
Poor Appetite in Frail Older Persons—A Systematic Review




Abstract
1. Introduction
2. Methods
2.1. Registration, Search Strategy and Eligibility for Inclusion
- ((frail* [Title/Abstract]) AND (appetite [Title/Abstract])) OR
- ((frail* [Title/Abstract]) AND (“anorexia of ageing” [Title/Abstract])) OR
- ((frail* [Title/Abstract]) AND (anorexia [Title/Abstract])) OR
- ((frail* [Title/Abstract]) AND (CNAQ [Title/Abstract])) OR
- ((frail* [Title/Abstract]) AND (Council on Nutrition Appetite Questionnaire [Title/Abstract])) OR
- ((frail* [Title/Abstract]) AND (SNAQ [Title/Abstract])) OR
- ((frail* [Title/Abstract]) AND (Simplified Nutritional Appetite Questionnaire [Title/Abstract])) OR
- ((frail* [Title/Abstract]) AND (“loss of appetite” [Title/Abstract]))
2.2. Appetite and Frailty Assessment Inventories
2.3. Statistical Analysis
3. Results
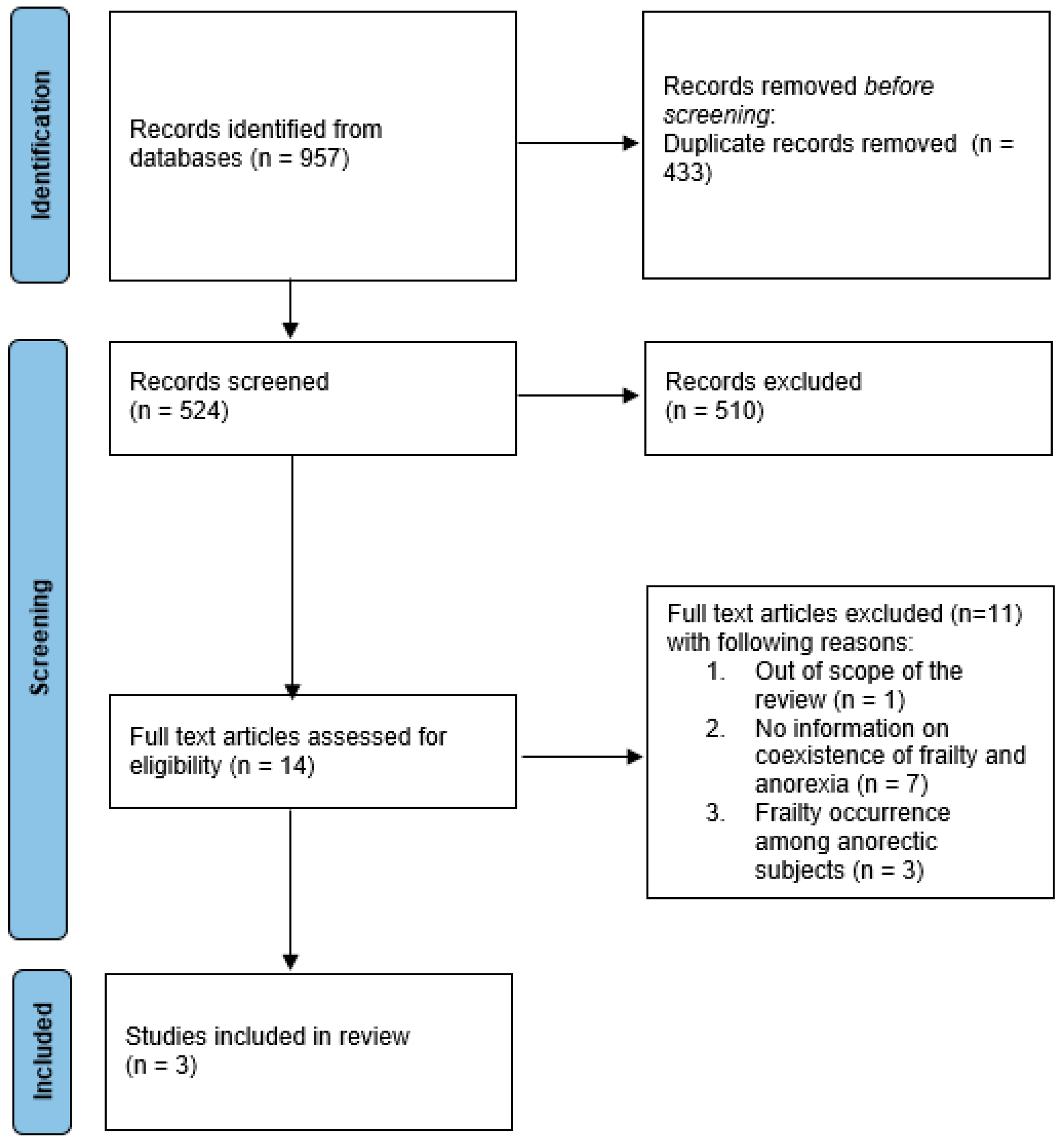
3.1. Description of Included Studies
3.2. Anorexia of Ageing–Prevalence and Probability of Co-Exitence with Frailty
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
PROSPERO registration
Conflicts of Interest
References
- Roy, M.; Gaudreau, P.; Payette, H. A scoping review of anorexia of aging correlates and their relevance to population health interventions. Appetite 2016, 105, 688–699. [Google Scholar] [CrossRef]
- Cox, N.J.; Morrison, L.; Ibrahim, K.; Robinson, S.M.; Sayer, A.A.; Roberts, H.C. New horizons in appetite and the anorexia of ageing. Age Ageing 2020, 49, 526–534. