
Survey of Dietary Habits and Physical Activity in Japanese Patients with Non-Obese Non-Alcoholic Fatty Liver Disease

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
2.2. Data Collection
2.3. Statistical Analysis
2.4. Ethics Approval and Consent to Participate
3. Results
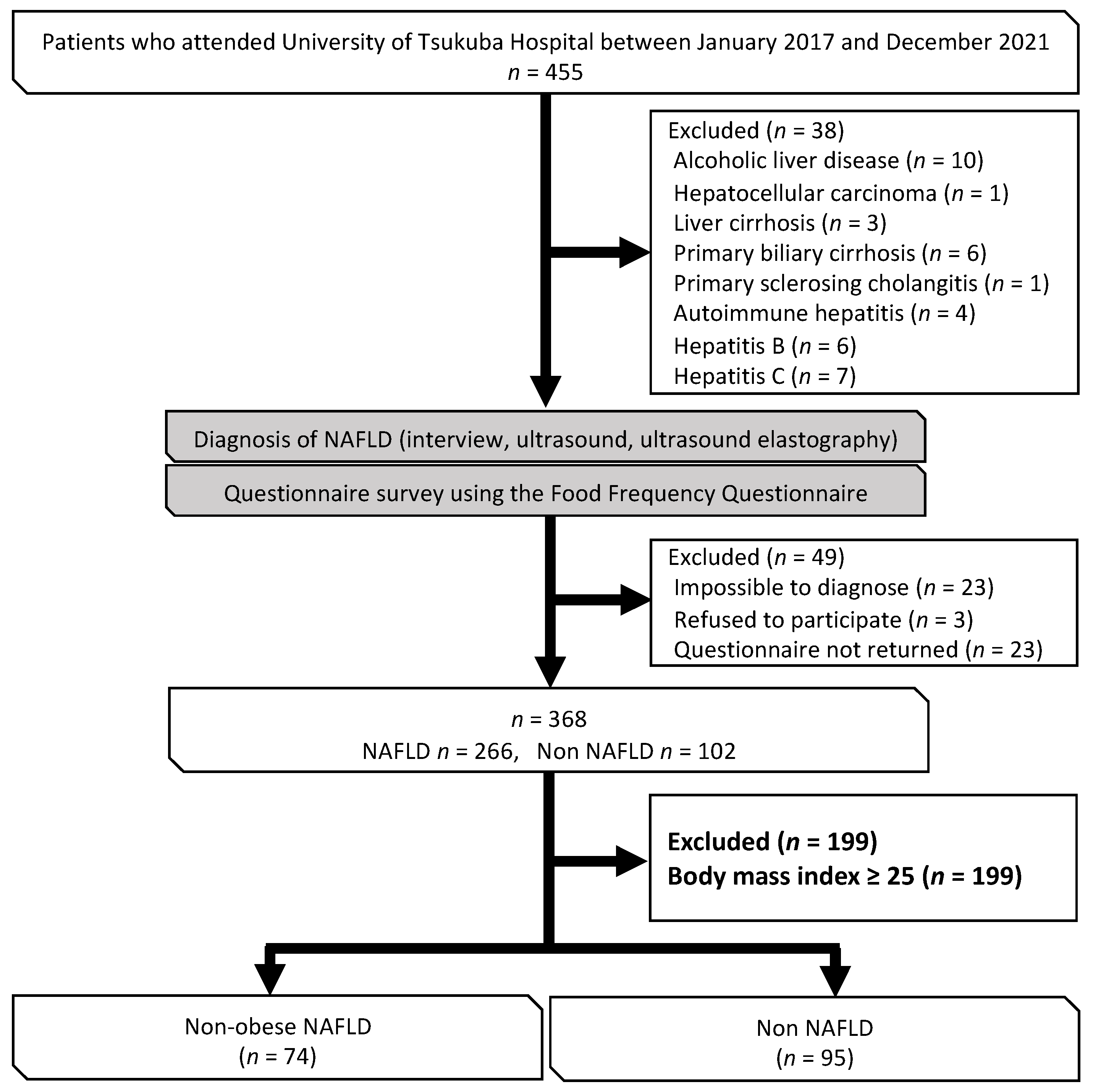
3.1. Cohort Formation and Patient Demographic and Clinical Characteristics
3.2. Questionnaire on Dietary Habits and Physical Activity
3.3. Association between Non-Obese NAFLD and Food Intake Frequency
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wong, V.W.; Wong, G.L.; Yeung, D.K.; Lau, T.K.; Chan, C.K.; Chim, A.M.; Abrigo, J.M.; Chan, R.S.; Woo, J.; Tse, Y.K.; et al. Incidence of non-alcoholic fatty liver disease in Hong Kong: A population study with paired proton-magnetic resonance spectroscopy. J. Hepatol. 2015, 62, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Chung, G.E.; Kim, D.; Kim, W.; Yim, J.Y.; Park, M.J.; Kim, Y.J.; Yoon, J.H.; Lee, H.S. Non-alcoholic fatty liver disease across the spectrum of hypothyroidism. J. Hepatol. 2012, 57, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.J. Prevalence and risk factors for non-alcoholic fatty liver disease in Asian people who are not obese. J. Gastroenterol. Hepatol. 2012, 27, 1555–1560. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.L.; Leung, J.C.; Loong, T.C.; Wong, G.L.; Yeung, D.K.; Chan, R.S.; Chan, H.L.; Chim, A.M.; Woo, J.; Chu, W.C.; et al. Prevalence and Severity of Nonalcoholic Fatty Liver Disease in Non-Obese Patients: A Population Study Using Proton-Magnetic Resonance Spectroscopy. Am. J. Gastroenterol. 2015, 110, 1306–1314; quiz 1315. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; George, J.; Bugianesi, E. Global burden of NAFLD and NASH: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 11–20. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Stepanova, M.; Negro, F.; Hallaji, S.; Younossi, Y.; Lam, B.; Srishord, M. Nonalcoholic fatty liver disease in lean individuals in the United States. Medicine 2012, 91, 319–327. [Google Scholar] [CrossRef]
- Kim, D.; Kim, W.R. Nonobese Fatty Liver Disease. Clin. Gastroenterol. Hepatol. 2017, 15, 474–485. [Google Scholar] [CrossRef]
- Ito, T.; Ishigami, M.; Zou, B.; Tanaka, T.; Takahashi, H.; Kurosaki, M.; Maeda, M.; Thin, K.N.; Tanaka, K.; Takahashi, Y.; et al. The epidemiology of NAFLD and lean NAFLD in Japan: A meta-analysis with individual and forecasting analysis, 1995–2040. Hepatol. Int. 2021, 15, 366–379. [Google Scholar] [CrossRef]
