
Exploring Rates of Adherence and Barriers to Time-Restricted Eating



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.1.1. Study Intervention
2.1.2. Participants
2.2. Adherence
2.2.1. Time-Stamped Dietary Assessment
2.2.2. Continuous Glucose Monitors (CGM)
2.2.3. Scoring Adherence
2.2.4. Exit Questionnaire
2.2.5. Exit Interviews
2.3. Preference towards TRE
Exit Questionnaire
2.4. Statistical and Thematic Analysis
3. Results
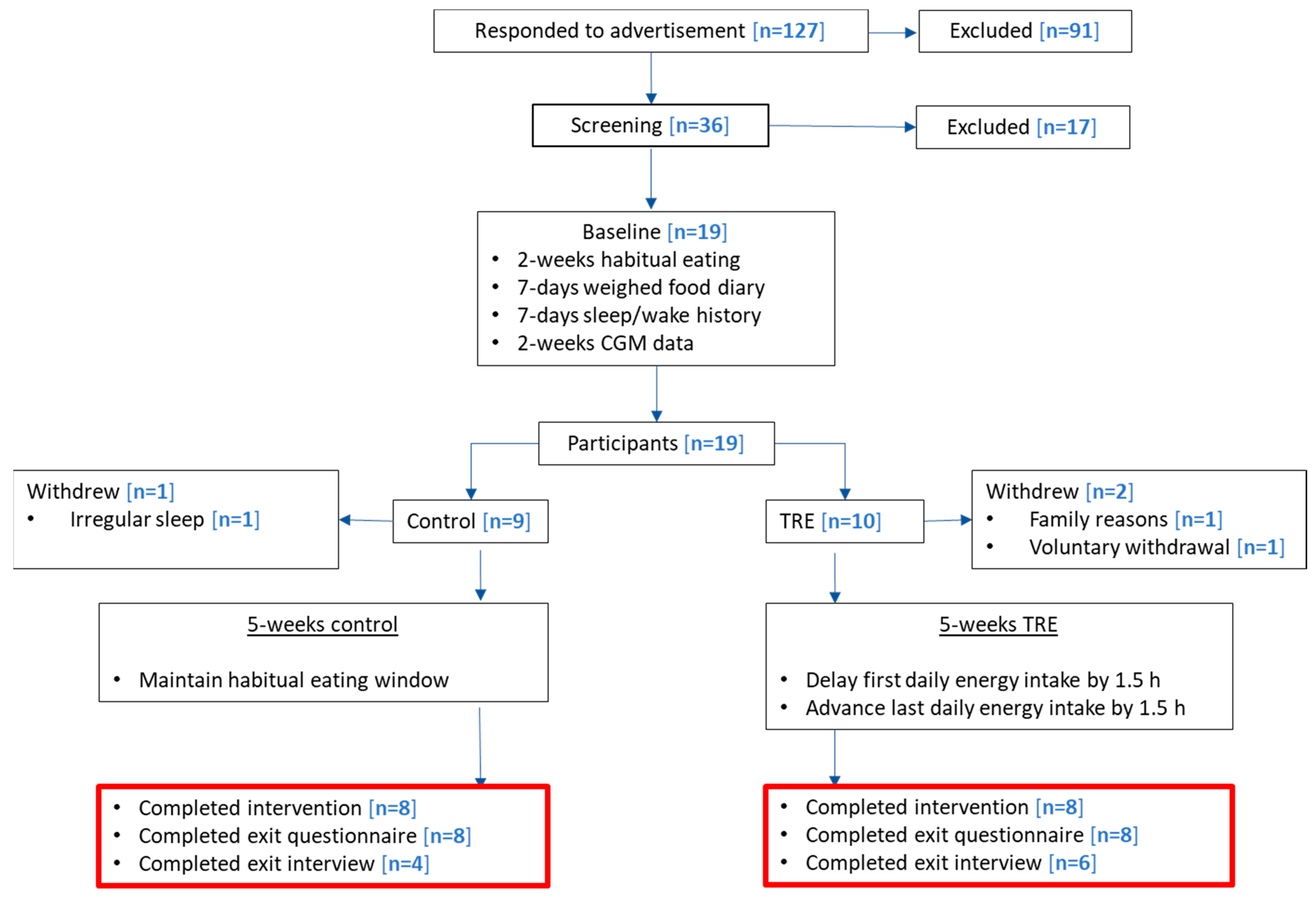
3.1. Participants
3.2. Adherence
3.2.1. Time-Stamped Dietary Assessment
3.2.2. Continuous Glucose Monitoring (CGM)
3.2.3. Exit Questionnaires
3.2.4. Exit Interviews
Summary of Adherence Themes
3.3. Preference towards TRE
3.3.1. Exit Questionnaire
Summary of Preference Themes
Positives of TRE
Negatives of TRE
Incentives of TRE
Barriers to TRE
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Menezes, M.C.; Duarte, C.K.; Costa, D.V.D.P.; Lopes, M.S.; de Freitas, P.P.; Campos, S.F.; Lopes, A.C. A systematic review of effects, potentialities, and limitations of nutritional interventions aimed at managing obesity in primary and secondary health care. Nutrition 2020, 75–76, 110784. [Google Scholar] [CrossRef] [PubMed]
- Fock, K.M.; Khoo, J. Diet and exercise in management of obesity and overweight. J. Gastroenterol. Hepatol. 2013, 28 (Suppl. S4), 59–63. [Google Scholar] [CrossRef] [PubMed]
- Dietz, W.H.; Baur, L.A.; Hall, K.; Puhl, R.M.; Taveras, E.M.; Uauy, R.; Kopelman, P. Management of obesity: Improvement of health-care training and systems for prevention and care. Lancet 2015, 385, 2521–2533. [Google Scholar] [CrossRef] [PubMed]
- Lean, M.E.; Leslie, W.S.; Barnes, A.C.; Brosnahan, N.; Thom, G.; McCombie, L.; Peters, C.; Zhyzhneuskaya, S.; Al-Mrabeh, A.; Hollingsworth, K.G.; et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): An open-label, cluster-randomised trial. Lancet 2018, 391, 541–551. [Google Scholar] [CrossRef] [PubMed]
- Antoni, R.; Robertson, T.M.; Robertson, M.D.; Johnston, J.D. A pilot feasibility study exploring the effects of a moderate time-restricted feeding intervention on energy intake, adiposity and metabolic physiology in free-living human subjects. J. Nutr. Sci. 2018, 7, e22. [Google Scholar] [CrossRef]
- Chow, L.S.; Manoogian, E.N.C.; Alvear, A.; Fleischer, J.; Thor, H.; Dietsche, K.; Wang, Q.; Hodges, J.S.; Esch, N.; Malaeb, S.; et al. Time-Restricted Eating Effects on Body Composition and Metabolic Measures in Humans who are Overweight: A Feasibility Study. Obesity 2020, 28, 860–869. [Google Scholar] [CrossRef]
