

Dietary Calcium Intake and Osteoporosis Risk in Arab Adults

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
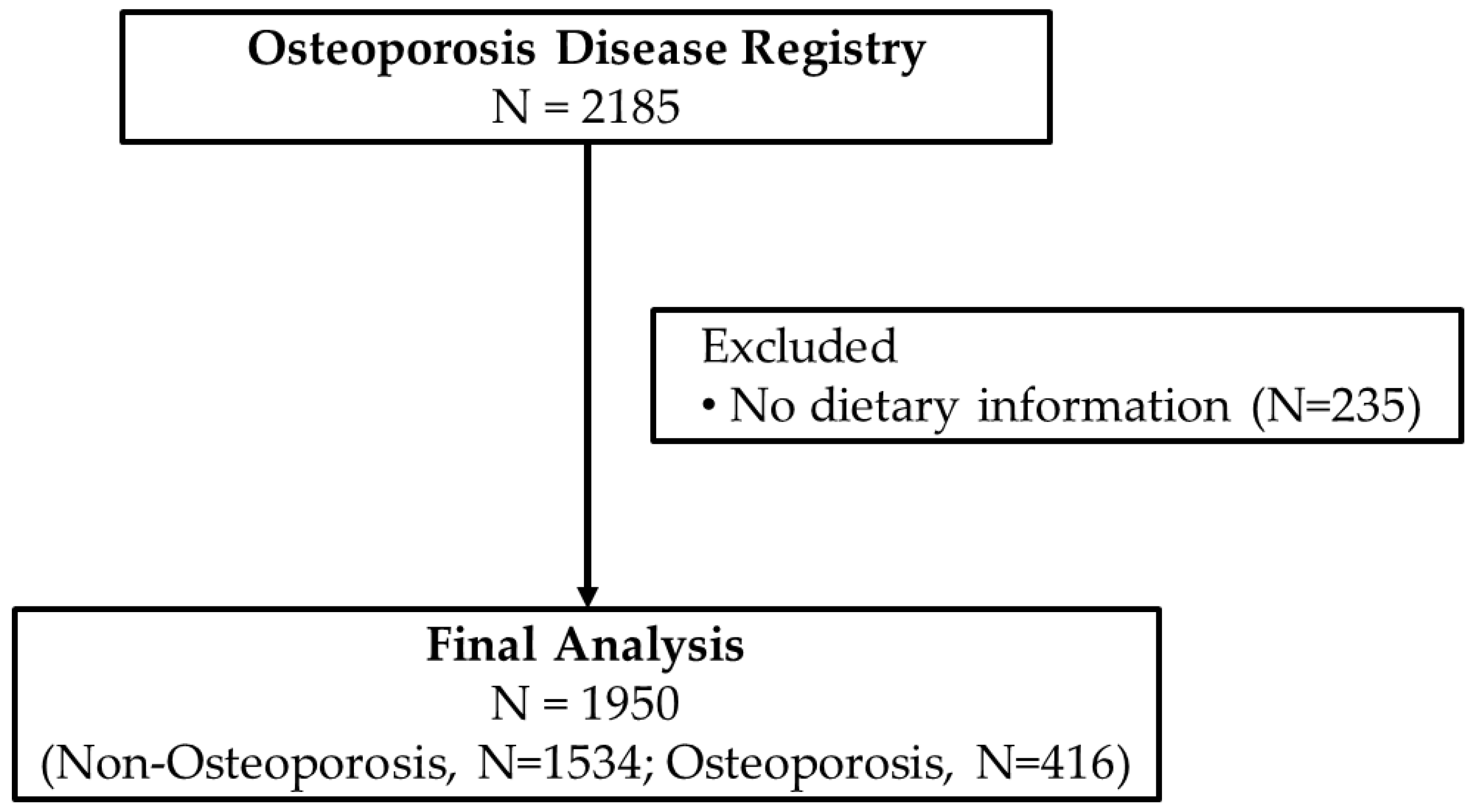
2.1. Study Design and Participants
2.2. Diagnosis of Osteoporosis
2.3. Anthropometry, Blood Collection and Sample Analysis
2.4. Dietary Intake
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Al-Daghri, N.M.; Sabico, S.; Al-Saleh, Y.; Sulimani, R.; Aljohani, N.J.; Sheshah, E.; Alodhayani, A.; Harvey, N.C.; Liu, E.; Lorentzon, M.; et al. The application of FRAX in Saudi Arabia. Arch. Osteoporos. 2021, 16, 166. [Google Scholar] [CrossRef]
- Kanis, J.A.; McCloskey, E.V.; Johansson, H.; Oden, A.; Melton, L.J., 3rd; Khaltaev, N. A reference standard for the description of osteoporosis. Bone 2008, 42, 467–475. [Google Scholar] [CrossRef]
- Sadat-Ali, M.; AlZamami, J.F.; AlNaimi, S.N.; Al-Noaimi, D.A.; AlDakheel, D.A.; AlSayed, H.N.; Al-Turki, H.A.; AlOmran, A.S. Osteoporosis: Is the prevalence increasing in Saudi Arabia. Ann. Afr. Med. 2022, 21, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Al Hamam, N.M.; Al-Moaibed, G.F.; Alfayez, E.H.; Alfayez, E.H.; Al-Mubaddil, M.S.; Alramadhan, N.A. Prevalence and risk factors for osteoporotic fracture among adults with comorbidities in Al-Ahsaa, Saudi Arabia. J. Fam. Med. Prim. Care 2020, 9, 877–882. [Google Scholar] [CrossRef]
- Rizzoli, R.; Bianchi, M.L.; Garabedian, M.; McKay, H.A.; Moreno, L.A. Maximizing bone mineral mass gain during growth for the prevention of fractures in the adolescents and the elderly. Bone 2010, 46, 294–305. [Google Scholar] [CrossRef]
- Ferrari, S.; Rizzoli, R.; Bonjour, J.P. Genetic aspects of osteoporosis. Curr. Opin. Rheumatol. 1999, 11, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Rizzoli, R. Nutrition: Its role in bone health. Best Pract. Res. Clin. Endocrinol. Metab. 2008, 22, 813–829. [Google Scholar] [CrossRef] [PubMed]
- Rizzoli, R. Dairy products, yogurts, and bone health. Am. J. Clin. Nutr. 2014, 99, 1256S–1262S. [Google Scholar] [CrossRef]
- Lorincz, C.; Manske, S.L.; Zernicke, R. Bone health: Part 1, nutrition. Sport. Health 2009, 1, 253–260. [Google Scholar] [CrossRef]
- Munoz-Garach, A.; Garcia-Fontana, B.; Munoz-Torres, M. Nutrients and Dietary Patterns Related to Osteoporosis. Nutrients 2020, 12, 1986. [Google Scholar] [CrossRef]
- Malmir, H.; Saneei, P.; Larijani, B.; Esmaillzadeh, A. Adherence to Mediterranean diet in relation to bone mineral density and risk of fracture: A systematic review and meta-analysis of observational studies. Eur. J. Nutr. 2018, 57, 2147–2160. [Google Scholar] [CrossRef]
