
Association between Healthy Eating Index-2015 and Age-Related Cataract in American Adults: A Cross-Sectional Study of NHANES 2005–2008


Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source and Study Population
2.2. Cataract Assessment
2.3. Healthy Eating Index-2015 Assessment
2.4. Covariates Assessment
2.5. Statistical Analysis
3. Results
3.1. Study Population Characteristics
3.2. Association of HEI-2015 and Cataract Risk Using Logistic Regression
3.3. Association of HEI-2015 and Cataract Using Propensity Score Weighted Regression
3.4. Association of HEI-2015 Components and Cataract
3.5. Investigation of Non-Linear Association Using Restricted Cubic Spline
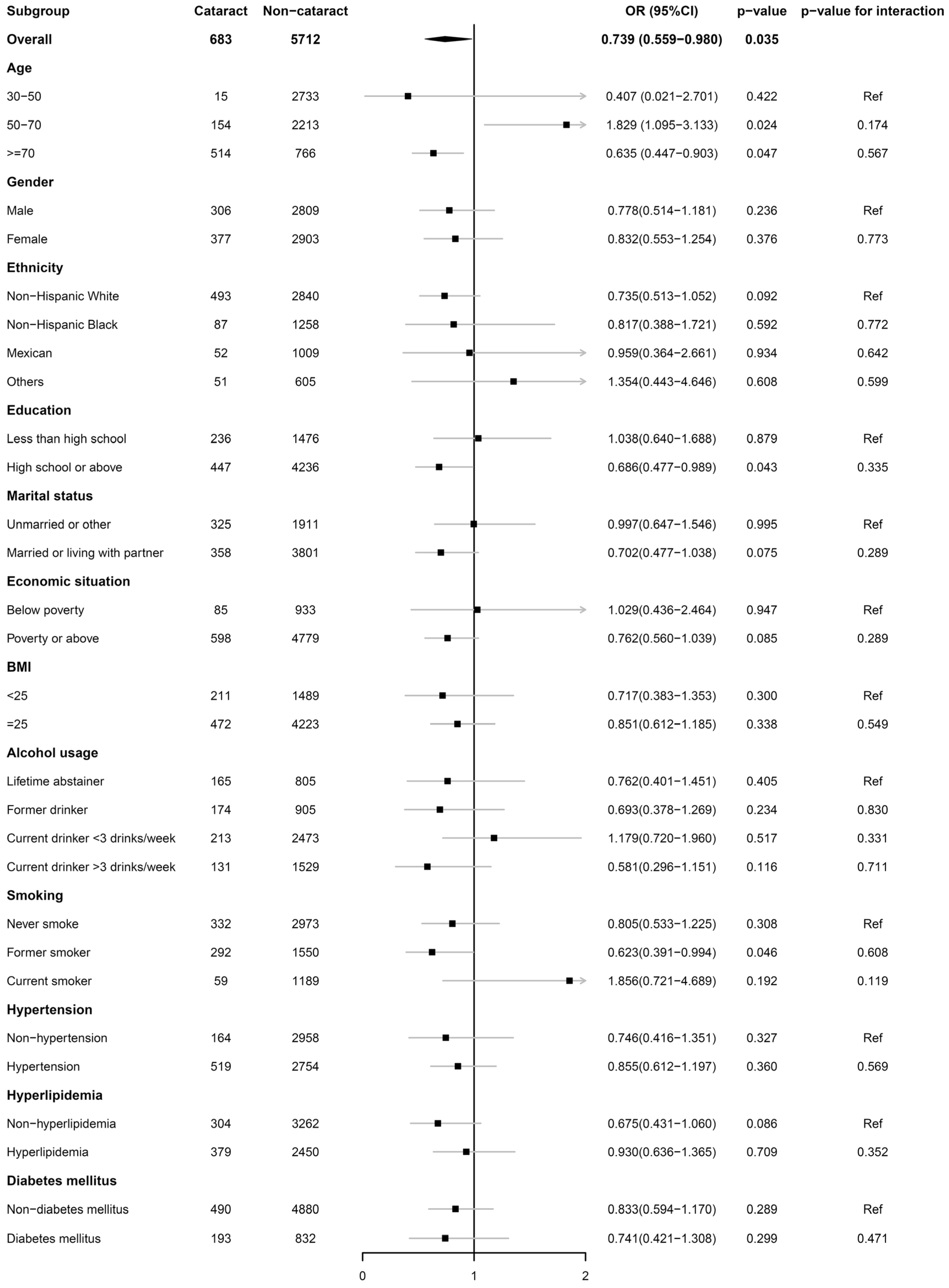
3.6. Subgroup Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2019 Blindness and Vision Impairment Collaborators; Vision Loss Expert Group of the Global Burden of Disease Study. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: The Right to Sight: An analysis for the Global Burden of Disease Study. Lancet Glob. Health 2021, 9, e144–e160. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Xu, J.; Chen, X.; Yao, K. Cataract: Advances in surgery and whether surgery remains the only treatment in future. Adv. Ophthalmol. Pract. Res. 2021, 1, 100008. [Google Scholar] [CrossRef]
- Liu, Y.C.; Wilkins, M.; Kim, T.; Malyugin, B.; Mehta, J.S. Cataracts. Lancet 2017, 390, 600–612. [Google Scholar] [CrossRef] [PubMed]
- Yan, W.; Wang, W.; van Wijngaarden, P.; Mueller, A.; He, M. Longitudinal changes in global cataract surgery rate inequality and associations with socioeconomic indices. Clin. Exp. Ophthalmol. 2019, 47, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Rehm, C.D.; Onopa, J.; Mozaffarian, D. Trends in Diet Quality Among Youth in the United States, 1999-2016. Jama 2020, 323, 1161–1174. [Google Scholar] [CrossRef] [PubMed]
- Francisco, S.G.; Smith, K.M.; Aragones, G.; Whitcomb, E.A.; Weinberg, J.; Wang, X.; Bejarano, E.; Taylor, A.; Rowan, S. Dietary Patterns, Carbohydrates, and Age-Related Eye Diseases. Nutrients 2020, 12, 2862. [Google Scholar] [CrossRef]
- Broadhead, G.K.; Hong, T.; Bahrami, B.; Flood, V.; Liew, G.; Chang, A.A. Diet and risk of visual impairment: A review of dietary factors and risk of common causes of visual impairment. Nutr. Rev. 2021, 79, 636–650. [Google Scholar] [CrossRef]
