


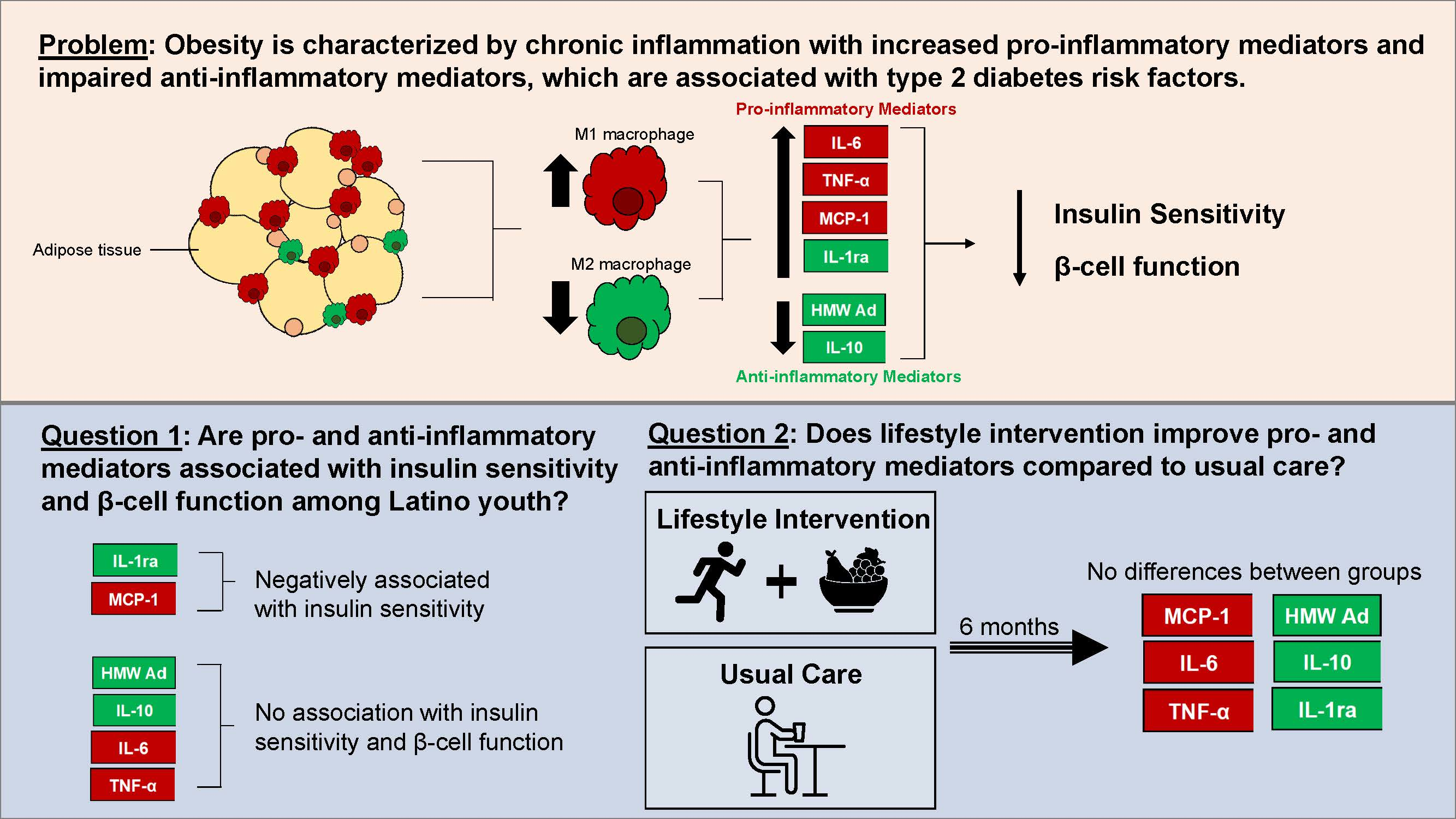
Inflammatory Mediators and Type 2 Diabetes Risk Factors before and in Response to Lifestyle Intervention among Latino Adolescents with Obesity

 ,
,  , , and
, , and
Abstract

1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shapouri-Moghaddam, A.; Mohammadian, S.; Vazini, H.; Taghadosi, M.; Esmaeili, S.-A.; Mardani, F.; Seifi, B.; Mohammadi, A.; Afshari, J.T.; Sahebkar, A. Macrophage plasticity, polarization, and function in health and disease. J. Cell. Physiol. 2018, 233, 6425–6440. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.-C.; Lee, J. Cellular and molecular players in adipose tissue inflammation in the development of obesity-induced insulin resistance. Biochim. Biophys. Acta BBA Mol. Basis Dis. 2013, 1842, 446–462. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Chen, L.; Zhang, Y.; Zhang, W.J.; Xu, W.; Qin, Y.; Xu, J.; Zou, D. TLR4 is required for the obesity-induced pancreatic beta cell dysfunction. Acta Biochim. Biophys. Sin. 2013, 45, 1030–1038. [Google Scholar] [CrossRef] [PubMed]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M.; Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef]
- Mather, K.J.; Funahashi, T.; Matsuzawa, Y.; Edelstein, S.; Bray, G.A.; Kahn, S.E.; Crandall, J.; Marcovina, S.; Goldstein, B.; Goldberg, R.; et al. Adiponectin, Change in Adiponectin, and Progression to Diabetes in the Diabetes Prevention Program. Diabetes 2008, 57, 980–986. [Google Scholar] [CrossRef]
- Paltoglou, G.; Schoina, M.; Valsamakis, G.; Salakos, N.; Avloniti, A.; Chatzinikolaou, A.; Margeli, A.; Skevaki, C.; Papagianni, M.; Kanaka-Gantenbein, C.; et al. Interrelations among the adipocytokines leptin and adiponectin, oxidative stress and aseptic inflammation markers in pre- and early-pubertal normal-weight and obese boys. Endocrine 2017, 55, 925–933. [Google Scholar] [CrossRef]
- Breslin, W.L.; Johnston, C.A.; Strohacker, K.; Carpenter, K.C.; Davidson, T.R.; Moreno, J.P.; Foreyt, J.P.; McFarlin, B.K. Obese Mexican American Children Have Elevated MCP-1, TNF-α, Monocyte Concentration, and Dyslipidemia. Pediatrics 2012, 129, e1180–e1186. [Google Scholar] [CrossRef]
- Chang, C.-J.; Jian, D.-Y.; Lin, M.-W.; Zhao, J.-Z.; Ho, L.-T.; Juan, C.-C. Evidence in Obese Children: Contribution of Hyperlipidemia, Obesity-Inflammation, and Insulin Sensitivity. PLoS ONE 2015, 10, e0125935. [Google Scholar] [CrossRef]
- Kanda, H.; Tateya, S.; Tamori, Y.; Kotani, K.; Hiasa, K.-I.; Kitazawa, R.; Kitazawa, S.; Miyachi, H.; Maeda, S.; Egashira, K.; et al. MCP-1 contributes to macrophage infiltration into adipose tissue, insulin resistance, and hepatic steatosis in obesity. J. Clin. Investig. 2006, 116, 1494–1505. [Google Scholar] [CrossRef]
- Parish, R.C.; Todman, S.; Jain, S.K. Resting Heart Rate Variability, Inflammation, and Insulin Resistance in Overweight and Obese Adolescents. Metab. Syndr. Relat. Disord. 2016, 14, 291–297. [Google Scholar] [CrossRef]
- Daniele, G.; Mendoza, R.G.; Winnier, D.; Fiorentino, T.V.; Pengou, Z.; Cornell, J.; Andreozzi, F.; Jenkinson, C.; Cersosimo, E.; Federici, M.; et al. The inflammatory status score including IL-6, TNF-α, osteopontin, fractalkine, MCP-1 and adiponectin underlies whole-body insulin resistance and hyperglycemia in type 2 diabetes mellitus. Acta Diabetol. 2013, 51, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Reyna, S.M.; Ghosh, S.; Tantiwong, P.; Meka, C.S.R.; Eagan, P.; Jenkinson, C.P.; Cersosimo, E.; DeFronzo, R.A.; Coletta, D.K.; Sriwijitkamol, A.; et al. Elevated Toll-Like Receptor 4 Expression and Signaling in Muscle from Insulin-Resistant Subjects. Diabetes 2008, 57, 2595–2602. [Google Scholar] [CrossRef] [PubMed]
