
Effectiveness and Components of Web-Based Interventions on Weight Changes in Adults Who Were Overweight and Obese: A Systematic Review with Meta-Analyses

 , , and
, , and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Methods
2.2. Criteria for Exclusion
2.3. Selection Process and Data Extraction
2.4. Data Synthesis
2.4.1. Quality of Evidence
2.4.2. Qualitative Analysis
2.4.3. Quantitative Analysis
2.4.4. Subgroup Analysis
3. Results
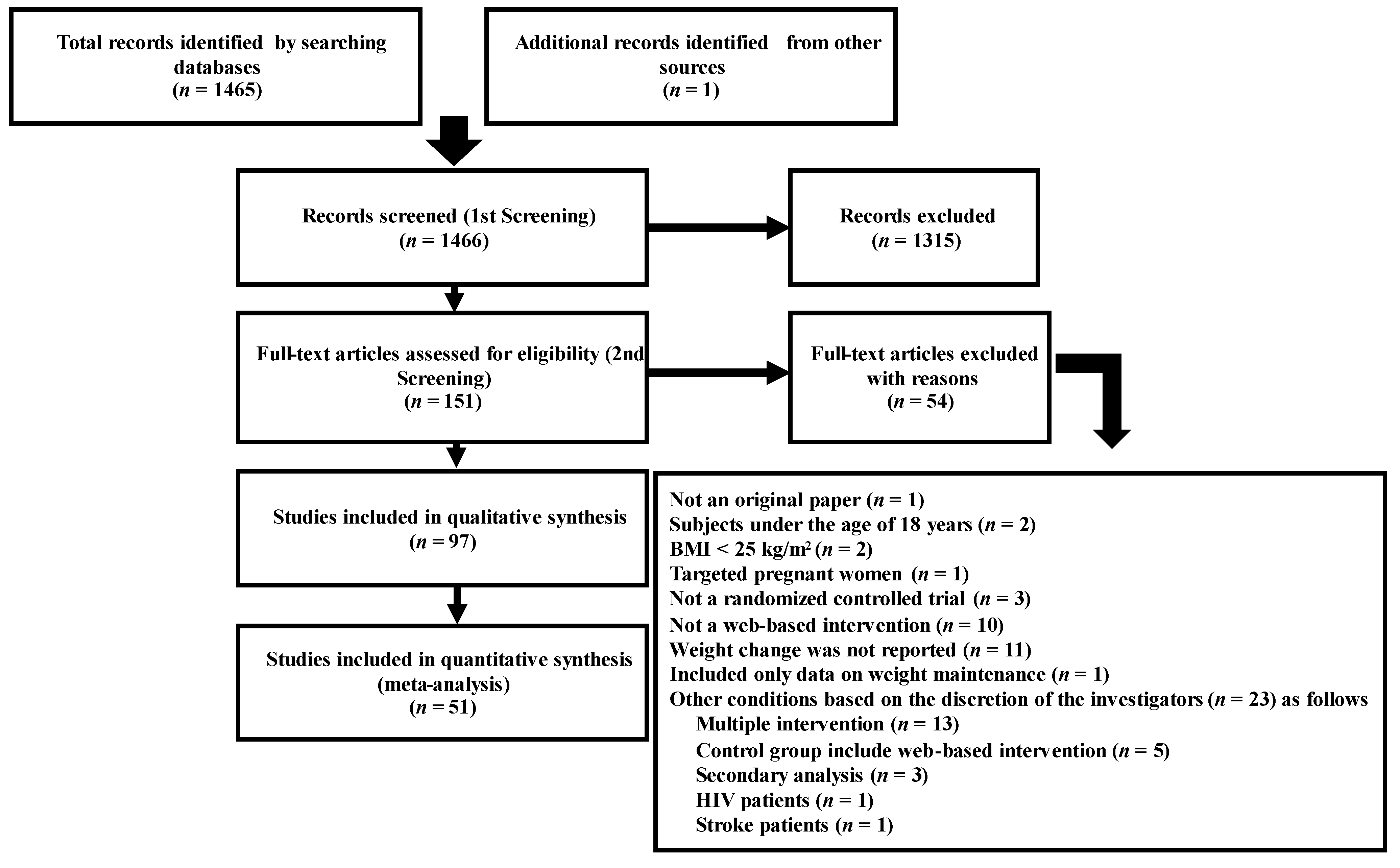
3.1. Description of Included Studies
3.2. Quality of the Evidence
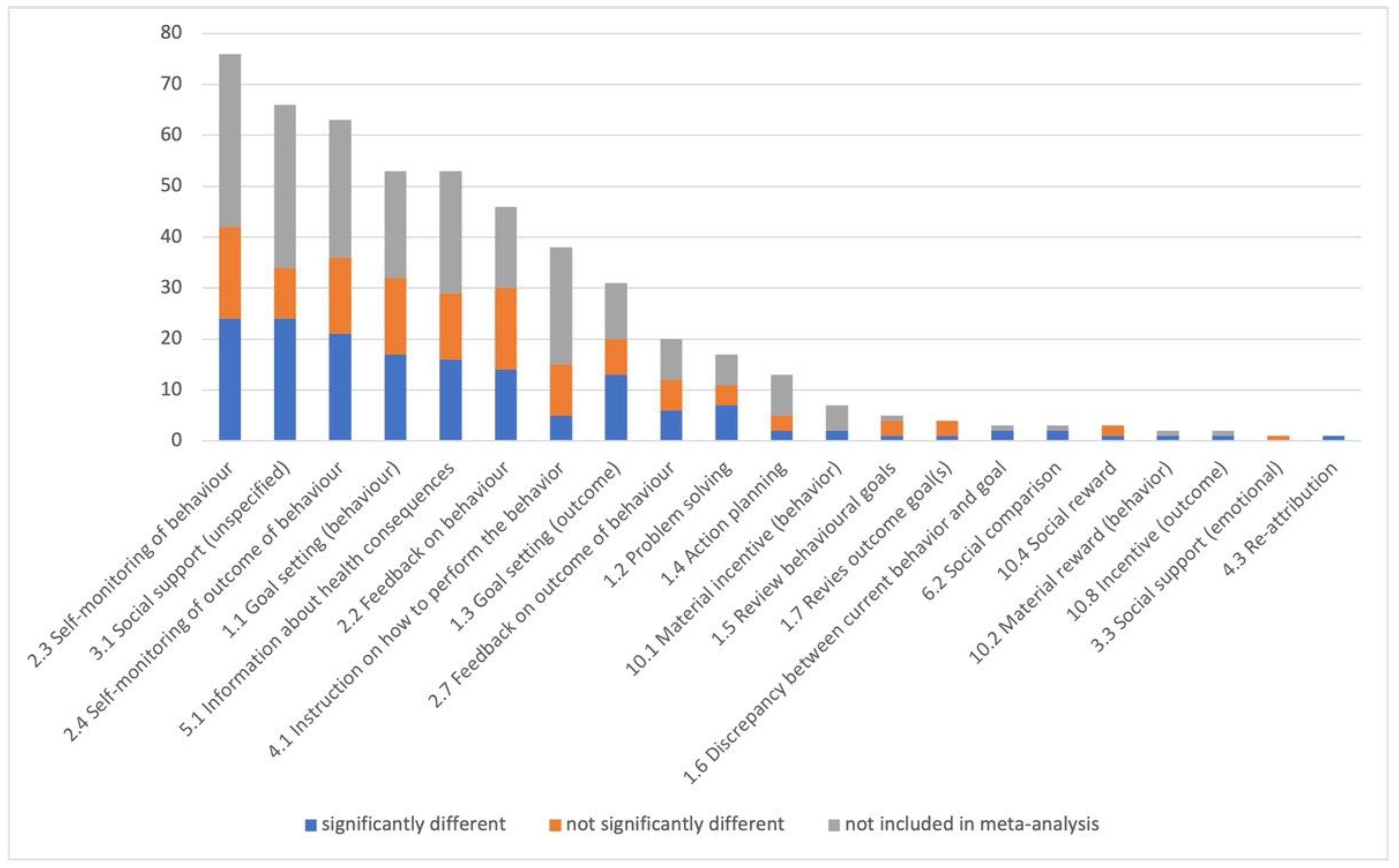
