
Identifying Effects of Urinary Metals on Type 2 Diabetes in U.S. Adults: Cross-Sectional Analysis of National Health and Nutrition Examination Survey 2011–2016




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. T2D Definition
2.3. Measurement of Urinary Metal Concentrations
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
3.2. Multi-Metal Selections
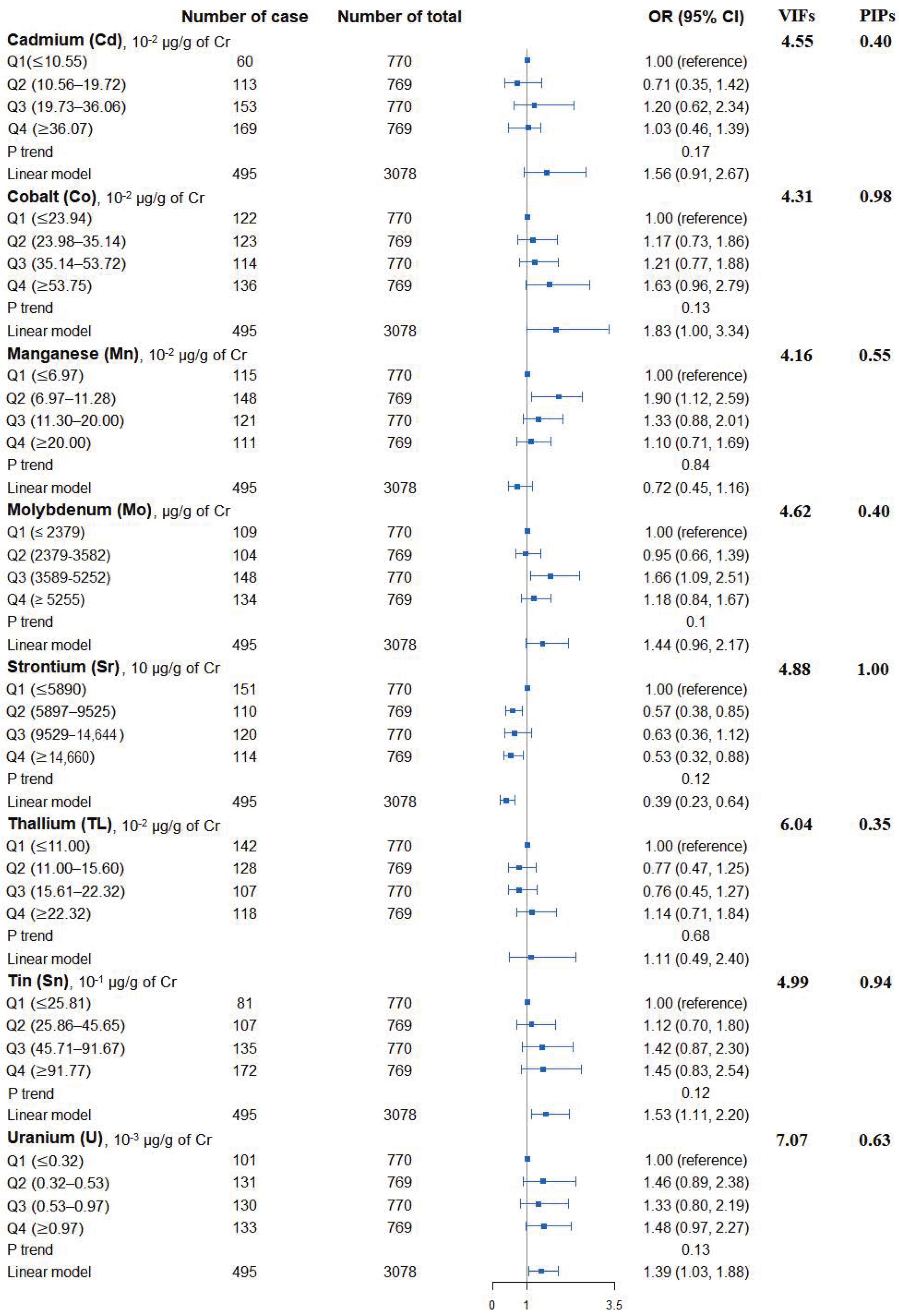
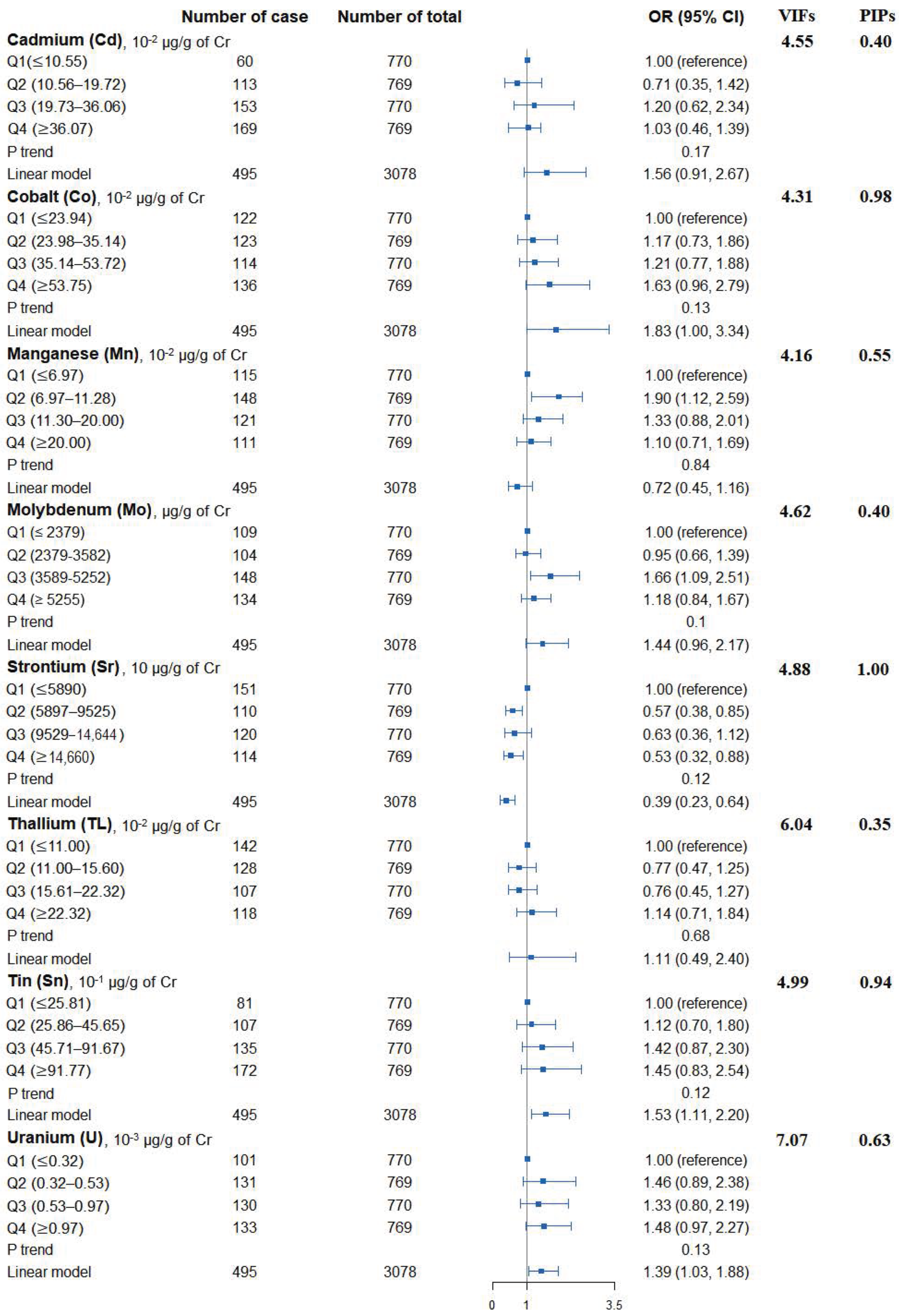
3.3. Single Urinary Metal Levels and the Risk of T2D
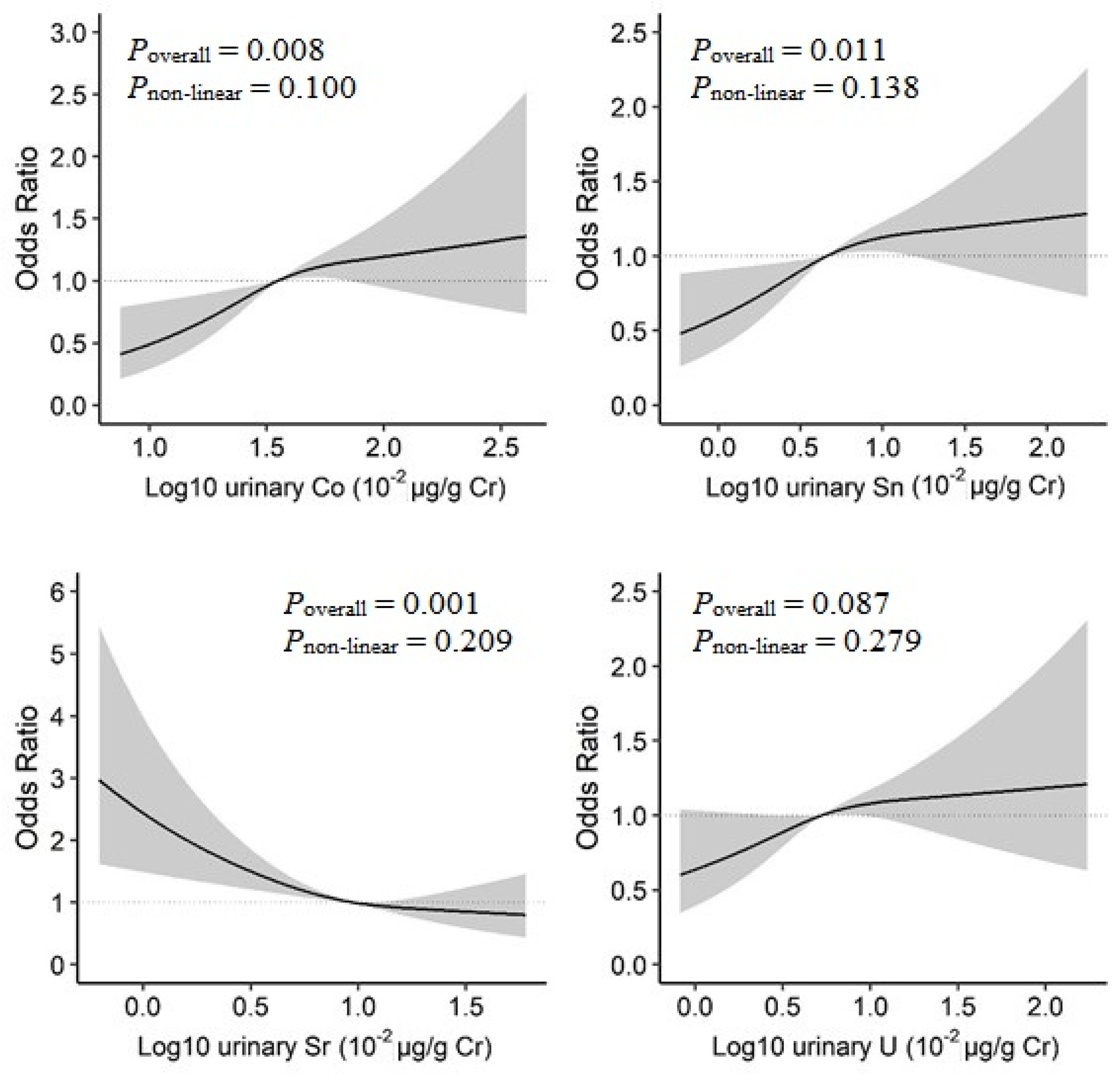
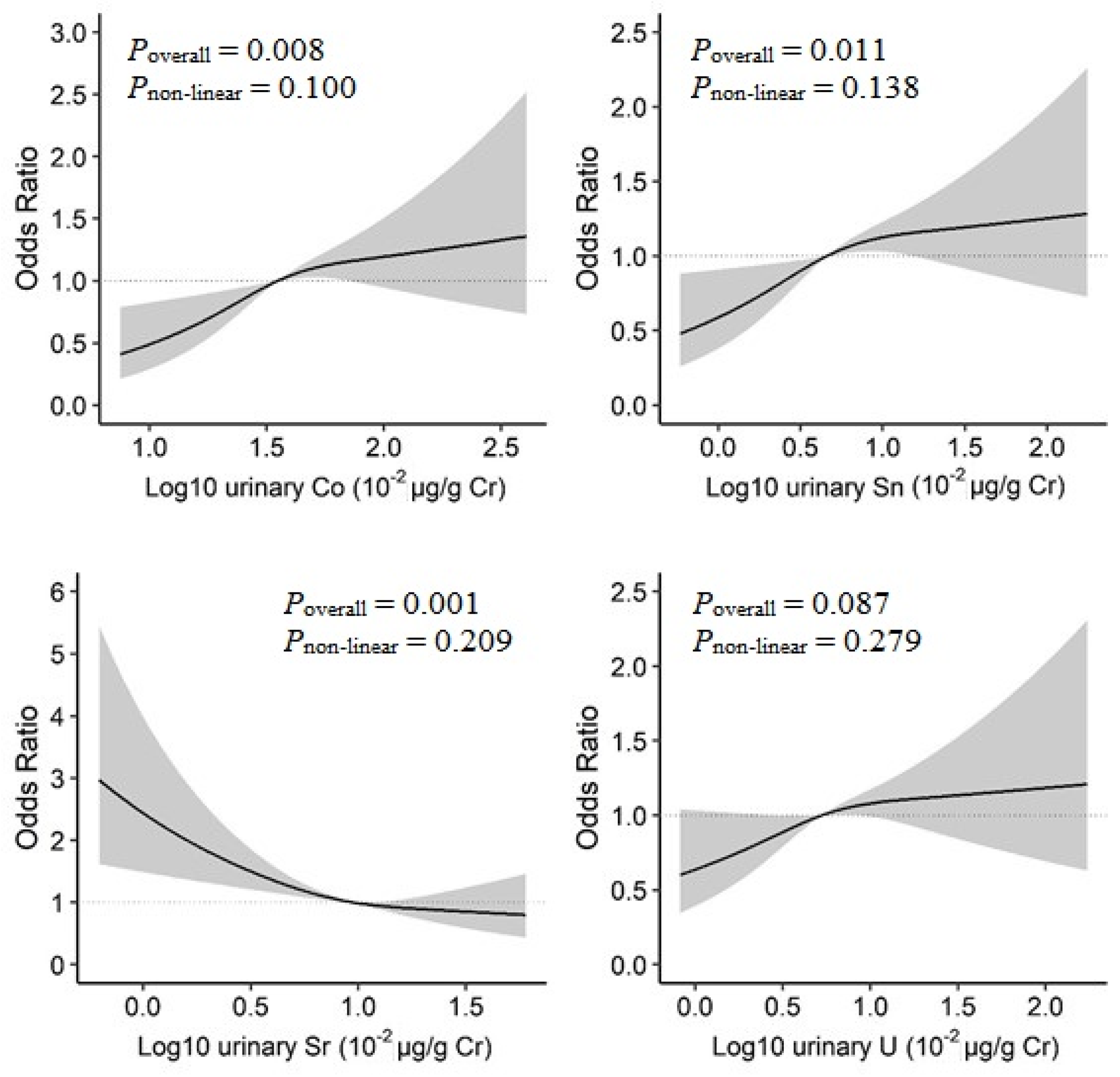
3.4. Dose–Response Associations and Their Interactions in Four Identified Metals
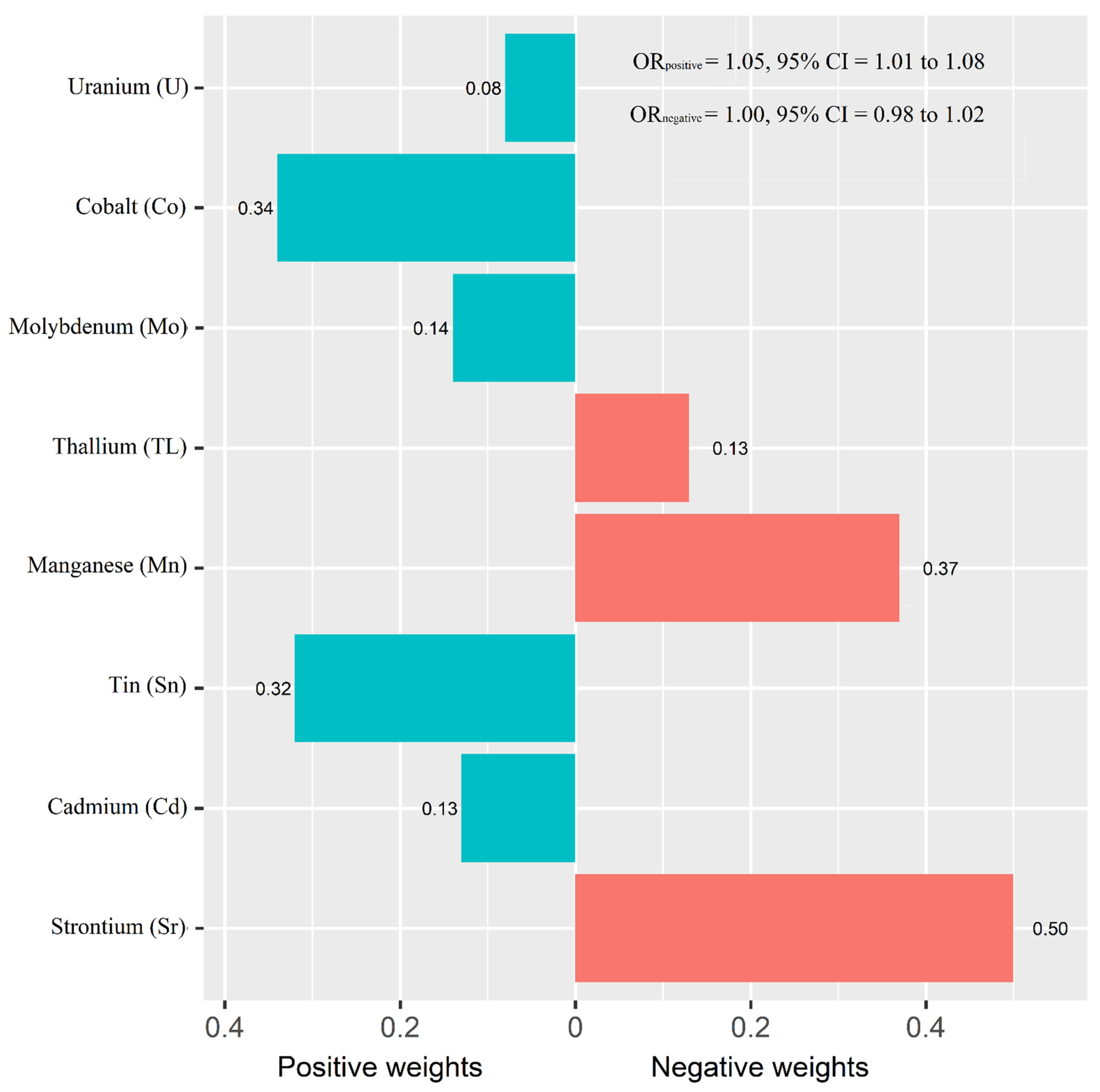
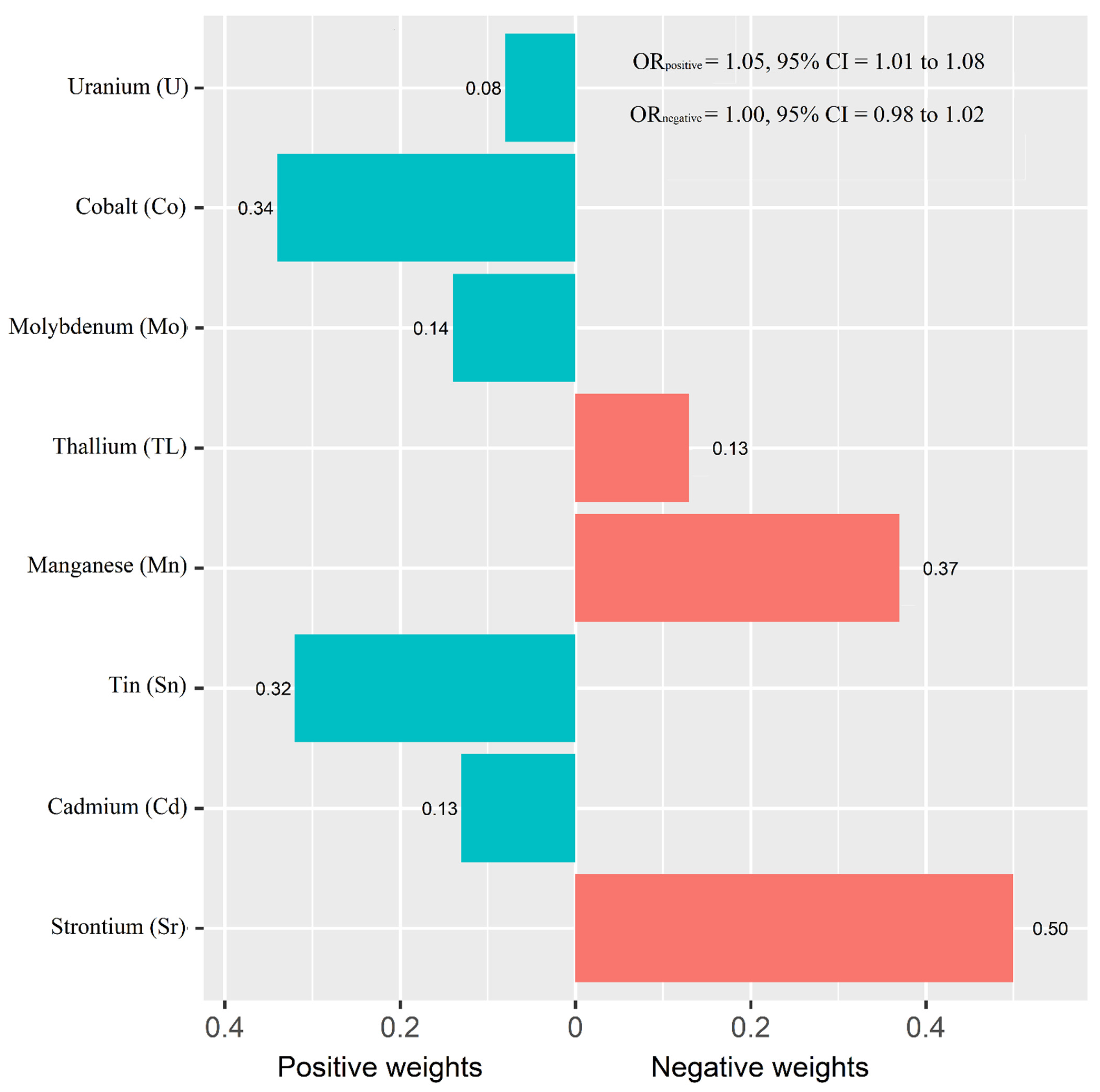
3.5. Comparing Overall Effects of the Combined Urinary Metal Mixture on T2D
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef] [PubMed]
- Zheng, T.; Liu, S.; Bai, Y.; Cheng, N.; Buka, S.; Yang, A.; Shi, K.; Zhang, X.; Li, Y.; Xu, S.; et al. Current Understanding of the Relationship between Metal Exposures and Risk of Type 2 Diabetes. Curr. Res. Diabetes Obes. J. 2018, 7, 40–48. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Yang, A.; Cheng, N.; Huang, W.; Huang, P.; Liu, N.; Bai, Y. Sex-specific associations of blood and urinary manganese levels with glucose levels, insulin resistance and kidney function in US adults: National health and nutrition examination survey 2011–2016. Chemosphere 2020, 258, 126940. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.M.; Lo, K.; Zheng, T.Z.; Yang, J.L.; Bai, Y.N.; Feng, Y.Q.; Cheng, N.; Liu, S.M. Environmental heavy metals and cardiovascular diseases: Status and future direction. Chronic Dis. Transl. Med. 2020, 6, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.; Liu, S.; Cheng, Z.; Pu, H.; Cheng, N.; Ding, J.; Li, J.; Li, H.; Hu, X.; Ren, X.; et al. Dose-response analysis of environmental exposure to multiple metals and their joint effects with fasting plasma glucose among occupational workers. Chemosphere 2017, 186, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Hill-Briggs, F.; Adler, N.E.; Berkowitz, S.A.; Chin, M.H.; Gary-Webb, T.L.; Navas-Acien, A.; Thornton, P.L.; Haire-Joshu, D. Social Determinants of Health and Diabetes: A Scientific Review. Diabetes Care 2020, 44, 258–279. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.C.N.; Lim, L.L.; Wareham, N.J.; Shaw, J.E.; Orchard, T.J.; Zhang, P.; Lau, E.S.H.; Eliasson, B.; Kong, A.P.S.; Ezzati, M.; et al. The Lancet Commission on diabetes: Using data to transform diabetes care and patient lives. Lancet 2021, 396, 2019–2082. [Google Scholar] [CrossRef]
