
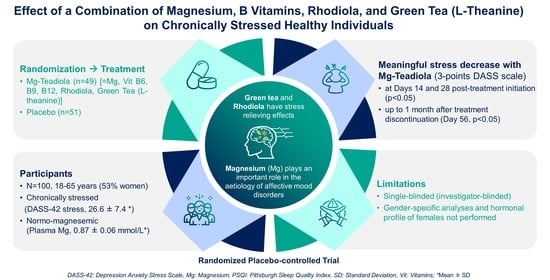
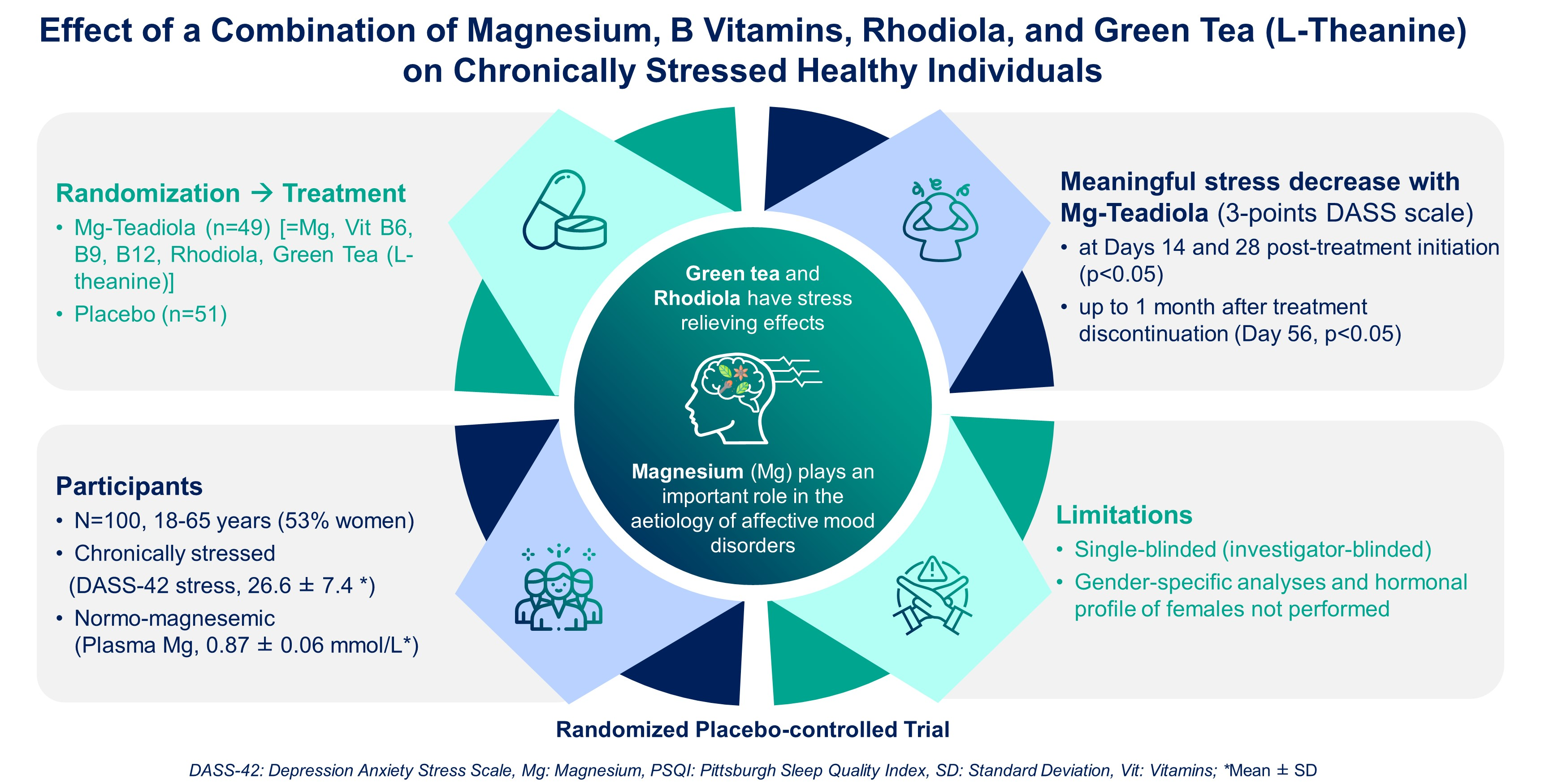
Effect of a Combination of Magnesium, B Vitamins, Rhodiola, and Green Tea (L-Theanine) on Chronically Stressed Healthy Individuals—A Randomized, Placebo-Controlled Study

 ,
,  , ,
, ,  and
and
Abstract
:
1. Introduction
2. Materials and Methods
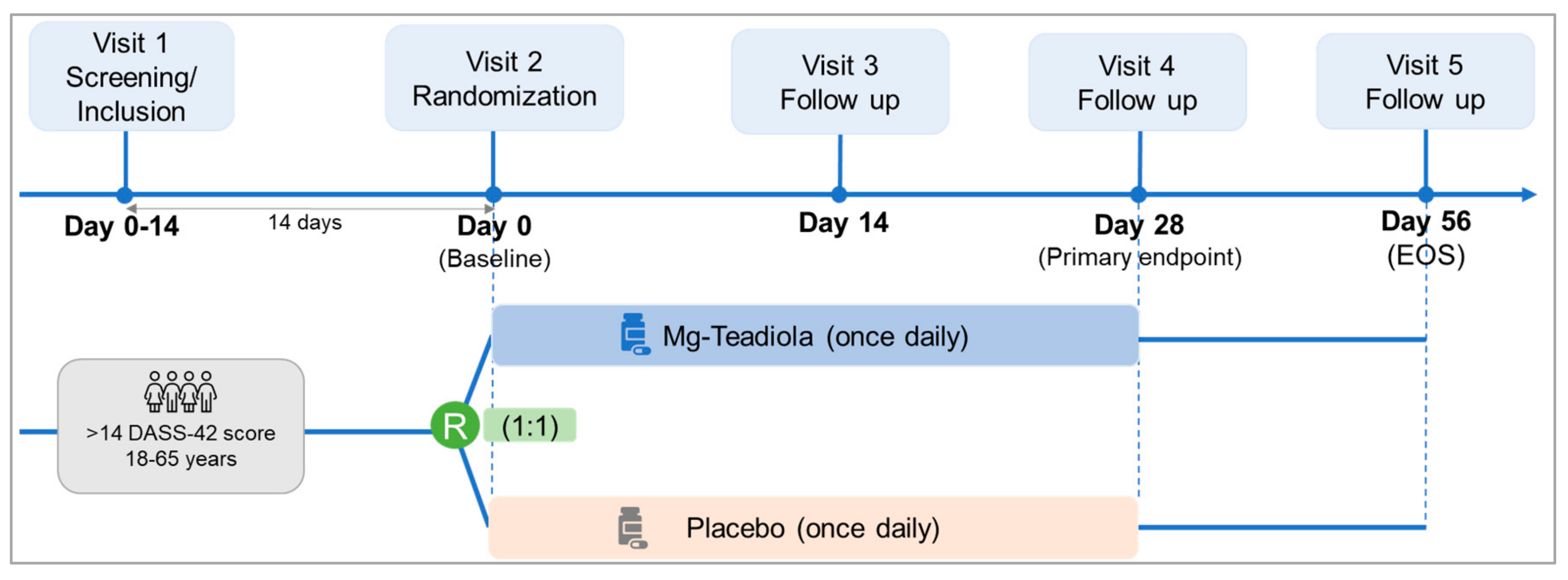
2.1. Study Design
2.2. Participants
2.3. Randomization, Masking, and Treatment
2.4. Study Objectives
2.5. Endpoints and Assessments
2.6. Statistical Analyses
2.6.1. Sample Size Calculation
2.6.2. Statistical Methods
3. Results
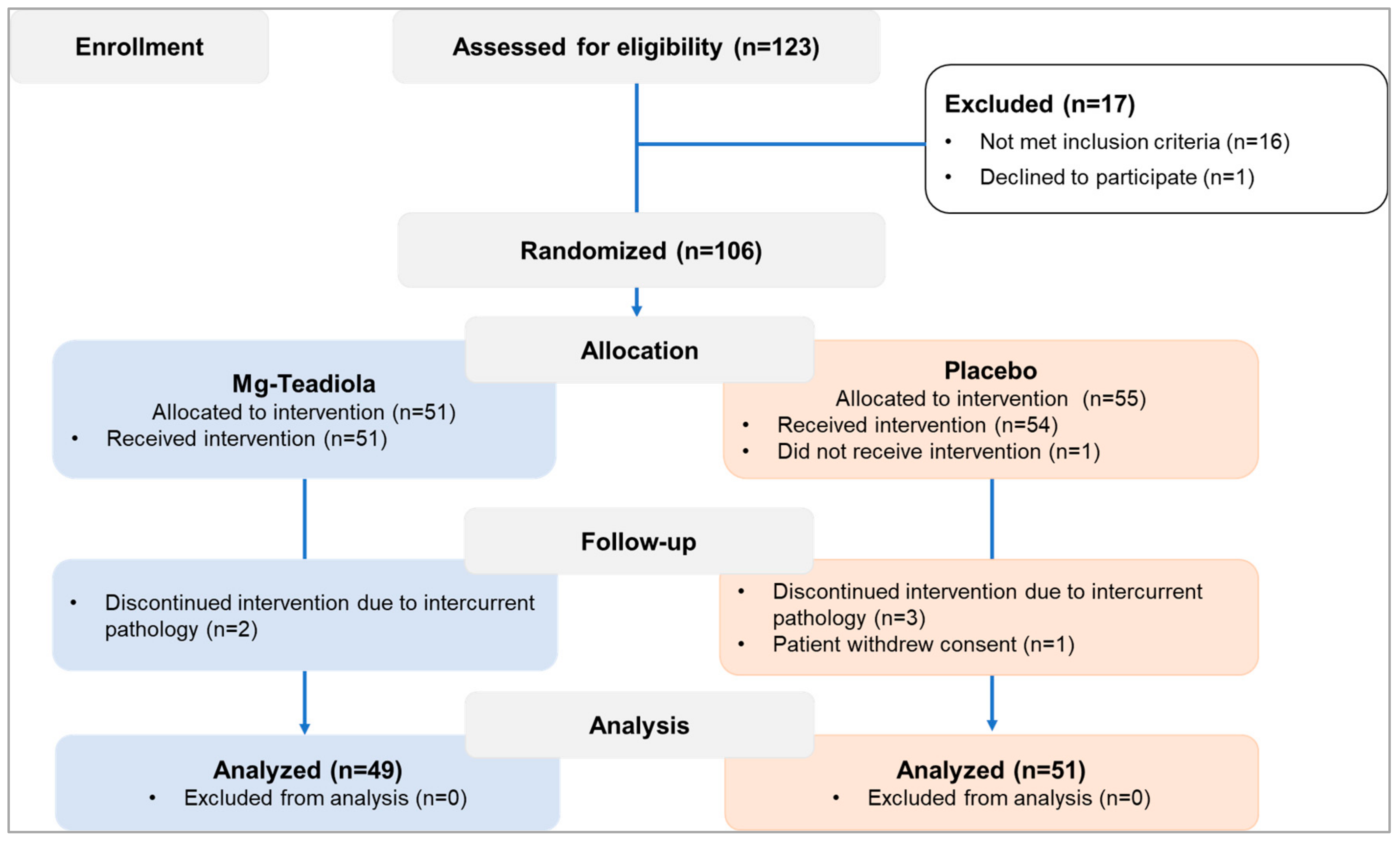
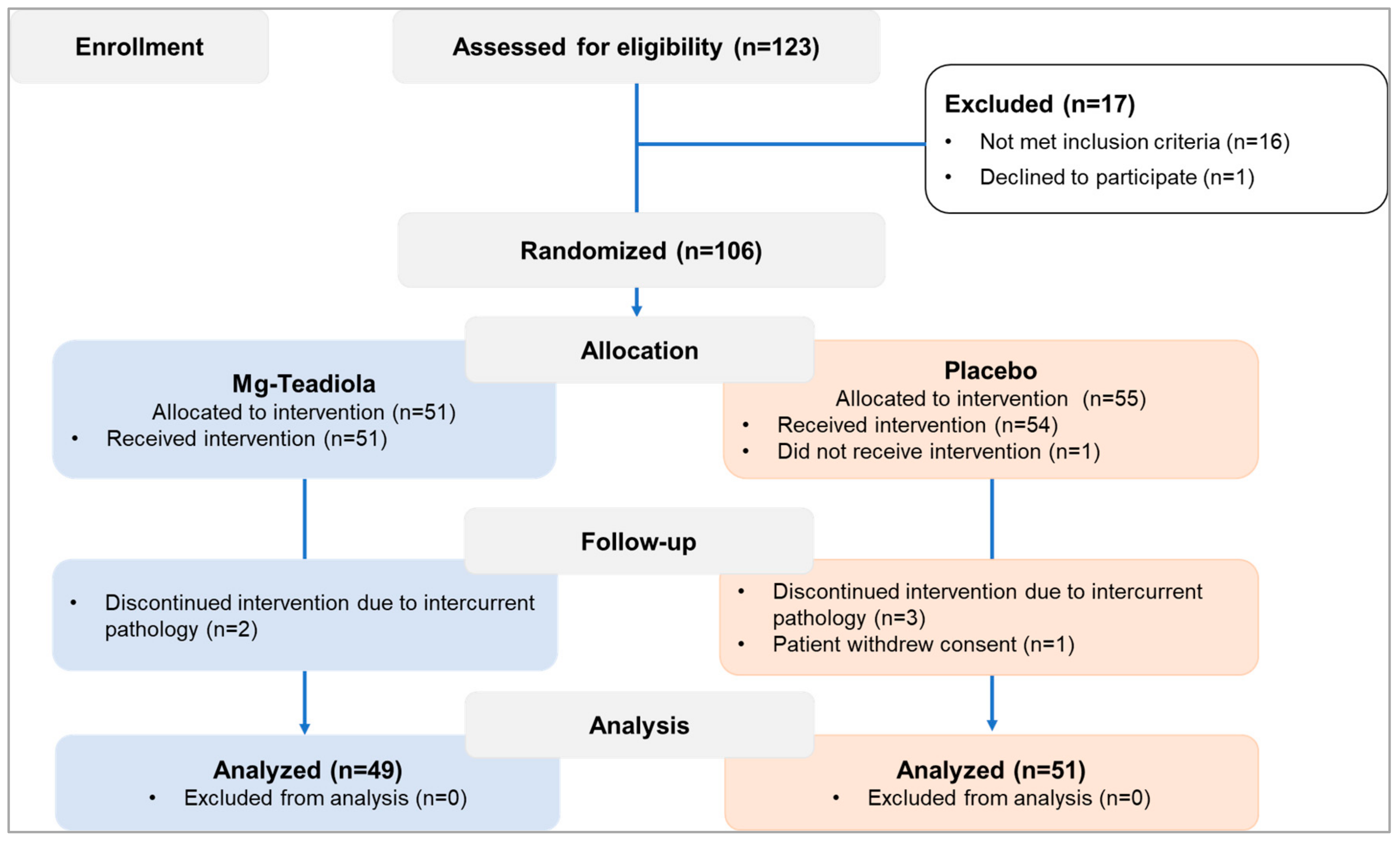
3.1. Patient Disposition and Baseline Characteristics
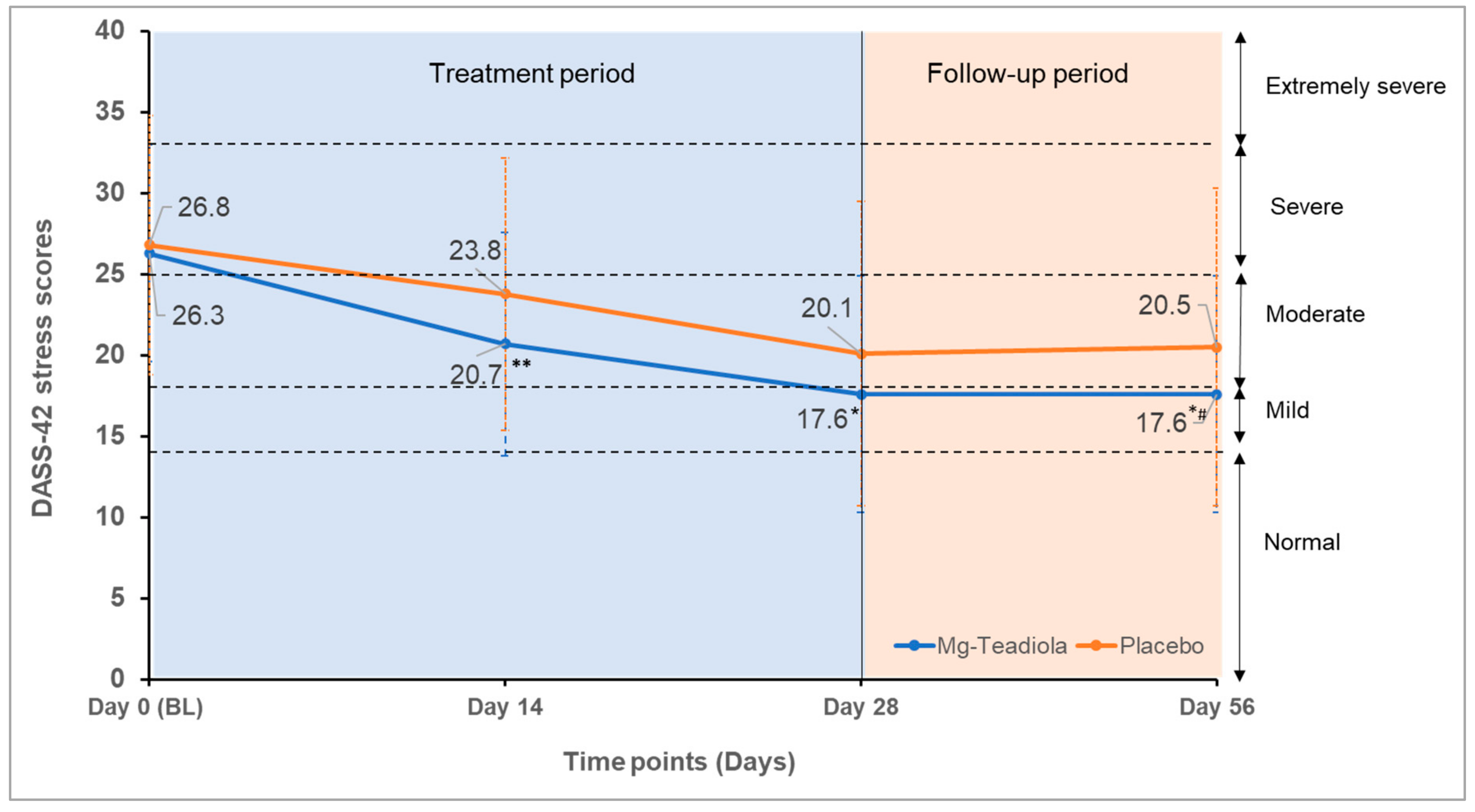
3.2. Efficacy Outcomes
3.3. Safety Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mahmud, S.; Hossain, S.; Muyeed, A.; Islam, M.M.; Mohsin, M. The global prevalence of depression, anxiety, stress, and, insomnia and its changes among health professionals during COVID-19 pandemic: A rapid systematic review and meta-analysis. Heliyon 2021, 7, e07393. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef] [PubMed]
- Yaribeygi, H.; Panahi, Y.; Sahraei, H.; Johnston, T.P.; Sahebkar, A. The impact of stress on body function: A review. EXCLI J. 2017, 16, 1057–1072. [Google Scholar] [CrossRef] [PubMed]
- Sartori, S.B.; Singewald, N. Novel pharmacological targets in drug development for the treatment of anxiety and anxiety-related disorders. Pharmacol. Ther. 2019, 204, 107402. [Google Scholar] [CrossRef]
- MentalHealth.net. An American Addiction Centers Resource. Available online: https://www.mentalhelp.net/stress/reduction/medication/ (accessed on 22 December 2021).
- Mancini, E.; Beglinger, C.; Drewe, J.; Zanchi, D.; Lang, U.E.; Borgwardt, S. Green tea effects on cognition, mood and human brain function: A systematic review. Phytomedicine 2017, 34, 26–37. [Google Scholar] [CrossRef] [Green Version]