- Cienfuegos, S.; Gabel, K.; Kalam, F.; Ezpeleta, M.; Wiseman, E.; Pavlou, V.; Lin, S.; Oliveira, M.L.; Varady, K.A. Effects of 4- and 6-h Time-Restricted Feeding on Weight and Cardiometabolic Health: A Randomized Controlled Trial in Adults with Obesity. Cell Metab. 2020, 32, 366–378.e3. [Google Scholar] [CrossRef]
- Gabel, K.; Hoddy, K.K.; Haggerty, N.; Song, J.; Kroeger, C.M.; Trepanowski, J.F.; Panda, S.; Varady, K.A. Effects of 8-hour time restricted feeding on body weight and metabolic disease risk factors in obese adults: A pilot study. Nutr. Healthy Aging 2018, 4, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Gill, S.; Panda, S. A Smartphone App Reveals Erratic Diurnal Eating Patterns in Humans that Can Be Modulated for Health Benefits. Cell Metab. 2015, 22, 789–798. [Google Scholar] [CrossRef]
- Schroder, J.D.; Falqueto, H.; Mânica, A.; Zanini, D.; de Oliveira, T.; de Sá, C.A.; Cardoso, A.M.; Manfredi, L.H. Effects of time-restricted feeding in weight loss, metabolic syndrome and cardiovascular risk in obese women. J. Transl. Med. 2021, 19, 3. [Google Scholar] [CrossRef]
- Wilkinson, M.J.; Manoogian, E.N.C.; Zadourian, A.; Lo, H.; Fakhouri, S.; Shoghi, A.; Wang, X.; Fleischer, J.G.; Navlakha, S.; Panda, S.; et al. Ten-hour time-restricted eating reduces weight, blood pressure, and atherogenic lipids in patients with metabolic syndrome. Cell Metab. 2020, 31, 92–104.e5. [Google Scholar] [CrossRef] [PubMed]
- Moro, T.; Tinsley, G.; Bianco, A.; Marcolin, G.; Pacelli, Q.F.; Battaglia, G.; Palma, A.; Gentil, P.; Neri, M.; Paoli, A. Effects of eight weeks of time-restricted feeding (16/8) on basal metabolism, maximal strength, body composition, inflammation, and cardiovascular risk factors in resistance-trained males. J. Transl. Med. 2016, 14, 290. [Google Scholar] [CrossRef] [PubMed]
- Tinsley, G.; Forsse, J.S.; Butler, N.K.; Paoli, A.; Bane, A.A.; La Bounty, P.M.; Morgan, G.B.; Grandjean, P.W. Time-restricted feeding in young men performing resistance training: A randomized controlled trial. Eur. J. Sport Sci. 2016, 17, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Tinsley, G.M.; Moore, M.L.; Graybeal, A.J.; Paoli, A.; Kim, Y.; Gonzales, J.U.; Harry, J.R.; VanDusseldorp, T.A.; Kennedy, D.N.; Cruz, M.R. Time-restricted feeding plus resistance training in active females: A randomized trial. Am. J. Clin. Nutr. 2019, 110, 628–640. [Google Scholar] [CrossRef] [PubMed]
