

Psychosocial Factors and the Need for Multidisciplinary Support in Nutrition Counselling for Cancer Chemotherapy Patients

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
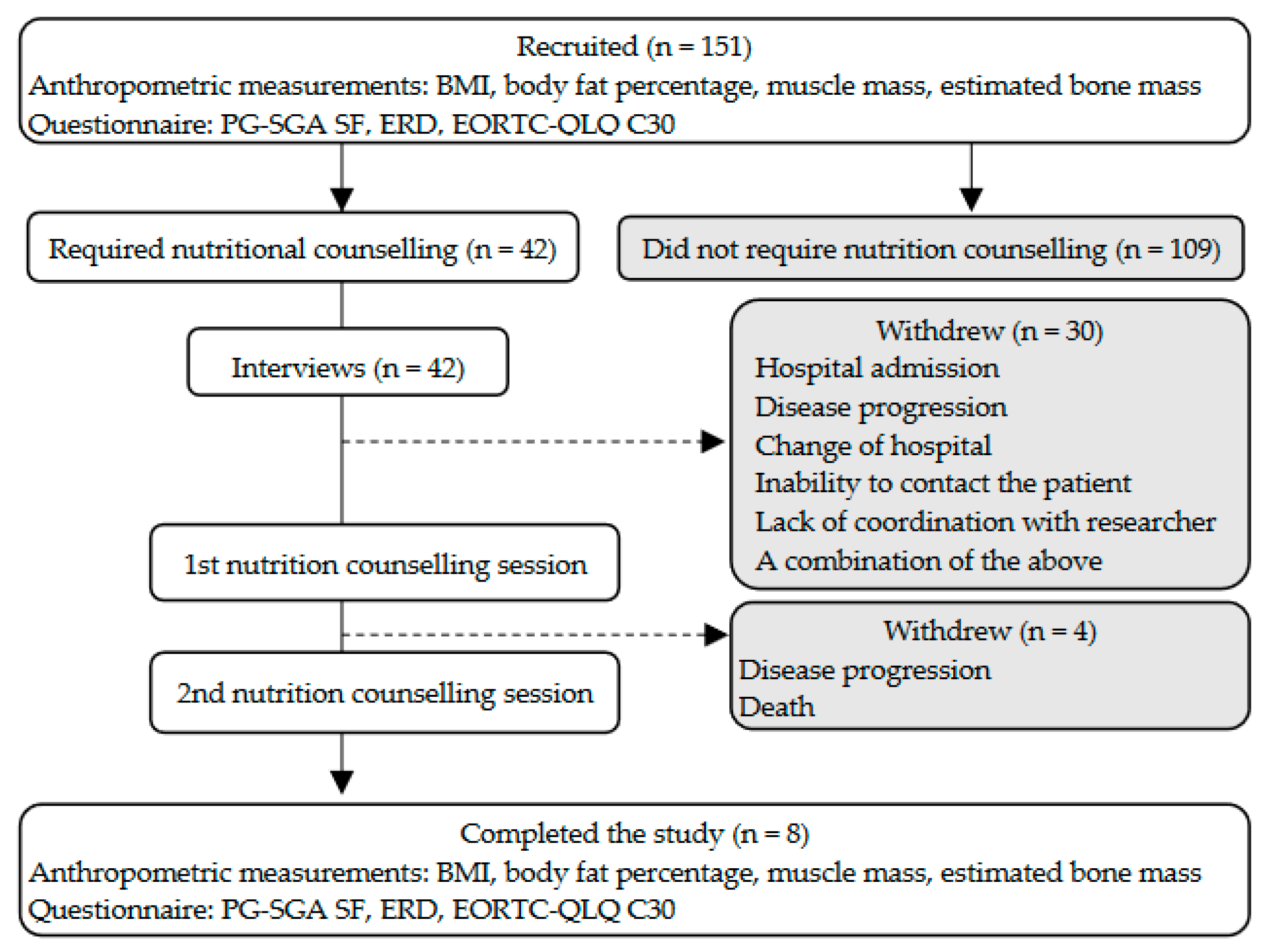
2.1. Participants
2.2. Ethical Considerations
2.3. Study Design
2.4. Questionnaires
2.5. Interviews
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Psychosocial Factors That Influenced Patients’ Requirements for Nutrition Counselling
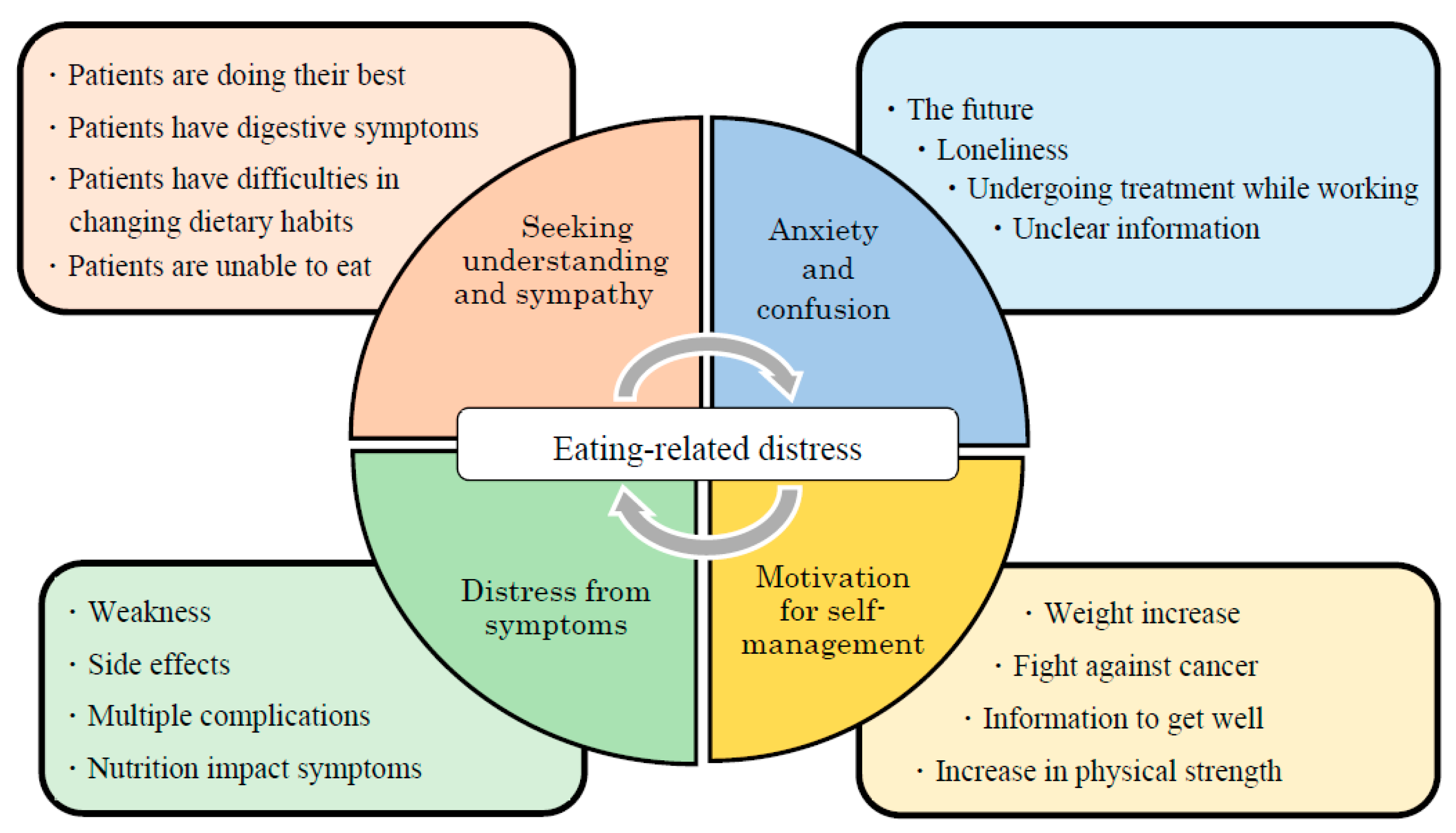
3.3. Specific Issues That Led to a Desire for Nutrition Counselling
- (1)
- Motivation for self-management: The participants regarded information about nutrition and diet positively, relating it to their treatment and physical condition.
- (2)
- Distress from symptoms: The participants struggled with nutrition and diet as they dealt with NIS, side effects of chemotherapy, and complications related to other symptoms.
- (3)
- Seeking understanding and sympathy: The participants felt that people around them needed to understand that they were trying to manage food intake levels and NIS.
