Abstract
Background: Patients with plaque psoriasis have an increased risk of metabolic syndrome. However, no studies have assessed the nutritional status or screening methods of this population. Aims: This review aimed to identify and summarise metabolic syndrome screening criteria and the tools/methods used in nutrition assessment in patients with plaque psoriasis. Data synthesis: PubMed, Web of Science, Ovid and Scopus were searched from inception to March 2023, following the Arkensey and O’Malley framework, to identify articles that report nutritional assessment methods/tools and metabolic screening criteria. Twenty-one studies were identified. Overall, these studies used four different screening criteria to define metabolic syndrome. Patients with psoriasis had a high prevalence of metabolic syndrome and had a poor nutritional status compared to controls. However, only anthropometric measures such as weight, height and waist circumference were employed to determine the nutritional status. Only two studies assessed the vitamin D status. Conclusions: Patients with psoriasis have a poor nutritional status, and they are at risk of nutrient deficiencies. However, these health aspects are not routinely assessed and may increase the risk of malnutrition among these patients. Therefore, additional assessments, such as body composition and dietary assessment, are needed to determine the nutritional status to provide a suitable intervention.
1. Introduction
Plaque psoriasis or psoriasis vulgaris is a chronic inflammatory autoimmune skin disease affecting 60 million people worldwide [1,2]. It is characterised by erythematous scaly patches covering large amounts of the skin, mainly on the extensor surfaces, such as the elbows and knees, as well as the scalp, trunk and gluteal fold [3]. Disease severity using the Psoriasis Area and Severity Index (PASI) score is widely used in research, but not routinely, to assess skin involvement, location, thickness, scaling and redness [4]. The pathogenesis of psoriasis involves genetic predisposition, a dysregulated immune response, inflammatory pathways and environmental factors such as obesity and nutrition [5,6,7]. Patients with psoriasis have an increased risk of developing cardiovascular diseases, type 2 diabetes, metabolic syndrome (MetS), obesity, autoimmune thyroid disease, gout, mental health diseases, gastrointestinal diseases, chronic kidney diseases and even malignancy [8], leading to an economic burden, poor quality of life and reduced productivity [9,10].
MetS is the most common comorbidity in patients with psoriasis, with a prevalence rate of 20–50% [11]. In a clinical setting, physicians often use one of these screening criteria distributors to diagnose MetS: the World Health Organization (WHO) [12], the National Cholesterol Education Program-Adult Treatment Panel III (NCEP-ATP III) [13] and the European Group for the Study of Insulin Resistance (EGIR) [14,15]. The main clinical feature of MetS is insulin resistance but measuring circulating insulin is not routine in clinical practice. The common surrogate measures for insulin resistance and its complications are waist circumference for abdominal adiposity, triglycerides (TG) and high-density lipoprotein (HDL) cholesterol levels for dyslipidaemia, fasting blood glucose for diabetes mellitus and blood pressure for hypertension [16]. The mechanism linking psoriasis and MetS is still unclear. Th1 and Th17 T-cell-mediated inflammation are associated with the expression of pro-inflammatory cytokines, such as IL-6 and TNF-alpha, which enter the systemic circulation, inducing metabolic disorders such as insulin resistance and endothelial dysfunction, thus increasing the risk of diabetes and cardiovascular diseases [17,18]. Meanwhile, abdominal adiposity in patients with psoriasis induces inflammation by mediating pro-inflammatory cytokines and adipokines such as leptin and resistin, contributing to the development of insulin resistance, dyslipidaemia and vascular dysfunction [19] (Figure 1).
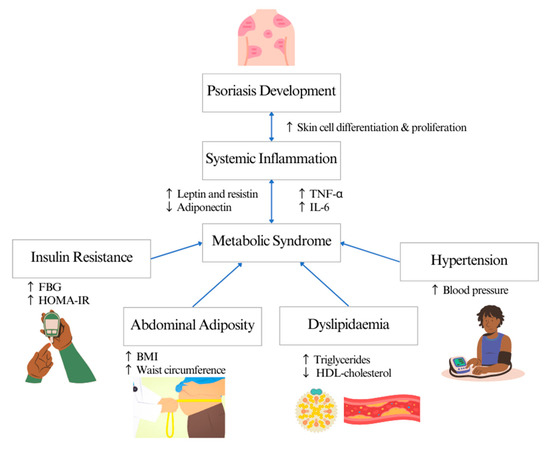
Figure 1.
Systematic inflammation linking psoriasis and metabolic syndrome.
All these measured parameters form part of the nutritional assessment, which is routinely performed in clinical practice by dietitians to identify nutritional problems or risks to optimise nutritional management and determine the nutritional status of an individual. Other measures include anthropometrical indices, biochemical evaluation, clinical evaluation and food and diet history. Measurement of anthropometry includes the weight, body mass index (BMI), skinfold measurement and body composition. However, recently, body composition using a bioimpedance analysis (BIA), dual X-ray absorptiometry (DXA) and computed tomography (CT) has been used to measure adiposity [20]. Meanwhile, biochemical parameters that are usually assessed include the complete blood count, electrolytes and liver parameters [21,22]. Clinical evaluation determines a patient’s inability to chew or swallow, loss of appetite, metabolic stress due to infection, gastrointestinal symptoms such as vomiting, diarrhoea and nausea, fluid retention and clinical signs on the skin indicating micronutrient deficiency, as well as functional assessment to determine muscle function [22]. Finally, the assessment of diet history involves food and beverage intake and the influence of cultural or religious factors, also taking into account allergies, food preference, supplement intake and intolerance to estimate total energy, carbohydrate, fat and protein intake [21]. Therefore, a comprehensive nutrition assessment is pertinent to determine the nutritional status of patients.
Although patients with psoriasis with MetS are more likely to be over-nourished due to obesity, the excess energy intake may be mainly from calorie-dense low-nutrient foods. A Brazilian study among male patients with psoriasis and patients with psoriasis arthritis aged between 19 and 60 years reported a high intake of calories, total fat and protein exceeding the recommended levels and a lower intake of fibre and minerals [23]. These results were similar to an Italian study assessing seven days of dietary intake whereby patients had a higher carbohydrate, total fat and polyunsaturated fatty acid (PUFA) intake and lower fibre intake compared to controls [24]. Meanwhile, in a Turkish case-control study, an association between low vitamin E intake and severity in patients was observed [25]. Although patients had higher BMI compared to controls, their overall intake was significantly lower compared to controls. It is evident that patients with psoriasis, particularly those with MetS, have a poor nutritional status and poor-quality diet that may lead to nutritional deficiencies. It is important for patients attending a clinic to complete a thorough nutritional assessment. Therefore, this scoping review was undertaken to identify and summarise current findings on the types of nutrition assessment in patients with psoriasis in clinical settings. This review also identifies knowledge gaps in planning treatment and relevant research in the future.
2. Methods
This scoping review was conducted following the framework outlined by Arkensey and O’Malley [26]. Five different steps were followed based on the framework: (1) identifying the research question; (2) identifying relevant studies; (3) selecting studies; (4) charting the data; and (5) collating, summarising and reporting results. Reporting of this review was in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) [27].
2.1. Identifying the Research Question
The research question was the following: what tools/methods are used for nutrition assessment in patients with psoriasis?
2.2. Identifying Relevant Studies
A literature search was performed on four electronic databases: PubMed, Scopus, Web of Science and Ovid in March 2023 using the search string “metabolic syndrome” AND (“psoriasis vulgaris” OR “plaque psoriasis”). No additional filter was applied.
2.3. Study Selection
Results of the search were imported to Zotero software (Corporation for Digital Scholarship, Vienna, VA, USA)) to organise and track relevant data. This software was used to remove duplicates; document and manage the screening process; and categorise publications that meet the inclusion and exclusion criteria. Two assessors (HH and SK) independently assessed titles and abstracts based on the selection criteria. Several meetings were held over the course of screening to compare the articles against selection criteria and disagreements between assessors were resolved with a third assessor (MA), providing a binding verdict to reach a consensus. This author also performed second layer of screening to determine the final inclusion in the review. Finally, the full texts were obtained when a paper was deemed relevant. Studies were included if screening for MetS was done using published criteria, in addition to the diagnosis of psoriasis by dermatologists. Animal and child studies, reviews, case reports, proceedings, editorials, commentaries, book chapters and opinion papers were excluded. Only full-text articles were included in the final analysis.
2.4. Charting the Data
Data extraction was performed by HH and cross-checked by SK by tabulating it using a standardised form. Data extraction included essential characteristics such as author(s), title, journal, publication year, country of the first author, aims/objectives, sample size, participant characteristics, study design, MetS definition criteria, nutritional assessment methods and primary and secondary outcomes. Poor nutritional status was determined when an abnormal marker of nutritional status was reported. Clinical outcomes of interest were related to the presence of MetS and all key findings and outcomes were described in narrative form.
2.5. Collating, Summarising and Reporting the Results
Sociodemographic criteria for defining MetS, type of nutritional assessment, nutritional status and major outcomes were summarised and reported.
3. Results
Based on the initial search, a total of 1693 articles were identified using PubMed, Web of Science, Ovid and Scopus. A total of 271 were removed due to duplication. The remaining 1422 titles and abstracts were further screened for eligibility and 76 full texts were assessed. These were then screened according to the exclusion criteria, and finally 21 articles were included in the analysis (Figure 2).

Figure 2.
Flow chart of search strategies.
3.1. Study Characteristics
A total of 21 studies were included in this review, published between 2015 and 2023. Study characteristics are presented in Table 1. A total of 61.9% of the studies were from Asian countries [28,29,30,31,32,33,34,35,36,37,38,39,40], and 52.4% were case-control studies [29,31,33,37,38,41,42,43,44,45,46] with a total of 4286 participants. Eight studies matched participants with age and sex [31,33,34,37,38,42,43,44], three studies matched for BMI [35,41,45] and only one study matched for ethnicity [45]. A total of 71.4% of studies had a higher number of males compared to females [28,29,30,31,32,33,34,35,37,38,40,41,44,46,47]. In total, 52.4% of patients with psoriasis were between 40 and 50 years old [30,31,32,35,36,38,39,41,44,46,47]. A total of 61.9% of the studies reported a mild psoriasis severity (PASI < 10) [30,31,32,33,34,35,36,38,40,41,43,45]. Nine out of twenty-one studies reported a disease duration of more than 10 years [36,39,40,41,42,43,45,47,48].