- Anton, S.D.; Lee, S.A.; Donahoo, W.T.; McLaren, C.; Manini, T.; Leeuwenburgh, C.; Pahor, M. The Effects of Time Restricted Feeding on Overweight, Older Adults: A Pilot Study. Nutrients 2019, 11, 1500. [Google Scholar] [CrossRef]
- Rui, L. Energy Metabolism in the Liver. Compr. Physiol. 2014, 4, 177–197. [Google Scholar] [CrossRef]
- Ravussin, E.; Beyl, R.A.; Poggiogalle, E.; Hsia, D.; Peterson, C.M. Early Time-Restricted Feeding Reduces Appetite and Increases Fat Oxidation But Does Not Affect Energy Expenditure in Humans. Obesity 2019, 27, 1244–1254. [Google Scholar] [CrossRef] [PubMed]
- Hutchison, A.T.; Regmi, P.; Manoogian, E.N.; Fleischer, J.G.; Wittert, G.A.; Panda, S.; Heilbronn, L.K. Time-restricted feeding improves glucose tolerance in men at risk for type 2 diabetes: A randomized crossover trial. Obesity 2019, 27, 724–732. [Google Scholar] [CrossRef]
- Jones, R.; Pabla, P.; Mallinson, J.; Nixon, A.; Taylor, T.; Bennett, A.; Tsintzas, K. Two weeks of early time-restricted feeding (eTRF) improves skeletal muscle insulin and anabolic sensitivity in healthy men. Am. J. Clin. Nutr. 2020, 112, 1015–1028. [Google Scholar] [CrossRef]
- Jamshed, H.; Beyl, R.A.; della Manna, D.L.; Yang, E.S.; Ravussin, E.; Peterson, C.M. Early Time-Restricted Feeding Improves 24-Hour Glucose Levels and Affects Markers of the Circadian Clock, Aging, and Autophagy in Humans. Nutrients 2019, 11, 1234. [Google Scholar] [CrossRef]
- Sutton, E.F.; Beyl, R.; Early, K.S.; Cefalu, W.T.; Ravussin, E.; Peterson, C.M. Early time-restricted feeding improves insulin sensitivity, blood pressure, and oxidative stress even without weight loss in men with prediabetes. Cell Metab. 2018, 27, 1212–1221.e3. [Google Scholar] [CrossRef]
- Jakubowicz, D.; Barnea, M.; Wainstein, J.; Froy, O. High Caloric intake at breakfast vs. dinner differentially influences weight loss of overweight and obese women. Obesity 2013, 21, 2504–2512. [Google Scholar] [CrossRef]
- Moroshko, I.; Brennan, L.; O’Brien, P. Predictors of dropout in weight loss interventions: A systematic review of the literature. Obes. Rev. 2011, 12, 912–934. [Google Scholar] [CrossRef]
- van Baak, M.A.; Mariman, E.C.M. Dietary Strategies for Weight Loss Maintenance. Nutrients 2019, 11, 1916. [Google Scholar] [CrossRef]
- Lowe, D.A.; Wu, N.; Rohdin-Bibby, L.; Moore, A.H.; Kelly, N.; Liu, Y.E.; Philip, E.; Vittinghoff, E.; Heymsfield, S.B.; Olgin, J.E.; et al. Effects of Time-Restricted Eating on Weight Loss and Other Metabolic Parameters in Women and Men with Overweight and Obesity. JAMA Intern. Med. 2020, 180, 1491. [Google Scholar] [CrossRef]