- Piemonti, L.; Leone, B.E.; Nano, R.; Saccani, A.; Monti, P.; Maffi, P.; Bianchi, G.; Sica, A.; Peri, G.; Melzi, R.; et al. Human Pancreatic Islets Produce and Secrete MCP-1/CCL2: Relevance in Human Islet Transplantation. Diabetes 2002, 51, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Xiao, T.; Peng, X.; Li, G.; Hu, F. APPLs: More than just adiponectin receptor binding proteins. Cell. Signal. 2017, 32, 76–84. [Google Scholar] [CrossRef]
- Acosta, J.R.; Tavira, B.; Douagi, I.; Kulyté, A.; Arner, P.; Rydén, M.; Laurencikiene, J. Human-Specific Function of IL-10 in Adipose Tissue Linked to Insulin Resistance. J. Clin. Endocrinol. Metab. 2019, 104, 4552–4562. [Google Scholar] [CrossRef]
- Chetboun, M.; Abitbol, G.; Rozenberg, K.; Rozenfeld, H.; Deutsch, A.; Sampson, S.R.; Rosenzweig, T. Maintenance of redox state and pancreatic beta-cell function: Role of leptin and adiponectin. J. Cell. Biochem. 2012, 113, 1966–1976. [Google Scholar] [CrossRef]
- Dorneles, G.P.; Haddad, D.O.; Fagundes, V.O.; Vargas, B.K.; Kloecker, A.; Romão, P.R.; Peres, A. High intensity interval exercise decreases IL-8 and enhances the immunomodulatory cytokine interleukin-10 in lean and overweight–obese individuals. Cytokine 2016, 77, 1–9. [Google Scholar] [CrossRef]
- Balagopal, P.; George, D.; Yarandi, H.; Funanage, V.; Bayne, E. Reversal of Obesity-Related Hypoadiponectinemia by Lifestyle Intervention: A Controlled, Randomized Study in Obese Adolescents. J. Clin. Endocrinol. Metab. 2005, 90, 6192–6197. [Google Scholar] [CrossRef]
- Seppä, S.; Tenhola, S.; Voutilainen, R. Serum IL-1 Receptor Antagonist Concentrations Associate with Unfavorable Metabolic Features in 12-year-old Children. J. Endocr. Soc. 2018, 2, 870–881. [Google Scholar] [CrossRef]
- Stoppa-Vaucher, S.; Dirlewanger, M.A.; Meier, C.A.; De Moerloose, P.; Reber, G.; Roux-Lombard, P.; Combescure, C.; Saudan, S.; Schwitzgebel, V.M. Inflammatory and Prothrombotic States in Obese Children of European Descent. Obesity 2012, 20, 1662–1668. [Google Scholar] [CrossRef]
- Darragh, J.; Ananieva, O.; Courtney, A.; Elcombe, S.; Arthur, J.S.C. MSK1 regulates the transcription of IL-1ra in response to TLR activation in macrophages. Biochem. J. 2010, 425, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Petersen, A.M.W.; Pedersen, B.K. The anti-inflammatory effect of exercise. J. Appl. Physiol. 2005, 98, 1154–1162. [Google Scholar] [CrossRef] [PubMed]
- Della Gatta, P.A.; Garnham, A.P.; Peake, J.M.; Cameron-Smith, D. Effect of exercise training on skeletal muscle cytokine expression in the elderly. Brain Behav. Immun. 2014, 39, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Annibalini, G.; Lucertini, F.; Agostini, D.; Vallorani, L.; Gioacchini, A.; Barbieri, E.; Guescini, M.; Casadei, L.; Passalia, A.; Del Sal, M.; et al. Concurrent Aerobic and Resistance Training Has Anti-Inflammatory Effects and Increases Both Plasma and Leukocyte Levels of IGF-1 in Late Middle-Aged Type 2 Diabetic Patients. Oxidative Med. Cell. Longev. 2017, 2017, 3937842. [Google Scholar] [CrossRef] [PubMed]
