

Vitamin D3 Supplementation at 5000 IU Daily for the Prevention of Influenza-like Illness in Healthcare Workers: A Pragmatic Randomized Clinical Trial

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects and Regulatory Approval
2.2. Recruitment and Randomization
2.3. Vitamin D
2.4. Survey Data Collection
2.5. Primary and Secondary Outcome Measurement
2.6. Safety Assessments
2.7. Adherence
2.8. Data & Statistical Analysis
3. Results
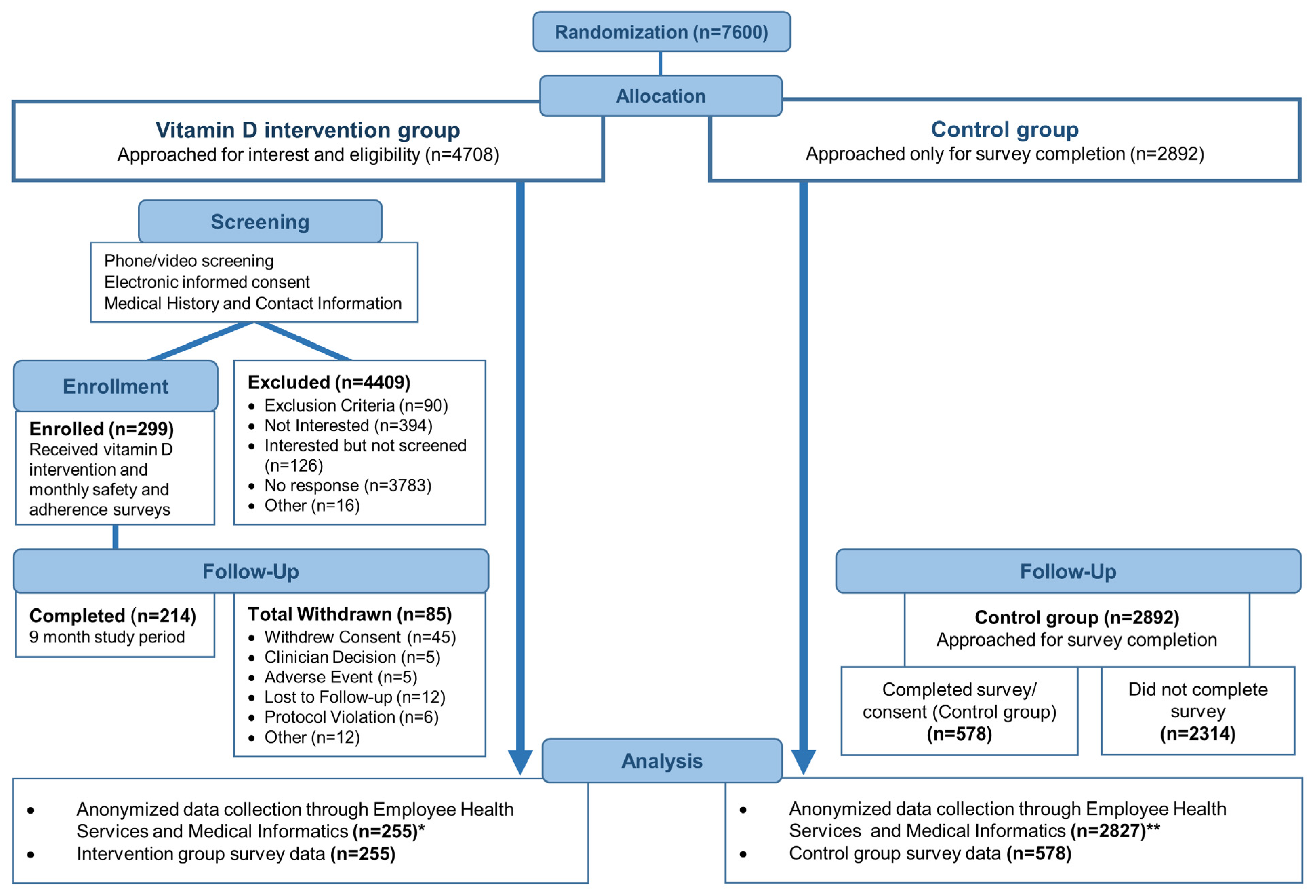
3.1. Trial Enrollment and Baseline Characteristics
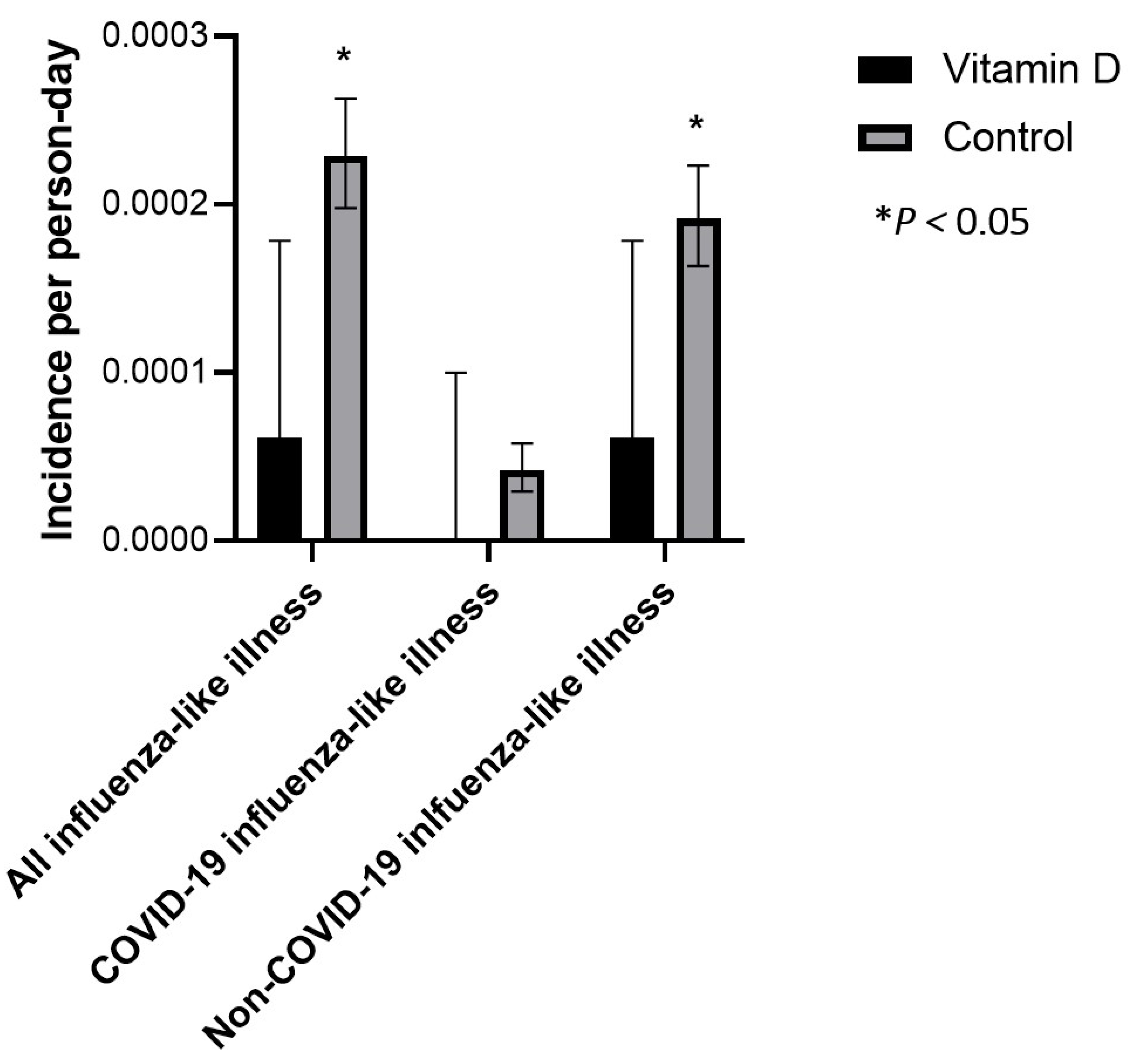
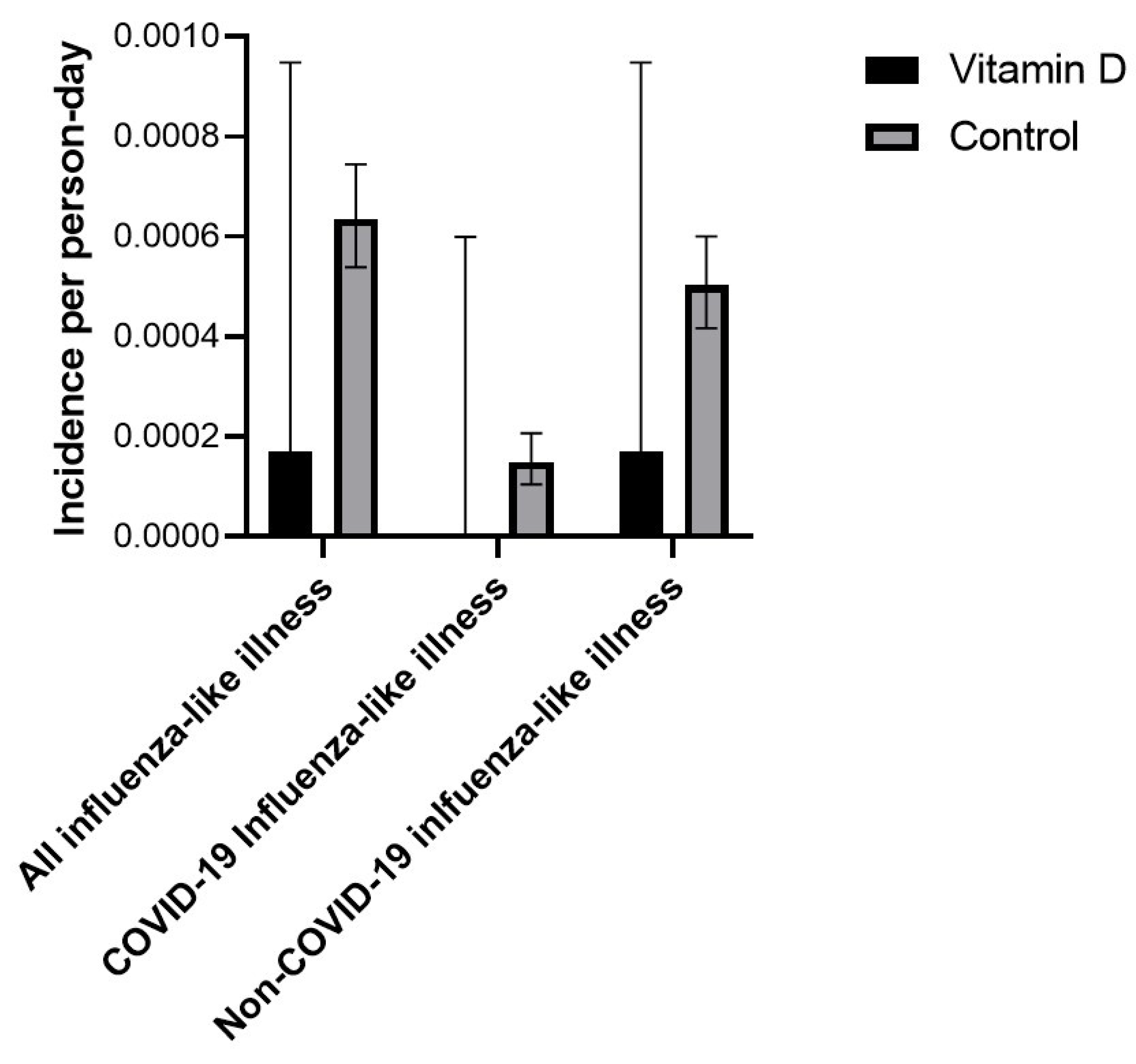
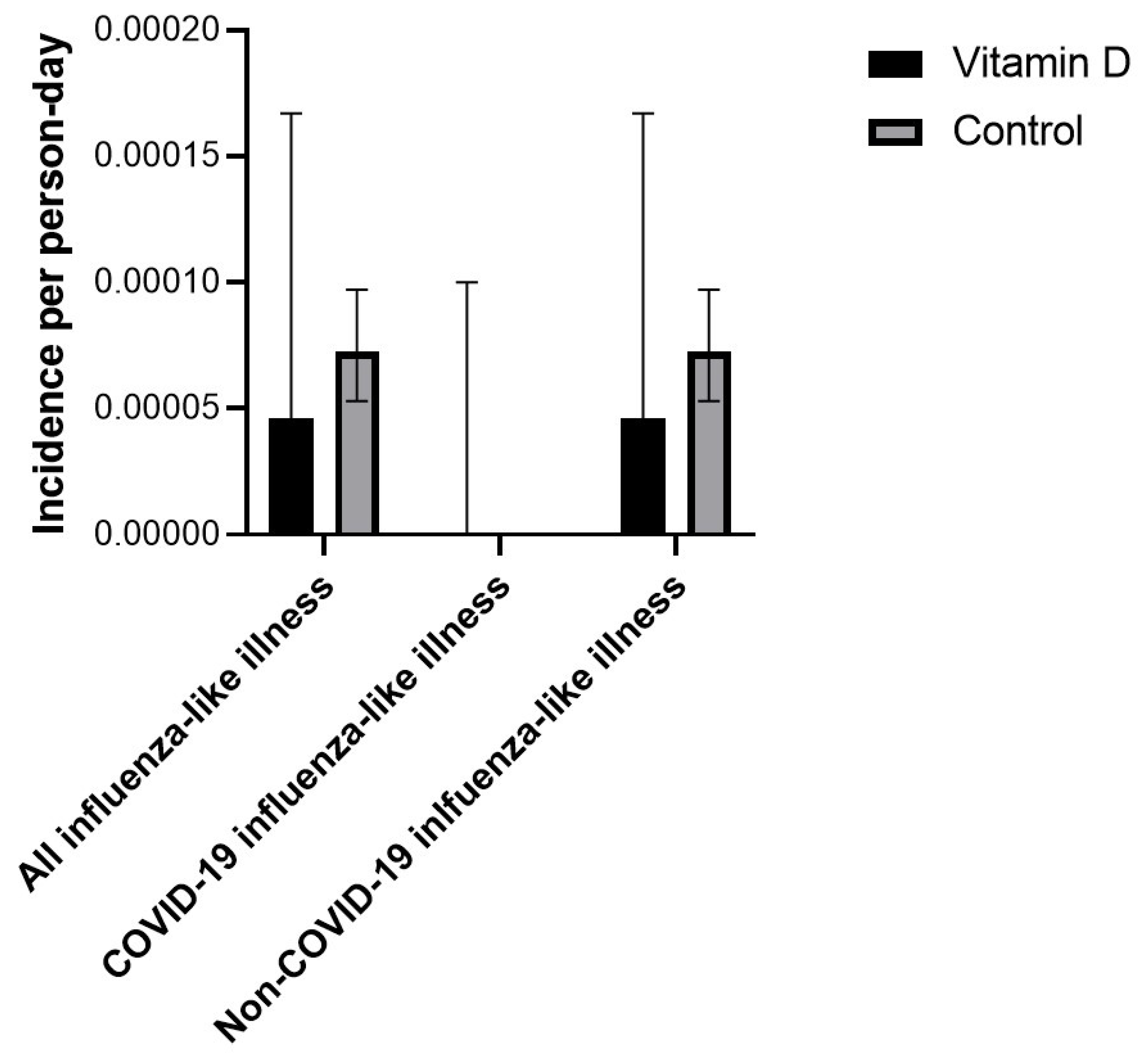
3.2. All Influenza-like Illness
3.3. COVID-19 Influenza-like Illness
3.4. Non-COVID-19 Influenza-like Illness
3.5. Treatment-Emergent Adverse Events (TEAEs)
3.6. Crossover
4. Discussion
4.1. Principal Findings
4.2. Influenza-like Illness
4.3. COVID-19 ILI
4.4. Clinical Implications
4.5. Methodological Considerations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Loef, B.; van Baarle, D.; van der Beek, A.J.; Sanders, E.A.M.; Bruijning-Verhagen, P.; Proper, K.I. Shift Work and Respiratory Infections in Health-Care Workers. Am. J. Epidemiol. 2019, 188, 509–517. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.-G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.-H.; et al. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Widera, E.; Chang, A.; Chen, H.L. Presenteeism: A public health hazard. J. Gen. Intern. Med. 2010, 25, 1244–1247. [Google Scholar] [CrossRef]
