

Phytanic Acid Intake and Lifestyle Modifications on Quality of Life in Individuals with Adult Refsum Disease: A Retrospective Survey Analysis

Abstract
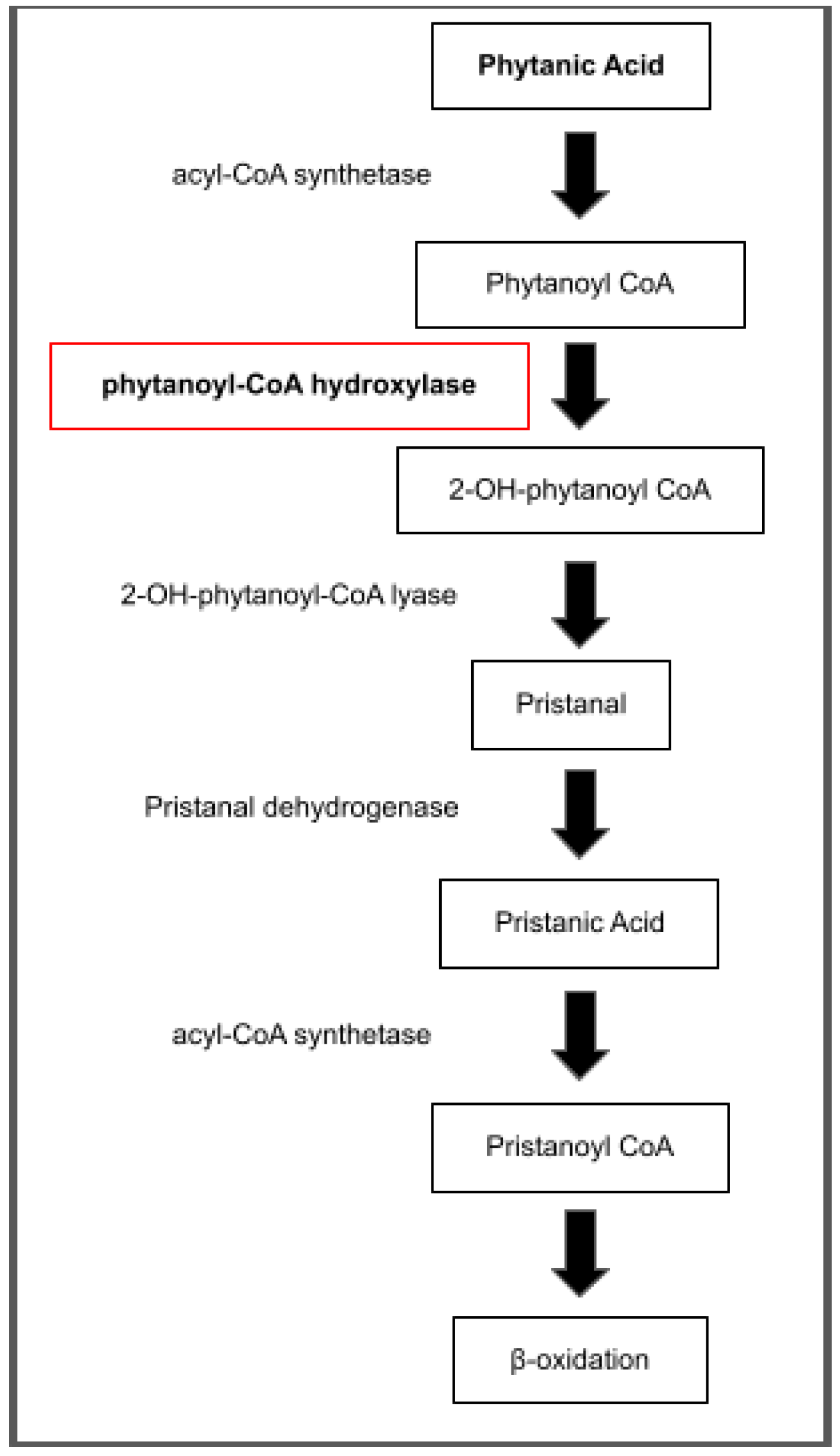
1. Introduction
2. Materials and Methods
3. Results
3.1. Demographics
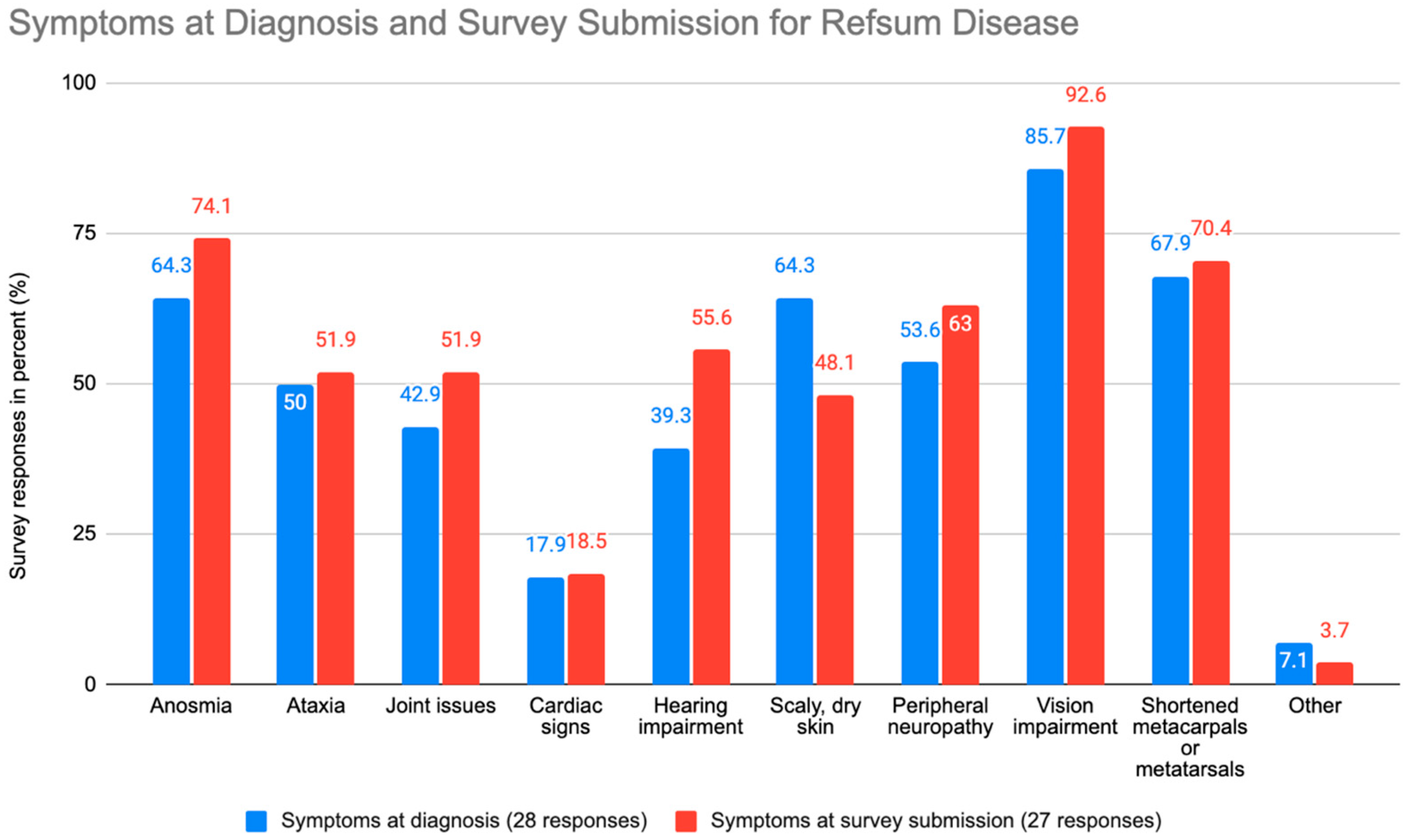
