
Effect of Vitamin D Supplementation on Primary Dysmenorrhea: A Systematic Review and Meta-Analysis of Randomized Clinical Trials

 ,
,  , , ,
, , ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria; PICO
2.4. Data Extraction, Synthesis, and Analysis
2.5. Quality Assessment and Risk of Bias (ROB)
2.6. Statistical Analysis
3. Results
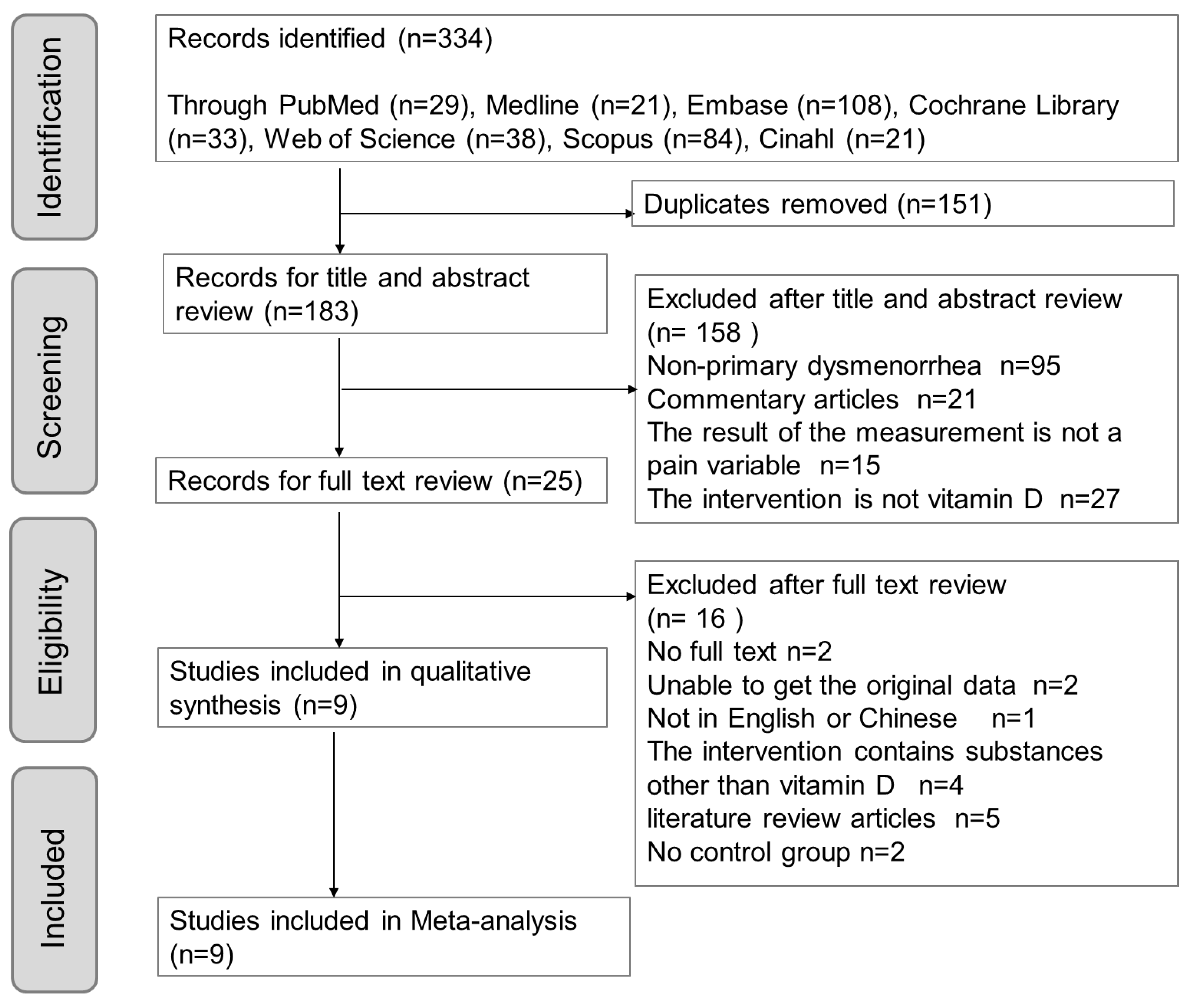
3.1. Eligible Studies Flow Chart
3.2. Quality ROB
3.3. RCT Characteristics
3.4. Intervention Details and Outcome Measurements
3.5. Overall Effect Size (ES)
3.6. Subgroups Analysis
4. Discussion
4.1. Study Strengths
4.2. Study Limitation
5. Summary and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| C | Comparator |
| CI | Confidence interval |
| CKAP2L | Cytoskeleton-associated protein 2-like |
| COX-2 | Cyclooxygenase 2 |
| GWAS | Genome-wide association studies |
| I | Intervention |
| IL | Interleukin |
| JAK | Janus activated kinase |
| KEGG | Kyoto Encyclopedia of Genes and Genomes |
| MAPK | mitogen activated protein kinase |
| MMPs | Matrix metalloproteinases |
| NF-κB | Nuclear factor kappa B cell |
| NRS | Numerical rating scale |
| NSAIDs | Non-steroidal anti-inflammatory drugs |
| O | Outcome |
| OCPs | Oral contraceptive pills |
| P | Population |
| PCOS | Polycystic ovary syndrome |
| PGs | Prostaglandins |
| RCTs | Randomized clinical trials |
| ROB | Risk-of-bias |
| RoB 2 | Cochrane risk of bias |
| SMD | Standardized mean difference |
| SRMA | Systemic review meta-analysis |
| STAT3 | Signal transducer and activator of transcription 3 |
| TNF-α | Tumor necrosis factor-alpha |
| V.C | Vasoconstriction |
| VAS | Visual analogue scale |
| VDR | Vitamin D receptor |
| VEGF | Vascular endothelial growth factor |
| Vit. D2 | Ergocalciferol |
| Vit. D3 | Cholecalciferol |
| Vit.D | Vitamin D |
References
- Proctor, M.; Farquhar, C. Diagnosis and management of dysmenorrhoea. BMJ 2006, 332, 1134–1138. [Google Scholar] [CrossRef] [PubMed]
- Burnett, M.; Lemyre, M. No. 345-primary dysmenorrhea consensus guideline. J. Obstet. Gynaecol. Can. 2017, 39, 585–595. [Google Scholar] [CrossRef] [PubMed]
- Iacovides, S.; Avidon, I.; Baker, F.C. What we know about primary dysmenorrhea today: A critical review. Hum. Reprod. Update 2015, 21, 762–778. [Google Scholar] [CrossRef]
- Nnoaham, K.E.; Hummelshoj, L.; Webster, P.; d’Hooghe, T.; de Cicco Nardone, F.; de Cicco Nardone, C.; Jenkinson, C.; Kennedy, S.H.; Zondervan, K.T. Impact of endometriosis on quality of life and work productivity: A multicenter study across ten countries. Fertil. Steril. 2011, 96, 366–373.e368. [Google Scholar] [CrossRef] [PubMed]