- Matia-Martin, P.; Torrego-Ellacuria, M.; Larrad-Sainz, A.; Fernandez-Perez, C.; Cuesta-Triana, F.; Rubio-Herrera, M.A. Effects of Milk and Dairy Products on the Prevention of Osteoporosis and Osteoporotic Fractures in Europeans and Non-Hispanic Whites from North America: A Systematic Review and Updated Meta-Analysis. Adv. Nutr. 2019, 10, S120–S143. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.T.; Feskanich, D. Dietary patterns and risk of hip fractures in postmenopausal women and men over 50 years. Osteoporos. Int. 2015, 26, 1825–1830. [Google Scholar] [CrossRef] [PubMed]
- Sun, K.; Wang, L.; Ma, Q.; Cui, Q.; Lv, Q.; Zhang, W.; Li, X. Association between tea consumption and osteoporosis: A meta-analysis. Medicine 2017, 96, e9034. [Google Scholar] [CrossRef]
- Pujia, R.; Ferro, Y.; Maurotti, S.; Mare, R.; Arturi, F.; Montalcini, T.; Pujia, A.; Mazza, E. Relationship between Osteoporosis, Multiple Fractures, and Egg Intake in Healthy Elderly. J. Midlife Health 2021, 12, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Calderon-Garcia, J.F.; Moran, J.M.; Roncero-Martin, R.; Rey-Sanchez, P.; Rodriguez-Velasco, F.J.; Pedrera-Zamorano, J.D. Dietary habits, nutrients and bone mass in Spanish premenopausal women: The contribution of fish to better bone health. Nutrients 2012, 5, 10–22. [Google Scholar] [CrossRef]
- Sabico, S.; Wani, K.; Grant, W.B.; Al-Daghri, N.M. Improved HDL Cholesterol through Vitamin D Status Correction Substantially Lowers 10-Year Atherosclerotic Cardiovascular Disease Risk Score in Vitamin D-Deficient Arab Adults. Nutrients 2023, 15, 551. [Google Scholar] [CrossRef]
- Alissa, E.M.; Qadi, S.G.; Alhujaili, N.A.; Alshehri, A.M.; Ferns, G.A. Effect of diet and lifestyle factors on bone health in postmenopausal women. J. Bone Miner. Metab. 2011, 29, 725–735. [Google Scholar] [CrossRef]
- Al-Daghri, N.M.; Yakout, S.; Sabico, S.; Wani, K.; Hussain, S.D.; Aljohani, N.; Uday, S.; Hogler, W. Establishing the Prevalence of Osteomalacia in Arab Adolescents Using Biochemical Markers of Bone Health. Nutrients 2022, 14, 5354. [Google Scholar] [CrossRef]
- Wani, K.; Yakout, S.M.; Ansari, M.G.A.; Sabico, S.; Hussain, S.D.; Alokail, M.S.; Sheshah, E.; Aljohani, N.J.; Al-Saleh, Y.; Reginster, J.Y.; et al. Metabolic Syndrome in Arab Adults with Low Bone Mineral Density. Nutrients 2019, 11, 1405. [Google Scholar] [CrossRef]