Table 1.
Study characteristics (n = 21).
3.2. Metabolic Syndrome Screening
There were four MetS definition criteria used to define MetS in the included studies, as shown in Table 2. In total, 57.1% of the studies used NCEP ATP II criteria [28,29,31,32,33,35,37,38,39,42,43,48], and 33.3% were using International Diabetes Federation (IDF) criteria for MetS [30,34,36,38,40,41,44]. Two studies used the harmonised guideline [45,47], and one study used the Polish Forum of Prevention criteria [46]. The prevalence of MetS in patients with psoriasis ranged from 13.2% [36] to 67.80% [37].
Table 2.
Metabolic syndrome screening criteria.
3.3. Nutritional Assessment in Patients with Psoriasis
The waist circumference, fasting blood glucose, HDL, TG and blood pressure were the most common assessments conducted in MetS patients.
Although waist circumference was measured in all studies, two studies did not report any values [29,35]. Variations in the cut-offs for the waist circumference were observed. Eight studies used the cut-off of 102 cm for males and 88 cm for females based on the NCEP ATP III criteria [28,29,33,36,39,42,43,47]. Six studies used a cut-off for Asians, which was 90 cm for males and more than 80 cm for females [30,31,32,34,37,38]. Meanwhile, another six studies used a cut-off of 94 cm for males and 80 cm for females [40,41,44,45,46,48]. Only one study from India used an Asian Indian cut-off of 85 cm for males and 80 cm for females [35].
A total of 13 studies also reported abdominal adiposity in percentages ranging from 26.4% [33] to 78.6% [39]. Seven studies reported that more than half of the subjects had a higher waist circumference [34,39,41,42,43,47,48]; meanwhile, six studies reported that less than 50% of the subjects had a higher waist circumference [30,31,33,37,38,44].
Although all studies measured fasting blood glucose, one did not report the results [48]. Elevated blood sugar was defined as more than 100 mg/dL or 6.1 mmol/L in all the studies. Fourteen studies reported mean or median fasting blood glucose levels between 85.80 mg/dL [40] and 140.09 mg/dL [29]. Twelve studies presented the data as the prevalence of elevated blood glucose ranging from 5.3% [35] to 42.1% [33] in patients with psoriasis.
Fasting TG were assessed in all studies. Elevated fasting TG were defined as more than 150 mg/dL or 1.7 mmol/L. Sixteen studies reported mean and median fasting TG between 90.5 mg/dL [32] and 203.68 mg/dL [39]. Meanwhile, 13 studies reported a prevalence of elevated fasting TG between 26.05% [44] and 83.0% [39] in patients with psoriasis.
All studies measured and reported fasting HDL cholesterol. Low HDL was defined as less than 40 mg/dL or 1.0 mmol/L in males and less than 50 mg/dL or 1.3 mmol/L in females. Fourteen studies reported a prevalence of low HDL cholesterol in patients between 18.0% [43] and 70% [38].
Although blood pressure was measured in all studies, only three studies reported the results [29,35,40]. High blood pressure or hypertension was defined as systolic blood pressure of more than 130 mmHg or diastolic blood pressure of more than 85 mmHg. Fourteen studies reported the prevalence of hypertension in patients with psoriasis between 18.95% [37] and 61% [47]. Nine studies reported mean systolic blood pressure between 120 mmHg [32] and 141 mmHg [45] and diastolic blood pressure between 70 mmHg [32] and 90.7 mmHg [33].
3.4. Nutritional Status of Plaque Patients with Psoriasis (Table 3)
Nineteen studies assessed BMI [28,29,30,31,32,33,34,36,38,39,40,41,42,43,44,45,46,47,48]. Nine out of 12 Asian studies reported a mean BMI of 24.0 kg/m2 [33] to 31.15 kg/m2 [39], which falls under the overweight and obese category using the Asia–Pacific cut-off. Meanwhile, five out of seven non-Asian studies reported a mean BMI of 26.24 kg/m2 [42] to 31.6 kg/m2 [45], which is defined as the overweight and obese category as per WHO guidelines. The BMI of patients with psoriasis was higher compared to controls. Other anthropometry assessments conducted were the hip circumference in two studies [45,47] and waist-to-hip ratio in two studies [45,46].
Table 3.
Nutrition assessment tools/methods and nutritional status.
Table 3.
Nutrition assessment tools/methods and nutritional status.
| Author (Year), Location and Study Design | Participant Characteristics (Cases) | Participant Characteristics (Controls) | Nutritional Status | Anthropometry Measure | Biochemical Parameter | Clinical Parameters |
|---|---|---|---|---|---|---|
| Gisondi et al., 2007 [43] Italy Case-control | Mean age: 62.1 ± 15.1 yrs Sex: 160/178 Sample size: (n = 338) MetS: 30.1% | Mean age: 63.8 ± 20.4 yrs Sex: 150/184 Sample size: (n = 334) MetS: 20.6% | Overweight 27.7 ± 4.8 kg/m2 | WC | x | BP |
| Pereira et al., 2011 [35] India Case-control | Mean age: 46.51 ± 13.53 yrs Sex: 62/15 Sample size: (n = 77) MetS: 18.2% PASI: 4.61 ± 4.18 | Mean age: 43.24 ± 12.33 yrs Sex: 63/29 Sample size: (n = 92) MetS: 17.4% | x | WC, WHR | OGTT, fasting insulin, post-prandial insulin, TC, HDL, TG, FBG | BP |
| Damevska et al., 2013 [42] Macedonia Case-control | Mean age: 51.52 ± 15.56 yrs Sex: 52/70 Sample size: (n = 122) MetS: 24.6% PASI: 14.75 ± 12.78 | Mean age: 51.56 ± 15.72 yrs Sex: 52/70 Sample size: (n = 122) MetS: 22.9% | Severe obesity PsO: 4.1% Control: 1.6% Obesity PsO: 16.4% Control: 9.8% | WC | x | BP |
| Akcali et al., 2014 [28] Turkey Case-control | Mean age: 49.51 ± 18.26 yrs Sex: 26/24 Sample size: (n = 50) MetS: 50% | Mean age: 47.87 ± 16.43 yrs Sex: 20/20 Sample size: Control (n = 40) MetS: 25% | Overweight PsO: 26.92 ± 4.11 kg/m2 Control: 25.73 ± 5.89 kg/m2 | WC | TG, HDL, FBG, homocysteine, fibrinogen, adiponectin | BP |
| Baeta et al., 2014 [48] Brazil Cross sectional cohort | Mean age: 51.5 ± 14 yrs Sex: 93/97 Sample size: (n = 190) MetS: 44.9% PASI: 3.4 ± 3.03 | x | Normal: 35.7% Overweight: 31.1% Obese I: 22.6% Obese II: 7.4% Obese III: 3.2% | WC | TC, LDL, HDL, TG | BP |
| Puig et al., 2014 [47] Spain RCT | Mean age: 43.9 ± 12.7 yrs Sex: 190/273 Sample size: (n = 273) MetS: 42% PASI: 21.2 ± 9.4 | x | Overweight Male: 28.3 ± 4.6 kg/m2 Female: 29.6 ± 7.5 kg/m2 | WC, HC | FBG, fasting insulin, HbA1c, TC, HDL, LDL, TG, ApoA1, ApoB, ApoA, adiponectin | BP |
| Ucak et al., 2014 [40] Turkey Case-control | Mean age: 32.24 ± 7.54 yrs Sex: 11/14 Sample size: (n = 25) MetS: 40% PASI: 1.96 ± 0.84 | Mean age: 31.40 ± 6.77 yrs Sex: 14/11 Sample size: (n = 25) MetS: 36% | Overweight PsO: 24.96 ± 2.53 kg/m2 Normal Control: 23.80 ± 1.50 kg/m2 | WC | FBG, LDL. HDL, TC, TG, HbA1c, insulin, c-peptide levels, TSH, T3, T4, ghrelin | BP |
| Albareda et al., 2014 [41] Spain Case-control | Mean age: 49.32 ± 13.47 yrs Sex: 55/47 Sample size: (n = 102) MetS: 52.9% PASI: 6.4 (0–36.6) | Mean age: 48.71 ± 13.84 yrs Sex: 55/47 Sample size: (n = 102) MetS: 34.3% | Overweight PsO: 27.7 (18.9–41.79) kg/m2 Control: 27.36 (18.24–40.5) kg/m2 | BMI, WC | x | BP |
| Irimie et al., 2015 [44] Romania Case-control | Mean age: 49.51 ± 18.26 yrs Sex: 75/67 Sample size: (n = 142) MetS: 13.4% | Mean age: 47.87 ± 16.43 yrs Sex: 88/79 Sample size: (n = 167) MetS: 10.8% | x | WC | TG, TC, HDL, LDL | BP |
| Kothiwala et al., 2016 [33] India Case-control | Mean age: 37.9 ± 13.26 yrs Sex: 102/38 Sample size: (n = 140) MetS: 39.3% | Mean age: 36.1 ± 11.63 Sex: 97/43 Sample size: (n = 140) MetS: 17.1% | Normal PsO: 24.0 ± 4.43 kg/m2 Control: 22.6 ± 3.71 kg/m2 | BMI, WC | x | Carotid intima media thickness (CIMT) and BP |
| Pongpit et al., 2016 [36] Thailand Cross-sectional cohort | Mean age: 49.2 ± 14.0 yrs Sex: 75/90 Sample size: (n = 165) MetS: 50.3% PASI: 3.0 ± 2.7 | x | Overweight 24.8 ± 4.7 kg/m2 | BMI, WC | FBG, total cholesterol, TGL, LDL, HDL, AST, ALT | BP |
| Sharma et al., 2016 [38] India Case-control | Mean age: 44.94 ± 11.08 yrs Sample size: (n = 100) MetS: 38% | Mean age: 43.28 ± 12.06 yrs Sample size: (n = 100) MetS: 12% | Overweight: 50% Obese: 50% | WC | x | x |
| Uczniak et al., 2016 [46] Poland Case-control | Mean age: 46 ± 13 yrs Sex: 138/108 Sample size: (n = 246) | Mean age: 46 ± 13 yrs Sex: 35/40 Sample size: (n = 75) | x | WC, WHR | x | BP |