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E.; Silver, A.J. Anorexia in the elderly. Neurobiol. Aging 1988, 9, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Russo, A.; Liperoti, R.; Tosato, M.; Barillaro, C.; Pahor, M.; Bernabei, R.; Onder, G. Anorexia, physical function, and incident disability among the frail elderly population: Results from the ilSIRENTE study. J. Am. Med. Dir. Assoc. 2010, 11, 268–274. [Google Scholar] [CrossRef]
- İlhan, B.; Bahat, G.; Erdoğan, T.; Kiliç, C.; Karan, M.A. Anorexia is Independently Associated with Decreased Muscle Mass and Strength in Community Dwelling Older Adults. J. Nutr. Health Aging 2019, 23, 202–206. [Google Scholar] [CrossRef]
- Dent, E.; Martin, F.C.; Bergman, H.; Woo, J.; Romero-Ortuno, R.; Walston, J.D. Management of frailty: Opportunities, challenges, and future directions. Lancet 2019, 394, 1376–1386. [Google Scholar] [CrossRef]
- Morley, J.E.; Vellas, B.; van Kan, G.A.; Anker, S.D.; Bauer, J.M.; Bernabei, R.; Cesari, M.; Chumlea, W.C.; Doehner, W.; Evans, J.; et al. Frailty consensus: A call to action. J. Am. Med. Dir. Assoc 2013, 14, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Ligthart-Melis, G.C.; Luiking, Y.C.; Kakourou, A.; Cederholm, T.; Maier, A.B.; de van der Schueren, M.A.E. Frailty, Sarcopenia, and Malnutrition Frequently (Co-)occur in Hospitalized Older Adults: A Systematic Review and Meta-analysis. J. Am. Med. Dir. Assoc. 2020, 21, 1216–1228. [Google Scholar] [CrossRef]
- High, K.P. Micronutrient Supplementation and Immune Function in the Elderly. Clin. Infect. Dis. 1999, 28, 717–722. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 29, 372:n71. [Google Scholar]
- Checklist for Prevalence Studies. Available online: https://jbi.global/critical-appraisal-tools (accessed on 14 May 2023).