- Al-Saleh, Y.; Al-Daghri, N.M.; Sabico, S.; Alessa, T.; Al Emadi, S.; Alawadi, F.; Al Qasaabi, S.; Alfutaisi, A.; Al Izzi, M.; Mukhaimer, J.; et al. Diagnosis and management of osteoporosis in postmenopausal women in Gulf Cooperation Council (GCC) countries: Consensus statement of the GCC countries’ osteoporosis societies under the auspices of the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO). Arch. Osteoporos. 2020, 15, 109. [Google Scholar] [CrossRef]
- Al-Saleh, Y.; Sulimani, R.; Sabico, S.; Alshahrani, F.M.; Fouda, M.A.; Almohaya, M.; Alaidarous, S.B.; Alkhawashki, H.M.; Alshaker, M.; Alrayes, H.; et al. Diagnosis and management of osteoporosis in Saudi Arabia: 2023 key updates from the Saudi Osteoporosis Society. Arch. Osteoporos. 2023, 18, 75. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, H.M.; Garland, A.; Burr, J.; Strachan, A.; Wood, A.D.; Jamil, N.A.; McLernon, D.; Black, A.J. Validation of a short questionnaire for estimating dietary calcium intakes. Osteoporos. Int. 2014, 25, 1765–1773. [Google Scholar] [CrossRef]
- Vannucci, L.; Fossi, C.; Quattrini, S.; Guasti, L.; Pampaloni, B.; Gronchi, G.; Giusti, F.; Romagnoli, C.; Cianferotti, L.; Marcucci, G.; et al. Calcium Intake in Bone Health: A Focus on Calcium-Rich Mineral Waters. Nutrients 2018, 10, 1930. [Google Scholar] [CrossRef]
- Caroli, A.; Poli, A.; Ricotta, D.; Banfi, G.; Cocchi, D. Invited review: Dairy intake and bone health: A viewpoint from the state of the art. J. Dairy Sci. 2011, 94, 5249–5262. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.J.; Tylavsky, F.A.; Halioua, L.; Metz, J.A. Determinants of peak bone mass in young adult women: A review. Osteoporos. Int. 1993, 3 (Suppl. S1), 32–36. [Google Scholar] [CrossRef] [PubMed]
- Sowers, M.R.; Galuska, D.A. Epidemiology of bone mass in premenopausal women. Epidemiol. Rev. 1993, 15, 374–398. [Google Scholar] [CrossRef]
- Balk, E.M.; Adam, G.P.; Langberg, V.N.; Earley, A.; Clark, P.; Ebeling, P.R.; Mithal, A.; Rizzoli, R.; Zerbini, C.A.F.; Pierroz, D.D.; et al. Global dietary calcium intake among adults: A systematic review. Osteoporos. Int. 2017, 28, 3315–3324. [Google Scholar] [CrossRef]
- Collaborators, G.B.D.D. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef]
- Al-Daghri, N.M.; Hussain, S.D.; Ansari, M.G.A.; Khattak, M.N.K.; Aljohani, N.; Al-Saleh, Y.; Al-Harbi, M.Y.; Sabico, S.; Alokail, M.S. Decreasing prevalence of vitamin D deficiency in the central region of Saudi Arabia (2008–2017). J. Steroid Biochem. Mol. Biol. 2021, 212, 105920. [Google Scholar] [CrossRef]
