
Association of Serum Oxysterols with Cholesterol Metabolism Markers and Clinical Factors in Patients with Coronary Artery Disease: A Covariance Structure Analysis

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2. Biomarker Assessment
2.3. Statistical Analysis
3. Results
3.1. Study Population
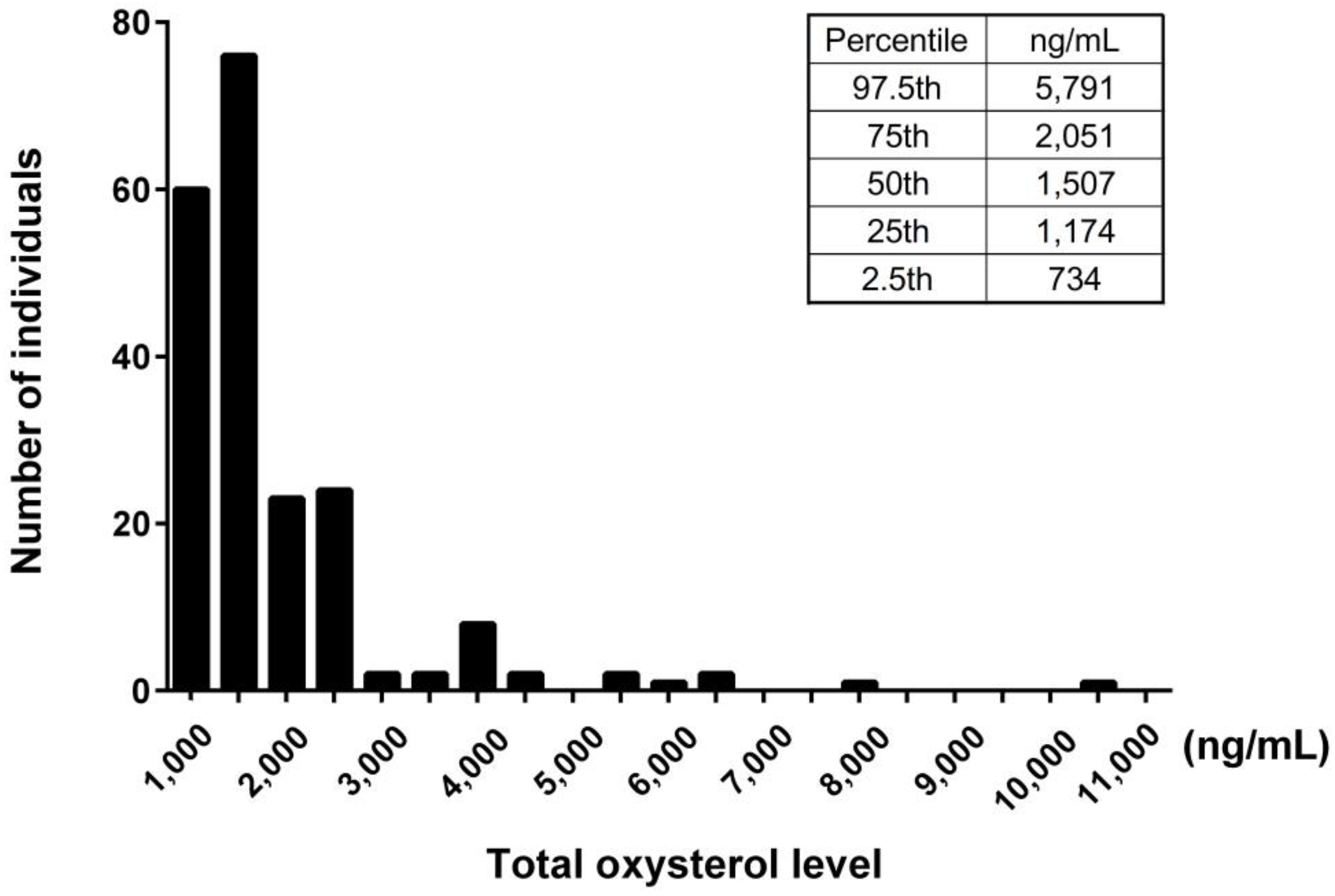
3.2. Analysis of Oxysterols in the Study Population
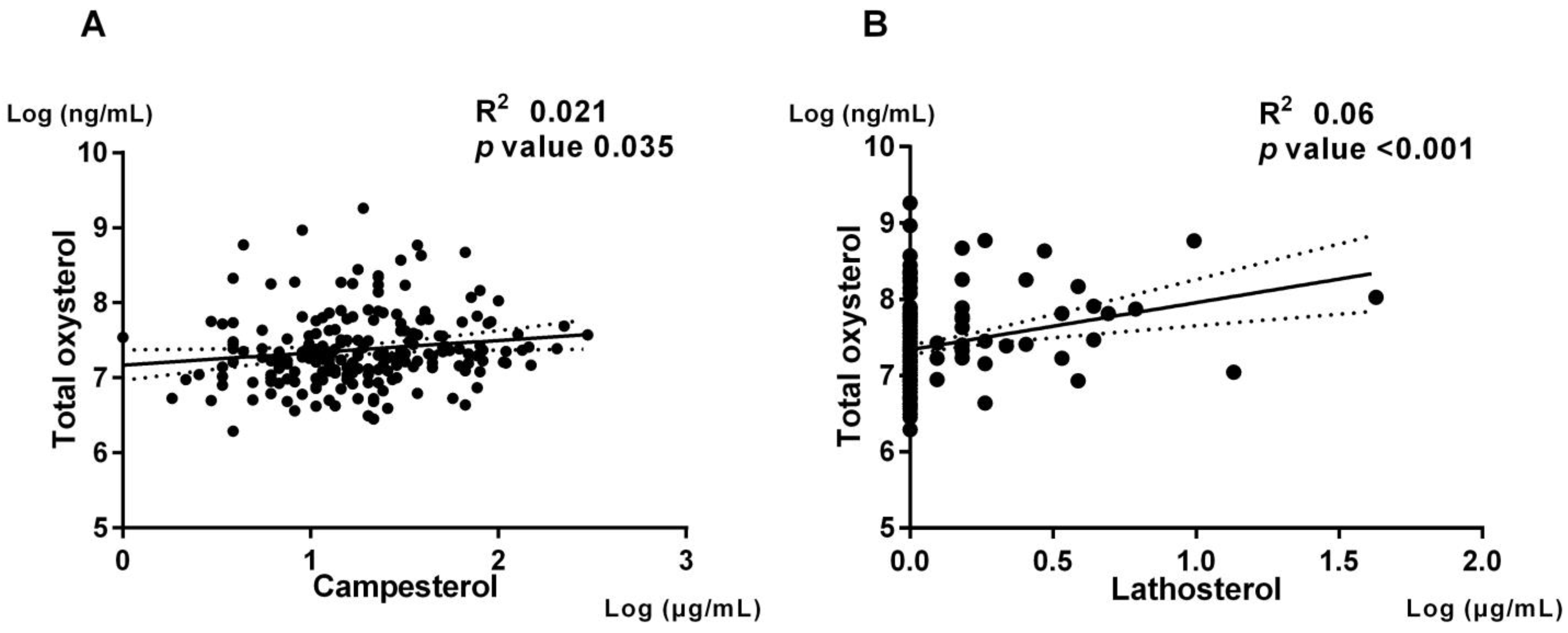
3.3. Association of Oxysterols with Cholesterol Absorption and Synthesis
3.4. Association of Cholesterol Absorption and Synthesis with Clinical and Biochemical Characteristics
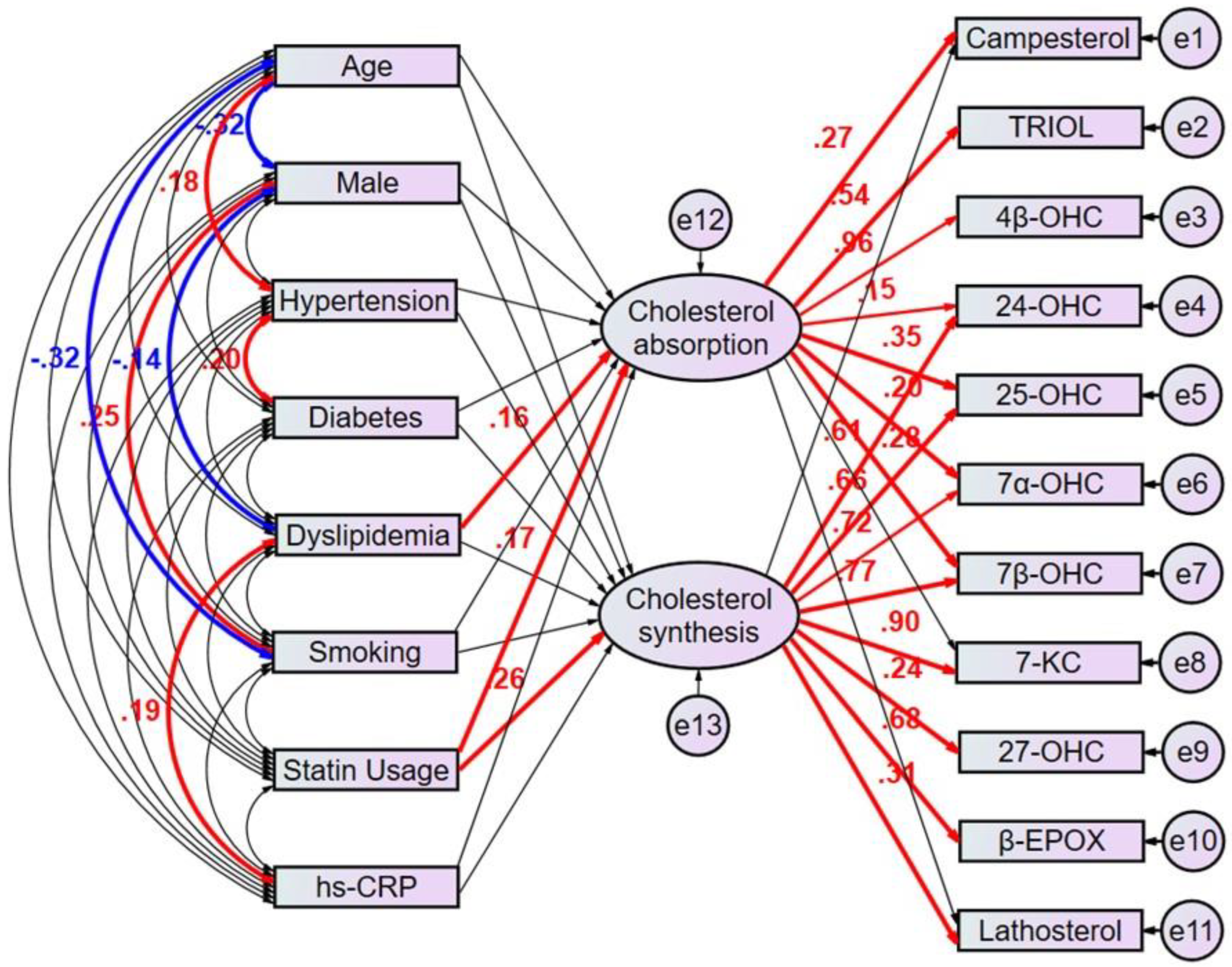
3.5. Path Model Estimated Regression Weights in Oxysterols Revealed Potential Clinical Factors Affecting Cholesterol Metabolism Markers
3.6. Path Model Revealed the Associations between Individual Oxysterols and Latent Cholesterol Absorption and Synthesis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schroepfer, G.J., Jr. Oxysterols: Modulators of cholesterol metabolism and other processes. Physiol. Rev. 2000, 80, 361–554. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.J.; Jessup, W. Oxysterols and atherosclerosis. Atherosclerosis 1999, 142, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Serviddio, G.; Blonda, M.; Bellanti, F.; Villani, R.; Iuliano, L.; Vendemiale, G. Oxysterols and redox signaling in the pathogenesis of non-alcoholic fatty liver disease. Free. Radic. Res. 2013, 47, 881–893. [Google Scholar] [CrossRef]
- Leoni, V.; Caccia, C. Oxysterols as biomarkers in neurodegenerative diseases. Chem. Phys. Lipids 2011, 164, 515–524. [Google Scholar] [CrossRef]
- Zhang, X.; Alhasani, R.H.; Zhou, X.; Reilly, J.; Zeng, Z.; Strang, N.; Shu, X. Oxysterols and retinal degeneration. Br. J. Pharmacol. 2021, 178, 3205–3219. [Google Scholar] [CrossRef] [PubMed]
- Kloudova, A.; Guengerich, F.P.; Soucek, P. The Role of Oxysterols in Human Cancer. Trends Endocrinol. Metab. 2017, 28, 485–496. [Google Scholar] [CrossRef]
- Samadi, A.; Gurlek, A.; Sendur, S.N.; Karahan, S.; Akbiyik, F.; Lay, I. Oxysterol species: Reliable markers of oxidative stress in diabetes mellitus. J. Endocrinol. Investig. 2019, 42, 7–17. [Google Scholar] [CrossRef]