3.3. Qualitative Analysis
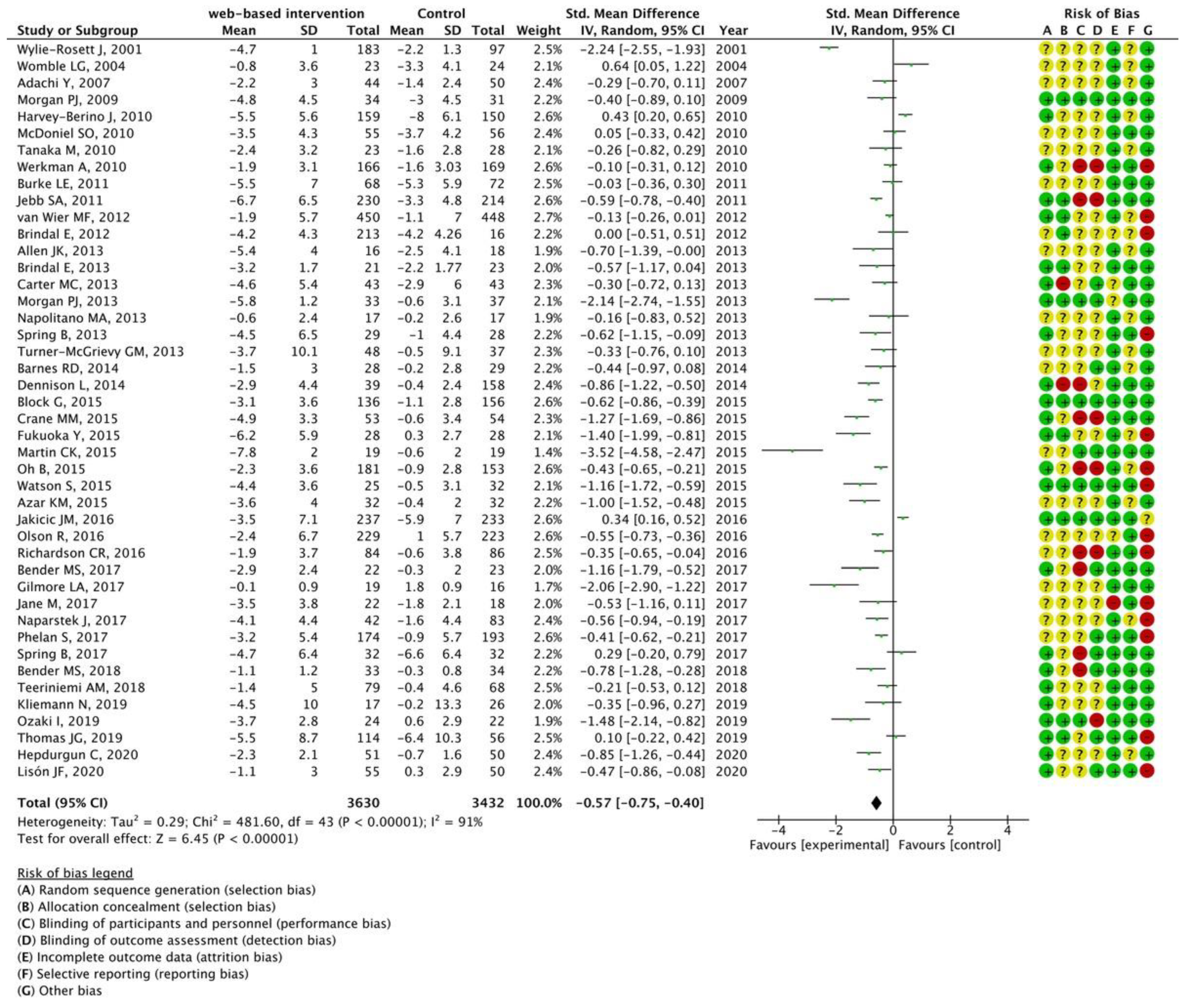
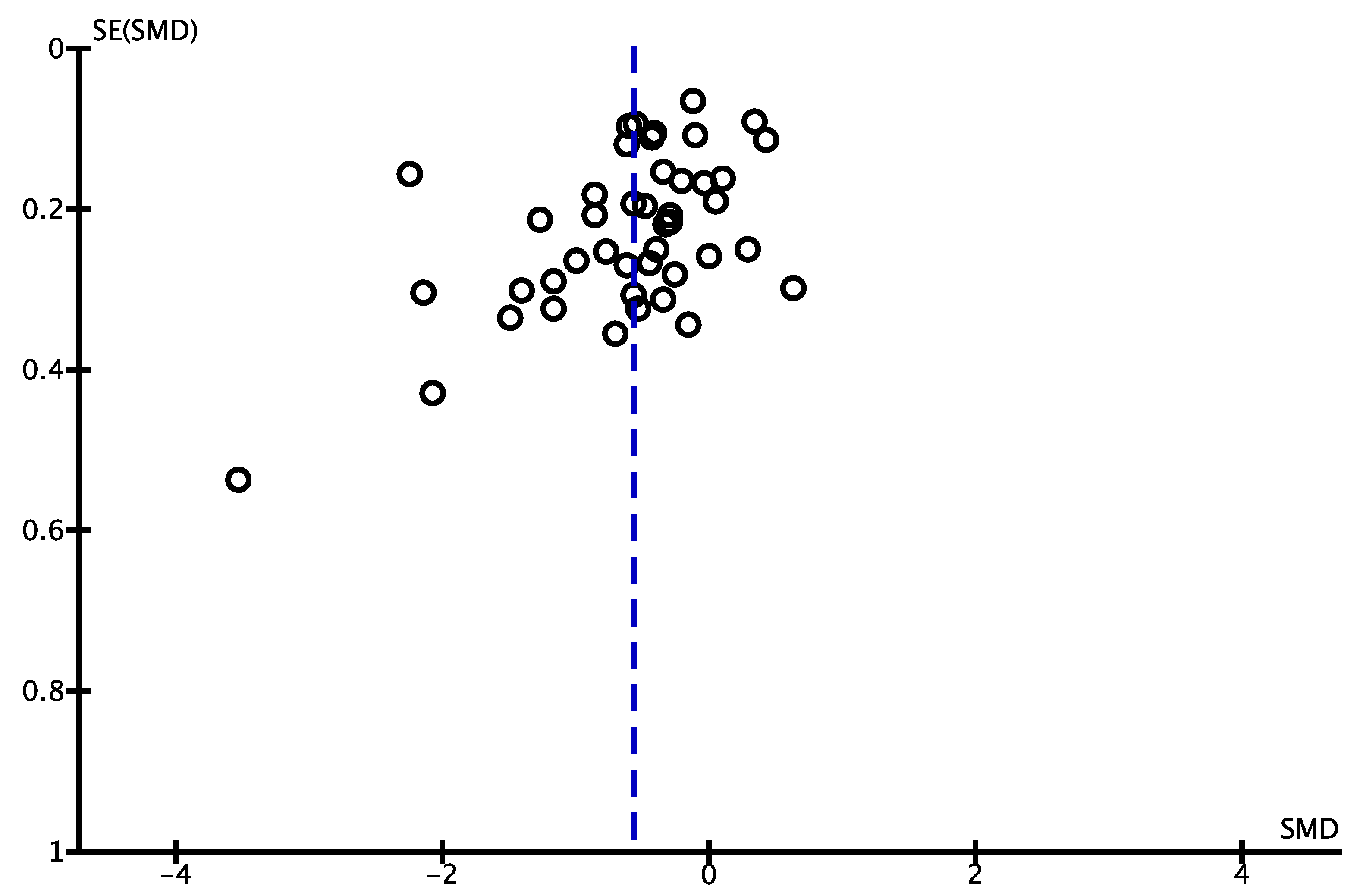
3.4. Quantitative Analysis
3.5. Subgroup Analyses
3.5.1. Intervention Medium (Computer or Smartphone)
3.5.2. Publication Year
3.5.3. Intervention Period