- Chen, Z.; Pettinger, M.B.; Ritenbaugh, C.; LaCroix, A.Z.; Robbins, J.; Caan, B.J.; Barad, D.H.; Hakim, I.A. Habitual tea consumption and risk of osteoporosis: A prospective study in the women’s health initiative observational cohort. Am. J. Epidemiol. 2003, 158, 772–781. [Google Scholar] [CrossRef] [PubMed]
- Barrett-Connor, E.; Chang, J.C.; Edelstein, S.L. Coffee-associated osteoporosis offset by daily milk consumption. The Rancho Bernardo Study. JAMA 1994, 271, 280–283. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.H.; Han, D.W.; Suh, H.; Ryu, G.H.; Hyon, S.H.; Cho, B.K.; Park, J.C. Protective effects of green tea polyphenol against reactive oxygen species-induced oxidative stress in cultured rat calvarial osteoblast. Cell Biol. Toxicol. 2003, 19, 325–337. [Google Scholar] [CrossRef]
- Farina, E.K.; Kiel, D.P.; Roubenoff, R.; Schaefer, E.J.; Cupples, L.A.; Tucker, K.L. Protective effects of fish intake and interactive effects of long-chain polyunsaturated fatty acid intakes on hip bone mineral density in older adults: The Framingham Osteoporosis Study. Am. J. Clin. Nutr. 2011, 93, 1142–1151. [Google Scholar] [CrossRef]
- Nawata, K.; Yamauchi, M.; Takaoka, S.; Yamaguchi, T.; Sugimoto, T. Association of n-3 polyunsaturated fatty acid intake with bone mineral density in postmenopausal women. Calcif. Tissue Int. 2013, 93, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Fan, F.; Xue, W.Q.; Wu, B.H.; He, M.G.; Xie, H.L.; Ouyang, W.F.; Tu, S.L.; Chen, Y.M. Higher fish intake is associated with a lower risk of hip fractures in Chinese men and women: A matched case-control study. PLoS ONE 2013, 8, e56849. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.M.; Ho, S.C.; Lam, S.S. Higher sea fish intake is associated with greater bone mass and lower osteoporosis risk in postmenopausal Chinese women. Osteoporos. Int. 2010, 21, 939–946. [Google Scholar] [CrossRef]
- Virtanen, J.K.; Mozaffarian, D.; Cauley, J.A.; Mukamal, K.J.; Robbins, J.; Siscovick, D.S. Fish consumption, bone mineral density, and risk of hip fracture among older adults: The cardiovascular health study. J. Bone Miner. Res. 2010, 25, 1972–1979. [Google Scholar] [CrossRef]
- Nouri, M.; Mahmoodi, M.; Shateri, Z.; Ghadiri, M.; Rajabzadeh-Dehkordi, M.; Vali, M.; Gargari, B.P. How do carbohydrate quality indices influence on bone mass density in postmenopausal women? A case-control study. BMC Womens Health 2023, 23, 42. [Google Scholar] [CrossRef]