- (4)
- Anxiety and confusion: The participants were confused and swayed by unclear information owing to their fear of not being able to eat.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Question Items | Likert Scale | |||
|---|---|---|---|---|
| Distress originating from the feelings of patients themselves (ERD-1) | No | Sometimes | Frequently | Always |
| I feel that lack of nutrition makes my condition worse. | 1 | 2 | 3 | 4 |
| I think that I cannot eat because of a lack of effort on my part. | 1 | 2 | 3 | 4 |
| I feel that it is the natural course of the disease that I cannot get enough nutrition and that I lose weight. | 1 | 2 | 3 | 4 |
| I am disappointed to find that I cannot eat enough. | 1 | 2 | 3 | 4 |
| I feel that I should make efforts to get enough nutrition even if I have a bad physical condition. | 1 | 2 | 3 | 4 |
| Distress originating from concerns regarding information about the patient’s diet (ERD-2) | No | Sometimes | Frequently | Always |
| I think that losing weight results from a lack of nutrition and that I can gain weight if I get enough nutrition. | 1 | 2 | 3 | 4 |
| I have eaten what I want without consideration of calories and nutritional composition. | 1 | 2 | 3 | 4 |
| I have made myself concerned about my daily diet. | 1 | 2 | 3 | 4 |
| I have tried to eat various foods. | 1 | 2 | 3 | 4 |
| I have tried to eat a high-calorie and well-balanced diet. | 1 | 2 | 3 | 4 |
| I have found it useless to consult medical staff about my daily diet. | 1 | 2 | 3 | 4 |
| I would like to consult an expert who has specific knowledge of nutrition therapy. | 1 | 2 | 3 | 4 |
| Distress originating from the relationship between patients and their families (ERD-3) | No | Sometimes | Frequently | Always |
| I am burdened by meals that are made for me with kindness. | 1 | 2 | 3 | 4 |
| I often experience conflict about meals when a person makes them for me. | 1 | 2 | 3 | 4 |
| I feel that I disregard the kindness of the person who makes meals for me when I cannot eat. | 1 | 2 | 3 | 4 |
| I try to have a good meal not for myself but for family members. | 1 | 2 | 3 | 4 |
| I avoid talking about food and eating with family members. | 1 | 2 | 3 | 4 |
| Although family members and friends recommend various foods to me, I am just confused. | 1 | 2 | 3 | 4 |
| I often feel that I am forced to eat. | 1 | 2 | 3 | 4 |
| Variable | Nutrition Counselling | p Value § | |
|---|---|---|---|
| Before | After | ||
| Mean ± SD | Mean ± SD | ||
| Age | 70.6 ± 5.9 | 70.6 ± 5.9 | - |
| Cancer Stage (median) | III | III | - |
| BMI (kg/m2) | 20.6 ± 2.1 | 20.5 ± 1.9 | 0.833 |
| Alb (g/dL) | 3.9 ± 0.4 | 3.6 ± 0.2 | 0.018 |
| CRP (mg/dL) | 0.4 ± 0.4 | 0.9 ± 1.0 | 0.063 |
| mGPS | 0.4 ± 0.5 | 0.5 ± 0.5 | 0.317 |
| PG-SGA SF Score | 7.3 ± 4.0 | 7.4 ± 4.3 | 1.000 |
| QOL (EORTC-QLQ C30) | |||
| Global Health Status | 58.3 ± 13.4 | 59.4 ± 21.5 | 0.854 |
| Physical Functioning | 82.5 ± 10.0 | 85.0 ± 7.8 | 0.461 |
| Role Functioning | 77.1 ± 21.7 | 87.5 ± 19.4 | 0.102 |
| Emotional Functioning | 85.4 ± 13.9 | 88.6 ± 11.7 | 0.581 |
| Cognitive Functioning | 91.7 ± 17.8 | 91.7 ± 17.8 | 1.000 |
| Social Functioning | 83.3 ± 21.8 | 91.7 ± 17.8 | 0.180 |
| Dyspnoea | 37.5 ± 21.4 | 29.1 ± 11.8 | 0.157 |
| Sleep Disorder | 16.7 ± 17.8 | 16.7 ± 25.2 | 0.705 |
| Poor Appetite | 29.2 ± 27.8 | 29.2 ± 27.8 | 1.000 |
| Diarrhea | 16.7 ± 35.4 | 12.5 ± 35.4 | 0.655 |
| Constipation | 20.8 ± 30.9 | 20.8 ± 24.8 | 1.000 |
| Pain | 20.8 ± 14.8 | 16.7 ± 17.8 | 0.715 |
| Fatigue | 47.2 ± 26.4 | 29.2 ± 23.0 | 0.042 |
| Nausea/Vomiting | 4.2 ± 7.7 | 2.1 ± 5.9 | 0.317 |
| Financial Problems | 12.5 ± 24.8 | 4.2 ± 11.8 | 0.180 |
| Question Items | Nutrition Counselling | ||
|---|---|---|---|
| Distress originating from the feelings of patients themselves (ERD-1) | before † | after † | p value § |
| I feel that lack of nutrition makes my condition worse. | 2.0 | 2.0 | 1.000 |
| I think that I cannot eat because of a lack of effort on my part. | 1.3 | 1.5 | 0.157 |