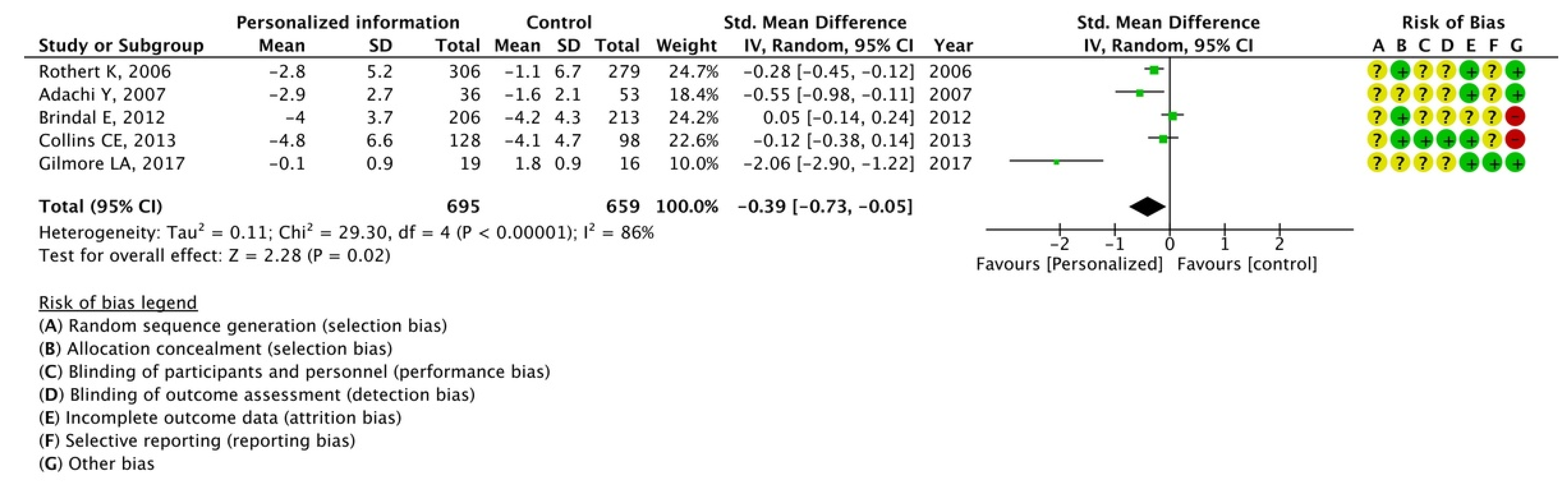
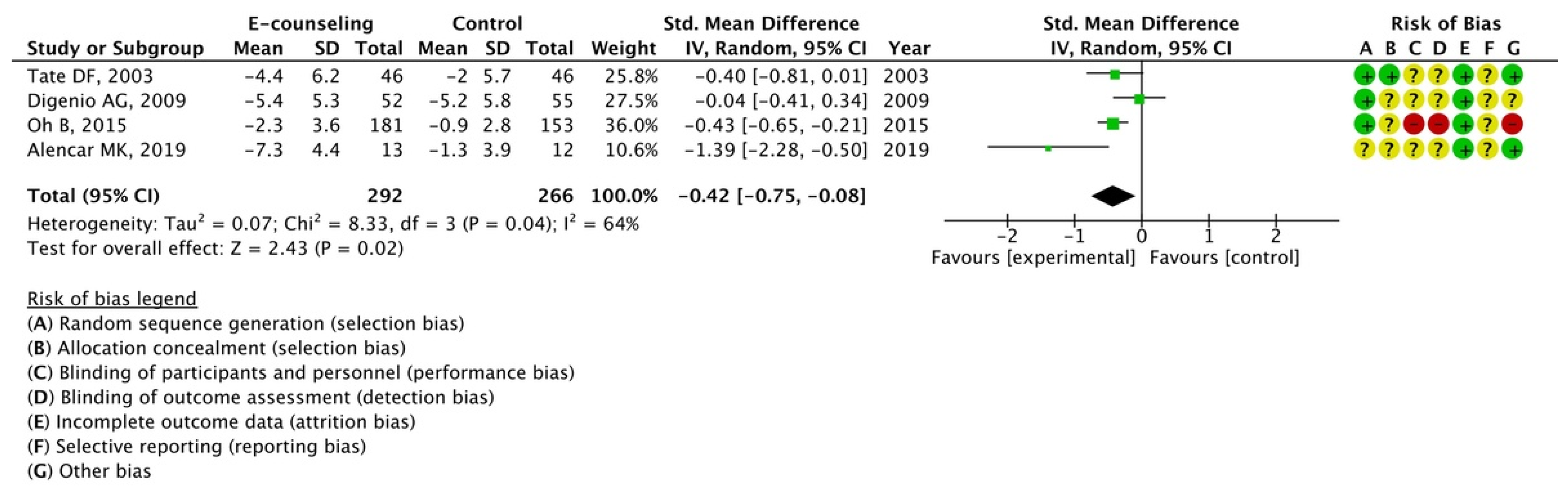
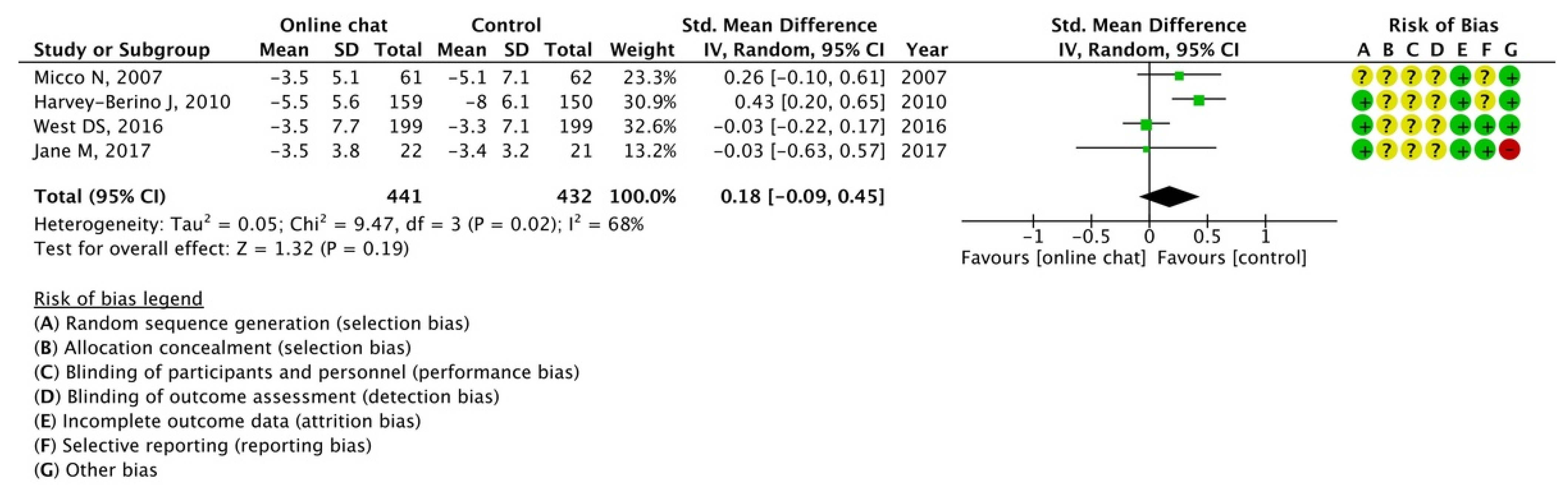
3.5.4. Intervention Component
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Obesity and Overweight. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 2 April 2022).