- Garcia-Gavilan, J.F.; Bullo, M.; Camacho-Barcia, L.; Rosique-Esteban, N.; Hernandez-Alonso, P.; Basora, J.; Martinez-Gonzalez, M.A.; Estruch, R.; Fito, M.; Salas-Salvado, J. Higher dietary glycemic index and glycemic load values increase the risk of osteoporotic fracture in the PREvencion con DIeta MEDiterranea (PREDIMED)-Reus trial. Am. J. Clin. Nutr. 2018, 107, 1035–1042. [Google Scholar] [CrossRef]
- Coxam, V. Current data with inulin-type fructans and calcium, targeting bone health in adults. J. Nutr. 2007, 137, 2527S–2533S. [Google Scholar] [CrossRef] [PubMed]
- Raschka, L.; Daniel, H. Mechanisms underlying the effects of inulin-type fructans on calcium absorption in the large intestine of rats. Bone 2005, 37, 728–735. [Google Scholar] [CrossRef]
- Qiu, R.; Cao, W.T.; Tian, H.Y.; He, J.; Chen, G.D.; Chen, Y.M. Greater Intake of Fruit and Vegetables Is Associated with Greater Bone Mineral Density and Lower Osteoporosis Risk in Middle-Aged and Elderly Adults. PLoS ONE 2017, 12, e0168906. [Google Scholar] [CrossRef] [PubMed]
- Wallace, T.C.; Bailey, R.L.; Lappe, J.; O’Brien, K.O.; Wang, D.D.; Sahni, S.; Weaver, C.M. Dairy intake and bone health across the lifespan: A systematic review and expert narrative. Crit. Rev. Food Sci. Nutr. 2021, 61, 3661–3707. [Google Scholar] [CrossRef] [PubMed]
- Feskanich, D.; Willett, W.C.; Stampfer, M.J.; Colditz, G.A. Milk, dietary calcium, and bone fractures in women: A 12-year prospective study. Am. J. Public Health 1997, 87, 992–997. [Google Scholar] [CrossRef] [PubMed]
- Cumming, R.G.; Klineberg, R.J. Case-control study of risk factors for hip fractures in the elderly. Am. J. Epidemiol. 1994, 139, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Feskanich, D.; Willett, W.C.; Colditz, G.A. Calcium, vitamin D, milk consumption, and hip fractures: A prospective study among postmenopausal women. Am. J. Clin. Nutr. 2003, 77, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Nel, J.H.; Steyn, N.P.; Senekal, M. Illustration of the Importance of Adjustment for within- and between-Person Variability in Dietary Intake Surveys for Assessment of Population Risk of Micronutrient Deficiency/Excess Using an Example Data Set. Nutrients 2022, 14, 285. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameters | Non-Osteoporosis | Osteoporosis | p-Value | p-Value * |
|---|---|---|---|---|
| N | 1534 | 416 | ||
| Age (years) | 53.3 ± 11.5 | 59.3 ± 8.7 | <0.001 | -- |
| BMI (kg/m2) | 32.3 ± 6.2 | 30.3 ± 6.1 | <0.001 | -- |