| I feel that it is the natural course of the disease that I cannot get enough nutrition and that I lose weight. | 1.7 | 1.7 | 1.000 |
| I am disappointed to find that I cannot eat enough. | 1.9 | 1.9 | 1.000 |
| I feel that I should make efforts to get enough nutrition even if I have a bad physical condition. | 2.4 | 2.1 | 0.680 |
| Distress originating from concerns regarding information about the patient’s diet (ERD-2) | before † | after † | p value § |
| I think that losing weight results from a lack of nutrition and that I can gain weight if I get enough nutrition. | 1.9 | 2.4 | 0.357 |
| I have eaten what I want without consideration of calories and nutritional composition. | 1.4 | 2.0 | 0.180 |
| I have made myself concerned about my daily diet. | 3.4 | 2.5 | 0.102 |
| I have tried to eat various foods. | 3.9 | 3.8 | 0.317 |
| I have tried to eat a high-calorie and well-balanced diet. | 3.4 | 3.4 | 1.000 |
| I have found it useless to consult medical staff about my daily diet. | 1.1 | 1.0 | 0.317 |
| I would like to consult an expert who has specific knowledge on nutrition therapy. | 2.9 | 2.4 | 0.336 |
| Distress originating from the relationship between patients and their families (ERD-3) | before † | after † | p value § |
| I am burdened by meals that are made for me with kindness. | 1.2 | 1.1 | 0.317 |
| I often experience conflict about meals when a person makes them for me. | 1.6 | 1.8 | 0.564 |
| I feel that I disregard the kindness of the person who makes meals for me when I cannot eat. | 1.6 | 1.6 | 1.000 |
| I try to have a good meal not for myself but for family members. | 1.5 | 1.5 | 1.000 |
| I avoid talking about food and eating with family members. | 1.1 | 1.0 | 0.317 |
| Although family members and friends recommend various foods to me, I am just confused. | 2.1 | 1.5 | 0.025 |
| I often feel that I am forced to eat. | 1.4 | 1.6 | 0.317 |
References
- Muscaritoli, M.; Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN practical guideline: Clinical Nutrition in cancer. Clin. Nutr. 2021, 40, 2898–2913. [Google Scholar] [CrossRef] [PubMed]
- Omlin, A.; Blum, D.; Wierecky, J.; Haile, S.R.; Ottery, F.D.; Strasser, F. Nutrition impact symptoms in advanced cancer patients: Frequency and specific interventions, a case-control study. J. Cachexia Sarcopenia Muscle 2013, 4, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Amano, K.; Satomi, E.; Oyamada, S.; Ishiki, H.; Sakashita, A.; Miura, T.; Maeda, I.; Hatano, Y.; Yamauchi, T.; Oya, K.; et al. The prevalence of artificially administered nutrition and hydration in different age groups among patients with advanced cancer admitted to palliative care units. Clin. Nutr. Open. Sci. 2021, 40, 69–78. [Google Scholar] [CrossRef]
- Bressan, V.; Bagnasco, A.; Aleo, G.; Catania, G.; Zanini, M.P.; Timmins, F.; Sasso, L. The life experience of nutrition impact symptoms during treatment for head and neck cancer patients: A systematic review and meta-synthesis. Support. Care Cancer 2017, 25, 1699–1712. [Google Scholar] [CrossRef]
- Kasvis, P.; Vigano, M.; Vigano, A. Health-related quality of life across cancer cachexia stages. Ann. Palliat. Med. 2018, 8, 33–42. [Google Scholar] [CrossRef]
- Baracos, V.E. Cancer-associated malnutrition. Eur. J. Clin. Nutr. 2018, 72, 1255–1259. [Google Scholar] [CrossRef]
- Amano, K.; Morita, T.; Koshimoto, S.; Uno, T.; Katayama, H.; Tatara, R. Eating-related distress in advanced cancer patients with cachexia and family members: A survey in palliative and supportive care settings. Support. Care Cancer 2019, 27, 2869–2876. [Google Scholar] [CrossRef]
- Bargetzi, L.; Brack, C.; Herrmann, J.; Bargetzi, A.; Hersberger, L.; Bargetzi, M.; Kaegi-Braun, N.; Tribolet, P.; Gomes, F.; Hoess, C.; et al. Nutritional support during the hospital stay reduces mortality in patients with different types of cancers: Secondary analysis of a prospective randomized trial. Ann. Oncol. 2021, 32, 1025–1033. [Google Scholar] [CrossRef]
