

Using Machine-Learning to Assess the Prognostic Value of Early Enteral Feeding Intolerance in Critically Ill Patients: A Retrospective Study
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Data Sources
2.3. Population
2.4. Features
Features Definitions
- Demographic characteristics included age, gender, BMI, and admission type;
- Severity scores included the APACHEII score and the SOFA score on day one and day three (0–24 h and 48–72 h after ICU admission, respectively);
- EFI markers were defined according to three common categories identified in a systematic review [8], including “large” gastric residual volumes (GRVs), GI symptoms, and “inadequate” delivery of EN. We included daily level markers under each category. Makers were preprocessed, using the following transformations:
- Daily ‘large’ GRV was defined according to a threshold of 250 mL, which was found to be the median value used in previous studies (ranging between 150 and 500 mL) [8]. The feature GRV on day x (x = 1–3) was coded into a dichotomous variable that denotes the occurrence/non-occurrence of a GRV amount greater than 250 mL in 24 h;
- Daily GI symptoms were defined according to established definitions [9]: Daily vomiting/regurgitation was defined as visible vomiting or regurgitation in any amount in 24 h. Daily diarrhea was defined as loose or liquid stool three or more times within 24 h. Daily GI bleeding was defined as the visible appearance of blood in vomitus, nasogastric aspirate, or stool in 24 h. The feature GI symptom on day x (x = 1–3) was coded into a dichotomous feature denoting the occurrence/non-occurrence of a symptom in 24 h;
- Inadequate delivery of EN was defined according to the proportion of ‘energy requirements’ delivered on day three [8], with a cutoff of energy administration below 70% of the defined target [1]. The feature of inadequate delivery of EN on day three was coded into a dichotomous feature denoting an administration of less than 70% of the calculated caloric needs.
- Medications applied to manage EFI refer to prokinetic agents. Daily prokinetic agent usage was defined according to the daily intake of metoclopramide and erythromycin. Prokinetic agent on day x (x = 1–3) was coded into a dichotomous feature denoting the use/no use of these medications in 24 h.
2.5. Missing Data
2.6. Outcomes
2.7. Prediction of Early EN Failure
2.8. Statistical Analysis
2.9. Model Development
2.10. Model Interpretation
2.11. Software
3. Results
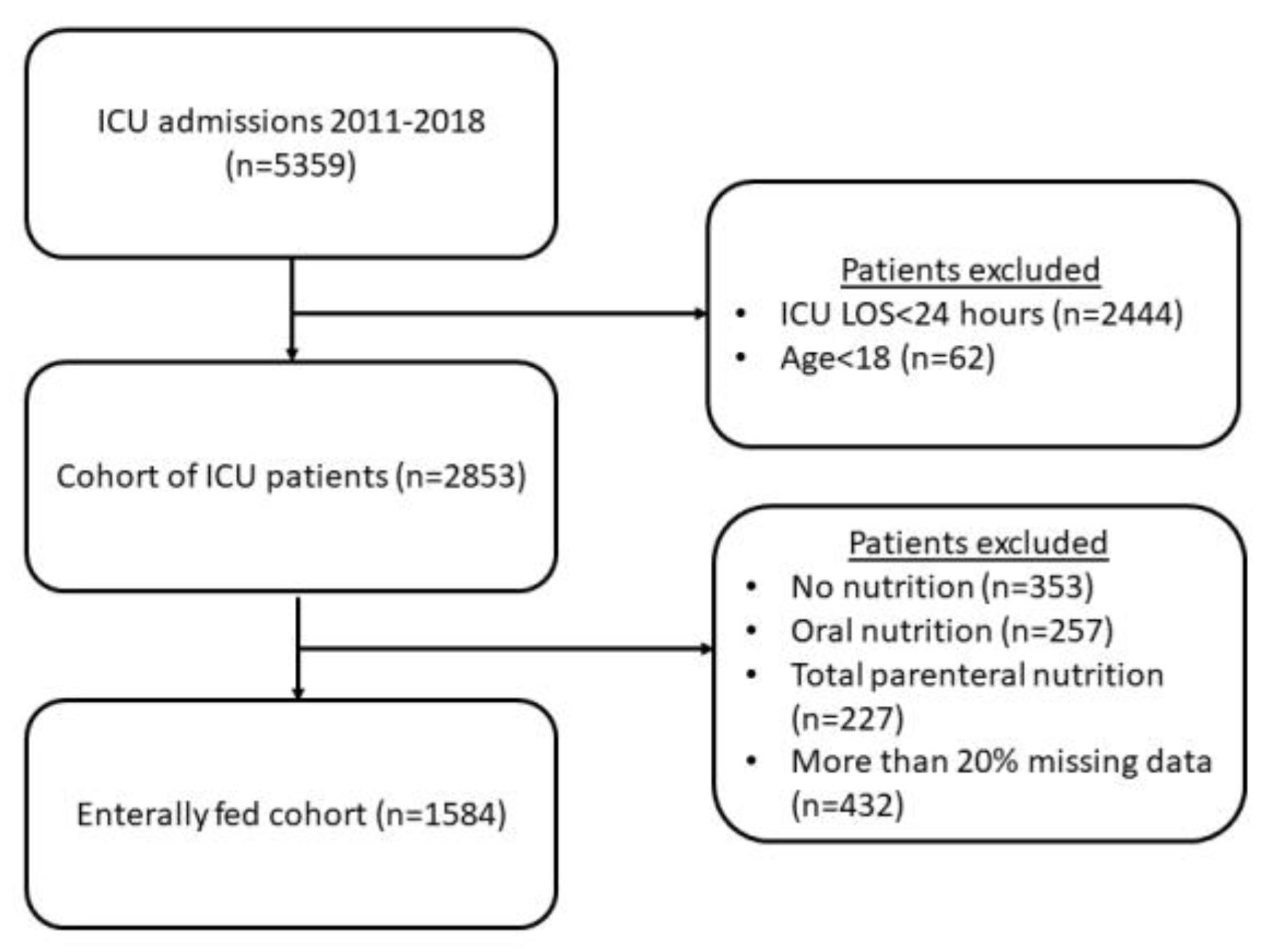
