
Prevalence of Vitamin D Insufficiency and Its Determinants among Women Undergoing In Vitro Fertilization Treatment for Infertility in Sweden

 , , ,
, , ,
Abstract
1. Introduction
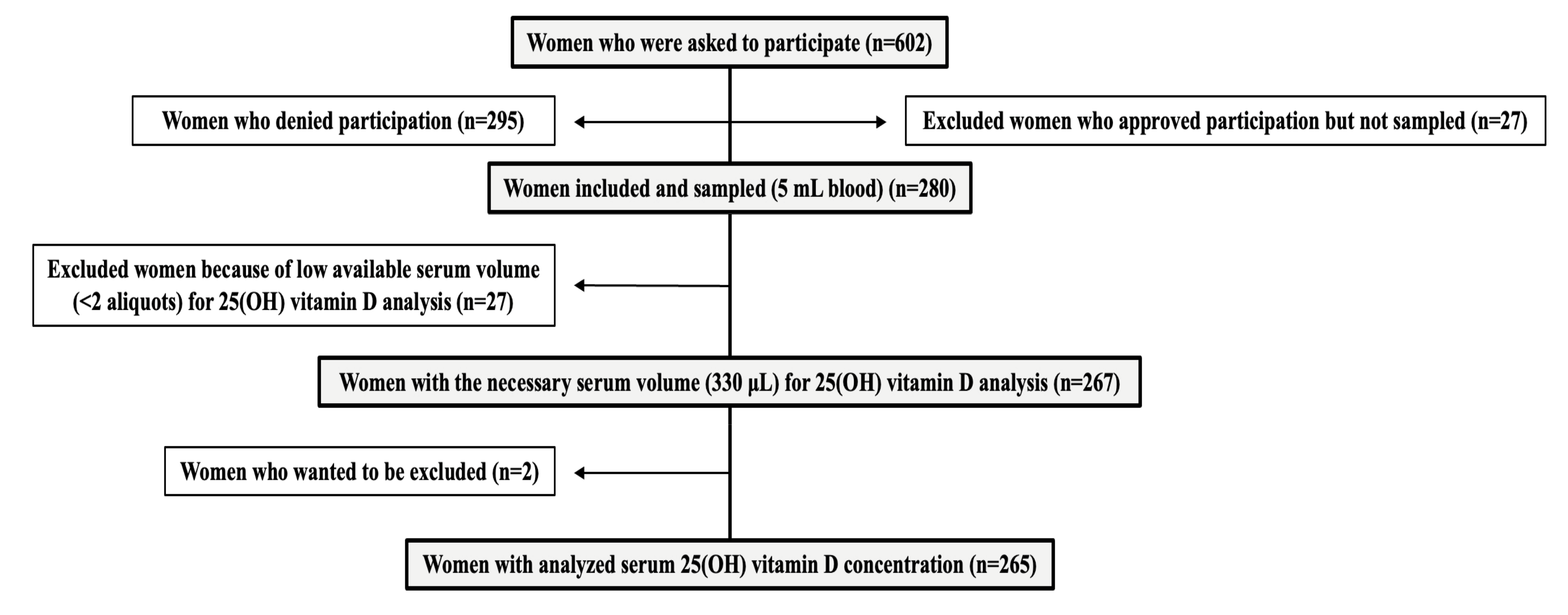
2. Materials and Methods
3. Results
3.1. Prevalence of Serum 25(OH)D Insufficiency
3.2. Determinants of 25(OH)D Insufficiency
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khazai, N.; Judd, S.E.; Tangpricha, V. Calcium and vitamin D: Skeletal and extraskeletal health. Curr. Rheumatol. Rep. 2008, 10, 110–117. [Google Scholar] [CrossRef]
- Moretti, R.; Morelli, M.E.; Caruso, P. Vitamin D in Neurological Diseases: A Rationale for a Pathogenic Impact. Int. J. Mol. Sci. 2018, 19, 2245. [Google Scholar] [CrossRef] [PubMed]
- Gnagnarella, P.; Raimondi, S.; Aristarco, V.; Johansson, H.A.; Bellerba, F.; Corso, F.; Gandini, S. Vitamin D Receptor Polymorphisms and Cancer. Adv. Exp. Med. Biol. 2020, 1268, 53–114. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Li, B.; Gao, X.; Tian, R.; Pan, Y.; Jiang, Y.; Gu, H.; Wang, Y.; Wang, Y.; Liu, G. Serum 25-hydroxyvitamin D and the risk of cardiovascular disease: Dose-response meta-analysis of prospective studies. Am. J. Clin. Nutr. 2017, 105, 810–819. [Google Scholar] [CrossRef] [PubMed]
- Lips, P. Vitamin D physiology. Prog. Biophys. Mol. Biol. 2006, 92, 4–8. [Google Scholar] [CrossRef]
- Institute of Medicine Committee to Review Dietary Reference Intakes for Vitamin D., Calcium. The National Academies Collection: Reports funded by National Institutes of Health. In Dietary Reference Intakes for Calcium and Vitamin D; Ross, A.C., Taylor, C.L., Yaktine, A.L., Del Valle, H.B., Eds.; National Academy of Sciences: Washington, DC, USA, 2011. [Google Scholar]
- Bresson, J.L.; Burlingame, B.; Dean, T.; Fairweather-Tait, S.; Heinonen, M.; Hirsch-Ernst, K.I.; Mangelsdorf, I.; McArdle, H.; Naska, A.; Neuhäuser-Berthold, M.; et al. EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies), 2016. Scientific opinion on dietary reference values for vitamin D. EFSA J. 2016, 14, e04547. [Google Scholar]
- Neville, J.J.; Palmieri, T.; Young, A.R. Physical Determinants of Vitamin D Photosynthesis: A Review. JBMR Plus 2021, 5, e10460. [Google Scholar] [CrossRef]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Kiely, M. Vitamin D deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef]
- Nälsén, C.; Becker, W.; Pearson, M.; Ridefelt, P.; Lindroos, A.K.; Kotova, N.; Mattisson, I. Vitamin D status in children and adults in Sweden: Dietary intake and 25-hydroxyvitamin D concentrations in children aged 10–12 years and adults aged 18–80 years. J. Nutr. Sci. 2020, 9, e47. [Google Scholar] [CrossRef]