- Koshimoto, S.; Arimoto, M.; Saitou, K.; Uchibori, M.; Hashizume, A.; Honda, A.; Amano, K.; Nakajima, Y.; Uetake, H.; Matsushima, E. Need and demand for nutritional counselling and their association with quality of life, nutritional status and eating-related distress among patients with cancer receiving outpatient chemotherapy: A cross-sectional study. Support. Care Cancer 2019, 27, 3385–3394. [Google Scholar] [CrossRef]
- Alderman, B.; Allan, L.; Amano, K.; Bouleuc, C.; Davis, M.; Lister-Flynn, S.; Mukhopadhyay, S.; Davies, A. Multinational Association of Supportive Care in Cancer (MASCC) expert opinion/guidance on the use of clinically assisted nutrition in patients with advanced cancer. Support. Care Cancer 2022, 30, 2983–2992. [Google Scholar] [CrossRef]
- Kok, A.; van der Lugt, C.; Leermakers-Vermeer, M.J.; de Roos, N.M.; Speksnijder, C.M.; de Bree, R. Nutritional interventions in patients with head and neck cancer undergoing chemoradiotherapy: Current practice at the Dutch Head and Neck Oncology centres. Eur. J. Cancer Care 2022, 31, e13518. [Google Scholar] [CrossRef]
- van Beek, F.E.; Jansen, F.; Mak, L.; Lissenberg-Witte, B.I.; Buter, J.; Vergeer, M.R.; Voortman, J.; Cuijpers, P.; Leemans, C.R.; Verdonck-de Leeuw, I.M. The course of symptoms of anxiety and depression from time of diagnosis up to 2 years follow-up in head and neck cancer patients treated with primary (chemo)radiation. Oral Oncol. 2020, 102, 104576. [Google Scholar] [CrossRef]
- Morse, L.; Kober, K.M.; Viele, C.; Cooper, B.A.; Paul, S.M.; Conley, Y.P.; Hammer, M.; Levine, J.D.; Miaskowski, C. Subgroups of patients undergoing chemotherapy with distinct cognitive fatigue and evening physical fatigue profiles. Support. Care Cancer 2021, 29, 7985–7998. [Google Scholar] [CrossRef] [PubMed]
- de Kruif, A.J.; Westerman, M.J.; Winkels, R.M.; Koster, M.S.; van der Staaij, I.M.; van den Berg, M.M.G.A.; de Vries, J.H.M.; de Boer, M.R.; Kampman, E.; Visser, M. Exploring changes in dietary intake, physical activity and body weight during chemotherapy in women with breast cancer: A Mixed-Methods Study. J. Hum. Nutr. Diet. 2021, 34, 550–561. [Google Scholar] [CrossRef] [PubMed]
- Ganzer, H.; Rothpletz-Puglia, P.; Byham-Gray, L.; Murphy, B.A.; Touger-Decker, R. The eating experience in long-term survivors of head and neck cancer: A mixed-methods study. Support. Care Cancer 2015, 23, 3257–3268. [Google Scholar] [CrossRef]
- Loeliger, J.; Dewar, S.; Kiss, N.; Drosdowsky, A.; Stewart, J. Patient and carer experiences of nutrition in cancer care: A mixed-methods study. Support. Care Cancer 2021, 29, 5475–5485. [Google Scholar] [CrossRef]
- Abbott, J.; Teleni, L.; McKavanagh, D.; Watson, J.; McCarthy, A.L.; Isenring, E. Patient-Generated Subjective Global Assessment Short Form (PG-SGA SF) is a valid screening tool in chemotherapy outpatients. Support. Care Cancer 2016, 24, 3883–3887. [Google Scholar] [CrossRef]
- Amano, K.; Morita, T.; Miyashita, M. Potential measurement properties of a questionnaire for eating-related distress among advanced cancer patients with cachexia: Preliminary findings of reliability and validity analysis. J. Palliat. Care 2022, 37, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Snyder, C.F.; Blackford, A.L.; Sussman, J.; Bainbridge, D.; Howell, D.; Seow, H.Y.; Carducci, M.A.; Wu, A.W. Identifying changes in scores on the EORTC-QLQ-C30 representing a change in patients’ supportive care needs. Qual. Life Res. 2015, 24, 1207–1216. [Google Scholar] [CrossRef]
- Krippendorff, K. Content Analysis: An Introduction to Its Methodology, 2nd ed.; Sage: Thousand Oaks, CA, USA, 1989. [Google Scholar]
- Arends, J. Struggling with nutrition in patients with advanced cancer: Nutrition and nourishment—Focusing on metabolism and supportive care. Ann. Oncol. 2018, 29, ii27–ii34. [Google Scholar] [CrossRef]
- Roeland, E.J.; Bohlke, K.; Baracos, V.E.; Bruera, E.; del Fabbro, E.; Dixon, S.; Fallon, M.; Herrstedt, J.; Lau, H.; Platek, M.; et al. Management of cancer cachexia: ASCO guideline. J. Clin. Oncol. 2020, 38, 2438–2453. [Google Scholar] [CrossRef]