3.1. Cohort Selection
3.2. Cohort Characteristics
3.3. Correlation between Features and 90-Day Mortality
3.4. Prediction of 90-Day Mortality
3.5. Prediction of Secondary Outcomes
3.6. Prediction of Early EN Failure
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singer, P.; Blaser, A.R.; Berger, M.M.; Alhazzani, W.; Calder, P.C.; Casaer, M.P.; Hiesmayr, M.; Mayer, K.; Montejo, J.C.; Pichard, C.; et al. ESPEN Guideline on Clinical Nutrition in the Intensive Care Unit. Clin. Nutr. 2019, 38, 48–79. [Google Scholar] [CrossRef] [PubMed]
- Reintam Blaser, A.; Starkopf, J.; Alhazzani, W.; Berger, M.M.; Casaer, M.P.; Deane, A.M.; Fruhwald, S.; Hiesmayr, M.; Ichai, C.; Jakob, S.M.; et al. Early Enteral Nutrition in Critically Ill Patients: ESICM Clinical Practice Guidelines. Intensive Care Med. 2017, 43, 380–398. [Google Scholar] [CrossRef] [PubMed]
- McClave, S.A.; Taylor, B.E.; Martindale, R.G.; Warren, M.M.; Johnson, D.R.; Braunschweig, C.; McCarthy, M.S.; Davanos, E.; Rice, T.W.; Cresci, G.A.; et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient. J. Parenter. Enter. Nutr. 2016, 40, 159–211. [Google Scholar] [CrossRef] [PubMed]
- Heyland, D.K.; Ortiz, A.; Stoppe, C.; Patel, J.J.; Yeh, D.D.; Dukes, G.; Chen, Y.J.; Almansa, C.; Day, A.G. Incidence, Risk Factors, and Clinical Consequence of Enteral Feeding Intolerance in the Mechanically Ventilated Critically Ill: An Analysis of a Multicenter, Multiyear Database. Crit. Care Med. 2021, 49, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Murthy, T.; Chapple, L.-A.S.; Lange, K.; Marathe, C.S.; Horowitz, M.; Peake, S.L.; Chapman, M.J. Gastrointestinal Dysfunction during Enteral Nutrition Delivery in Intensive Care Unit (ICU) Patients: Risk Factors, Natural History, and Clinical Implications. A Post-Hoc Analysis of The Augmented versus Routine Approach to Giving Energy Trial (TARGET). Am. J. Clin. Nutr. 2022, 116, 589–598. [Google Scholar] [CrossRef] [PubMed]
- Reintam Blaser, A.; Deane, A.M.; Preiser, J.C.; Arabi, Y.M.; Jakob, S.M. Enteral Feeding Intolerance: Updates in Definitions and Pathophysiology. Nutr. Clin. Pract. 2021, 36, 40–49. [Google Scholar] [CrossRef]
- Reintam Blaser, A.; Malbrain, M.L.N.G.; Starkopf, J.; Fruhwald, S.; Jakob, S.M.; De Waele, J.; Braun, J.-P.; Poeze, M.; Spies, C. Gastrointestinal Function in Intensive Care Patients: Terminology, Definitions and Management. Recommendations of the ESICM Working Group on Abdominal Problems. Intensive Care Med. 2012, 38, 384–394. [Google Scholar] [CrossRef]