- Wilson, M.M.; Thomas, D.R.; Rubenstein, L.Z.; Chibnall, J.T.; Anderson, S.; Baxi, A.; Diebold, M.R.; Morley, J.E. Appetite assessment: Simple appetite questionnaire predicts weight loss in community-dwelling adults and nursing home residents. Am. J. Clin. Nutr. 2005, 82, 1074–1081. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E.; Malmstrom, T.K.; Miller, D.K. A simple frailty questionnaire (FRAIL) predicts outcomes in middle aged African Americans. J. Nutr. Health Aging 2012, 16, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Aprahamian, I.; Cezar, N.O.C.; Izbicki, R.; Lin, S.M.; Paulo, D.L.V.; Fattori, A.; Biella, M.M.; Jacob Filho, W.; Yassuda, M.S. Screening for Frailty with the FRAIL Scale: A Comparison with the Phenotype Criteria. J. Am. Med. Dir. Assoc. 2017, 18, 592–596. [Google Scholar] [CrossRef]
- de Lima, E.S.; Zukeran, M.S.; Valentini Neto, J.; Romanini, C.V.; Mingardi, S.V.B.; Cipolli, G.C.; Aprahamian, I.; Ribeiro, S.M.L. Factors related to malnutrition and their association with frailty in community-dwelling older adults registered at a geriatric clinic. Exp. Gerontol. 2022, 165, 111865. [Google Scholar] [CrossRef] [PubMed]
- Tsutsumimoto, K.; Doi, T.; Makizako, H.; Hotta, R.; Nakakubo, S.; Makino, K.; Suzuki, T.; Shimada, H. The association between anorexia of aging and physical frailty: Results from the national center for geriatrics and gerontology’s study of geriatric syndromes. Maturitas 2017, 97, 32–37. [Google Scholar] [CrossRef]
- Alex, D.; Fauzi, A.B.; Mohan, D. Online Multi-Domain Geriatric Health Screening in Urban Community Dwelling Older Malaysians: A Pilot Study. Front. Public Health 2021, 8, 612154. [Google Scholar] [CrossRef]
- Nakakubo, S.; Doi, T.; Tsutsumimoto, K.; Kurita, S.; Ishii, H.; Suzuki, T.; Shimada, H. The Association of Sleep Habits and Advancing Age in Japanese Older Adults: Results from the National Center for Geriatrics and Gerontology Study of Geriatric Syndromes. Gerontology 2022, 68, 209–213. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Galvin, J.E.; Roe, C.M.; Powlishta, K.K.; Coats, M.A.; Muich, S.J.; Grant, E.; Miller, J.P.; Storandt, M.; Morris, J.C. The AD8: A brief informant interview to detect dementia. Neurology 2005, 65, 559–564. [Google Scholar] [CrossRef]
- Aprahamian, I.; Mamoni, R.L.; Cervigne, N.K.; Augusto, T.M.; Romanini, C.V.; Petrella, M.; da Costa, D.L.; Lima, N.A.; Borges, M.K.; Oude Voshaar, R.C. Design and protocol of the multimorbidity and mental health cohort study in frailty and aging (MiMiCS-FRAIL): Unraveling the clinical and molecular associations between frailty, somatic disease burden and late life depression. BMC Psychiatry 2020, 20, 573. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Moola, S.; Lisy, K.; Riitano, D.; Tufanaru, C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int. J. Evid. Based Healthc. 2015, 13, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E.; Levine, A.S.; Gosnell, B.A.; Mitchell, J.E.; Krahn, D.D.; Nizielski, S.E. Peptides and feeding. Peptides 1985, 6, 181–192. [Google Scholar] [CrossRef]
- Zukeran, M.S.; Valentini Neto, J.; Romanini, C.V.; Mingardi, S.V.B.; Cipolli, G.C.; Aprahamian, I.; Lima Ribeiro, S.M. The association between appetite loss, frailty, and psychosocial factors in community-dwelling older adults adults. Clin. Nutr. ESPEN 2022, 47, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Tsutsumimoto, K.; Doi, T.; Makizako, H.; Hotta, R.; Nakakubo, S.; Makino, K.; Suzuki, T.; Shimada, H. Aging-related anorexia and its association with disability and frailty. J. Cachexia Sarcopenia Muscle 2018, 9, 834–843. [Google Scholar] [CrossRef] [PubMed]