- Zang, R.; Case, J.B.; Yutuc, E.; Ma, X.; Shen, S.; Gomez Castro, M.F.; Liu, M.F.; Zeng, Z.; Zhao, Q.; Son, H.; et al. Cholesterol 25-hydroxylase suppresses SARS-CoV-2 replication by blocking membrane fusion. Proc. Natl. Acad. Sci. USA 2020, 117, 32105–32113. [Google Scholar] [CrossRef] [PubMed]
- Weingärtner, O.; Lütjohann, D.; Vanmierlo, T.; Müller, S.; Günther, L.; Herrmann, W.; Böhm, M.; Laufs, U.; Herrmann, M. Markers of enhanced cholesterol absorption are a strong predictor for cardiovascular diseases in patients without diabetes mellitus. Chem. Phys. Lipids 2011, 164, 451–456. [Google Scholar] [CrossRef]
- Altmann, S.W.; Davis, H.R., Jr.; Zhu, L.-J.; Yao, X.; Hoos, L.M.; Tetzloff, G.; Iyer, S.P.N.; Maguire, M.; Golovko, A.; Zeng, M.; et al. Niemann-Pick C1 Like 1 protein is critical for intestinal cholesterol absorption. Science 2004, 303, 1201–1204. [Google Scholar] [CrossRef] [PubMed]
- Miettinen, T.A.; Tilvis, R.S.; Kesäniemi, Y.A. Serum plant sterols and cholesterol precursors reflect cholesterol absorption and synthesis in volunteers of a randomly selected male population. Am. J. Epidemiol. 1990, 131, 20–31. [Google Scholar] [CrossRef]
- Silbernagel, G.; Fauler, G.; Renner, W.; Landl, E.M.; Hoffmann, M.M.; Winkelmann, B.R.; Boehm, B.O.; März, W. The relationships of cholesterol metabolism and plasma plant sterols with the severity of coronary artery disease. J. Lipid Res. 2009, 50, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Matthan, N.R.; Pencina, M.; LaRocque, J.M.; Jacques, P.F.; D’Agostino, R.B.; Schaefer, E.J.; Lichtenstein, E.J.; Alice, H. Alterations in cholesterol absorption/synthesis markers characterize Framingham offspring study participants with CHD. J. Lipid Res. 2009, 50, 1927–1935. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, T.; Ishigaki, Y.; Nakagami, T.; Akiyama, Y.; Ishibashi, Y.; Ishida, T.; Fujii, H.; Harada-Shiba, M.; Kabata, D.; Kihara, Y.; et al. Relationship between Diabetes Mellitus and Serum Lathosterol and Campesterol Levels: The CACHE Study DM Analysis. J. Atheroscler. Thromb. 2022, 63725. [Google Scholar] [CrossRef]
