
Efficacy of Different Dietary Patterns in the Treatment of Functional Gastrointestinal Disorders in Children and Adolescents: A Systematic Review of Intervention Studies

Abstract
1. Introduction
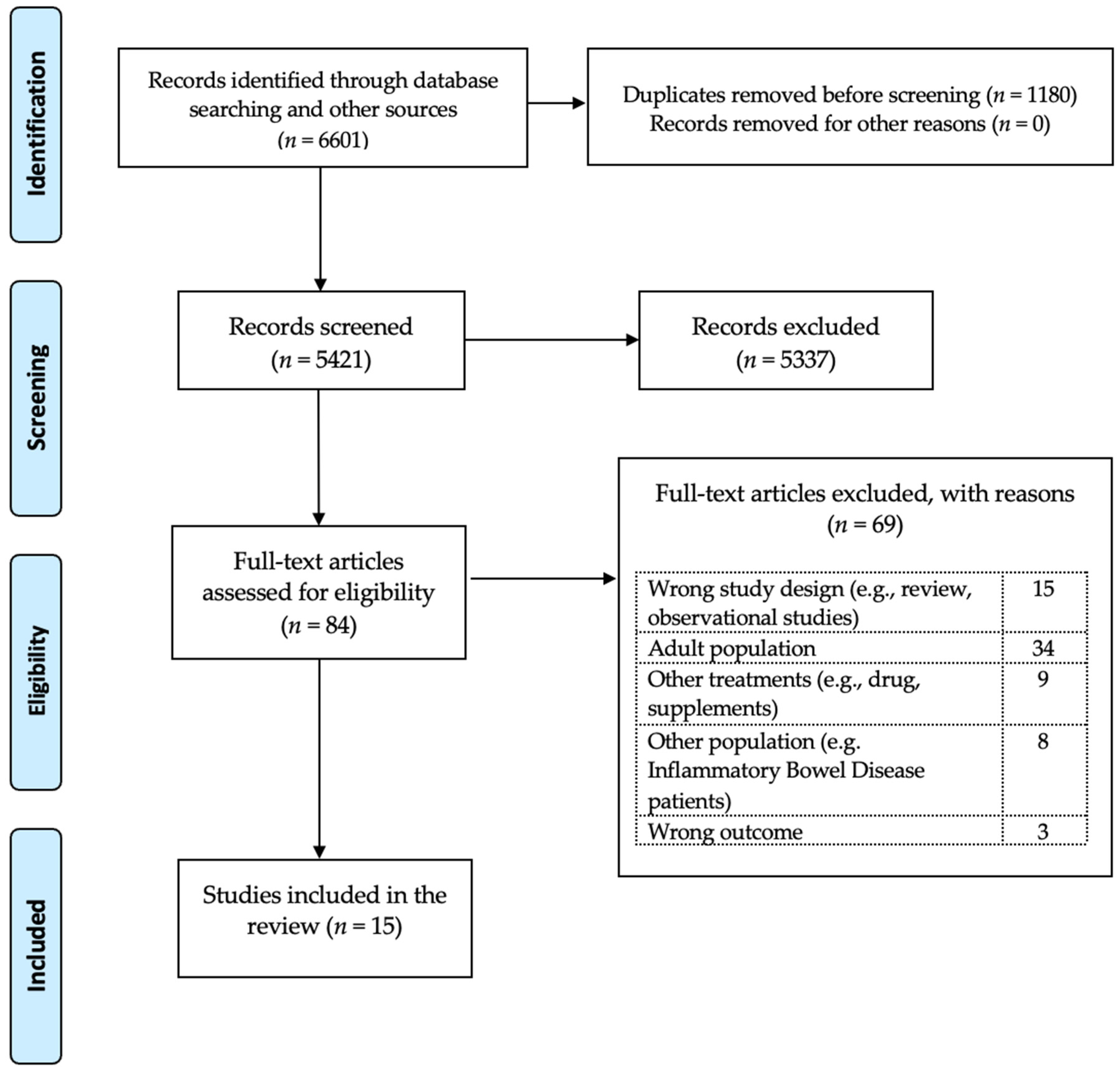
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Data Extraction
2.3. Outcome Measured
2.4. Study Quality
3. Results
3.1. Low-FODMAP Diet
3.2. Fructose-Restricted Diet
3.3. Gluten-Free Diet
3.4. Mediterranean Diet
4. Discussion
4.1. Summary of the Primary and Secondary Outcomes
4.2. Literature Documention
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Lewis, M.L.; Palsson, O.S.; Whitehead, W.E.; van Tilburg, M.A. Prevalence of functional gastrointestinal disorders in children and adolescents. J. Pediatr. 2016, 177, 39–43.e3. [Google Scholar] [CrossRef] [PubMed]
- Baaleman, D.F.; Di Lorenzo, C.; Benninga, M.A.; Saps, M. The Effects of the Rome IV Criteria on Pediatric Gastrointestinal Practice. Curr. Gastroenterol. Rep. 2020, 22, 21. [Google Scholar] [CrossRef] [PubMed]
- Robin, S.G.; Keller, C.; Zwiener, R.; Hyman, P.E.; Nurko, S.; Saps, M.; Di Lorenzo, C.; Shulman, R.J.; Hyams, J.S.; Palsson, O. Prevalence of pediatric functional gastrointestinal disorders utilizing the Rome IV criteria. J. Pediatr. 2018, 195, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Hyams, J.S.; Di Lorenzo, C.; Saps, M.; Shulman, R.J.; Staiano, A.; van Tilburg, M. Childhood functional gastrointestinal disorders: Child/adolescent. Gastroenterology 2016, 150, 1456–1468.e1452. [Google Scholar] [CrossRef] [PubMed]
- Hyman, P.E.; Milla, P.J.; Benninga, M.A.; Davidson, G.P.; Fleisher, D.F.; Taminiau, J. Childhood functional gastrointestinal disorders: Neonate/toddler. Gastroenterology 2006, 130, 1519–1526. [Google Scholar] [CrossRef]
- Rasquin, A.; Di Lorenzo, C.; Forbes, D.; Guiraldes, E.; Hyams, J.S.; Staiano, A.; Walker, L.S. Childhood functional gastrointestinal disorders: Child/adolescent. Gastroenterology 2006, 130, 1527–1537. [Google Scholar] [CrossRef]
- Vernon-Roberts, A.; Alexander, I.; Day, A.S. Systematic Review of Pediatric Functional Gastrointestinal Disorders (Rome IV Criteria). J. Clin. Med. 2021, 10, 5087. [Google Scholar] [CrossRef]
- Boronat, A.C.; Ferreira-Maia, A.P.; Matijasevich, A.; Wang, Y.-P. Epidemiology of functional gastrointestinal disorders in children and adolescents: A systematic review. World J. Gastroenterol. 2017, 23, 3915. [Google Scholar] [CrossRef]
- Strisciuglio, C.; Cenni, S.; Serra, M.R.; Dolce, P.; Kolacek, S.; Sila, S.; Trivic, I.; Bar Lev, M.R.; Shamir, R.; Kostovski, A.; et al. Diet and Pediatric Functional Gastrointestinal Disorders in Mediterranean Countries. Nutrients 2022, 14, 2335. [Google Scholar] [CrossRef]
- Drossman, D.A. Functional Gastrointestinal Disorders: History, Pathophysiology, Clinical Features, and Rome IV. Gastroenterology 2016, 150, 1262–1279.e1262. [Google Scholar] [CrossRef]
- Camilleri, M.; Carlson, P.; McKinzie, S.; Zucchelli, M.; D’Amato, M.; Busciglio, I.; Burton, D.; Zinsmeister, A.R. Genetic susceptibility to inflammation and colonic transit in lower functional gastrointestinal disorders: Preliminary analysis. Neurogastroenterol. Motil. 2011, 23, 935-e398. [Google Scholar] [CrossRef] [PubMed]
- Mayer, E.A.; Ryu, H.J.; Bhatt, R.R. The neurobiology of irritable bowel syndrome. Mol. Psychiatry 2023, 28, 1451–1465. [Google Scholar] [CrossRef] [PubMed]
- Azpiroz, F.; Bouin, M.; Camilleri, M.; Mayer, E.A.; Poitras, P.; Serra, J.; Spiller, R.C. Mechanisms of hypersensitivity in IBS and functional disorders. Neurogastroenterol. Motil. 2007, 19, 62–88. [Google Scholar] [CrossRef]
- Burns, G.L.; Hoedt, E.C.; Walker, M.M.; Talley, N.J.; Keely, S. Physiological mechanisms of unexplained (functional) gastrointestinal disorders. J. Physiol. 2021, 599, 5141–5161. [Google Scholar] [CrossRef] [PubMed]
- De Palma, G.; Collins, S.M.; Bercik, P. The microbiota-gut-brain axis in functional gastrointestinal disorders. Gut Microbes 2014, 5, 419–429. [Google Scholar] [CrossRef]