- Fatouros, I.G.; Tournis, S.; Leontsini, D.; Jamurtas, A.Z.; Sxina, M.; Thomakos, P.; Manousaki, M.; Douroudos, I.; Taxildaris, K.; Mitrakou, A. Leptin and Adiponectin Responses in Overweight Inactive Elderly following Resistance Training and Detraining Are Intensity Related. J. Clin. Endocrinol. Metab. 2005, 90, 5970–5977. [Google Scholar] [CrossRef] [PubMed]
- Da Luz, G.; Frederico, M.J.S.; Da Silva, S.; Vitto, M.F.; Cesconetto, P.A.; Pinho, R.; Pauli, J.R.; da Silva, A.S.R.; Cintra, D.; Ropelle, E.; et al. Endurance exercise training ameliorates insulin resistance and reticulum stress in adipose and hepatic tissue in obese rats. Eur. J. Appl. Physiol. 2011, 111, 2015–2023. [Google Scholar] [CrossRef]
- Dietary Guidelines Advisory Committee DePS. Dietary Patterns and Risk of Cardiovascular Disease: A Systematic Review; USDA Nutrition Evidence Systematic Review: Alexandria, VA, USA, 2020. [Google Scholar]
- Lenighan, Y.M.; McNulty, B.; Roche, H.M. Dietary fat composition: Replacement of saturated fatty acids with PUFA as a public health strategy, with an emphasis on α-linolenic acid. Proc. Nutr. Soc. 2019, 78, 234–245. [Google Scholar] [CrossRef]
- Martínez-Fernández, L.; Laiglesia, L.M.; Huerta, A.E.; Martínez, J.A.; Moreno-Aliaga, M.J. Omega-3 fatty acids and adipose tissue function in obesity and metabolic syndrome. Prostaglandins Other Lipid Mediat. 2015, 121 Pt A, 24–41. [Google Scholar] [CrossRef]
- Hosseini, B.; Berthon, B.S.; Saedisomeolia, A.; Starkey, M.R.; Collison, A.; Wark, P.A.B.; Wood, L.G. Effects of fruit and vegetable consumption on inflammatory biomarkers and immune cell populations: A systematic literature review and meta-analysis. Am. J. Clin. Nutr. 2018, 108, 136–155. [Google Scholar] [CrossRef]
- Balagopal, P.; George, D.; Patton, N.; Yarandi, H.; Roberts, W.L.; Bayne, E.; Gidding, S. Lifestyle-only intervention attenuates the inflammatory state associated with obesity: A randomized controlled study in adolescents. J. Pediatr. 2005, 146, 342–348. [Google Scholar] [CrossRef]
- Cambuli, V.M.; Musiu, M.C.; Incani, M.; Paderi, M.; Serpe, R.; Marras, V.; Cossu, E.; Cavallo, M.G.; Mariotti, S.; Loche, S.; et al. Assessment of Adiponectin and Leptin as Biomarkers of Positive Metabolic Outcomes after Lifestyle Intervention in Overweight and Obese Children. J. Clin. Endocrinol. Metab. 2008, 93, 3051–3057. [Google Scholar] [CrossRef] [PubMed]
- Mayerhofer, E.; Ratzinger, F.; Kienreich, N.E.; Stiel, A.; Witzeneder, N.; Schrefl, E.; Greiner, G.; Wegscheider, C.; Graf, I.; Schmetterer, K.; et al. A Multidisciplinary Intervention in Childhood Obesity Acutely Improves Insulin Resistance and Inflammatory Markers Independent from Body Composition. Front. Pediatr. 2020, 8, 52. [Google Scholar] [CrossRef] [PubMed]
- Rambhojan, C.; Bouaziz-Amar, E.; Larifla, L.; Deloumeaux, J.; Clepier, J.; Plumasseau, J.; Lacorte, J.-M.; Foucan, L. Ghrelin, adipokines, metabolic factors in relation with weight status in school-children and results of a 1-year lifestyle intervention program. Nutr. Metab. 2015, 12, 43. [Google Scholar] [CrossRef]
- Soltero, E.G.; Konopken, Y.P.; Olson, M.L.; Keller, C.S.; Castro, F.G.; Williams, A.N.; Patrick, D.L.; Ayers, S.; Hu, H.H.; Sandoval, M.; et al. Preventing diabetes in obese Latino youth with prediabetes: A study protocol for a randomized controlled trial. BMC Public Health 2017, 17, 261. [Google Scholar] [CrossRef]
