
Prevalence of Malnutrition in People with Dementia in Long-Term Care: A Systematic Review and Meta-Analysis

Abstract
1. Introduction
2. Materials and Methods
2.1. Information Sources
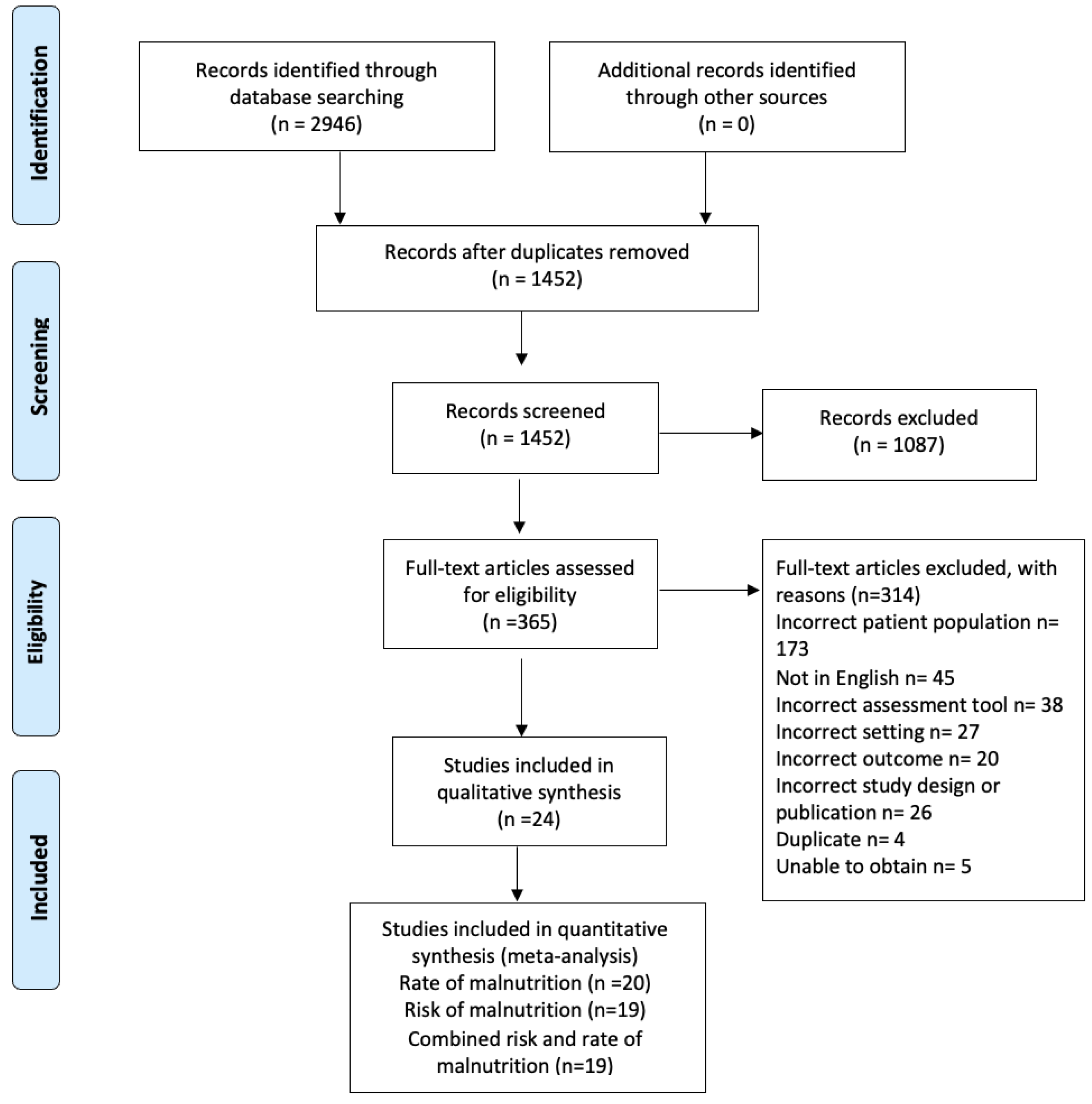
2.2. Study Selection