- Parr, E.B.; Devlin, B.L.; Radford, B.E.; Hawley, J.A. A Delayed Morning and Earlier Evening Time-Restricted Feeding Protocol for Improving Glycemic Control and Dietary Adherence in Men with Overweight/Obesity: A Randomized Controlled Trial. Nutrients 2020, 12, 505. [Google Scholar] [CrossRef]
- Che, T.; Yan, C.; Tian, D.; Zhang, X.; Liu, X.; Wu, Z. Time-restricted feeding improves blood glucose and insulin sensitivity in overweight patients with type 2 diabetes: A randomised controlled trial. Nutr. Metab. 2021, 18, 88. [Google Scholar] [CrossRef]
- Isenmann, E.; Dissemond, J.; Geisler, S. The Effects of a Macronutrient-Based Diet and Time-Restricted Feeding (16:8) on Body Composition in Physically Active Individuals—A 14-Week Randomised Controlled Trial. Nutrients 2021, 13, 3122. [Google Scholar] [CrossRef]
- Jefcoate, P.W.; Robertson, M.D.; Ogden, J.; Johnston, J.D. Identification of factors influencing motivation to undertake time-restricted feeding in humans. Appetite 2021, 164, 105240. [Google Scholar] [CrossRef]
- O’Connor, S.G.; Boyd, P.; Bailey, C.P.; Nebeling, L.; Reedy, J.; Czajkowski, S.M.; Shams-White, M.M. A qualitative exploration of facilitators and barriers of adherence to time-restricted eating. Appetite 2022, 178, 106266. [Google Scholar] [CrossRef]
- Parr, E.B.; Devlin, B.L.; Lim, K.H.C.; Moresi, L.N.Z.; Geils, C.; Brennan, L.; Hawley, J.A. Time-Restricted Eating as a Nutrition Strategy for Individuals with Type 2 Diabetes: A Feasibility Study. Nutrients 2020, 12, 3228. [Google Scholar] [CrossRef]
- Bjerre, N.; Holm, L.; Quist, J.S.; Færch, K.; Hempler, N.F. Watching, keeping and squeezing time to lose weight: Implications of time-restricted eating in daily life. Appetite 2021, 161, 105138. [Google Scholar] [CrossRef] [PubMed]
- Bingham, S.A.; Gill, C.; Welch, A.; Day, K.; Cassidy, A.; Khaw, K.T.; Sneyd, M.J.; Key, T.J.A.; Roe, L.; Day, N.E. Comparison of dietary assessment methods in nutritional epidemiology: Weighed records v. 24 h recalls, food-frequency questionnaires and estimated-diet records. Br. J. Nutr. 1994, 72, 619–643. [Google Scholar] [CrossRef] [PubMed]
- Jamshed, H.; Steger, F.L.; Bryan, D.R.; Richman, J.S.; Warriner, A.H.; Hanick, C.J.; Martin, C.K.; Salvy, S.-J.; Peterson, C.M. Effectiveness of Early Time-Restricted Eating for Weight Loss, Fat Loss, and Cardiometabolic Health in Adults with Obesity. JAMA Intern. Med. 2022, 182, 953. [Google Scholar] [CrossRef] [PubMed]
- Bao, R.; Sun, Y.; Jiang, Y.; Ye, L.; Hong, J.; Wang, W. Effects of Time-Restricted Feeding on Energy Balance: A Cross-Over Trial in Healthy Subjects. Front. Endocrinol. 2022, 13, 870054. [Google Scholar] [CrossRef]