- Rogacev, K.S.; Pinsdorf, T.; Weingärtner, O.; Gerhart, M.K.; Welzel, E.; van Bentum, K.; Julius, P.; Andreas, M.; Danilo, F.; Heine, G.H.; et al. Cholesterol synthesis, cholesterol absorption, and mortality in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2012, 7, 943–948. [Google Scholar] [CrossRef]
- Miettinen, T.A.; Gylling, H. Effect of statins on noncholesterol sterol levels: Implications for use of plant stanols and sterols. Am. J. Cardiol. 2005, 96, 40D–46D. [Google Scholar] [CrossRef] [PubMed]
- Strandberg, T.E.; Tilvis, R.S.; Pitkala, K.H.; Miettinen, T.A. Cholesterol and glucose metabolism and recurrent cardiovascular events among the elderly: A prospective study. J. Am. Coll. Cardiol. 2006, 48, 708–714. [Google Scholar] [CrossRef]
- Katsuki, S.; Matoba, T.; Akiyama, Y.; Yoshida, H.; Kotani, K.; Fujii, H.; Harada-Shiba, M.; Ishibashi, Y.; Ishida, T.; Ishigaki, Y.; et al. Association of Serum Levels of Cholesterol Absorption and Synthesis Markers with the Presence of Cardiovascular Disease: The CACHE Study CVD Analysis. J. Atheroscler. Thromb. 2023, 64119. [Google Scholar] [CrossRef]
- Takase, S.; Matoba, T.; Nakashiro, S.; Mukai, Y.; Inoue, S.; Oi, K.; Taiki, H.; Shunsuke, K.; Masao, T.; Suematsu, N.; et al. Ezetimibe in Combination with Statins Ameliorates Endothelial Dysfunction in Coronary Arteries After Stenting: The CuVIC Trial (Effect of Cholesterol Absorption Inhibitor Usage on Target Vessel Dysfunction After Coronary Stenting), a Multicenter Randomized Controlled Trial. Arterioscler. Thromb. Vasc. Biol. 2017, 37, 350–358. [Google Scholar]
- Björkhem, I.; Lövgren-Sandblom, A.; Leoni, V.; Meaney, S.; Brodin, L.; Salveson, L.; Winge, K.; Pålhagen, S.; Svenningsson, P. Oxysterols and Parkinson’s disease: Evidence that levels of 24S-hydroxycholesterol in cerebrospinal fluid correlates with the duration of the disease. Neurosci. Lett. 2013, 555, 102–105. [Google Scholar] [CrossRef]
- Mutemberezi, V.; Guillemot-Legris, O.; Muccioli, G.G. Oxysterols: From cholesterol metabolites to key mediators. Prog. Lipid Res. 2016, 64, 152–169. [Google Scholar] [CrossRef]
- Piche, M.E.; Tchernof, A.; Despres, J.P. Obesity Phenotypes, Diabetes, and Cardiovascular Diseases. Circ. Res. 2020, 126, 1477–1500. [Google Scholar] [CrossRef]