- Kuo, C.C.; Navas-Acien, A. Commentary: Environmental chemicals and diabetes: Which ones are we missing? Int. J. Epidemiol. 2015, 44, 248–250. [Google Scholar] [CrossRef] [Green Version]
- Liu, B.; Feng, W.; Wang, J.; Li, Y.; Han, X.; Hu, H.; Guo, H.; Zhang, X.; He, M. Association of urinary metals levels with type 2 diabetes risk in coke oven workers. Environ. Pollut. 2016, 210, 1–8. [Google Scholar] [CrossRef]
- Hansen, A.F.; Simic, A.; Asvold, B.O.; Romundstad, P.R.; Midthjell, K.; Syversen, T.; Flaten, T.P. Trace elements in early phase type 2 diabetes mellitus-A population-based study. The HUNT study in Norway. J. Trace Elem. Med. Biol. Organ Soc. Miner. Trace Elem. GMS 2017, 40, 46–53. [Google Scholar] [CrossRef]
- Moon, S.S. Association of lead, mercury and cadmium with diabetes in the Korean population: The Korea National Health and Nutrition Examination Survey (KNHANES) 2009–2010. Diabet. Med. A J. Br. Diabet. Assoc. 2013, 30, e143–e148. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.; Liu, S.; Cheng, N.; Pu, H.; Dai, M.; Ding, J.; Li, J.; Li, H.; Hu, X.; Ren, X.; et al. Multiple metals exposure, elevated blood glucose and dysglycemia among Chinese occupational workers. J. Diabetes Its Complicat. 2017, 31, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Menke, A.; Guallar, E.; Cowie, C.C. Metals in Urine and Diabetes in U.S. Adults. Diabetes 2016, 65, 164–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bobb, J.F.; Claus