- Giannini, C.; Weiss, R.; Cali, A.; Bonadonna, R.; Santoro, N.; Pierpont, B.; Shaw, M.; Caprio, S. Evidence for early defects in insulin sensitivity and secretion before the onset of glucose dysregulation in obese youths: A longitudinal study. Diabetes 2012, 61, 606–614. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Liu, F. Regulation of adiponectin multimerization, signaling and function. Best Pract. Res. Clin. Endocrinol. Metab. 2014, 28, 25–31. [Google Scholar] [CrossRef]
- Yeckel, C.W.; Weiss, R.; Dziura, J.; Taksali, S.E.; Dufour, S.; Burgert, T.S.; Tamborlane, W.V.; Caprio, S. Validation of Insulin Sensitivity Indices from Oral Glucose Tolerance Test Parameters in Obese Children and Adolescents. J. Clin. Endocrinol. Metab. 2004, 89, 1096–1101. [Google Scholar] [CrossRef]
- Sjaarda, L.G.; Bacha, F.; Lee, S.; Tfayli, H.; Andreatta, E.; Arslanian, S. Oral Disposition Index in Obese Youth from Normal to Prediabetes to Diabetes: Relationship to Clamp Disposition Index. J. Pediatr. 2012, 161, 51–57. [Google Scholar] [CrossRef]
- Peña, A.; Olson, M.L.; Hooker, E.; Ayers, S.L.; Castro, F.G.; Patrick, D.L.; Corral, L.; Lish, E.; Knowler, W.C.; Shaibi, G.Q. Effects of a Diabetes Prevention Program on Type 2 Diabetes Risk Factors and Quality of Life Among Latino Youths with Prediabetes: A Randomized Clinical Trial. JAMA Netw. Open 2022, 5, e2231196. [Google Scholar] [CrossRef]
- Savoye, M.; Caprio, S.; Dziura, J.; Camp, A.; Germain, G.; Summers, C.; Li, F.; Shaw, M.; Nowicka, P.; Kursawe, R.; et al. Reversal of Early Abnormalities in Glucose Metabolism in Obese Youth: Results of an Intensive Lifestyle Randomized Controlled Trial. Diabetes Care 2014, 37, 317–324. [Google Scholar] [CrossRef]
- Soltero, E.G.; Olson, M.L.; Williams, A.N.; Konopken, Y.P.; Castro, F.G.; Arcoleo, K.J.; Keller, C.S.; Patrick, D.L.; Ayers, S.L.; Barraza, E.; et al. Effects of a Community-Based Diabetes Prevention Program for Latino Youth with Obesity: A Randomized Controlled Trial. Obesity 2018, 26, 1856–1865. [Google Scholar] [CrossRef] [PubMed]
- Akcan, N.; Obaid, M.; Salem, J.; Bundak, R. Evidence in obese children: Contribution of tri-ponderal mass index or body mass index to dyslipidemia, obesity-inflammation, and insulin sensitivity. J. Pediatr. Endocrinol. Metab. 2019, 33, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Morishita, R.; Franco, M.D.C.; de Souza, F.I.S.; Solé, D.; Puccini, R.F.; Strufaldi, M.W.L. Body mass index, adipokines and insulin resistance in asthmatic children and adolescents. J. Asthma 2016, 53, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Westwell-Roper, C.Y.; Chehroudi, C.A.; Denroche, H.; Courtade, J.A.; Ehses, J.; Verchere, C.B. IL-1 mediates amyloid-associated islet dysfunction and inflammation in human islet amyloid polypeptide transgenic mice. Diabetologia 2014, 58, 575–585. [Google Scholar] [CrossRef] [PubMed]
- Orlando, A.; Nava, E.; Giussani, M.; Genovesi, S. Adiponectin and Cardiovascular Risk. From Pathophysiology to Clinic: Focus on Children and Adolescents. Int. J. Mol. Sci. 2019, 20, 3228. [Google Scholar] [CrossRef]
- Cruz, M.; García-Macedo, R.; García-Valerio, Y.; Gutiérrez, M.; Medina-Navarro, R.; Duran, G.; Wacher, N.; Kumate, J. Low Adiponectin Levels Predict Type 2 Diabetes in Mexican Children. Diabetes Care 2004, 27, 1451–1453. [Google Scholar] [CrossRef] [PubMed]