- Koloski, N.; Holtmann, G.; Talley, N.J. Is there a causal link between psychological disorders and functional gastrointestinal disorders? Expert Rev. Gastroenterol. Hepatol. 2020, 14, 1047–1059. [Google Scholar] [CrossRef]
- Defrees, D.N.; Bailey, J. Irritable bowel syndrome: Epidemiology, pathophysiology, diagnosis, and treatment. Prim. Care Clin. Off. Pract. 2017, 44, 655–671. [Google Scholar] [CrossRef]
- Velasco-Benítez, C.A.; Gómez-Oliveros, L.F.; Rubio-Molina, L.M.; Tovar-Cuevas, J.R.; Saps, M. Diagnostic Accuracy of the Rome IV Criteria for the Diagnosis of Functional Gastrointestinal Disorders in Children. J. Pediatr. Gastroenterol. Nutr. 2021, 72, 538–541. [Google Scholar] [CrossRef]
- Horvath, A.; Dziechciarz, P.; Szajewska, H. Systematic review of randomized controlled trials: Fiber supplements for abdominal pain-related functional gastrointestinal disorders in childhood. Ann. Nutr. Metab. 2012, 61, 95–101. [Google Scholar] [CrossRef]
- Capozza, M.; Laforgia, N.; Rizzo, V.; Salvatore, S.; Guandalini, S.; Baldassarre, M. Probiotics and Functional Gastrointestinal Disorders in Pediatric Age: A Narrative Review. Front. Pediatr. 2022, 10, 805466. [Google Scholar] [CrossRef]
- Korte, C.; Friedberg, R.D. Cognitive behavioral therapy for comorbid pediatric functional gastrointestinal disorders and anxiety: Systematic review and clinical applications. J. Clin. Exp. Gastroenterol. 2023, 2, 19–26. [Google Scholar]
- Palermo, T.M. Pain prevention and management must begin in childhood: The key role of psychological interventions. Pain 2020, 161, S114. [Google Scholar] [CrossRef]
- Pinn, D.; Aroniadis, O.; Brandt, L. Is fecal microbiota transplantation (FMT) an effective treatment for patients with functional gastrointestinal disorders (FGID)? Neurogastroenterol. Motil. 2015, 27, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Bonilla, S.; Nurko, S. Focus on the use of antidepressants to treat pediatric functional abdominal pain: Current perspectives. Clin. Exp. Gastroenterol. 2018, 11, 365–372. [Google Scholar] [CrossRef]
- Korterink, J.J.; Rutten, J.M.; Venmans, L.; Benninga, M.A.; Tabbers, M.M. Pharmacologic treatment in pediatric functional abdominal pain disorders: A systematic review. J. Pediatr. 2015, 166, 424–431.e426. [Google Scholar] [CrossRef]
- Singh, R.; Zogg, H.; Ghoshal, U.C.; Ro, S. Current Treatment Options and Therapeutic Insights for Gastrointestinal Dysmotility and Functional Gastrointestinal Disorders. Front. Pharmacol. 2022, 13, 808195. [Google Scholar] [CrossRef] [PubMed]
- Tuck, C.J.; Reed, D.E.; Muir, J.G.; Vanner, S.J. Implementation of the low FODMAP diet in functional gastrointestinal symptoms: A real-world experience. Neurogastroenterol. Motil. 2020, 32, e13730. [Google Scholar] [CrossRef]
- Wirth, S.; Klodt, C.; Wintermeyer, P.; Berrang, J.; Hensel, K.; Langer, T.; Heusch, A. Positive or negative fructose breath test results do not predict response to fructose restricted diet in children with recurrent abdominal pain: Results from a prospective randomized trial. Klin. Pädiatrie 2014, 226, 268–273. [Google Scholar] [CrossRef]
- Rej, A.; Avery, A.; Aziz, I.; Black, C.J.; Bowyer, R.K.; Buckle, R.L.; Seamark, L.; Shaw, C.C.; Thompson, J.; Trott, N.; et al. Diet and irritable bowel syndrome: An update from a UK consensus meeting. BMC Med. 2022, 20, 287. [Google Scholar] [CrossRef]
- Cenni, S.; Sesenna, V.; Boiardi, G.; Casertano, M.; Di Nardo, G.; Esposito, S.; Strisciuglio, C. The Mediterranean Diet in Paediatric Gastrointestinal Disorders. Nutrients 2023, 15, 79. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, W-65–W-94. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Hernán, M.A.; McAleenan, A.; Reeves, B.C.; Higgins, J.P. Chapter 25: Assessing risk of bias in a non-randomized study. Cochrane Handbook for Systematic Reviews of Intervention. Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; version 6.3; Cochrane. 2022. Available online: www.training.cochrane.org/handbook (accessed on 4 May 2023).