2.3. Data Extraction and Summary Measures
2.4. Quality Appraisal
2.5. Results Synthesis
3. Results
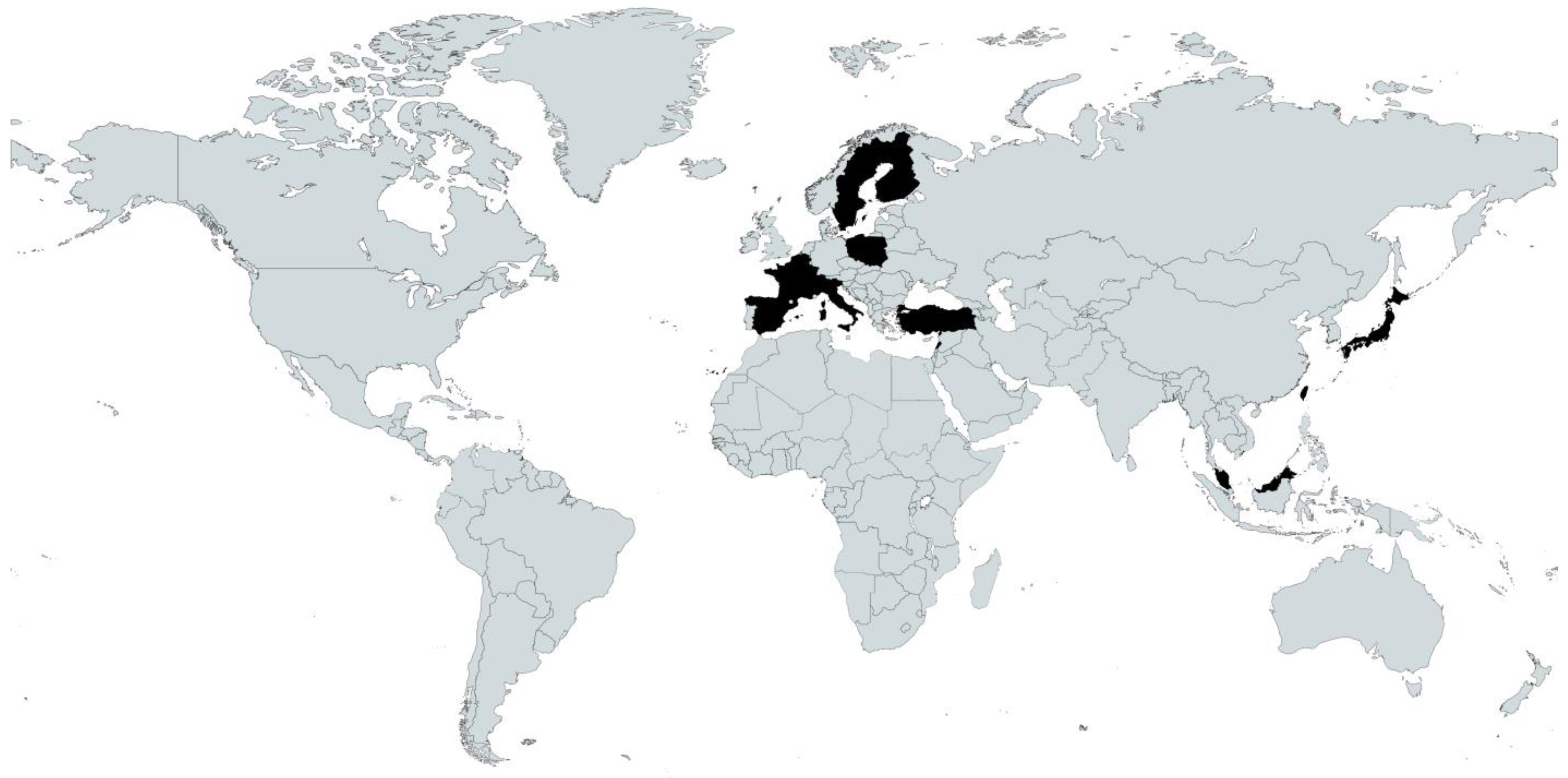
3.1. Participants
3.2. Assessment Tools Used
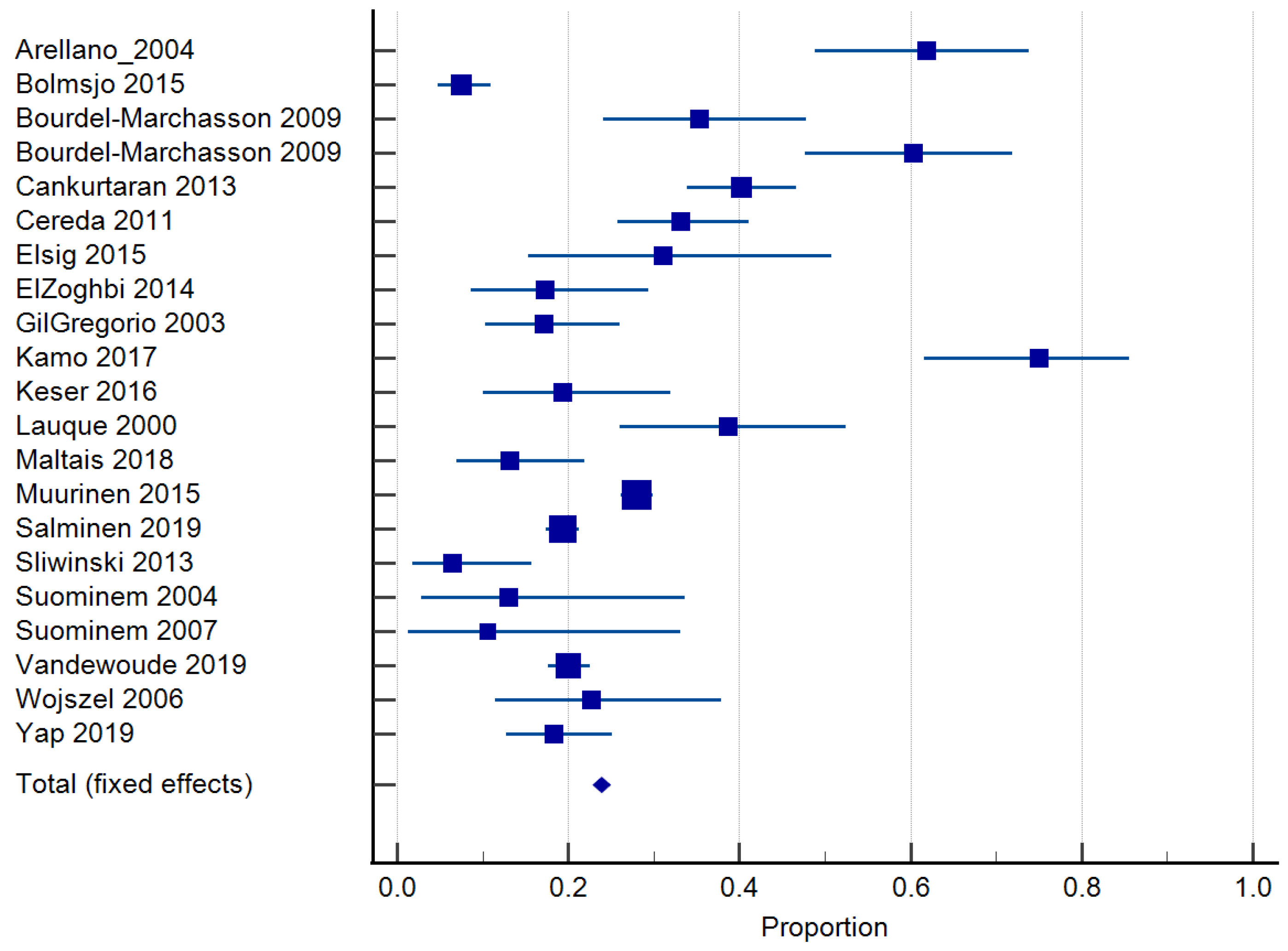
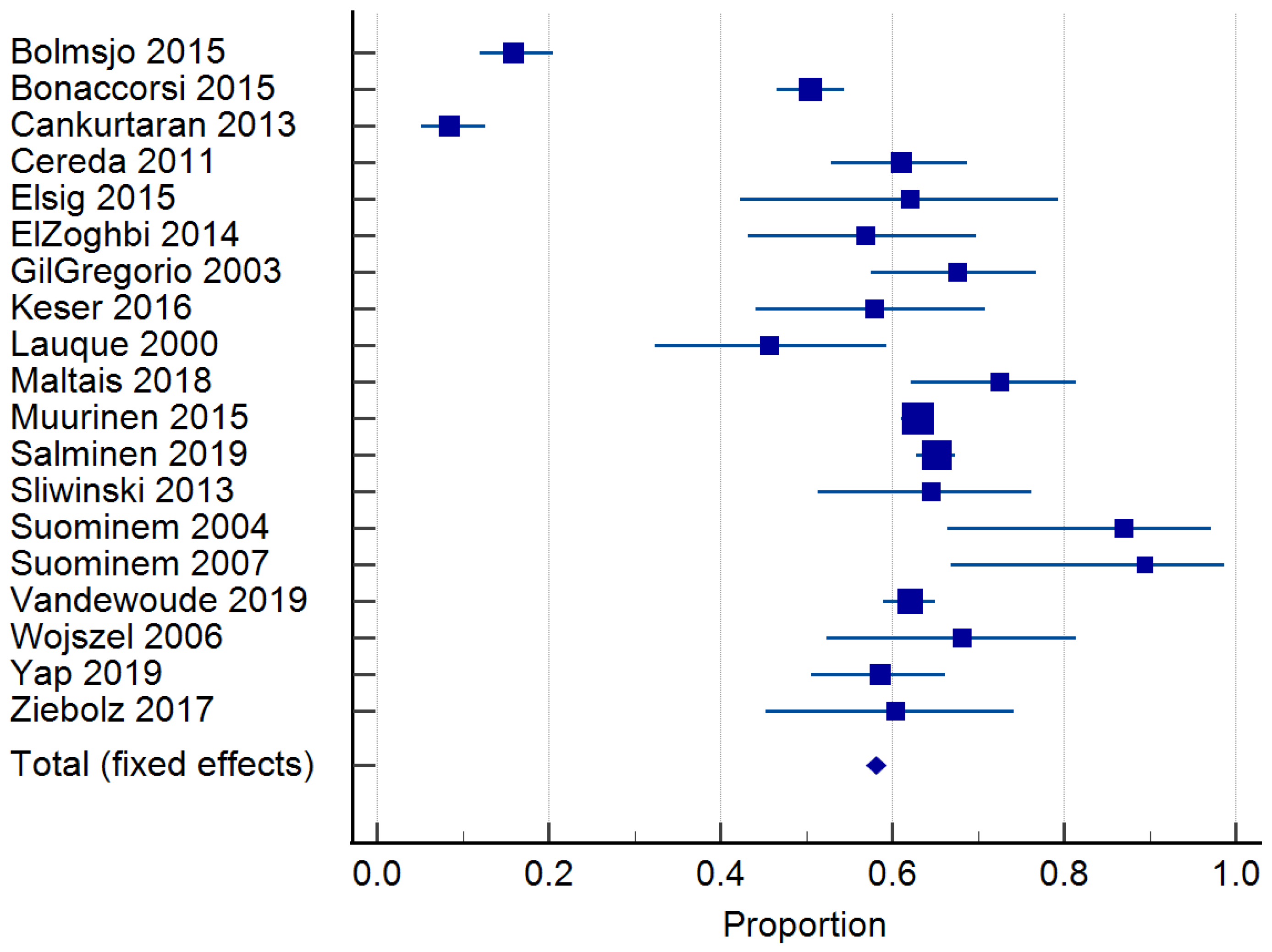