- Steger, F.L.; Jamshed, H.; Bryan, D.R.; Richman, J.S.; Warriner, A.H.; Hanick, C.J.; Martin, C.K.; Salvy, S.; Peterson, C.M. Early time-restricted eating affects weight, metabolic health, mood, and sleep in adherent completers: A secondary analysis. Obesity 2022, 31, 96–107. [Google Scholar] [CrossRef]
- Queiroz, J.D.N.; Macedo, R.C.O.; dos Santos, G.C.; Munhoz, S.V.; Machado, C.L.F.; de Menezes, R.L.; Menzem, E.N.; Moritz, C.E.J.; Pinto, R.S.; Tinsley, G.M.; et al. Cardiometabolic effects of early v. delayed time-restricted eating plus energetic restriction in adults with overweight and obesity: An exploratory randomised clinical trial. Br. J. Nutr. 2022, 129, 637–649. [Google Scholar] [CrossRef]
- Windhauser, M.M.; Evans, M.A.; Mccullough, M.L.; Swain, J.F.; Lin, P.-H.; Hoben, K.P.; Plaisted, C.S.; Karanja, N.M.; Vollmer, W.M. Dietary Adherence in the Dietary Approaches to Stop Hypertension Trial. J. Am. Diet. Assoc. 1999, 99, S76–S83. [Google Scholar] [CrossRef]
- Lee, S.A.; Sypniewski, C.; Bensadon, B.A.; McLaren, C.; Donahoo, W.T.; Sibille, K.T.; Anton, S. Determinants of Adherence in Time-Restricted Feeding in Older Adults: Lessons from a Pilot Study. Nutrients 2020, 12, 874. [Google Scholar] [CrossRef]
- Shea, S.A.; Hilton, M.F.; Orlova, C.; Ayers, R.T.; Mantzoros, C.S. Independent Circadian and Sleep/Wake Regulation of Adipokines and Glucose in Humans. J. Clin. Endocrinol. Metab. 2005, 90, 2537–2544. [Google Scholar] [CrossRef]
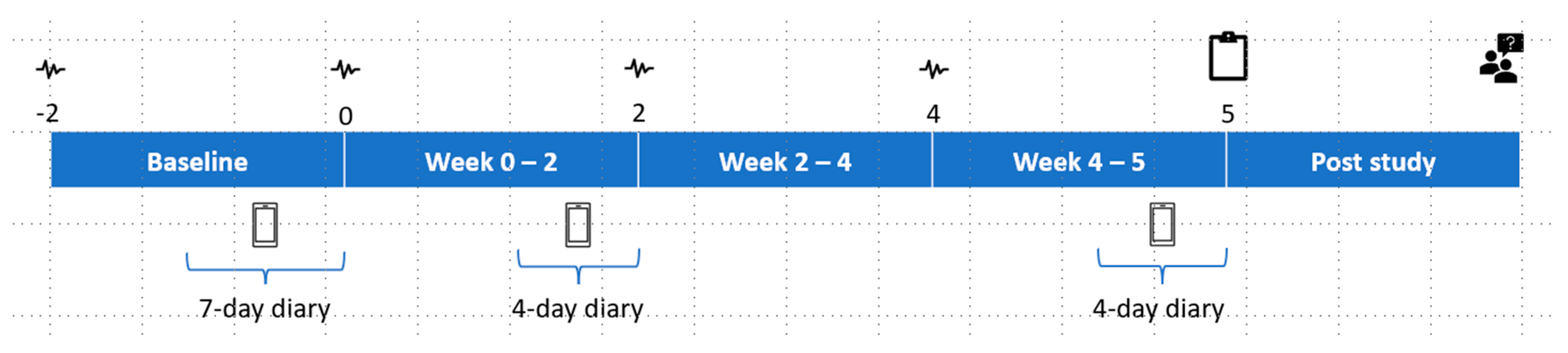
 were changed every two weeks beginning at the start of baseline (Week −2) until the beginning of Week 4. Data collected at home included a diet diary
were changed every two weeks beginning at the start of baseline (Week −2) until the beginning of Week 4. Data collected at home included a diet diary  on three separate occasions (Week −2–0, Week 0–2, and Week 4–5). End of study data collected included an exit questionnaire
on three separate occasions (Week −2–0, Week 0–2, and Week 4–5). End of study data collected included an exit questionnaire  (Week 5) and exit interview
(Week 5) and exit interview  (Post study).
were changed every two weeks beginning at the start of baseline (Week −2) until the beginning of Week 4. Data collected at home included a diet diary on three separate occasions (Week −2–0, Week 0–2, and Week 4–5). End of study data collected included an exit questionnaire (Week 5) and exit interview (Post study).
