
Creatine Supplementation for Muscle Growth: A Scoping Review of Randomized Clinical Trials from 2012 to 2021

 ,
,  ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Identifying the Research Questions
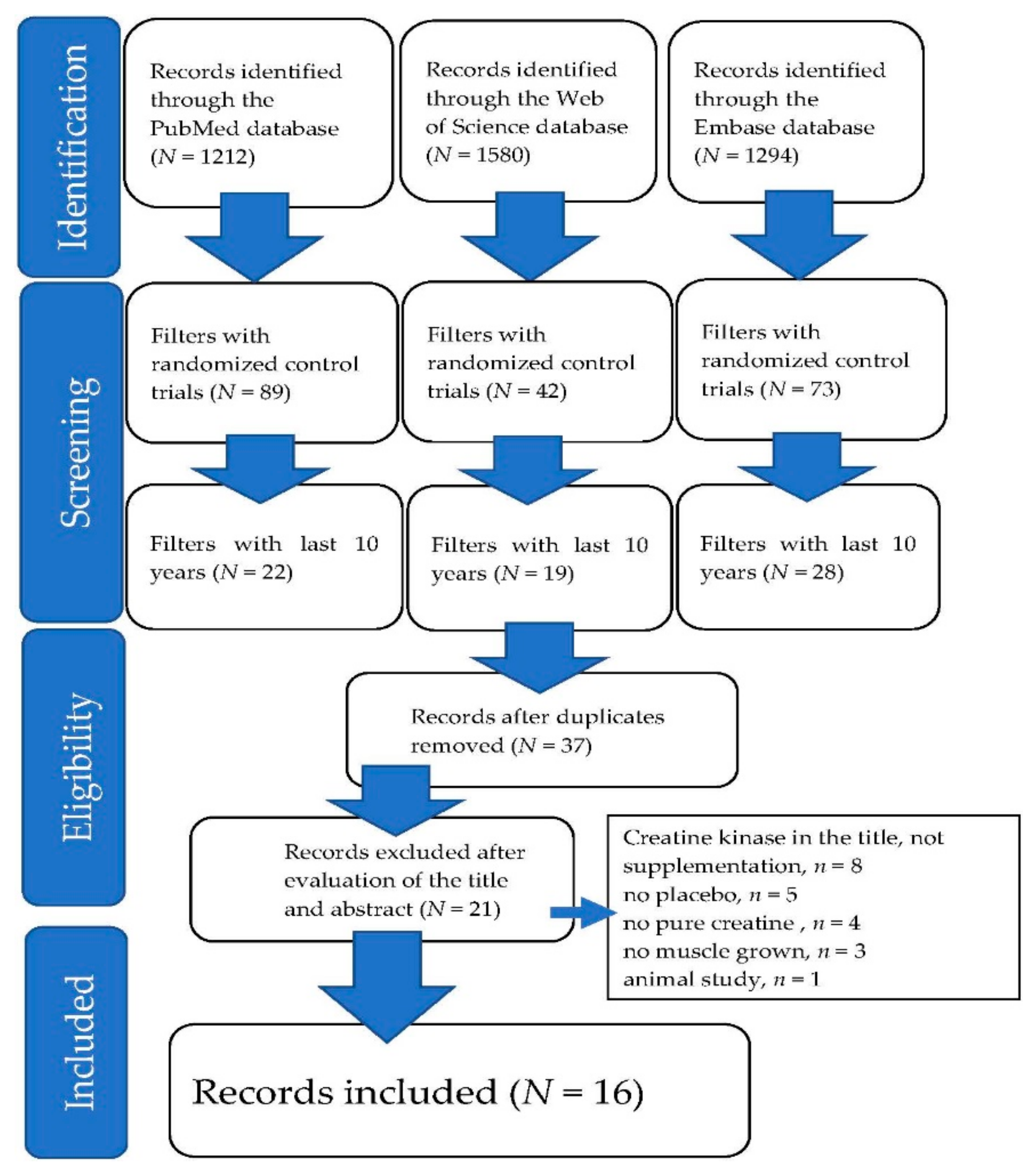
2.2. Identifying Relevant Studies
2.3. Selecting Studies
2.4. Charting the Data
Assessment of the Quality of the Methodologies of the Studies
2.5. Collating, Summarizing, and Reporting the Results
3. Results
3.1. Main Results
3.2. Included Studies
3.3. Study Outcomes
3.3.1. Healthy Untrained Young Subjects
3.3.2. Healthy Trained Young Subjects
3.3.3. Mimic Immobilization Subjects
3.3.4. Healthy Untrained Older Subjects
3.3.5. Subjects with Diseases
3.4. Three Major Themes That Affect Muscle Growth Due to Creatine Supplementation
3.4.1. Theme 1: Subjects of Creatine Supplementation
3.4.2. Theme 2: Training of Subjects
3.4.3. Theme 3: Future Direction and Recommendations for Research on Creatine Supplementation for Muscle Growth
4. Discussion
4.1. Dosage Strategies of Creatine Supplementation
4.2. Exercise and Its Relationship with Creatine Supplementation
4.2.1. Type of Exercise That Benefits from Creatine Supplementation
4.2.2. Without Exercise during the Creatine Supplementation Period
4.3. The Effect of Creatine Supplementation on Muscle Damage or Recovery
4.4. The Effect of Creatine Supplementation on Mitigating or Attenuating the Loss of Muscle Mass or Muscular Strength during Immobilization
4.5. The Effect of Creatine Supplementation on Older Populations
4.6. The Effect of Creatine Supplementation on Patients
4.7. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hartono, F.A.; Martin-Arrowsmith, P.W.; Peeters, W.M.; Churchward-Venne, T.A. The Effects of Dietary Protein Supplementation on Acute Changes in Muscle Protein Synthesis and Longer-Term Changes in Muscle Mass, Strength, and Aerobic Capacity in Response to Concurrent Resistance and Endurance Exercise in Healthy Adults: A Systematic Review. Sports Med. 2022. [Google Scholar] [CrossRef]