- Zogović, D.; Pešić, V.; Dmitrašinović, G.; Dajak, M.; Plećaš, B.; Batinić, B.; Popović, D.; Ignjatović, S. Pituitary-gonadal, pituitary-adrenocortical hormones and IL-6 levels following long-term magnesium supplementation in male students. J. Med. Biochem. 2014, 33, 291–298. [Google Scholar] [CrossRef] [Green Version]
- Mattioli, L.; Funari, C.; Perfumi, M. Effects of Rhodiola rosea L. extract on behavioural and physiological alterations induced by chronic mild stress in female rats. J. Psychopharmacol. 2009, 23, 130–142. [Google Scholar] [CrossRef]
- Pouteau, E.; Kabir-Ahmadi, M.; Noah, L.; Mazur, A.; Dye, L.; Hellhammer, J.; Pickering, G.; Dubray, C. Superiority of magnesium and vitamin B6 over magnesium alone on severe stress in healthy adults with low magnesemia: A randomized, single-blind clinical trial. PLoS ONE 2018, 13, e0208454. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, D.O.; Veasey, R.; Watson, A.; Dodd, F.; Jones, E.; Maggini, S.; Haskell, C.F. Effects of high-dose B vitamin complex with vitamin C and minerals on subjective mood and performance in healthy males. Psychopharmacology 2010, 211, 55–68. [Google Scholar] [CrossRef] [Green Version]
- Harris, E.; Kirk, J.; Rowsell, R.; Vitetta, L.; Sali, A.; Scholey, A.B.; Pipingas, A. The effect of multivitamin supplementation on mood and stress in healthy older men. Hum. Psychopharmacol. 2011, 26, 560–567. [Google Scholar] [CrossRef]
- Boyle, N.B.; Billington, J.; Lawton, C.; Quadt, F.; Dye, L. A combination of green tea, rhodiola, magnesium and B vitamins modulates brain activity and protects against the effects of induced social stress in healthy volunteers. Nutr. Neurosci. 2021, 1–15, Ahead-of-print. [Google Scholar] [CrossRef]