| Bulur et al., 2017 [29] Turkey Case-control | Mets Mean age: 39.00 ± 13.59 yrs Sex: 23/16 Sample size: (n = 39) No MetS Mean age: 46.95 ± 10.68 9 yrs Sex: 11/10 Sample size: (n = 21) MetS: 65% | Mean age: 36.73 ± 10.07 yrs Sex: 7/8 Sample size: (n = 12) | Overweight PsO with MetS: 26.35 ± 4.92 kg/m2 Control: 25.56 ± 2.92 kg/m2 Obese PsO without MetS: 33.55 ± 5.16 kg/m2 | WC | FBG, TG, TC, LDL, HDL | BP |
| Girisha et al., 2017 [31] India Case-control | Mean age: 45.5 ± 12.6 yrs Sex: 118/38 Sample size: (n = 156) MetS: 28.8% | Mean age: 45.4 ± 12.5 yrs Sex: 118/38 Sample size: (n = 156) MetS: 16.7% | Normal PsO 24 ± 4.8 kg/m2 Overweight Control 25.2 ± 2.2 kg/m2 | BMI, WC | x | BP |
| Salunke et al., 2017 [37] India Case-control | Mean age: 36.88 ± 13.37 yrs Sex: 71/24 Sample size: (n = 95) MetS: 38.9% | Mean age: 36.30 ± 13.07 yrs Sex: 73/22 Sample size: (n = 95) MetS: 21.05% | x | WC | FBS, TG, HDL | BP |
| Korkmaz et al., 2018 [32] Turkey Case-control | MetS Mean age: 44.2 ± 10.1 yrs Sex: 18/20 Sample size: (n = 38) PASI: 2.51 ± 1.90 No MetS Mean age: 43 ± 9.3 yrs Sex: 22/16 Sample size: (n = 38) PASI: 30.04 ± 2.18 MetS without PsO Mean age: 45.8 ± 9.7 yrs Sex: 19/19 Sample size: (n = 38) | Mean age: 42 ± 10.4 yrs Sex: 18/17 Sample size: (n = 35) | Obese MetS: 34 ± 9.3 kg/m2 Overweight PsO with MetS: 29.9 ± 6.6 kg/m2 PsO: 28 ± 4.2 kg/m2 Normal Control: 25 ± 5.4 kg/m2 | BMI, WC | FBG, urea, creatinine, TC, HDL, LDL, TG, TSH, ft3, ft4, platelets | BP |
| Mahyoodeen et al., 2019 [45] South Africa Case-control | Mean age: 53.3 ± 14.5 yrs Sex: 48/55 Sample size: (n = 103) MetS: 52.4% PASI: 4.80 (2.40–11.7) | Mean age: 47.9 ± 14.5 yrs Sex: 37/61 Sample size: (n = 98) MetS: 33.7% | Obesity PsO: 31.6 ± 8.42 kg/m2 Vitamin D deficiency 19.0 (12.6, 24.1) Overweight Control: 29.3 ± 6.67 kg/m2 Vitamin D deficiency 18.1 (13.1, 24.3) | BMI, WC, HC, WHR | FBG, HbA1c, TC, TG, HDL, LDL, TG, lipoprotein A, urea, creatinine, CRP, serum vitamin D | BP |
| Tas et al., 2021 [39] Turkey Cross sectional cohort | Mean age: 46.5 ± 13.2 yrs Sex: 53/59 Sample size: (n = 112) MetS: 67.8% | x | Obesity PsO with MetS: 31.15 ± 4.88 kg/m2 Overweight PsO without MetS: 28.33 ± 4.08 kg/m2 | WC | x | x |
| Deoghare et al., 2022 [30] India Cross-sectional cohort | Mean age: 40.45 ± 12.42 yrs Sex: 23/9 Sample size: (n = 32) MetS 37.5% PASI: 8.63 ± 7.49 | x | x | WC | FBS, TG, HDL | BP, carotid intima thickness, epicardial fat thickness |
| Patil et al., 2022 [34] India Case-control | Mean age: 39.67 ± 12.36 yrs Sex: 26/16 Sample size: (n = 42) MetS: 36% PASI: 6.42 ± 4.16 | Mean age: 39.71 ± 12.32 yrs Sex: 26/16 Sample size: (n = 42) MetS: 24% | Overweight and vitamin D deficiency: 26.96 ± 5.67 kg/m2 Overweight and insufficient vitamin D: 26.06 ± 5.98 kg/m2 | WC | FBG, TG, HDL, serum 25(OH)D levels | BP |
Abbreviations: ALT: alanine transaminase, AST: aspartate aminotransferase, ApoA1: apolipoprotein A1, ApoA: apolipoprotein A, ApoB: apolipoprotein B, BP: blood pressure, BMI: body mass index, CRP: c-reactive protein, FBG: fasting blood sugar, ft3: free triiodothyronine, ft4: free thyroxine, HDL: high-density lipoprotein, LDL: low-density lipoprotein, MetS: metabolic syndrome, OGTT: oral glucose tolerance, PASI: psoriasis area severity index, PsO: patients with psoriasis, TSH: thyroid-stimulating hormones, T3: triiodothyronine, T4: thyroxine, TC: total cholesterol, TGL: triglycerides, WC: waist circumference, WHR: waist–hip ratio, yrs: years, 25 (OH) D: 25-hydroxy vitamin D.
3.5. Other Additional Biomarkers Assessed
Two studies that measured patient HbA1c levels found these to be elevated [45,47]. Meanwhile, an oral glucose tolerance test (OGTT) was performed in two studies [35,41]. Fasting insulin was also measured in six studies and used to calculate insulin resistance using the homeostasis model assessment of insulin resistance (HOMA-IR) formula [35,36,39,40,41,47]. Only one study measured post-prandial insulin. A total of 11 studies measured total cholesterol [29,31,32,35,36,40,41,44,45,47,48], and 10 studies measured low-density lipoprotein (LDL) [29,32,35,36,40,41,44,45,47,48]. Three studies reported a prevalence of elevated total cholesterol between 18.5% [48] and 37.7% [35] in patients with psoriasis. Mean and median total cholesterol levels in seven studies ranged from 176.38 [29] to 223.42 mg/dL [44]. Three studies reported a prevalence of elevated LDL cholesterol between 16.9% [48] and 50.6% [35] among patients with psoriasis. Other biochemical assessments conducted were serum vitamin D levels [34,45], adiponectin [28,47], hs-CRP [45,47], apoprotein A [47], apoprotein B [47], leptin [47], homocysteine [28], fibrinogen [28], AST [36], ALT [36], platelets [32], c-peptide [40], ghrelin [40] and eGFR [45].
Other clinical assessments were the carotid intima thickness in two studies [30,33], epicardial fat thickness in one study [30] and ultrasonography of the liver in one study [36].
3.6. Psoriasis Area and Severity Index
Only 11 studies assessed the PASI with a score ranging from 1.9 to 21.2 [30,32,34,35,36,40,41,42,45,47,48]. Of these, three studies reported moderate scores [30,34,41], one reported a severe score [42] and two reported a very severe score [32,47].
4. Discussion
In this scoping review, we have summarised nutritional assessments performed in patients with psoriasis who were at risk of MetS. The nutritional assessments conducted were simple anthropometric measurements such as the weight and height to calculate BMI, waist circumference to predict abdominal adiposity, metabolic markers such as fasting blood glucose, TG, LDL and HDL cholesterol and blood pressure. These assessments were part of the MetS screening criteria to ascertain insulin resistance among patients with MetS. However, several studies also performed additional assessments to assess insulin resistance, liver impairment, kidney dysfunction and inflammation. Although most of the studies performed nutritional assessment, we were not able to deduce the nutritional status as the assessments were incomplete. Only 17 studies reported BMI results and we were not able to determine if all Asian studies used the Asia–Pacific cut-off instead of the WHO cut-off for BMI. Most patients with psoriasis suffered from poor nutritional status compared to controls. Only two studies assessed the vitamin D status among patients, which indicated vitamin D deficiency. However, no studies assessed the dietary intake of patients even though there is a possibility of obese patients being at risk of malnutrition.
Patients with psoriasis in the studies reviewed were mostly overweight or obese. An increased body mass could potentially decrease the drug distribution in the body, reducing the effectiveness of systemic or biological treatment [49,50]. In addition, a higher BMI also increases psoriasis severity [50,51,52] and induces inflammation [24,53], thus increasing the risk of comorbidities in patients.
Therefore, early detection of comorbidities and weight loss has been recommended for patients with psoriasis [54,55,56]. In the included studies, obesity was assessed by BMI, whereas abdominal obesity was assessed using the waist circumference and waist-to-hip ratio. BMI is widely used in clinical settings as it is a convenient index to determine nutritional status. However, it has its limitations, as a nutritional status determined through BMI does not distinguish the difference between fat mass and muscle mass, as it measures excess weight rather than excess fat. As BMI cannot determine the distribution of body fat [57], waist circumference is a better predictor of adiposity compared to BMI and is an important measure of central obesity, a predisposing factor for psoriasis [58]. A high volume of visceral adipose tissue (VAT) is associated with chronic inflammation [59]. White adipose tissue that is mostly formed as VAT induces inflammation and cell dysfunction, reduces insulin sensitivity and disrupts glucose and lipids by releasing proinflammatory adipokines [53,60]. However, it is recommended that both BMI and waist circumference are interpreted together to determine those who are abdominally obese with increased risks [61].