3.2. Common Symptoms
3.3. Retinitis Pigmentosa, Gene Mutations, and Hospitalizations
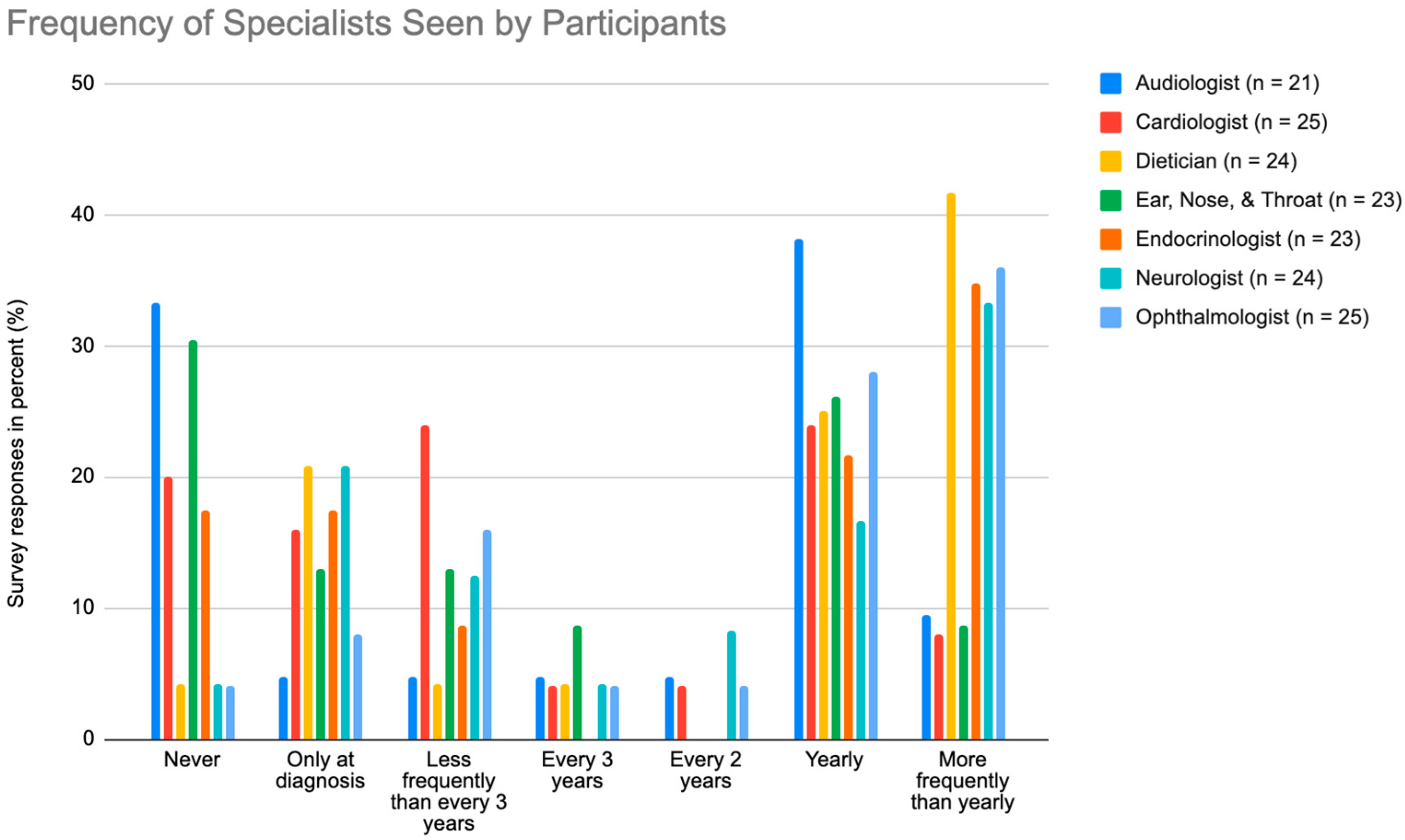
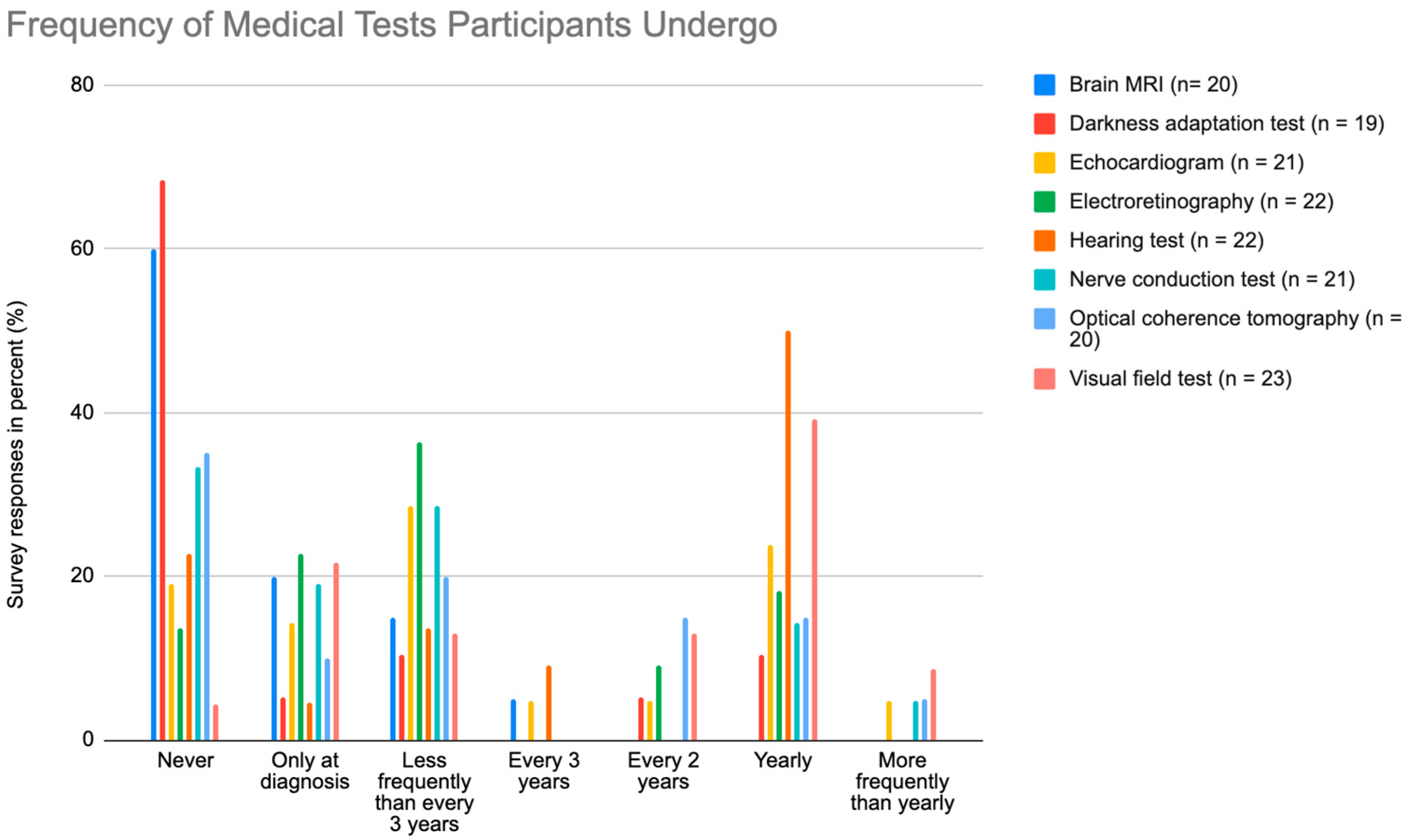
3.4. Specialists and Medical Tests
3.5. Limitations with Health, Activity, and Pain
3.6. Mobility and Exercise
3.7. Modifications in Diet
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jansen, G.A.; Oftnan, R.; Ferdinandusse, S.; Ijlst, L.; Muijsers, A.O.; Skjeldal, O.H.; Stokke, O.; Jakobs, C.; Besley, G.T.; Wraith, J.E.; et al. Refsum disease is caused by mutations in the phytanoyl-CoA hydroxylase gene. Nat. Genet. 1997, 17, 190–193. [Google Scholar] [CrossRef] [PubMed]
- Waterham, H.R.; Wanders, R.J.; Leroy, B.P. Refsum Disease. In GeneReviews; Adam, M.P., Ardinger, H.H., Pagon, R.A., Wallace, S.E., Bean, L.J.H., Gripp, K.W., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 2021; Available online: https://www.ncbi.nlm.nih.gov/books/NBK1353/ (accessed on 14 March 2023).