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Higgins, J.P.; Li, T.; Sterne, J. Revised Cochrane risk of bias tool for randomized trials (RoB 2): Additional considerations for crossover trials. Cochrane Methods 2021, 1–6. [Google Scholar]
- Chumpitazi, B.P.; Cope, J.L.; Hollister, E.B.; Tsai, C.M.; McMeans, A.R.; Luna, R.A.; Versalovic, J.; Shulman, R.J. Randomised clinical trial: Gut microbiome biomarkers are associated with clinical response to a low FODMAP diet in children with the irritable bowel syndrome. Aliment. Pharmacol. Ther. 2015, 42, 418–427. [Google Scholar] [CrossRef] [PubMed]
- Chumpitazi, B.P.; Hollister, E.B.; Oezguen, N.; Tsai, C.M.; McMeans, A.R.; Luna, R.A.; Savidge, T.C.; Versalovic, J.; Shulman, R.J. Gut microbiota influences low fermentable substrate diet efficacy in children with irritable bowel syndrome. Gut Microbes 2014, 5, 165–175. [Google Scholar] [CrossRef]
- Dogan, G.; Yavuz, S.; Aslantas, H.; Ozyurt, B.; Kasirga, E. Is low FODMAP diet effective in children with irritable bowel syndrome? North. Clin. Istanb. 2020, 7, 433–437. [Google Scholar] [PubMed]
- Baranguan Castro, M.L.; Ros Arnal, I.; Garcia Romero, R.; Rodriguez Martinez, G.; Ubalde Sainz, E. Implementation of a low FODMAP diet for functional abdominal pain. An. Pediatr. 2019, 90, 180–186. [Google Scholar] [CrossRef]
- Boradyn, K.M.; Przybyłowicz, K.E.; Jarocka-Cyrta, E. Low FODMAP diet is not effective in children with functional abdominal pain: A randomized controlled trial. Ann. Nutr. Metab. 2020, 76, 334–344. [Google Scholar] [CrossRef]
- Cyrkot, S.; Marcon, M.; Brill, H.; Mileski, H.; Dowhaniuk, J.; Frankish, A.; Carroll, M.W.; Persad, R.; Turner, J.M.; Mager, D.R. FODMAP intake in children with coeliac disease influences diet quality and health-related quality of life and has no impact on gastrointestinal symptoms. Int. J. Food Sci. Nutr. 2021, 72, 956–967. [Google Scholar] [CrossRef]
- Nogay, N.H.; Walton, J.; Roberts, K.M.; Nahikian-Nelms, M.; Witwer, A.N. The effect of the low FODMAP diet on gastrointestinal symptoms, behavioral problems and nutrient intake in children with autism spectrum disorder: A randomized controlled pilot trial. J. Autism Dev. Disord. 2021, 51, 2800–2811. [Google Scholar] [CrossRef]
- Wintermeyer, P.; Baur, M.; Pilic, D.; Schmidt-Choudhury, A.; Zilbauer, M.; Wirth, S. Fructose malabsorption in children with recurrent abdominal pain: Positive effects of dietary treatment. Klin. Padiatr. 2012, 224, 17–21. [Google Scholar] [CrossRef]
- Escobar Jr, M.A.; Lustig, D.; Pflugeisen, B.M.; Amoroso, P.J.; Sherif, D.; Saeed, R.; Shamdeen, S.; Tuider, J.; Abdullah, B. Fructose intolerance/malabsorption and recurrent abdominal pain in children. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 498–501. [Google Scholar] [CrossRef]
- Gijsbers, C.F.; Kneepkens, C.M.; Buller, H.A. Lactose and fructose malabsorption in children with recurrent abdominal pain: Results of double-blinded testing. Acta. Paediatr. 2012, 101, e411–e415. [Google Scholar] [CrossRef]
- Gremse, D.A.; Greer, A.S.; Vacik, J.; Dipalma, J.A. Abdominal Pain Associated with Lactose Ingestion in Children with Lactose Intolerance. Clin. Pediatr. 2003, 42, 341–345. [Google Scholar] [CrossRef]
- Francavilla, R.; Cristofori, F.; Verzillo, L.; Gentile, A.; Castellaneta, S.; Polloni, C.; Giorgio, V.; Verduci, E.; D’angelo, E.; Dellatte, S. Randomized double-blind placebo-controlled crossover trial for the diagnosis of non-celiac gluten sensitivity in children. Off. J. Am. Coll. Gastroenterol.|ACG 2018, 113, 421–430. [Google Scholar] [CrossRef] [PubMed]
- Piwowarczyk, A.; Horvath, A.; Pisula, E.; Kawa, R.; Szajewska, H. Gluten-free diet in children with autism spectrum disorders: A randomized, controlled, single-blinded trial. J. Autism Dev. Disord. 2020, 50, 482–490. [Google Scholar] [CrossRef] [PubMed]
- Ghalichi, F.; Ghaemmaghami, J.; Malek, A.; Ostadrahimi, A. Effect of gluten free diet on gastrointestinal and behavioral indices for children with autism spectrum disorders: A randomized clinical trial. World J. Pediatr. 2016, 12, 436–442. [Google Scholar] [CrossRef]
- Al-Biltagi, M.; El Amrousy, D.; El Ashry, H.; Maher, S.; Mohammed, M.A.; Hasan, S. Effects of adherence to the Mediterranean diet in children and adolescents with irritable bowel syndrome. World J. Clin. Pediatr. 2022, 11, 330–340. [Google Scholar] [CrossRef] [PubMed]
- Black, C.J.; Staudacher, H.M.; Ford, A.C. Efficacy of a low FODMAP diet in irritable bowel syndrome: Systematic review and network meta-analysis. Gut 2022, 71, 1117–1126. [Google Scholar] [CrossRef]
- Ford, A.C.; Moayyedi, P.; Lacy, B.E.; Lembo, A.J.; Saito, Y.A.; Schiller, L.R.; Soffer, E.E.; Spiegel, B.M.; Quigley, E.M. American College of Gastroenterology monograph on the management of irritable bowel syndrome and chronic idiopathic constipation. Off. J. Am. Coll. Gastroenterol.|ACG 2014, 109, S2–S26. [Google Scholar] [CrossRef] [PubMed]
- Moayyedi, P.; Marsiglio, M.; Andrews, C.N.; Graff, L.A.; Korownyk, C.; Kvern, B.; Lazarescu, A.; Liu, L.; MacQueen, G.; Paterson, W.G. Patient Engagement and Multidisciplinary Involvement has an Impact on Clinical Guideline Development and Decisions: A Comparison of Two Irritable Bowel Syndrome Guidelines Using the Same Data; Oxford University Press US: New York, NY, USA, 2019; Volume 2, pp. 30–36. [Google Scholar]
- Mullin, G.E.; Shepherd, S.J.; Chander Roland, B.; Ireton-Jones, C.; Matarese, L.E. Irritable bowel syndrome: Contemporary nutrition management strategies. J. Parenter. Enter. Nutr. 2014, 38, 781–799. [Google Scholar] [CrossRef]
- Halmos, E.P.; Power, V.A.; Shepherd, S.J.; Gibson, P.R.; Muir, J.G. A diet low in FODMAPs reduces symptoms of irritable bowel syndrome. Gastroenterology 2014, 146, 67–75.e65. [Google Scholar] [CrossRef] [PubMed]