- Shan, Z.; Li, Y.; Baden, M.Y.; Bhupathiraju, S.N.; Wang, D.D.; Sun, Q.; Rexrode, K.M.; Rimm, E.B.; Qi, L.; Willett, W.C.; et al. Association Between Healthy Eating Patterns and Risk of Cardiovascular Disease. JAMA Intern. Med. 2020, 180, 1090–1100. [Google Scholar] [CrossRef]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans, 8th ed.; U.S. Department of Agriculture: Washington, DC, USA, 2015. [Google Scholar]
- U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025, 9th ed.; U.S. Department of Agriculture: Washington, DC, USA, 2020. [Google Scholar]
- Zhang, Y.; Lu, C.; Li, X.; Fan, Y.; Li, J.; Liu, Y.; Yu, Y.; Zhou, L. Healthy Eating Index-2015 and Predicted 10-Year Cardiovascular Disease Risk, as Well as Heart Age. Front. Nutr. 2022, 9, 888966. [Google Scholar] [CrossRef]
- Chen, Y.Y.; Chen, G.C.; Abittan, N.; Xing, J.; Mossavar-Rahmani, Y.; Sotres-Alvarez, D.; Mattei, J.; Daviglus, M.; Isasi, C.R.; Hu, F.B.; et al. Healthy dietary patterns and risk of cardiovascular disease in US Hispanics/Latinos: The Hispanic Community Health Study/Study of Latinos (HCHS/SOL). Am. J. Clin. Nutr. 2022, 116, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Zhao, L.; Dong, J.; Chen, H.; Li, D.; Zhang, X.; Hassan, M.M.; Steck, S.E.; Li, X.; Xiang, Y.B.; et al. The role of dietary factors in nonalcoholic fatty liver disease to hepatocellular carcinoma progression: A systematic review. Clin. Nutr. 2022, 41, 2295–2307. [Google Scholar] [CrossRef] [PubMed]
- Peng, S.; Yu, Y.; Yu, X.; Guo, D.; Su, L.; Li, H.; Luo, P.; Chen, P.; Wu, S.; Huang, Y.; et al. Adherence to the Chinese dietary guidelines and metabolic syndrome among children aged 6–14 years. Food Funct. 2022, 13, 9772–9781. [Google Scholar] [CrossRef] [PubMed]
- Onvani, S.; Haghighatdoost, F.; Surkan, P.J.; Larijani, B.; Azadbakht, L. Adherence to the Healthy Eating Index and Alternative Healthy Eating Index dietary patterns and mortality from all causes, cardiovascular disease and cancer: A meta-analysis of observational studies. J. Hum. Nutr. Diet. 2017, 30, 216–226. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention; National Center for Health Statistics. NHANES-National Health and Nutrition Examination Survey Homepage. Available online: https://www.cdc.gov/nchs/nhanes/about_nhanes.htm (accessed on 18 October 2022).