- Oniki, K.; Saruwatari, J.; Izuka, T.; Kajiwara, A.; Morita, K.; Sakata, M.; Otake, K.; Ogata, Y.; Nakagawa, K. Influence of the PNPLA3 rs738409 Polymorphism on Non-Alcoholic Fatty Liver Disease and Renal Function among Normal Weight Subjects. PLoS ONE 2015, 10, e0132640. [Google Scholar] [CrossRef]
- Nishioji, K.; Mochizuki, N.; Kobayashi, M.; Kamaguchi, M.; Sumida, Y.; Nishimura, T.; Yamaguchi, K.; Kadotani, H.; Itoh, Y. The Impact of PNPLA3 rs738409 Genetic Polymorphism and Weight Gain ≥10 kg after Age 20 on Non-Alcoholic Fatty Liver Disease in Non-Obese Japanese Individuals. PLoS ONE 2015, 10, e0140427. [Google Scholar] [CrossRef]
- Shida, T.; Oshida, N.; Suzuki, H.; Okada, K.; Watahiki, T.; Oh, S.; Kim, T.; Isobe, T.; Okamoto, Y.; Ariizumi, S.I.; et al. Clinical and anthropometric characteristics of non-obese non-alcoholic fatty liver disease subjects in Japan. Hepatol. Res. 2020, 50, 1032–1046. [Google Scholar] [CrossRef]
- Dela Cruz, A.C.; Bugianesi, E.; George, J.; Day, C.; Liaquat, H.; Charatcharoenwitthaya, P.; Mills, P.; Dam-Larsen, S.; Bjõrnsson, E.; Haflidadottir, S.; et al. 379 Characteristics and Long-Term Prognosis of Lean Patients with Nonalcoholic Fatty Liver Disease. Gastroenterology 2014, 146, S-909. [Google Scholar] [CrossRef]
- Wong, V.W.; Wong, G.L.; Chan, R.S.; Shu, S.S.; Cheung, B.H.; Li, L.S.; Chim, A.M.; Chan, C.K.; Leung, J.K.; Chu, W.C.; et al. Beneficial effects of lifestyle intervention in non-obese patients with non-alcoholic fatty liver disease. J. Hepatol. 2018, 69, 1349–1356. [Google Scholar] [CrossRef]
- Romero-Gómez, M.; Aller, R.; Martín-Bermudo, F. Dietary Recommendations for the Management of Non-alcoholic Fatty Liver Disease (NAFLD): A Nutritional Geometry Perspective. Semin. Liver Dis. 2022, 42, 434–445. [Google Scholar] [CrossRef]
- Noto, H.; Tokushige, K.; Hashimoto, E.; Taniai, M.; Shiratori, K. Questionnaire survey on lifestyle of patients with nonalcoholic steatohepatitis. J. Clin. Biochem. Nutr. 2014, 55, 191–195. [Google Scholar] [CrossRef]
- Romero-Gómez, M.; Zelber-Sagi, S.; Trenell, M. Treatment of NAFLD with diet, physical activity and exercise. J. Hepatol. 2017, 67, 829–846. [Google Scholar] [CrossRef]
- Sánchez-Calvo, B.; Cassina, A.; Mastrogiovanni, M.; Santos, M.; Trias, E.; Kelley, E.E.; Rubbo, H.; Trostchansky, A. Olive oil-derived nitro-fatty acids: Protection of mitochondrial function in non-alcoholic fatty liver disease. J. Nutr. Biochem. 2021, 94, 108646. [Google Scholar] [CrossRef]