- Dye, L.; Billington, J.; Lawton, C.; Boyle, N. A combination of magnesium, B vitamins, green tea and rhodiola attenuates the negative effects of acute psychosocial stress on subjective state in adults. Curr. Dev. Nutr. 2020, 4, 1796. [Google Scholar] [CrossRef]
- Akin, A.; Çetin, B. The Depression Anxiety and Stress Scale (DASS): The Study of Validity and Reliability. Educ. Sci. Theory Pract. 2007, 7, 241–268. [Google Scholar]
- Schneiderman, N.; Ironson, G.; Siegel, S.D. Stress and health: Psychological, behavioral, and biological determinants. Annu. Rev. Clin. Psychol. 2005, 1, 607–628. [Google Scholar] [CrossRef] [Green Version]
- Yang, L.; Zhao, Y.; Wang, Y.; Liu, L.; Zhang, X.; Li, B.; Cui, R. The Effects of Psychological Stress on Depression. Curr. Neuropharmacol. 2015, 13, 494–504. [Google Scholar] [CrossRef] [Green Version]
- Alotaibi, A.D.; Alosaimi, F.M.; Alajlan, A.A.; Bin Abdulrahman, K.A. The relationship between sleep quality, stress, and academic performance among medical students. J. Family Community Med. 2020, 27, 23–28. [Google Scholar] [CrossRef]
- Becker, N.; Jesus, S.; Marguilho, R.; Viseu, J.; Alexandra, K.; João, K.; Buela-Casal, G. Sleep quality and stress: A literature review. In Advanced Research in Health, Education and Social Sciences: Towards a Better Practice; Editora Universitária: Brasília, Brazil, 2015; pp. 53–61. [Google Scholar]
- Imbe, H.; Iwai-Liao, Y.; Senba, E. Stress-induced hyperalgesia: Animal models and putative mechanisms. Front. Biosci. 2006, 11, 2179–2192. [Google Scholar] [CrossRef] [Green Version]
- Crettaz, B.; Marziniak, M.; Willeke, P.; Young, P.; Hellhammer, D.; Stumpf, A.; Burgmer, M. Stress-induced allodynia—Evidence of increased pain sensitivity in healthy humans and patients with chronic pain after experimentally induced psychosocial stress. PLoS ONE 2013, 8, e69460. [Google Scholar] [CrossRef] [Green Version]
- European Food Safety Authority (EFSA) Recommendations. Available online: https://multimedia.efsa.europa.eu/drvs/index.htm (accessed on 20 April 2022).