It was also observed that most studies did not classify waist circumference according to sex, leading to a possibility of misclassification. Waist circumference is also prone to measurement errors if it is not measured by trained staff. Therefore, there is potentially a need for a more reliable assessment of body composition to provide better data on the nutritional status, such as the use of bioelectrical impedance analysis (BIA), a safe, inexpensive, non-invasive technique that can distinguish the fat and muscle mass. The associated bioelectrical device employs a small electric current to estimate the resistance and reactance of various tissues in the body. Areas with high fat stores will show a high impedance reading compared to areas with high muscle stores that largely store body water [62]. It is also pertinent to assess the appendicular muscle mass due to an increased risk of sarcopenic obesity, particularly in older adults [63,64]. A study on patients with chronic plaque psoriasis found an association with myosteatosis and not sarcopenia, but the sample size in this study was small and the mean age of respondents was 45 years, which warrants further investigation in this population [65]. Meanwhile, several other studies have shown that sarcopenic obesity may also increase the risk of MetS [66,67,68], which poses a concern, stressing the importance of body composition measures.
Biochemical parameters that were mainly assessed were fasting blood glucose, HDL cholesterol and TG. Several studies also assessed the complete lipid profile including total cholesterol and LDL cholesterol. However, not all studies classified HDL cholesterol according to sex. There was a 16.6% increased risk of psoriasis in those with low HDL and the risk was higher in females, which was 16.9% [69]. Therefore, classification according to sex is necessary.
Although insulin resistance was not compulsory to define MetS, a few studies assessed this using various indexes. One of them was HOMA-IR, whereby the measured fasting insulin was multiplied by fasting blood glucose and a value of <2.5 was considered part of the normal range [70]. Although this method is simple, the values in subjects treated with insulin might not be accurate [71]. C-peptide was also used in a study to calculate the HOMA-IR and this is used interchangeably with fasting insulin as it has a longer half-life compared to insulin. A value less than 0.2 nmol/L indicates the diagnosis of type 1 diabetes mellitus and it is also a marker for microvascular and macrovascular complications [72]. However, both measures were mainly used to determine insulin resistance in patients with psoriasis [73,74].
In addition, the quantitative insulin-sensitivity check (QUICKI) was also determined by log transforming values of fasting glucose and the fasting insulin level with a cut-off of <0.33 for insulin resistance [75]. This index is consistent and precise but there are significant variations in the normal range based on the assays performed in the laboratory [71]. The OGTT was also performed in some studies to assess insulin sensitivity using the Matsuda index. The index is calculated from plasma glucose and insulin concentrations in the fasting state and during the OGTT [73]. A value of < 4.3 is used to predict insulin resistance. Although this index represents both hepatic and peripheral tissue sensitivity, it has a weak correlation with insulin resistance in those with diabetes [71]. Meanwhile, HbA1c was also assessed; values between 5.7% and 6.4% were considered markers of an increased risk for diabetes [74]. Apart from fasting insulin, HbA1c and OGTT are routinely performed to screen for diabetes and are performed in a clinical setting.
Other biochemical parameters such as apolipoprotein levels were measured to determine cardiovascular risk in patients. The ratio of apolipoprotein B (ApoB) to apolipoprotein AI (ApoAI) is a marker for lipid disturbances as ApoAI is associated with HDL particles and it can predict the risk of myocardial infarction [76,77]. As patients with psoriasis have a greater risk of developing cardiovascular diseases, ApoB has been demonstrated as a better predictor for cardiovascular disease risk compared to LDL [78,79]. Other parameters related to cardiovascular risk such as serum homocysteine, platelets and fibrinogen were also assessed. Elevated homocysteine levels have also been associated with severity of psoriasis. Meanwhile, platelet activation has been associated with endothelial dysfunction, inflammation and immune function in patients with psoriasis [80]. An increased level of fibrinogen has also been associated with severity in patients with psoriasis [81]. Meanwhile, the thyroid status was also assessed by measuring the thyroid-stimulating hormone (TSH), triiodothyronine (T4) and thyroxine (T4). T3 is the active hormone converted from T4. A high amount of produced T3/T4 will suppress TSH through negative feedback inhibition and vice versa [82]. Smoking, BMI and iodine intake have been associated with changes in TSH, whereby smoking led to hypothyroidism, high iodine intake led to hyperthyroidism and there was a positive correlation between BMI levels and TSH [83]. Meanwhile, thyroid dysfunction, particularly hypothyroidism, has been observed in patients with psoriasis [84,85].
Adiponectin and c-reactive protein (CRP) were assessed as inflammatory markers—increased levels were usually associated with the severity of psoriasis [86,87]. Meanwhile, higher levels of ghrelin were associated with an improved psoriasis severity score in a mouse model [88], and have also been assessed to determine the efficacy of biologics, which were also measured in the studies included [89]. Other biochemical markers assessing kidney functions (e.g., urea and creatinine) and liver function (e.g., alanine transaminase and aspartate aminotransferase) were also measured in several studies. Patients with psoriasis have an increased risk of developing chronic kidney failure as a result of psoriatic inflammation [90,91]. Meanwhile, non-alcoholic fatty liver disease was associated with psoriasis, particularly among men [92], as a result of insulin resistance due to an increased level of proinflammatory adipokines [93]. 25-hydroxyvitamin D was the only biochemical measure that assessed the nutritional status, as this test was able to determine the vitamin D status in the body. It has been demonstrated that patients with psoriasis are at risk of vitamin D deficiency [94,95]. As vitamin D is involved in bone growth, low levels may lead to bone loss, thereby increasing the risk of osteoporosis in these patients [96].
Clinical parameters that were assessed were mainly blood pressure, carotid intima thickness and epicardial fat thickness. Blood pressure is one of the most important clinical markers to define MetS, as hypertension is a cardiovascular risk factor and psoriasis is reported to be associated with an increased risk of hypertension [97,98]. Meanwhile, the carotid intima and epicardial fat thickness are markers for atherosclerosis and coronary artery diseases, respectively, and they are associated with visceral adiposity in patients with psoriasis [99,100].
It was observed that most of the patients with psoriasis in the studies included were either overweight or obese with abdominal adiposity. Studies that measured serum vitamin D showed that patients with psoriasis were at risk of vitamin D deficiency related to poor dietary intake or a lack of exposure to sunlight [101]. Although the aim of these studies was to determine the MetS status in these patients, some of the nutritional assessments performed were useful in determining the nutritional status of patients with psoriasis, such as the BMI, waist circumference and vitamin D status. These anthropometry methods were non-invasive, easy and quick to perform and could be conducted routinely in a clinical setting.
Besides vitamin D deficiency, patients with psoriasis could also be at risk of other nutritional deficiencies related to their dietary practices. An Italian study reported the presence of eating disorders among patients with psoriasis [102]. Meanwhile, other studies have reported an imbalance of nutrient intake related to a diet high in fat and simple carbohydrates and low in fibre [23,24]. Dietary intake is related to psoriasis severity whereby a diet high in saturated fat and red and simple sugar is associated with inflammation. Meanwhile, vitamin D, vitamin B12, vitamin A and selenium play an important role in improving severity [6,103,104]. Therefore, dietary assessment is pertinent to determine the nutritional status of patients with psoriasis. Several dietary assessment methods can be used to determine the dietary intake of patients with psoriasis. Trained dietitians or researchers could conduct a quick 24-h multiple-pass recall by asking open-ended questions to patients to enquire about actual intake in a specific period. Although this recall may rely on the patient’s ability to recall intake, a trained individual may be able to prompt patients to gather sufficient information in multiple passes such as dietary recall for the past 24-h, followed by details of food and beverages consumed, the portion size or ingredients and a summary of the entire day’s intake. This method is used daily in busy clinical practices by dietitians or nutritionists [105,106]. Meanwhile, in the research setting, food frequency questionnaires or food records could be employed. A food frequency questionnaire is used to estimate the usual intake over 6 months to a year. It is a closed method using a questionnaire and may be subjected to recall bias. However, it is still considered a reliable tool for dietary intake and is used in epidemiological studies [106,107]. A food record or diary is a very useful tool in research whereby patients could record their daily intake for a period of 3, 4 or 7 days with the help of a guide to assist them in recording their food and beverages. Although it is time-consuming and there is a tendency to under-report or over-report, this tool could capture current intake, timing or meals, frequency or eating out. Cooking methods are also very useful in assessing nutrient deficiencies and trained researchers could clarify missing information through a debriefing process [106,108]. Although each of these proposed methods has its limitations, these can be minimised either by skilled professionals or by the use of technology to assist reporting.
Patients with psoriasis who are overweight and obese are more likely to develop MetS. Therefore, early dietary intervention is needed to improve the nutritional status, reduce the risk of metabolic disorders and improve the effectiveness of treatments [103,104,109,110]. Dietary recommendations are often individualised based on the patients’ comorbidities. Obese or overweight patients with psoriasis without MetS would usually be advised on caloric restriction and weight reduction. A low-calorie diet lowers BMI and reduces inflammation and oxidative stress, thus improving the response to treatment [54,110]. Meanwhile, patients with MetS will require a more in-depth dietary consultation based on their elevated biochemical and clinical parameters. Besides caloric restriction and weight reduction, recommendations also include the restriction of total fat and refined carbohydrates. A Mediterranean diet is more appropriate for these patients as it is a balanced diet, as well as high in antioxidants, polyphenols and mono-unsaturated fats. The anti-inflammatory effect of the diet has been associated with reducing coronary heart disease, increasing immunity and reducing the inflammatory response [103,111]. Dietary supplementation, particularly with vitamin D, could also be recommended for patients with deficiency [103].