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults. Circulation 2014, 129, S102–S138. [Google Scholar] [CrossRef] [PubMed]
- Kemp, S. Digital. DataReportal–Global Digital Insights. Oct. Glob. Statshot Rep. 2021, 2021. Available online: https://datareportal.com/reports/6-in-10-people-around-the-world-now-use-the-internet (accessed on 18 April 2022).
- Sullivan, A.N.; Lachman, M.E. Behavior change with fitness technology in sedentary adults: A review of the evidence for increasing physical activity. Front. Public Health 2016, 4, 289. [Google Scholar] [CrossRef]
- Buckingham, S.A.; Williams, A.J.; Morrissey, K.; Price, L.; Harrison, J. Mobile health interventions to promote physical activity and reduce sedentary behaviour in the workplace: A systematic review. Digit Health 2019, 5, 2055207619839883. [Google Scholar] [CrossRef] [PubMed]
- Beleigoli, A.M.; Andrade, A.Q.; Cançado, A.G.; Paulo, M.N.; Diniz, M.F.H.; Ribeiro, A.L. Web-based digital health interventions for weight loss and lifestyle habit changes in overweight and obese adults: Systematic review and meta-analysis. J. Med. Internet Res. 2019, 21, e298. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- NPO Japan Medical Abstracts Society. About “ICHUSHI”. 2018. Available online: https://www.jamas.or.jp/english/ (accessed on 2 April 2022).
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Werkman, A.; Hulshof, P.J.; Stafleu, A.; Kremers, S.P.; Kok, F.J.; Schouten, E.G.; Schuit, A.J. Effect of an individually tailored one-year energy balance programme on body weight, body composition and lifestyle in recent retirees: A cluster randomised controlled trial. BMC Public Health 2010, 10, 110. [Google Scholar] [CrossRef]
- Wylie-Rosett, J.; Swencionis, C.; Ginsberg, M.; Cimino, C.; Wassertheil-Smoller, S.; Caban, A.; Segal-Isaacson, C.J.; Martin, T.; Lewis, J. Computerized weight loss intervention optimizes staff time: The clinical and cost results of a controlled clinical trial conducted in a managed care setting. J. Am. Diet Assoc. 2001, 101, 1155–1162; quiz 1163. [Google Scholar] [CrossRef]
- Tate, D.F.; Jackvony, E.H.; Wing, R.R. Effects of Internet behavioral counseling on weight loss in adults at risk for type 2 diabetes: A randomized trial. JAMA 2003, 289, 1833–1836. [Google Scholar] [CrossRef] [PubMed]
- Womble, L.G.; Wadden, T.A.; McGuckin, B.G.; Sargent, S.L.; Rothman, R.A.; Krauthamer-Ewing, E.S. A randomized controlled trial of a commercial internet weight loss program. Obes. Res. 2004, 12, 1011–1018. [Google Scholar] [CrossRef] [PubMed]
- Rothert, K.; Strecher, V.J.; Doyle, L.A.; Caplan, W.M.; Joyce, J.S.; Jimison, H.B.; Karm, L.M.; Mims, A.D.; Roth, M.A. Web-based weight management programs in an integrated health care setting: A randomized, controlled trial. Obesity 2006, 14, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Adachi, Y.; Sato, C.; Yamatsu, K.; Ito, S.; Adachi, K.; Yamagami, T. A randomized controlled trial on the long-term effects of a 1-month behavioral weight control program assisted by computer tailored advice. Behav. Res. Ther. 2007, 45, 459–470. [Google Scholar] [CrossRef]
- Micco, N.; Gold, B.; Buzzell, P.; Leonard, H.; Pintauro, S.; Harvey-Berino, J. Minimal in-person support as an adjunct to internet obesity treatment. Ann. Behav. Med. 2007, 33, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Digenio, A.G.; Mancuso, J.P.; Gerber, R.A.; Dvorak, R.V. Comparison of methods for delivering a lifestyle modification program for obese patients: A randomized trial. Ann. Intern. Med. 2009, 150, 255–262. [Google Scholar] [CrossRef]
- Morgan, P.J.; Lubans, D.R.; Collins, C.E.; Warren, J.M.; Callister, R. The SHED-IT randomized controlled trial: Evaluation of an Internet-based weight-loss program for men. Obesity 2009, 17, 2025–2032. [Google Scholar] [CrossRef]
- Harvey-Berino, J.; West, D.; Krukowski, R.; Prewitt, E.; VanBiervliet, A.; Ashikaga, T.; Skelly, J. Internet delivered behavioral obesity treatment. Prev. Med. 2010, 51, 123–128. [Google Scholar] [CrossRef]
- McDoniel, S.O.; Wolskee, P.; Shen, J. Treating obesity with a novel hand-held device, computer software program, and Internet technology in primary care: The SMART motivational trial. Patient Educ. Couns. Patient Educ. Couns. 2010, 79, 185–191. [Google Scholar] [CrossRef]
- Tanaka, M.; Adachi, Y.; Adachi, K.; Sato, C. Effects of a non-face-to-face behavioral weight-control program among Japanese overweight males: A randomized controlled trial. Int. J. Behav. Med. 2010, 17, 17–24. [Google Scholar] [CrossRef]