- Wanders, R.J.; Jansen, G.A.; Skjeldal, O.H. Refsum Disease, Peroxisomes and Phytanic Acid Oxidation: A Review. J. Neuropathol. Exp. Neurol. 2001, 60, 1021–1031. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; De Jesus, O. Refsum Disease. In StatPearls; StatPearls Publishing: Tampa, FL, USA, 2023; Available online: https://www.ncbi.nlm.nih.gov/books/NBK560618/ (accessed on 14 March 2023).
- Pakzad-Vaezi, K.L.; Maberley, D.A.L. Infantile Refsum disease in a young adult: Case presentation and brief review. Retin. Cases Brief Rep. 2014, 8, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Tranchant, C.; Aubourg, P.; Mohr, M.; Rocchiccioli, F.; Zaenker, C.; Warter, J.M. A new peroxisomal disease with impaired phytanic and pipecolic acid oxidation. Neurology 1993, 43, 2044–2048. [Google Scholar] [CrossRef] [PubMed]
- Mandel, H.; Meiron, D.; Schutgens, R.B.; Wanders, R.J.; Berant, M. Infantile refsum disease: Gastrointestinal presentation of a peroxisomal disorder. J. Pediatr. Gastroenterol. Nutr. 1992, 14, 83–85. Available online: https://pubmed.ncbi.nlm.nih.gov/1374125/ (accessed on 14 March 2023). [CrossRef] [PubMed]
- Gibberd, F.B.; Feher, M.D.; Sidey, M.C.; Wierzbicki, A.S. Smell testing: An additional tool for identification of adult Refsum’s disease. J. Neurol. Neurosurg. Psychiatr. 2004, 75, 1334–1336. [Google Scholar] [CrossRef] [PubMed]
- Wierzbicki, A.S.; Lloyd, M.D.; Schofield, C.J.; Feher, M.D.; Gibberd, F.B. Refsum’s disease: A peroxisomal disorder affecting phytanic acid alpha-oxidation. J. Neurochem. 2002, 80, 727–735. [Google Scholar] [CrossRef] [PubMed]
- Gutsche, H.U.; Siegmund, J.B.; Hoppmann, I. Lipapheresis: An immunoglobulin-sparing treatment for Refsum’s disease. Acta Neurol. Scand. 1996, 94, 190–193. [Google Scholar] [CrossRef] [PubMed]
- Gibberd, F.B.; Billimoria, J.D.; Page, N.G.; Retsas, S. Heredopathia atactica polyneuritiformis (refsum’s disease) treated by diet and plasma-exchange. Lancet 1979, 1, 575–578. [Google Scholar] [CrossRef] [PubMed]
- Kohlschütter, A.; Santer, R.; Lukacs, Z.; Altenburg, C.; Kemper, M.J.; Rüther, K. A child with night blindness: Preventing serious symptoms of Refsum disease. J. Child Neurol. 2012, 27, 654–656. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, E.J.; Gibberd, F.B.; Harley, C.; Sidey, M.C.; Feher, M.D.; Wierzbicki, A.S. The effectiveness of long-term dietary therapy in the treatment of adult Refsum disease. J. Neurol. Neurosurg. Psychiatr. 2010, 81, 954–957. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.; Agosta, P.; McKee, C.; Walker, K.; Mazzella, M.; Alamri, A.; Svinarich, D.; Chaudhry, G.R. Human primitive mesenchymal stem cell-derived retinal progenitor cells improved neuroprotection, neurogenesis, and vision in rd12 mouse model of retinitis pigmentosa. Stem Cell Res. Ther. 2022, 13, 148. [Google Scholar] [CrossRef] [PubMed]
- Mukherji, M.; Kershaw, N.J.; MacKinnon, C.H.; Clifton, I.J.; Wierzbicki, A.S.; Schofield, C.J.; Lloyd, M.D. “Chemical co-substrate rescue” of phytanoyl-CoA 2-hydroxylase mutants causing Refsum’s Disease. Chem. Commun. 2001, 972–973. [Google Scholar] [CrossRef]