| M/F | 389/1145 | 27/389 | <0.001 | -- |
| T2DM | 725 (47.3) | 193 (46.4) | 0.30 | 0.06 |
| Hypertension | 547 (35.7) | 128 (30.8) | 0.06 | 0.01 |
| WHR | 0.9 ± 0.4 | 0.9 ± 0.2 | 0.40 | 0.26 |
| Systolic BP (mmHg) | 125.3 ± 16.4 | 124.4 ± 17.8 | 0.36 | 0.05 |
| Diastolic BP (mmHg) | 77.5 ± 10.0 | 76.2 ± 10.3 | 0.02 | 0.005 |
| Total Cholesterol (mmol/L) | 5.1 ± 1.2 | 5.1 ± 1.1 | 0.64 | 0.57 |
| Glucose (mmol/L) | 6.4 (5.3–9.5) | 6.2 (5.3–8.8) | 0.76 | 0.01 |
| HDL-C (mmol/L) | 1.1 ± 0.4 | 1.2 ± 0.4 | 0.18 | 0.12 |
| Triglycerides (mmol/L) | 1.6 (1.2–2.2) | 1.5 (1.1–2.0) | 0.006 | 0.001 |
| 25(OH) D (nmol/L) | 59.4 (36.9–89.1) | 72.2 (44.8–100.1) | <0.001 | 0.09 |
| Ca (mmol/L) | 2.3 ± 0.3 | 2.3 ± 0.3 | 0.16 | 0.49 |
| Phosphorous (mmol/L) | 1.3 (1.0–1.7) | 1.2 (1.0–1.7) | 0.61 | 0.50 |
| BMD Spine | 1.0 ± 0.3 | 0.8 ± 0.2 | <0.001 | <0.001 |
| BMD Femur | 1.0 ± 0.1 | 0.9 ± 0.2 | <0.001 | <0.001 |
| T-score Spine | −0.8 ± 1.2 | −3.1 ± 0.6 | <0.001 | <0.001 |
| T-score Femur | −0.1 ± 2.9 | −1.3 ± 0.9 | <0.001 | <0.001 |
| Tea with Milk (cups/wk) | 0.8 ± 2.9 | 0.7 ± 3.3 | <0.001 | 0.53 |
| Coffee with milk (cups/wk) | 0.5 ± 2.9 | 0.2 ± 1.0 | <0.001 | 0.12 |
| Slices (Count/wk) | 5.6 ± 7.5 | 6.5 ± 6.9 | <0.001 | 0.42 |
| Biscuits (Count/wk) | 0.9 ± 2.9 | 0.7 ± 2.2 | 0.06 | 0.92 |
| Cake (Portion/wk) | 0.8 ± 4.7 | 0.6 ± 3.0 | 0.001 | 0.33 |
| Pancakes (Count/wk) | 0.3 ± 3.3 | 0.2 ± 0.7 | 0.40 | 0.99 |
| Lasagna (Portion/wk) | 1.0 ± 11.2 | 0.8 ± 10.4 | 0.45 | 0.76 |
| Whole meal Slices (Count/wk) | 0.6 ± 2.2 | 0.5 ± 1.7 | 0.19 | 0.38 |
| Milky drinks (Count/wk) | 2.7 ± 5.7 | 2.9 ± 6.4 | 0.44 | 0.67 |
| Milk with cereal (Portion/wk) | 0.2 ± 1.6 | 0.1 ± 0.6 | 0.15 | 0.95 |
| Cheese (Triangle/wk) | 2.5 ± 11.3 | 2.5 ± 8.8 | 0.20 | 0.48 |
| Milk pudding (Portion/wk) | 0.4 ± 3.7 | 0.2 ± 1.5 | 0.001 | 0.16 |
| Cottage Cheese (Portion/wk) | 1.5 ± 6.0 | 1.4 ± 6.5 | 0.45 | 0.16 |
| Sardines pilchards (Portion/wk) | 0.9 ± 7.9 | 0.5 ± 6.0 | 0.002 | 0.05 |
| Fish (Portion/wk) | 1.1 ± 7.9 | 0.7 ± 4.7 | 0.04 | 0.87 |
| Eggs (Eggs/wk) | 1.2 ± 3.7 | 0.8 ± 2.4 | <0.001 | 0.60 |
| Cheese omelet (Count/wk) | 0.4 ± 6.0 | 0.5 ± 6.2 | 0.16 | 0.83 |
| Porridge (Portion/wk) | 0.2 ± 2.1 | 0.2 ± 0.6 | 0.87 | 0.98 |
| Muesli (Portion/wk) | 0.9 ± 5.3 | 0.8 ± 5.6 | 0.001 | 0.97 |
| Green vegetable (Portion/wk) | 3.5 ± 5.9 | 3.9 ± 6.8 | 0.08 | 0.20 |
| Parameters | Non-Osteoporosis | Osteoporosis | Univariate | Adjusted * | p-Value | p-Value * | ||