- Lovibond, S.H.; Lovibond, P.F. Depression Anxiety and Stress Scales (DASS); Psychology Foundation of Australia: Sydney, Australia, 2013. [Google Scholar]
- Brown, T.A.; Chorpita, B.F.; Korotitsch, W.; Barlow, D.H. Psychometric properties of the Depression Anxiety Stress Scales (DASS) in clinical samples. Behav. Res. Ther. 1997, 35, 79–89. [Google Scholar] [CrossRef]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales, 2nd ed.; Psychology Foundation: Sydney, Australia, 1995. [Google Scholar]
- Basha, E.; Kaya, M. Depression, Anxiety and Stress Scale (DASS): The Study of Validity and Reliability. Univers. J. Educ. Res. 2016, 4, 2701–2705. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, M.; Bishop, S.; Pivik, J. The Pain Catastrophizing Scale: Development and validation. Psychol. Assess. 1995, 7, 524–532. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Verdugo, R.; Ochoa, J.L. Quantitative somatosensory thermotest. A key method for functional evaluation of small calibre afferent channels. Brain 1992, 115, 893–913. [Google Scholar] [CrossRef]
- Gitelman, H.J.; Hurt, C.; Lutwak, L. An automated spectrophotometric method for magnesium analysis. Anal. Biochem. 1966, 14, 106–120. [Google Scholar] [CrossRef]
- Yohannes, A.M.; Dryden, S.; Hanania, N.A. Validity and Responsiveness of the Depression Anxiety Stress Scales-21 (DASS-21) in COPD. Chest 2019, 155, 1166–1177. [Google Scholar] [CrossRef]
- Vickers, A.J.; Altman, D.G. Statistics notes: Analysing controlled trials with baseline and follow up measurements. BMJ 2001, 323, 1123–1124. [Google Scholar] [CrossRef] [Green Version]
- Bender, R.; Lange, S. Adjusting for multiple testing—When and how? J. Clin. Epidemiol. 2001, 54, 343–349. [Google Scholar] [CrossRef]
- Feise, R.J. Do multiple outcome measures require p-value adjustment? BMC Med. Res. Methodol. 2002, 2, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chong, H.X.; Yusoff, N.A.A.; Hor, Y.Y.; Lew, L.C.; Jaafar, M.H.; Choi, S.B.; Yusoff, M.S.B.; Wahid, N.; Abdullah, M.; Zakaria, N.; et al. Lactobacillus plantarum DR7 alleviates stress and anxiety in adults: A randomised, double-blind, placebo-controlled study. Benef. Microbes 2019, 10, 355–373. [Google Scholar] [CrossRef] [PubMed]
- Lew, L.C.; Hor, Y.Y.; Yusoff, N.A.A.; Choi, S.B.; Yusoff, M.S.B.; Roslan, N.S.; Ahmad, A.; Mohammad, J.A.M.; Abdullah, M.; Zakaria, N.; et al. Probiotic Lactobacillus plantarum P8 alleviated stress and anxiety while enhancing memory and cognition in stressed adults: A randomised, double-blind, placebo-controlled study. Clin. Nutr. 2019, 38, 2053–2064. [Google Scholar] [CrossRef] [PubMed]
- Kell, G.; Rao, A.; Beccaria, G.; Clayton, P.; Inarejos-García, A.M.; Prodanov, M. Affron® a novel saffron extract (Crocus sativus L.) improves mood in healthy adults over 4 weeks in a double-blind, parallel, randomized, placebo-controlled clinical trial. Complement. Ther. Med. 2017, 33, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekhar, K.; Kapoor, J.; Anishetty, S. A prospective, randomized double-blind, placebo-controlled study of safety and efficacy of a high-concentration full-spectrum extract of ashwagandha root in reducing stress and anxiety in adults. Indian J. Psychol. Med. 2012, 34, 255–262. [Google Scholar] [CrossRef] [Green Version]