- Burke, L.E.; Conroy, M.B.; Sereika, S.M.; Elci, O.U.; Styn, M.A.; Acharya, S.D.; Sevick, M.A.; Ewing, L.J.; Glanz, K. The effect of electronic self-monitoring on weight loss and dietary intake: A randomized behavioral weight loss trial. Obesity 2011, 19, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Jebb, S.A.; Ahern, A.L.; Olson, A.D.; Aston, L.M.; Holzapfel, C.; Stoll, J.; Amann-Gassner, U.; Simpson, A.E.; Fuller, N.R.; Pearson, S.; et al. Primary care referral to a commercial provider for weight loss treatment versus standard care: A randomised controlled trial. Lancet 2011, 378, 1485–1492. [Google Scholar] [CrossRef]
- Brindal, E.; Freyne, J.; Saunders, I.; Berkovsky, S.; Smith, G.; Noakes, M. Features predicting weight loss in overweight or obese participants in a web-based intervention: Randomized trial. J. Med. Internet Res. 2012, 14, e173. [Google Scholar] [CrossRef]
- van Wier, M.F.; Dekkers, J.C.; Bosmans, J.E.; Heymans, M.W.; Hendriksen, I.J.; Pronk, N.P.; van Mechelen, W.; van Tulder, M.W. Economic evaluation of a weight control program with e-mail and telephone counseling among overweight employees: A randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 112. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.K.; Stephens, J.; Dennison Himmelfarb, C.R.; Stewart, K.J.; Hauck, S. Randomized controlled pilot study testing use of smartphone technology for obesity treatment. J. Obes. 2013, 2013, 151597. [Google Scholar] [CrossRef] [PubMed]
- Brindal, E.; Hendrie, G.; Freyne, J.; Coombe, M.; Berkovsky, S.; Noakes, M. Design and pilot results of a mobile phone weight-loss application for women starting a meal replacement programme. J. Telemed. Telecare. 2013, 19, 166–174. [Google Scholar] [CrossRef]
- Carter, M.C.; Burley, V.J.; Nykjaer, C.; Cade, J.E. Adherence to a smartphone application for weight loss compared to website and paper diary: Pilot randomized controlled trial. J. Med. Internet Res. 2013, 15, e32. [Google Scholar] [CrossRef]
- Collins, C.E.; Morgan, P.J.; Hutchesson, M.J.; Callister, R. Efficacy of standard versus enhanced features in a web-based commercial weight-loss program for obese adults, part 2: Randomized controlled trial. J. Med. Internet Res. 2013, 15, e140. [Google Scholar] [CrossRef]
- Morgan, P.J.; Callister, R.; Collins, C.E.; Plotnikoff, R.C.; Young, M.D.; Berry, N.; McElduff, P.; Burrows, T.; Aguiar, E.; Saunders, K.L. The SHED-IT community trial: A randomized controlled trial of internet- and paper-based weight loss programs tailored for overweight and obese men. Ann. Behav. Med. 2013, 45, 139–152. [Google Scholar] [CrossRef]
- Napolitano, M.A.; Hayes, S.; Bennett, G.G.; Ives, A.K.; Foster, G.D. Using Facebook and text messaging to deliver a weight loss program to college students. Obesity 2013, 21, 25–31. [Google Scholar] [CrossRef]
- Spring, B.; Duncan, J.M.; Janke, E.A.; Kozak, A.T.; McFadden, H.G.; DeMott, A.; Pictor, A.; Epstein, L.H.; Siddique, J.; Pellegrini, C.A.; et al. Integrating technology into standard weight loss treatment: A randomized controlled trial. JAMA Intern. Med. 2013, 173, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Turner-McGrievy, G.M.; Beets, M.W.; Moore, J.B.; Kaczynski, A.T.; Barr-Anderson, D.J.; Tate, D.F. Comparison of traditional versus mobile app self-monitoring of physical activity and dietary intake among overweight adults participating in an mhealth weight loss program. J. Am. Med. Inform. Assoc. 2013, 20, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Barnes, R.D.; White, M.A.; Martino, S.; Grilo, C.M. A randomized controlled trial comparing scalable weight loss treatments in primary care. Obesity 2014, 22, 2508–2516. [Google Scholar] [CrossRef] [PubMed]
- Dennison, L.; Morrison, L.; Lloyd, S.; Phillips, D.; Stuart, B.; Williams, S.; Bradbury, K.; Roderick, P.; Murray, E.; Michie, S.; et al. Does brief telephone support improve engagement with a web-based weight management intervention? Randomized controlled trial. J. Med. Internet Res. 2014, 16, e95. [Google Scholar] [CrossRef]
- Azar, K.M.; Aurora, M.; Wang, E.J.; Muzaffar, A.; Pressman, A.; Palaniappan, L.P. Virtual small groups for weight management: An innovative delivery mechanism for evidence-based lifestyle interventions among obese men. Transl. Behav. Med. 2015, 5, 37–44. [Google Scholar] [CrossRef]
- Block, G.; Azar, K.M.; Romanelli, R.J.; Block, T.J.; Hopkins, D.; Carpenter, H.A.; Dolginsky, M.S.; Hudes, M.L.; Palaniappan, L.P.; Block, C.H.; et al. Diabetes prevention and weight loss with a fully automated behavioral intervention by email, web, and mobile phone: A randomized controlled trial among persons with prediabetes [Web]. J. Med. Internet Res. 2015, 17, e240. [Google Scholar] [CrossRef]