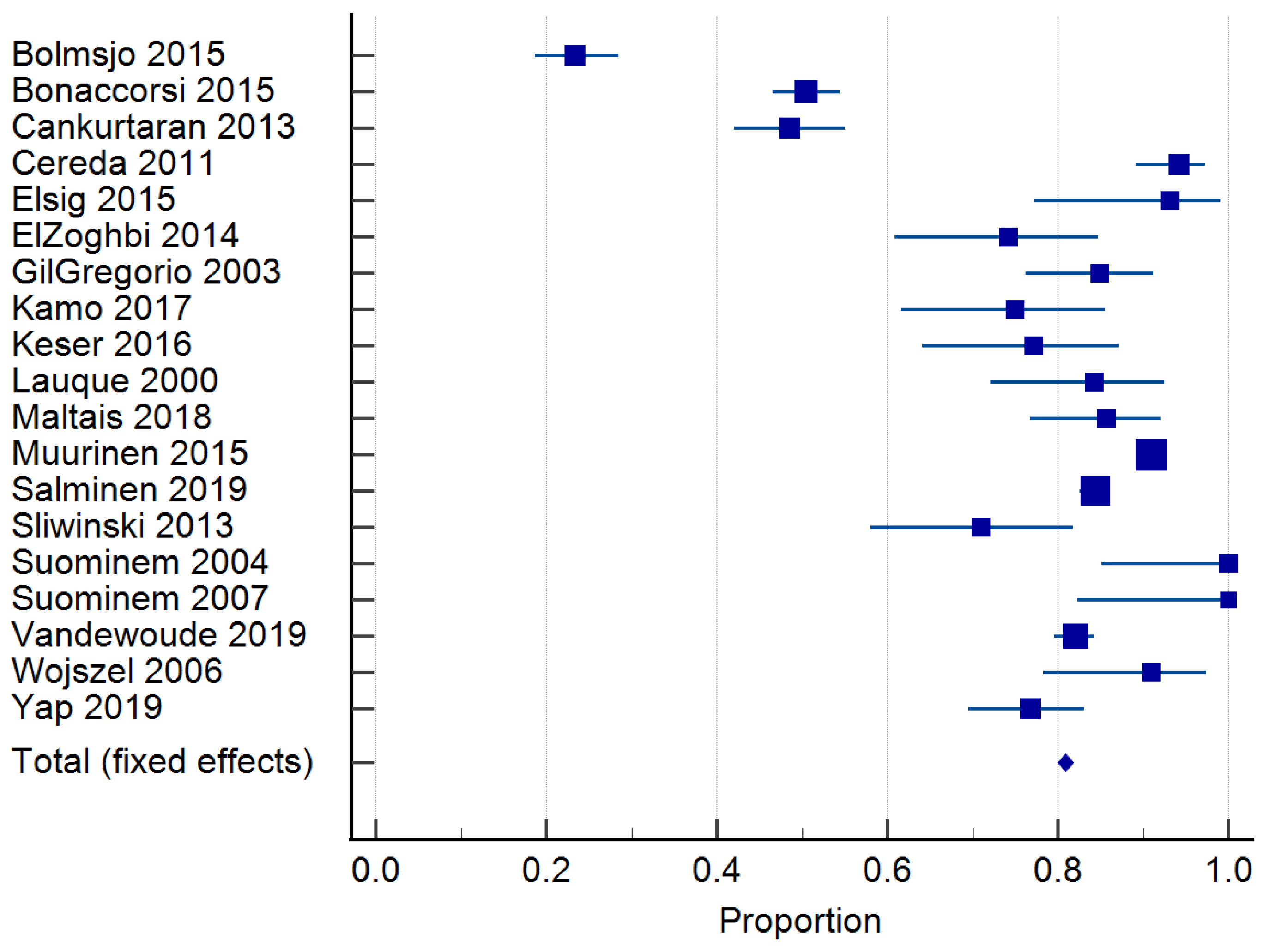
3.3. Prevalence of Malnutrition
3.4. Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organisation. Dementia: A Public Health Priority. Available online: https://apps.who.int/iris/handle/10665/75263 (accessed on 25 June 2023).