- Sekiya, M.; Yahagi, N.; Matsuzaka, T.; Najima, Y.; Nakakuki, M.; Nagai, R.; Ishibashi, S.; Osuga, J.; Yamada, N.; Shimano, H. Polyunsaturated fatty acids ameliorate hepatic steatosis in obese mice by SREBP-1 suppression. Hepatology 2003, 38, 1529–1539. [Google Scholar] [CrossRef]
- Levy, J.R.; Clore, J.N.; Stevens, W. Dietary n-3 polyunsaturated fatty acids decrease hepatic triglycerides in Fischer 344 rats. Hepatology 2004, 39, 608–616. [Google Scholar] [CrossRef]
- Mizowaki, Y.; Sugawara, S.; Yamamoto, K.; Sakamoto, Y.; Iwagaki, Y.; Kawakami, Y.; Igarashi, M.; Tsuduki, T. Comparison of the Effects of the 1975 Japanese Diet and the Modern Mediterranean Diet on Lipid Metabolism in Mice. J. Oleo Sci. 2017, 66, 507–519. [Google Scholar] [CrossRef]
- Oh, S.; Shida, T.; Yamagishi, K.; Tanaka, K.; So, R.; Tsujimoto, T.; Shoda, J. Moderate to vigorous physical activity volume is an important factor for managing nonalcoholic fatty liver disease: A retrospective study. Hepatology 2015, 61, 1205–1215. [Google Scholar] [CrossRef] [PubMed]
- Yabe, Y.; Kim, T.; Oh, S.; Shida, T.; Oshida, N.; Hasegawa, N.; Okada, K.; Someya, N.; Mizokami, Y.; Shoda, J. Relationships of Dietary Habits and Physical Activity Status with Non-Alcoholic Fatty Liver Disease Featuring Advanced Fibrosis. Int. J. Environ. Res. Public Health 2021, 18, 8918. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The diagnosis and management of non-alcoholic fatty liver disease: Practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroenterology 2012, 142, 1592–1609. [Google Scholar] [CrossRef] [PubMed]
- Shida, T.; Akiyama, K.; Oh, S.; Sawai, A.; Isobe, T.; Okamoto, Y.; Ishige, K.; Mizokami, Y.; Yamagata, K.; Onizawa, K.; et al. Skeletal muscle mass to visceral fat area ratio is an important determinant affecting hepatic conditions of non-alcoholic fatty liver disease. J. Gastroenterol. 2018, 53, 535–547. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, R.N.; Koehler, K.M.; Gallagher, D.; Romero, L.; Heymsfield, S.B.; Ross, R.R.; Garry, P.J.; Lindeman, R.D. Epidemiology of sarcopenia among the elderly in New Mexico. Am. J. Epidemiol. 1998, 147, 755–763. [Google Scholar] [CrossRef]
- Studenski, S.A.; Peters, K.W.; Alley, D.E.; Cawthon, P.M.; McLean, R.R.; Harris, T.B.; Ferrucci, L.; Guralnik, J.M.; Fragala, M.S.; Kenny, A.M.; et al. The FNIH sarcopenia project: Rationale, study description, conference recommendations, and final estimates. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 547–558. [Google Scholar] [CrossRef]