- Çelebi, G.; Pişkin, N.; Çelik Bekleviç, A.; Altunay, Y.; Salcı Keleş, A.; Tüz, M.A.; Altınsoy, B.; Hacıseyitoğlu, D. Specific risk factors for SARS-CoV-2 transmission among health care workers in a university hospital. Am. J. Infect. Control 2020, 48, 1225–1230. [Google Scholar] [CrossRef]
- Mascha, E.J.; Schober, P.; Schefold, J.C.; Stueber, F.; Luedi, M.M. Staffing with Disease-Based Epidemiologic Indices May Reduce Shortage of Intensive Care Unit Staff During the COVID-19 Pandemic. Anesth. Analg. 2020, 131, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Jolliffe, D.A.; Camargo, C.A., Jr.; Sluyter, J.D.; Aglipay, M.; Aloia, J.F.; Ganmaa, D.; Bergman, P.; Bischoff-Ferrari, H.A.; Borzutzky, A.; Damsgaard, C.T.; et al. Vitamin D supplementation to prevent acute respiratory infections: A systematic review and meta-analysis of aggregate data from randomised controlled trials. Lancet Diabetes Endocrinol. 2021, 9, 276–292. [Google Scholar] [CrossRef]
- Martineau, A.R.; Jolliffe, D.A.; Hooper, R.L.; Greenberg, L.; Aloia, J.F.; Bergman, P.; Dubnov-Raz, G.; Esposito, S.; Ganmaa, D.; Ginde, A.A.; et al. Vitamin D supplementation to prevent acute respiratory tract infections: Systematic review and meta-analysis of individual participant data. BMJ 2017, 356, i6583. [Google Scholar] [CrossRef]
- Bergman, P.; Lindh, A.U.; Björkhem-Bergman, L.; Lindh, J.D. Vitamin D and Respiratory Tract Infections: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. PLoS ONE 2013, 8, e65835. [Google Scholar] [CrossRef]