- Alzheimers Association. 2022 Alzheimer’s disease facts and figures. Alzheimer Dement. 2022, 18, 700–789. [Google Scholar] [CrossRef]
- Prince, M.; Bryce, R.; Albanese, E.; Wimo, A.; Ribeiro, W.; Ferri, C.P. The global prevalence of dementia: A systematic review and metaanalysis. Alzheimer’s Dement. 2013, 9, 63–75. [Google Scholar] [CrossRef] [PubMed]
- Prince, M.; Wimo, A.; Guerchet, M.; Ali, G.-C.; Wu, Y.-T.; Prina, M. World Alzheimer Report 2015. The Global Impact of Dementia. An Analysis of Prevalence, Incidence, Cost & Trends. Available online: https://www.alzint.org/u/WorldAlzheimerReport2015.pdf (accessed on 25 June 2023).
- Chowdhary, N.; Barbui, C.; Anstey, K.; Kivipelto, M.; Barbera, M.; Peters, R.; Zheng, L.; Kulmala, J.; Stephen, R.; Ferri, C.; et al. Reducing the Risk of Cognitive Decline and Dementia: WHO Recommendations. Front. Neurol. 2022, 12, 765584. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, C.C.G.; Lucetti, C.; Danti, S.; Nuti, A. Eating Behaviors and Dietary Changes in Patients With Dementia. Am. J. Alzheimer’s Dis. Dement. 2016, 31, 706–716. [Google Scholar] [CrossRef] [PubMed]
- Hanson, L.C.; Ersek, M.; Lin, F.C.; Carey, T.S. Outcomes of feeding problems in advanced dementia in a nursing home population. J. Am. Geriatr. Soc. 2013, 61, 1692–1697. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Dementia in Australia. Available online: https://www.aihw.gov.au/reports/dementia/dementia-in-aus/contents/aged-care-and-support-services-used-by-people-with-dementia/residential-aged-care (accessed on 25 June 2023).
- Soeters, P.; Bozzetti, F.; Cynober, L.; Forbes, A.; Shenkin, A.; Sobotka, L. Defining malnutrition: A plea to rethink. Clin. Nutr. 2017, 36, 896–901. [Google Scholar] [CrossRef]
- Chang, C.-C.; Roberts, B.L. Malnutrition and feeding difficulty in Taiwanese older with dementia. J. Clin. Nurs. 2011, 20, 2153–2161. [Google Scholar] [CrossRef]
- Arellano, M.; Garcia-Caselles, M.P.; Pi-Figueras, M.; Miralles, R.; Torres, R.M.; Aguilera, A.; Cervera, A.M. Clinical impact of different scores of the Mini Nutritional Assessment (MNA) in the diagnosis of malnutrition in patients with cognitive impairment. Arch. Gerontol. Geriatr. 2004, 38, 27–31. [Google Scholar] [CrossRef]
- Harris, D. Malnutrition screening in the elderly population. J. R. Soc. Med. 2005, 98, 411–414. [Google Scholar] [CrossRef]
- Winter, J.; Flanagan, D.; McNaughton, S.A.; Nowson, C. Nutrition screening of older people in a community general practice, using the MNA-SF. J. Nutr. Health Aging 2013, 17, 322–325. [Google Scholar] [CrossRef]
- Keller, H.; Vucea, V.; Slaughter, S.E.; Jager-Wittenaar, H.; Lengyel, C.; Ottery, F.D.; Carrier, N. Prevalence of Malnutrition or Risk in Residents in Long Term Care: Comparison of Four Tools. J. Nutr. Gerontol. Geriatr. 2019, 38, 329–344. [Google Scholar] [CrossRef] [PubMed]
- Khater, M.S.; Abouelezz, N.F. Nutritional status in older adults with mild cognitive impairment living in elderly homes in Cairo, Egypt. J. Nutr. Health Aging 2011, 15, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Khater, M.S.; Mousa, S.M. Predicting falls among Egyptian nursing home residents: A 1-year longitudinal study. J. Clin. Gerontol. Geriatr. 2012, 3, 73–76. [Google Scholar] [CrossRef]
- Velázquez-Alva, M.C.; Irigoyen-Camacho, M.E.; Cabrer-Rosales, M.F.; Lazarevich, I.; Arrieta-Cruz, I.; Gutiérrez-Juárez, R.; Zepeda-Zepeda, M.A. Prevalence of malnutrition and depression in older adults living in nursing homes in Mexico City. Nutrients 2020, 12, 2429. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Chen, S.; Jiang, F.; Zhou, C.; Tang, S. Malnutrition and Physical Frailty among Nursing Home Residents: A Cross-Sectional Study in China. J. Nutr. Health Aging 2020, 24, 500–506. [Google Scholar] [CrossRef] [PubMed]
- Vellas, B.; Guigoz, Y.; Garry, P.J.; Nourhashemi, F.; Bennahum, D.; Lauque, S.; Albarede, J.L. The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition 1999, 15, 116–122. [Google Scholar] [CrossRef]
- Jager-Wittenaar, H.; Ottery, F.D. Assessing nutritional status in cancer. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 322–329. [Google Scholar] [CrossRef]
- Detsky, A.S.; McLaughlin, J.R.; Baker, J.P.; Johnston, N.; Whittaker, S.; Mendelson, R.A.; Jeejeebhoy, K.N. What is subjective global assessment of nutritional status? J. Parenter Enter. Nutr. 1987, 11, 8–13. [Google Scholar] [CrossRef]
- Rubenstein, L.Z.; Harker, J.O.; Salvà, A.; Guigoz, Y.; Vellas, B. Screening for undernutrition in geriatric practice: Developing the short-form mini-nutritional assessment (MNA-SF). J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M366–M372. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Covidence Systematic Review Software, Veritas Health Innovation, Melbourne, Australia. 2022. Available online: www.covidence.org (accessed on 25 June 2023).