- Kim, T.N.; Park, M.S.; Lim, K.I.; Yang, S.J.; Yoo, H.J.; Kang, H.J.; Song, W.; Seo, J.A.; Kim, S.G.; Kim, N.H.; et al. Skeletal muscle mass to visceral fat area ratio is associated with metabolic syndrome and arterial stiffness: The Korean Sarcopenic Obesity Study (KSOS). Diabetes Res. Clin. Pract. 2011, 93, 285–291. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Vallet-Pichard, A.; Mallet, V.; Nalpas, B.; Verkarre, V.; Nalpas, A.; Dhalluin-Venier, V.; Fontaine, H.; Pol, S. FIB-4: An inexpensive and accurate marker of fibrosis in HCV infection. comparison with liver biopsy and fibrotest. Hepatology 2007, 46, 32–36. [Google Scholar] [CrossRef]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD fibrosis score: A noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef]
- Newsome, P.N.; Sasso, M.; Deeks, J.J.; Paredes, A.; Boursier, J.; Chan, W.K.; Yilmaz, Y.; Czernichow, S.; Zheng, M.H.; Wong, V.W.; et al. FibroScan-AST (FAST) score for the non-invasive identification of patients with non-alcoholic steatohepatitis with significant activity and fibrosis: A prospective derivation and global validation study. Lancet Gastroenterol. Hepatol. 2020, 5, 362–373. [Google Scholar] [CrossRef]
- Nobuo, Y.; Fumi, H.; Yukari, T.; Keiko, M.; Fukue, S. A New Food Guide in Japan: The Japanese Food Guide Spinning Top. Nutr. Rev. 2007, 65, 149–154. [Google Scholar]
- Haukoos, J.S.; Lewis, R.J. The Propensity Score. JAMA 2015, 314, 1637–1638. [Google Scholar] [CrossRef]
- Ministry of Education, Culture, Sports, Science and Technology. Standards Tables of Food Composition in Japan, 17th ed.; Documentation and Table; Ministry of Education, Culture, Sports, Science and Technology: Tokyo, Japan, 2015. [Google Scholar]
- Kato, H.; Tillotson, J.; Nichaman, M.Z.; Rhoads, G.G.; Hamilton, H.B. Epidemiologic studies of coronary heart disease and stroke in Japanese men living in Japan, Hawaii and California. Am. J. Epidemiol. 1973, 97, 372–385. [Google Scholar] [CrossRef]
- Bray, G.A.; Nielsen, S.J.; Popkin, B.M. Consumption of high-fructose corn syrup in beverages may play a role in the epidemic of obesity. Am. J. Clin. Nutr. 2004, 79, 537–543. [Google Scholar] [CrossRef]
- Scorletti, E.; Byrne, C.D. Omega-3 fatty acids and non-alcoholic fatty liver disease: Evidence of efficacy and mechanism of action. Mol. Aspects Med. 2018, 64, 135–146. [Google Scholar] [CrossRef]
- Molendi-Coste, O.; Legry, V.; Leclercq, I.A. Dietary lipids and NAFLD: Suggestions for improved nutrition. Acta Gastroenterol. Belg. 2010, 73, 431–436. [Google Scholar]
- Hussein, O.; Grosovski, M.; Lasri, E.; Svalb, S.; Ravid, U.; Assy, N. Monounsaturated fat decreases hepatic lipid content in non-alcoholic fatty liver disease in rats. World J. Gastroenterol. 2007, 13, 361–368. [Google Scholar] [CrossRef]