- Hopkinson, J. Psychosocial impact of cancer cachexia. J. Cachexia Sarcopenia Muscle 2014, 5, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Lize, N.; IJmker-Hemink, V.; van Lieshout, R.; Wijnholds-Roeters, Y.; van den Berg, M.; Soud, M.Y.-E.; Beijer, S.; Raijmakers, N. Experiences of patients with cancer with information and support for psychosocial consequences of reduced ability to eat: A qualitative interview study. Support. Care Cancer 2021, 29, 6343–6352. [Google Scholar] [CrossRef] [PubMed]
- Brenne, E.; Loge, J.H.; Kaasa, S.; Heitzer, E.; Knudsen, A.K.; Wasteson, E. Depressed patients with incurable cancer: Which depressive symptoms do they experience? Palliat. Support. Care 2013, 11, 491–501. [Google Scholar] [CrossRef]
- Çıracı, Y.; Nural, N.; Saltürk, Z. Loneliness of oncology patients at the end of life. Support. Care Cancer 2016, 24, 3525–3531. [Google Scholar] [CrossRef] [PubMed]
- Warner, E.L.; Basen-Engquist, K.M.; Badger, T.A.; Crane, T.E.; Raber-Ramsey, M. The Online Cancer Nutrition Misinformation: A framework of behavior change based on exposure to cancer nutrition misinformation. Cancer 2022, 128, 2540–2548. [Google Scholar] [CrossRef]
- Padilla, G.V. Psychological aspects of nutrition and cancer. Nutr. Cancer II 1986, 66, 1121–1135. [Google Scholar] [CrossRef]
- McQuestion, M.; Fitch, M.; Howell, D. The changed meaning of food: Physical, social and emotional loss for patients having received radiation treatment for head and neck cancer. Eur. J. Oncol. Nurs. 2011, 15, 145–151. [Google Scholar] [CrossRef]
- Wallin, V.; Carlander, I.; Sandman, P.-O.; Håkanson, C. Meanings of eating deficiencies for people admitted to palliative home care. Palliat. Support. Care 2015, 13, 1231–1239. [Google Scholar] [CrossRef]
- del Fabbro, E. Combination therapy in cachexia. Ann. Palliat. Med. 2019, 8, 59–66. [Google Scholar] [CrossRef]
- Hopkinson, J. Psychosocial support in cancer cachexia syndrome: The evidence for supported self-management of eating problems during radiotherapy or chemotherapy treatment. Asia Pac. J. Oncol. Nurs. 2018, 5, 358–368. [Google Scholar] [CrossRef] [PubMed]
- Hopkinson, J.B.; Kazmi, C.; Elias, J.; Wheelwright, S.; Williams, R.; Russell, A.; Shaw, C. Diet and weight management by people with nonmetastatic colorectal cancer during chemotherapy: Mixed methods research. Color. Cancer 2020, 9, CRC16. [Google Scholar] [CrossRef]
- Maddocks, M.; Hopkinson, J.; Conibear, J.; Reeves, A.; Shaw, C.; Fearon, K.C.H. Practical multimodal care for cancer cachexia. Curr. Opin. Support. Palliat. Care 2016, 10, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Koshimoto, S.; Yamazaki, T.; Amano, K.; Kako, J.; Arimoto, M.; Saitou, K.; Hashizume, A.; Takeuchi, T.; Matsushima, E. Psychosocial support and nutrition counselling among patients with cancer receiving chemotherapy: A mixed-methods study. Resh Sq. 2021, preprint. [Google Scholar] [CrossRef]


| Variable | Required Nutrition Counselling (n = 42) | Did Not Require Nutrition Counselling (n = 109) |
|---|---|---|
| age (years) * | 65.5 ± 9.1 | 66.9 ± 8.8 |
| female n (%) | 11 (26.2) | 41 (37.6) |
| male n (%) | 31 (73.8) | 68 (62.4) |
| PS (median) | 2 | 2 |
| cancer site n (%) | ||
| head and neck | 2 (4.8) | 13 (11.9) |
| oesophageal | 5 (11.9) | 7 (6.4) |
| gastric | 4 (9.5) | 18 (16.5) |
| colorectal | 17 (40.5) | 32 (29.4) |
| lung | 14 (33.3) | 39 (35.8) |
| disease stage (median) | III | III |
| BMI kg/(cm)2 * | 21.1 ± 3.6 | 21.8 ± 4.1 |
| serum albumin g/dL * | 3.8 ± 0.4 | 3.5 ± 1.0 |
| C-reactive protein mg/dl * | 0.8 ± 1.2 | 0.7 ± 1.3 |
| mGPS (median) | 2 | 2 |
| symptoms n (%) | ||
| anorexia | 19 (45.2) | 43 (39.4) |
| weight loss of 2% or more | 9 (21.4) | 13 (11.9) |
| constipation | 16 (38.1) | 27 (24.8) |
| diarrhea | 7 (16.7) | 23 (21.1) |
| thirst | 9 (24.4) | 21 (19.3) |
| dysgeusia | 20 (47.6) | 40 (36.7) |
| olfactory disorder | 11 (26.2) | 15 (13.8) |
| vomiting | 10 (23.8) | 21 (19.3) |
| dysphagia | 8 (19.0) | 21 (19.3) |
| early satiety | 9 (21.4) | 29 (26.6) |
| fatigue | 22 (52.4) | 51 (46.8) |