- Microsoft Corporation. Microsoft Excel, Office365; Microsoft Corporation: Redmond, WA, USA, 2022. [Google Scholar]
- Handu, D.M.L.; Wolfram, T.; Ziegler, P.; Acosta, A.; Steiber, A. Academy of Nutrition and Dietetics Methodology for Conducting Systematic Reviews for the Evidence Analysis Library. J. Acad. Nutr. Diet. 2016, 116, 311–318. [Google Scholar] [CrossRef] [PubMed]
- MedCalc Software Ltd. MedCalc® Statistical Software; Version 20.010; MedCalc Software Ltd.: Ostend, Belgium, 2021. [Google Scholar]
- Jesus, P.; Desport, J.C.; Massoulard, A.; Villemonteix, C.; Baptiste, A.; Gindre-Poulvelarie, L.; Lorgueuilleux, S.; Javerliat, V.; Fraysse, J.L.; Preux, P.M. Nutritional assessment and follow-up of residents with and without dementia in nursing homes in the Limousin region of France: A health network initiative. J. Nutr. Health Aging 2012, 16, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, M.; Haglin, L.; Rosendahl, E.; Gustafson, Y. Poor nutritional status is associated with urinary tract infection among older people living in residential care facilities. J. Nutr. Health Aging 2013, 17, 186–191. [Google Scholar] [CrossRef]
- Bonaccorsi, G.; Collini, F.; Castagnoli, M.; Di Bari, M.; Cavallini, M.C.; Zaffarana, N.; Pepe, P.; Mugelli, A.; Lucenteforte, E.; Vannacci, A.; et al. A cross-sectional survey to investigate the quality of care in Tuscan (Italy) nursing homes: The structural, process and outcome indicators of nutritional care. BMC Health Serv. Res. 2015, 15, 223. [Google Scholar] [CrossRef]
- Cankurtaran, M.; Saka, B.; Sahin, S.; Varli, M.; Doventas, A.; Yavuz, B.B.; Halil, M.; Curgunlu, A.; Ulger, Z.; Tekin, N.; et al. Turkish nursing homes and care homes nutritional status assessment project (THN-malnutrition). Eur. Geriatr. Med. 2013, 4, 329–334. [Google Scholar] [CrossRef]
- Bourdel-Marchasson, I.; Rolland, C.; Jutand, M.-A.; Egea, C.; Baratchart, B.; Barberger-Gateau, P. Undernutrition in geriatric institutions in South-West France: Policies and risk factors. Nutrition 2009, 25, 155–164. [Google Scholar] [CrossRef]
- Boström, A.-M.; Van Soest, D.; Kolewaski, B.; Milke, D.L.; Estabrooks, C.A. Nutrition Status Among Residents Living in a Veterans’ Long-Term Care Facility in Western Canada: A Pilot Study. J. Am. Med. Dir. Assoc. 2011, 12, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Elsig, F.; Schimmel, M.; Duvernay, E.; Giannelli, S.V.; Graf, C.E.; Carlier, S.; Herrmann, F.R.; Michel, J.P.; Gold, G.; Zekry, D.; et al. Tooth loss, chewing efficiency and cognitive impairment in geriatric patients. Gerodontology 2015, 32, 149–156. [Google Scholar] [CrossRef] [PubMed]
- El Zoghbi, M.; Boulos, C.; Awada, S.; Rachidi, S.; Al-Hajje, A.; Bawab, W.; Saleh, N.; Salameh, P. Prevalence of malnutrition and its correlates in older adults living in long stay institutions situated in Beirut, Lebanon. J. Res. Health Sci. 2014, 14, 11–17. [Google Scholar]
- Keser, A.; Yildirim, F. Evaluation of the relationship between nutritional status and quality of life among nursing home residents with alzheimer’s disease. Improv. Qual. Life Dement. Patients Prog. Detect. Treat. Care 2016, 42–73. [Google Scholar] [CrossRef]
- Muurinen, S.; Savikko, N.; Soini, H.; Suominen, M.; Pitkälä, K. Nutrition and psychological well-being among long-term care residents with dementia. J. Nutr. Health Aging 2015, 19, 178–182. [Google Scholar] [CrossRef] [PubMed]
- Salminen, K.S.; Suominen, M.H.; Soini, H.; Kautiainen, H.; Savikko, N.; Saarela, R.K.T.; Muurinen, S.; Pitkala, K.H. Associations Between Nutritional Status and Health-Related Quality of Life Among Long-Term Care Residents in Helsinki. J. Nutr. Health Aging 2019, 23, 474–478. [Google Scholar] [CrossRef]
- Sliwinski, Z.; Matlok, M.; Starczynska, M.; Makara-Studzinska, M. Mental and physical performance of dementia patients in long-term residential care. Med. Stud. Stud. Med. 2013, 29, 230–233. [Google Scholar] [CrossRef]
- Suominem, M.; Laine, T.; Routasalo, P.; Pitkala, K.H.; Rasanen, L. Nutrient content of served food, nutrient intake and nutritional status of residents with dementia in a finnish nursing home. J. Nutr. Health Aging 2004, 8, 234–238. [Google Scholar] [PubMed]
- Vandewoude, M.F.J.; van Wijngaarden, J.P.; De Maesschalck, L.; Luiking, Y.C.; Van Gossum, A. The prevalence and health burden of malnutrition in Belgian older people in the community or residing in nursing homes: Results of the NutriAction II study. Aging Clin. Exp. Res. 2019, 31, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Yap, S.F.; Boo, N.Y.; Shenoy, P.D.; Liew, S.F.; Woo, L.F.; Choo, P.Y.; Leong, P.P.; Hatta, N.M. Nutritional status of elderly residents of long-term care homes in Klang Valley, Malaysia: A cross-sectional study. Asian J. Gerontol. Geriatr. 2019, 14, 89–95. [Google Scholar] [CrossRef]
- Ziebolz, D.; Werner, C.; Schmalz, G.; Nitschke, I.; Haak, R.; Mausberg, R.F.; Chenot, J.-F. Oral Health and nutritional status in nursing home residents-results of an explorative cross-sectional pilot study. BMC Geriatr. 2017, 17, 39. [Google Scholar] [CrossRef]
- Gil Gregorio, P.; Ramirez Diaz, S.P.; Ribera Casado, J.M.; Tobaruela, J.L.; Neira, R.; Medina, J.; González, P.; Navarro, C.; Robledillo, R.; Moreno, J.; et al. Dementia and nutrition. Intervention study in institutionalized patients with Alzheimer Disease. J. Nutr. Health Aging 2003, 7, 304–308. [Google Scholar]
- Lauque, S.; Arnaud-Battandier, F.; Mansourian, R.; Guigoz, Y.; Paintin, M.; Nourhashemi, F.; Vellas, B. Protein-energy oral supplementation in malnourished nursing-home residents. A controlled trial. Age Ageing 2000, 29, 51–56. [Google Scholar] [CrossRef]