Although the severity of psoriasis has been associated with MetS in several studies, it is not routinely assessed in clinical practice. The PASI is commonly used to determine the efficacy of treatment in clinical trials, as scores reflect improvement or worsening of the condition. The scoring is based on the redness, thickness and scaliness of target plaques on the head, upper limbs, trunk and lower limbs. The scoring is from 0 to 6 and is based on the percentage of skin or body surface area (BSA) covered with psoriasis. A score of 0 indicates no involvement, 1 = <10% BSA, 2 = 10–29% BSA, 3 = 30–49% BSA, 4 = 50–69% BSA, 5 = 70–89% BSA and 6 = 90–100% BSA [4]. However, the BSA is further categorised as mild (0–5%), moderate (>5–10%), severe (>10–15%) and very severe (>15%) [112]. Psoriasis severity has been associated with MetS whereby overexpression of proinflammatory cytokines leads to inflammation, causing prolonged tissue damage, increasing the risk of comorbidities such as obesity, MetS, non-alcoholic fatty liver disease, psoriatic arthritis and inflammatory bowel disease [113,114,115]. However, no significant association between severity and MetS was reported in any of the studies reviewed, which is inconsistent with published meta-analyses [113,116].
It is also important to note that psoriasis begins in childhood in almost one-third of cases. With obesity, insulin resistance and MetS developing in even younger children of pre-pubertal ages, early screening and detection are necessary [117,118]. Obesity, particularly central obesity, is more prevalent in children with psoriasis and is usually assessed using the waist circumference percentile, weight-to-height ratio and body mass percentile [117,118,119]. Several other studies have also observed insulin resistance [117,119] and cardiovascular comorbidities such as hypertension in children [120,121,122]. However, studies assessing MetS in children are still scarce compared to adults, possibly due to a lack of standardised international guidelines to screen children for MetS. As treatment options are limited for children, dietary intervention should be commenced as early as possible.
This scoping review summarised the nutrition assessment and nutritional status of patients with psoriasis with MetS. Although we were able to address the research gaps, there are also several limitations in this review. Firstly, only studies that assessed MetS using published criteria were included, thereby limiting the number of studies in the review. Secondly, studies with self-reported psoriasis were not included in this review. Therefore, this may have excluded some relevant studies that may have assessed the nutritional status of patients with psoriasis.
5. Conclusions
In conclusion, patients with psoriasis are at risk of MetS and an increase in body mass and adiposity may play a role. Although anthropometry measurement is employed to determine the nutritional status, it is also evident that patients with psoriasis may have a risk of nutrient deficiencies, which is not assessed in clinical practice or research settings. Additional assessments, such as body composition and dietary intake, need to be performed to determine the nutritional status of these patients and assess their health risk, and subsequently devise a suitable intervention. This review provides practical insights for an integrative collaboration between dermatologists and dietitians for better treatment and intervention.
Author Contributions
Conceptualization, S.K., N.H.M.H. and K.-Y.C.; methodology, S.K., N.H.M.H., K.-Y.C. and M.A.; writing—original draft preparation, N.H.M.H., S.K. and V.M.; writing—review and editing, N.H.M.H., S.K., K.-Y.C., V.M. and M.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research has received internal funding from the Centre for Research and Instrumentation (CRIM) and Faculty of Health Sciences, Universiti Kebangsaan Malaysia, Malaysia. The funding number is GGPM, 2020-024.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO. Global Report on Psoriasis; World Health Organization: Geneva, Switzerland, 2016; ISBN 978-92-4-156518-9. [Google Scholar]
- Michalek, I.M.; Loring, B.; John, S.M. A Systematic Review of Worldwide Epidemiology of Psoriasis. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.W.; Read, C. Pathophysiology, Clinical Presentation, and Treatment of Psoriasis: A Review. JAMA 2020, 323, 1945–1960. [Google Scholar] [CrossRef]
- Fredriksson, T.; Pettersson, U. Severe Psoriasis—Oral Therapy with a New Retinoid. Dermatology 1978, 157, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Bellinato, F.; Girolomoni, G.; Albanesi, C. Pathogenesis of Chronic Plaque Psoriasis and Its Intersection With Cardio-Metabolic Comorbidities. Front. Pharmacol. 2020, 11, 117. [Google Scholar] [CrossRef]
- Kanda, N.; Hoashi, T.; Saeki, H. Nutrition and Psoriasis. Int. J. Mol. Sci. 2020, 21, 5405. [Google Scholar] [CrossRef]
- Kunz, M.; Simon, J.C.; Saalbach, A. Psoriasis: Obesity and Fatty Acids. Front. Immunol. 2019, 10, 1807. [Google Scholar] [CrossRef]
- Bu, J.; Ding, R.; Zhou, L.; Chen, X.; Shen, E. Epidemiology of Psoriasis and Comorbid Diseases: A Narrative Review. Front. Immunol. 2022, 13, 880201. [Google Scholar] [CrossRef]
- Takeshita, J.; Grewal, S.; Langan, S.M.; Mehta, N.N.; Ogdie, A.; Van Voorhees, A.S.; Gelfand, J.M. Psoriasis and Comorbid Diseases. J. Am. Acad. Dermatol. 2017, 76, 393–403. [Google Scholar] [CrossRef] [PubMed]
- Vanderpuye-Orgle, J.; Zhao, Y.; Lu, J.; Shrestha, A.; Sexton, A.; Seabury, S.; Lebwohl, M. Evaluating the Economic Burden of Psoriasis in the United States. J. Am. Acad. Dermatol. 2015, 72, 961–967.e5. [Google Scholar] [CrossRef]
- Gisondi, P.; Fostini, A.C.; Fossà, I.; Girolomoni, G.; Targher, G. Psoriasis and the Metabolic Syndrome. Clin. Dermatol. 2018, 36, 21–28. [Google Scholar] [CrossRef]
- Alberti, K.G.; Zimmet, P.Z. Definition, Diagnosis and Classification of Diabetes Mellitus and Its Complications. Part 1: Diagnosis and Classification of Diabetes Mellitus Provisional Report of a WHO Consultation. Diabet. Med. J. Br. Diabet. Assoc. 1998, 15, 539–553. [Google Scholar] [CrossRef]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [CrossRef]
- Balkau, B.; Charles, M.A. Comment on the Provisional Report from the WHO Consultation. European Group for the Study of Insulin Resistance (EGIR). Diabet. Med. J. Br. Diabet. Assoc. 1999, 16, 442–443. [Google Scholar] [CrossRef]
- Einhorn, D.; Reaven, G.M.; Cobin, R.H.; Ford, E.; Ganda, O.P.; Handelsman, Y.; Hellman, R.; Jellinger, P.S.; Kendall, D.; Krauss, R.M.; et al. American College of Endocrinology Position Statement on the Insulin Resistance Syndrome. Endocr. Pract. 2003, 9, 237–252. [Google Scholar] [CrossRef] [PubMed]
- Lemieux, I.; Després, J.-P. Metabolic Syndrome: Past, Present and Future. Nutrients 2020, 12, 3501. [Google Scholar] [CrossRef]
- Gelfand, J.M.; Yeung, H. Metabolic syndrome in patients with psoriatic disease. J. Rheumatol. Suppl. 2012, 89, 24–28. [Google Scholar] [CrossRef]
- Wu, J.J.; Kavanaugh, A.; Lebwohl, M.G.; Gniadecki, R.; Merola, J.F. Psoriasis and metabolic syndrome: Implications for the management and treatment of psoriasis. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 797–806. [Google Scholar] [CrossRef]
- Rodríguez-Cerdeira, C.; Cordeiro-Rodríguez, M.; Carnero-Gregorio, M.; López-Barcenas, A.; Martínez-Herrera, E.; Fabbrocini, G.; Sinani, A.; Arenas-Guzmán, R.; González-Cespón, J.L. Biomarkers of Inflammation in Obesity-Psoriatic Patients. Mediat. Inflamm. 2019, 28, 7353420. [Google Scholar] [CrossRef]
- Blake, T.; Gullick, N.J.; Hutchinson, C.E.; Barber, T.M. Psoriatic Disease and Body Composition: A Systematic Review and Narrative Synthesis. PLoS ONE 2020, 15, e0237598. [Google Scholar] [CrossRef]
- Reber, E.; Gomes, F.; Vasiloglou, M.F.; Schuetz, P.; Stanga, Z. Nutritional Risk Screening and Assessment. J. Clin. Med. 2019, 8, 1065. [Google Scholar] [CrossRef]
- Truijen, S.P.M.; Hayhoe, R.P.G.; Hooper, L.; Schoenmakers, I.; Forbes, A.; Welch, A.A. Predicting Malnutrition Risk with Data from Routinely Measured Clinical Biochemical Diagnostic Tests in Free-Living Older Populations. Nutrients 2021, 13, 1883. [Google Scholar] [CrossRef] [PubMed]