| pain | 15 (35.7) | 21 (19.3) |
| PG-SGA SF * | 8.6 ± 5.0 | 7.1 ± 5.1 |
| QOL score (EORTC-QLQ C30) * | ||
| global health status | 52.8 ± 16.0 | 60.2 ± 18.8 |
| physical functioning | 75.4 ± 22.7 | 79.0 ± 18.1 |
| role functioning | 76.6 ± 24.7 | 77.5 ± 28.0 |
| emotional functioning | 80.2 ± 18.1 | 87.1 ± 15.7 |
| cognitive functioning | 82.5 ± 19.6 | 90.6 ± 15.0 |
| social functioning | 72.4 ± 26.0 | 82.1 ± 22.7 |
| Independent Variables | Required Nutrition Counselling (n = 42) | Did Not Require Nutrition Counselling (n = 109) | p-Value | ||
|---|---|---|---|---|---|
| Number of people in the household (one or two) n (%) | 33 (80.5) | 62 (57.4) | 0.009 | ||
| Employment status (working) n (%) | 18 (42.9) | 34 (31.8) | 0.203 | ||
| Global health status on QOL * (mean ± SD) | 52.8 ± 16.0 | 60.3 ± 18.8 | 0.028 | ||
| ERD-2 † (mean ± SD) | 2.4 ± 0.6 | 2.1 ± 0.5 | 0.002 | ||
| Independent variables | Partial regression coefficient | Odds ratio | 95% confidence interval | p-value | |
| min. | max. | ||||
| Number of people in the household | 1.39 | 4.00 | 1.33 | 12.02 | 0.014 * |
| Employment status | −1.14 | 0.32 | 0.13 | 0.80 | 0.015 * |
| Global health status on QOL * | −0.03 | 0.97 | 0.95 | 1.00 | 0.023 * |
| Distress from ERD treatment † | 0.93 | 2.52 | 1.06 | 6.00 | 0.036 * |
| Category | Sub-Categories (n) | Codes (n) |
|---|---|---|
| Motivation for self-management | Information regarding nutritional balance (11) | I want to know about the absorption of fats and nutrients, and meal combinations. (2) |
| I want advice about specific foods. (3) | ||
| I want to know more about nutrients. (1) | ||
| I want to know more about quality/quantity and nutrition. (2) | ||
| I want informational materials about the classification of nutrients. (1) | ||
| What meals have a high nutrient content and provide a good nutritional balance? (1) | ||
| Are my portion sizes large enough? (1) | ||
| Information on how to adjust diet to improve physical condition (6) | Which foods are easy to digest? (2) | |
| Which foods increase physical strength? (1) | ||
| How can I increase my weight? No matter what I do, my weight does not seem to increase. (1) | ||
| What can I eat and is easy for me to eat? (1) | ||
| I have heard that massaging the salivary gland is good. Please teach me how to do it. (1) | ||
| Information regarding foods beneficial for treatment (7) | What foods can I eat despite having cancer? (2) | |
| What foods should I not eat owing to cancer? (1) | ||
| Which foods are effective against cancer? (2) | ||
| How can I adjust my foods, nutrition, and meals according to my type of cancer? (1) | ||
| Which foods can help with the treatment without supplements? (1) | ||
| Distress from symptoms | Distress from nutrition impact symptoms and side effects (12) | I do not know about suitable menus during chemotherapy. (1) |
| I do not know how to manage medication with food (ingredients). (1) | ||
| Which cooking methods are suitable for my symptoms? (1) | ||
| How can I deal with the smell of certain foods? (1) | ||
| It is difficult to improve my anaemia. (1) | ||
| I worry that chemotherapy will harm the function of my kidneys and liver. What should I eat to prevent this? (1) | ||
| How can I supplement my nutrition when I cannot eat owing to mouth ulcers? (1) | ||
| How can I deal with taste disorders? (1) | ||
| It is difficult to control constipation. (1) | ||
| What can I eat when my condition worsens owing to side effects? (1) | ||
| It is difficult to control medication timings when I cannot eat owing to side effects. (2) | ||
| Difficulty in handling multiple complications (6) | It is difficult to coordinate diabetes and cancer treatments. (4) | |
| I have both hypertension and diabetes; therefore, I am confused over which treatment to prioritize. (1) | ||
| What can I eat when I have intestinal obstruction? (1) | ||
| Seeking understanding and sympathy | Eagerness for others to understand their inability to eat (10) | I am doing my best but cannot eat because my throat hurts. (1) |