- Kruse, M.; von Loeffelholz, C.; Hoffmann, D.; Pohlmann, A.; Seltmann, A.C.; Osterhoff, M.; Hornemann, S.; Pivovarova, O.; Rohn, S.; Jahreis, G.; et al. Dietary rapeseed/canola-oil supplementation reduces serum lipids and liver enzymes and alters postprandial inflammatory responses in adipose tissue compared to olive-oil supplementation in obese men. Mol. Nutr. Food Res. 2015, 59, 507–519. [Google Scholar] [CrossRef]
- Zhao, Y.C.; Zhao, G.J.; Chen, Z.; She, Z.G.; Cai, J.; Li, H. Nonalcoholic Fatty Liver Disease: An Emerging Driver of Hypertension. Hypertension 2020, 75, 275–284. [Google Scholar] [CrossRef]
- Choi, Y.; Lee, J.E.; Chang, Y.; Kim, M.K.; Sung, E.; Shin, H.; Ryu, S. Dietary sodium and potassium intake in relation to non-alcoholic fatty liver disease. Br. J. Nutr. 2016, 116, 1447–1456. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.; Tsujimoto, T.; Kim, B.; Uchida, F.; Suzuki, H.; Iizumi, S.; Isobe, T.; Sakae, T.; Tanaka, K.; Shoda, J. Weight-loss-independent benefits of exercise on liver steatosis and stiffness in Japanese men with NAFLD. JHEP Rep. 2021, 3, 100253. [Google Scholar] [CrossRef] [PubMed]
- Nelson, M.; Black, A.E.; Morris, J.A.; Cole, T.J. Between- and within-subject variation in nutrient intake from infancy to old age: Estimating the number of days required to rank dietary intakes with desired precision. Am. J. Clin. Nutr. 1989, 50, 155–167. [Google Scholar] [CrossRef] [PubMed]
- Okubo, H.; Sasaki, S.; Hirota, N.; Notsu, A.; Todoriki, H.; Miura, A.; Fukui, M.; Date, C. The influence of age and body mass index on relative accuracy of energy intake among Japanese adults. Public Health Nutr. 2006, 9, 651–657. [Google Scholar] [CrossRef]


{kind=link}
| Non-Obese NAFLD | Non-NAFLD | ||||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p-Value | |||
| Age, years | 61.7 | ± | 14.2 | 58.7 | ± | 18.0 | 0.663 |
| Male sex, n (%) | 35 (47.3) | 27 (28.4) | 0.012 | ||||
| Body mass index | 22.6 | ± | 2.0 | 21.4 | ± | 2.1 | <0.001 |
| Fat, kg | 16.4 | ± | 3.9 | 14.1 | ± | 4.3 | <0.001 |
| Percent body fat, % | 28.0 | ± | 6.6 | 25.7 | ± | 7.8 | 0.021 |
| Waist-to-hip ratio | 0.9 | ± | 0.1 | 0.8 | ± | 0.0 | <0.001 |
| Skeletal muscle mass, Kg | 23.0 | ± | 5.0 | 21.9 | ± | 5.1 | 0.121 |
| Arm muscle, kg | 2.1 | ± | 0.6 | 1.9 | ± | 0.6 | 0.018 |
| Trunk muscle, kg | 18.8 | ± | 3.8 | 17.6 | ± | 3.9 | 0.022 |
| Leg muscle, kg | 6.4 | ± | 1.5 | 6.2 | ± | 1.5 | 0.230 |