- Arslanian, S.; El Ghormli, L.; Bacha, F.; Caprio, S.; Goland, R.; Haymond, M.W.; Levitsky, L.; Nadeau, K.J.; White, N.H.; Willi, S.M.; et al. Adiponectin, Insulin Sensitivity, β-Cell Function, and Racial/Ethnic Disparity in Treatment Failure Rates in TODAY. Diabetes Care 2016, 40, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Dixon, D.; Goldberg, R.; Schneiderman, N.; Delamater, A. Gender differences in TNF-α levels among obese vs nonobese Latino children. Eur. J. Clin. Nutr. 2004, 58, 696–699. [Google Scholar] [CrossRef] [PubMed]
- Hosick, P.A.; McMurray, R.G.; Hackney, A.; Battaglini, C.L.; Combs, T.P.; Harrell, J.S. Resting IL-6 and TNF-α level in children of different weight and fitness status. Pediatr. Exerc. Sci. 2013, 25, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Reinehr, T.; Stoffel-Wagner, B.; Roth, C.L.; Andler, W. High-sensitive C-reactive protein, tumor necrosis factor α, and cardiovascular risk factors before and after weight loss in obese children. Metabolism 2005, 54, 1155–1161. [Google Scholar] [CrossRef]
- Reinehr, T.; Karges, B.; Meissner, T.; Wiegand, S.; Stoffel-Wagner, B.; Holl, R.W.; Woelfle, J. Inflammatory Markers in Obese Adolescents with Type 2 Diabetes and Their Relationship to Hepatokines and Adipokines. J. Pediatr. 2016, 173, 131–135. [Google Scholar] [CrossRef]
- Nemet, D.; Wang, P.; Funahashi, T.; Matsuzawa, Y.; Tanaka, S.; Engelman, L.; Cooper, D.M. Adipocytokines, Body Composition, and Fitness in Children. Pediatr. Res. 2003, 53, 148–152. [Google Scholar] [CrossRef] [PubMed]
- McFarlin, B.K.; Johnston, C.A.; Tyler, C.; Hutchison, A.T.; Kueht, M.L.; Reeves, R.; Foreyt, J.P. Inflammatory markers are elevated in overweight Mexican-American children. Pediatr. Obes. 2007, 2, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Himani, K.; Vani, G.; Mishra, S.; Mahdi, A.A.; Shally, A. Association of serum Interleukin-10, omentin-1 and visfatin concentration with metabolic risk factors in obese children. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 2069–2074. [Google Scholar] [CrossRef] [PubMed]
- Aguilar, T.; Nava, G.M.; Olvera-Ramírez, A.M.; Ronquillo, D.; Camacho, M.; Zavala, G.A.; Caamaño, M.C.; Acevedo-Whitehouse, K.; Rosado, J.L.; García, O.P. Gut Bacterial Families Are Associated with Body Composition and Metabolic Risk Markers in School-Aged Children in Rural Mexico. Child. Obes. 2020, 16, 358–366. [Google Scholar] [CrossRef]
- Chang, J.-S.; Li, Y.-L.; Lu, C.-H.; Owaga, E.; Chen, W.-Y.; Chiou, H.Y. Interleukin-10 as a potential regulator of hepcidin homeostasis in overweight and obese children: A cross-sectional study in Taiwan. Nutrition 2014, 30, 1165–1170. [Google Scholar] [CrossRef]
- Selvaraju, V.; Babu, J.R.; Geetha, T. Association of salivary C-reactive protein with the obesity measures and markers in children. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 1239–1247. [Google Scholar] [CrossRef]
- Black, D.D. Impact of Bariatric Surgery on Adipose Tissue and Liver Inflammation in Adolescents with Nonalcoholic Steatohepatitis. J. Pediatr. 2019, 216, 7–9. [Google Scholar] [CrossRef]
- Kelly, A.S.; Ryder, J.; Marlatt, K.L.; Rudser, K.D.; Jenkins, T.; Inge, T.H. Changes in inflammation, oxidative stress and adipokines following bariatric surgery among adolescents with severe obesity. Int. J. Obes. 2015, 40, 275–280. [Google Scholar] [CrossRef]
- Frühbeck, G.; Catalán, V.; Ramírez, B.; Valentí, V.; Becerril, S.; Rodríguez, A.; Moncada, R.; Baixauli, J.; Silva, C.; Escalada, J.; et al. Serum Levels of IL-1 RA Increase with Obesity and Type 2 Diabetes in Relation to Adipose Tissue Dysfunction and are Reduced After Bariatric Surgery in Parallel to Adiposity. J. Inflamm. Res. 2022, 15, 1331–1345. [Google Scholar] [CrossRef]