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Median (Q1–Q3) | Mean ± SD | Median (Q1–Q3) | OR (95%CI) | OR (95%CI) | |||
| Tea with Milk | 33.6 ± 117.2 | 0.0 | 26.4 ± 132.7 | 0.0 | 0.7 (0.6–0.8) | 0.8 (0.6–0.9) | <0.001 | <0.001 |
| Coffee with Milk | 23.9 ± 144.1 | 0.0 | 8.5 ± 50.7 | 0.0 | 0.6 (0.5–0.8) | 0.8 (0.6–1.0) | <0.001 | 0.05 |
| Biscuits, cake, bread slices | 479.5 ± 2920.0 | 240.0 (110.0–350.0) | 432.3 ± 2618.1 | 260.0 (150.0–360.0) | 1.1 (0.9–1.3) | 1.2 (1.0–1.5) | 0.30 | 0.02 |
| Milk and milk products | 1627.9 ± 4794.6 | 1000.0 (335.0–2000.0) | 1641.3 ± 4389.7 | 975.0 (320.0–1850.0) | 1.0 (0.9–1.1) | 1.0 (0.9–1.1) | 0.78 | 0.61 |
| Green vegetables | 140.8 ± 235.5 | 120.0 (40.0–200.0) | 154.5 ± 272.4 | 120.0 (40.0–200.0) | 1.1 (1.0–1.3) | 1.1 (1.0–1.3) | 0.13 | 0.15 |
| Fish and eggs | 601.4 ± 4720.7 | 50.0 (0.0–222.0) | 457.5 ± 5244.5 | 37.0 (0.0–100.0) | 0.8 (0.7–0.9) | 0.8 (0.8–0.9) | <0.001 | 0.001 |
| Porridge and oats | 96.4 ± 553.1 | 0.0 (0.0–100.0) | 80.8 ± 561.9 | 0.0 (0.0–37.0) | 0.8 (0.8–0.9) | 1.0 (0.8–1.1) | 0.005 | 0.37 |
| Model 1 | Model 2 | |||
|---|---|---|---|---|
| OR (95%CI) | p-Value | OR (95%CI) | p-Value | |
| Tea with Milk | 0.8 (0.7–0.9) | 0.005 | 0.8 (0.7–1.0) | 0.02 |
| Coffee with Milk | 0.7 (0.6–0.9) | 0.007 | 0.8 (0.6–1.1) | 0.18 |
| Biscuits, Cakes, Pancakes, Bread | 1.1 (0.9–1.4) | 0.22 | 1.3 (1.0–1.5) | 0.02 |
| Milk and Milk products | 1.0 (0.9–1.1) | 0.83 | 0.9 (0.8–1.1) | 0.30 |
| Green vegetables | 1.2 (1.0–1.4) | 0.08 | 1.1 (0.9–1.3) | 0.32 |
| Fish and Eggs | 0.8 (0.8–0.9) | 0.002 | 0.9 (0.8–1.0) | 0.01 |
| Porridge, Muesli and Oats | 0.9 (0.8–1.0) | 0.18 | 1.0 (0.9–1.1) | 0.94 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Daghri, N.M.; Hussain, S.D.; Alnaami, A.M.; Aljohani, N.; Sabico, S. Dietary Calcium Intake and Osteoporosis Risk in Arab Adults. Nutrients 2023, 15, 2829. https://doi.org/10.3390/nu15132829
Al-Daghri NM, Hussain SD, Alnaami AM, Aljohani N, Sabico S. Dietary Calcium Intake and Osteoporosis Risk in Arab Adults. Nutrients. 2023; 15(13):2829. https://doi.org/10.3390/nu15132829
Chicago/Turabian StyleAl-Daghri, Nasser M., Syed Danish Hussain, Abdullah M. Alnaami, Naji Aljohani, and Shaun Sabico. 2023. "Dietary Calcium Intake and Osteoporosis Risk in Arab Adults" Nutrients 15, no. 13: 2829. https://doi.org/10.3390/nu15132829
APA StyleAl-Daghri, N. M., Hussain, S. D., Alnaami, A. M., Aljohani, N., & Sabico, S. (2023). Dietary Calcium Intake and Osteoporosis Risk in Arab Adults. Nutrients, 15(13), 2829. https://doi.org/10.3390/nu15132829