- Reintam Blaser, A.; Starkopf, J.; Kirsimägi, Ü.; Deane, A.M. Definition, Prevalence, and Outcome of Feeding Intolerance in Intensive Care: A Systematic Review and Meta-Analysis. Acta Anaesthesiol. Scand. 2014, 58, 914–922. [Google Scholar] [CrossRef]
- Reintam Blaser, A.; Poeze, M. Gastrointestinal Symptoms during the First Week of Intensive Care Are Associated with Poor Outcome: A Prospective Multicentre Study. Intensive Care Med. 2013, 39, 899–909. [Google Scholar] [CrossRef]
- McClave, S.A.; Gualdoni, J.; Nagengast, A.; Marsano, L.S.; Bandy, K.; Martindale, R.G. Gastrointestinal Dysfunction and Feeding Intolerance in Critical Illness: Do We Need an Objective Scoring System? Curr. Gastroenterol. Rep. 2020, 22, 1. [Google Scholar] [CrossRef]
- Reintam Blaser, A.; Padar, M.; Mändul, M.; Elke, G.; Engel, C.; Fischer, K.; Giabicani, M.; Gold, T.; Hess, B.; Hiesmayr, M. Development of the Gastrointestinal Dysfunction Score (GIDS) for Critically Ill Patients—A Prospective Multicenter Observational Study (ISOFA Study). Clin. Nutr. 2021, 40, 4932–4940. [Google Scholar] [CrossRef] [PubMed]
- Preiser, J.-C.; Arabi, Y.M.; Berger, M.M.; Casaer, M.; McClave, S.; Montejo-González, J.C.; Peake, S.; Reintam Blaser, A.; Van den Berghe, G.; van Zanten, A.; et al. A Guide to Enteral Nutrition in Intensive Care Units: 10 Expert Tips for the Daily Practice. Crit. Care 2021, 25, 424. [Google Scholar] [CrossRef] [PubMed]
- Reintam Blaser, A.; Hiesmayr, M. Enteral Feeding, Even When the Gut Does Not Feel Very Good? Curr. Opin. Clin. Nutr. Metab. Care 2022, 25, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Rajkomar, A.; Dean, J.; Kohane, I. Machine Learning in Medicine. N. Engl. J. Med. 2019, 380, 1347–1358. [Google Scholar] [CrossRef]
- van de Sande, D.; van Genderen, M.E.; Huiskens, J.; Gommers, D.; van Bommel, J. Moving from Bytes to Bedside: A Systematic Review on the Use of Artificial Intelligence in the Intensive Care Unit. Intensive Care Med. 2021, 47, 750–760. [Google Scholar] [CrossRef]
- Shillan, D.; Sterne, J.A.C.; Champneys, A.; Gibbison, B. Use of Machine Learning to Analyse Routinely Collected Intensive Care Unit Data: A Systematic Review. Crit. Care 2019, 23, 284. [Google Scholar] [CrossRef]
- Fleuren, L.M.; Klausch, T.L.T.; Zwager, C.L.; Schoonmade, L.J.; Guo, T.; Roggeveen, L.F.; Swart, E.L.; Girbes, A.R.J.; Thoral, P.; Ercole, A.; et al. Machine Learning for the Prediction of Sepsis: A Systematic Review and Meta-Analysis of Diagnostic Test Accuracy. Intensive Care Med. 2020, 46, 383–400. [Google Scholar] [CrossRef]