Henn, B.; Valeri, L.; Coull, B.A. Statistical software for analyzing the health effects of multiple concurrent exposures via Bayesian kernel machine regression. Environ. Health A Glob. Access Sci. Source 2018, 17, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Gao, D.; Zhang, G.; Zhang, X.; Li, Q.; Gao, Q.; Chen, R.; Xu, S.; Huang, L.; Zhang, Y.; et al. Exposure to multiple metals in early pregnancy and gestational diabetes mellitus: A prospective cohort study. Environ. Int. 2020, 135, 105370. [Google Scholar] [CrossRef]
- Yuan, Y.; Xiao, Y.; Yu, Y.; Liu, Y.; Feng, W.; Qiu, G.; Wang, H.; Liu, B.; Wang, J.; Zhou, L.; et al. Associations of multiple plasma metals with incident type 2 diabetes in Chinese adults: The Dongfeng-Tongji Cohort. Environ. Pollut. 2018, 237, 917–925. [Google Scholar] [CrossRef]
- Bobb, J.F.; Valeri, L.; Claus Henn, B.; Christiani, D.C.; Wright, R.O.; Mazumdar, M.; Godleski, J.J.; Coull, B.A. Bayesian kernel machine regression for estimating the health effects of multi-pollutant mixtures. Biostatistics Oxf. Engl. 2015, 16, 493–508. [Google Scholar] [CrossRef]
- Zipf, G.; Chiappa, M.; Porter, K.S.; Ostchega, Y.; Lewis, B.G.; Dostal, J. National health and nutrition examination survey: Plan and operations, 1999–2010. Vital Health Stat. Ser. 1 Programs Collect. Proced. 2013, 56, 1–37. [Google Scholar]