- van Lanen, A.-S.; de Bree, A.; Greyling, A. Efficacy of a low-FODMAP diet in adult irritable bowel syndrome: A systematic review and meta-analysis. Eur. J. Nutr. 2021, 60, 3505–3522. [Google Scholar] [CrossRef] [PubMed]
- Thomassen, R.; Luque, V.; Assa, A.; Borrelli, O.; Broekaert, I.; Dolinsek, J.; Martin-de-Carpi, J.; Mas, E.; Miele, E.; Norsa, L. An ESPGHAN Position Paper on the Use of Low-FODMAP Diet in Pediatric Gastroenterology. J. Pediatr. Gastroenterol. Nutr. 2022, 75, 356–368. [Google Scholar] [CrossRef] [PubMed]
- Rezaie, A.; Buresi, M.; Lembo, A.; Lin, H.; McCallum, R.; Rao, S.; Schmulson, M.; Valdovinos, M.; Zakko, S.; Pimentel, M. Hydrogen and methane-based breath testing in gastrointestinal disorders: The North American Consensus. Am. J. Gastroenterol. 2017, 112, 775. [Google Scholar] [CrossRef] [PubMed]
- Storhaug, C.L.; Fosse, S.K.; Fadnes, L.T. Country, regional, and global estimates for lactose malabsorption in adults: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2017, 2, 738–746. [Google Scholar] [CrossRef]
- Misselwitz, B.; Butter, M.; Verbeke, K.; Fox, M.R. Update on lactose malabsorption and intolerance: Pathogenesis, diagnosis and clinical management. Gut 2019, 68, 2080–2091. [Google Scholar] [CrossRef] [PubMed]
- Kwiecień, J.; Hajzler, W.; Kosek, K.; Balcerowicz, S.; Grzanka, D.; Gościniak, W.; Górowska-Kowolik, K. No Correlation between Positive Fructose Hydrogen Breath Test and Clinical Symptoms in Children with Functional Gastrointestinal Disorders: A Retrospective Single-Centre Study. Nutrients 2021, 13, 2891. [Google Scholar] [CrossRef] [PubMed]
- Gibson, P.R.; Newnham, E.; Barrett, J.S.; Shepherd, S.J.; Muir, J.G. Review article: Fructose malabsorption and the bigger picture. Aliment Pharmacol. Ther. 2007, 25, 349–363. [Google Scholar] [CrossRef]
- Lozinsky, A.C.; Boé, C.; Palmero, R.; Fagundes-Neto, U. Fructose malabsorption in children with functional digestive disorders. Arq Gastroenterol. 2013, 50, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Pawłowska, K.; Umławska, W.; Iwańczak, B. Prevalence of Lactose Malabsorption and Lactose Intolerance in Pediatric Patients with Selected Gastrointestinal Diseases. Adv. Clin. Exp. Med. 2015, 24, 863–871. [Google Scholar] [CrossRef] [PubMed]
- Pensabene, L.; Salvatore, S.; Turco, R.; Tarsitano, F.; Concolino, D.; Baldassarre, M.E.; Borrelli, O.; Thapar, N.; Vandenplas, Y.; Staiano, A. Low FODMAPs diet for functional abdominal pain disorders in children: Critical review of current knowledge. J. Pediatr. 2019, 95, 642–656. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Comparisons against baseline within randomised groups are often used and can be highly misleading. Trials 2011, 12, 264. [Google Scholar] [CrossRef]
- Volta, U.; Pinto-Sanchez, M.I.; Boschetti, E.; Caio, G.; De Giorgio, R.; Verdu, E.F. Dietary Triggers in Irritable Bowel Syndrome: Is There a Role for Gluten? J. Neurogastroenterol. Motil. 2016, 22, 547–557. [Google Scholar] [CrossRef]
- Koumbi, L.; Giouleme, O.; Vassilopoulou, E. Non-Celiac Gluten Sensitivity and Irritable Bowel Disease: Looking for the Culprits. Curr. Dev. Nutr. 2020, 4, nzaa176. [Google Scholar] [CrossRef]
- Biesiekierski, J.R.; Newnham, E.D.; Irving, P.M.; Barrett, J.S.; Haines, M.; Doecke, J.D.; Shepherd, S.J.; Muir, J.G.; Gibson, P.R. Gluten causes gastrointestinal symptoms in subjects without celiac disease: A double-blind randomized placebo-controlled trial. Off. J. Am. Coll. Gastroenterol.|ACG 2011, 106, 508–514. [Google Scholar] [CrossRef]
- Carroccio, A.; Mansueto, P.; Iacono, G.; Soresi, M.; D’alcamo, A.; Cavataio, F.; Brusca, I.; Florena, A.M.; Ambrosiano, G.; Seidita, A. Non-celiac wheat sensitivity diagnosed by double-blind placebo-controlled challenge: Exploring a new clinical entity. Off. J. Am. Coll. Gastroenterol.|ACG 2012, 107, 1898–1906. [Google Scholar] [CrossRef]
- de Bruijn, C.M.; Rexwinkel, R.; Gordon, M.; Sinopoulou, V.; Benninga, M.A.; Tabbers, M.M. Dietary interventions for functional abdominal pain disorders in children: A systematic review and meta-analysis. Expert Rev. Gastroenterol. Hepatol. 2022, 16, 359–371. [Google Scholar] [CrossRef] [PubMed]
- Barbaro, M.R.; Cremon, C.; Wrona, D.; Fuschi, D.; Marasco, G.; Stanghellini, V.; Barbara, G. Non-Celiac Gluten Sensitivity in the Context of Functional Gastrointestinal Disorders. Nutrients 2020, 12, 3725. [Google Scholar] [CrossRef]
- Devulapalli, C.S. Gluten-free diet in children: A fad or necessity? Arch. Dis. Child. 2021, 106, 628–629. [Google Scholar] [CrossRef]
- Devulapalli, C.S. Non-coeliac gluten sensitivity in children. Tidsskr Nor Laegeforen 2020, 140. [Google Scholar] [CrossRef]
- Catassi, C.; Elli, L.; Bonaz, B.; Bouma, G.; Carroccio, A.; Castillejo, G.; Cellier, C.; Cristofori, F.; de Magistris, L.; Dolinsek, J.; et al. Diagnosis of Non-Celiac Gluten Sensitivity (NCGS): The Salerno Experts’ Criteria. Nutrients 2015, 7, 4966–4977. [Google Scholar] [CrossRef]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61, 1402S–1406S. [Google Scholar] [CrossRef]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Morze, J.; Hoffmann, G. Mediterranean diet and health status: Active ingredients and pharmacological mechanisms. Br. J. Pharmacol. 2020, 177, 1241–1257. [Google Scholar] [CrossRef]
- Zito, F.P.; Polese, B.; Vozzella, L.; Gala, A.; Genovese, D.; Verlezza, V.; Medugno, F.; Santini, A.; Barrea, L.; Cargiolli, M. Good adherence to mediterranean diet can prevent gastrointestinal symptoms: A survey from Southern Italy. World J. Gastrointest. Pharmacol. Ther. 2016, 7, 564. [Google Scholar] [CrossRef]