- Garcia-Layana, A.; Ciufo, G.; Toledo, E.; Martinez-Gonzalez, M.A.; Corella, D.; Fito, M.; Estruch, R.; Gomez-Gracia, E.; Fiol, M.; Lapetra, J.; et al. The Effect of a Mediterranean Diet on the Incidence of Cataract Surgery. Nutrients 2017, 9, 453. [Google Scholar] [CrossRef]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef]
- Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef]
- Li, X.Y.; Wen, M.Z.; Xu, Y.H.; Shen, Y.C.; Yang, X.T. The association of healthy eating index with periodontitis in NHANES 2013–2014. Front. Nutr. 2022, 9, 968073. [Google Scholar] [CrossRef]
- Nie, J.; Deng, M.G.; Wang, K.; Liu, F.; Xu, H.; Feng, Q.; Li, X.; Yang, Y.; Zhang, R.; Wang, S. Higher HEI-2015 scores are associated with lower risk of gout and hyperuricemia: Results from the national health and nutrition examination survey 2007–2016. Front. Nutr. 2022, 9, 921550. [Google Scholar] [CrossRef]
- Yin, S.; Wang, J.; Bai, Y.; Yang, Z.; Cui, J.; Xiao, Y.; Wang, J. Association Between Healthy Eating Index-2015 and Kidney Stones in American Adults: A Cross-Sectional Analysis of NHANES 2007–2018. Front. Nutr. 2022, 9, 820190. [Google Scholar] [CrossRef]
- Tan, A.G.; Kifley, A.; Flood, V.M.; Russell, J.; Burlutsky, G.; Cumming, R.G.; Mitchell, P.; Wang, J.J. The Combination of Healthy Diet and Healthy Body Weight Is Associated with Lower Risk of Nuclear Cataract in the Blue Mountains Eye Study. J. Nutr. 2019, 149, 1617–1622. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention; National Center for Health Statistics. NHIS-Adult Alcohol Use-Glossary. Available online: https://www.cdc.gov/nchs/nhis/alcohol/alcohol_glossary.htm (accessed on 18 October 2022).
- Centers for Disease Control and Prevention; National Center for Health Statistics. NHIS-Adult Tobacco Use-Glossary. Available online: https://www.cdc.gov/nchs/nhis/tobacco/tobacco_glossary.htm (accessed on 18 October 2022).
- Naimi, A.I.; Moodie, E.E.M.; Auger, N.; Kaufman, J.S. Constructing Inverse Probability Weights for Continuous Exposures: A Comparison of Methods. Epidemiology 2014, 25, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Moeller, S.M.; Taylor, A.; Tucker, K.L.; McCullough, M.L.; Chylack, L.T., Jr.; Hankinson, S.E.; Willett, W.C.; Jacques, P.F. Overall adherence to the dietary guidelines for americans is associated with reduced prevalence of early age-related nuclear lens opacities in women. J. Nutr. 2004, 134, 1812–1819. [Google Scholar] [CrossRef] [PubMed]
- Ghanavati, M.; Behrooz, M.; Rashidkhani, B.; Ashtray-Larky, D.; Zameni, S.D.; Alipour, M. Healthy Eating Index in Patients With Cataract: A Case-Control Study. Iran. Red Crescent Med. J. 2015, 17, e22490. [Google Scholar] [CrossRef] [PubMed]
- Mares, J.A.; Voland, R.; Adler, R.; Tinker, L.; Millen, A.E.; Moeller, S.M.; Blodi, B.; Gehrs, K.M.; Wallace, R.B.; Chappell, R.J.; et al. Healthy Diets and the Subsequent Prevalence of Nuclear Cataract in Women. Arch. Ophthalmol. 2010, 128, 738–749. [Google Scholar] [CrossRef]