- Jääskeläinen, T.; Itkonen, S.T.; Lundqvist, A.; Erkkola, M.; Koskela, T.; Lakkala, K.; Dowling, K.G.; Hull, G.L.; Kröger, H.; Karppinen, J.; et al. The positive impact of general vitamin D food fortification policy on vitamin D status in a representative adult Finnish population: Evidence from an 11-y follow-up based on standardized 25-hydroxyvitamin D data. Am. J. Clin. Nutr. 2017, 105, 1512–1520. [Google Scholar] [CrossRef]
- Itkonen, S.T.; Andersen, R.; Björk, A.K.; Konde, Å.B.; Eneroth, H.; Erkkola, M.; Holvik, K.; Madar, A.A.; Meyer, H.E.; Tetens, I.; et al. Vitamin D status and current policies to achieve adequate vitamin D intake in the Nordic countries. Scand. J. Public Health 2021, 49, 616–627. [Google Scholar] [CrossRef]
- Granlund, L.; Ramnemark, A.; Andersson, C.; Lindkvist, M.; Fhärm, E.; Norberg, M. Prevalence of vitamin D deficiency and its association with nutrition, travelling and clothing habits in an immigrant population in Northern Sweden. Eur. J. Clin. Nutr. 2016, 70, 373–379. [Google Scholar] [CrossRef]
- Osmancevic, A.; Demeke, T.; Gillstedt, M.; Angesjö, E.; Sinclair, H.; Abd El-Gawad, G.; Landin-Wilhelmsen, K. Vitamin D treatment in Somali women living in Sweden—Two randomized, placebo-controlled studies. Clin. Endocrinol. 2016, 85, 535–543. [Google Scholar] [CrossRef]
- He, C.; Lin, Z.; Robb, S.W.; Ezeamama, A.E. Serum Vitamin D Levels and Polycystic Ovary syndrome: A Systematic Review and Meta-Analysis. Nutrients 2015, 7, 4555–4577. [Google Scholar] [CrossRef] [PubMed]
- Somigliana, E.; Panina-Bordignon, P.; Murone, S.; Di Lucia, P.; Vercellini, P.; Vigano, P. Vitamin D reserve is higher in women with endometriosis. Hum. Reprod. 2007, 22, 2273–2278. [Google Scholar] [CrossRef]
- Vienonen, A.; Miettinen, S.; Bläuer, M.; Martikainen, P.M.; Tomás, E.; Heinonen, P.K.; Ylikomi, T. Expression of nuclear receptors and cofactors in human endometrium and myometrium. J. Soc. Gynecol. Investig. 2004, 11, 104–112. [Google Scholar] [CrossRef]
- Bagot, C.N.; Troy, P.J.; Taylor, H.S. Alteration of maternal Hoxa10 expression by in vivo gene transfection affects implantation. Gene Ther. 2000, 7, 1378–1384. [Google Scholar] [CrossRef]
- Du, H.; Daftary, G.S.; Lalwani, S.I.; Taylor, H.S. Direct regulation of HOXA10 by 1,25-(OH)2D3 in human myelomonocytic cells and human endometrial stromal cells. Mol. Endocrinol. 2005, 19, 2222–2233. [Google Scholar] [CrossRef]
