchmanowicz, I.; Juárez-Vela, R.; Młynarska, A.; Łokieć, K.; Czapla, M. Sex-Related Differences in the Impact of Nutritional Status on In-Hospital Mortality in Heart Failure: A Retrospective Cohort Study. Eur. J. Cardiovasc. Nurs. 2023. [CrossRef]
- Raparelli, V.; Proietti, M.; Lenzi, A.; Basili, S.; Collaborators, E. Sex and Gender Differences in Ischemic Heart Disease: Endocrine Vascular Disease Approach (EVA) Study Design. J. Cardiovasc. Transl. Res. 2018, 13, 14–25. [Google Scholar] [CrossRef]
- Hlatky, M.A.; Boineau, R.E.; Higginbotham, M.B.; Lee, K.L.; Mark, D.B.; Califf, R.M.; Cobb, F.R.; Pryor, D.B. A Brief Self-Administered Questionnaire to Determine Functional Capacity (The Duke Activity Status Index). Am. J. Cardiol. 1989, 64, 651–654. [Google Scholar] [CrossRef]
- Johnson, J.L.; Greaves, L.; Repta, R. Better Science with Sex and Gender: A Primer for Health Research; Women’s Health Research Network: Vancouver, BC, Canada, 2007.
- Bem, S.L. The Measurement of Psychological Androgyny. J. Consult. Clin. Psychol. 1974, 42, 155–162. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J. Health Soc. Behav. 1983, 24, 385. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-Item Mediterranean Diet Assessment Tool and Obesity Indexes among High-Risk Subjects: The PREDIMED Trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Lagiou, P. Healthy Traditional Mediterranean Diet: An Expression of Culture, History, and Lifestyle. Nutr. Rev. 1997, 55, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Cesari, F.; Abbate, R.; Gensini, G.F.; Casini, A. Adherence to Mediterranean Diet and Health Status: Meta-Analysis. BMJ 2008, 337, 673–675. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- De Lorgeril, M.; Salen, P.; Martin, J.L.; Monjaud, I.; Delaye, J.; Mamelle, N. Mediterranean Diet, Traditional Risk Factors, and the Rate of Cardiovascular Complications after Myocardial Infarction: Final Report of the Lyon Diet Heart Study. Circulation 1999, 99, 779–785. [Google Scholar] [CrossRef]
- Lehmann, N.; Paul, A.; Moebus, S.; Budde, T.; Dobos, G.J.; Michalsen, A. Effects of Lifestyle Modification on Coronary Artery Calcium Progression and Prognostic Factors in Coronary Patients—3-Year Results of the Randomized SAFE-LIFE Trial. Atherosclerosis 2011, 219, 630–636. [Google Scholar] [CrossRef]
- Delgado-Lista, J.; Alcala-Diaz, J.F.; Torres-Peña, J.D.; Quintana-Navarro, G.M.; Fuentes, F.; Garcia-Rios, A.; Ortiz-Morales, A.M.; Gonzalez-Requero, A.I.; Perez-Caballero, A.I.; Yubero-Serrano, E.M.; et al. Long-Term Secondary Prevention of Cardiovascular Disease with a Mediterranean Diet and a Low-Fat Diet (CORDIOPREV): A Randomised Controlled Trial. Lancet 2022, 399, 1876–1885. [Google Scholar] [CrossRef]
- Raparelli, V.; Nocella, C.; Proietti, M.; Romiti, G.F.; Corica, B.; Bartimoccia, S.; Stefanini, L.; Lenzi, A.; Viceconte, N.; Tanzilli, G.; et al. Testosterone-to-Estradiol Ratio and Platelet Thromboxane Release in Ischemic Heart Disease: The EVA Project. J. Endocrinol. Investig. 2022, 45, 1367–1377. [Google Scholar] [CrossRef]
- Teo, P.S.; Van Dam, R.M.; Whitton, C.; Tan, L.W.L.; Forde, C.G. Consumption of Foods with Higher Energy Intake Rates Is Associated with Greater Energy Intake, Adiposity, and Cardiovascular Risk Factors in Adults. J. Nutr. 2021, 151, 370–378. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Low Adherence (n = 126) | Medium Adherence (n = 326) | High Adherence (n = 51) | p |
|---|---|---|---|---|
| Age, years | 65.7 ± 11.9 | 67.4 ± 11.1 | 66.3 ± 9.5 | 0.353 |
| BMI, kg/m2 | 27.2 ± 4.2 | 26.9 ± 4.5 | 26.8 ± 4.0 | 0.824 |
| Female sex, n (%) | 37 (29%) | 102 (31%) | 9 (18%) | 0.139 |
| Previous MI, n (%) | 31 (25%) | 85 (26%) | 8 (16%) | 0.278 |
| HF, n (%) | 14 (11%) | 48 (15%) | 5 (10%) | 0.442 |
| Hypertension, n (%) | 103 (82%) | 259 (79%) | 41 (80%) | 0.859 |
| Dyslipidemia, n (%) | 66 (52%) | 167 (51%) | 24 (47%) | 0.811 |
| T2DM, n (%) | 37 (29%) | 86 (26%) | 9 (18%) | 0.275 |
| Stroke/TIA, n (%) | 13 (10.3%) | 39 (12%) | 7 (14%) | 0.796 |