- Ayan, M.; Sogut, E.; Tas, U.; Erdemir, F.; Sahin, M.; Suren, M.; Kaya, Z.; Demirturk, F. Pain levels associated with renal colic and primary dysmenorrhea: A prospective controlled study with objective and subjective outcomes. Arch. Gynecol. Obstet. 2012, 286, 403–409. [Google Scholar] [CrossRef]
- Wong, L.P.; Khoo, E.M. Dysmenorrhea in a multiethnic population of adolescent asian girls. Int. J. Gynaecol. Obstet. 2010, 108, 139–142. [Google Scholar] [CrossRef]
- Marjoribanks, J.; Ayeleke, R.O.; Farquhar, C.; Proctor, M. Nonsteroidal anti-inflammatory drugs for dysmenorrhoea. Cochrane Database Syst. Rev. 2015, 2015, Cd001751. [Google Scholar] [CrossRef] [PubMed]
- Osayande, A.S.; Mehulic, S. Diagnosis and initial management of dysmenorrhea. Am. Fam. Physician 2014, 89, 341–346. [Google Scholar]
- Pakniat, H.; Chegini, V.; Ranjkesh, F.; Hosseini, M.A. Comparison of the effect of vitamin e, vitamin d and ginger on the severity of primary dysmenorrhea: A single-blind clinical trial. Obstet. Gynecol. Sci. 2019, 62, 462–468. [Google Scholar] [CrossRef]
- Kanehisa, M.; Sato, Y.; Kawashima, M. Kegg mapping tools for uncovering hidden features in biological data. Protein Sci. 2022, 31, 47–53. [Google Scholar] [CrossRef]
- Bashmakova, N.V.; Lisovskaya, T.V.; Vlasova, V.Y. Pathogenetic role of vitamin d deficiency in the development of menstrual dysfunction in pubertal girls: A literature review. Gynecol. Endocrinol. Off. J. Int. Soc. Gynecol. Endocrinol. 2017, 33, 52–55. [Google Scholar] [CrossRef]
- Wong, J.; Chiang, Y.F.; Shih, Y.H.; Chiu, C.H.; Chen, H.Y.; Shieh, T.M.; Wang, K.L.; Huang, T.C.; Hong, Y.H.; Hsia, S.M. Salvia sclarea l. Essential oil extract and its antioxidative phytochemical sclareol inhibit oxytocin-induced uterine hypercontraction dysmenorrhea model by inhibiting the ca(2+)-mlck-mlc20 signaling cascade: An ex vivo and in vivo study. Antioxidants 2020, 9, 991. [Google Scholar] [CrossRef]
- Abdul-Razzak, K.K.; Ayoub, N.M.; Abu-Taleb, A.A.; Obeidat, B.A. Influence of dietary intake of dairy products on dysmenorrhea. J. Obstet. Gynaecol. Res. 2010, 36, 377–383. [Google Scholar] [CrossRef]
- Alshahrani, F.; Aljohani, N. Vitamin d: Deficiency, sufficiency and toxicity. Nutrients 2013, 5, 3605–3616. [Google Scholar] [CrossRef] [PubMed]
- Alikamali, M.; Mohammad-Alizadeh-Charandabi, S.; Maghalian, M.; Mirghafourvand, M. The effects of vitamin e on the intensity of primary dysmenorrhea: A systematic review and meta-analysis. Clin. Nutr. ESPEN 2022, 52, 50–59. [Google Scholar] [CrossRef]