- Franklin, S.S.; Pio, J.R.; Wong, N.D.; Larson, M.G.; Leip, E.P.; Vasan, R.S.; Levy, D. Predictors of new-onset diastolic and systolic hypertension: The Framingham Heart Study. Circulation 2005, 111, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- Shiba, N.; Nochioka, K.; Miura, M.; Kohno, H.; Shimokawa, H. Trend of westernization of etiology and clinical characteristics of heart failure patients in Japan--first report from the CHART-2 study. Circ. J. 2011, 75, 823–833. [Google Scholar] [CrossRef] [PubMed]
- Honda, K.; Matoba, T.; Antoku, Y.; Koga, J.I.; Ichi, I.; Nakano, K.; Hiroyuki, T.; Kensuke, E. Lipid-Lowering Therapy with Ezetimibe Decreases Spontaneous Atherothrombotic Occlusions in a Rabbit Model of Plaque Erosion: A Role of Serum Oxysterols. Arterioscler. Thromb. Vasc. Biol. 2018, 38, 757–771. [Google Scholar] [CrossRef]
- Uchikawa, T.; Matoba, T.; Kawahara, T.; Baba, I.; Katsuki, S.; Koga, J.-I.; Hashimoto, Y.; Yamasaki, R.; Ichi, I.; Akita, H.; et al. Dietary 7-ketocholesterol exacerbates myocardial ischemia-reperfusion injury in mice through monocyte/macrophage-mediated inflammation. Sci. Rep. 2022, 12, 14902. [Google Scholar] [CrossRef]
- Umetani, M.; Ghosh, P.; Ishikawa, T.; Umetani, J.; Ahmed, M.; Mineo, C.; Shaul, P.W. The cholesterol metabolite 27-hydroxycholesterol promotes atherosclerosis via proinflammatory processes mediated by estrogen receptor alpha. Cell. Metab. 2014, 20, 172–182. [Google Scholar] [CrossRef] [PubMed]
- Stiles, A.R.; Kozlitina, J.; Thompson, B.M.; McDonald, J.G.; King, K.S.; Russell, D.W. Genetic, anatomic, and clinical determinants of human serum sterol and vitamin D levels. Proc. Natl. Acad. Sci. USA 2014, 111, E4006-14. [Google Scholar] [CrossRef]
- Babiker, A.; Diczfalusy, U. Transport of side-chain oxidized oxysterols in the human circulation. Biochim. Biophys. Acta 1998, 1392, 333–339. [Google Scholar] [CrossRef]
- Berge, K.E.; von Bergmann, K.; Lutjohann, D.; Guerra, R.; Grundy, S.M.; Hobbs, H.H.; Cohen, J.C. Heritability of plasma noncholesterol sterols and relationship to DNA sequence polymorphism in ABCG5 and ABCG8. J. Lipid Res. 2002, 43, 486–494. [Google Scholar] [CrossRef]