| Active smoking, n (%) | 36 (29%) | 85 (26%) | 9 (18%) | 0.319 |
| Physical inactivity, n (%) | 108 (87%) | 249 (77%) | 35 (69%) | 0.013 |
| DASI (median and IQR) | 38 (23–58) | 33 (19–50) | 45 (27–58) | 0.046 |
| Variables | Low Adherence (n = 126) | Medium Adherence (n = 326) | High Adherence (n = 51) | p |
|---|---|---|---|---|
| Obstructive CAD | 98 (78%) | 234 (72%) | 34 (67%) | 0.254 |
| Presentation as ACS | 68 (54%) | 160 (49%) | 19 (38%) | 0.161 |
| Variables | Low Adherence (n = 126) | Medium Adherence (n = 326) | High Adherence (n = 51) | p |
|---|---|---|---|---|
| Married/living with partner, n (%) | 95 (75%) | 222 (68%) | 36 (71%) | 0.314 |
| Male BSRI (mean ± SD) | 4.85 ± 1.13 | 4.94 ± 0.91 | 5.31 ± 0.74 | 0.031 |
| Female BSRI (mean ± SD) | 5.71 ± 0.72 | 5.84 ± 0.75 | 5.91 ± 0.72 | 0.349 |
| Neutral BSRI (mean ± SD) | 4.84 ± 0.67 | 4.84 ± 0.66 | 4.85 ± 0.57 | 0.993 |
| PSS-10 (median and IQR) | 19 (11–22) | 16 (12–21) | 15 (10–22) | 0.362 |
| Living with a smoker, n (%) | 14 (11%) | 22 (7%) | 1 (2%) | 0.001 |
| Active employment, n (%) | 50 (40%) | 118 (36%) | 23 (45%) | 0.396 |
| Less than secondary school education level, n (%) * | 29 (33%) | 88 (35%) | 16 (35%) | 0.886 |
| Low social support, n (%) * | 11 (13%) | 21 (8%) | 5 (11%) | 0.392 |
| Variables | HR | 95% CI | p | |
|---|---|---|---|---|
| Female sex | 1.098 | 0.602 | 2.002 | 0.760 |
| Age | 1.044 | 1.014 | 1.075 | 0.004 |
| BMI | 0.962 | 0.898 | 1.031 | 0.273 |
| Previous MI | 1.148 | 0.607 | 2.170 | 0.671 |
| HF | 4.119 | 2.293 | 7.398 | <0.001 |
| Hypertension | 2.146 | 0.850 | 5.418 | 0.106 |
| Dyslipidemia | 1.049 | 0.595 | 1.851 | 0.869 |
| T2DM | 2.249 | 1.271 | 3.979 | 0.005 |
| Stroke/TIA | 1.116 | 0.474 | 2.626 | 0.801 |
| Active smoking | 1.201 | 0.644 | 2.238 | 0.564 |
| Physical inactivity | 1.616 | 0.725 | 3.603 | 0.241 |
| Living with a smoker | 1.056 | 0.574 | 1.946 | 0.860 |
| DASI | 0.976 | 0.959 | 0.992 | 0.004 |
| Male BSRI | 1.421 | 0.903 | 2.236 | 0.129 |
| Med-diet Adherence | 0.492 | 0.300 | 0.809 | 0.005 |
| Obstructive CAD | 3.909 | 1.404 | 10.881 | 0.009 |
| Presentation as ACS | 1.394 | 0.780 | 2.491 | 0.262 |
| Variables | HR | 95% CI | p | |
|---|---|---|---|---|
| Obstructive CAD (vs. non-obstructive CAD) | 3.069 | 1.097 | 8.586 | 0.033 |
| HF | 3.695 | 2.029 | 6.728 | <0.001 |
| T2DM | 1.887 | 1.058 | 3.364 | 0.031 |
| Med-diet Adherence (high and medium vs. low adherence) | 0.491 | 0.295 | 0.818 | 0.006 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cangemi, R.; Miglionico, M.; D’Amico, T.; Fasano, S.; Proietti, M.; Romiti, G.F.; Corica, B.; Stefanini, L.; Tanzilli, G.; Basili, S.; et al. Adherence to the Mediterranean Diet in Preventing Major Cardiovascular Events in Patients with Ischemic Heart Disease: The EVA Study. Nutrients 2023, 15, 3150. https://doi.org/10.3390/nu15143150
Cangemi R, Miglionico M, D’Amico T, Fasano S, Proietti M, Romiti GF, Corica B, Stefanini L, Tanzilli G, Basili S, et al. Adherence to the Mediterranean Diet in Preventing Major Cardiovascular Events in Patients with Ischemic Heart Disease: The EVA Study. Nutrients. 2023; 15(14):3150. https://doi.org/10.3390/nu15143150
Chicago/Turabian StyleCangemi, Roberto, Marzia Miglionico, Tania D’Amico, Salvatore Fasano, Marco Proietti, Giulio Francesco Romiti, Bernadette Corica, Lucia Stefanini, Gaetano Tanzilli, Stefania Basili, and et al. 2023. "Adherence to the Mediterranean Diet in Preventing Major Cardiovascular Events in Patients with Ischemic Heart Disease: The EVA Study" Nutrients 15, no. 14: 3150. https://doi.org/10.3390/nu15143150
APA StyleCangemi, R., Miglionico, M., D’Amico, T., Fasano, S., Proietti, M., Romiti, G. F., Corica, B., Stefanini, L., Tanzilli, G., Basili, S., Raparelli, V., Tarsitano, M. G., & EVA Collaborative Group. (2023). Adherence to the Mediterranean Diet in Preventing Major Cardiovascular Events in Patients with Ischemic Heart Disease: The EVA Study. Nutrients, 15(14), 3150. https://doi.org/10.3390/nu15143150