- Elmaliklis, I.-N.; Liveri, A.; Ntelis, B.; Paraskeva, K.; Goulis, I.; Koutelidakis, A.E. Increased functional foods’ consumption and Mediterranean diet adherence may have a protective effect in the appearance of gastrointestinal diseases: A case–control study. Medicines 2019, 6, 50. [Google Scholar] [CrossRef] [PubMed]
- Stróżyk, A.; Horvath, A.; Szajewska, H. FODMAP dietary restrictions in the management of children with functional abdominal pain disorders: A systematic review. Neurogastroenterol. Motil. 2022, 34, e14345. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.C.; Whelan, K.; Gearry, R.B.; Day, A.S. Low FODMAP diet in children and adolescents with functional bowel disorder: A clinical case note review. JGH Open 2020, 4, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Turco, R.; Salvatore, S.; Miele, E.; Romano, C.; Marseglia, G.L.; Staiano, A. Does a low FODMAPs diet reduce symptoms of functional abdominal pain disorders? A systematic review in adult and paediatric population, on behalf of Italian Society of Pediatrics. Ital. J. Pediatr. 2018, 44, 53. [Google Scholar] [CrossRef]
- Axelrod, C.H.; Saps, M. The Role of Fiber in the Treatment of Functional Gastrointestinal Disorders in Children. Nutrients 2018, 10, 1650. [Google Scholar] [CrossRef]
- Pärtty, A.; Rautava, S.; Kalliomäki, M. Probiotics on Pediatric Functional Gastrointestinal Disorders. Nutrients 2018, 10, 1836. [Google Scholar] [CrossRef] [PubMed]
- Korterink, J.J.; Ockeloen, L.; Benninga, M.A.; Tabbers, M.M.; Hilbink, M.; Deckers-Kocken, J.M. Probiotics for childhood functional gastrointestinal disorders: A systematic review and meta-analysis. Acta Paediatr. 2014, 103, 365–372. [Google Scholar] [CrossRef]
- Hojsak, I.; Kolaček, S.; Mihatsch, W.; Mosca, A.; Shamir, R.; Szajewska, H.; Vandenplas, Y.; van den Akker, C.H.; Berni Canani, R.; Dinleyici, E.C. Synbiotics in the Management of Pediatric Gastrointestinal Disorders: Position Paper of the ESPGHAN Special Interest Group on Gut Microbiota and Modifications. J. Pediatr. Gastroenterol. Nutr. 2023, 76, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Scarpato, E.; Auricchio, R.; Penagini, F.; Campanozzi, A.; Zuccotti, G.V.; Troncone, R. Efficacy of the gluten free diet in the management of functional gastrointestinal disorders: A systematic review on behalf of the Italian Society of Paediatrics. Ital. J. Pediatr. 2019, 45, 9. [Google Scholar] [CrossRef]
- Axelrod, C.H.; Saps, M. Global Dietary Patterns and Functional Gastrointestinal Disorders. Children 2020, 7, 152. [Google Scholar] [CrossRef]
- Tabbers, M.; DiLorenzo, C.; Berger, M.; Faure, C.; Langendam, M.; Nurko, S.; Staiano, A.; Vandenplas, Y.; Benninga, M. Evaluation and treatment of functional constipation in infants and children: Evidence-based recommendations from ESPGHAN and NASPGHAN. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 258–274. [Google Scholar] [CrossRef]
- Alfaro Cruz, L.; Minard, C.; Guffey, D.; Chumpitazi, B.P.; Shulman, R.J. Does a Minority of Children with Functional Gastrointestinal Disorders Receive Formal Diet Advice? J. Parenter. Enter. Nutr. 2020, 44, 1525–1529. [Google Scholar] [CrossRef]
- López-Gil, J.F.; García-Hermoso, A.; Sotos-Prieto, M.; Cavero-Redondo, I.; Martínez-Vizcaíno, V.; Kales, S.N. Mediterranean diet-based interventions to improve anthropometric and obesity indicators in children and adolescents: A systematic review with meta-analysis of randomized controlled trials. Adv. Nutr. 2023. [Google Scholar] [CrossRef] [PubMed]
- Bouhanick, B.; Sosner, P.; Brochard, K.; Mounier-Véhier, C.; Plu-Bureau, G.; Hascoet, S.; Ranchin, B.; Pietrement, C.; Martinerie, L.; Boivin, J.M.; et al. Hypertension in Children and Adolescents: A Position Statement From a Panel of Multidisciplinary Experts Coordinated by the French Society of Hypertension. Front. Pediatr. 2021, 9, 680803. [Google Scholar] [CrossRef] [PubMed]
- Mearin, M.L.; Agardh, D.; Antunes, H.; Al-Toma, A.; Auricchio, R.; Castillejo, G.; Catassi, C.; Ciacci, C.; Discepolo, V.; Dolinsek, J.; et al. ESPGHAN Position Paper on Management and Follow-up of Children and Adolescents With Celiac Disease. J. Pediatr. Gastroenterol. Nutr. 2022, 75, 369–386. [Google Scholar] [CrossRef]
- Llanos-Chea, A.; Fasano, A. Gluten and Functional Abdominal Pain Disorders in Children. Nutrients 2018, 10, 1491. [Google Scholar] [CrossRef]
- Biesiekierski, J.R.; Peters, S.L.; Newnham, E.D.; Rosella, O.; Muir, J.G.; Gibson, P.R. No Effects of Gluten in Patients with Self-Reported Non-Celiac Gluten Sensitivity After Dietary Reduction of Fermentable, Poorly Absorbed, Short-Chain Carbohydrates. Gastroenterology 2013, 145, 320–328.e323. [Google Scholar] [CrossRef]
- Agakidis, C.; Kotzakioulafi, E.; Petridis, D.; Apostolidou, K.; Karagiozoglou-Lampoudi, T. Mediterranean Diet Adherence is Associated with Lower Prevalence of Functional Gastrointestinal Disorders in Children and Adolescents. Nutrients 2019, 11, 1283. [Google Scholar] [CrossRef]
- Howatson, A.; Wall, C.; Turner-Benny, P. The contribution of dietitians to the primary health care workforce. J. Prim. Health Care 2015, 7, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Alfaro-Cruz, L.; Heitkemper, M.; Chumpitazi, B.P.; Shulman, R.J. Literature review: Dietary intervention adherence and adherence barriers in functional gastrointestinal disorder studies. J. Clin. Gastroenterol. 2020, 54, 203–211. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author- Journal- Year of Publication | Type of Study | Sample | Diagnosis | Study Groups | Intervention | Duration | Follow-Up | Age | Outcomes | Tools Used | Study Results | Adherence to the Intervention |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Chumpitazi, B.P. et al. Alimentary pharmacology & therapeutics 2015 [36] | double-blind, crossover RCT-5 days washout period between intervention diets | 33 | IBS (Rome III criteria) | low-FODMAP diet group (n = 16) or TACD (n = 17) | The low FODMAP diet contained 0.15 g/kg/day (maximum 9 g/day) of FODMAPs. The TACD contained 0.7 g/kg / day (maximum 50 g/day) of FODMAPs. | 48 h | 7–17 years | Pain episodes (i.e., abdominal pain location, severity and duration), associated daily GI symptoms, microbiome composition/metabolic capacity, gas production (hydrogen & methane) | 7-day pain and stool diary before intervention and for the 2 days in each group, 0–10 Likert scale for GI symptoms, modified Bristol stool form chart for stool characterization. Adherence was based on food records and weight-ins. | Less abdominal pain episodes/day in the FODMAP diet vs. TACD [1.1 ± 0.2 vs. 1.7 ± 0.4, p < 0.05] and compared to baseline (1.4 ± 0.2) (p < 0.01) but more episodes during the TACD (p < 0.01). | 90% | |