- Locatelli, S.; Lutjohann, D.; Schmidt, H.H.; Otto, C.; Beisiegel, U.; von Bergmann, K. Reduction of plasma 24S-hydroxycholesterol (cerebrosterol) levels using high-dosage simvastatin in patients with hypercholesterolemia: Evidence that simvastatin affects cholesterol metabolism in the human brain. Arch. Neurol. 2002, 59, 213–216. [Google Scholar] [CrossRef]
- Dias, I.H.K.; Milic, I.; Lip, G.Y.H.; Devitt, A.; Polidori, M.C.; Griffiths, H.R. Simvastatin reduces circulating oxysterol levels in men with hypercholesterolaemia. Redox Biol. 2018, 16, 139–145. [Google Scholar] [CrossRef]
- Reboldi, A.; Dang, E.V.; McDonald, J.G.; Liang, G.; Russell, D.W.; Cyster, J.G. Inflammation. 25-Hydroxycholesterol suppresses interleukin-1-driven inflammation downstream of type I interferon. Science 2014, 345, 679–684. [Google Scholar] [CrossRef]
- Liu, C.; Yang, X.V.; Wu, J.; Kuei, C.; Mani, N.S.; Zhang, L.; Yu, J.; Sutton, S.W.; Qin, N.; Banie, H.; et al. Oxysterols direct B-cell migration through EBI2. Nature 2011, 475, 519–523. [Google Scholar] [CrossRef]
- Lally, S.; Tan, C.Y.; Owens, D.; Tomkin, G.H. Messenger RNA levels of genes involved in dysregulation of postprandial lipoproteins in type 2 diabetes: The role of Niemann-Pick C1-like 1, ATP-binding cassette, transporters G5 and G8, and of microsomal triglyceride transfer protein. Diabetologia 2006, 49, 1008–1016. [Google Scholar] [CrossRef] [PubMed]
- Simonen, P.P.; Gylling, H.K.; Miettinen, T.A. Diabetes contributes to cholesterol metabolism regardless of obesity. Diabetes Care 2002, 25, 1511–1515. [Google Scholar] [CrossRef] [PubMed]
- Iuliano, L. Pathways of cholesterol oxidation via non-enzymatic mechanisms. Chem. Phys. Lipids 2011, 164, 457–468. [Google Scholar] [CrossRef]
- Sato, K.; Nakano, K.; Katsuki, S.; Matoba, T.; Osada, K.; Sawamura, T.; Sunagawa, K.; Egashira, K. Dietary cholesterol oxidation products accelerate plaque destabilization and rupture associated with monocyte infiltration/activation via the MCP-1-CCR2 pathway in mouse brachiocephalic arteries: Therapeutic effects of ezetimibe. J. Atheroscler. Thromb. 2012, 19, 986–998. [Google Scholar] [CrossRef] [PubMed]