| Total body water, L | 31.1 | ± | 6.0 | 29.7 | ± | 5.8 | 0.111 |
| Soft lean mass, kg | 39.9 | ± | 7.8 | 38.4 | ± | 7.8 | 0.159 |
| Fat free mass, kg | 42.2 | ± | 8.1 | 40.1 | ± | 7.9 | 0.081 |
| Visceral fat cross-sectional area, cm2 | 74.6 | ± | 23.6 | 64.7 | ± | 26.9 | 0.002 |
| SMI, kg/m2 | 6.5 | ± | 0.9 | 6.3 | ± | 0.9 | 0.079 |
| SI, kg/(kg/m2) | 0.8 | ± | 0.2 | 0.8 | ± | 0.2 | 0.736 |
| SV ratio, kg/cm2 | 339.4 | ± | 129.4 | 408.7 | ± | 246.0 | 0.094 |
| Hand grip, kgf | 28.9 | ± | 7.9 | 27.0 | ± | 8.3 | 0.072 |
| Knee extension stretch, kgf | 36.0 | ± | 10.6 | 34.8 | ± | 12.4 | 0.201 |
| LSM, kPa | 6.2 | ± | 3.3 | 4.7 | ± | 3.4 | <0.001 |
| CAP, dB/m | 280.4 | ± | 39.5 | 190.5 | ± | 34.8 | <0.001 |
| TP, g/dL | 7.4 | ± | 0.5 | 7.2 | ± | 0.5 | 0.032 |
| Albumin, g/dL | 4.4 | ± | 0.3 | 4.3 | ± | 0.3 | 0.120 |
| AST, U/L | 33.0 | ± | 17.1 | 23.8 | ± | 8.8 | <0.001 |
| ALT, U/L | 39.2 | ± | 30.9 | 20.0 | ± | 12.8 | <0.001 |
| LD, U/L | 174.6 | ± | 33.4 | 183.2 | ± | 40.5 | 0.309 |
| ALP, U/L | 207.8 | ± | 99.8 | 189.4 | ± | 88.9 | 0.211 |
| CHE, U/L | 350.1 | ± | 89.2 | 319.4 | ± | 78.6 | 0.001 |
| γ-GT, U/L | 50.8 | ± | 44.1 | 32.3 | ± | 41.0 | <0.001 |
| Creatinine, mg/dL | 0.7 | ± | 0.2 | 0.7 | ± | 0.2 | 0.178 |
| Fasting glucose, mg/dL | 118.3 | ± | 32.0 | 101.9 | ± | 25.2 | <0.001 |
| HbA1c, % | 6.2 | ± | 0.8 | 5.7 | ± | 0.7 | <0.001 |
| Insulin | 13.3 | ± | 17.0 | 6.0 | ± | 5.1 | <0.001 |
| HOMA-IR | 4.0 | ± | 6.0 | 1.5 | ± | 1.3 | <0.001 |
| CHO, mg/dL | 199.8 | ± | 44.3 | 210.8 | ± | 37.0 | 0.094 |
| HDL-C, mg/dL | 51.2 | ± | 12.7 | 69.7 | ± | 16.4 | <0.001 |
| LDL-C, mg/dL | 119.9 | ± | 35.5 | 116.9 | ± | 28.5 | 0.493 |
| Triglycerides, mg/dL | 132.8 | ± | 81.2 | 82.4 | ± | 43.1 | <0.001 |
| Platelets, mg/dL | 226.9 | ± | 62.9 | 221.0 | ± | 56.4 | 0.960 |
| CRP, ng/mL | 0.2 | ± | 0.3 | 0.1 | ± | 0.2 | <0.001 |
| Ferritin, ng/mL | 130.7 | ± | 129.4 | 76.0 | ± | 57.6 | 0.001 |
| Hyaluronic acid, ng/mL | 51.6 | ± | 54.4 | 48.2 | ± | 48.5 | 0.707 |
| Type IV collagen, ng/mL | 118.3 | ± | 36.2 | 116.1 | ± | 42.9 | 0.755 |
| M2BPGi, C.O.I. | 0.8 | ± | 0.5 | 0.7 | ± | 0.5 | 0.199 |
| FAST score | 0.24 | ± | 0.20 | 0.08 | ± | 0.09 | <0.001 |
| FIB-4 index | 1.76 | ± | 1.12 | 1.96 | ± | 3.03 | 0.751 |
| NAFLD fibrosis score | −1.67 | ± | 1.78 | −1.64 | ± | 1.61 | 0.889 |
| Systolic BP, mmHg | 133.1 | ± | 17.2 | 123.9 | ± | 14.9 | <0.001 |
| Diastolic BP, mmHg | 78.9 | ± | 12.4 | 73.8 | ± | 10.3 | 0.002 |
| Diabetes mellitus, n (%) | 27 (37.5) | 11 (12.1) | <0.001 | ||||
| Hypertension, n (%) | 37 (50.0) | 24 (25.3) | 0.001 | ||||