- Shang, J.; Ye, G.; Shi, K.; Wan, Y.; Luo, C.; Aihara, H.; Geng, Q.; Auerbach, A.; Li, F. Structural basis of receptor recognition by SARS-CoV-2. Nature 2020, 581, 221–224. [Google Scholar] [CrossRef]
- Li, Y.C.; Kong, J.; Wei, M.; Chen, Z.F.; Liu, S.Q.; Cao, L.P. 1,25-Dihydroxyvitamin D(3) is a negative endocrine regulator of the renin-angiotensin system. J. Clin. Investig. 2002, 110, 229–238. [Google Scholar] [CrossRef]
- Grant, W.B.; Lahore, H.; McDonnell, S.L.; Baggerly, C.A.; French, C.B.; Aliano, J.L.; Bhattoa, H.P. Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths. Nutrients 2020, 12, 988. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, A.; Bhansali, A.; Khare, N.; Suri, V.; Yaddanapudi, N.; Sachdeva, N.; Puri, G.D.; Malhotra, P. Short term, high-dose vitamin D supplementation for COVID-19 disease: A randomised, placebo-controlled, study (SHADE study). Postgrad. Med. J. 2022, 98, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Entrenas Castillo, M.; Entrenas Costa, L.M.; Vaquero Barrios, J.M.; Alcalá Díaz, J.F.; López Miranda, J.; Bouillon, R.; Quesada Gomez, J.M. Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study. J. Steroid Biochem. Mol. Biol. 2020, 203, 105751. [Google Scholar] [CrossRef] [PubMed]
- Murai, I.H.; Fernandes, A.L.; Sales, L.P.; Pinto, A.J.; Goessler, K.F.; Duran, C.S.C.; Silva, C.B.R.; Franco, A.S.; Macedo, M.B.; Dalmolin, H.H.H.; et al. Effect of a Single High Dose of Vitamin D3 on Hospital Length of Stay in Patients with Moderate to Severe COVID-19: A Randomized Clinical Trial. JAMA 2021, 325, 1053–1060. [Google Scholar] [CrossRef]