- Heydari, A.; Ziaee, E.S.; Gazrani, A. Relationship between Awareness of Disease and Adherence to Therapeutic Regimen among Cardiac Patients. Int. J. Community Based Nurs. Midwifery 2015, 3, 23–30. Available online: https://pubmed.ncbi.nlm.nih.gov/25553331/ (accessed on 14 March 2023). [PubMed]
- O’Neal, T.B.; Luther, E.E. Retinitis Pigmentosa. In StatPearls; StatPearls Publishing: Tampa, FL, USA, 2023. [Google Scholar]
- Pozuelo, L.; Tesar, G.; Zhang, J.; Penn, M.; Franco, K.; Jiang, W. Depression and heart disease: What do we know, and where are we headed? Cleve. Clin. J. Med. 2009, 76, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Wang, H. Micrornas, multiple sclerosis, and depression. Int. J. Mol. Sci. 2021, 22, 7802. [Google Scholar] [CrossRef] [PubMed]
- Yohannes, A.M.; Alexopoulos, G.S. Depression and anxiety in patients with COPD. Eur. Respir. Rev. 2014, 23, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Tian, J.; Kang, Y.; Liu, P.; Yu, H. Effect of Physical Activity on Depression in Patients with Parkinson’s Disease: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 6849. [Google Scholar] [CrossRef] [PubMed]
- Saeed, S.A.; Cunningham, K.; Bloch, R.M. Depression and Anxiety Disorders: Benefits of Exercise, Yoga, and Meditation|AAFP. American Family Physician. 15 May 2019. Available online: https://www.aafp.org/pubs/afp/issues/2019/0515/p620.html (accessed on 14 March 2023).
- Global Patient Registry for Refsum Disease. Available online: https://www.defeatadultrefsumeverywhere.org/refsum-patient-registry (accessed on 12 March 2023).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age at survey submission, years | |||
| n = 32 | |||
| Mean | Standard deviation (SD) | 47.4 | 17.2 |
| Median | min, max | 48 | 7, 79 |
| Age at diagnosis, years | |||
| n = 24 | |||
| Mean | SD | 35.5 | 14.5 |
| Median | min, max | 37 | 6, 64 |
| Age at first symptoms, years | |||
| n = 15 | |||
| Mean | SD | 18.5 | 16.8 |
| Median | min, max | 15 | 1, 61 |
| Race | |||
| n = 28 | n | % | |
| White | 26 | 92.9 | |
| Asian | 1 | 3.6 | |
| Other/Refuse to answer | 1 | 3.6 | |
| Sex at birth | |||
| n = 22 | n | % | |
| Male | 8 | 36.4 | |
| Female | 14 | 63.6 | |
| Country of birth | |||
| n = 21 | n | % | |
| United States of America | 5 | 23.8 | |
| Australia | 2 | 9.5 | |
| Canada | 1 | 4.8 | |
| UK | 5 | 23.8 | |
| Netherlands | 1 | 4.8 | |
| South Africa | 2 | 9.5 | |
| Ireland | 1 | 4.8 | |
| Argentina | 1 | 4.8 | |
| Austria | 3 | 14.3 | |
| Which of the following categories best describes the participant’s employment status? | |||
| 27 responses | n | % | |
| Student | 4 | 14.8 | |
| Employed, part-time | 3 | 11.1 | |
| Employed, full-time | 8 | 29.6 | |
| Stay at home parent | 1 | 3.7 | |
| Not employed, looking for work | 0 | 0 | |
| Not employed, not looking for work | 1 | 3.7 | |
| Retired | 4 | 14.8 | |
| Disabled, not able to work | 6 | 22.2 | |
| If not working or working part-time, is this due to Refsum disease? | |||
| n = 18 | n | % | |
| Yes | 11 | 61.1 | |
| No | 7 | 38.9 |