- ADA. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S13–S28. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey; (NHANES) Laboratory Procedures Manual. 2011. Available online: https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/manuals.aspx?BeginYear=2011 (accessed on 28 March 2022).
- Succop, P.A.; Clark, S.; Chen, M.; Galke, W. Imputation of data values that are less than a detection limit. J. Occup. Environ. Hyg. 2004, 1, 436–441. [Google Scholar] [CrossRef]
- Zheng, Y.; Ley, S.H.; Hu, F.B. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat. Rev. Endocrinol. 2018, 14, 88–98. [Google Scholar] [CrossRef] [PubMed]
- VanderWeele, T.J. Principles of confounder selection. Eur. J. Epidemiol. 2019, 34, 211–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tyrrell, J.; Melzer, D.; Henley, W.; Galloway, T.S.; Osborne, N.J. Associations between socioeconomic status and environmental toxicant concentrations in adults in the USA: NHANES 2001–2010. Environ. Int. 2013, 59, 328–335. [Google Scholar] [CrossRef]
- Marriott, B.P.; Hunt, K.J.; Malek, A.M.; Newman, J.C. Trends in Intake of Energy and Total Sugar from Sugar-Sweetened Beverages in the United States among Children and Adults, NHANES 2003–2016. Nutrients 2019, 11, 2004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd ed.; U.S. Department of Health and Human Services: Washington, DC, USA, 2018.