- Lasco, A.; Catalano, A.; Benvenga, S. Improvement of primary dysmenorrhea caused by a single oral dose of vitamin d: Results of a randomized, double-blind, placebo-controlled study. Arch. Intern. Med. 2012, 172, 366–367. [Google Scholar] [CrossRef] [PubMed]
- Ataee, M.; Zangeneh, M.; Mahboubi, M.J.J.B.T.W. Cholecalciferol for primary dysmenorrhea in a college aged population—A clinical trial. J. Biol. Todays World. 2015, 4, 54–57. [Google Scholar] [CrossRef]
- Moini, A.; Ebrahimi, T.; Shirzad, N.; Hosseini, R.; Radfar, M.; Bandarian, F.; Jafari-Adli, S.; Qorbani, M.; Hemmatabadi, M. The effect of vitamin d on primary dysmenorrhea with vitamin d deficiency: A randomized double-blind controlled clinical trial. Gynecol. Endocrinol. Off. J. Int. Soc. Gynecol. Endocrinol. 2016, 32, 502–505. [Google Scholar] [CrossRef]
- Zarei, S.; Mohammad-Alizadeh-Charandabi, S.; Mirghafourvand, M.; Javadzadeh, Y.; Effati-Daryani, F. Effects of calcium-vitamin d and calcium-alone on pain intensity and menstrual blood loss in women with primary dysmenorrhea: A randomized controlled trial. Pain Med. 2017, 18, 3–13. [Google Scholar] [CrossRef]
- Fareena Begum, A. Study of Prevalence of Vitamin d Deficiency in Primary Dysmenorrhea and Administration of a Single Oral Dose of Vitamind to Improve Primary Dysmenorrhea. Master’s Thesis, Coimbatore Medical College, Coimbatore, India, 2017. [Google Scholar]
- Lama, A.; Najla, A.; Azzah, A.; Areej, A.; Alaa, E.; Alsuwaidan, S. Vitamin d supplements as adjunctive therapy with analgesics for primary dysmenorrhea: A randomized clinical trial. Int. J. Reprod. Med. Gynecol. 2019, 5, 004–014. [Google Scholar]
- Rahnemaei, F.A.; Gholamrezaei, A.; Afrakhteh, M.; Zayeri, F.; Vafa, M.R.; Rashidi, A.; Ozgoli, G. Vitamin d supplementation for primary dysmenorrhea: A double-blind, randomized, placebo-controlled trial. Obstet. Gynecol. Sci. 2021, 64, 353–363. [Google Scholar] [CrossRef]
- Amzajerdi, A.; Keshavarz, M.; Ghorbali, E.; Pezaro, S.; Sarvi, F. The effect of vitamin d on the severity of dysmenorrhea and menstrual blood loss: A randomized clinical trial. BMC Women’s Health 2023, 23, 138. [Google Scholar] [CrossRef]
- Ginde, A.A.; Liu, M.C.; Camargo, C.A., Jr. Demographic differences and trends of vitamin d insufficiency in the us population, 1988-2004. Arch. Intern. Med. 2009, 169, 626–632. [Google Scholar] [CrossRef]