| Chumpitazi, B.P. et al. Gut microbes 2014 [37] | open-label pilot study | 12 (n = 8 completed the study) | IBS (Rome III criteria) | low FODMAP diet group (no control gorup) | Instructions to decrease high FODMAP foods, sample menus and a table detailing foods to avoid and foods allowed, option to contact dietitian | 1 week | 7–16 years | Abdominal pain severity & frequency, Stooling characteristics and transit time, gas production (hydrogen & methane), microbial communities and associated metabolites | 7-day pain and stool diary, 3-day food record, stool for microbiome composition, validated 0–10 scale for measuring abdominal pain (0 = “no pain at all” and 10 = "worst pain you can imagine") | Pain frequency (p < 0.05), pain severity (p < 0.05), and pain-related interference with activities (p < 0.05) decreased in the subjects while on the low-FODMAP diet. Responders vs. non-responders: four children (50%) were identified as responders (>50% decrease in abdominal pain frequency while on the low-FODMAP diet). There were no differences between responders and non-responders with respect to hydrogen production, methane production, stooling characteristics, or gut transit time. | High adherence defined as increased consumption of low-FODMAP foods | |
| Dogan, G. et al. Northern clinics of Istanbul 2020 [38] | RCT | 60 | IBS (Rome IV criteria) | low-FODMAP diet group (n = 30) or protective GI diet group (n = 30) | FODMAP intake was less than 0.5 g per meal. A healthy diet list was given to the control group. | 2 months | 2 months | 6-18 years | Abdominal pain severity, abdominal distention, defecation habits, clinical status (i.e., abdominal pain, boalting and general well-being status of the patient) at the end of the study and after 2-month of follow-up (no intervention given) | 10cm Visual Analogue Scale (VAS) for abdominal pain, Clinical Global Impression Improvement scale (CGI-I) for the assessement of clinical status by doctors. No specific tool was reported with regards to adherence to the diets. | Post intervention: Decrease in VAS score in low-FODMAP group vs. control group (3.80 ± 1.10 vs. 2.03 ± 1.03, p = 0.0001) and in CGI-I (p = 0.0001). At follow-up: increase in VAS score in low-FODMAP group vs. control group (2.97 ± 1.10 1.63 ± 0.71, p = 0.0001), but desease in CGI-I score (p = 0.0007). | 100% adherence in 2 months |
| Baranguan Castro, M.L. et al. An Pediatr (Engl Ed) 2019 [39] | open-label prospective study | 22 (n = 20 completed the study) | various FAPDs; FAP, IBS, or FD (Rome III criteria) | low FODMAP diet group (no control gorup) | A table of ‘‘allowed’’ or ‘‘not allowed’’ foods based on their FODMAP content was given. | 2 weeks | 5–15 years | Abdominal pain (number and severity per/w) Interference with daily activities, stools characteristics, associated symptoms, such as abdominal distension, gas, vomiting, nausea and other | 10-cm Visual Analogue Scale (VAS) for abdominal pain intensity, 4-point Likert scale for the assessment of interference with daily activities, Bristol stool scale modified for children, 5-point Liker scale for assessing the degree of the adherence to the diet. | Less number of abdominal pain episodes per day compared to baseline [1.16, (0.41–3.33) vs.2, (1.33–6.33), p = 0.024], lower 10-cm VAS compared to baseline [1.41 (0.32–5.23) vs. 4.63 (2.51–6.39), p = 0.035], less interference with daily activities, fewer associated symptoms like abdominal distension or gas, no differences in stool charasteristics | 13/20 substancial adherence, 6 good adherence,1 fair adherence | |
| Boradyn, K.M. et al. Annals of Nutrition and Metabolism 2020 [40] | double-blind RCT | 29 (27 completed the study) | FAP (Rome III criteria) | low-FODMAP diet (n = 13) vs. NICE (n = 14) | Pre-cooked meals prepared based on the food grading system proposed by the Monash University in the Low FODMAP Diet AppTM. | 4 weeks | 5–12 years | Abdominal pain (frequency & intensity), Stool consistency | Wong-Baker FACES Pain Rating Scale for pain severity. Daily leftovers and times of noncompliance were assessed for evaluating adherence to diets. | No between groups significant changes in the abdominal pain intensity and frequency as well as in stool frequency and consistency. No significant changes within low-FODMAP group but significant reduction in abdominal pain intensity and frequency (p < 0.01) and improvement in stool consistency (93% reporting normal stool, p < 0.05) in the NICE group. | Higher noncompliance to the diet was observed during the second week in the low FODMAP group compared to NICE group. No significant differences were seen in the average percentage amount of daily leftovers in any week between groups. | |