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., III; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Stafoggia, M.; Breitner, S.; Hampel, R.; Basagana, X. Statistical Approaches to Address Multi-Pollutant Mixtures and Multiple Exposures: The State of the Science. Curr. Environ. Health Rep. 2017, 4, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Hou, Q.; Huang, L.; Ge, X.; Yang, A.; Luo, X.; Huang, S.; Xiao, Y.; Jiang, C.; Li, L.; Pan, Z.; et al. Associations between multiple serum metal exposures and low birth weight infants in Chinese pregnant women: A nested case-control study. Chemosphere 2019, 231, 225–232. [Google Scholar] [CrossRef]
- Zhao, H.; Tang, J.; Zhu, Q.; He, H.; Li, S.; Jin, L.; Zhang, X.; Zhu, L.; Guo, J.; Zhang, D.; et al. Associations of prenatal heavy metals exposure with placental characteristics and birth weight in Hangzhou Birth Cohort: Multi-pollutant models based on elastic net regression. Sci. Total Environ. 2020, 742, 140613. [Google Scholar] [CrossRef]
- Yang, J.; Lu, Y.; Bai, Y.; Cheng, Z. Sex-specific and dose-response relationships of urinary cobalt and molybdenum levels with glucose levels and insulin resistance in U.S. adults. J. Environ. Sci. 2023, 124, 42–49. [Google Scholar] [CrossRef]
- Midi, H.; Sarkar, S.K.; Rana, S. Collinearity diagnostics of binary logistic regression model. J. Interdiscip. Math. 2010, 13, 253–267. [Google Scholar] [CrossRef]
- Carrico, C.; Gennings, C.; Wheeler, D.C.; Factor-Litvak, P. Characterization of Weighted Quantile Sum Regression for Highly Correlated Data in a Risk Analysis Setting. J. Agric. Biol. Environ. Stat. 2015, 20, 100–120. [Google Scholar] [CrossRef]
- Jin, R.; Zhu, X.; Shrubsole, M.J.; Yu, C.; Xia, Z.; Dai, Q. Associations of renal function with urinary excretion of metals: Evidence from NHANES 2003-2012. Environ. Int. 2018, 121, 1355–1362. [Google Scholar] [CrossRef] [PubMed]
- Knol, M.J.; VanderWeele, T.J.; Groenwold, R.H.; Klungel, O.H.; Rovers, M.M.; Grobbee, D.E. Estimating measures of interaction on an additive scale for preventive exposures. Eur. J. Epidemiol. 2011, 26, 433–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domingo-Relloso, A.; Grau-Perez, M.; Briongos-Figuero, L.; Gomez-Ariza, J.L.; Garcia-Barrera, T.; Duenas-Laita, A.; Bobb, J.F.; Chaves, F.J.; Kioumourtzoglou, M.A.; Navas-Acien, A.; et al. The association of urine metals and metal mixtures with cardiovascular incidence in an adult population from Spain: The Hortega Follow-Up Study. Int. J. Epidemiol. 2019, 48, 1839–1849. [Google Scholar] [CrossRef] [PubMed]
- Lo, K.; Yang, J.L.; Chen, C.L.; Liu, L.; Huang, Y.Q.; Feng, Y.Q.; Yang, A.M. Associations between blood and urinary manganese with metabolic syndrome and its components: Cross-sectional analysis of National Health and Nutrition Examination Survey 2011–2016. Sci. Total Environ. 2021, 780, 146527. [Google Scholar] [CrossRef]
- Bertuloso, B.D.; Podratz, P.L.; Merlo, E.; de Araújo, J.F.; Lima, L.C.; de Miguel, E.C.; de Souza, L.N.; Gava, A.L.; de Oliveira, M.; Miranda-Alves, L.; et al. Tributyltin chloride leads to adiposity and impairs metabolic functions in the rat liver and pancreas. Toxicol. Lett. 2015, 235, 45–59. [Google Scholar] [CrossRef]
- Miura, Y.; Hori, Y.; Kimura, S.; Hachiya, H.; Sakurai, Y.; Inoue, K.; Sawada, T.; Kubota, K. Triphenyltin impairs insulin secretion by decreasing glucose-induced NADP(H) and ATP production in hamster pancreatic beta-cells. Toxicology 2012, 299, 165–171. [Google Scholar] [CrossRef]
- Chen, Y.W.; Lan, K.C.; Tsai, J.R.; Weng, T.I.; Yang, C.Y.; Liu, S.H. Tributyltin exposure at noncytotoxic doses dysregulates pancreatic beta-cell function in vitro and in vivo. Arch. Toxicol. 2017, 91, 3135–3144. [Google Scholar] [CrossRef]
- Zuo, Z.; Wu, T.; Lin, M.; Zhang, S.; Yan, F.; Yang, Z.; Wang, Y.; Wang, C. Chronic exposure to tributyltin chloride induces pancreatic islet cell apoptosis and disrupts glucose homeostasis in male mice. Environ. Sci. Technol. 2014, 48, 5179–5186. [Google Scholar] [CrossRef]
- Liu, B.; Sun, Y.; Lehmler, H.J.; Bao, W. Association between urinary tin concentration and diabetes in nationally representative sample of US adults. J. Diabetes 2018, 10, 977–983. [Google Scholar] [CrossRef]