(Post study).
were changed every two weeks beginning at the start of baseline (Week −2) until the beginning of Week 4. Data collected at home included a diet diary on three separate occasions (Week −2–0, Week 0–2, and Week 4–5). End of study data collected included an exit questionnaire (Week 5) and exit interview (Post study).

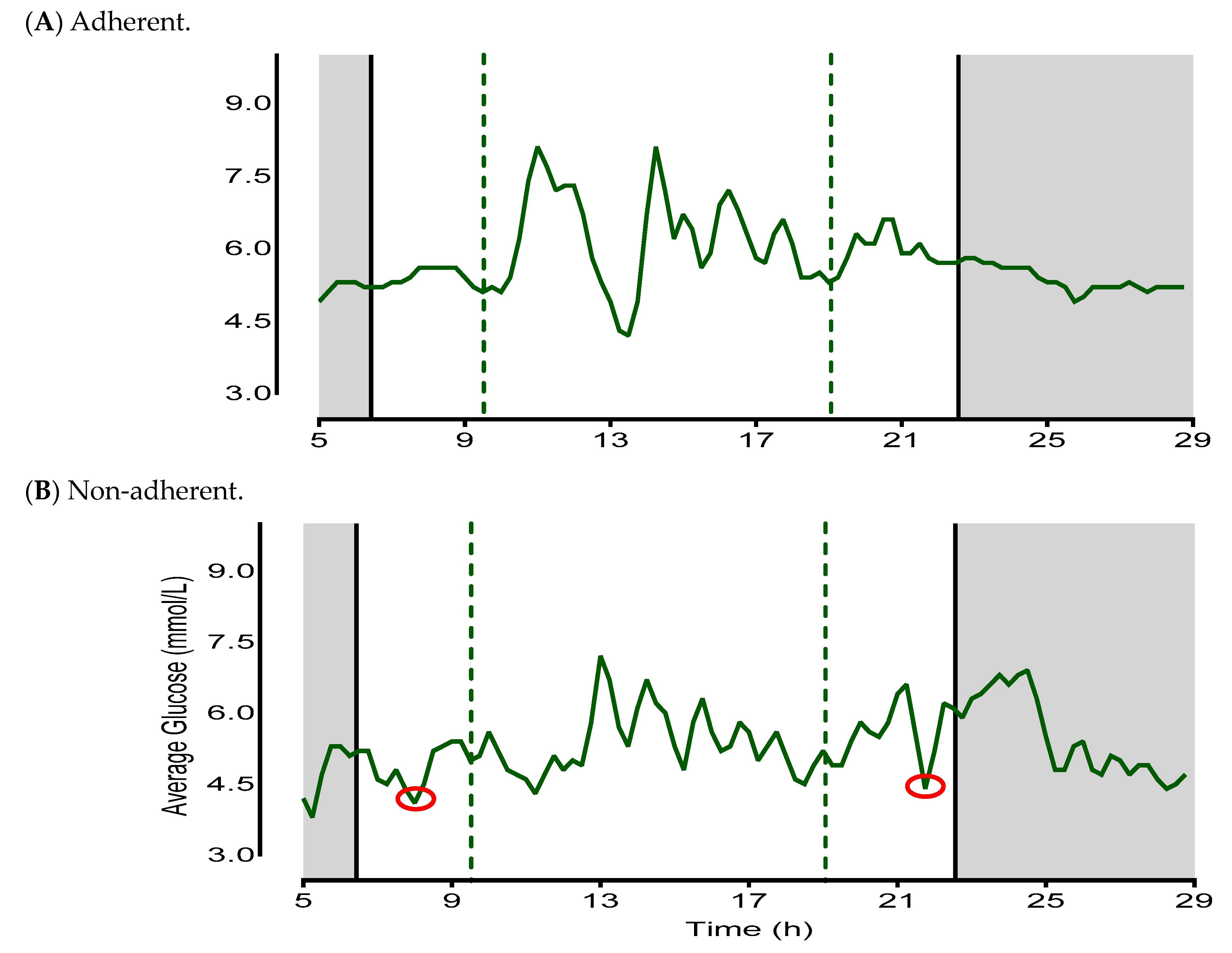
 = glucose levels;
= glucose levels;  = mean delayed and advanced eating occasions;
= mean delayed and advanced eating occasions;  = mean sleep and wake times;
= mean sleep and wake times;  = sleep phase;
= sleep phase;  = suspected energy intake outside of reported eating window. (A) is an example of an adherent day with the CGM response in close correspondence to the reported mean first and last eating occasion, and the overall eating window is <12 h. (B) is an example of a non-adherent day where CGM responses appear before and after the reported mean first and last eating occasions of the day, and the overall eating window is >12 h.