- Miller, P.E.; Reedy, J.; Kirkpatrick, S.I.; Krebs-Smith, S.M. The United States food supply is not consistent with dietary guidance: Evidence from an evaluation using the Healthy Eating Index-2010. J. Acad. Nutr. Diet 2015, 115, 95–100. [Google Scholar] [CrossRef]
- Kirkpatrick, S.I.; Reedy, J.; Kahle, L.L.; Harris, J.L.; Ohri-Vachaspati, P.; Krebs-Smith, S.M. Fast-food menu offerings vary in dietary quality, but are consistently poor. Public Health Nutr. 2014, 17, 924–931. [Google Scholar] [CrossRef]
- Jahns, L.; Scheett, A.J.; Johnson, L.K.; Krebs-Smith, S.M.; Payne, C.R.; Whigham, L.D.; Hoverson, B.S.; Kranz, S. Diet Quality of Items Advertised in Supermarket Sales Circulars Compared to Diets of the US Population, as Assessed by the Healthy Eating Index-2010. J. Acad. Nutr. Diet 2016, 116, 115–122.e1. [Google Scholar] [CrossRef]
- Truscott, R.J. Age-related nuclear cataract-oxidation is the key. Exp. Eye Res. 2005, 80, 709–725. [Google Scholar] [CrossRef]
- Ruiss, M.; Findl, O.; Kronschläger, M. The human lens: An antioxidant-dependent tissue revealed by the role of caffeine. Ageing Res. Rev. 2022, 79, 101664. [Google Scholar] [CrossRef]
- Williams, D.L. Oxidation, antioxidants and cataract formation: A literature review. Vet. Ophthalmol. 2006, 9, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Leske, M.C.; Chylack, L.T., Jr.; He, Q.; Wu, S.Y.; Schoenfeld, E.; Friend, J.; Wolfe, J. Antioxidant vitamins and nuclear opacities: The longitudinal study of cataract. Ophthalmology 1998, 105, 831–836. [Google Scholar] [CrossRef] [PubMed]
- Cumming, R.G.; Mitchell, P.; Smith, W. Diet and cataract: The Blue Mountains Eye Study. Ophthalmology 2000, 107, 450–456. [Google Scholar] [CrossRef] [PubMed]
- Mares-Perlman, J.A.; Lyle, B.J.; Klein, R.; Fisher, A.I.; Brady, W.E.; VandenLangenberg, G.M.; Trabulsi, J.N.; Palta, M. Vitamin supplement use and incident cataracts in a population-based study. Arch. Ophthalmol. 2000, 118, 1556–1563. [Google Scholar] [CrossRef]
- Age-Related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E and beta carotene for age-related cataract and vision loss: AREDS report no. 9. Arch. Ophthalmol. 2001, 119, 1439–1452. [Google Scholar] [CrossRef]
- Kuzniarz, M.; Mitchell, P.; Cumming, R.G.; Flood, V.M. Use of vitamin supplements and cataract: The Blue Mountains Eye Study. Am. J. Ophthalmol. 2001, 132, 19–26. [Google Scholar] [CrossRef]
- Taylor, A.; Jacques, P.F.; Chylack, L.T., Jr.; Hankinson, S.E.; Khu, P.M.; Rogers, G.; Friend, J.; Tung, W.; Wolfe, J.K.; Padhye, N.; et al. Long-term intake of vitamins and carotenoids and odds of early age-related cortical and posterior subcapsular lens opacities. Am. J. Clin. Nutr. 2002, 75, 540–549. [Google Scholar] [CrossRef]
- Mares, J.A. High-dose antioxidant supplementation and cataract risk. Nutr. Rev. 2004, 62, 28–32. [Google Scholar] [CrossRef]
- Yoshida, M.; Takashima, Y.; Inoue, M.; Iwasaki, M.; Otani, T.; Sasaki, S.; Tsugane, S. Prospective study showing that dietary vitamin C reduced the risk of age-related cataracts in a middle-aged Japanese population. Eur. J. Nutr. 2007, 46, 118–124. [Google Scholar] [CrossRef]