- Aperstein, Y.; Cohen, L.; Bendavid, I.; Cohen, J.; Grozovsky, E.; Rotem, T.; Singer, P. Improved ICU Mortality Prediction Based on SOFA Scores and Gastrointestinal Parameters. PLoS ONE 2019, 14, e0222599. [Google Scholar] [CrossRef]
- Hu, K.; Deng, X.L.; Han, L.; Xiang, S.; Xiong, B.; Pinhu, L. Development and Validation of a Predictive Model for Feeding Intolerance in Intensive Care Unit Patients with Sepsis. Saudi J. Gastroenterol. Off. J. Saudi Gastroenterol. Assoc. 2022, 28, 32–38. [Google Scholar] [CrossRef]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M. Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis Or Diagnosis (TRIPOD): The TRIPOD Statement. Ann. Intern. Med. 2015, 162, 55–63. [Google Scholar] [CrossRef]
- Lundberg, S.; Lee, S.-I. A Unified Approach to Interpreting Model Predictions. Adv. Neural Inf. Process. Syst. 2017, 30, 4766–4775. [Google Scholar]
- Salciute-Simene, E.; Stasiunaitis, R.; Ambrasas, E.; Tutkus, J.; Milkevicius, I.; Sostakaite, G.; Klimasauskas, A.; Kekstas, G. Impact of Enteral Nutrition Interruptions on Underfeeding in Intensive Care Unit. Clin. Nutr. 2021, 40, 1310–1317. [Google Scholar] [CrossRef] [PubMed]
- Yeh, D.D.; Ortiz-Reyes, L.A.; Quraishi, S.A.; Chokengarmwong, N.; Avery, L.; Kaafarani, H.M.A.; Lee, J.; Fagenholz, P.; Chang, Y.; DeMoya, M.; et al. Early Nutritional Inadequacy Is Associated with Psoas Muscle Deterioration and Worse Clinical Outcomes in Critically Ill Surgical Patients. J. Crit. Care 2018, 45, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Roimi, M.; Neuberger, A.; Shrot, A.; Paul, M.; Geffen, Y.; Bar-Lavie, Y. Early Diagnosis of Bloodstream Infections in the Intensive Care Unit Using Machine-Learning Algorithms. Intensive Care Med. 2020, 46, 454–462. [Google Scholar] [CrossRef]
- Ferreira, F.L.; Bota, D.P.; Bross, A.; Mélot, C.; Vincent, J.L. Serial Evaluation of the SOFA Score to Predict Outcome in Critically Ill Patients. JAMA 2001, 286, 1754–1758. [Google Scholar] [CrossRef]
- Bendavid, I.; Statlender, L.; Shvartser, L.; Teppler, S.; Azullay, R.; Sapir, R.; Singer, P. A Novel Machine Learning Model to Predict Respiratory Failure and Invasive Mechanical Ventilation in Critically Ill Patients Suffering from COVID-19. Sci. Rep. 2022, 12, 10573. [Google Scholar] [CrossRef]
- Messmer, A.S.; Moser, M.; Zuercher, P.; Schefold, J.C.; Müller, M.; Pfortmueller, C.A. Fluid Overload Phenotypes in Critical Illness—A Machine Learning Approach. J. Clin. Med. 2022, 11, 336. [Google Scholar] [CrossRef]