- Solis, M.Y.; de Melo, N.S.; Macedo, M.E.M.; Carneiro, F.P.; Sabbag, C.Y.; Lancha Júnior, A.H.; Frangella, V.S. Nutritional Status and Food Intake of Patients with Systemic Psoriasis and Psoriatic Arthritis Associated. Einstein 2012, 10, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Macchia, P.E.; Tarantino, G.; Di Somma, C.; Pane, E.; Balato, N.; Napolitano, M.; Colao, A.; Savastano, S. Nutrition: A Key Environmental Dietary Factor in Clinical Severity and Cardio-Metabolic Risk in Psoriatic Male Patients Evaluated by 7-Day Food-Frequency Questionnaire. J. Transl. Med. 2015, 13, 303. [Google Scholar] [CrossRef] [PubMed]
- Atayoglu, A.T.; Çapar, A.G.; Basmisirlioglu, E.; Yasar, Y.; Aykemat, Y.; Guner Atayoglu, A.; Inanc, N. Investigation of the Relationship between the Disease Severity and Quality of Life of Patients with psoriasis and Their Anthropometric Measurements and Diets. Healthcare 2022, 10, 2323. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Akcali, C.; Buyukcelik, B.; Kirtak, N.; Inaloz, S. Clinical and Laboratory Parameters Associated with Metabolic Syndrome in Turkish Patients with Psoriasis. J. Int. Med. Res. 2014, 42, 386–394. [Google Scholar] [CrossRef]
- Bulur, I.; Erdogan, H.; Ciftci, E.; Canaz, F.; Yigitaslan, S.; Yildiz, P.; Saracoglu, Z.; Bilgin, M. Evaluating the Role of Neurotrophins in the Psoriasis and Metabolic Syndrome Relationship. Turk. J. Dermatol./Turk Derm. Derg. 2017, 11, 168–173. [Google Scholar] [CrossRef]
- Deoghare, S.; Talanikar, H.; Deora, M.S.; Kothari, R.; Sharma, Y.K.; Dalve, K.; Kapoor, A.; Patil, A. A Cross-Sectional Study to Assess Sub-Clinical Atherosclerosis in Patients of Psoriasis Independent of Metabolic Syndrome. Indian J. Dermatol. 2022, 67, 328–333. [Google Scholar] [CrossRef]
- Girisha, B.S.; Thomas, N. Metabolic Syndrome in Psoriasis among Urban South Indians: A Case Control Study Using SAM-NCEP Criteria. J. Clin. Diagn. Res. 2017, 11, WC01–WC04. [Google Scholar] [CrossRef]
- Korkmaz, S. Mean Platelet Volume and Platelet Distribution Width Levels in Patients with Mild Psoriasis Vulgaris with Metabolic Syndrome. Adv. Dermatol. Allergol./Postępy Dermatol. I Alergol. 2018, 35, 367–371. [Google Scholar] [CrossRef]
- Kothiwala, S.K.; Khanna, N.; Tandon, N.; Naik, N.; Sharma, V.K.; Sharma, S.; Sreenivas, V. Prevalence of Metabolic Syndrome and Cardiovascular Changes in Patients with Chronic Plaque Psoriasis and Their Correlation with Disease Severity: A Hospital-Based Cross-Sectional Study. Indian J. Dermatol. Venereol. Leprol. 2016, 82, 510–518. [Google Scholar] [CrossRef]
- Patil, A.; Deo, K.; Kalyan, D.; Deora, M.; Sharma, Y.; Deoghare, S. Association of Vitamin D Deficiency with Psoriasis and Metabolic Syndrome: A Case-Control Study in Indian Patients. Indian J. Dermatol. 2022, 67, 92. [Google Scholar] [CrossRef]
- Pereira, R.; Amladi, S.; Varthakavi, P. A Study of the Prevalence of Diabetes, Insulin Resistance, Lipid Abnormalities, and Cardiovascular Risk Factors in Patients with Chronic Plaque Psoriasis. Indian J. Dermatol. 2011, 56, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Pongpit, J.; Porntharukchareon, S.; Kaewduang, P.; Promson, K.; Stitchantrakul, W.; Petraksa, S.; Thakkinstian, A.; Kositchaiwat, C.; Rajatanavin, N.; Sobhonslidsuk, A. Liver Stiffness Measurement in Psoriasis: Do Metabolic or Disease Factors Play the Important Role? BioMed Res. Int. 2016, 2016, 7963972. [Google Scholar] [CrossRef] [PubMed]
- Salunke, A.S.; Nagargoje, M.V.; Belgaumkar, V.A.; Tolat, S.N.; Chavan, R.B. Association of Metabolic Syndrome in Chronic Plaque Patients with psoriasis and Their Correlation with Disease Severity, Duration and Age: A Case Control Study from Western Maharashtra. J. Clin. Diagn. Res. 2017, 11, WC06–WC10. [Google Scholar] [CrossRef] [PubMed]
- Sharma, Y.K.; Prakash, N.; Gupta, A. Prevalence of Metabolic Syndrome as per the NCEP and IDF Definitions Vis-a-Vis Severity and Duration of Psoriasis in a Semi-Urban Maharashtrian Population: A Case Control Study. Diabetes Metab. Syndr. Clin. Res. Rev. 2016, 10, S72–S76. [Google Scholar] [CrossRef] [PubMed]
- Tas, B.; Kabeloglu, V. Prevalence of Metabolic Syndrome and Its Parameters and Their Correlations With Psoriasis Duration, Severity, and Sleep Quality In Patients with psoriasis: A Cross-Sectional Study. Dermatol. Pract. Concept. 2021, 11, e2021049. [Google Scholar] [CrossRef]
- Ucak, H.; Demir, B.; Cicek, D.; Erden, I.; Aydin, S.; Dertlioglu, S.B.; Arica, M. Metabolic Changes and Serum Ghrelin Level in Patients with Psoriasis. Dermatol. Res. Pract. 2014, 2014, 175693. [Google Scholar] [CrossRef]
- Albareda, M.; Ravella, A.; Castello, M.; Saborit, S.; Peramiquel, L.; Vila, L. Metabolic Syndrome and Its Components in Patients with Psoriasis. Springerplus 2014, 3, 612. [Google Scholar] [CrossRef]
- Damevska, K.; Neloska, L.; Gocev, G.; Mihova, M. Metabolic Syndrome in Untreated Patients with Psoriasis: Case-Control Study. JDDG J. Der Dtsch. Dermatol. Ges. 2013, 11, 1169–1175. [Google Scholar] [CrossRef]
- Gisondi, P.; Tessari, G.; Conti, A.; Piaserico, S.; Schianchi, S.; Peserico, A.; Giannetti, A.; Girolomoni, G. Prevalence of Metabolic Syndrome in Patients with Psoriasis: A Hospital-Based Case-Control Study. Br. J. Dermatol. 2007, 157, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Irimie, M.; Oanţă, A.; Irimie, C.A.; Fekete, L.G.; Minea, D.I.; Pascu, A. Cardiovascular Risk Factors in Patients with Chronic Plaque Psoriasis: A Case-Control Study on the Brasov County Population. Acta Dermatovenerol. Croat. 2015, 23, 28–35. [Google Scholar]
- Mahyoodeen, N.; Crowther, N.; Snyman, T.; Pillay, L.; Tikly, M. High Burden of the Metabolic Syndrome and Its Component Disorders in South Africans with Psoriasis. Int. J. Dermatol. 2019, 58, 557–562. [Google Scholar] [CrossRef]
- Uczniak, S.; Gerlicz, Z.A.; Kozłowska, M.; Kaszuba, A. Presence of Selected Metabolic Syndrome Components in Patients with Psoriasis Vulgaris. Adv. Dermatol. Allergol./Postępy Dermatol. I Alergol. 2016, 33, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Puig, L.; Strohal, R.; Fuiman, J.; Pedersen, R.; Szumski, A.; Koenig, A.S.; Robertson, D.; Drexel, H. Cardiometabolic Biomarkers in Chronic Plaque Psoriasis before and after Etanercept Treatment. J. Dermatol. Treat. 2014, 25, 470–481. [Google Scholar] [CrossRef] [PubMed]
- Baeta, I.G.R.; Bittencourt, F.V.; Gontijo, B.; Goulart, E.M.A. Comorbidities and Cardiovascular Risk Factors in Patients with Psoriasis. An. Bras. De Dermatol. 2014, 89, 735–744. [Google Scholar] [CrossRef]
- Carrascosa, J.M.; Rocamora, V.; Fernandez-Torres, R.M.; Jimenez-Puya, R.; Moreno, J.C.; Coll-Puigserver, N.; Fonseca, E. Obesity and Psoriasis: Inflammatory Nature of Obesity, Relationship between Psoriasis and Obesity, and Therapeutic Implications. Actas Dermo-Sifiliográficas 2014, 105, 31–44. [Google Scholar] [CrossRef]
- Fleming, P.; Kraft, J.; Gulliver, W.P.; Lynde, C. The Relationship of Obesity With the Severity of Psoriasis: A Systematic Review. J. Cutan. Med. Surg. 2015, 19, 450–456. [Google Scholar] [CrossRef]
- Lin, I.-C.; Heck, J.E.; Chen, L.; Feldman, S.R. Psoriasis Severity and Cardiometabolic Risk Factors in a Representative US National Study. Am. J. Clin. Dermatol. 2021, 22, 719–730. [Google Scholar] [CrossRef]
- Paroutoglou, K.; Papadavid, E.; Christodoulatos, G.S.; Dalamaga, M. Deciphering the Association Between Psoriasis and Obesity: Current Evidence and Treatment Considerations. Curr. Obes. Rep. 2020, 9, 165–178. [Google Scholar] [CrossRef]
- Zorena, K.; Jachimowicz-Duda, O.; Ślęzak, D.; Robakowska, M.; Mrugacz, M. Adipokines and Obesity. Potential Link to Metabolic Disorders and Chronic Complications. Int. J. Mol. Sci. 2020, 21, 3570. [Google Scholar] [CrossRef]
- Barrea, L.; Megna, M.; Cacciapuoti, S.; Frias-Toral, E.; Fabbrocini, G.; Savastano, S.; Colao, A.; Muscogiuri, G. Very Low-Calorie Ketogenic Diet (VLCKD) in Patients with Psoriasis and Obesity: An Update for Dermatologists and Nutritionists. Crit. Rev. Food Sci. Nutr. 2022, 62, 398–414. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Del Giglio, M.; Girolomoni, G. Considerations for Systemic Treatment of Psoriasis in Obese Patients. Am. J. Clin. Dermatol. 2016, 17, 609–615. [Google Scholar] [CrossRef]