- Karacin, O.; Mutlu, I.; Kose, M.; Celik, F.; Kanat-Pektas, M.; Yilmazer, M.J.T.J.o.O.; Gynecology. Serum vitamin d concentrations in young turkish women with primary dysmenorrhea: A randomized controlled study. Taiwan. J. Obstet. Gynecol. 2018, 57, 58–63. [Google Scholar] [CrossRef]
- Bahrami, A.; Bahrami-Taghanaki, H.; Afkhamizadeh, M.; Avan, A.; Mazloum Khorasani, Z.; Esmaeili, H.; Amin, B.; Jazebi, S.; Kamali, D.; Ferns, G.A.; et al. Menstrual disorders and premenstrual symptoms in adolescents: Prevalence and relationship to serum calcium and vitamin d concentrations. J. Obstet. Gynaecol. 2018, 38, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin d deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Chiang, Y.F.; Hung, H.C.; Chen, H.Y.; Huang, K.C.; Lin, P.H.; Chang, J.Y.; Huang, T.C.; Hsia, S.M. The inhibitory effect of extra virgin olive oil and its active compound oleocanthal on prostaglandin-induced uterine hypercontraction and pain-ex vivo and in vivo study. Nutrients 2020, 12, 3012. [Google Scholar] [CrossRef]
- Viganò, P.; Lattuada, D.; Mangioni, S.; Ermellino, L.; Vignali, M.; Caporizzo, E.; Panina-Bordignon, P.; Besozzi, M.; Di Blasio, A.M. Cycling and early pregnant endometrium as a site of regulated expression of the vitamin d system. J. Mol. Endocrinol. 2006, 36, 415–424. [Google Scholar] [CrossRef]
- Adams, J.S.; Hewison, M. Extrarenal expression of the 25-hydroxyvitamin d-1-hydroxylase. Arch. Biochem. Biophys. 2012, 523, 95–102. [Google Scholar] [CrossRef]
- Unsal, A.; Ayranci, U.; Tozun, M.; Arslan, G.; Calik, E. Prevalence of dysmenorrhea and its effect on quality of life among a group of female university students. Ups. J. Med. Sci. 2010, 115, 138–145. [Google Scholar] [CrossRef]
- Jamieson, D.J.; Steege, J.F. The prevalence of dysmenorrhea, dyspareunia, pelvic pain, and irritable bowel syndrome in primary care practices. Obstet. Gynecol. 1996, 87, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, M.; Mori, N. Prostaglandin and leukotriene concentration of the peritoneal fluid of endometriosis and other gynecologic disorders in the secretory phase. Prostaglandins Leukot. Essent. Fatty Acids 1990, 39, 43–45. [Google Scholar] [CrossRef] [PubMed]
- Arosh, J.; Banu, S. Molecular, cellular, and epigenetic signatures of prostaglandin e2 in endometriosis. Current Women s Health Reviews 2018, 14, 127–146. [Google Scholar] [CrossRef]
- Krishnan, A.V.; Feldman, D. Mechanisms of the anti-cancer and anti-inflammatory actions of vitamin d. Annu. Rev. Pharmacol. Toxicol. 2011, 51, 311–336. [Google Scholar] [CrossRef] [PubMed]