- Hallikainen, M.; Lyyra-Laitinen, T.; Laitinen, T.; Ågren, J.J.; Pihlajamäki, J.; Rauramaa, R.; Miettinen, T.A.; Gylling, H. Endothelial function in hypercholesterolemic subjects: Effects of plant stanol and sterol esters. Atherosclerosis 2006, 188, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Matsue, Y.; Kamiya, K.; Saito, H.; Saito, K.; Ogasahara, Y.; Maekawa, E.; Konishi, M.; Kitai, T.; Iwata, K.; Jujo, K.; et al. Prevalence and prognostic impact of the coexistence of multiple frailty domains in elderly patients with heart failure: The FRAGILE-HF cohort study. Eur. J. Heart Fail. 2020, 22, 2112–2119. [Google Scholar] [CrossRef]
- Boutin, E.; Natella, P.-A.; Schott, A.-M.; Bastuji-Garin, S.; David, J.-P.; Paillaud, E.; Rolland, Y.; Canouï-Poitrine, F. Interrelations between body mass index, frailty, and clinical adverse events in older community-dwelling women: The EPIDOS cohort study. Clin. Nutr. 2018, 37, 1638–1644. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2021 Update: A Report from the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef]
- Song, J.; Wang, D.; Chen, H.; Huang, X.; Zhong, Y.; Jiang, N.; Chen, C.; Xia, M. Association of Plasma 7-Ketocholesterol with Cardiovascular Outcomes and Total Mortality in Patients with Coronary Artery Disease. Circ. Res. 2017, 120, 1622–1631. [Google Scholar] [CrossRef] [PubMed]
- Sawamura, A.; Okumura, T.; Hiraiwa, H.; Aoki, S.; Kondo, T.; Ichii, T.; Furusawa, K.; Watanabe, N.; Kano, N.; Fukaya, K.; et al. Cholesterol metabolism as a prognostic marker in patients with mildly symptomatic nonischemic dilated cardiomyopathy. J. Cardiol. 2017, 69, 888–894. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Whole Cohort |
|---|---|
| Sex Male | 163 (78%) |
| Age (years) | 66 [61–78] |
| Weight (kg) | 63.3 [57.6–73.3] |
| BMI (kg/m2) | 24.3 [22–26.7] |
| Metabolic syndrome | 74 (36%) |
| Hypertension | 147 (71%) |
| Diabetes | 98 (47%) |
| Dyslipidemia | 186 (89%) |
| Family History | 38 (18%) |
| Smoking | 65 (31%) |
| ACS at index PCI | 79 (38%) |
| T-Chol (mg/dL) | 162 [139.5–196] |
| TG (mg/dL) | 122 [90–168] |
| HDL-C (mg/dL) | 43 [35–51] |
| LDL-C (mg/dL) | 92 [73–118] |
| apoA1 (mg/dL) | 116 [106–128] |
| apoB (mg/dL) | 69 [60–83] |
| Campesterol (μg/mL) | 3.5 [2.7–4.7] |
| Sitosterol (μg/mL) | 1.7 [1.3–2.5] |
| Lathosterol (μg/mL) | 1 [1–1.2] |
| MDA-LDL (U/L) | 66 [51–85] |
| hs-CRP (mg/dL) | 0.24 [0.09–0.49] |