- Viganò, P.; Lattuada, D.; Mangioni, S.; Ermellino, L.; Vignali, M.; Caporizzo, E.; Panina-Bordignon, P.; Besozzi, M.; Di Blasio, A.M. Cycling and early pregnant endometrium as a site of regulated expression of the vitamin D system. J. Mol. Endocrinol. 2006, 36, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Paffoni, A.; Ferrari, S.; Viganò, P.; Pagliardini, L.; Papaleo, E.; Candiani, M.; Tirelli, A.; Fedele, L.; Somigliana, E. Vitamin D Deficiency and Infertility: Insights From in vitro Fertilization Cycles. J. Clin. Endocrinol. Metab. 2014, 99, E2372–E2376. [Google Scholar] [CrossRef] [PubMed]
- Polyzos, N.P.; Anckaert, E.; Guzman, L.; Schiettecatte, J.; Van Landuyt, L.; Camus, M.; Smitz, J.; Tournaye, H. Vitamin D deficiency and pregnancy rates in women undergoing single embryo, blastocyst stage, transfer (SET) for IVF/ICSI. Hum. Reprod. 2014, 29, 2032–2040. [Google Scholar] [CrossRef] [PubMed]
- Banker, M.; Sorathiya, D.; Shah, S. Vitamin D deficiency does not influence reproductive outcomes of IVF-ICSI: A study of oocyte donors and recipients. J. Hum. Reprod. Sci. 2017, 10, 79–85. [Google Scholar] [CrossRef] [PubMed]
- van de Vijver, A.; Drakopoulos, P.; Van Landuyt, L.; Vaiarelli, A.; Blockeel, C.; Santos-Ribeiro, S.; Tournaye, H.; Polyzos, N.P. Vitamin D deficiency and pregnancy rates following frozen–thawed embryo transfer: A prospective cohort study. Hum. Reprod. 2016, 31, 1749–1754. [Google Scholar] [CrossRef] [PubMed]
- Iliuta, F.; Pijoan, J.I.; Lainz, L.; Exposito, A.; Matorras, R. Women’s vitamin D levels and IVF results: A systematic review of the literature and meta-analysis, considering three categories of vitamin status (replete, insufficient and deficient). Hum. Fertility 2022, 25, 228–246. [Google Scholar] [CrossRef]
- Bärebring, L.; Amberntsson, A.; Winkvist, A.; Augustin, H. Validation of Dietary Vitamin D Intake from Two Food Frequency Questionnaires, Using Food Records and the Biomarker 25-Hydroxyvitamin D among Pregnant Women. Nutrients 2018, 10, 745. [Google Scholar] [CrossRef]
- Fitzpatrick, T.B. The validity and practicality of sun-reactive skin types I through VI. Arch Dermatol. 1988, 124, 869–871. [Google Scholar] [CrossRef]
- Lee, J.-Y.; Choi, J.-W. Estimation of Regional Body Surface Area Covered by Clothing. J. Hum.-Environ. Syst. 2009, 12, 35–45. [Google Scholar] [CrossRef]
- Seifer, D.B.; Sharara, F.I.; Jain, T. The Disparities in ART (DART) Hypothesis of Racial and Ethnic Disparities in Access and Outcomes of IVF Treatment in the USA. Reprod. Sci. 2022, 29, 2084–2088. [Google Scholar] [CrossRef]


{kind=link}
| 25(OH)D Insufficiency (<50 nmol/L) (n = 72) | 25(OH)D Sufficiency (≥50 nmol/L) (n = 193) | Crude p-Value Pairwise Analyses (*) | |
|---|---|---|---|
| Age (years) | 32 ± 7 (20–39) | 32 ± 6 (23–39) | 0.384 |
| BMI (Kg/m2) | 24.7 ± 6 (19–38) | 23.5 ± 6.5 (17–35) | 0.068 |
| Season of blood sampling | 0.021 | ||