- Lopresti, A.L.; Smith, S.J.; Malvi, H.; Kodgule, R. An investigation into the stress-relieving and pharmacological actions of an ashwagandha (Withania somnifera) extract: A randomized, double-blind, placebo-controlled study. Medicine 2019, 98, e17186. [Google Scholar] [CrossRef] [PubMed]
- Camfield, D.A.; Stough, C.; Farrimond, J.; Scholey, A.B. Acute effects of tea constituents L-theanine, caffeine, and epigallocatechin gallate on cognitive function and mood: A systematic review and meta-analysis. Nutr. Rev. 2014, 72, 507–522. [Google Scholar] [CrossRef] [PubMed]
- Panossian, A.; Wikman, G.; Sarris, J. Rosenroot (Rhodiola rosea): Traditional use, chemical composition, pharmacology and clinical efficacy. Phytomedicine 2010, 17, 481–493. [Google Scholar] [CrossRef] [PubMed]
- Hozawa, A.; Kuriyama, S.; Nakaya, N.; Ohmori-Matsuda, K.; Kakizaki, M.; Sone, T.; Nagai, M.; Sugawara, Y.; Nitta, A.; Tomata, Y.; et al. Green tea consumption is associated with lower psychological distress in a general population: The Ohsaki Cohort 2006 Study. Am. J. Clin. Nutr. 2009, 90, 1390–1396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimura, K.; Ozeki, M.; Juneja, L.R.; Ohira, H. L-Theanine reduces psychological and physiological stress responses. Biol. Psychol. 2007, 74, 39–45. [Google Scholar] [CrossRef] [PubMed]
- White, D.J.; de Klerk, S.; Woods, W.; Gondalia, S.; Noonan, C.; Scholey, A.B. Anti-stress, behavioural and magnetoencephalography Effects of an L-Theanine-Based Nutrient Drink: A Randomised, Double-Blind, Placebo-Controlled, Crossover Trial. Nutrients 2016, 8, 53. [Google Scholar] [CrossRef] [Green Version]
- Yoto, A.; Motoki, M.; Murao, S.; Yokogoshi, H. Effects of L-theanine or caffeine intake on changes in blood pressure under physical and psychological stresses. J. Physiol. Anthropol. 2012, 31, 28. [Google Scholar] [CrossRef] [Green Version]
- Edwards, D.; Heufelder, A.; Zimmermann, A. Therapeutic effects and safety of Rhodiola rosea extract WS® 1375 in subjects with life-stress symptoms—Results of an open-label study. Phytother. Res. 2012, 26, 1220–1225. [Google Scholar] [CrossRef]
- Cropley, M.; Banks, A.P.; Boyle, J. The Effects of Rhodiola rosea L. Extract on Anxiety, Stress, Cognition and Other Mood Symptoms. Phytother. Res. 2015, 29, 1934–1939. [Google Scholar] [CrossRef]
- De Bock, K.; Eijnde, B.O.; Ramaekers, M.; Hespel, P. Acute Rhodiola rosea intake can improve endurance exercise performance. Int. J. Sport Nutr. Exerc. Metab. 2004, 14, 298–307. [Google Scholar] [CrossRef] [Green Version]
- Shevtsov, V.A.; Zholus, B.I.; Shervarly, V.I.; Vol’skij, V.B.; Korovin, Y.P.; Khristich, M.P.; Roslyakova, N.A.; Wikman, G. A randomized trial of two different doses of a SHR-5 Rhodiola rosea extract versus placebo and control of capacity for mental work. Phytomedicine 2003, 10, 95–105. [Google Scholar] [CrossRef] [Green Version]