- Jolliffe, D.A.; Holt, H.; Greenig, M.; Talaei, M.; Perdek, N.; Pfeffer, P.; Maltby, S.; Symons, J.; Barlow, N.L.; Normandale, A.; et al. Vitamin D Supplements for Prevention of COVID-19 or other Acute Respiratory Infections: A Phase 3 Randomized Controlled Trial (CORONAVIT). medRxiv 2022, 378, e071230. [Google Scholar] [CrossRef]
- Villasis-Keever, M.A.; López-Alarcón, M.G.; Miranda-Novales, G.; Zurita-Cruz, J.N.; Barrada-Vázquez, A.S.; González-Ibarra, J.; Martínez-Reyes, M.; Grajales-Muñiz, C.; Santacruz-Tinoco, C.E.; Martínez-Miguel, B.; et al. Efficacy and Safety of Vitamin D Supplementation to Prevent COVID-19 in Frontline Healthcare Workers. A Randomized Clinical Trial. Arch. Med. Res. 2022, 53, 423–430. [Google Scholar] [CrossRef]
- Hoang, B.X.; Shaw, G.; Fang, W.; Han, B. Possible application of high-dose vitamin C in the prevention and therapy of coronavirus infection. J. Glob. Antimicrob. Resist. 2020, 23, 256–262. [Google Scholar] [CrossRef]
- Sinopoli, A.; Caminada, S.; Isonne, C.; Maria Mercedes, S.; Baccolini, V. What Are the Effects of Vitamin A Oral Supplementation in the Prevention and Management of Viral Infections? A Systematic Review of Randomized Clinical Trials. Nutrients 2022, 14, 4081. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef]
- Zelen, M. A new design for randomized clinical trials. N. Engl. J. Med. 1979, 300, 1242–1245. [Google Scholar] [CrossRef]
- Torgerson, D.J.; Roland, M. What is Zelen’s design? BMJ 1998, 316, 606. [Google Scholar] [CrossRef]