| Spring (29.8%) | 17 (21.5%) | 62 (78.5%) | |
| Summer (10.2%) | 2 (7.4%) | 25 (92.6%) | 0.011 (summer vs. winter) * |
| Autumn (29.8%) | 17 (21.5%) | 62 (78.5%) | |
| Winter (29%) | 25 (32.5%) | 52 (67.5%) | |
| Serum 25(OH)D (nmol/L) | 39 ± 15 (15–49) | 70 ± 20 (50–141) | <0.001 |
| Spring (21.5% with insufficiency) | 37 ± 15 (15–49) | 64 ± 19 (50–114) | <0.001 |
| Summer (7.4% with insufficiency) | 39 ± 0 (37–41) | 75 ± 18 (52–113) | 0.030 |
| Autumn (21.5% with insufficiency) | 37 ± 19 (21–49) | 73 ± 20 (51–136) | <0.001 |
| Winter (32.5% with insufficiency) | 42 ± 14 (19–49) | 69.5 ± 19 (51–141) | <0.001 |
| Previous pregnancies | 0.958 | ||
| Yes | 24 (30.4%) | 65 (69.6%) | |
| No | 48 (27.3%) | 128 (72.3%) | |
| Previous children | 0.766 | ||
| Yes | 3 (20%) | 12 (80%) | |
| No | 69 (27.6%) | 181 (72.4%) | |
| Infertility cause | 0.889 | ||
| Unexplained | 2 (2.4%) | 81 (97.6%) | |
| Male | 21 (27.3%) | 56 (72.3%) | |
| Anovulation | 10 (25%) | 30 (75%) | |
| Endometriosis | 5 (35.7%) | 9 (64.3%) | |
| Tubal | 7 (33.3%) | 14 (66.7%) | |
| Uterine | - | 1 (100%) | |
| Premature ovarian insufficiency | 1 (50%) | 1 (50%) | |
| (missing data n = 1, 0.4%) | |||
| Infertility duration (months) | 36 ± 24 (17–120) | 24 ± 12 (12–96) | <0.001 |
| Mean antral follicle count | 10 ± 7 (1–29) | 9 ± 8 (1–30) | 0.989 |
| Country of origin | <0.001 | ||
| Nordic | 30 (16.5%) | 152 (83.5%) | |
| Non-Nordic European | 12 (41.4%) | 17 (58.6%) | 0.003 (Nordic vs. Non-Nordic European) * |
| Middle Eastern | 19 (63.3%) | 11 (36.7%) | <0.001 (Nordic vs. Middle East) * |
| Asian | 8 (50%) | 8 (50%) | 0.003 (Nordic vs. Asian) * |
| African | 1 (33.3%) | 2 (66.7%) | |
| Central/South American | 1 (50%) | 1 (50%) | |
| (missing data n = 3, 1.1%) | |||
| Education level | 0.062 | ||
| Elementary school | 3 (37.5%) | 5 (62.5%) | |
| High school | 28 (35.4%) | 51 (64.6%) | |
| University | 38 (22%) | 135 (78%) | |
| (missing data n = 5, 1.9%) | |||
| Smoking/snuffing | 0.584 | ||
| No | 65 (26.5%) | 180 (73.5%) | |
| Yes | 6 (33.3%) | 12 (66.7%) | |
| (missing data n = 2, 0.8%) | |||
| Use of vitamin D supplements | 0.001 | ||
| Yes | 25 (18.3%) | 112 (81.7%) | |
| No | 47 (36.7%) | 81 (63.3%) | |
| Daily dietary vitamin D intake (μg) | 5.8 ± 6.8 (3.4–10.2) | 6.9 ± 6 (4.2–10.2) | 0.122 |
| Skin phototypes (Fitzpatrick scale) | 0.007 | ||
| Type I | 2 (28.6%) | 5 (71.4%) | |
| Type II | 23 (27.1%) | 62 (72.9%) | 0.004 (Type II vs. Type V) * |
| Type III | 24 (22.2%) | 84 (77.8%) | 0.001 (Type III vs. Type V) * |
| Type IV | 11 (27.5%) | 29 (72.5%) | |
| Type V | 11 (64.7%) | 6 (35.3%) | |
| Type VI | 1 (100%) | - | |
| (missing data n = 7, 2.6%) | |||