- Scheufele, P.; Rappl, A.; Visser, M.; Kiesswetter, E.; Volkert, D. Characterisation of community-dwelling older adults with poor appetite. Eur. J. Nutr 2023. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- van der Meij, B.S.; Wijnhoven, H.A.H.; Lee, J.S.; Houston, D.K.; Hue, T.; Harris, T.B.; Kritchevsky, S.B.; Newman, A.B.; Visser, M. Poor Appetite and Dietary Intake in Community-Dwelling Older Adults. J. Am. Geriatr. Soc. 2017, 65, 2190–2197. [Google Scholar] [CrossRef]
- Donini, L.M.; Dominguez, L.J.; Barbagallo, M.; Savina, C.; Castellaneta, E.; Cucinotta, D.; Fiorito, A.; Inelmen, E.M.; Sergi, G.; Enzi, G.; et al. Senile anorexia in different geriatric settings in Italy. J. Nutr. Health Aging 2011, 15, 775–781. [Google Scholar] [CrossRef]
- Pilgrim, A.L.; Baylis, D.; Jameson, K.A.; Cooper, C.; Sayer, A.A.; Robinson, S.M.; Roberts, H.C. Measuring Appetite with the Simplified Nutritional Appetite Questionnaire Identifies Hospitalised Older People at Risk of Worse Health Outcomes. J. Nutr. Health Aging 2016, 20, 3–7. [Google Scholar] [CrossRef] [PubMed]
- de Souto Barreto, P.; Cesari, M.; Morley, J.E.; Roberts, S.; Landi, F.; Cederholm, T.; Rolland, Y.; Vellas, B.; Fielding, R. Appetite Loss and Anorexia of Aging in Clinical Care: An ICFSR Task Force Report. J. Frailty Aging 2022, 11, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.N.; Fries, B.E.; Steel, K.; Ikegami, N.; Bernabei, R.; Carpenter, G.I.; Gilgen, R.; Hirdes, J.P.; Topinková, E. Comprehensive clinical assessment in community setting: Applicability of the MDS-HC. J. Am. Geriatr. Soc. 1997, 45, 1017–1024. [Google Scholar] [CrossRef] [PubMed]
- Volkert, D.; Chourdakis, M.; Faxen-Irving, G.; Frühwald, T.; Landi, F.; Suominen, M.H.; Vandewoude, M.; Wirth, R.; Schneider, S.M. ESPEN guidelines on nutrition in dementia. Clin. Nutr. 2015, 34, 1052–1073. [Google Scholar] [CrossRef]
- Watson, R.; MacDonald, J.; McReady, T. The Edinburgh Feeding Evaluation in Dementia Scale #2 (EdFED #2): Inter- and intra-rater reliability. Clin. Eff. Nurs. 2001, 5, 184–186. [Google Scholar]
- Hybels, C.F.; Landerman, L.R.; Blazer, D.G. Age differences in symptom expression in patients with major depression: Age differences in depressive symptoms. Int. J. Geriatr. Psychiatry 2012, 27, 601–611. [Google Scholar] [CrossRef]
- Kwan, R.Y.C.; Leung, A.Y.M.; Yee, A.; Lau, L.T.; Xu, X.Y.; Dai, D.L.K. Cognitive Frailty and Its Association with Nutrition and Depression in Community-Dwelling Older People. J. Nutr. Health Aging 2019, 23, 943–948. [Google Scholar] [CrossRef]
- Aprahamian, I.; Romanini, C.V.; Lima, N.A.; An, V.N.; Aguirre, B.N.; Galdeano, J.R.; da Costa, D.L.; Petrella, M.; Ribeiro, S.M.L.; Borges, M.K.; et al. The concept of anorexia of aging in late life depression: A cross-sectional analysis of a cohort study. Arch. Gerontol. Geriatr. 2021, 95, 104410. [Google Scholar] [CrossRef]
- Rockwood, K. A global clinical measure of fitness and frailty in elderly people. Can. Med. Assoc. J. 2005, 173, 489–495. [Google Scholar] [CrossRef]
- Dent, E.; Morley, J.E.; Cruz-Jentoft, A.J.; Woodhouse, L.; Rodríguez-Mañas, L.; Fried, L.P.; Woo, J.; Aprahamian, I.; Sanford, A.; Lundy, J.; et al. Physical Frailty: ICFSR International Clinical Practice Guidelines for Identification and Management. J. Nutr. Health Aging 2019, 23, 771–787. [Google Scholar] [CrossRef]
- Rolfson, D.; Majumdar, S.; Tsuyuki, R.; Tahir, A.; Rockwood, K. Validity and reliability of the Edmonton Frail Scale. Age Ageing 2006, 35, 526–529. [Google Scholar] [CrossRef] [PubMed]