| Dyslipidemia, n (%) | 49 (70.0) | 27 (33.8) | <0.001 | ||||
| Non-Obese NAFLD | Non-NAFLD | |||||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p-Value | ||||
| PAL | 1.60 | ± | 0.3 | 1.7 | ± | 0.5 | 0.054 | |
| Ex | METs/hours/week | 8.00 | ± | 14.1 | 11.5 | ± | 21.7 | 0.485 |
| Potatoes, pumpkin, and lotus root | times/week | 2.15 | ± | 0.46 | 2.19 | ± | 0.7 | 0.982 |
| Fruit | times/week | 2.59 | ± | 0.91 | 2.82 | ± | 0.9 | 0.089 |
| Meat and meat products | times/week | 2.82 | ± | 0.69 | 2.71 | ± | 0.7 | 0.362 |
| Fish and fish products | times/week | 2.28 | ± | 0.61 | 2.56 | ± | 0.7 | 0.004 |
| Seafood | times/week | 2.05 | ± | 0.58 | 2.17 | ± | 0.7 | 0.269 |
| Eggs | times/week | 2.77 | ± | 0.73 | 2.82 | ± | 0.8 | 0.647 |
| Soybeans and soybean products | times/week | 2.96 | ± | 0.78 | 2.97 | ± | 0.8 | 0.749 |
| Milk and milk products | times/week | 3.11 | ± | 0.85 | 3.17 | ± | 0.9 | 0.647 |
| Seaweed | times/week | 2.35 | ± | 0.67 | 2.42 | ± | 0.8 | 0.650 |
| Small fish | times/week | 1.92 | ± | 0.64 | 1.93 | ± | 0.8 | 0.687 |
| Green and yellow vegetables | times/week | 3.23 | ± | 0.73 | 3.37 | ± | 0.8 | 0.156 |
| Light-colored vegetables | times/week | 2.96 | ± | 0.80 | 3.12 | ± | 0.8 | 0.201 |
| Oligosaccharide | times/week | 1.53 | ± | 0.69 | 1.57 | ± | 0.7 | 0.818 |
| Jam and honey | times/week | 2.22 | ± | 0.90 | 2.38 | ± | 0.9 | 0.226 |
| Simmered food | times/week | 2.32 | ± | 0.64 | 2.42 | ± | 0.6 | 0.338 |
| Vinegared and dressed vegetables | times/week | 2.00 | ± | 0.72 | 2.03 | ± | 0.8 | 0.780 |
| Japanese sweets | times/week | 1.89 | ± | 0.64 | 1.80 | ± | 0.7 | 0.255 |
| Pastries and cake | times/week | 2.09 | ± | 0.69 | 1.79 | ± | 0.7 | 0.003 |
| Snack foods and fried sweets | times/week | 1.69 | ± | 0.68 | 1.51 | ± | 0.7 | 0.046 |
| Rice crackers and cookies | times/week | 2.05 | ± | 0.59 | 1.90 | ± | 0.8 | 0.062 |
| Ice cream | times/week | 1.77 | ± | 0.73 | 1.60 | ± | 0.7 | 0.111 |
| Chocolate | times/week | 2.00 | ± | 0.79 | 1.82 | ± | 0.7 | 0.152 |
| Candy and caramels | times/week | 1.55 | ± | 0.71 | 1.30 | ± | 0.5 | 0.011 |
| Jelly and pudding | times/week | 1.55 | ± | 0.64 | 1.44 | ± | 0.5 | 0.346 |
| Soft drink | times/week | 2.04 | ± | 1.05 | 1.86 | ± | 0.9 | 0.337 |
| Fried food | times/week | 2.18 | ± | 0.56 | 2.04 | ± | 0.5 | 0.100 |
| Stir-fries | times/week | 2.38 | ± | 0.61 | 2.45 | ± | 0.6 | 0.513 |
| Mayonnaise and dressing | times/week | 2.41 | ± | 0.74 | 2.39 | ± | 0.9 | 0.763 |
| Margarine and fat spread | times/week | 1.73 | ± | 0.82 | 1.54 | ± | 0.8 | 0.079 |