= glucose levels; = mean delayed and advanced eating occasions; = mean sleep and wake times; = sleep phase; = suspected energy intake outside of reported eating window. (A) is an example of an adherent day with the CGM response in close correspondence to the reported mean first and last eating occasion, and the overall eating window is <12 h. (B) is an example of a non-adherent day where CGM responses appear before and after the reported mean first and last eating occasions of the day, and the overall eating window is >12 h.
= suspected energy intake outside of reported eating window. (A) is an example of an adherent day with the CGM response in close correspondence to the reported mean first and last eating occasion, and the overall eating window is <12 h. (B) is an example of a non-adherent day where CGM responses appear before and after the reported mean first and last eating occasions of the day, and the overall eating window is >12 h.
= glucose levels; = mean delayed and advanced eating occasions; = mean sleep and wake times; = sleep phase; = suspected energy intake outside of reported eating window. (A) is an example of an adherent day with the CGM response in close correspondence to the reported mean first and last eating occasion, and the overall eating window is <12 h. (B) is an example of a non-adherent day where CGM responses appear before and after the reported mean first and last eating occasions of the day, and the overall eating window is >12 h.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TRE Group Experience of TRE | Control Group Attitude towards TRE |
|---|---|
| How did you find following the TRE intervention? Why was that? | How do you think you would find following the TRE intervention? Why is that? |
| What were the negatives of following TRE? What were the positives of following TRE? | What do you think the negatives of following TRE would be? What do you think the positives of following TRE would be? |
| Did it affect your day-to-day living in any way? Did it affect your food choices in any way? Did it affect your sleep in any way? | Do you think it would affect your day-to-day living in any way? Do you think it would affect your food choices in any way? Do you think it would affect your sleep in any way? |
| Adherence | Adherence |
| On how many days of the week were you able to comply with the 1.5 h delay to the timing of first energy intake in the morning? What enabled you to achieve this? What restricted you from achieving this? | On how many days of the week do you think you would be able to comply with the 1.5 h delay to the timing of first energy intake in the morning? What would enable you to achieve this? What would restrict you from achieving this? |
| On how many days of the week were you able to comply with the 1.5 h advance to the timing of last energy intake in the evening? What enabled you to achieve this? What restricted you from achieving this? | On how many days of the week do you think you would be able to comply with the 1.5 h advance to the timing of last energy intake in the evening? What would enable you to achieve this? What would restrict you from achieving this? |
| Were you able to reduce your eating window by 3 h overall by choosing your own feeding window? What did you do? | Do you think you would be able to reduce your eating window by 3 h overall if you were able to choose your own feeding restriction? What would this look like? |
| TRE (n = 8) | Control (n = 8) | p | |
|---|---|---|---|