| Nogay, N.H. et al. Journal of Autism and Developmental Disorders 2021 [42] | pilot single-site, RCT | 15 | ASD with constipation and/or abdominal pain (Rome IV criteria) | low FODMAP diet (n = 7) or control group (habitual diet, n = 8). | Detailed nutrition education by the investigator (Dietitian) concerning the low FODMAP diet | 2 weeks | 6–17 years | GI module total score, GI symptoms total score. Stool frequency and consistency. Behavioral problems | Dietary food record (3 days before start to study and the last 3 days of the study), stool consistency/frequency record (3 days before start to study and the last 3 days of the study). Aberrant Behavior Checklist-Community and Pediatric Quality of Life Inventory Gastrointestinal Module | Reduced rates of constipation, GI module and symptoms scores (p < 0.01) (i.e., reduced stomach pain and hurt, gas and bloating, stomach discomfort when eating, nausea and vomiting, and diarrhea) in the low-FODMAP group compared to the control group. No statistical significance in the stool frequency and consistency both in the low FODMAP diet and control groups compared to baseline. | NR |
| Author- Journal- Year of Publication | Type of Study | Diagnosis | Study Groups and Sample | Intervention | Duration | Age | Outcomes | Tools Used | Evaluation | Study Results | Adherence to the Intervention |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Fructose Intolerance/Malabsorption | |||||||||||
| Wirth, S. et al. Klin Padiatr 2014 [28] | 2 site-prospective, blinded RCT | Children with RAP for >3 months with positive F-HBT | n = 116 total sample/n = 103 completed the study. FRD (n = 51) or regular diet (RD) (n = 52) | FRD: detailed dietary counselling for fructose restriction plus 10 recipes for warm meals. Regular diet: instructions no to alter their diet | 2 weeks (plus 2 additional weeks for children with positive F-HBT within FRD group). | 3–18 years (3.4 to 16.4 years, n = 103) | abdominal pain intensity, changes of pain frequency, secondary symptom score (SSS) (range 0–24) 8 parameters evaluated: nausea, vomiting, fatigue, sleep disturbance, headache, dizziness, anorexia and use of pain relievers (Scores 0 to 3). | 10-point Likert scale (0 = no pain, 10 = very strong pain) for pain intesity, 3-poin scale (0 = never, 3 = frequent) for SSS, pain frequency was recorded through questainnaire. Adherence to the diets was assessed through questionnaire at the 2-week follow up. | F-HBT with 1 g fructose/kg body weight and a maximum of 25 g in a 10% solution after 8h fasting. | Abdominal pain intensity: reduced in FRD (p < 0.001) but not in RD (p > 0.5). Within FRD, children with both positive and negative F-HBTs reduced abdominal pain. Abdominal pain frequency: both groups reduced pain frequency (74% vs. 57%). SSS results: FRD: SSS reduced from 6 to 3.5, p < 0.002, RD: no statistical change. Within FRD, children with negative F-HBTs reduced SSS (p < 0.004). | No data reported although adherence was assessed by the authors. |
| Wintermeyer, P. et al. Klin Padiatr 2012 [43] | single arm clinical trial | Children with RAP for the previous 3 months with positive F-HBT | n = 75 in FRD / no control group | FRD:detailed dietary advice with a list of allowed and not allowed foods were given / option to call dietitian in case of questions. | 4 weeks | 3–14 years | Frequency and intensity of abdominal pain, stool frequency per day, nausea, problems to fall asleep, missed school days per week, and use of pain relievers | A questionnaire asking participants for clinical symptoms, e.g. frequency of pain, pain intensity, GI symptoms and adherence to the diet was used. Pain intensity was assessed through a 10-point Likert scale questionnaire (0 = no pain, 10 = very strong pain) | F-HBT with 1 g fructose/ kg body weight with a maximum of 25 g in a 10% solution after an 8–12 h fasting period | At the end of the study, pain frequency/w (1 vs.4, p < 0.001) and the intensity of pain (3 vs.6, p < 0.001) reduced compared to baseline. Daily stool frequency, nausea, problems to fall asleep, missed school days also improved significantly (all p < 0.05). | 80% of patients declared adherence to fructose restricted diet for more than 3 weeks and 88% for more than 2 weeks. |
| Escobar, J. et al. Gastroenterology 2014 [44] | single arm clinical trial | Children with chronic abdominal pain | 121 of 222 patients (54.5%) with positive F-HBT were placed on FRD | 1-hour individual consultation with a dietitian, a list of allowed and not allowed foods and a sample menu | 2 months | 2−19 years | Resolution of GI symptoms | A standard pain scale. Adherence to the diet was assessed through patient report. | F-HBT with 1 g/kg fructose to a maximum of 25 g after 12 h of fasting | At the end of the study, 93/121 patients (76.9%) reported resolution of GI with FRD (p < 0.0001). Moreover, 55/101 patients (54.4%) with negative F-BHT reported resolution of symptoms without a FRD (p = 0.37). | All patients with positive F-HBT reported near universal adherence to the dietary restrictions. |
| Fructose or Lactose Intolerance/Malabsorption | |||||||||||
| Gijsbers, R. et al. Acta Paediatrica 2012 [45] | randomized double-blind placebo-controlled trial | Children with RAP and positive F-HBT or L-HBT | LM/LI patients => initial screen phase: n = 210 with 57 positive L-HBT, elimination phase: n = 38/57 with 24 positive L-HBT. Open provocation phase: n = 23/24 with n = 7 positive L-HBT. DBPC phase: n = 6/7 with n = 6 negative L-HBT. FM/FI patients => initial screen phase: n = 121 with 79 positive F-HBTs, elimination phase: n = 49/79 with n = 32 positive F-HBTs, provocation phase: n = 31/32 with n = 13 positive F-HBTs, DBPC phase: n = 8/13 with n = 8 negative F-HBTs. | DBPC: containers with 25 g lactose or fructose and 2 with glucose in amounts that resulted in the same sweetness, numbered 1 through 4 in a randomized way. | 6 months | 4.1–16.0 years [mean age 8.8] | Resolution of GI symptoms | Not defined | F-HBTs and L-HBTs of 2 g/kg, with a maximum of 50 g in a 16.7% (50 g/300 mL) solution | After the DBPC phase, all patients with positive F-HBTs or positive-HBTs tested negative. No causal relationship between DBPC and FAP was proven by researchers. | NR |