- Roth, C.L.; Kratz, M.; Ralston, M.M.; Reinehr, T. Changes in adipose-derived inflammatory cytokines and chemokines after successful lifestyle intervention in obese children. Metabolism 2011, 60, 445–452. [Google Scholar] [CrossRef] [PubMed]
- Hamman, R.F.; Wing, R.R.; Edelstein, S.L.; Lachin, J.M.; Bray, G.A.; Delahanty, L.; Hoskin, M.; Kriska, A.M.; Mayer-Davis, E.J.; Pi-Sunyer, X.; et al. Effect of Weight Loss with Lifestyle Intervention on Risk of Diabetes. Diabetes Care 2006, 29, 2102–2107. [Google Scholar] [CrossRef] [PubMed]
- Gokulakrishnan, K.; Ranjani, H.; Weber, M.B.; Pandey, G.K.; Anjana, R.M.; Balasubramanyam, M.; Prabhakaran, D.; Tandon, N.; Narayan, K.M.; Mohan, V. Effect of lifestyle improvement program on the biomarkers of adiposity, inflammation and gut hormones in overweight/obese Asian Indians with prediabetes. Acta Diabetol. 2017, 54, 843–852. [Google Scholar] [CrossRef]
- Miller, G.D.; Isom, S.; Morgan, T.M.; Vitolins, M.Z.; Blackwell, C.; Brosnihan, K.B.; Diz, D.I.; Katula, J.; Goff, D. Effects of a community-based weight loss intervention on adipose tissue circulating factors. Diabetes Metab. Syndr. Clin. Res. Rev. 2014, 8, 205–211. [Google Scholar] [CrossRef]
- Reinehr, T. Lifestyle intervention in childhood obesity: Changes and challenges. Nat. Rev. Endocrinol. 2013, 9, 607–614. [Google Scholar] [CrossRef]
- Barry, J.C.; Simtchouk, S.; Durrer, C.; Jung, M.E.; Little, J.P. Short-Term Exercise Training Alters Leukocyte Chemokine Receptors in Obese Adults. Med. Sci. Sport. Exerc. 2017, 49, 1631–1640. [Google Scholar] [CrossRef] [PubMed]
- Fischer, C.P. Interleukin-6 in acute exercise and training: What is the biological relevance? Exerc. Immunol. Rev. 2006, 12, 6–33. [Google Scholar]
- Mendham, A.E.; Donges, C.E.; Liberts, E.A.; Duffield, R. Effects of mode and intensity on the acute exercise-induced IL-6 and CRP responses in a sedentary, overweight population. Eur. J. Appl. Physiol. 2010, 111, 1035–1045. [Google Scholar] [CrossRef]
- Pedersen, B.K. Anti-inflammatory effects of exercise: Role in diabetes and cardiovascular disease. Eur. J. Clin. Investig. 2017, 47, 600–611. [Google Scholar] [CrossRef]
- Lee, M.K.; Jekal, Y.; Im, J.-A.; Kim, E.; Lee, S.H.; Park, J.-H.; Chu, S.H.; Chung, K.-M.; Lee, H.C.; Oh, E.G.; et al. Reduced serum vaspin concentrations in obese children following short-term intensive lifestyle modification. Clin. Chim. Acta 2010, 411, 381–385. [Google Scholar] [CrossRef]
- Roche, J.; Isacco, L.; Perret, F.; Dumoulin, G.; Gillet, V.; Mougin, F. Beneficial effects of a lifestyle intervention program on C-reactive protein: Impact of cardiorespiratory fitness in obese adolescents with sleep disturbances. Am. J. Physiol. Integr. Comp. Physiol. 2019, 316, R376–R386. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, M.; Nonas, C.; Weil, R.; Horlick, M.; Fennoy, I.; Vargas, I.; Kringas, P.; The El Camino Diabetes Prevention Group. School-Based Intervention Acutely Improves Insulin Sensitivity and Decreases Inflammatory Markers and Body Fatness in Junior High School Students. J. Clin. Endocrinol. Metab. 2006, 92, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Lira, F.S.; Rosa, J.C.; dos Santos, R.V.; Venancio, D.P.; Carnier, J.; Sanches, P.D.L.; Nascimento, C.M.O.D.; de Piano, A.; Tock, L.; Tufik, S.; et al. Visceral fat decreased by long-term interdisciplinary lifestyle therapy correlated positively with interleukin-6 and tumor necrosis factor–α and negatively with adiponectin levels in obese adolescents. Metabolism 2011, 60, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Roberts, C.K.; Izadpanah, A.; Angadi, S.S.; Barnard, R.J. Effects of an intensive short-term diet and exercise intervention: Comparison between normal-weight and obese children. Am. J. Physiol. Integr. Comp. Physiol. 2013, 305, R552–R557. [Google Scholar] [CrossRef]