- Maltais, M.; Rolland, Y.; Hay, P.E.; Armaingaud, D.; Cestac, P.; Rouch, L.; Barreto, P.D. The Effect of Exercise and Social Activity Interventions on Nutritional Status in Older Adults with Dementia Living in Nursing Homes: A Randomised Controlled Trial. J. Nutr. Health Aging 2018, 22, 824–828. [Google Scholar] [CrossRef]
- Bolmsjo, B.B.; Jakobsson, U.; Molstad, S.; Ostgren, C.J.; Midlov, P. The nutritional situation in Swedish nursing homes—A longitudinal study. Arch. Gerontol. Geriatr. 2015, 60, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-S.; Lin, S.-Y.; Chou, M.-Y.; Chen, L.-Y.; Wang, K.-Y.; Chen, L.-K.; Lin, Y.-T.; Loh, C.-H. Hospitalization and associated factors in people with Alzheimer’s disease residing in a long-term care facility in southern Taiwan. Geriatr. Gerontol. Int. 2017, 17 (Suppl. S1), 50–56. [Google Scholar] [CrossRef] [PubMed]
- Cereda, E.; Pedrolli, C.; Zagami, A.; Vanotti, A.; Piffer, S.; Opizzi, A.; Rondanelli, M.; Caccialanza, R. Nutritional screening and mortality in newly institutionalised elderly: A comparison between the Geriatric Nutritional Risk Index and the Mini Nutritional Assessment. Clin. Nutr. 2011, 30, 793–798. [Google Scholar] [CrossRef]
- Kamo, T.; Takayama, K.; Ishii, H.; Suzuki, K.; Eguchi, K.; Nishida, Y. Coexisting severe frailty and malnutrition predict mortality among the oldest old in nursing homes: A 1-year prospective study. Arch. Gerontol. Geriatr. 2017, 70, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Suominen, M.H.; Kivisto, S.M.; Pitkala, K.H. The effects of nutrition education on professionals’ practice and on the nutrition of aged residents in dementia wards. Eur. J. Clin. Nutr. 2007, 61, 1226–1232. [Google Scholar] [CrossRef]
- Wojszel, Z.B. Determinants of nutritional status of older people in long-term care settings on the example of the nursing home in Białystok. Adv. Med. Sci. 2006, 51, 168–173. [Google Scholar]
- MapChart.com. World Map—Simple: Create a Custom Map. MapChart. Available online: https://www.mapchart.net/world.html (accessed on 22 May 2023).
- Kaiser, M.J.; Bauer, J.M.; Ramsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.; Charlton, K.E.; Maggio, M.; et al. Validation of the Mini Nutritional Assessment short-form (MNA-SF): A practical tool for identification of nutritional status. J. Nutr. Health Aging 2009, 13, 782–788. [Google Scholar] [CrossRef]
- Stratton, R.J.; Hackston, A.; Longmore, D.; Dixon, R.; Price, S.; Stroud, M.; King, C.; Elia, M. Malnutrition in hospital outpatients and inpatients: Prevalence, concurrent validity and ease of use of the ‘malnutrition universal screening tool’ (‘MUST’) for adults. Br. J. Nutr. 2004, 92, 799–808. [Google Scholar] [CrossRef]
- Plassman, B.L.; Langa, K.M.; McCammon, R.J.; Fisher, G.G.; Potter, G.G.; Burke, J.R.; Steffens, D.C.; Foster, N.L.; Giordani, B.; Unverzagt, F.W.; et al. Incidence of dementia and cognitive impairment, not dementia in the United States. Ann. Neurol. 2011, 70, 418–426. [Google Scholar] [CrossRef]
- Prince, M.; Knapp, M.; Guerchet, M.; McCrone, P.; Prina, M.; Comas Herrera, A.; Wittenberg, A.; Adelaja, R.; Hu, B.; King, B.; et al. Dementia UK Update; Alzheimer’s Society: Plymouth, UK, 2014. [Google Scholar]
- Robb, L.; Walsh, C.M.; Nel, M.; Nel, A.; Odendaal, H.; van Aardt, R. Malnutrition in the elderly residing in long-term care facilities: A cross sectional survey using the Mini Nutritional Assessment (MNA®) screening tool. S. Afr. J. Clin. Nutr. 2017, 30, 34–40. [Google Scholar] [CrossRef]
- Yalcin, A.; Silay, K. Sarcopenia and health-related quality of life in turkish nursing home residents: A cross-sectional study. Asian J. Gerontol. Geriatr. 2017, 12, 42–46. [Google Scholar]
- Eisenmann, Y.; Golla, H.; Schmidt, H.; Voltz, R.; Perrar, K.M. Palliative Care in Advanced Dementia. Front. Psychiatry 2020, 11, 699. [Google Scholar] [CrossRef] [PubMed]
- Cereda, E.; Pedrolli, C.; Klersy, C.; Bonardi, C.; Quarleri, L.; Cappello, S.; Turri, A.; Rondanelli, M.; Caccialanza, R. Nutritional status in older persons according to healthcare setting: A systematic review and meta-analysis of prevalence data using MNA (R). Clin. Nutr. 2016, 35, 1282–1290. [Google Scholar] [CrossRef]
- Donini, L.M.; Neri, B.; De Chiara, S.; Poggiogalle, E.; Muscaritoli, M. Nutritional Care in a Nursing Home in Italy. PLoS ONE 2013, 8, e55804. [Google Scholar] [CrossRef]
- Kabir, Z.N.; Ferdous, T.; Cederholm, T.; Khanam, M.A.; Streatfied, K.; Wahlin, A. Mini Nutritional Assessment of rural elderly people in Bangladesh: The impact of demographic, socio-economic and health factors. Public Health Nutr. 2006, 9, 968–974. [Google Scholar] [CrossRef]
- Crichton, M.; Craven, D.; Mackay, H.; Marx, W.; De Van Der Schueren, M.; Marshall, S. A systematic review, meta-analysis and meta-regression of the prevalence of protein-energy malnutrition: Associations with geographical region and sex. Age Ageing 2018, 48, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Tom, S.E.; Hubbard, R.A.; Crane, P.K.; Haneuse, S.J.; Bowen, J.; McCormick, W.C.; McCurry, S.; Larson, E.B. Characterization of dementia and Alzheimer’s disease in an older population: Updated incidence and life expectancy with and without dementia. Am. J. Public Health 2015, 105, 408–413. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. People Using Aged Care. Available online: https://www.gen-agedcaredata.gov.au/Topics/People-using-aged-care (accessed on 27 September 2022).