- Crane, M.M.; Lutes, L.D.; Ward, D.S.; Bowling, J.M.; Tate, D.F. A randomized trial testing the efficacy of a novel approach to weight loss among men with overweight and obesity. Obesity 2015, 23, 2398–2405. [Google Scholar] [CrossRef]
- Fukuoka, Y.; Gay, C.L.; Joiner, K.L.; Vittinghoff, E. A novel diabetes prevention intervention using a mobile app: A randomized controlled trial with overweight adults at risk. Am. J. Prev. Med. 2015, 49, 223–237. [Google Scholar] [CrossRef]
- Martin, C.K.; Miller, A.C.; Thomas, D.M.; Champagne, C.M.; Han, H.; Church, T. Efficacy of SmartLoss, a smartphone-based weight loss intervention: Results from a randomized controlled trial. Obesity 2015, 23, 935–942. [Google Scholar] [CrossRef]
- Oh, B.; Cho, B.; Han, M.K.; Choi, H.; Lee, M.N.; Kang, H.C.; Lee, C.H.; Yun, H.; Kim, Y. The effectiveness of mobile phone-based care for weight control in metabolic syndrome patients: Randomized controlled trial. JMIR MHealth UHealth. 2015, 3, e83. [Google Scholar] [CrossRef]
- Watson, S.; Woodside, J.V.; Ware, L.J.; Hunter, S.J.; McGrath, A.; Cardwell, C.R.; Appleton, K.M.; Young, I.S.; McKinley, M.C. Effect of a web-based behavior change program on weight loss and cardiovascular risk factors in overweight and obese adults at high risk of developing cardiovascular disease: Randomized controlled trial. J. Med. Internet Res. 2015, 17, e177. [Google Scholar] [CrossRef] [PubMed]
- Jakicic, J.M.; Davis, K.K.; Rogers, R.J.; King, W.C.; Marcus, M.D.; Helsel, D.; Rickman, A.D.; Wahed, A.S.; Belle, S.H. Effect of wearable technology combined with a lifestyle intervention on long-term weight loss: The IDEA randomized clinical trial. JAMA 2016, 316, 1161–1171. [Google Scholar] [CrossRef] [PubMed]
- Olson, R.; Wipfli, B.; Thompson, S.V.; Elliot, D.L.; Anger, W.K.; Bodner, T.; Hammer, L.B.; Perrin, N.A. Weight control intervention for truck drivers: The shift randomized controlled trial, United States. Am. J. Public Health 2016, 106, 1698–1706. [Google Scholar] [CrossRef] [PubMed]
- Richardson, C.R.; Goodrich, D.E.; Larkin, A.R.; Ronis, D.; Holleman, R.G.; Damschroder, L.J.; Lowery, J.C. A comparative effectiveness trial of three walking self-monitoring strategies. Transl. J. Am. Coll. Sports Med. 2016, 1, 133–142. [Google Scholar] [CrossRef] [PubMed]
- West, D.S.; Harvey, J.R.; Krukowski, R.A.; Prewitt, T.E.; Priest, J.; Ashikaga, T. Do individual, online motivational interviewing chat sessions enhance weight loss in a group-based, online weight control program? Obesity 2016, 24, 2334–2340. [Google Scholar] [CrossRef] [PubMed]
- Bender, M.S.; Cooper, B.A.; Park, L.G.; Padash, S.; Arai, S. A feasible and efficacious mobile-phone based lifestyle intervention for Filipino Americans with type 2 diabetes: Randomized controlled trial. JMIR Diabetes 2017, 2, e30. [Google Scholar] [CrossRef]
- Gilmore, L.A.; Klempel, M.C.; Martin, C.K.; Myers, C.A.; Burton, J.H.; Sutton, E.F.; Redman, L.M. Personalized mobile health intervention for health and weight loss in postpartum women receiving women, infants, and children benefit: A randomized controlled pilot study. J. Womens Health 2017, 26, 719–727. [Google Scholar] [CrossRef]
- Jane, M.; Hagger, M.; Foster, J.; Ho, S.; Kane, R.; Pal, S. Effects of a weight management program delivered by social media on weight and metabolic syndrome risk factors in overweight and obese adults: A randomised controlled trial. PLoS ONE 2017, 12, e0178326. [Google Scholar] [CrossRef]
- Naparstek, J.; Wing, R.R.; Xu, X.; Leahey, T.M. Internet-delivered obesity treatment improves symptoms of and risk for depression. Obesity 2017, 25, 671–675. [Google Scholar] [CrossRef]
- Phelan, S.; Hagobian, T.; Brannen, A.; Hatley, K.E.; Schaffner, A.; Muñoz-Christian, K.; Tate, D.F. Effect of an internet-based program on weight loss for low-income postpartum women: A randomized clinical trial. JAMA 2017, 317, 2381–2391. [Google Scholar] [CrossRef]
- Spring, B.; Pellegrini, C.A.; Pfammatter, A.; Duncan, J.M.; Pictor, A.; McFadden, H.G.; Siddique, J.; Hedeker, D. Effects of an abbreviated obesity intervention supported by mobile technology: The ENGAGED randomized clinical trial. Obesity 2017, 25, 1191–1198. [Google Scholar] [CrossRef] [PubMed]