- Miyashita, M.; Koga, K.; Izumi, G.; Sue, F.; Makabe, T.; Taguchi, A.; Nagai, M.; Urata, Y.; Takamura, M.; Harada, M.; et al. Effects of 1,25-dihydroxy vitamin d3 on endometriosis. J. Clin. Endocrinol. Metab. 2016, 101, 2371–2379. [Google Scholar] [CrossRef]
- Kattawy, H. The effect of vitamin d3 on the contractile response of isolated rat uterus. Med. J. Cairo Univ. 2019, 87, 4379–4386. [Google Scholar]
- Vieth, R. Why the optimal requirement for vitamin d3 is probably much higher than what is officially recommended for adults. J. Steroid Biochem. Mol. Biol. 2004, 89–90, 575–579. [Google Scholar] [CrossRef]
- Venugopal, Y.; Hatta, S.; Musa, N.; Rahman, S.A.; Ratnasingam, J.; Paramasivam, S.S.; Lim, L.L.; Ibrahim, L.; Choong, K.; Tan, A.T.; et al. Maintenance vitamin d3 dosage requirements in chinese women with post menopausal osteoporosis living in the tropics. Asia Pac. J. Clin. Nutr. 2017, 26, 412–420. [Google Scholar]
- Abdi, F.; Amjadi, M.A.; Zaheri, F.; Rahnemaei, F.A. Role of vitamin d and calcium in the relief of primary dysmenorrhea: A systematic review. Obstet. Gynecol. Sci. 2021, 64, 13–26. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin d deficiency: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef]
- Vieth, R. Critique of the considerations for establishing the tolerable upper intake level for vitamin d: Critical need for revision upwards. J. Nutr. 2006, 136, 1117–1122. [Google Scholar] [CrossRef] [PubMed]
- Galior, K.; Grebe, S.; Singh, R. Development of vitamin d toxicity from overcorrection of vitamin d deficiency: A review of case reports. Nutrients 2018, 10, 953. [Google Scholar] [CrossRef]
- Heaney, R.P. Functional indices of vitamin d status and ramifications of vitamin d deficiency. Am. J. Clin. Nutr. 2004, 80, 1706s–1709s. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 report on dietary reference intakes for calcium and vitamin d from the institute of medicine: What clinicians need to know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef]
- Toth, B.; Takacs, I.; Szekeres, L.; Szabo, B.; Bakos, B.; Lakatos, P. Safety and efficacy of weekly 30,000 iu vitamin d supplementation as a slower loading dose administration compared to a daily maintenance schedule in deficient patients: A randomized, controlled clinical trial. J. Pharmacovigil. 2017, 5, 4. [Google Scholar] [CrossRef]
- Dawson-Hughes, B.; Mithal, A.; Bonjour, J.P.; Boonen, S.; Burckhardt, P.; Fuleihan, G.E.; Josse, R.G.; Lips, P.; Morales-Torres, J.; Yoshimura, N. Iof position statement: Vitamin d recommendations for older adults. Osteoporos. Int. 2010, 21, 1151–1154. [Google Scholar] [CrossRef] [PubMed]