- Choi, T.Y.; Chang, M.-Y.; Heo, S.; Jang, J.Y. Explainable Machine Learning Model to Predict Refeeding Hypophosphatemia. Clin. Nutr. ESPEN 2021, 45, 213–219. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients (n = 1584) | Survivors (90-Day) (n = 972) | Non-Survivors (90-Day) (n = 612) | p-Value |
|---|---|---|---|---|
| age Mean ± SD | 59.05 ± 17.5 | 55.8 ± 18.3 | 64.1 ± 14.7 | 0.00 |
| gender (female) n (%) | 590 (37%) | 372 (38.3%) | 218 (35.6%) | ns |
| BMI Median [IQR] | 26.5 [23.5, 30.8] | 26.4 [23.4, 30.8] | 26.6 [23.8, 30.6] | ns |
| Severity scores on day one and day three Median [IQR] | ||||
| APACHEII | 23 [18, 28] | 21 [16, 26] | 26 [21, 31] | 0.00 |
| SOFA-d1 | 8 [5, 11] | 7 [4, 10] | 9 [7, 11] | 0.00 |
| SOFA-d3 | 8 [5, 11] | 7 [4, 10] | 10 [7, 13] | 0.00 |
| Daily GI symptoms on days 1–3 n (%) | ||||
| Diarrhea-d1 | 57 (3.6%) | 25 (2.6%) | 32 (6.2%) | 0.006 |
| Diarrhea-d2 | 80 (5.1%) | 43 (4.4%) | 37 (6%) | ns |
| Diarrhea-d3 | 122 (7.7%) | 69 (7.1%) | 53 (8.7%) | ns |
| GI bleeding-d1 | 28 (1.8%) | 14 (1.4%) | 14 (2.3%) | ns |
| GI bleeding-d2 | 27 (1.7%) | 15 (1.5%) | 12 (1.9%) | ns |
| GI bleeding-d3 | 24 (1.5%) | 15 (1.5%) | 9 (1.5%) | ns |
| Vomiting-d1 | 48 (3%) | 30 (3.1%) | 18 (2.9%) | ns |
| Vomiting-d2 | 40 (2.5%) | 26 (2.7%) | 14 (2.3%) | ns |
| Vomiting-d3 | 47 (3%) | 33 (3.4%) | 14 (2.3%) | ns |
| Daily large gastric residual volume on days 1–3 n (%) | ||||
| GRV > 250-d1 | 383 (24.2%) | 212 (21.8%) | 171 (27.9%) | 0.006 |
| GRV > 250-d2 | 334 (21.1%) | 164 (16.9%) | 170 (27.8%) | 0.00 |
| GRV > 250-d3 | 340 (21.5%) | 164 (16.9%) | 176 (28.8%) | 0.00 |
| Inadequate delivery of EN on day three n (%) | ||||
| Target Fail-d3 (<70%) | 1019 (64.3%) | 630 (65.1%) | 389 (63.7%) | ns |
| Daily prokinetic intake on days 1–3 n (%) | ||||
| Metoclopramide-d1 | 207 (14%) | 132 (14.6%) | 75 (13.2%) | ns |
| Metoclopramide-d2 | 371 (27%) | 225 (27.3%) | 146 (26.7%) | ns |
| Metoclopramide-d3 | 392 (30.9%) | 231 (31.3%) | 161 (30.7%) | ns |
| Erythromycin-d1 | 17(1.2%) | 10 (1.1%) | 7 (1.2%) | ns |
| Erythromycin-d2 | 30 (2.2%) | 10(1.2%) | 20 (3.7%) | 0.002 |
| Erythromycin-d3 | 36 (2.8%) | 13 (1.8%) | 23 (4.3%) | 0.007 |
| Clinical outcomes | ||||
| LOS Median [IQR] | 9.5 [5, 19] | 9 [5, 19] | 10 [6, 18] | ns |
| Prolonged LOS (LOS > 7 d) | 952 (60.1%) | 556 (57.2%) | 396 (64.7%) | 0.003 |
| 90-day mortality n (%) | 612 (38.6%) | |||
| 28-day mortality n (%) | 444 (28%) | |||