- Torgerson, D. The use of Zelen’s design in randomised trials. BJOG 2004, 111, 2. [Google Scholar] [CrossRef]
- House, A.; Knapp, P. Informed consent. Trials that use Zelen’s procedure should be acceptable. BMJ 1997, 315, 251. [Google Scholar] [PubMed]
- Adamson, J.; Cockayne, S.; Puffer, S.; Torgerson, D.J. Review of randomised trials using the post-randomised consent (Zelen’s) design. Contemp. Clin. Trials 2006, 27, 305–319. [Google Scholar] [CrossRef] [PubMed]
- Aloia, J.F.; Patel, M.; Dimaano, R.; Li-Ng, M.; Talwar, S.A.; Mikhail, M.; Pollack, S.; Yeh, J.K. Vitamin D intake to attain a desired serum 25-hydroxyvitamin D concentration. Am. J. Clin. Nutr. 2008, 87, 1952–1958. [Google Scholar] [CrossRef] [PubMed]
- Gabbard, J.; Pajewski, N.M.; Callahan, K.E.; Dharod, A.; Foley, K.; Ferris, K.; Moses, A.; Grey, C.; Williamson, J. Advance care planning for vulnerable older adults within an Accountable Care Organization: Study protocol for the IMPACT randomised controlled trial. BMJ Open 2019, 9, e032732. [Google Scholar] [CrossRef] [PubMed]
- Hardcastle, J.D.; Chamberlain, J.O.; Robinson, M.H.; Moss, S.M.; Amar, S.S.; Balfour, T.W.; James, P.D.; Mangham, C.M. Randomised controlled trial of faecal-occult-blood screening for colorectal cancer. Lancet 1996, 348, 1472–1477. [Google Scholar] [CrossRef]
- New Jersey Department of Health. New Jersey State Health Asssessment Data 2020; New Jersey Department of Health: Trenton, NJ, USA, 2020. [Google Scholar]