- Christen, W.G.; Liu, S.; Glynn, R.J.; Gaziano, J.M.; Buring, J.E. Dietary carotenoids, vitamins C and E, and risk of cataract in women: A prospective study. Arch. Ophthalmol. 2008, 126, 102–109. [Google Scholar] [CrossRef]
- Ravindran, R.D.; Vashist, P.; Gupta, S.K.; Young, I.S.; Maraini, G.; Camparini, M.; Jayanthi, R.; John, N.; Fitzpatrick, K.E.; Chakravarthy, U.; et al. Inverse association of vitamin C with cataract in older people in India. Ophthalmology 2011, 118, 1958–1965.e2. [Google Scholar] [CrossRef] [PubMed]
- Glaser, T.S.; Doss, L.E.; Shih, G.; Nigam, D.; Sperduto, R.D.; Ferris, F.L., 3rd; Agrón, E.; Clemons, T.E.; Chew, E.Y. The Association of Dietary Lutein plus Zeaxanthin and B Vitamins with Cataracts in the Age-Related Eye Disease Study: AREDS Report No. 37. Ophthalmology 2015, 122, 1471–1479. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.; Wu, L.; Qiu, L.; Lai, J.; Huang, Z.; Liao, L. Association between vegetables consumption and the risk of age-related cataract: A meta-analysis. Int. J. Clin. Exp. Med. 2015, 8, 18455–18461. [Google Scholar] [PubMed]
- Jiang, H.; Yin, Y.; Wu, C.R.; Liu, Y.; Guo, F.; Li, M.; Ma, L. Dietary vitamin and carotenoid intake and risk of age-related cataract. Am. J. Clin. Nutr. 2019, 109, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Chiu, T.H.T.; Chang, C.C.; Lin, C.L.; Lin, M.N. A Vegetarian Diet Is Associated with a Lower Risk of Cataract, Particularly Among Individuals with Overweight: A Prospective Study. J. Acad. Nutr. Diet 2021, 121, 669–677.e1. [Google Scholar] [CrossRef] [PubMed]
- Schaumberg, D.A.; Liu, S.; Seddon, J.M.; Willett, W.C.; Hankinson, S.E. Dietary glycemic load and risk of age-related cataract. Am. J. Clin. Nutr. 2004, 80, 489–495. [Google Scholar] [CrossRef][Green Version]
- Chiu, C.J.; Milton, R.C.; Gensler, G.; Taylor, A. Dietary carbohydrate intake and glycemic index in relation to cortical and nuclear lens opacities in the Age-Related Eye Disease Study. Am. J. Clin. Nutr. 2006, 83, 1177–1184. [Google Scholar] [CrossRef][Green Version]
- Tan, J.; Wang, J.J.; Flood, V.; Kaushik, S.; Barclay, A.; Brand-Miller, J.; Mitchell, P. Carbohydrate nutrition, glycemic index, and the 10-y incidence of cataract. Am. J. Clin. Nutr. 2007, 86, 1502–1508. [Google Scholar] [CrossRef][Green Version]
- Rautiainen, S.; Lindblad, B.E.; Morgenstern, R.; Wolk, A. Total antioxidant capacity of the diet and risk of age-related cataract: A population-based prospective cohort of women. JAMA Ophthalmol. 2014, 132, 247–252. [Google Scholar] [CrossRef]
- Mares, J. Food antioxidants to prevent cataract. Jama 2015, 313, 1048–1049. [Google Scholar] [CrossRef]
- Salari-Moghaddam, A.; Nouri-Majd, S.; Keshteli, A.H.; Emami, F.; Esmaillzadeh, A.; Adibi, P. Association Between Dietary Total Antioxidant Capacity and Diet Quality in Adults. Front. Nutr. 2022, 9, 838752. [Google Scholar] [CrossRef] [PubMed]
- Aleksandrova, K.; Koelman, L.; Rodrigues, C.E. Dietary patterns and biomarkers of oxidative stress and inflammation: A systematic review of observational and intervention studies. Redox Biol. 2021, 42, 101869. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All | Non-Cataract | Cataract | p Value | |