- Cox, N.; Ibrahim, K.; Sayer, A.; Robinson, S.; Roberts, H. Assessment and Treatment of the Anorexia of Aging: A Systematic Review. Nutrients 2019, 11, 144. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author, Publication Year (Reference) | Cohort | Frailty | Appetite according to Frailty Status | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Country | Setting | Age * <minimum, (Mean [SD]) Years | Tool (Reference) | % (n) | Tool | Anorexia of Ageing (%) within Frailty Status Group (n) | p | SNAQ Mean (SD) | ||
| 1. | Tsutsumimoto et al., 2017 [17] | 4417 | Japan | Community | ≥70 (75.8 [4.3]) | Fried et al. [13] | FRAIL 10.7% (472) | Simplified nutritional appetite questionnaire (SNAQ); cut-off: ≤13 | Among frail participants: 21.2% (100) | <0.001 (ANOVA) | 14.5 (1.5) |
| PRE-FRAIL 19.3% (853) | Among pre-frail participants: 14.8% (126) | 15.0 (1.5) | |||||||||
| NON-FRAIL 70% (3092) | Among non-frail participants: 7.9% (244) | 15.5 (1.4) | |||||||||
| 2. | Alex et al., 2021 [18] | 134 | Malaysia | Online survey | ≥60 (66.4 [5.3]) | FRAIL [14] | FRAIL: 4.5% (6) | Simplified nutritional appetite questionnaire (SNAQ); cut-off: ≤14 | Among frail and pre-frail participants: 24.1% (21) | 0.007 | … |
| PRE-FRAIL: 30.6% (41) | … | ||||||||||
| NON-FRAIL: 64.9% (87) | Among non-frail participants: 48.9% (23) | … | |||||||||
| 3. | de Lima et al., 2022 [16] | 106 | Brazil | Community | ≥60 (71.4 [8.0]) | FRAIL-BR [15] | FRAIL: 31.1% (33) | Simplified nutritional appetite questionnaire (SNAQ); cut-off: ≤14 | Among frail participants: 33.3% (11) | 0.005 (ANOVA) | … |
| PRE-FRAIL: 30.2% (32) | Among pre-frail participants: 28.1% (9) | … | |||||||||
| NON-FRAIL: 38.7% (41) | Among non-frail participants: 2.4% (1) | … | |||||||||
| Tsutsumimoto et al., 2017 [17] | Alex et al., 2021 [18] | De Lima et al., 2022 [16] | |
|---|---|---|---|
| Was the sample frame appropriate to address the target population? | Yes | Yes | Yes |
| Were study participants sampled in an appropriate way? | Unclear | No | No |
| Was the sample size adequate? | Unclear | Unclear | Unclear |
| Were the study subjects and the setting described in detail? | Yes | Yes | Yes |
| Was the data analysis conducted with sufficient coverage of the identified sample? | Yes | Yes | Yes |
| Were valid methods used for the identification of the condition? | Yes | Yes | Yes |
| Was the condition measured in a standard, reliable way for all participants? | Unclear | Yes | Yes |
| Was there appropriate statistical analysis? | Yes | Yes | Yes |
| Was the response rate adequate, and if not, was the low response rate managed appropriately? | Unclear | Yes | Yes |
| Overall quality | Moderate | Moderate | Moderate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rudzińska, A.; Piotrowicz, K.; Perera, I.; Gryglewska, B.; Gąsowski, J. Poor Appetite in Frail Older Persons—A Systematic Review. Nutrients 2023, 15, 2966. https://doi.org/10.3390/nu15132966
Rudzińska A, Piotrowicz K, Perera I, Gryglewska B, Gąsowski J. Poor Appetite in Frail Older Persons—A Systematic Review. Nutrients. 2023; 15(13):2966. https://doi.org/10.3390/nu15132966
Chicago/Turabian StyleRudzińska, Anna, Karolina Piotrowicz, Ian Perera, Barbara Gryglewska, and Jerzy Gąsowski. 2023. "Poor Appetite in Frail Older Persons—A Systematic Review" Nutrients 15, no. 13: 2966. https://doi.org/10.3390/nu15132966
APA StyleRudzińska, A., Piotrowicz, K., Perera, I., Gryglewska, B., & Gąsowski, J. (2023). Poor Appetite in Frail Older Persons—A Systematic Review. Nutrients, 15(13), 2966. https://doi.org/10.3390/nu15132966