- Ekwaru, J.P.; Zwicker, J.D.; Holick, M.F.; Giovannucci, E.; Veugelers, P.J. The importance of body weight for the dose response relationship of oral vitamin D supplementation and serum 25-hydroxyvitamin D in healthy volunteers. PLoS ONE 2014, 9, e111265. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inf. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inf. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Pepper, K.J.; Judd, S.E.; Nanes, M.S.; Tangpricha, V. Evaluation of vitamin D repletion regimens to correct vitamin D status in adults. Endocr. Pract. 2009, 15, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Kimball, S.M.; Mirhosseini, N.; Holick, M.F. Evaluation of vitamin D3 intakes up to 15,000 international units/day and serum 25-hydroxyvitamin D concentrations up to 300 nmol/L on calcium metabolism in a community setting. Derm.-Endocrinol. 2017, 9, e1300213. [Google Scholar] [CrossRef] [PubMed]
- Hathcock, J.N.; Shao, A.; Vieth, R.; Heaney, R. Risk assessment for vitamin D. Am. J. Clin. Nutr. 2007, 85, 6–18. [Google Scholar] [CrossRef] [PubMed]
- Vieth, R. Vitamin D toxicity, policy, and science. J. Bone Miner. Res. 2007, 22 (Suppl. S2), V64–V68. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D Is Not as Toxic as Was Once Thought: A Historical and an Up-to-Date Perspective. Mayo Clin. Proc. 2015, 90, 561–564. [Google Scholar] [CrossRef]
- Mayo Clinic. Hypercalcemia. Available online: https://www.mayoclinic.org/diseases-conditions/hypercalcemia/symptoms-causes/syc-20355523 (accessed on 27 June 2022).