|---|---|---|---|---|
| Number | 6395 | 5712 (89.3) | 683 (10.7) | |
| Gender (N, %) | 0.034 | |||
| Male | 3115 (48.7) | 2809 (49.2) | 306 (44.8) | |
| Female | 3280 (51.3) | 2903 (50.8) | 377 (55.2) | |
| Age (years, mean (SD)) | 48.7 (15.3) | 51.7 (14.1) | 74.4 (9.0) | <0.001 |
| Race (N, %) | <0.001 | |||
| Non-Hispanic White | 3333 (52.1) | 2840 (49.7) | 493 (72.2) | |
| Non-Hispanic Black | 1345 (21.0) | 1258 (22.0) | 87 (12.7) | |
| Mexican American | 1061 (16.6) | 1009 (17.7) | 52 (7.6) | |
| Other | 656 (10.3) | 605 (10.6) | 51 (7.5) | |
| Education (N, %) | <0.001 | |||
| Less than high school | 1712 (26.6) | 1476 (25.8) | 236 (34.6) | |
| High school or above | 4683 (73.4) | 4236 (74.2) | 447 (65.4) | |
| Marital status (N, %) | <0.001 | |||
| Unmarried or other | 2236 (35.0) | 1911 (33.5) | 325 (47.6) | |
| Married or living with partner | 4159 (65.3) | 3801 (66.5) | 358 (52.4) | |
| Economic situation (N, %) | <0.001 | |||
| Below poverty | 1018 (15.9) | 933 (16.3) | 85 (12.4) | |
| Poverty or above | 5377 (84.1) | 4779 (83.7) | 598 (87.6) | |
| BMI (N, %) | 0.018 | |||
| <18.5 | 83 (1.3) | 75 (1.3) | 8 (1.2) | |
| 18.5~25 | 1617 (25.3) | 1414 (24.8) | 203 (29.7) | |
| ≥25 | 4695 (73.4) | 4223 (73.9) | 472 (69.1) | |
| Alcohol usage (N, %) | <0.001 | |||
| Lifetime abstainer | 970 (15.2) | 805 (14.1) | 165 (24.2) | |
| Former drinker | 1079 (16.9) | 905 (15.8) | 174 (25.5) | |
| Current drinker ≤ 3 drinks/week | 2686 (42.0) | 2473 (43.3) | 213 (31.2) | |
| Current drinker > 3 drinks/week | 1660 (26.0) | 1529 (26.8) | 131 (19.2) | |
| Smoking (N, %) | <0.001 | |||
| Never smoke | 3305 (51.7) | 2973 (52.0) | 332 (48.6) | |
| Former smoker | 1842 (28.8) | 1550 (27.1) | 292 (42.8) | |
| Current smoker | 1248 (19.5) | 1189 (20.8) | 59 (8.6) | |
| Hypertension (N, %) | <0.001 | |||
| No | 3122 (48.8) | 2958 (51.8) | 164 (24.0) | |
| Yes | 3273 (51.2) | 2754 (48.2) | 519 (76.0) | |
| Hyperlipidemia (N, %) | <0.001 | |||
| No | 3566 (55.8) | 3262 (57.1) | 304 (44.5) | |
| Yes | 2829 (44.2) | 2450 (42.9) | 379 (55.5) | |
| Diabetes mellitus (N, %) | <0.001 | |||
| No | 5370 (84.0) | 4880 (85.4) | 490 (71.7) | |
| Yes | 1025 (16.0) | 832 (14.6) | 193 (28.3) | |
| HEI-2015 (mean (SD)) | 49.5 (14.6) | 49.8 (14.6) | 53.0 (14.3) | <0.001 |
| HEI-2015 quartile (N, %) | ||||
| Q1 (9.3–39.6) | 1599 (25.0) | 1473 (25.8) | 126 (18.4) | <0.001 |
| Q2 (39.6–49.5) | 1599 (25.0) | 1447 (25.3) | 152 (22.3) | |
| Q3 (49.5–60.2) | 1598 (25.0) | 1412 (24.7) | 186 (27.2) | |
| Q4 (60.2–96.1) | 1599 (25.0) | 1380 (24.2) | 219 (32.1) |
| Model 1 a | Model 2 b | Model 3 c | |
|---|---|---|---|
| HEI-2015 | 1.019 (1.014–1.024), <0.001 | 0.991 (0.984–0.997), 0.002 | 0.991 (0.984–0.997), 0.006 |
| HEI-2015 quartile | |||
| Q1 | Ref | Ref | Ref |
| Q2 | 1.197 (0.932–1.539), 0.160 | 0.857 (0.633–1.162), 0.320 | 0.856 (0.630–1.164), 0.320 |
| Q3 | 1.586 (1.251–2.016), <0.001 | 0.838 (0.627–1.121), 0.232 | 0.841 (0.630–1.131), 0.251 |
| Q4 | 2.121 (1.692–2.671), <0.001 | 0.751 (0.569–0.940), 0.044 | 0.739 (0.559–0.980), 0.035 |