- Hamdy, N.M.; Suwailem, S.M.; El-Mesallamy, H.O. Influence of vitamin E supplementation on endothelial complications in type 2 diabetes mellitus patients who underwent coronary artery bypass graft. J. Diabetes Complicat. 2009, 23, 167–173. [Google Scholar] [CrossRef] [PubMed]
- El-Derany, M.O.; Hamdy, N.M.; Al-Ansari, N.L.; El-Mesallamy, H.O. Integrative role of vitamin D related and Interleukin-28B genes polymorphism in predicting treatment outcomes of Chronic Hepatitis C. BMC Gastroenterol. 2016, 16, 19. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| RCT Author Name Year [Ref.] | Bias | ||||
|---|---|---|---|---|---|
| Selection | Performance | Detection | Attrition | Reporting | |
| Lasco 2012 [16] | ? | + | + | + | + |
| Ataee 2015 [17] | + | + | + | + | + |
| Moini 2016 [18] | ? | + | + | + | + |
| Zarei 2016 [19] | + | + | + | + | + |
| Begum 2017 [20] | + | ? | ? | + | + |
| Pakniat 2019 [9] | + | + | − | + | + |
| Lama 2019 [21] | + | − | − | + | + |
| Rahnemaei 2021 [22] | + | + | + | + | + |
| Amzajerdi 2023 [23] | + | + | + | + | + |
| RCT Author Name Year [Ref.] | Study Country | Sample Size | Age Range (Years) | Menstrual Cycle Intervals (Days) | Assessment Tool/Scale | Blindness Design |
|---|---|---|---|---|---|---|
| Lasco A (2012) [16] | Italy | 40 | 18–40 | 21–35 | VAS | Double |
| Ataee (2015) [17] | Iran | 54 | 18–30 | 21–35 | VAS | Double |
| Moini A (2016) [18] | Iran | 50 | 18–30 | NA | VAS | Double |
| Zarei S (2016) [19] | Iran | 85 | 18–32 | 21–35 | VAS | Double |
| Begum (2017) [20] | India | 50 | 18–25 | 21–35 | VAS | Single |
| Pakniat (2019) [9] | Iran | 200 | 18–25 | 21–35 | VAS | Single |
| Lama (2019) [21] | Saudi Arabia | 22 | 13–40 | NA | VAS | Open-label |
| Rahnemaei (2021) [22] | Iran | 116 | 18–32 | 22–35 | NRS | Double |
| Amzajerdi (2023) [23] | Iran | 78 | 18–25 | 21–35 | VAS | Double |
| RCT Author Name Year [Ref.] | Study Duration (Months) | Serum 25(OH)D Level | Primary Pain Score | Dosage Frequency | Dose Interval | Total Dose | Weekly Dose | Note/ Remarks | Significant Results for | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Vit. D | Control | Vit. D | Control | IU | (Time) | IU | IU | ||||
| Lasco A (2012) [16] | 0 | 27.2 ± 7.5 | 29.9 ± 7.6 | 5.85 ± 2.0 | 5.6 ± 1.9 | 300,000 single | month | 600,000 | 75,000 | Control/placebo pill Intervention time: 5 days before next period | D |
| 1 | NA | NA | 3.7 ± 1.34 | 5.4 ± 1.8 | |||||||
| 2 | NA | NA | 3.5 ± 1.3 | 5.7 ± 1.6 | |||||||