- Simonsen, L.O.; Harbak, H.; Bennekou, P. Cobalt metabolism and toxicology—a brief update. Sci. Total Environ. 2012, 432, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Saker, F.; Ybarra, J.; Leahy, P.; Hanson, R.W.; Kalhan, S.C.; Ismail-Beigi, F. Glycemia-lowering effect of cobalt chloride in the diabetic rat: Role of decreased gluconeogenesis. Am. J. Physiol. 1998, 274, E984–E991. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Huang, H.; He, X.; Duan, W.; Mo, X. Sex differences in the link between blood cobalt concentrations and insulin resistance in adults without diabetes. Environ. Health Prev. Med. 2021, 26, 42. [Google Scholar] [CrossRef] [PubMed]
- Cao, B.; Fang, C.; Peng, X.; Li, X.; Hu, X.; Xiang, P.; Zhou, L.; Liu, H.; Huang, Y.; Zhang, Q.; et al. U-shaped association between plasma cobalt levels and type 2 diabetes. Chemosphere 2021, 267, 129224. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Guo, Q.; Wang, Q.; Luo, C.; Chen, S.; Wen, S.; Tan, A.; Yang, W.; Bao, W.; Hu, F.B.; et al. Association between plasma strontium, a bone-seeking element, and type 2 diabetes mellitus. Clin. Nutr. Edinb. Scotl. 2020, 39, 2151–2157. [Google Scholar] [CrossRef]
- Hellman, B.; Gylfe, E.; Bergsten, P.; Grapengiesser, E.; Berts, A.; Liu, Y.J.; Tengholm, A.; Westerlund, J. Oscillatory signaling and insulin release in human pancreatic beta-cells exposed to strontium. Endocrinology 1997, 138, 3161–3165. [Google Scholar] [CrossRef]
- Maehira, F.; Ishimine, N.; Miyagi, I.; Eguchi, Y.; Shimada, K.; Kawaguchi, D.; Oshiro, Y. Anti-diabetic effects including diabetic nephropathy of anti-osteoporotic trace minerals on diabetic mice. Nutrition 2011, 27, 488–495. [Google Scholar] [CrossRef]
- Barneo-Caragol, C.; Martinez-Morillo, E.; Rodriguez-Gonzalez, S.; Lequerica-Fernandez, P.; Vega-Naredo, I.; Alvarez Menendez, F.V. Strontium and oxidative stress in normal pregnancy. J. Trace Elem. Med. Biol. Organ Soc. Miner. Trace Elem. 2018, 45, 57–63. [Google Scholar] [CrossRef]
- Vidal, C.; Gunaratnam, K.; Tong, J.; Duque, G. Biochemical changes induced by strontium ranelate in differentiating adipocytes. Biochimie 2013, 95, 793–798. [Google Scholar] [CrossRef]
- Ge, X.; Yang, A.; Huang, S.; Luo, X.; Hou, Q.; Huang, L.; Zhou, Y.; Li, D.; Lv, Y.; Li, L.; et al. Sex-specific associations of plasma metals and metal mixtures with glucose metabolism: An occupational population-based study in China. Sci. Total Environ. 2021, 760, 143906. [Google Scholar] [CrossRef]
- Rana, J. Comparison of Different Methods to Handle Chemical Mixtures in Environmental Epidemiology Studies. Master’s Thesis, University of Massachusetts Amherst, Amherst, MA, USA, 2019. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variables a | Non-T2D (n = 2583) | With T2D (n = 495) | Total (n = 3078) | p-Value |
|---|---|---|---|---|
| Survey cycle | 0.002 | |||
| 2011–2012 | 782 (30.3) | 156 (31.5) | 938 (30.5) | |
| 2013–2014 | 963 (37.3) | 146 (29.5) | 1109 (36.0) | |
| 2015–2016 | 838 (32.4) | 193 (39.0) | 1031 (33.5) | |
| Men | 1363 (52.8) | 302 (61.0) | 1665 (54.1) | <0.001 |
| Age, years old | 44.1 ± 16.6 | 58.2 ± 13.6 | 46.4 ± 17.0 | <0.001 |
| 18–39 | 1181 (45.7) | 54 (10.9) | 1235 (40.1) | |
| 40–59 | 854 (33.1) | 184 (37.2) | 1038 (33.7) | |
| ≥60 | 548 (21.2) | 257 (51.9) | 805 (26.2) | |
| Race | 0.038 | |||
| Non-Hispanic White | 1112 (43.1) | 186 (37.6) | 1298 (42.2) | |
| Non-Hispanic Black | 528 (20.4) | 109 (22.0) | 637 (20.7) | |
| Hispanics | 589 (22.8) | 138 (27.9) | 727 (23.6) | |
| Other race | 354 (13.7) | 62 (12.5) | 416 (13.5) | |
| Education | <0.001 | |||
| Less than high school | 411 (15.9) | 117 (23.6) | 528 (17.2) | |
| High school | 529 (20.5) | 110 (22.2) | 639 (20.8) | |
| At least some college | 1643 (63.6) | 268 (54.1) | 1911 (62.1) | |
| Poverty income ratio | 0.684 | |||
| Below poverty (<1) | 627 (24.3) | 125 (25.3) | 752 (24.4) | |
| At or above poverty (≥1) | 1956 (75.7) | 370 (74.7) | 2326 (75.6) | |
| BMI, kg/m2 | <0.001 | |||
| ≤25 | 860 (33.3) | 70 (14.1) | 930 (30.2) | |
| 25.1–29.9 | 866 (33.5) | 143 (28.9) | 1009 (32.8) | |
| ≥30 | 857 (33.2) | 282 (57.0) | 1139 (37.0) | |
| Smoking status | <0.001 | |||
| Never smoker | 1392 (53.9) | 222 (44.8) | 1614 (52.4) | |
| Former smoker | 600 (23.2) | 172 (34.7) | 772 (25.1) | |
| Current smoker | 591 (22.9) | 101 (20.4) | 692 (22.5) | |