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 2013. [Google Scholar]
- Stuart, E.A.; Lee, B.K.; Leacy, F.P. Prognostic score-based balance measures can be a useful diagnostic for propensity score methods in comparative effectiveness research. J. Clin. Epidemiol. 2013, 66, S84–S90.e81. [Google Scholar] [CrossRef]
- Sahai, H.; Khurshid, A. Statistics in Epidemiology: Methods, Techniques, and Applications; CRC Press, INC: Boca Raton, FL, USA, 1996. [Google Scholar]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against COVID-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef]
- Leaf, D.E.; Ginde, A.A. Vitamin D3 to Treat COVID-19: Different Disease, Same Answer. JAMA 2021, 325, 1047–1048. [Google Scholar] [CrossRef]
- Kinman, G.; Grant, C. Presenteeism during the COVID-19 pandemic: Risks and solutions. Occup. Med. 2020, 71, 243–244. [Google Scholar] [CrossRef] [PubMed]
- Keech, M.; Beardsworth, P. The impact of influenza on working days lost: A review of the literature. PharmacoEconomics 2008, 26, 911–924. [Google Scholar] [CrossRef] [PubMed]
- Tsai, Y.; Zhou, F.; Kim, I.K. The burden of influenza-like illness in the US workforce. Occup. Med. 2014, 64, 341–347. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
|
| Vitamin D3 (n = 255) | Control (n = 578) | Standardized Difference | |
|---|---|---|---|
| Age at enrollment in years, mean ± SD | 47 ± 12 | 50 ± 13 | 0.24 |
| Gender, n (%) | |||
| Man | 55 (22) | 131 (23) | 0.12 |
| Woman | 199 (78) | 446 (77) | 0.02 |
| Other | 1 (0.4) | 1 (0.2) | 0.45 |
| Race, n (%) | |||
| American Indian/Alaska Native | 1 (0.4) | 1 (0.2) | 0.45 |
| Asian | 12 (5) | 36 (6) | 0.04 |
| Black/African American | 27 (11) | 47 (8) | 0.10 |
| Native Hawaiian/other Pacific Islander | 2 (0.8) | 0 (0) | 0.42 |
| White | 194 (76) | 456 (79) | 0.07 |
| More than one race | 7 (3) | 20 (4) | 0.05 |
| Other | 12 (5) | 18 (3) | 0.10 |
| Ethnicity, n (%) | |||
| Hispanic or Latino | 24 (9) | 28 (5) | 0.16 |
| Not Hispanic or Latino | 231 (91) | 547 (95) | 0.16 |
| Body mass index in kg/m2, mean ± SD | 30 ± 6 | 29 ± 6 | 0.17 |
| Comorbidities, n (%) | |||
| Cardiovascular disease | 60 (24) | 157 (27) | 0.07 |
| Respiratory disease | 47 (18) | 106 (18) | 0 |
| Eye disease | 11 (4) | 16 (3) | 0.05 |
| Gastrointestinal disease | 97 (38) | 213 (37) | 0.02 |
| Urological disease | 19 (8) | 62 (11) | 0.02 |
| Liver disease | 3 (1) | 8 (1) | 0.10 |
| Hematological disease | 27 (11) | 51 (9) | 0 |
| Dermatological disease | 42 (17) | 76 (13) | 0.07 |
| Diabetes | 14 (6) | 44 (8) | 0.11 |
| Endocrine disease (other) | 38 (15) | 77 (13) | 0.08 |
| Malignant disease | 15 (6) | 33 (6) | 0 |
| History of vitamin D deficiency, n (%) | 62 (24) | 174 (30) | 0.14 |
| Previous COVID-19, n (%) | 16 (6) | 29 (5) | 0.06 |
| Illness | Intervention Group | Control Group | Absolute Incidence Rate Difference | 95%-CI | p-Value | Relative Incidence Rate | 95%-CI | p-Value |
|---|---|---|---|---|---|---|---|---|
| Incidence Rate | Incidence Rate | |||||||
| All ILI | 6.104 × 10−5 | 2.288 × 10−4 | −1.677 × 10−4 | −3.025 × 10−4 to −3.3 × 10−5 | 0.0147 | 2.668 × 10−1 | 5.456 × 10−2 to 7.913 × 10−1 | 0.0060 |