| I want you to know that it is difficult to prepare meals because of severe numbness. (1) | ||
| You may not realize it, but I cannot eat because of my mouth ulcers. (1) | ||
| I know I must eat, but it is difficult owing to perleche and taste disorder. (1) | ||
| I want to eat, but when I do, the food gets stuck in my throat, and I cannot eat enough. (1) | ||
| I had nutrition counselling in the past, but I could not do all the things I was advised. (1) | ||
| I understand that I should eat what I can when I want to eat, but I cannot eat. (2) | ||
| Desire for others to understand their symptoms (3) | I am worried about having diarrhea at work. (2) | |
| I want my spouse to understand the changes in my sense of taste and provide foods that are easy to eat. (1) | ||
| Anxiety and confusion | Anxiety about being unable to eat in the future (8) | What should I do if I cannot eat? (4) |
| What will happen in the future? (2) | ||
| I would like advice regarding losing weight if the need arises. (2) | ||
| The burden of changing dietary habit (5) | I always eat the same things. (1) | |
| I have no appetite, but I can drink alcoholic beverages. (1) | ||
| It is difficult to find foods I can and should eat. (1) | ||
| I am struggling with my dislike of vegetables. (1) | ||
| I am struggling with being a picky eater. (1) | ||
| Swayed by unclear information about foods (6) | Can I eat meat, eel, or purified rice? I heard these foods are bad. (1) | |
| Are carrots, juice made from green leafy vegetables, and hydrogen water effective? Is there any scientific basis for this? (1) | ||
| I cannot eat vegetables, but is it okay to drink juice made from green leafy vegetables? (1) | ||
| I read a cookbook by Dr. A of a certain university, which said that I should prepare meals with brown rice, vegetables, and fish. However, I lost weight when I followed that advice. (1) | ||
| I heard that unpolished rice is good against cancer, but I lost weight when I followed this advice. (1) | ||
| Does a low-carbohydrate diet inhibit the growth of cancer cells? (1) | ||
| Fixated on dietary rules (5) | I am worried about getting an infection when I take off my mask to eat. (1) | |
| I was told to avoid raw foods in post-operative counselling, and so I have avoided them for years. (1) | ||
| I was told to avoid brown rice and seaweed in post-operative counselling, and so I have avoided them for years. (1) | ||
| I use steroids to improve my appetite; can I take them with milk to protect my stomach? (1) | ||
| I suck on candy to reduce the side effects, but my family says that I have no appetite because of this. Does candy suppress one’s appetite? (1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koshimoto, S.; Yamazaki, T.; Amano, K.; Kako, J.; Arimoto, M.; Saitou, K.; Hashizume, A.; Takeuchi, T.; Matsushima, E. Psychosocial Factors and the Need for Multidisciplinary Support in Nutrition Counselling for Cancer Chemotherapy Patients. Nutrients 2023, 15, 2712. https://doi.org/10.3390/nu15122712
Koshimoto S, Yamazaki T, Amano K, Kako J, Arimoto M, Saitou K, Hashizume A, Takeuchi T, Matsushima E. Psychosocial Factors and the Need for Multidisciplinary Support in Nutrition Counselling for Cancer Chemotherapy Patients. Nutrients. 2023; 15(12):2712. https://doi.org/10.3390/nu15122712
Chicago/Turabian StyleKoshimoto, Saori, Tomoko Yamazaki, Koji Amano, Jun Kako, Masako Arimoto, Keiko Saitou, Akiko Hashizume, Takashi Takeuchi, and Eisuke Matsushima. 2023. "Psychosocial Factors and the Need for Multidisciplinary Support in Nutrition Counselling for Cancer Chemotherapy Patients" Nutrients 15, no. 12: 2712. https://doi.org/10.3390/nu15122712
APA StyleKoshimoto, S., Yamazaki, T., Amano, K., Kako, J., Arimoto, M., Saitou, K., Hashizume, A., Takeuchi, T., & Matsushima, E. (2023). Psychosocial Factors and the Need for Multidisciplinary Support in Nutrition Counselling for Cancer Chemotherapy Patients. Nutrients, 15(12), 2712. https://doi.org/10.3390/nu15122712