| Age at retinitis pigmentosa diagnosis, years | |||
| n = 23 | |||
| Mean | Standard deviation (SD) | 22.8 | 15.7 |
| Median | min, max | 18 | 2, 61 |
| Phytanic acid levels at diagnosis, µmol/L | |||
| n = 11 | |||
| Mean | Standard deviation (SD) | 689.1 | 1188.2 |
| Median | min, max | 375 | 16, 4243 |
| Gene mutation | |||
| n = 23 | n | % | |
| PHYH | 16 | 69.6 | |
| PEX7 | 1 | 4.3 | |
| Unknown | 6 | 26.1 | |
| Participant received cataract surgery | |||
| n = 25 | n | % | |
| Yes | 16 | 64.0 | |
| No | 9 | 36.0 | |
| Participant’s vision required use of the following: | |||
| n = 24 | n | % | |
| Guide dog | 2 | 8.3 | |
| Long cane | 3 | 12.5 | |
| Signal cane | 5 | 20.8 | |
| None | 14 | 58.3 | |
| Refsum-related hospitalizations | |||
| n = 25 | n | % | |
| None | 12 | 48.0 | |
| Only at diagnosis | 5 | 20.0 | |
| <5 since diagnosis | 5 | 20.0 | |
| >5 since diagnosis | 3 | 12.0 |
| In general, would the participant say his/her health is… | ||
| n = 29 | n | % |
| Poor | 4 | 13.8 |
| Fair | 5 | 17.2 |
| Good | 13 | 44.8 |
| Very good | 6 | 20.7 |
| Excellent | 1 | 3.4 |
| Does the participant’s health currently limit him/her in doing vigorous activities? | ||
| n = 29 | n | % |
| Always | 10 | 34.5 |
| Often | 5 | 17.2 |
| Sometimes | 8 | 27.6 |
| Rarely | 4 | 13.8 |
| Never | 2 | 6.9 |
| What is the participant’s typical daily pain level? | ||
| n = 26 | n | % |
| None | 12 | 46.2 |
| Low (1 to 3) | 11 | 42.3 |
| Moderate (4 to 6) | 3 | 11.5 |
| High (7 to 10) | 0 | 0 |
| How much does pain interfere with the participant’s enjoyment of life? | ||
| n = 29 | n | % |
| Always | 1 | 3.4 |
| Often | 6 | 20.7 |
| Sometimes | 6 | 20.7 |
| Rarely | 10 | 34.5 |
| Never | 6 | 20.7 |
| Is the participant discouraged about having Refsum disease? | ||
| n = 26 | n | % |
| None of the time | 3 | 11.5 |
| A little bit of the time | 7 | 26.9 |
| Some of the time | 10 | 38.5 |
| A good bit of the time | 4 | 15.4 |
| Most of the time | 1 | 3.8 |
| All of the time | 1 | 3.8 |
| Is the participant worried about having Refsum disease? | ||
| n = 26 | n | % |
| None of the time | 3 | 11.5 |
| A little bit of the time | 6 | 23.1 |
| Some of the time | 12 | 46.2 |
| A good bit of the time | 2 | 7.7 |
| Most of the time | 0 | 0 |
| All of the time | 3 | 11.5 |
| How often does the participant feel depressed? | ||
| n = 29 | n | % |
| Always | 2 | 6.9 |
| Often | 2 | 6.9 |
| Sometimes | 6 | 20.7 |
| Rarely | 15 | 51.7 |
| Never | 4 | 13.8 |
| What is the participant’s level of mobility? | ||
| n = 27 | n | % |
| No mobility | 1 | 3.7 |
| Limited (requires full assistance) | 2 | 7.4 |
| Moderate (walk semi-assisted, need a railing to walk up and down stairs) | 8 | 29.6 |
| High (can walk unassisted, very steady, able to walk on uneven surfaces) | 16 | 59.3 |
| How would the participant describe the current level of balance? | ||
| n = 27 | n | % |
| Good | 11 | 40.7 |
| Moderate | 12 | 44.4 |
| Poor | 4 | 14.8 |
| How many days in a week does the participant usually exercise? | ||
| n = 27 | n | % |
| 0 days | 2 | 7.4 |
| 1 day | 1 | 3.7 |
| 2–3 days | 9 | 33.3 |
| 4–6 days | 9 | 33.3 |