| COVID-19 ILI | 0.0 | 4.181 × 10−5 | −4.181 × 10−5 | −9.897 × 10−5 to 1.536 × 10−5 | 0.1517 | N/A | N/A | N/A |
| Non-COVID-19 ILI | 6.104 × 10−5 | 1.916 × 10−4 | −1.306 × 10−4 | −2.541 × 10−4 to −7.1 × 10−6 | 0.0382 | 3.186 × 10−1 | 6.503 × 10−2 to 9.474 × 10−1 | 0.0229 |
| Not Fully Vaccinated Observation Period | Intervention Group | Control Group | Absolute Incidence Rate Difference | 95%-CI | p-Value | Relative Incidence Rate | 95%-CI | p-Value |
|---|---|---|---|---|---|---|---|---|
| Incidence Rate | Incidence Rate | |||||||
| All ILI | 1.701 × 10−4 | 6.354 × 10−4 | −4.653 × 10−4 | −1.1118 × 10−3 to 1.811 × 10−4 | 0.1583 | 2.677 × 10−1 | 6.734 × 10−3 to 1.5139 × 100 | 0.1403 |
| COVID-19 ILI | 0.0 | 1.495 × 10−4 | −1.495 × 10−4 | −4.621 × 10−4 to 1.63 × 10−4 | 0.3485 | N/A | N/A | N/A |
| Non-COVID-19 ILI | 1.701 × 10−4 | 5.025 × 10−4 | −3.324 × 10−4 | −9.078 × 10−4 to 2.43 × 10−4 | 0.2575 | 3.385 × 10−1 | 8.500 × 10−3 to 1.9219 × 100 | 0.2624 |
| Fully vaccinated observation period | Intervention Group | Control Group | Absolute Incidence Rate Difference | 95%-CI | p-value | Relative Incidence Rate | 95%-CI | p-value |
| Incidence Rate | Incidence Rate | |||||||
| All ILI | 4.622 × 10−5 | 7.254 × 10−5 | −2.632 × 10−5 | −1.0833 × 10−4 to 5.57 × 10−5 | 0.5294 | 6.372 × 10−1 | 7.488 × 10−2 to 2.4395 × 100 | 0.5809 |
| COVID-19 ILI | 0.0 | 0.0 | 0.0 | 0.0 to 1.0 × 10−4 | - | N/A | N/A | N/A |
| Non-COVID-19 ILI | 4.622 × 10−5 | 7.254 × 10−5 | −2.632 × 10−5 | −1.0833 × 10−4 to 5.57 × 10−5 | 0.5294 | 6.372 × 10−1 | 7.488 × 10−2 to 2.4395 × 100 | 0.5809 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Helmond, N.; Brobyn, T.L.; LaRiccia, P.J.; Cafaro, T.; Hunter, K.; Roy, S.; Bandomer, B.; Ng, K.Q.; Goldstein, H.; Mitrev, L.V.; et al. Vitamin D3 Supplementation at 5000 IU Daily for the Prevention of Influenza-like Illness in Healthcare Workers: A Pragmatic Randomized Clinical Trial. Nutrients 2023, 15, 180. https://doi.org/10.3390/nu15010180
van Helmond N, Brobyn TL, LaRiccia PJ, Cafaro T, Hunter K, Roy S, Bandomer B, Ng KQ, Goldstein H, Mitrev LV, et al. Vitamin D3 Supplementation at 5000 IU Daily for the Prevention of Influenza-like Illness in Healthcare Workers: A Pragmatic Randomized Clinical Trial. Nutrients. 2023; 15(1):180. https://doi.org/10.3390/nu15010180
Chicago/Turabian Stylevan Helmond, Noud, Tracy L. Brobyn, Patrick J. LaRiccia, Teresa Cafaro, Krystal Hunter, Satyajeet Roy, Brigid Bandomer, Kevin Q. Ng, Helen Goldstein, Ludmil V. Mitrev, and et al. 2023. "Vitamin D3 Supplementation at 5000 IU Daily for the Prevention of Influenza-like Illness in Healthcare Workers: A Pragmatic Randomized Clinical Trial" Nutrients 15, no. 1: 180. https://doi.org/10.3390/nu15010180
APA Stylevan Helmond, N., Brobyn, T. L., LaRiccia, P. J., Cafaro, T., Hunter, K., Roy, S., Bandomer, B., Ng, K. Q., Goldstein, H., Mitrev, L. V., Tsai, A., Thwing, D., Maag, M. A., & Chung, M. K. (2023). Vitamin D3 Supplementation at 5000 IU Daily for the Prevention of Influenza-like Illness in Healthcare Workers: A Pragmatic Randomized Clinical Trial. Nutrients, 15(1), 180. https://doi.org/10.3390/nu15010180