- Jensen, P.; Zachariae, C.; Christensen, R.; Geiker, N.R.W.; Schaadt, B.K.; Stender, S.; Astrup, A.; Hansen, P.R.; Skov, L. Effect of Weight Loss on the Cardiovascular Risk Profile of Obese Patients with Psoriasis. Acta Derm. Venereol. 2014, 94, 691–694. [Google Scholar] [CrossRef] [PubMed]
- Madden, A.M.; Smith, S. Body Composition and Morphological Assessment of Nutritional Status in Adults: A Review of Anthropometric Variables. J. Hum. Nutr. Diet. 2016, 29, 7–25. [Google Scholar] [CrossRef] [PubMed]
- Han, J.H.; Lee, J.H.; Han, K.D.; Kim, H.-N.; Bang, C.H.; Park, Y.M.; Lee, J.Y.; Kim, T.Y. Increased Risk of Psoriasis in Subjects with Abdominal Obesity: A Nationwide Population-Based Study. J. Dermatol. 2019, 46, 695–701. [Google Scholar] [CrossRef]
- Sajja, A.; Abdelrahman, K.M.; Reddy, A.S.; Dey, A.K.; Uceda, D.E.; Lateef, S.S.; Sorokin, A.V.; Teague, H.L.; Chung, J.; Rivers, J.; et al. Chronic Inflammation in Psoriasis Promotes Visceral Adiposity Associated with Noncalcified Coronary Burden over Time. J. Clin. Investig. 2020, 5, e142534. [Google Scholar] [CrossRef]
- Wolk, K.; Sabat, R. Adipokines in Psoriasis: An Important Link between Skin Inflammation and Metabolic Alterations. Rev. Endocr. Metab. Disord. 2016, 17, 305–317. [Google Scholar] [CrossRef]
- Ross, R.; Neeland, I.J.; Yamashita, S.; Shai, I.; Seidell, J.; Magni, P.; Santos, R.D.; Arsenault, B.; Cuevas, A.; Hu, F.B.; et al. Waist Circumference as a Vital Sign in Clinical Practice: A Consensus Statement from the IAS and ICCR Working Group on Visceral Obesity. Nat. Rev. Endocrinol. 2020, 16, 177–189. [Google Scholar] [CrossRef]
- Khalil, S.F.; Mohktar, M.S.; Ibrahim, F. The Theory and Fundamentals of Bioimpedance Analysis in Clinical Status Monitoring and Diagnosis of Diseases. Sensors 2014, 14, 10895–10928. [Google Scholar] [CrossRef]
- von Berens, Å.; Obling, S.R.; Nydahl, M.; Koochek, A.; Lissner, L.; Skoog, I.; Frändin, K.; Skoglund, E.; Rothenberg, E.; Cederholm, T. Sarcopenic Obesity and Associations with Mortality in Older Women and Men–A Prospective Observational Study. BMC Geriatr. 2020, 20, 199. [Google Scholar] [CrossRef] [PubMed]
- Wagenaar, C.A.; Dekker, L.H.; Navis, G.J. Prevalence of Sarcopenic Obesity and Sarcopenic Overweight in the General Population: The Lifelines Cohort Study. Clin. Nutr. 2021, 40, 4422–4429. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Xiang, H.; Tan, L.; Zhou, J.; Tang, J.; Hu, X.; Yang, M. Psoriasis Is Associated With Myosteatosis but Not Sarcopenia: A Case-Control Study. Front. Med. 2021, 8, 754932. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Jeong, J.B.; Kang, J.; Ahn, D.-W.; Kim, J.W.; Kim, B.G.; Lee, K.L.; Oh, S.; Yoon, S.H.; Park, S.J.; et al. Association between Sarcopenia Level and Metabolic Syndrome. PLoS ONE 2021, 16, e0248856. [Google Scholar] [CrossRef]
- Park, S.-J.; Ryu, S.-Y.; Park, J.; Choi, S.-W. Association of Sarcopenia with Metabolic Syndrome in Korean Population Using 2009–2010 Korea National Health and Nutrition Examination Survey. Metab. Syndr. Relat. Disord. 2019, 17, 494–499. [Google Scholar] [CrossRef]
- Zhang, H.; Lin, S.; Gao, T.; Zhong, F.; Cai, J.; Sun, Y.; Ma, A. Association between Sarcopenia and Metabolic Syndrome in Middle-Aged and Older Non-Obese Adults: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 364. [Google Scholar] [CrossRef]
- Xiao, Y.; Jing, D.; Tang, Z.; Peng, C.; Yin, M.; Liu, H.; Chen, X.; Shen, M. Serum Lipids and Risk of Incident Psoriasis: A Prospective Cohort Study from the UK Biobank Study and Mendelian Randomization Analysis. J. Investig. Dermatol. 2022, 142, 3192–3199.e12. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis Model Assessment: Insulin Resistance and Beta-Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Gutch, M.; Kumar, S.; Razi, S.M.; Gupta, K.K.; Gupta, A. Assessment of Insulin Sensitivity/Resistance. Indian J. Endocrinol. Metab. 2015, 19, 160–164. [Google Scholar] [CrossRef]
- Leighton, E.; Sainsbury, C.A.; Jones, G.C. A Practical Review of C-Peptide Testing in Diabetes. Diabetes Ther. 2017, 8, 475–487. [Google Scholar] [CrossRef]
- Gyldenløve, M.; Storgaard, H.; Holst, J.J.; Vilsbøll, T.; Knop, F.K.; Skov, L. Patients with Psoriasis Are Insulin Resistant. J. Am. Acad. Dermatol. 2015, 72, 599–605. [Google Scholar] [CrossRef]
- Karadag, A.S.; Yavuz, B.; Ertugrul, D.T.; Akin, K.O.; Yalcin, A.A.; Deveci, O.S.; Ata, N.; Kucukazman, M.; Dal, K. Is Psoriasis a Pre-Atherosclerotic Disease? Increased Insulin Resistance and Impaired Endothelial Function in Patients with Psoriasis. Int. J. Dermatol. 2010, 49, 642–646. [Google Scholar] [CrossRef] [PubMed]
- Katz, A.; Nambi, S.S.; Mather, K.; Baron, A.D.; Follmann, D.A.; Sullivan, G.; Quon, M.J. Quantitative Insulin Sensitivity Check Index: A Simple, Accurate Method for Assessing Insulin Sensitivity in Humans. J. Clin. Endocrinol. Metab. 2000, 85, 2402–2410. [Google Scholar] [CrossRef] [PubMed]
- Lind, L.; Vessby, B.; Sundström, J. The Apolipoprotein B/AI Ratio and the Metabolic Syndrome Independently Predict Risk for Myocardial Infarction in Middle-Aged Men. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 406–410. [Google Scholar] [CrossRef]
- McQueen, M.J.; Hawken, S.; Wang, X.; Ounpuu, S.; Sniderman, A.; Probstfield, J.; Steyn, K.; Sanderson, J.E.; Hasani, M.; Volkova, E.; et al. Lipids, Lipoproteins, and Apolipoproteins as Risk Markers of Myocardial Infarction in 52 Countries (the INTERHEART Study): A Case-Control Study. Lancet Lond. Engl. 2008, 372, 224–233. [Google Scholar] [CrossRef]
- Nemati, H.; Khodarahmi, R.; Rahmani, A.; Ebrahimi, A.; Amani, M.; Eftekhari, K. Serum Lipid Profile in Psoriatic Patients: Correlation between Vascular Adhesion Protein 1 and Lipoprotein (a). Cell Biochem. Funct. 2013, 31, 36–40. [Google Scholar] [CrossRef]
- Ramezani, M.; Zavattaro, E.; Sadeghi, M. Evaluation of Serum Lipid, Lipoprotein, and Apolipoprotein Levels in Psoriatic Patients: A Systematic Review and Meta-Analysis of Case-Control Studies. Adv. Dermatol. Allergol. Dermatol. Alergol. 2019, 36, 692–702. [Google Scholar] [CrossRef]
- Anyfanti, P.; Margouta, A.; Goulas, K.; Gavriilaki, M.; Lazaridou, E.; Patsatsi, A.; Gkaliagkousi, E. Endothelial Dysfunction in Psoriasis: An Updated Review. Front. Med. 2022, 9, 864185. [Google Scholar] [CrossRef] [PubMed]
- Marongiu, F.; Sorano, G.G.; Bibbò, C.; Pistis, M.P.; Conti, M.; Mulas, P.; Balestrieri, A.; Biggio, P. Abnormalities of Blood Coagulation and Fibrinolysis in Psoriasis. Dermatology 1994, 189, 32–37. [Google Scholar] [CrossRef]
- Dayan, C.; Panicker, V. Management of Hypothyroidism with Combination Thyroxine (T4) and Triiodothyronine (T3) Hormone Replacement in Clinical Practice: A Review of Suggested Guidance. Thyroid. Res. 2018, 11, 1. [Google Scholar] [CrossRef]
- Babić Leko, M.; Gunjača, I.; Pleić, N.; Zemunik, T. Environmental Factors Affecting Thyroid-Stimulating Hormone and Thyroid Hormone Levels. Int. J. Mol. Sci. 2021, 22, 6521. [Google Scholar] [CrossRef]
- Cira, C.-I.; Carsote, M.; Nistor, C.; Petca, A.; Petca, R.-C.; Sandru, F. Conundrum for Psoriasis and Thyroid Involvement. Int. J. Mol. Sci. 2023, 24, 4894. [Google Scholar] [CrossRef]
- Ruffilli, I.; Ragusa, F.; Benvenga, S.; Vita, R.; Antonelli, A.; Fallahi, P.; Ferrari, S.M. Psoriasis, Psoriatic Arthritis, and Thyroid Autoimmunity. Front. Endocrinol. 2017, 8, 139. [Google Scholar] [CrossRef] [PubMed]
- Baran, A.; Flisiak, I.; Jaroszewicz, J.; Świderska, M. Effect of Psoriasis Activity on Serum Adiponectin and Leptin Levels. Adv. Dermatol. Allergol./Postępy Dermatol. I Alergol. 2015, 32, 101–106. [Google Scholar] [CrossRef]
- Shibata, S.; Tada, Y.; Hau, C.S.; Mitsui, A.; Kamata, M.; Asano, Y.; Sugaya, M.; Kadono, T.; Masamoto, Y.; Kurokawa, M.; et al. Adiponectin Regulates Psoriasiform Skin Inflammation by Suppressing IL-17 Production from Γδ-T Cells. Nat. Commun. 2015, 6, 7687. [Google Scholar] [CrossRef] [PubMed]