- Abbasi, B.; Kimiagar, M.; Sadeghniiat, K.; Shirazi, M.M.; Hedayati, M.; Rashidkhani, B. The effect of magnesium supplementation on primary insomnia in elderly: A double-blind placebo-controlled clinical trial. J. Res. Med. Sci. 2012, 17, 1161–1169. [Google Scholar]
- Pickering, G.; Mazur, A.; Trousselard, M.; Bienkowski, P.; Yaltsewa, N.; Amessou, M.; Noah, L.; Pouteau, E. Magnesium Status and Stress: The Vicious Circle Concept Revisited. Nutrients 2020, 12, 3672. [Google Scholar] [CrossRef]
- Noah, L.; Dye, L.; Bois De Fer, B.; Mazur, A.; Pickering, G.; Pouteau, E. Effect of magnesium and vitamin B6 supplementation on mental health and quality of life in stressed healthy adults: Post-hoc analysis of a randomised controlled trial. Stress Health 2021, 37, 1000–1009. [Google Scholar] [CrossRef]
- Ahmad, A.H.; Zakaria, R. Pain in Times of Stress. Malays. J. Med. Sci. 2015, 22, 52–61. [Google Scholar]
- Fitzcharles, M.-A.; Cohen, S.P.; Clauw, D.J.; Littlejohn, G.; Usui, C.; Häuser, W. Nociplastic pain: Towards an understanding of prevalent pain conditions. Lancet 2021, 397, 2098–2110. [Google Scholar] [CrossRef]
- Zetterman, T.; Markkula, R.; Partanen, J.V.; Miettinen, T.; Estlander, A.-M.; Kalso, E. Muscle activity and acute stress in fibromyalgia. BMC Musculoskelet. Disord. 2021, 22, 183. [Google Scholar] [CrossRef]
- Pellissier, S.; Bonaz, B. The place of stress and emotions in the irritable bowel syndrome. Vitam. Horm. 2017, 103, 327–354. [Google Scholar] [CrossRef]
- Shin, H.-J.; Na, H.-S.; Do, S.-H. Magnesium and Pain. Nutrients 2020, 12, 2184. [Google Scholar] [CrossRef]
- Kvæl, L.A.H.; Løchting, I.; Molin, M. Use of dietary supplements and perceived knowledge among adults living with fibromyalgia in Norway: A cross-sectional study. Nutrients 2022, 14, 5. [Google Scholar] [CrossRef]
- Morel, V.; Pickering, M.-E.; Goubayon, J.; Djobo, M.; Macian, N.; Pickering, G. Magnesium for Pain Treatment in 2021? State of the Art. Nutrients 2021, 13, 1397. [Google Scholar] [CrossRef]
- Koc, B.; Kizildag, S.; Hosgorler, F.; Gümüş, H.; Kandis, S.; Ates, M.; Uysal, N. Magnesium citrate increases pain threshold and reduces TLR4 concentration in the brain. Biol. Trace Elem. Res. 2021, 199, 1954–1966. [Google Scholar] [CrossRef]
- Lolignier, S.; Gkika, D.; Andersson, D.; Leipold, E.; Vetter, I.; Viana, F.; Noël, J.; Busserolles, J. New Insight in Cold Pain: Role of Ion Channels, Modulation, and Clinical Perspectives. J. Neurosci. 2016, 36, 11435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sałat, K. Chemotherapy-induced peripheral neuropathy-part 2: Focus on the prevention of oxaliplatin-induced neurotoxicity. Pharmacol. Rep. 2020, 72, 508–527. [Google Scholar] [CrossRef] [PubMed]
- Kaur, P.; Robin; Makanjuola, V.O.; Arora, R.; Singh, B.; Arora, S. Immunopotentiating significance of conventionally used plant adaptogens as modulators in biochemical and molecular signalling pathways in cell mediated processes. Biomed. Pharmacother. 2017, 95, 1815–1829. [Google Scholar] [CrossRef]