- Doorduijn, A.S.; de van der Schueren, M.A.E.; van de Rest, O.; de Leeuw, F.A.; Hendriksen, H.M.A.; Teunissen, C.E.; Scheltens, P.; van der Flier, W.M.; Visser, M. Energy intake and expenditure in patients with Alzheimer’s disease and mild cognitive impairment: The NUDAD project. Alzheimers Res. 2020, 12, 116. [Google Scholar] [CrossRef]
- Spencer, J.C.; Damanik, R.; Ho, M.-H.; Montayre, J.; Traynor, V.; Chang, C.-C.; Chang, H.-C. Review of Food Intake Difficulty Assessment Tools for People with Dementia. West. J. Nurs. Res. 2021, 43, 1132–1145. [Google Scholar] [CrossRef]
- Chang, C.-C.; Lin, Y.-F.; Chiu, C.-H.; Liao, Y.-M.; Ho, M.-H.; Lin, Y.-K.; Chou, K.-R.; Liu, M.F. Prevalence and factors associated with food intake difficulties among residents with dementia. PLoS ONE 2017, 12, e0171770. [Google Scholar] [CrossRef]
- Namasivayam, A.M.; Steele, C.M. Malnutrition and Dysphagia in Long-Term Care: A Systematic Review. J. Nutr. Gerontol. Geriatr. 2015, 34, 1–21. [Google Scholar] [CrossRef]
- KS, S.; MH, S.; H, K.; HM, R.; KH, P. Energy Intake and Severity of Dementia Are Both Associated with Health-Related Quality of Life among Older Long-Term Care Residents. Nutrients 2019, 11, 2261. [Google Scholar] [CrossRef]
- Kondrup, J.; Allison, S.P.; Elia, M.; Vellas, B.; Plauth, M. ESPEN Guidelines for Nutrition Screening 2002. Clin. Nutr. 2003, 22, 415–421. [Google Scholar] [CrossRef]
- Kellett, J.; Kyle, G.; Itsiopoulos, C.; Naunton, M. Nutrition screening practices amongst australian Residential Aged Care Facilities. J. Nutr. Health Aging 2016, 20, 1040–1044. [Google Scholar] [CrossRef] [PubMed]
- Baek, M.-H.; Heo, Y.-R. Evaluation of the efficacy of nutritional screening tools to predict malnutrition in the elderly at a geriatric care hospital. Nutr. Res. Pract. 2015, 9, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Rodríguez, D.; Annweiler, C.; Ronquillo-Moreno, N.; Tortosa-Rodríguez, A.; Guillén-Solà, A.; Vázquez-Ibar, O.; Escalada, F.; Muniesa, J.M.; Marco, E. Clinical application of the basic definition of malnutrition proposed by the European Society for Clinical Nutrition and Metabolism (ESPEN): Comparison with classical tools in geriatric care. Arch. Gerontol. Geriatr. 2018, 76, 210–214. [Google Scholar] [CrossRef] [PubMed]
- Diekmann, R.; Winning, K.; Uter, W.; Kaiser, M.; Sieber, C.; Volkert, D.; Bauer, J. Screening for malnutrition among nursing home residents—A comparative analysis of the Mini Nutritional Assessment, the Nutritional Risk Screening, and the Malnutrition Universal Screening Tool. J. Nutr. Health Aging 2013, 17, 326–331. [Google Scholar] [CrossRef]
- Gorji, H.A.; Alikhani, M.; Mohseni, M.; Moradi-Joo, M.; Ziaiifar, H.; Moosavi, A. The prevalence of malnutrition in iranian elderly: A review article. Iran. J. Public Health 2017, 46, 1603–1610. [Google Scholar]
- Kokura, Y.; Momosaki, R. Prevalence of Malnutrition Assessed by the GLIM Criteria and Association with Activities of Daily Living in Older Residents in an Integrated Facility for Medical and Long-Term Care. Nutrients 2022, 14, 3656. [Google Scholar] [CrossRef]
- Bajeux, E.; Corvol, A.; Somme, D. Integrated Care for Older People in France in 2020: Findings, Challenges, and Prospects. Int. J. Integr. Care 2021, 21, 16. [Google Scholar] [CrossRef]
- Grosshauser, F.J.; Kiesswetter, E.; Torbahn, G.; Sieber, C.C.; Volkert, D. Reasons for and against Nutritional Interventions. An Exploration in the Nursing Home Setting. Geriatrics 2021, 6, 90. [Google Scholar] [CrossRef] [PubMed]
- Suominen, M.H.; Sandelin, E.; Soini, H.; Pitkala, K.H. How well do nurses recognize malnutrition in elderly patients? Eur. J. Clin. Nutr. 2009, 63, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Beattie, E.; O’Reilly, M.; Strange, E.; Franklin, S.; Isenring, E. How much do residential aged care staff members know about the nutritional needs of residents? Int. J. Older People Nurs. 2014, 9, 54–64. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year Country | Study Type | Tool Used for Dementia Diagnosis | Number with Dementia | Mean Age (Years) | Gender Mix (% Female) | Mean Time Since Dementia Diagnosis (Months) | Mean Time Since Admission | Nutrition Assessment Tool/Assessor | Proportion of Well Nourished/at Risk of Malnutrition/Malnourished |
|---|---|---|---|---|---|---|---|---|---|
| Arellano et al., 2004 [11] Spain | Cross sectional | MMSE | n = 63 | 80.1 ± 8.1 | 75% | Not stated | Not stated | MNA/Not stated | Well nourished: 1.5% At risk: 36.5% Malnourished: 61.9% |
| Bolmsjo et al., 2015 [47] Sweden | Prospective cohort | Medical records | n = 107 | Not stated | Not stated | Not stated | Not stated | MNA and MNA-SF/Nurses | Well nourished: 32.7% At risk: 45.8% Malnourished: 21.5% |
| Bonaccorsi et al., 2015 [30] Italy | Cross sectional | GDS and Pfeiffer test | Dementia: n = 640 Cognitive impairment: n = 1089 | Not stated | Not stated | Not stated | Not stated | MUST/Nurses | At risk: Severe dementia: 50.5% Severe cognitive impairment: 47.3% |
| Bourdel-Marchasson et al., 2009 [32] France | Cross sectional | Dietitian confirmed as part of MNA | Severe dementia or depression: n = 868 Mild dementia: n = 24 | Not stated | Not stated | Not stated | Not stated | MNA and MNA-SF/Dietitian | Malnourished Mild dementia: 35.3% Severe dementia: 60.3% |