- Park, T.-G.; Hong, H.-R.; Lee, J.; Kang, H.-S. Lifestyle plus Exercise Intervention Improves Metabolic Syndrome Markers without Change in Adiponectin in Obese Girls. Ann. Nutr. Metab. 2007, 51, 197–203. [Google Scholar] [CrossRef]
- Chae, H.-W.; Kwon, Y.-N.; Rhie, Y.-J.; Kim, H.-S.; Kim, Y.-S.; Paik, I.-Y.; Suh, S.-H.; Kim, D.-H. Effects of a Structured Exercise Program on Insulin Resistance, Inflammatory Markers and Physical Fitness in Obese Korean Children. J. Pediatr. Endocrinol. Metab. 2010, 23, 1065–1072. [Google Scholar] [CrossRef]
- Richter, E.A.; Hargreaves, M. Exercise, GLUT4, and Skeletal Muscle Glucose Uptake. Physiol. Rev. 2013, 93, 993–1017. [Google Scholar] [CrossRef]
- Rains, J.L.; Jain, S.K. Oxidative stress, insulin signaling, and diabetes. Free Radic. Biol. Med. 2011, 50, 567–575. [Google Scholar] [CrossRef]
- McMurray, F.; Patten, D.A.; Harper, M.-E. Reactive Oxygen Species and Oxidative Stress in Obesity-Recent Findings and Empirical Approaches. Obesity 2016, 24, 2301–2310. [Google Scholar] [CrossRef]
- Capurso, C.; Capurso, A. From excess adiposity to insulin resistance: The role of free fatty acids. Vasc. Pharmacol. 2012, 57, 91–97. [Google Scholar] [CrossRef]
- Liu, X.-H.; Bauman, W.A.; Cardozo, C.P. Myostatin inhibits glucose uptake via suppression of insulin-dependent and -independent signaling pathways in myoblasts. Physiol. Rep. 2018, 6, e13837. [Google Scholar] [CrossRef] [PubMed]
- Caprio, S.; Perry, R.; Kursawe, R. Adolescent Obesity and Insulin Resistance: Roles of Ectopic Fat Accumulation and Adipose Inflammation. Gastroenterology 2017, 152, 1638–1646. [Google Scholar] [CrossRef]
- Rodríguez-Rodríguez, E.; Salas-González, M.D.; Ortega, R.M.; López-Sobaler, A.M. Leukocytes and Neutrophil–Lymphocyte Ratio as Indicators of Insulin Resistance in Overweight/Obese School-Children. Front. Nutr. 2022, 8, 811081. [Google Scholar] [CrossRef] [PubMed]
- Caprio, S. The Oral Disposition Index: A Valuable Estimate of β-Cell Function in Obese Youth. J. Pediatr. 2012, 161, 3–4. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Parameter | All (n = 64) | INT (n = 40) | UCC (n = 24) | p-Value |
|---|---|---|---|---|
| Age, y | 13.3 ± 1.4 | 13.4 ± 1.4 | 13.2 ± 1.4 | 0.482 |
| Female, n (%) | 26 (40.6%) | 16 (40.0%) | 9 (37.5%) | 0.843 |
| BMI, kg/m2 | 32.7 ± 4.8 | 32.1 ± 3.7 | 33.7 ± 6.3 | 0.19 |
| BMI-z | 2.2 ± 0.3 | 2.2 ± 0.3 | 2.3 ± 0.4 | 0.275 |
| Fat mass, kg | 37.6 ± 9.4 | 36.2 ± 7.1 | 40.0 ± 12.2 | 0.102 |
| WBISI | 1.7 ± 1.1 | 1.8 ± 1.3 | 1.6 ± 1.0 | 0.417 |
| oDI | 4.5 ± 2.5 | 4.8 ± 2.5 | 4.0 ± 2.4 | 0.15 |
| IL-6, pg/mL | 2.3 ± 1.9 | 1.9 ± 1.7 | 2.8 ± 2.2 | 0.091 |
| TNF-α, pg/mL | 1.7 ± 0.5 | 1.7 ± 0.5 | 1.7 ± 0.4 | 0.983 |
| MCP-1, pg/mL | 644 ± 271 | 646 ± 250 | 641 ± 308 | 0.981 |
| HMW Adpn, ug/mL | 1.5 ± 1.7 | 1.7 ± 0.8 | 1.3 ± 0.6 | 0.112 |
| IL-10, pg/mL | 0.6 ± 1.0 | 0.6 ± 1.2 | 0.6 ± 0.5 | 0.885 |
| IL-1ra, pg/mL | 1150 ± 920 | 1003 ± 729 | 1394 ± 1148 | 0.088 |