| Alcohol consumption | <0.001 | |||
| No | 1352 (52.3) | 209 (42.2) | 1561 (50.7) | |
| Yes | 1231 (47.7) | 286 (57.8) | 1517 (49.3) | |
| Physical activity | 0.034 | |||
| Substandard | 2208 (85.5) | 441 (89.1) | 2649 (86.1) | |
| Standard | 375 (14.5) | 54 (10.9) | 429 (13.9) | |
| Average daily energy intake | 0.004 | |||
| Q1 (<1515 kcal) | 519 (20.1) | 117 (23.6) | 636 (20.7) | |
| Q2 (1515–2054 kcal) | 536 (20.8) | 120 (24.2) | 656 (21.3) | |
| Q3 (2065–2697 kcal) | 631 (24.4) | 126 (25.5) | 757 (24.6) | |
| Q4 (≥2697 kcal) | 897 (34.7) | 132 (26.7) | 1029 (33.4) | |
| With hypertension | 849 (32.9) | 346 (69.9) | 1195 (38.8) | <0.001 |
| Family history of diabetes | 566 (21.9) | 54 (10.9) | 620 (20.1) | <0.001 |
| ALT | <0.001 | |||
| Normal | 2262 (87.6) | 401 (81.0) | 2663 (86.5) | |
| High | 321 (12.4) | 94 (19.0) | 415 (13.5) | |
| GGT | <0.001 | |||
| Normal | 2342 (90.7) | 410 (82.8) | 2752 (89.4) | |
| High | 241 (9.3) | 85 (17.2) | 326 (10.6) | |
| eGFR (ml/min per 1.73 m2) | 143 ± 12.2 | 141 ± 15.4 | 142 ± 12.8 | <0.001 |
| Urinary metal concentrations | ||||
| Antimony (Sb), 10−2 µg/g of Cr | 4.83 (3.31, 7.44) | 4.97 (3.56, 7.12) | 4.85 (3.35, 7.27) | <0.001 |
| Arsenic (As), µg/g of Cr | 6.77 (3.96, 14.37) | 7.52 (4.39, 14.34) | 6.86 (4.02, 14.35) | <0.001 |
| Barium (Ba), µg/g of Cr | 1.15 (0.65, 2.07) | 1.03 (0.51, 2.23) | 1.13 (0.62, 2.08) | <0.001 |
| Cadmium (Cd), µg/g of Cr | 0.19 (9.85, 34.20) | 0.26 (0.16, 0.44) | 0.20 (0.12, 0.36) | <0.001 |
| Cesium (Cs), µg/g of Cr | 4.12 (3.03, 5.85) | 4.41 (3.10, 5.82) | 4.15 (3.03, 5.85) | <0.001 |
| Cobalt (Co), µg/g of Cr | 0.35 (0.24, 0.53) | 0.36 (0.24, 0.56) | 0.35 (0.24, 0.54) | <0.001 |
| Lead (Pb), µg/g of Cr | 0.35 (0.22, 0.58) | 0.40 (0.25, 0.60) | 0.36 (0.22, 0.58) | <0.001 |
| Manganese (Mn), 10−1 µg/g of Cr | 1.14 (0.69, 2.00) | 1.06 (0.70, 1.85) | 1.13 (0.70, 2.00) | <0.001 |
| Mercury (Hg), µg/g of Cr | 0.28 (0.14, 0.58) | 0.27 (0.13, 0.56) | 0.28 (0.14, 0.58) | <0.001 |
| Molybdenum (Mo), µg/g of Cr | 35.18 (23.41, 52.22) | 39.08 (25.71, 53.64) | 35.86 (23.79, 52.52) | <0.001 |
| Strontium (Sr), 10 µg/g of Cr | 9.60 (6.01, 14.78) | 9.03 (4.83, 13.92) | 9.53 (5.89, 14.66) | <0.001 |
| Thallium (Tl), µg/g of Cr | 0.16 (0.1, 0.22) | 0.15 (0.10, 0.22) | 0.16 (0.11, 0.22) | <0.001 |
| Tin (Sn), µg/g of Cr | 0.43 (0.25, 0.85) | 0.59 (0.34, 1.28) | 0.46 (0.26, 0.92) | <0.001 |
| Tungsten (W), 10−2 µg/g of Cr | 5.93 (3.51, 10.59) | 6.19 (3.71, 10.28) | 5.97 (3.53, 10.53) | <0.001 |
| Uranium (U), 10−3 µg/g of Cr | 5.21 (3.13, 9.62) | 5.67 (3.44, 10.20) | 5.26 (3.19, 9.71) | <0.001 |
| RERI (Relative Excess Risk Due to Interaction) | AP (Attributable Proportion) | Pmulti-interaction a | |
|---|---|---|---|
| Co and Sn | 0.14 (−0.39, 0.67) | 0.09 (−0.25, 0.43) | 0.75 |
| Co and Sr | −0.23 (−0.79, 0.33) | −0.21 (−0.73, 0.30) | 0.45 |
| Co and U | −0.02 (−0.53, 0.48) | −0.02 (−0.41, 0.38) | 0.89 |
| Sn and Sr | 0.57 (0.18, 0.96) * | 0.48 (0.16, 0.80) * | 0.01 * |
| Sn and U | 0.02 (−0.51, 0.55) | 0.01 (−0.36, 0.38) | 0.96 |
| Sr and U | −0.02 (−0.48, 0.44) | −0.02 (−0.46, 0.41) | 0.95 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, J.; Chan, K.; Choi, C.; Yang, A.; Lo, K. Identifying Effects of Urinary Metals on Type 2 Diabetes in U.S. Adults: Cross-Sectional Analysis of National Health and Nutrition Examination Survey 2011–2016. Nutrients 2022, 14, 1552. https://doi.org/10.3390/nu14081552
Yang J, Chan K, Choi C, Yang A, Lo K. Identifying Effects of Urinary Metals on Type 2 Diabetes in U.S. Adults: Cross-Sectional Analysis of National Health and Nutrition Examination Survey 2011–2016. Nutrients. 2022; 14(8):1552. https://doi.org/10.3390/nu14081552
Chicago/Turabian StyleYang, Jingli, Kayue Chan, Cheukling Choi, Aimin Yang, and Kenneth Lo. 2022. "Identifying Effects of Urinary Metals on Type 2 Diabetes in U.S. Adults: Cross-Sectional Analysis of National Health and Nutrition Examination Survey 2011–2016" Nutrients 14, no. 8: 1552. https://doi.org/10.3390/nu14081552
APA StyleYang, J., Chan, K., Choi, C., Yang, A., & Lo, K. (2022). Identifying Effects of Urinary Metals on Type 2 Diabetes in U.S. Adults: Cross-Sectional Analysis of National Health and Nutrition Examination Survey 2011–2016. Nutrients, 14(8), 1552. https://doi.org/10.3390/nu14081552