| Cankurtaran et al., 2013 [31] Turkey | Cross sectional | Pre-existing | n = 420 | Not stated | Not stated | Not stated | Not stated | MNA and MNA-SF/Nurses | Well nourished 29.3% At risk: 47.9% Malnourished: 22.9% |
| Cereda et al., 2011 [49] Italy | Prospective observational study | Medical records or having the patients interviewed and physically examined | n = 154 | Not stated | Not stated | Not stated | Not stated | MNA/Dietitian | Well nourished: 5.8% At risk: 61.0% Malnourished: 33.1% |
| Chang et al., 2011 [10] Taiwan | Cross sectional | Medical records | n = 83 | 81.5 ± 7.52 | 59% | 51.1 ± 26.9 | Not stated | MNA and MNA-SF/Research assistants | Well nourished 9.6% At risk: 90.4% |
| Elsig et al., 2015 [34] Switzerland | Cross sectional | Various tools including MMSE, CERAD, CDR, DAD, VVPAT -WMS, the Stroop test and phonemic fluency | n = 29 | 82.5 ± 6.3 | 76% | Not stated | Not stated | MNA/Not stated | Well nourished: 6.9% At risk: 62.1% Malnourished: 31.0% |
| El Zoghbi et al., 2014 [35] Lebanon | Cross sectional | MMSE | n = 58 | Not stated | Not stated | Not stated | Not stated | MNA/Not stated | Well nourished: 25.9% At risk: 56.9% Malnourished: 17.2% |
| GilGregorio et al., 2003 [44] Spain | RCT | NINCDS- ADRDA | n = 99 | 86.5 ± 6.1 | 79.8% | 49.1 ± 24 | 20.2 ± 18.8 months | MNA/Not stated | Well nourished: 14.4% At risk: 68.1% Malnourished: 17.5% |
| Kamo et al., 2017 [50] Japan | Prospective observational study | Medical records | n = 56 | Not stated | Not stated | Not stated | Not stated | MNA-SF/Not stated | At risk or well nourished: 24.4% Malnourished: 75.6% |
| Keser et al., 2016 [36] Turkey | Cross sectional | Medical records | n = 57 | 76.0 ± 9.84 | 61.4% | Not stated | 2.4 ± 1.3 years | MNA/Not stated | Well nourished: 22.8% At risk: 57.9% Malnourished: 19.3% |
| Lauque et al., 2000 [45] France | RCT | Family/legal guardians/medical record | n = 57 | Not stated | Not stated | Not stated | Not stated | MNA/Researcher | Well nourished: 15.8% At risk: 45.6% Malnourished: 38.6% |
| Lin et al., 2017 [48] Taiwan | Prospective cohort study | DSM and NINCDS- ADRDA | n = 70 | 86.1 ± 4.0 | Not stated | Not stated | Not stated | MNA-SF/Not stated | Well nourished: 37.1% Malnourished or at risk: 62.9% |
| Maltais et al., 2018 [46] France | RCT | DSM and MMSE | n = 91 | Not stated | Not stated | Not stated | Not stated | MNA/Not stated | Control—Baseline Well nourished: 4.2% At risk: 76.6% Malnutrition: 19.2% Control—6 months Well nourished: 10.6% At risk: 78.7% Malnutrition: 10.6% Exercise—Baseline Well nourished: 25% Risk: 68.2% Malnutrition: 6.8% Exercise—6 months Well nourished: 31.8% Risk: 61.4% Malnourished: 6.8% |
| Muurinen et al., 2015 [37] Finland | Cross sectional | Medical records | n = 2379 | 85 | 78% | Not stated | Not stated | MNA/Nurses | Well nourished 9% At risk: 63% Malnourished: 28% |
| Salminen et al., 2019 [38] Finland | Cross sectional | Medical records | n = 1680 | Not stated | Not stated | Not stated | Not stated | MNA/Nurses | Well nourished: 15.6% Risk: 65.1% Malnutrition: 19.3% |
| Sliwinski et al., 2013 [39] Poland | Cross sectional | GDS | n = 62 | Women: 81.5 ± 6.92 Men: 74.5 ± 7.68 | 60% | Not stated | Not stated | MNA/Not stated | Well nourished: 28% Risk: 65% Malnourished: 7% |
| Suominem et al., 2004 [40] Finland | Cross sectional | MMSE | n = 2 | 82 | 100% | Not stated | Not stated | MNA-SF and PG-SGA/Nurses | Well nourished: 0% At risk: 87% Malnourished: 13% |
| Suominen et al., 2007 [51] Finland | Before–After study | Medical record | n = 19 | 85 | 100% | Not stated | Not stated | MNA/Nurses | Before education Well nourished: 0% At risk: 89% Malnourished: 11% After education Well nourished: 16% At risk: 63% Malnourished: 21% |
| Vandewoudeet al., 2019 [41] Belgium | Cross sectional | Medical record | n = 1051 | Not stated | Not stated | Not stated | Not stated | MNA-SF/Nurses, GPs and other health care providers | Well nourished 18% At risk: 62% Malnourished: 20% |
| Wojszel et al., 2006 [52] Poland | Pre-Post study | AMTS | n = 44 | Not stated | Not stated | Not stated | Not stated | MNA/Nurses | Well nourished: 8.9% At risk: 68.9% Malnutrition 22.2% |
| Yap et al., 2019 [42] Malaysia | Cross sectional | Mini-cog test | n = 164 | Not stated | Not stated | Not stated | Not stated | MNA/Trained healthcare personnel | Well nourished: 23.2% At risk: 58.5% Malnourished: 18.3% |
| Ziebolz et al., 2017 [43] Germany | Cross sectional | Medical records | n = 48 | Not stated | Not stated | Not stated | Not stated | MNA/Dentist | Well nourished 0% At risk: 60% Not at risk: 40% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perry, E.; Walton, K.; Lambert, K. Prevalence of Malnutrition in People with Dementia in Long-Term Care: A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 2927. https://doi.org/10.3390/nu15132927
Perry E, Walton K, Lambert K. Prevalence of Malnutrition in People with Dementia in Long-Term Care: A Systematic Review and Meta-Analysis. Nutrients. 2023; 15(13):2927. https://doi.org/10.3390/nu15132927
Chicago/Turabian StylePerry, Emma, Karen Walton, and Kelly Lambert. 2023. "Prevalence of Malnutrition in People with Dementia in Long-Term Care: A Systematic Review and Meta-Analysis" Nutrients 15, no. 13: 2927. https://doi.org/10.3390/nu15132927
APA StylePerry, E., Walton, K., & Lambert, K. (2023). Prevalence of Malnutrition in People with Dementia in Long-Term Care: A Systematic Review and Meta-Analysis. Nutrients, 15(13), 2927. https://doi.org/10.3390/nu15132927