| BNP (pg/mL) | 52.3 [18.9–118.3] |
| Uric acid (mg/dL) | 5.7 [4.9–6.6] |
| Creatinine (mg/dL) | 0.82 [0.7–0.98] |
| Glucose (mg/dL) | 110 [95–133] |
| HbA1C (%) | 5.9 [5.4–6.7] |
| β-Blocker | 126 (61%) |
| ACE inhibitor | 63 (30%) |
| ARB | 80 (38%) |
| CCB | 87 (42%) |
| Nitrate | 42 (20%) |
| Antidiabetics | 71 (34%) |
| Insulin | 19 (9%) |
| Statins before entry | 131 (62%) |
| Dietary oxysterol (ng/mL) | 738 [513–1121] |
| β-epoxy-C (ng/mL) | 121 [75–178] |
| β-TRIOL (ng/mL) | 119 [85–175] |
| 7β-OH-C (ng/mL) | 101 [65–203] |
| 7-keto-C (ng/mL) | 323 [215–582] |
| Intrinsic oxysterol (ng/mL) | 522 [434–664] |
| 4β-OH-C (ng/mL) | 91 [61–125] |
| 22R-OH-C (ng/mL) | 0.31 [0–0.04] |
| 24-OH-C (ng/mL) | 21 [14–36] |
| 27-OH-C (ng/mL) | 401 [323–489] |
| Dietary and intrinsic (ng/mL) | 174 [122–299] |
| 7α-OH-C (ng/mL) | 152 [106–267] |
| 25-OH-C (ng/mL) | 22 [13–39] |
| Total oxysterol (ng/mL) | 1507 [1174–2036] |
| Campesterol | ||||
|---|---|---|---|---|
| Low (n = 107) | High (n = 100) | p Value | ||
| Lipid Profiles | ||||
| T-Chol, (mg/dL) | 156 ± 39 | 168 ± 38 | 0.01 | |
| TG, (mg/dL) | 129 ± 75 | 113 ± 75 | 0.83 | |
| HDL-C, (mg/dL) | 41 ± 12 | 45 ± 12 | <0.01 | |
| LDL-C, (mg/dL) | 85 ± 32 | 98 ± 35 | 0.049 | |
| MDA-LDL, (U/I) | 73 ± 29 | 67 ± 24 | 0.23 | |
| Oxysterols, (ng/mL) | Origin | |||
| Total oxysterol | 1422 ± 1071 | 1569 ± 1400 | 0.025 | |
| β-epoxy-C | N | 115 ± 157 | 130 ± 131 | 0.67 |
| TRIOL | N | 106 ± 138 | 130 ± 99 | 0.035 |
| 4β-OH-C | E | 84 ± 60 | 96 ± 49 | 0.046 |
| 7α-OH-C | E/N | 138 ± 206 | 158 ± 196 | <0.001 |
| 7β-OH-C | N | 90 ± 139 | 119 ± 194 | 0.03 |
| 7-keto-C | N | 299 ± 581 | 375 ± 814 | 0.02 |
| 22R-OH-C | E | 0.38 ± 1.9 | 0.22 ± 0.55 | 0.74 |
| 24-OH-C | E | 19 ± 42 | 24 ± 38 | 0.02 |
| 25-OH-C | E/N | 19 ± 55 | 26 ± 63 | 0.054 |
| 27-OH-C | E | 389 ± 158 | 409 ± 140 | 0.31 |
| Lathosterol | ||||
|---|---|---|---|---|
| Low (n = 174) | High (n = 33) | p Value | ||
| Lipid Profiles | ||||
| T-Chol, (mg/dL) | 168 ± 40 | 178 ± 33 | 0.19 | |
| TG, (mg/dL) | 135 ± 71 | 165 ± 75 | 0.027 | |
| HDL-C, (mg/dL) | 44 ± 12 | 43 ± 11 | 0.83 | |
| LDL-C, (mg/dL) | 97 ± 34 | 100 ± 28 | 0.56 | |
| MDA-LDL, (U/I) | 68 ± 26 | 80 ± 28 | 0.018 | |