| Sun vacations | 0.649 | ||
| Yes | 2 (20%) | 8 (80%) | |
| No | 70 (27.5%) | 185 (72.5%) | |
| Length of sun exposure on sunny days | 0.109 | ||
| Less than 1 h | 15 (38.5%) | 24 (61.5%) | |
| Between 1–2 h | 25 (29.8%) | 59 (70.2%) | |
| More than 2 h | 31 (23%) | 104 (77%) | |
| (missing data n = 7, 2.6%) | |||
| Type of sun exposure on sunny days | 0.022 | ||
| In the sun all the time | 10 (15.4%) | 55 (84.6%) | |
| Both in the sun and shade | 54 (30.7%) | 122 (69.3%) | |
| In the shade all the time | 8 (42.1%) | 11 (57.9%) | 0.016 (In the sun all the time vs. in the shade all the time) * |
| (missing data n = 5, 1.9%) | |||
| Sun-exposed regional body surface area (%) | 82 ± 62 (0–90) | 89.5 ± 15 (0–90) | <0.001 |
| Odds Ratio | 95% CI | Adjusted p-Value | |
|---|---|---|---|
| Country of origin | <0.001 | ||
| Non-Nordic European vs. Nordic | 2.92 | 1.03–8.26 | 0.043 |
| Middle Eastern vs. Nordic | 9.90 | 3.32–29.41 | <0.001 |
| Asian vs. Nordic | 5.49 | 1.30–23.25 | 0.020 |
| Use of vitamin D supplements | 3.32 | 1.55–7.10 | 0.002 |
| Type of sun exposure on sunny days | 0.049 | ||
| “In the shade all the time “ vs. “In the sun all the time” | 3.24 | 1.22–8.62 | 0.018 |
| “In the shade all the time “ vs. “Both in the sun and shade” | 1.45 | 0.27–7.87 | 0.664 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maaherra Armstrong, P.; Augustin, H.; Bärebring, L.; Osmancevic, A.; Bullarbo, M.; Thurin-Kjellberg, A.; Tsiartas, P. Prevalence of Vitamin D Insufficiency and Its Determinants among Women Undergoing In Vitro Fertilization Treatment for Infertility in Sweden. Nutrients 2023, 15, 2820. https://doi.org/10.3390/nu15122820
Maaherra Armstrong P, Augustin H, Bärebring L, Osmancevic A, Bullarbo M, Thurin-Kjellberg A, Tsiartas P. Prevalence of Vitamin D Insufficiency and Its Determinants among Women Undergoing In Vitro Fertilization Treatment for Infertility in Sweden. Nutrients. 2023; 15(12):2820. https://doi.org/10.3390/nu15122820
Chicago/Turabian StyleMaaherra Armstrong, Paulina, Hanna Augustin, Linnea Bärebring, Amra Osmancevic, Maria Bullarbo, Ann Thurin-Kjellberg, and Panagiotis Tsiartas. 2023. "Prevalence of Vitamin D Insufficiency and Its Determinants among Women Undergoing In Vitro Fertilization Treatment for Infertility in Sweden" Nutrients 15, no. 12: 2820. https://doi.org/10.3390/nu15122820
APA StyleMaaherra Armstrong, P., Augustin, H., Bärebring, L., Osmancevic, A., Bullarbo, M., Thurin-Kjellberg, A., & Tsiartas, P. (2023). Prevalence of Vitamin D Insufficiency and Its Determinants among Women Undergoing In Vitro Fertilization Treatment for Infertility in Sweden. Nutrients, 15(12), 2820. https://doi.org/10.3390/nu15122820