- Chen, S.M.; Wang, M.H.; Soung, H.S.; Tseng, H.C.; Fang, C.H.; Lin, Y.W.; Yang, C.C.; Tsai, C.C. Neuroprotective effect of (l)-theanine in a rat model of chronic constriction injury of sciatic nerve-induced neuropathic pain. J. Formos. Med. Assoc. 2021, 121, 802–814. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Visit 2 (Baseline) | Visit 3 (Day 14) | Visit 4 (Day 28) | Visit 5 (Day 56) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mg-Teadiola n = 49 | Placebo n = 51 | Mg-Teadiola n = 49 | Placebo n = 51 | ES (95%CI), p-Value | Mg-Teadiola n = 49 | Placebo n = 51 | ES (95%CI), p-Value | Mg-Teadiola n = 49 | Placebo n = 51 | ES (95%CI), p-Value | |
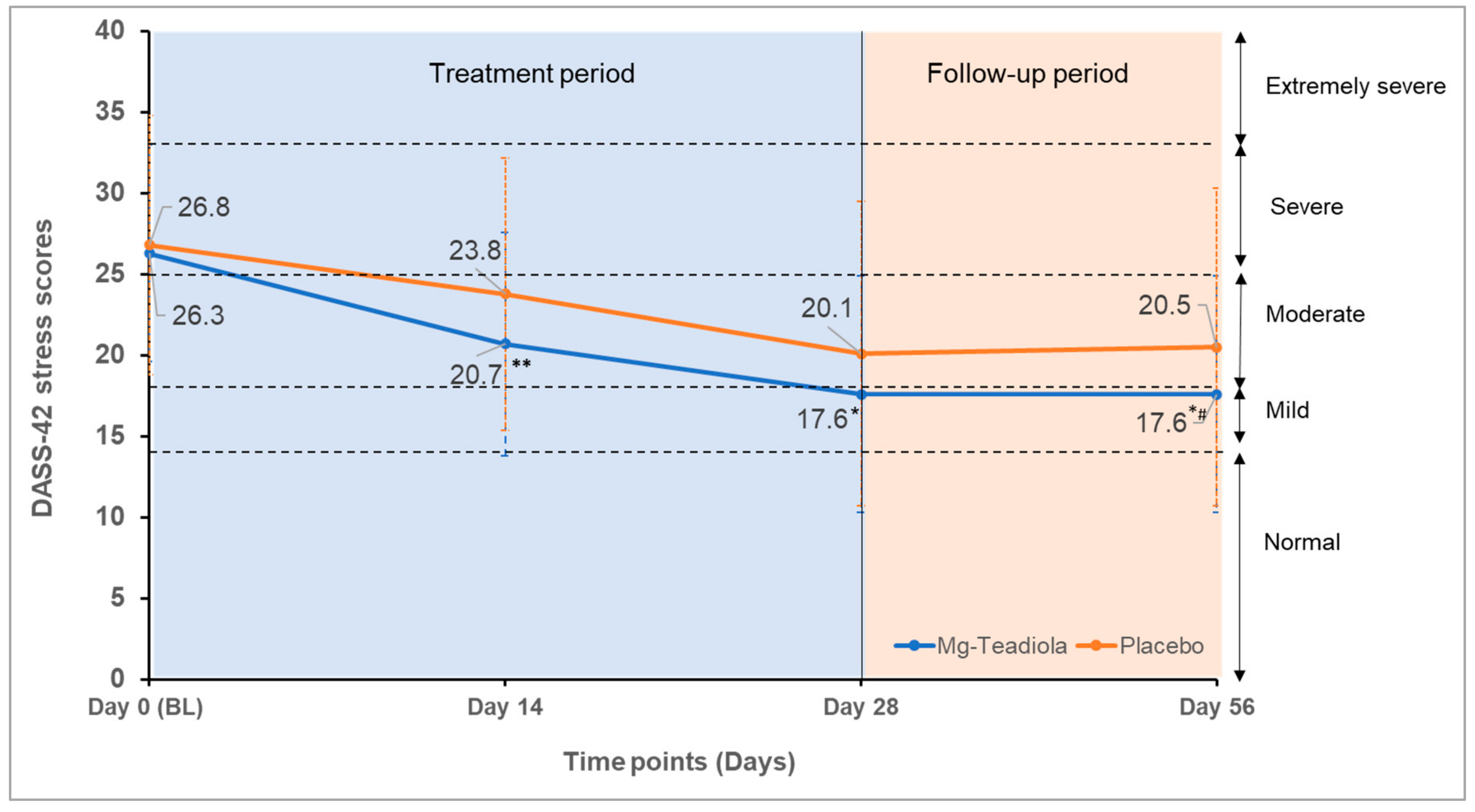
| DASS stress | 26.3 ± 6.7 | 26.8 ± 8.0 | 20.7 ± 6.9 | 23.8 ± 8.4 | −0.40 (−0.68; −0.11), 0.006 | 17.6 ± 7.3 | 20.1 ± 9.4 | −0.29 (−0.57; −0.01), 0.04 | 17.6 ± 7.3 | 20.5 ± 9.8 | −0.34 (−0.62; −0.06], 0.02 |
| DASS anxiety | 14.2 ± 7.8 | 14.1 ± 8.1 | 11.1 ± 6.7 | 10.6 ± 7.2 | 0.07 (−0.21; 0.35), 0.61 | 9.1 ± 6.8 | 9.2 ± 7.7 | −0.02 (−0.30; 0.26), 0.90 | 8.5 ± 6.7 | 8.8 ± 7.6 | −0.05 (−0.33; 0.23) 0.75 |
| DASS depression | 13.4 ± 10.2 | 13.4 ± 8.4 | 9.0 ± 8.7 | 8.3 ± 6.9 | −0.06 (−0.34; 0.22), 0.68 | 7.0 ± 6.7 | 7.1 ± 6.3 | −0.14 (−0.43; 0.13), 0.31 | 7.5 ± 8.4 | 6.8 ± 6.7 | −0.05 (−0.33; 0.23), 0.70 |
| PCS | 16.9 ± 9.9 | 15.3 ± 10.9 | 14.5 ± 10.0 | 14.0 ± 10.6 | −0.07 (−0.35; 0.21), 0.62 | 13.0 ± 10.8 | 12.6 ± 10.5 | −0.08 (−0.36; 0.20), 0.57 | 12.5 ± 11.2 | 12.7 ± 10.6 | −0.14 (−0.42; 0.14), 0.34 |
| Rumination | 6.0 ± 4.1 | 5.6 ± 4.6 | 5.2 ± 4.1 | 4.9 ± 4.1 | 0.02 (−0.26; 0.30), 0.90 | 4.3 ± 3.8 | 4.5 ± 4.3 | −0.08 (−0.36; 0.20), 0.57 | 3.8 ± 3.9 | 4.2 ± 3.8 | −0.15 (−0.43; 0.13), 0.30 |
| Magnification | 4.6 ± 2.7 | 4.1 ± 2.9 | 3.6 ± 2.7 | 3.8 ± 2.9 | −0.19 (−0.47; 0.09), 0.19 | 3.4 ± 3.0 | 3.4 ± 2.6 | −0.10 (−0.38; 0.18), 0.49 | 3.4 ± 3.1 | 3.5 ± 2.8 | −0.11 (−0.39; 0.17), 0.44 |
| Helplessness | 6.3 ± 4.7 | 5.6 ± 5.0 | 5.7 ± 4.3 | 5.3 ± 5.1 | −0.02 (−0.30; 0.26), 0.87 | 5.3 ± 4.9 | 4.8 ± 5.1 | 0.00 (−0.28; 0.28), 0.99 | 5.3 ± 5.1 | 5.1 ± 5.1 | −0.07 (−0.35; 0.21), 0.61 |
| PSQI-sleep | 7.2 ± 2.5 | 7.8 ± 2.9 | 6.3 ± 2.4 | 7.0 ± 3.1 | −0.14 (−0.42; 0.14), 0.33 | 5.6 ± 2.6 | 6.2 ± 3.1 | −0.10 (−0.38; 0.18), 0.49 | 5.3 ± 2.4 | 3.2 ± 3.1 | −0.07 (−0.35; 0.21), 0.63 |
| Component 1 | 1.6 ± 0.7 | 1.6 ± 0.7 | 1.4 ± 0.7 | 1.5 ± 0.8 | −0.07 (−0.35; 0.21), 0.64 | 1.3 ± 0.7 | 1.4 ± 0.7 | −0.02 (−0.30; 0.26), 0.90 | 1.3 ± 0.6 | 1.3 ± 0.7 | −0.01 (−0.28; 0.28), 0.99 |
| Component 2 | 1.8 ± 1.0 | 1.8 ± 1.0 | 1.4 ± 1.0 | 1.3 ± 1.1 | −0.14 (−0.42; 0.14), 0.33 | 1.2 ± 1.0 | 1.4 ± 1.1 | −0.15 (−0.43; 0.14), 0.31 | 1.4 ± 0.9 | 1.5 ± 1.0 | −0.09 (−0.37; 0.20), 0.55 |
| Component 3 | 0.8 ± 0.7 | 0.9 ± 0.8 | 0.7 ± 0.7 | 0.8 ± 0.8 | −0.05 (−0.33; 0.23), 0.74 | 0.7 ± 0.8 | 0.6 ± 0.7 | 0.21 (−0.07; 0.49), 0.14 | 0.7 ± 0.7 | 0.6 ± 0.7 | 0.15 (−0.13; 0.43), 0.30 |
| Component 4 | 0.3 ± 0.6 | 0.6 ± 0.8 | 0.3 ± 0.5 | 0.5 ± 0.9 | −0.20 (−0.48; 0.08), 0.17 | 0.3 ± 0.6 | 0.4 ± 0.7 | −0.10 (−0.38; 0.18), 0.50 | 0.3 ± 0.5 | 0.4 ± 0.8 | 0.05 (−0.23; 0.33), 0.72 |