| Dependent Variables | ||||||
|---|---|---|---|---|---|---|
| WBISI | oDI | |||||
| Predictors | β | SE | p-Value | β | SE | p-Value |
| IL-6 | −0.06 | 0.15 | 0.677 | 0.14 | 0.20 | 0.488 |
| TNF-α | −0.5 | 0.5 | 0.300 | 1.2 | 0.8 | 0.126 |
| MCP-1 | −0.12 | 0.05 | 0.027 | −0.013 | 0.010 | 0.165 |
| HMW Adpn | 0.1 | 0.1 | 0.364 | 0.5 | 0.4 | 0.199 |
| IL-10 | 0.3 | 0.4 | 0.786 | −0.5 | 0.4 | 0.200 |
| IL-1ra | −0.03 | 0.01 | 0.005 | −0.007 | 0.004 | 0.074 |
| UC (n = 24) | INT (n = 40) | Treatment Effect | |||||
|---|---|---|---|---|---|---|---|
| Parameters | T1 | T2 | Within-Group Effect p-Value | T1 | T2 | Within-Group Effect p-Value | ΔT2-T1 (95%CI) p-Value |
| IL-6 | 2.8 ± 0.4 | 2.4 ± 0.2 | 0.236 | 1.9 ± 0.3 | 1.8 ± 0.2 | 0.675 | 0.2 (−0.6, 1.1) 0.574 |
| TNF-α | 1.7 ± 0.1 | 1.7 ± 0.1 | 0.926 | 1.7 ± 0.1 | 1.4 ± 0.1 | 0.067 | −0.1 (−0.3, 0.1) 0.223 |
| MCP-1 | 641 ± 51 | 603 ± 49 | 0.167 | 646 ± 36 | 914 ± 228 | 0.239 | 30.7 (−143.3, 756.9) 0.182 |
| HMW Adpn | 1.28 ± 0.11 | 1.21 ± 0.11 | 0.303 | 1.67 ± 0.12 | 1.42 ± 0.11 | 0.001 | −0.18 (−0.37, 0.02) 0.079 |
| IL-10 | 0.6 ± 0.11 | 0.5 ± 0.09 | 0.496 | 0.6 ± 0.18 | 0.3 ± 0.03 | 0.096 | −0.2 (−0.7, 0.2) 0.351 |
| IL-1ra | 1394 ± 219 | 1230 ± 193 | 0.235 | 1003 ± 110 | 843 ± 95 | 0.086 | 0.4 (−325.3, 326.1) 0.981 |
| WBISI | 1.6 ± 0.2 | 2.8 ± 0.5 | 0.002 | 1.8 ± 0.2 | 2.6 ± 0.4 | 0.005 | −0.4 (−1.4, 0.5) 0.352 |
| oDI | 4.0 ± 0.5 | 3.9 ± 0.5 | 0.781 | 4.8 ± 0.4 | 5.4 ± 0.5 | 0.323 | 0.7 (−0.7, 2.1) 0.345 |
| Weight | 89 ± 4 | 92 ± 4 | <0.001 | 86 ± 2 | 88 ± 2 | 0.006 | −1.3 (−3.2, 0.5) 0.143 |
| BMI | 33.7 ± 1.1 | 34.0 ± 1.2 | 0.200 | 32.1 ± 0.5 | 32.1 ± 0.6 | 0.805 | −0.3 (−0.9, 0.4) 0.426 |
| BMI-z | 2.28 ± 0.07 | 2.24 ± 0.09 | 0.245 | 2.19 ± 0.04 | 2.15 ± 0.05 | 0.059 | −0.009 (−0.07, 0.68) 0.796 |
| Fat Mass | 40.0 ± 2.3 | 40.5 ± 2.4 | 0.393 | 36.2 ± 1.0 | 35.3 ± 1.1 | 0.094 | −1.4 (−2.9, 0.2) 0.085 |
| Body Fat % | 47.0 ± 0.9 | 46.3 ± 1.0 | 0.055 | 44.5 ± 0.6 | 42.7 ± 0.7 | <0.001 | −1.0 (0.02, 2.078) 0.045 |
| Lean Mass | 42 ± 1 | 44 ± 1 | <0.001 | 43 ± 1 | 45 ± 1 | <0.001 | 0.1 (−0.08, 0.06) 0.840 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peña, A.; Olson, M.L.; Ayers, S.L.; Sears, D.D.; Vega-López, S.; Colburn, A.T.; Shaibi, G.Q. Inflammatory Mediators and Type 2 Diabetes Risk Factors before and in Response to Lifestyle Intervention among Latino Adolescents with Obesity. Nutrients 2023, 15, 2442. https://doi.org/10.3390/nu15112442
Peña A, Olson ML, Ayers SL, Sears DD, Vega-López S, Colburn AT, Shaibi GQ. Inflammatory Mediators and Type 2 Diabetes Risk Factors before and in Response to Lifestyle Intervention among Latino Adolescents with Obesity. Nutrients. 2023; 15(11):2442. https://doi.org/10.3390/nu15112442
Chicago/Turabian StylePeña, Armando, Micah L. Olson, Stephanie L. Ayers, Dorothy D. Sears, Sonia Vega-López, Abigail T. Colburn, and Gabriel Q. Shaibi. 2023. "Inflammatory Mediators and Type 2 Diabetes Risk Factors before and in Response to Lifestyle Intervention among Latino Adolescents with Obesity" Nutrients 15, no. 11: 2442. https://doi.org/10.3390/nu15112442
APA StylePeña, A., Olson, M. L., Ayers, S. L., Sears, D. D., Vega-López, S., Colburn, A. T., & Shaibi, G. Q. (2023). Inflammatory Mediators and Type 2 Diabetes Risk Factors before and in Response to Lifestyle Intervention among Latino Adolescents with Obesity. Nutrients, 15(11), 2442. https://doi.org/10.3390/nu15112442