| Ataee (2015) [17] | 0 | 7.3 ± 3.6 | 6.3 ± 2.8 | 7.13 ± 1.85 | 7.38 ± 1.56 | 300,000 single | month | 900,000 | 75,000 | Control/placebo pill Intervention time: 5 days before next period | D |
| 1 | NA | NA | 5.30 ± 2.24 | 5.21 ± 2.35 | |||||||
| 2 | NA | NA | 3.97 ± 1.90 | 5.24 ± 2.27 | |||||||
| 3 | NA | NA | 3.77 ± 1.77 | 5.55 ± 2.02 | |||||||
| Moini A (2016) [18] | 0 | 9.7 ± 5.09 | 11.5 ± 3.7 | 8.50 | 9.60 | 50,000 weekly | week | 400,000 | 50,000 | Control/placebo pill | D |
| 2 | 55.4 ± 6.02 | 13.57 ± 4 | 2.50 | 7.60 | |||||||
| Zarei S (2016) [19] | 0 | NA | NA | 6.20 ± 1.60 | 6.30 ± 1.80 | 5000 | day | 300,000 | 25,000 | Control/placebo + 1000 mg Ca Intervention time: 20 days /menstruation period | Ca > Ca + D >placebo |
| 1 | 5.40 ± 2.30 | 4.7 ± 2.30 | |||||||||
| 2 | 4.70 ± 2.20 | 4.2 ± 2.20 | |||||||||
| 3 | 4.60 ± 2.60 | 3.6 ± 2.20 | |||||||||
| 4 | 5.00 ± 2.60 | 3.9 ± 2.50 | |||||||||
| Begum (2017) [20] | 0 | 17.8 ± 10.1 | 19.10 | 8.76 ± 0.97 | 8.80 ± 0.95 | 300,000 single | once | 300,000 | 18,750 | Control/placebo pill | D |
| 2 | NA | NA | 2.72 ± 1.17 | 8.20 ± 0.74 | |||||||
| 4 | 34.7 ± 8.1 | 19.34 | 3.56 ± 0.76 | 8.20 ± 0.74 | |||||||
| Pakniat (2019) [9] | 0 | NA | NA | 7.01 ± 0.11 | 7.24 ± 0.56 | 3000 | month | 6000 | 750 | Vit D: 3000 IU + 500 mg mefenamic acid | D |
| 2 | NA | NA | 5.20 ± 1.34 | 6.00 ± 0.70 | Control/placebo + 500 mg mefenamic | ||||||
| Lama (2019) [21] | 0 | 30.1 ± 13.4 | 19.5 ± 5.5 | 7.8 ± 1 | 6.9 ± 1.2 | 50,000 | week | 400,000 | 50,000 | Vit D: 50,000 IU + NSAID Control: NSAID | D |
| 2 | 80.2 ± 14.3 | 19.70 ± 5.6 | 3.6 ± 1.2 | 6.4 ± 1.1 | |||||||
| Rahnemaei (2021) [22] | 0 | 20 ± 6 | 19.5 ± 5.5 | 7.0 ± 1.7 | 6.6 ± 1.5 | 50,000 | week | 400,000 | 50,000 | Vit D: 50,000 IU +NSAID or acetaminophen | D |
| 2 | 37.2 ± 9.4 | 19.7 ± 5.6 | 5.6 ± 1.7 | 6.5 ± 1.6 | |||||||
| Amzajerdi (2023) [23] | 0 | 5.10 ± 3.31 | 6.6 ± 5.63 | 6.71 ± 2.25 | 6.64 ± 2.46 | 300,000 single | once | 300,000 | 18,750 | Control/placebo pill | D |
| 1 | 30.63 ± 5.43 | 9.73 ± 4.72 | 5.33 ± 2.39 | 6.53 ± 2.30 | |||||||
| 2 | 3.92 ± 2.36 | 6.79 ± 2.17 | |||||||||
| Subgroup | SMD | 95% CI |
|---|---|---|
| Total dose | ||
| Average weekly ≥ 50,000 IU | ||
| a. Total dose ≥ 400,000 | −1.056 * | −1.619 to −0.493 |
| b. Total dose < 400,000 | NA | NA |
| Heterogeneity (Tau2 = 0.225, df (Q) = 3 (p = 0.013), I2 = 72.287%) | ||
| Average weekly < 50,000 IU | ||
| a. Total dose ≥ 400,000 | NA | NA |
| b. Total dose < 400,000 | −1.709 * | −2.947 to −0.472 |
| Heterogeneity (Tau2 = 1.851, df (Q) = 4 (p = 0.000), I2 = 95.569%) | ||
| Study duration | ||
| Average weekly ≥ 50,000 IU | ||