- Bender, M.S.; Cooper, B.A.; Flowers, E.; Ma, R.; Arai, S. Filipinos Fit and Trim–A feasible and efficacious DPP-based intervention trial. Contemp. Clin. Trials Commun. 2018, 12, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Teeriniemi, A.M.; Salonurmi, T.; Jokelainen, T.; Vähänikkilä, H.; Alahäivälä, T.; Karppinen, P.; Enwald, H.; Huotari, M.L.; Laitinen, J.; Oinas-Kukkonen, H.; et al. A randomized clinical trial of the effectiveness of a web-based health behaviour change support system and group lifestyle counselling on body weight loss in overweight and obese subjects: 2-year outcomes. J. Intern. Med. 2018, 284, 534–545. [Google Scholar] [CrossRef]
- Alencar, M.K.; Johnson, K.; Mullur, R.; Gray, V.; Gutierrez, E.; Korosteleva, O. The efficacy of a telemedicine-based weight loss program with video conference health coaching support. J. Telemed. Telecare 2019, 25, 151–157. [Google Scholar] [CrossRef]
- Kliemann, N.; Croker, H.; Johnson, F.; Beeken, R.J. Development of the Top Tips habit-based weight loss app and preliminary indications of its usage, effectiveness, and acceptability: Mixed-methods pilot study. JMIR MHealth UHealth. 2019, 7, e12326. [Google Scholar] [CrossRef] [PubMed]
- Ozaki, I.; Watai, I.; Nishijima, M.; Saito, N. Randomized controlled trial of web-based weight-loss intervention with human support for male workers under 40. J. Occup. Health. 2019, 61, 110–120. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.G.; Bond, D.S.; Raynor, H.A.; Papandonatos, G.D.; Wing, R.R. Comparison of smartphone-based behavioral obesity treatment with gold standard group treatment and control: A randomized trial. Obesity 2019, 27, 572–580. [Google Scholar] [CrossRef] [PubMed]
- Hepdurgun, C.; Özalay, Ö.; Pırıldar, Ş.; Rudarlı Nalçakan, G.; Saygılı, L.F.; Seçkiner, S.; Ünalır, M.O.; Elbi, H. Testing an internet-based Turkish obesity behavioral therapy program: A randomized study. Türk. Psikiyatr. Derg. 2020, 31, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Lisón, J.F.; Palomar, G.; Mensorio, M.S.; Baños, R.M.; Cebolla-Martí, A.; Botella, C.; Benavent-Caballer, V.; Rodilla, E. Impact of a web-based exercise and nutritional education intervention in patients who are obese with hypertension: Randomized wait-list controlled trial. J. Med. Internet Res. 2020, 22, e14196. [Google Scholar] [CrossRef]
- Khaylis, A.; Yiaslas, T.; Bergstrom, J.; Gore-Felton, C. A review of efficacious technology-based weight-loss interventions: Five key components. Telemed. J. E Health 2010, 16, 931–938. [Google Scholar] [CrossRef]
- Roser, M.; Ritchie, H.; Ortiz-Ospina, E. Internet. 2015, Volume 2022. Available online: https://ourworldindata.org/internet (accessed on 23 May 2022).
- Pai, A. Fitness App Installs to Grow 60 Percent by 2017. 2013. Available online: https://www.mobihealthnews.com/23649/fitness-app-installs-to-grow-60-percent-by-2017 (accessed on 18 April 2022).
- Neve, M.; Morgan, P.J.; Jones, P.R.; Collins, C.E. Effectiveness of web-based interventions in achieving weight loss and weight loss maintenance in overweight and obese adults: A systematic review with meta-analysis. Obes. Rev. 2010, 11, 306–321. [Google Scholar] [CrossRef] [PubMed]
- Norman, G.J.; Zabinski, M.F.; Adams, M.A.; Rosenberg, D.E.; Yaroch, A.L.; Atienza, A.A. A review of ehealth interventions for physical activity and dietary behavior change. Am. J. Prev. Med. 2007, 33, 336–345. [Google Scholar] [CrossRef] [PubMed]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shi, Y.; Wakaba, K.; Kiyohara, K.; Hayashi, F.; Tsushita, K.; Nakata, Y. Effectiveness and Components of Web-Based Interventions on Weight Changes in Adults Who Were Overweight and Obese: A Systematic Review with Meta-Analyses. Nutrients 2023, 15, 179. https://doi.org/10.3390/nu15010179
Shi Y, Wakaba K, Kiyohara K, Hayashi F, Tsushita K, Nakata Y. Effectiveness and Components of Web-Based Interventions on Weight Changes in Adults Who Were Overweight and Obese: A Systematic Review with Meta-Analyses. Nutrients. 2023; 15(1):179. https://doi.org/10.3390/nu15010179
Chicago/Turabian StyleShi, Yutong, Kyohsuke Wakaba, Kosuke Kiyohara, Fumi Hayashi, Kazuyo Tsushita, and Yoshio Nakata. 2023. "Effectiveness and Components of Web-Based Interventions on Weight Changes in Adults Who Were Overweight and Obese: A Systematic Review with Meta-Analyses" Nutrients 15, no. 1: 179. https://doi.org/10.3390/nu15010179
APA StyleShi, Y., Wakaba, K., Kiyohara, K., Hayashi, F., Tsushita, K., & Nakata, Y. (2023). Effectiveness and Components of Web-Based Interventions on Weight Changes in Adults Who Were Overweight and Obese: A Systematic Review with Meta-Analyses. Nutrients, 15(1), 179. https://doi.org/10.3390/nu15010179