| Component 5 | 1.3 ± 0.5 | 1.4 ± 0.5 | 1.3 ± 0.4 | 1.3 ± 0.4 | 0.07 (−0.21; 0.35), 0.63 | 1.2 ± 0.4 | 1.2 ± 0.5 | −0.02 (−0.30; 0.26), 0.88 | 1.2 ± 0.4 | 1.1 ± 0.5 | 0.22 (−0.06; 0.50), 0.13 |
| Component 6 | 0.1 ± 0.2 | 0.2 ± 0.6 | 0.1 ± 0.1 | 0.2 ± 0.6 | −0.17 (−0.45; 0.11), 0.23 | 0.1 ± 0.1 | 0.1 ± 0.5 | −0.12 (−0.40; 0.16), 0.39 | 0.1 ± 0.3 | 0.2 ± 0.6 | −0.02 (−0.30; 0.26), 0.88 |
| Component 7 | 1.4 ± 0.6 | 1.4 ± 0.7 | 1.2 ± 0.6 | 1.2 ± 0.7 | −0.03 (−0.31; 0.25), 0.85 | 0.8 ± 0.7 | 1.1 ± 0.8 | −0.27 (−0.55; 0.01), 0.06 | 0.7 ± 0.6 | 1.2 ± 0.8 | −0.54 (−0.82; −0.26), <0.001 |
| Pain, QST,°C | Data not collected | Data not collected | |||||||||
| Warm sensibility | 34.0 ± 1.3 | 33.5 ± 0.7 | 33.8 ± 0.8 | 33.9 ± 1.2 | −0.07 (−0.35; 0.21), 0.61 | ||||||
| Cold sensibility | 30.8 ± 1.1 | 31.0 ± 0.7 | 30.7 ± 0.9 | 30.6 ± 1.2 | 0.17 (−0.11, 0.45), 0.22 | ||||||
| Warm pain | 42.5 ± 3.7 | 42.5 ± 3.5 | 43.2 ± 3.2 | 42.2 ± 2.9 | 0.27 (−0.01; 0.55), 0.06 | ||||||
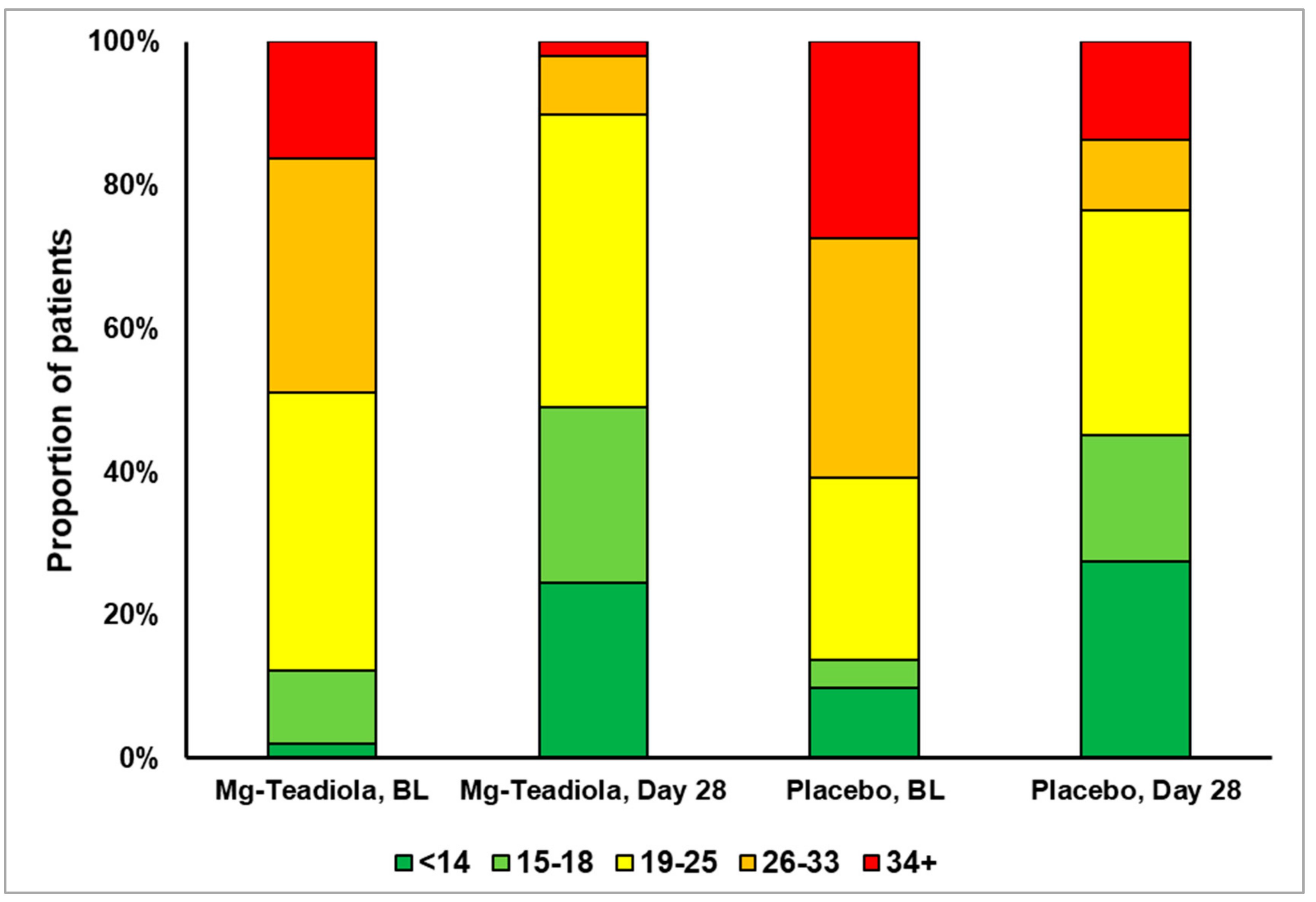
| Cold pain | 17.3 ± 10.7 | 18.0 ± 9.9 | 15.6 ± 10.3 | 19.9 ± 9.3 | −0.36 (−0.64; −0.08), 0.01 | ||||||
| Concentration of Mg | |||||||||||
| Plasma, mmol/L | 0.87 ± 0.07 | 0.87 ± 0.06 | 0.87 ± 0.06 | 0.87 ± 0.06 | 0.08 (−0.33; 0.48), 0.71 | 0.87 ± 0.01 | 0.88 ± 0.01 | −0.26 (−0.14; 0.66), 0.20 | 0.88 ± 0.06 | 0.88 ± 0.05 | −0.02 (−0.41; 0.38), 0.94 |
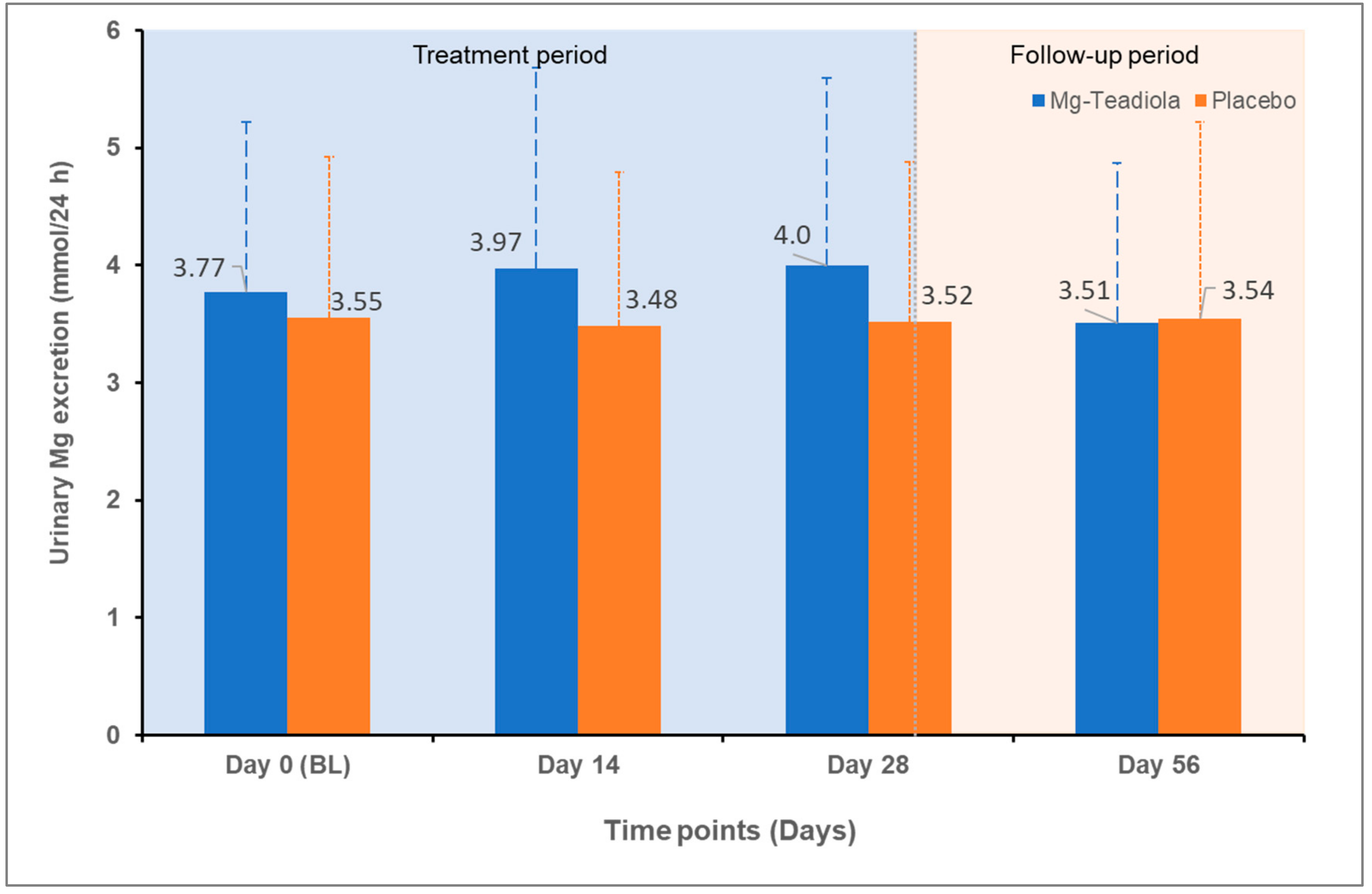
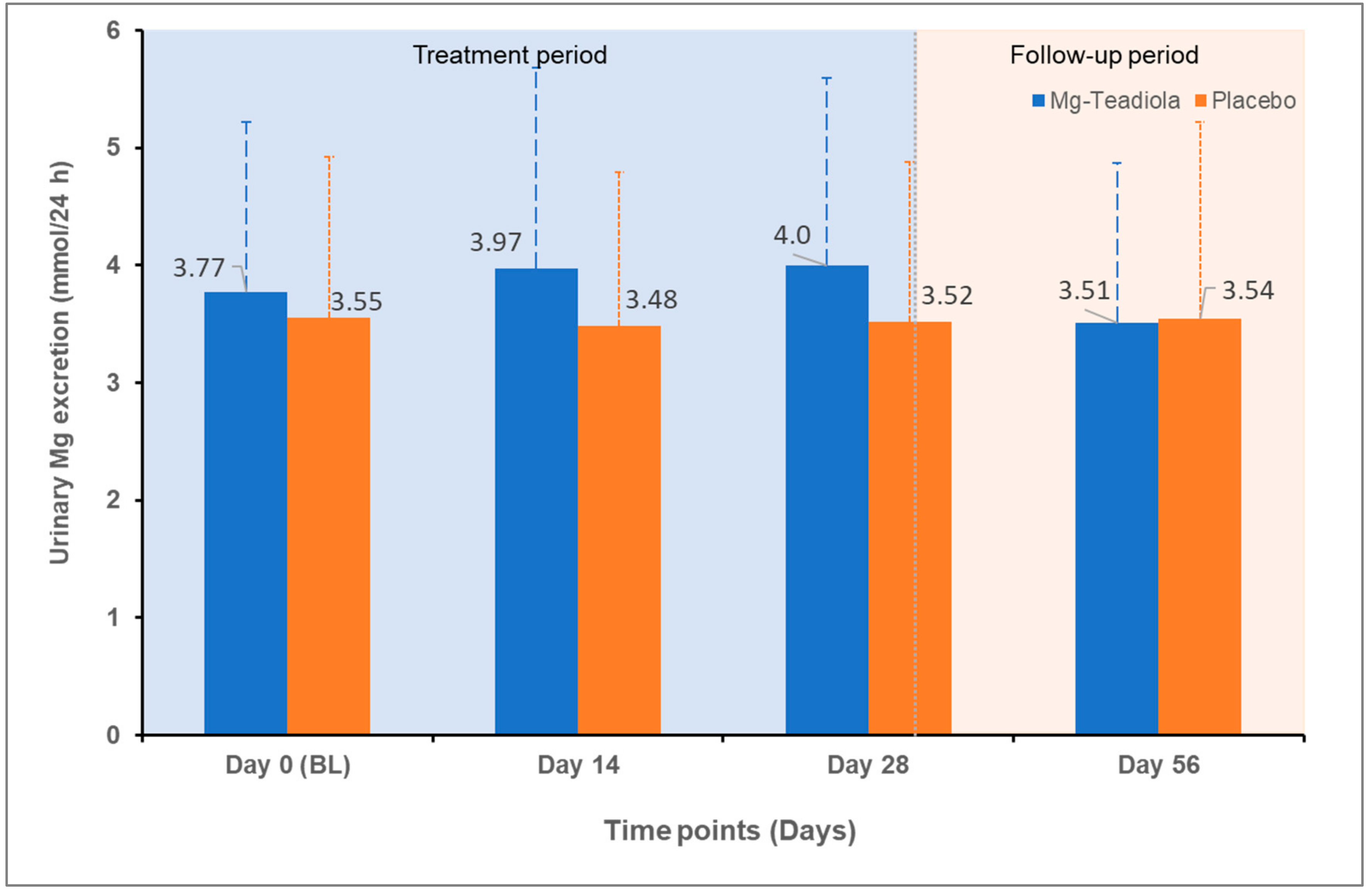
| Urine, mmol/24 h | 3.77 ± 1.45 | 3.55 ± 1.37 | 3.97 ± 1.71 | 3.48 ± 1.31 | 0.32 (−0.08; 0.72), 0.12 | 4.00 ± 1.59 | 3.52 ± 1.36 | 0.32 (−0.07; 0.72), 0.11 | 3.51 ± 1.36 | 3.54 ± 1.68 | 0.32 (−0.08; 0.72), 0.92 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noah, L.; Morel, V.; Bertin, C.; Pouteau, E.; Macian, N.; Dualé, C.; Pereira, B.; Pickering, G. Effect of a Combination of Magnesium, B Vitamins, Rhodiola, and Green Tea (L-Theanine) on Chronically Stressed Healthy Individuals—A Randomized, Placebo-Controlled Study. Nutrients 2022, 14, 1863. https://doi.org/10.3390/nu14091863
Noah L, Morel V, Bertin C, Pouteau E, Macian N, Dualé C, Pereira B, Pickering G. Effect of a Combination of Magnesium, B Vitamins, Rhodiola, and Green Tea (L-Theanine) on Chronically Stressed Healthy Individuals—A Randomized, Placebo-Controlled Study. Nutrients. 2022; 14(9):1863. https://doi.org/10.3390/nu14091863
Chicago/Turabian StyleNoah, Lionel, Veronique Morel, Claire Bertin, Etienne Pouteau, Nicolas Macian, Christian Dualé, Bruno Pereira, and Gisèle Pickering. 2022. "Effect of a Combination of Magnesium, B Vitamins, Rhodiola, and Green Tea (L-Theanine) on Chronically Stressed Healthy Individuals—A Randomized, Placebo-Controlled Study" Nutrients 14, no. 9: 1863. https://doi.org/10.3390/nu14091863
APA StyleNoah, L., Morel, V., Bertin, C., Pouteau, E., Macian, N., Dualé, C., Pereira, B., & Pickering, G. (2022). Effect of a Combination of Magnesium, B Vitamins, Rhodiola, and Green Tea (L-Theanine) on Chronically Stressed Healthy Individuals—A Randomized, Placebo-Controlled Study. Nutrients, 14(9), 1863. https://doi.org/10.3390/nu14091863