| a. Study duration ≥ 70 days | −0.937 * | −1.499 to −0.375 |
| Heterogeneity (Tau2 = 0.000, df (Q) = 0 (p = 1.000), I2 = 0.000%) | ||
| b. Study duration < 70 days | −1.171 * | −2.007 to −0.334 |
| Heterogeneity (Tau2 = 0.422, df (Q) = 2 (p = 0.005), I2 = 81.236%) | ||
| Average weekly < 50,000 IU | ||
| a. Study duration ≥ 70 days | −2.856 | −9.324 to 3.612 |
| Heterogeneity (Tau2 = 21.518, df (Q) = 1 (p = 0.000), I2 = 98.773%) | ||
| b. Study duration < 70 days | −1.122 * | −1.578 to −0.666 |
| Heterogeneity (Tau2 = 0.092, df (Q) = 2 (p = 0.097), I2 = 57.066%) | ||
| Dose interval | ||
| Average weekly ≥ 50,000 IU | ||
| a. Monthly or once | −0.937 * | −1.499 to −0.375 |
| Heterogeneity (Tau2 = 0.000, df (Q) = 0 (p = 1.000), I2 = 0.000%) | ||
| b. Weekly or daily | −1.171 * | −2.007 to −0.334 |
| Heterogeneity (Tau2 = 0.422, df (Q) = 2 (p = 0.005), I2 = 81.236%) | ||
| Average weekly < 50,000 IU | ||
| a. Monthly or once | −2.258 * | −3.617 to −0.899 |
| Heterogeneity (Tau2 = 1.762, df (Q) = 3 (p = 0.000), I2 = 94.925%) | ||
| b. Weekly or daily | 0.415 | −0.110 to 0.939 |
| Heterogeneity (Tau2 = 0.000, df (Q) = 0 (p = 1.000), I2 = 0.000%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-C.; Chiang, Y.-F.; Lin, Y.-J.; Huang, K.-C.; Chen, H.-Y.; Hamdy, N.M.; Huang, T.-C.; Chang, H.-Y.; Shieh, T.-M.; Huang, Y.-J.; et al. Effect of Vitamin D Supplementation on Primary Dysmenorrhea: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Nutrients 2023, 15, 2830. https://doi.org/10.3390/nu15132830
Chen Y-C, Chiang Y-F, Lin Y-J, Huang K-C, Chen H-Y, Hamdy NM, Huang T-C, Chang H-Y, Shieh T-M, Huang Y-J, et al. Effect of Vitamin D Supplementation on Primary Dysmenorrhea: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Nutrients. 2023; 15(13):2830. https://doi.org/10.3390/nu15132830
Chicago/Turabian StyleChen, Yi-Chun, Yi-Fen Chiang, Ying-Jiun Lin, Ko-Chieh Huang, Hsin-Yuan Chen, Nadia M. Hamdy, Tsui-Chin Huang, Hsin-Yi Chang, Tzong-Ming Shieh, Yun-Ju Huang, and et al. 2023. "Effect of Vitamin D Supplementation on Primary Dysmenorrhea: A Systematic Review and Meta-Analysis of Randomized Clinical Trials" Nutrients 15, no. 13: 2830. https://doi.org/10.3390/nu15132830
APA StyleChen, Y.-C., Chiang, Y.-F., Lin, Y.-J., Huang, K.-C., Chen, H.-Y., Hamdy, N. M., Huang, T.-C., Chang, H.-Y., Shieh, T.-M., Huang, Y.-J., & Hsia, S.-M. (2023). Effect of Vitamin D Supplementation on Primary Dysmenorrhea: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Nutrients, 15(13), 2830. https://doi.org/10.3390/nu15132830