| Model 1 a | Model 2 b | Model 3 c | |
|---|---|---|---|
| HEI-2015 | 0.991 (0.985–0.996), <0.001 | 0.992 (0.984–0.996), 0.002 | 0.990 (0.984–0.995), 0.002 |
| HEI-2015 quartile | |||
| Q1 | Ref | Ref | Ref |
| Q2 | 0.770 (0.625–0.947), 0.014 | 0.824 (0.637–1.064), 0.139 | 0.824 (0.634–1.068), 0.144 |
| Q3 | 0.760 (0.616–0.936), 0.010 | 0.779 (0.601–1.008), 0.058 | 0.780 (0.600–1.012), 0.062 |
| Q4 | 0.748 (0.605–0.923), 0.007 | 0.747 (0.576–0.967), 0.027 | 0.744 (0.572–0.967), 0.027 |
| HEI-2015 Component Score | Model 1 a | Model 2 b | Model 3 c |
|---|---|---|---|
| Adequacy component score | |||
| Total fruits | 1.135 (1.093–1.179), <0.001 | 0.939 (0.895–0.984), 0.008 | 0.947 (0.903–0.993), 0.027 |
| Whole fruits | 1.114 (1.076–1.153), <0.001 | 0.945 (0.905–0.985), 0.009 | 0.948 (0.907–0.991), 0.016 |
| Total vegetables | 1.094 (1.042–1.149), <0.001 | 0.991 (0.936–1.050), 0.763 | 0.985 (0.930–1.044), 0.610 |
| Greens and beans | 0.981 (0.943–1.020), 0.349 | 0.990 (0.953–1.046), 0.965 | 1.005 (0.959–1.054), 0.820 |
| Total protein foods | 0.939 (0.883–0.998), 0.042 | 0.986 (0.915–1.064), 0.718 | 0.979 (0.907–1.057), 0.581 |
| Seafood and plant proteins | 1.002 (0.967–1.040), 0.870 | 0.974 (0.933–1.017), 0.239 | 0.983 (0.941–1.027), 0.446 |
| Whole grains | 1.076 (1.051–1.102), <0.001 | 0.968 (0.940–0.997), 0.029 | 0.966 (0.937–0.995), 0.024 |
| Dairy | 1.030 (1.006–1.054), 0.013 | 0.981 (0.953–1.010), 0.198 | 0.981 (0.953–1.010), 0.201 |
| Fatty acids | 0.999 (0.977–1.021), 0.941 | 1.003 (0.977–1.030), 0.806 | 1.004 (0.978–1.031), 0.752 |
| Moderation component score | |||
| Sodium | 0.975 (0.954–0.997), 0.252 | 0.972 (0.947–0.997), 0.031 | 0.979 (0.954–1.005), 0.113 |
| Refined grains | 0.995 (0.974–1.017), 0.672 | 0.953 (0.927–0.979), <0.001 | 0.958 (0.932–0.985), 0.002 |
| Added sugars | 0.987 (0.968–1.006), 0.071 | 0.964 (0.929–1.000), 0.050 | 0.971 (0.916–1.026), 0.485 |
| Saturated fats | 1.034 (1.021–1.048), <0.001 | 1.003 (0.987–1.019), 0.696 | 1.001 (0.984–1.017), 0.935 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, J.; Lou, L.; Jin, K.; Ye, J. Association between Healthy Eating Index-2015 and Age-Related Cataract in American Adults: A Cross-Sectional Study of NHANES 2005–2008. Nutrients 2023, 15, 98. https://doi.org/10.3390/nu15010098
Zhou J, Lou L, Jin K, Ye J. Association between Healthy Eating Index-2015 and Age-Related Cataract in American Adults: A Cross-Sectional Study of NHANES 2005–2008. Nutrients. 2023; 15(1):98. https://doi.org/10.3390/nu15010098
Chicago/Turabian StyleZhou, Jingxin, Lixia Lou, Kai Jin, and Juan Ye. 2023. "Association between Healthy Eating Index-2015 and Age-Related Cataract in American Adults: A Cross-Sectional Study of NHANES 2005–2008" Nutrients 15, no. 1: 98. https://doi.org/10.3390/nu15010098
APA StyleZhou, J., Lou, L., Jin, K., & Ye, J. (2023). Association between Healthy Eating Index-2015 and Age-Related Cataract in American Adults: A Cross-Sectional Study of NHANES 2005–2008. Nutrients, 15(1), 98. https://doi.org/10.3390/nu15010098