- Qu, R.; Chen, X.; Hu, J.; Fu, Y.; Peng, J.; Li, Y.; Chen, J.; Li, P.; Liu, L.; Cao, J.; et al. Ghrelin Protects against Contact Dermatitis and Psoriasiform Skin Inflammation by Antagonizing TNF-α/NF-ΚB Signaling Pathways. Sci. Rep. 2019, 9, 1348. [Google Scholar] [CrossRef] [PubMed]
- Ozdemir, M.; Yüksel, M.; Gökbel, H.; Okudan, N.; Mevlitoğlu, I. Serum Leptin, Adiponectin, Resistin and Ghrelin Levels in Psoriatic Patients Treated with Cyclosporin. J. Dermatol. 2012, 39, 443–448. [Google Scholar] [CrossRef]
- Al-Harbi, N.O.; Nadeem, A.; Ansari, M.A.; Al-Harbi, M.M.; Alotaibi, M.R.; AlSaad, A.M.S.; Ahmad, S.F. Psoriasis-like Inflammation Leads to Renal Dysfunction via Upregulation of NADPH Oxidases and Inducible Nitric Oxide Synthase. Int. Immunopharmacol. 2017, 46, 1–8. [Google Scholar] [CrossRef]
- Conti, A.; Giovannini, L.; Mandel, V.D.; Odorici, G.; Lasagni, C.; Bigi, L.; Pellacani, G.; Cappelli, G. Chronic Kidney Disease in Psoriasis: A Cohort Study. JDDG J. Der Dtsch. Dermatol. Ges. 2020, 18, 438–445. [Google Scholar] [CrossRef]
- Ruan, Z.; Lu, T.; Chen, Y.; Yuan, M.; Yu, H.; Liu, R.; Xie, X. Association Between Psoriasis and Nonalcoholic Fatty Liver Disease Among Outpatient US Adults. JAMA Dermatol. 2022, 158, 745–753. [Google Scholar] [CrossRef]
- Prussick, R.B.; Miele, L. Nonalcoholic Fatty Liver Disease in Patients with Psoriasis: A Consequence of Systemic Inflammatory Burden? Br. J. Dermatol. 2018, 179, 16–29. [Google Scholar] [CrossRef] [PubMed]
- Gamonal, S.B.L.; Gamonal, A.C.C.; Marques, N.C.V.; Brandão, M.A.F.; Raposo, N.R.B. 25-Hydroxyvitamin D as a Biomarker of Vitamin D Status in Plaque Psoriasis and Other Dermatological Diseases: A Cross-Sectional Study. Sao Paulo Med. J. 2022, 141, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Song, G.G. Association between Circulating 25-Hydroxyvitamin D Levels and Psoriasis, and Correlation with Disease Severity: A Meta-Analysis. Clin. Exp. Dermatol. 2018, 43, 529–535. [Google Scholar] [CrossRef] [PubMed]
- De Martinis, M.; Allegra, A.; Sirufo, M.M.; Tonacci, A.; Pioggia, G.; Raggiunti, M.; Ginaldi, L.; Gangemi, S. Vitamin D Deficiency, Osteoporosis and Effect on Autoimmune Diseases and Hematopoiesis: A Review. Int. J. Mol. Sci. 2021, 22, 8855. [Google Scholar] [CrossRef] [PubMed]
- Duan, X.; Liu, J.; Mu, Y.; Liu, T.; Chen, Y.; Yu, R.; Xiong, X.; Wu, T. A Systematic Review and Meta-Analysis of the Association between Psoriasis and Hypertension with Adjustment for Covariates. Medicine 2020, 99, e19303. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-N.; Han, K.; Song, S.-W.; Lee, J.H. Hypertension and Risk of Psoriasis Incidence: An 11-Year Nationwide Population-Based Cohort Study. PLoS ONE 2018, 13, e0202854. [Google Scholar] [CrossRef]
- Bulbul Sen, B.; Atci, N.; Rifaioglu, E.N.; Ekiz, O.; Kartal, I.; Buyukkaya, E.; Kurt, M.; Karakas, M.F.; Buyukkaya, S.; Akcay, A.B.; et al. Increased Epicardial Fat Tissue Is a Marker of Subclinical Atherosclerosis in Patients with Psoriasis. Br. J. Dermatol. 2013, 169, 1081–1086. [Google Scholar] [CrossRef]
- Girisha, B.S.; Shibina, S.; Raghuraja, U.; Subramanyam, K. Carotid Intima-Media Thickness and Epicardial Fat Thickness Predict Precoronary Artery Disease Status in Psoriasis. Indian J. Dermatol. Venereol. Leprol. 2021, 87, 357–363. [Google Scholar] [CrossRef]
- Barrea, L.; Savanelli, M.C.; Di Somma, C.; Napolitano, M.; Megna, M.; Colao, A.; Savastano, S. Vitamin D and Its Role in Psoriasis: An Overview of the Dermatologist and Nutritionist. Rev. Endocr. Metab. Disord. 2017, 18, 195–205. [Google Scholar] [CrossRef]
- Crosta, M.L.; Caldarola, G.; Fraietta, S.; Craba, A.; Benedetti, C.; Coco, V.; Janiri, L.; Rinaldi, L.; De Simone, C. Psychopathology and Eating Disorders in Patients with Psoriasis. G. Ital. Dermatol. E Venereol. 2014, 149, 355–361. [Google Scholar]
- Musumeci, M.L.; Nasca, M.R.; Boscaglia, S.; Micali, G. The Role of Lifestyle and Nutrition in Psoriasis: Current Status of Knowledge and Interventions. Dermatol. Ther. 2022, 35, e15685. [Google Scholar] [CrossRef] [PubMed]
- Pona, A.; Haidari, W.; Kolli, S.S.; Feldman, S.R. Diet and Psoriasis. Dermatol. Online J. 2019, 25, 13030/qt1p37435s. [Google Scholar] [CrossRef]
- Conway, J.M.; Ingwersen, L.A.; Moshfegh, A.J. Accuracy of Dietary Recall Using the USDA Five-Step Multiple-Pass Method in Men: An Observational Validation Study. J. Am. Diet. Assoc. 2004, 104, 595–603. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.-S.; Oh, K.; Kim, H.C. Dietary Assessment Methods in Epidemiologic Studies. Epidemiol. Health 2014, 36, e2014009. [Google Scholar] [CrossRef]
- Cui, Q.; Xia, Y.; Wu, Q.; Chang, Q.; Niu, K.; Zhao, Y. A Meta-Analysis of the Reproducibility of Food Frequency Questionnaires in Nutritional Epidemiological Studies. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 12. [Google Scholar] [CrossRef]
- Cantwell, M.M.; Millen, A.E.; Carroll, R.; Mittl, B.L.; Hermansen, S.; Brinton, L.A.; Potischman, N. A Debriefing Session with a Nutritionist Can Improve Dietary Assessment Using Food Diaries. J. Nutr. 2006, 136, 440–445. [Google Scholar] [CrossRef]
- Chung, M.; Bartholomew, E.; Yeroushalmi, S.; Hakimi, M.; Bhutani, T.; Liao, W. Dietary Intervention and Supplements in the Management of Psoriasis: Current Perspectives. Psoriasis Targets Ther. 2022, 12, 151–176. [Google Scholar] [CrossRef] [PubMed]
- Garbicz, J.; Całyniuk, B.; Górski, M.; Buczkowska, M.; Piecuch, M.; Kulik, A.; Rozentryt, P. Nutritional Therapy in Persons Suffering from Psoriasis. Nutrients 2021, 14, 119. [Google Scholar] [CrossRef]
- Katsimbri, P.; Korakas, E.; Kountouri, A.; Ikonomidis, I.; Tsougos, E.; Vlachos, D.; Papadavid, E.; Raptis, A.; Lambadiari, V. The Effect of Antioxidant and Anti-Inflammatory Capacity of Diet on Psoriasis and Psoriatic Arthritis Phenotype: Nutrition as Therapeutic Tool? Antioxidants 2021, 10, 157. [Google Scholar] [CrossRef] [PubMed]
- Finlay, A.Y. Current Severe Psoriasis and the Rule of Tens. Br. J. Dermatol. 2005, 152, 861–867. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Young, P.; Armstrong, A. An Update on Psoriasis and Metabolic Syndrome: A Meta-Analysis of Observational Studies. PLoS ONE 2017, 12, e0181039. [Google Scholar] [CrossRef]
- Korman, N.J. Management of Psoriasis as a Systemic Disease: What Is the Evidence? Br. J. Dermatol. 2020, 182, 840–848. [Google Scholar] [CrossRef]
- Bhatia, B.K.; Millsop, J.W.; Debbaneh, M.; Koo, J.; Linos, E.; Liao, W. Diet and Psoriasis: Part 2. Celiac Disease and Role of a Gluten-Free Diet. J. Am. Acad. Dermatol. 2014, 71, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.W.; Harskamp, C.T.; Armstrong, E.J. Psoriasis and metabolic syndrome: A systematic review and meta-analysis of observational studies. J. Am. Acad. Dermatol. 2013, 68, 654–662. [Google Scholar] [CrossRef]
- Caroppo, F.; Galderisi, A.; Ventura, L.; Fortina, A.B. Metabolic syndrome and insulin resistance in pre-pubertal children with psoriasis. Eur. J. Pediatr. 2021, 180, 739–1745. [Google Scholar] [CrossRef] [PubMed]
- Hunjan, M.K.; Maradit Kremers, H.; Lohse, C.; Tollefson, M. Association between obesity and pediatric psoriasis. Pediatr. Dermatol. 2018, 35, e304–e305. [Google Scholar] [CrossRef] [PubMed]
- Guidolin, L.; Borin, M.; Fontana, E.; Caroppo, F.; Piaserico, S.; Fortina, A.B. Central Obesity in Children with Psoriasis. Acta Derm. -Venereol. 2018, 98, 282–283. [Google Scholar] [CrossRef] [PubMed]
- Pietrzak, A.; Grywalska, E.; Walankiewicz, M.; Lotti, T.; Roliński, J.; Myśliński, W.; Chabros, P.; Piekarska-Myślińska, D.; Reich, K. Psoriasis and metabolic syndrome in children: Current data. Clin. Exp. Dermatol. 2017, 42, 131–136. [Google Scholar] [CrossRef]
- Badaoui, A.; Tounian, P.; Mahé, E. Psoriasis and metabolic and cardiovascular comorbidities in children: A systematic review. Arch Pediatr. 2019, 26, 86–94. [Google Scholar] [CrossRef]
- Phan, K.; Lee, G.; Fischer, G. Pediatric psoriasis and association with cardiovascular and metabolic comorbidities: Systematic review and meta-analysis. Pediatr. Dermatol. 2020, 37, 661–669. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).