| 7 days | 6 | 22.2 |
| Over the course of one week, what is the total number of minutes the participant exercise or does an activity? | ||
| n = 26 | n | % |
| Not active/does not exercise | 1 | 3.8 |
| <30 min | 0 | 0 |
| 31–60 min | 4 | 15.4 |
| 61–90 min | 7 | 26.9 |
| 91–120 min | 2 | 7.7 |
| 121–150 min | 1 | 3.8 |
| >150 min | 11 | 42.3 |
| What is the participant’s maximum exercise intensity level? | ||
| n = 26 | n | % |
| No exercise | 1 | 3.8 |
| Light (yoga, walking) | 15 | 57.7 |
| Moderate (cycling, swimming) | 7 | 26.9 |
| Hard (running, interval training) | 3 | 11.5 |
| Has Refsum disease prevented the participant from doing certain type(s) of exercise? | ||
| n = 25 | n | % |
| Yes | 13 | 52.0 |
| No | 12 | 48.0 |
| How often does the participant have a Phytanic Acid Level done? | ||
| n = 26 | n | % |
| More often than every month | 1 | 3.8 |
| Every month | 2 | 7.7 |
| Every other month | 1 | 3.8 |
| Every 3 months | 3 | 11.5 |
| Every 6 months | 6 | 23.1 |
| Yearly | 7 | 26.9 |
| Never | 1 | 3.8 |
| Unknown | 5 | 19.2 |
| Is the participant on a low-phytanic-acid diet? | ||
| n = 26 | n | % |
| Yes | 25 | 96.2 |
| No | 1 | 3.8 |
| What is the participant’s compliance with the low-phytanic-acid diet within the last year? | ||
| n = 25 | n | % |
| Very strict | 15 | 60 |
| Good | 9 | 36 |
| Intermittent | 1 | 4 |
| Poor | 0 | 0 |
| Not following the diet | 0 | 0 |
| How many times a day does the participant eat, including snacks? | ||
| n = 23 | n | % |
| <3 | 5 | 21.7 |
| 3–6 | 17 | 73.9 |
| >6 | 1 | 4.3 |
| On average, what is the longest period during the day the participant would go without eating between meals/snacks? | ||
| n = 23 | n | % |
| <2 h | 2 | 8.7 |
| 2–3 h | 6 | 26.1 |
| 4–6 h | 13 | 56.5 |
| >6 h | 2 | 8.7 |
| What impact does the low-phytanic-acid diet have on the participant’s quality of life? (e.g., eating out, social activities) | ||
| n = 23 | n | % |
| No impact | 3 | 13 |
| Low impact | 11 | 47.8 |
| Moderate impact | 6 | 26.1 |
| High impact | 3 | 13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.J.; Kim, J.J.; Nausheen, F. Phytanic Acid Intake and Lifestyle Modifications on Quality of Life in Individuals with Adult Refsum Disease: A Retrospective Survey Analysis. Nutrients 2023, 15, 2551. https://doi.org/10.3390/nu15112551
Li JJ, Kim JJ, Nausheen F. Phytanic Acid Intake and Lifestyle Modifications on Quality of Life in Individuals with Adult Refsum Disease: A Retrospective Survey Analysis. Nutrients. 2023; 15(11):2551. https://doi.org/10.3390/nu15112551
Chicago/Turabian StyleLi, Jeffrey J., Jane J. Kim, and Fauzia Nausheen. 2023. "Phytanic Acid Intake and Lifestyle Modifications on Quality of Life in Individuals with Adult Refsum Disease: A Retrospective Survey Analysis" Nutrients 15, no. 11: 2551. https://doi.org/10.3390/nu15112551
APA StyleLi, J. J., Kim, J. J., & Nausheen, F. (2023). Phytanic Acid Intake and Lifestyle Modifications on Quality of Life in Individuals with Adult Refsum Disease: A Retrospective Survey Analysis. Nutrients, 15(11), 2551. https://doi.org/10.3390/nu15112551