| Butter, lard, and beef tallow | times/week | 1.68 | ± | 0.70 | 1.65 | ± | 0.8 | 0.595 |
| Peanuts and almonds | times/week | 1.86 | ± | 0.80 | 1.98 | ± | 0.9 | 0.479 |
| Sesame | times/week | 2.00 | ± | 0.64 | 2.00 | ± | 0.7 | 0.994 |
| Olive oil and canola/rapeseed oil | times/week | 2.40 | ± | 0.75 | 2.66 | ± | 0.7 | 0.031 |
| Safflower oil, cottonseed oil, and soybean oil | times/week | 1.46 | ± | 0.76 | 1.47 | ± | 0.8 | 0.961 |
| Perilla oil, egoma oil, and flaxseed oil | times/week | 1.41 | ± | 0.66 | 1.50 | ± | 0.9 | 0.996 |
| Salty foods | times/week | 2.14 | ± | 0.73 | 1.82 | ± | 0.8 | 0.004 |
| Pickles | times/week | 2.47 | ± | 0.86 | 1.98 | ± | 0.9 | <0.001 |
| Tabletop soy sauce and sauces | times/week | 2.71 | ± | 0.77 | 2.61 | ± | 0.9 | 0.475 |
| Miso soup | times/week | 2.65 | ± | 0.90 | 2.76 | ± | 0.9 | 0.383 |
| Soup other than miso soup | times/week | 1.82 | ± | 0.58 | 1.70 | ± | 0.7 | 0.125 |
| Noodles | times/week | 2.05 | ± | 0.55 | 1.98 | ± | 0.6 | 0.383 |
| NAFLD | ||||
|---|---|---|---|---|
| OR | 95% CI | p-Value | ||
| Lower | Upper | |||
| Propensity score | 218.518 | 14.177 | 3368.249 | <0.001 |
| Fish and fish products ≥ 4 times/week | 0.261 | 0.114 | 0.594 | 0.001 |
| Pastries and cake ≥ 4 times/week | 1.801 | 0.588 | 5.515 | 0.303 |
| Candy and caramels ≥ 4 times/week | 3.097 | 0.302 | 31.704 | 0.341 |
| Pickles ≥ 4 times/week | 2.880 | 1.264 | 6.558 | 0.012 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yabe, Y.; Chihara, K.; Oshida, N.; Kamimaki, T.; Hasegawa, N.; Isobe, T.; Shoda, J. Survey of Dietary Habits and Physical Activity in Japanese Patients with Non-Obese Non-Alcoholic Fatty Liver Disease. Nutrients 2023, 15, 2764. https://doi.org/10.3390/nu15122764
Yabe Y, Chihara K, Oshida N, Kamimaki T, Hasegawa N, Isobe T, Shoda J. Survey of Dietary Habits and Physical Activity in Japanese Patients with Non-Obese Non-Alcoholic Fatty Liver Disease. Nutrients. 2023; 15(12):2764. https://doi.org/10.3390/nu15122764
Chicago/Turabian StyleYabe, Yoshito, Kanako Chihara, Natsumi Oshida, Takashi Kamimaki, Naoyuki Hasegawa, Tomonori Isobe, and Junichi Shoda. 2023. "Survey of Dietary Habits and Physical Activity in Japanese Patients with Non-Obese Non-Alcoholic Fatty Liver Disease" Nutrients 15, no. 12: 2764. https://doi.org/10.3390/nu15122764
APA StyleYabe, Y., Chihara, K., Oshida, N., Kamimaki, T., Hasegawa, N., Isobe, T., & Shoda, J. (2023). Survey of Dietary Habits and Physical Activity in Japanese Patients with Non-Obese Non-Alcoholic Fatty Liver Disease. Nutrients, 15(12), 2764. https://doi.org/10.3390/nu15122764