| Lactose Intolerance/malabsoprtion | |||||||||||
| Gremse, D.A. et al. Clin Pediatrics, 2003 [46] | double-blind, crossover RCT | Children with IBS and positive L-HBT | Interventiong group: 240 mL of lactose-hydrolyzed milk or lactose-containing milk along with LRD (n = 33 in a crossover design) | Intervention group: Lactose-free milk prepared with 2.0 g of lactase per 1.9 L milk. Control group: lactose-containing milk +aspartame 1.5 g per 1.9 L of milk. | 2 weeks | 3–17 years | pain severity, total GI symptoms score | Food diaries were used to assess adherence to the LFD, pain diaries collected weekly, pain severity assesed by with a 4- likert scale (0, no symptoms; to 4, severe symptoms), total symptom score for each patient. | L-HBTs of 1 g/kg (up to 50 g) was given in a 10% solution after overning fasting | At the end of the study, abdominal pain severity decreased in the intervention compared to the control group (4.1 ± 1.4 vs. 7.5 ± 2.7, p = 0.021). Within the control group, 23/30 reported more symptoms. However, 7/30 reported less or no symptoms, although compliant with the diet. | Fully adherence to the LFD. |
| Author- Journal- Year of Publication | Type of Study | Diagnosis | Phases and Sample | Intervention | Duration | Age | Outcomes | Tools Used | Study Results | Adherence to the Intervention |
|---|---|---|---|---|---|---|---|---|---|---|
| Piwowarczyk, A. et al. Journal of Autism and Developmental Disorders 2020 [48] | Single arm- blind RCT | Children with autism spectrum disorders (ASD) plus FAP and FC (Rome III criteria) | (a) 8-week run in period, (b) 6-month GFD (n = 28 of which 27 had FGIDs) or GD (n = 30 of which 29 had FGIDs) | GFD: no consumption of gluten, GD: at least one normal meal containing gluten per day | 6 months | 36–69 months | autistic symptoms, maladaptive behaviors, intellectual abilities and GI symptoms | ADOS-2 for autism symptoms, SCQ &ASRS for diagnosis of ASD, VABS-2 for child’s adaptive capabilities, Leiter International Performance Scale for participants’ cognitive abilities, Rome III, adherence to the diets was assessed through food records. | No significant results in autistic symptoms, maladaptive behaviors, intellectual abilities or GI symptoms after the intervention between GFD and CG groups (all p > 0.05). | 91% in the GFD and 85% in GD at 12-week follow-up. |
| Francavilla, R. et al. Am J Gastroenterol 2018 [47] | Double-blind, placebo controlled crossover CT-1 week washout period | Children with a positive history of FGIDs (i.e., chronic abdominal pain, diarrhea, bloating, dyspeptic symptoms) with or without extra-intestinal manifestations (Rome III criteria) | (a) 2-week run-in period (n = 36), (b) 2-week open GFD (n = 31) (c) 2-week double-blind placebo-controlled crossover gluten challenge (n = 28) | Gluten (10 g/daily) and placebo (rice starch) given as placebo or gluten sachets (one per day) | 2 weeks for each phase | 11.4 ± 4.3 (GFD responsive) | pain severity, prevalence of NCGS, clinical and/or laboratory parameters at baseline, NCGS clinical profile | Global VAS, IBS-SS, STAIC, adherence was evaluated through interviews and was calculated by the percentage of returned and ingested sachets. | Eleven children (39.2%; 95% CI: 23.6–53.6%) tested positive for NCGS. No significant differences were observed in global VAS and IBS-SS as well as in clinical and biochemical characteristics of children when comparing challenges with gluten to placebo (all p > 0.05). | Not exact percentage was reported but the minimun accepted adherence was >80% with no drop outs. |
| Ghalichi, F. et al. World J of Pediatrics 2016 [49] | RCT | Children with autism spectrum disorders (ASD) plus part of them with FGIDs (stomachache, bloating, constipation, diarrhea) (Rome III criteria) | n = 38 in GFD (55.3% with FGIDs) and n = 38 in RD (52.6% with FGIDs) | GFD: no consumption of gluten, RD: regular diet | 6 weeks | 7.92 ± 3.37 (total sample) | GI symptoms, behavioral indices | Rome III, ADI-R, GARS-2 | GFD: GI symptoms decreased (40.57% vs. 17.10%, p < 0.05) and behavioral tests improved (80.03 ± 14.07 vs. 75.82 ± 15.37, p < 0.05). RD: no statistical changes observed in GI symptoms or behavioral test. No between groups comparisons provided. | NR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katsagoni, C.N.; Karagianni, V.-M.; Papadopoulou, A. Efficacy of Different Dietary Patterns in the Treatment of Functional Gastrointestinal Disorders in Children and Adolescents: A Systematic Review of Intervention Studies. Nutrients 2023, 15, 2708. https://doi.org/10.3390/nu15122708
Katsagoni CN, Karagianni V-M, Papadopoulou A. Efficacy of Different Dietary Patterns in the Treatment of Functional Gastrointestinal Disorders in Children and Adolescents: A Systematic Review of Intervention Studies. Nutrients. 2023; 15(12):2708. https://doi.org/10.3390/nu15122708
Chicago/Turabian StyleKatsagoni, Christina N., Vasiliki-Maria Karagianni, and Alexandra Papadopoulou. 2023. "Efficacy of Different Dietary Patterns in the Treatment of Functional Gastrointestinal Disorders in Children and Adolescents: A Systematic Review of Intervention Studies" Nutrients 15, no. 12: 2708. https://doi.org/10.3390/nu15122708
APA StyleKatsagoni, C. N., Karagianni, V.-M., & Papadopoulou, A. (2023). Efficacy of Different Dietary Patterns in the Treatment of Functional Gastrointestinal Disorders in Children and Adolescents: A Systematic Review of Intervention Studies. Nutrients, 15(12), 2708. https://doi.org/10.3390/nu15122708