| ICU mortality n (%) | 358 (22.6% | |||
| Hospital mortality n (%) | 518 (32.7%) | |||
| Accuracy (SD) | Precision (SD) | Recall (SD) | Specificity (SD) | F1 (SD) | AUCROC (95% CI) | |
|---|---|---|---|---|---|---|
| Features on Days 1–3 | ||||||
| Gradient Boosting Classifier | 0.68 (0.03) | 0.63 (0.06) | 0.54 (0.04) | 0.77 (0.04) | 0.58 (0.05) | 0.73 (0.71–0.75) |
| Random Forest Classifier | 0.66 (0.03) | 0.61 (0.06) | 0.53 (0.05) | 0.75 (0.04) | 0.57 (0.04) | 0.71 (0.69–0.73) |
| Logistic Regression | 0.66 (0.04) | 0.62 (0.04) | 0.53 (0.05) | 0.76 (0.04) | 0.57 (0.04) | 0.71 (0.67–0.75) |
| AdaBoost Classifier | 0.64 (0.04) | 0.59 (0.09) | 0.53 (0.06) | 0.72 (0.08) | 0.55 (0.05) | 0.69 (0.65–0.73) |
| XGB Classifier | 0.63 (0.03) | 0.57 (0.06) | 0.54 (0.04) | 0.71 (0.06) | 0.55 (0.04) | 0.69 (0.66–0.72) |
| KN neighbors Classifier | 0.65 (0.03) | 0.59 (0.05) | 0.52 (0.04) | 0.74 (0.03) | 0.55 (0.04) | 0.68 (0.66–0.70) |
| Decision Tree Classifier | 0.60 (0.02) | 0.52 (0.05) | 0.51 (0.05) | 0.66 (0.02) | 0.51 (0.04) | 0.58 (0.56–0.60) |
| Baseline comparator: APACHE II | ||||||
| Logistic Regression | 0.65 (0.03) | 0.62 (0.09) | 0.45 (0.05) | 0.76 (0.06) | 0.52 (0.05) | 0.70 (0.66–0.74) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raphaeli, O.; Statlender, L.; Hajaj, C.; Bendavid, I.; Goldstein, A.; Robinson, E.; Singer, P. Using Machine-Learning to Assess the Prognostic Value of Early Enteral Feeding Intolerance in Critically Ill Patients: A Retrospective Study. Nutrients 2023, 15, 2705. https://doi.org/10.3390/nu15122705
Raphaeli O, Statlender L, Hajaj C, Bendavid I, Goldstein A, Robinson E, Singer P. Using Machine-Learning to Assess the Prognostic Value of Early Enteral Feeding Intolerance in Critically Ill Patients: A Retrospective Study. Nutrients. 2023; 15(12):2705. https://doi.org/10.3390/nu15122705
Chicago/Turabian StyleRaphaeli, Orit, Liran Statlender, Chen Hajaj, Itai Bendavid, Anat Goldstein, Eyal Robinson, and Pierre Singer. 2023. "Using Machine-Learning to Assess the Prognostic Value of Early Enteral Feeding Intolerance in Critically Ill Patients: A Retrospective Study" Nutrients 15, no. 12: 2705. https://doi.org/10.3390/nu15122705
APA StyleRaphaeli, O., Statlender, L., Hajaj, C., Bendavid, I., Goldstein, A., Robinson, E., & Singer, P. (2023). Using Machine-Learning to Assess the Prognostic Value of Early Enteral Feeding Intolerance in Critically Ill Patients: A Retrospective Study. Nutrients, 15(12), 2705. https://doi.org/10.3390/nu15122705