| Oxysterols, (ng/mL) | Origin | |||
| Total oxysterol | 1710 ± 1142 | 2528 ± 1556 | 0.001 | |
| β-epoxy-C | N | 144 ± 117 | 218 ± 236 | 0.007 |
| TRIOL | N | 148 ± 117 | 159 ± 140 | 0.63 |
| 4β-OH-C | E/N | 98 ± 54 | 105 ± 63 | 0.49 |
| 7α-OH-C | E/N | 183 ± 180 | 340 ± 246 | <0.001 |
| 7β-OH-C | N | 149 ± 151 | 240 ± 231 | 0.005 |
| 7-keto-C | N | 494 ± 671 | 848 ± 831 | 0.008 |
| 22R-OH-C | E | 0.31 ± 1.5 | 0.31 ± 0.9 | 0.99 |
| 24-OH-C | E | 31 ± 38 | 50 ± 45 | 0.014 |
| 25-OH-C | E/N | 35 ± 45 | 69 ± 103 | 0.027 |
| 27-OH-C | E | 418 ± 145 | 489 ± 163 | 0.013 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akiyama, Y.; Katsuki, S.; Matoba, T.; Nakano, Y.; Takase, S.; Nakashiro, S.; Yamamoto, M.; Mukai, Y.; Inoue, S.; Oi, K.; et al. Association of Serum Oxysterols with Cholesterol Metabolism Markers and Clinical Factors in Patients with Coronary Artery Disease: A Covariance Structure Analysis. Nutrients 2023, 15, 2997. https://doi.org/10.3390/nu15132997
Akiyama Y, Katsuki S, Matoba T, Nakano Y, Takase S, Nakashiro S, Yamamoto M, Mukai Y, Inoue S, Oi K, et al. Association of Serum Oxysterols with Cholesterol Metabolism Markers and Clinical Factors in Patients with Coronary Artery Disease: A Covariance Structure Analysis. Nutrients. 2023; 15(13):2997. https://doi.org/10.3390/nu15132997
Chicago/Turabian StyleAkiyama, Yusuke, Shunsuke Katsuki, Tetsuya Matoba, Yasuhiro Nakano, Susumu Takase, Soichi Nakashiro, Mitsutaka Yamamoto, Yasushi Mukai, Shujiro Inoue, Keiji Oi, and et al. 2023. "Association of Serum Oxysterols with Cholesterol Metabolism Markers and Clinical Factors in Patients with Coronary Artery Disease: A Covariance Structure Analysis" Nutrients 15, no. 13: 2997. https://doi.org/10.3390/nu15132997
APA StyleAkiyama, Y., Katsuki, S., Matoba, T., Nakano, Y., Takase, S., Nakashiro, S., Yamamoto, M., Mukai, Y., Inoue, S., Oi, K., Higo, T., Takemoto, M., Suematsu, N., Eshima, K., Miyata, K., Usui, M., Sadamatsu, K., Kadokami, T., Hironaga, K., ... Tsutsui, H. (2023). Association of Serum Oxysterols with Cholesterol Metabolism Markers and Clinical Factors in Patients with Coronary Artery Disease: A Covariance Structure Analysis. Nutrients, 15(13), 2997. https://doi.org/10.3390/nu15132997