| Sex (F:M) | 8:0 | 7:1 | 0.351 |
| Age (y) | 28 ± 9.5 | 27.4 ± 8.1 | 0.889 |
| Weight (kg) | 66.4 ± 10.1 | 66.6 ± 10.1 | 0.970 |
| BMI (kg/m2) | 24.1 ± 3.0 | 23.0 ± 1.6 | 0.435 |
| TRE n = 7 | Control n = 5 | Time | Group | Group × Time | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| W0 | W2 | W5 | Mean | W0 | W2 | W5 | Mean | p | p | p | |
| Adherence (%) | 75.3 (7.1) | 60.1 (8.3) | 65.2 (8.0) | 62.7 (8.2) | 82.7 (2.6) | 82.4 (8.9) | 75.2 (2.7) | 78.8 (5.8) | 0.400 | 0.176 | 0.435 |
| Mean ± SEM | t | p | ||
|---|---|---|---|---|
| TRE | How did you find the TRE intervention? | 3.1 ± 1.0 | 0.266 | 0.794 |
| Control | How do you think you would find the TRE intervention? | 3.3 ± 0.9 | ||
| TRE | On how many days of the week were you able to comply with the 1.5 h delay to the timing of first energy intake in the morning? | 4.9 ± 0.4 | −4.320 | <0.001 |
| Control | On how many days of the week do you think you would be able to comply with the 1.5 h delay to the timing of first energy intake in the morning? | 3.4 ± 0.9 | ||
| TRE | On how many days of the week were you able to comply with the 1.5 h advance to the timing of last energy intake in the evening? | 4.1 ± 0.6 | −4.075 | <0.001 |
| Control | On how many days of the week do you think you would be able to comply with the 1.5 h advance to the timing of last energy intake in the evening? | 2.8 ± 0.7 | ||
| TRE | Were you able to reduce your eating window by 3 h overall? | 4.3 ± 0.7 | −3.989 | <0.001 |
| Control | Do you think you would be able to reduce your eating window by 3 h overall? | 3.0 ± 0.5 | ||
| Area of Investigation | Summary of Thematic Analysis | TRE | Control |
|---|---|---|---|
| Experience of TRE |
| ☒ | ☒ |
| ☒ | ☒ | |
| ☒ | ☐ | |
| ☒ | ☐ | |
| ☒ | ☒ | |
| ☒ | ☒ | |
| ☒ | ☐ | |
| ☒ | ☐ | |
| Positives of TRE |
| ☒ | ☒ |
| ☒ | ☐ | |
| ☒ | ☐ | |
| ☒ | ☒ | |
| ☒ | ☒ | |
| Negatives of TRE |
| ☒ | ☒ |
| ☒ | ☐ | |
| ☒ | ☐ | |
| ☐ | ☒ | |
| Incentives to follow TRE |
| ☒ | ☒ |
| ☒ | ☒ | |
| ☒ | ☐ | |
| ☒ | ☐ | |
| ☒ | ☒ | |
| Barriers to following TRE |
| ☒ | ☒ |
| ☒ | ☒ | |
| ☒ | ☐ | |
| ☒ | ☒ | |
| ☒ | ☐ | |
| Preference towards TRE |
| ☒ | ☒ |
| ☒ | ☐ | |
| Additional comments |
| ☒ | ☒ |
| ☒ | ☐ |
| TRE n = 8 | Control n = 8 | t | p | |
|---|---|---|---|---|
| How many days a week do you plan to continue following TRE on? | 3.0 (0.9) | 3.4 (0.9) | 0.814 | 0.429 |
| Realistically, how many days per week do you think you could follow TRE on? | 4.6 (1.5) | 3.6 (0.1) | −1.372 | 0.192 |
| Please select the duration of time you could consistently adhere to in terms of restricting daily eating window | 3.6 (0.7) | 3.3 (0.7) | −1.033 | 0.319 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jefcoate, P.W.; Robertson, M.D.; Ogden, J.; Johnston, J.D. Exploring Rates of Adherence and Barriers to Time-Restricted Eating. Nutrients 2023, 15, 2336. https://doi.org/10.3390/nu15102336
Jefcoate PW, Robertson MD, Ogden J, Johnston JD. Exploring Rates of Adherence and Barriers to Time-Restricted Eating. Nutrients. 2023; 15(10):2336. https://doi.org/10.3390/nu15102336
Chicago/Turabian StyleJefcoate, Paul W., M. Denise Robertson, Jane Ogden, and Jonathan D. Johnston. 2023. "Exploring Rates of Adherence and Barriers to Time-Restricted Eating" Nutrients 15, no. 10: 2336. https://doi.org/10.3390/nu15102336
APA StyleJefcoate, P. W., Robertson, M. D., Ogden, J., & Johnston, J. D. (2023). Exploring Rates of Adherence and Barriers to Time-Restricted Eating. Nutrients, 15(10), 2336. https://doi.org/10.3390/nu15102336