- Schoenfeld, B.J.; Grgic, J.; Van Every, D.W.; Plotkin, D.L. Loading Recommendations for Muscle Strength, Hypertrophy, and Local Endurance: A Re-Examination of the Repetition Continuum. Sports 2021, 9, 32. [Google Scholar] [CrossRef] [PubMed]
- Beaudart, C.; Rizzoli, R.; Bruyère, O.; Reginster, J.Y.; Biver, E. Sarcopenia: Burden and challenges for public health. Arch. Public Health 2014, 72, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welch, C.; Majid, Z.; Greig, C.; Gladman, J.; Masud, T.; Jackson, T. Interventions to ameliorate reductions in muscle quantity and function in hospitalised older adults: A systematic review towards acute sarcopenia treatment. Age Ageing 2021, 50, 394–404. [Google Scholar] [CrossRef] [PubMed]
- Rossato, L.T.; Schoenfeld, B.J.; de Oliveira, E.P. Is there sufficient evidence to supplement omega-3 fatty acids to increase muscle mass and strength in young and older adults? Clin. Nutr. 2020, 39, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Bear, D.E.; Langan, A.; Dimidi, E.; Wandrag, L.; Harridge, S.D.R.; Hart, N.; Connolly, B.; Whelan, K. β-Hydroxy-β-methylbutyrate and its impact on skeletal muscle mass and physical function in clinical practice: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2019, 109, 1119–1132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joy, J.M.; Vogel, R.M.; Shane Broughton, K.; Kudla, U.; Kerr, N.Y.; Davison, J.M.; Wildman, R.E.C.; DiMarco, N.M. Daytime and nighttime casein supplements similarly increase muscle size and strength in response to resistance training earlier in the day: A preliminary investigation. J. Int. Soc. Sports Nutr. 2018, 15, 24. [Google Scholar] [CrossRef] [Green Version]
- Nabuco, H.C.G.; Tomeleri, C.M.; Sugihara Junior, P.; Fernandes, R.R.; Cavalcante, E.F.; Antunes, M.; Ribeiro, A.S.; Teixeira, D.C.; Silva, A.M.; Sardinha, L.B.; et al. Effects of Whey Protein Supplementation Pre- or Post-Resistance Training on Muscle Mass, Muscular Strength, and Functional Capacity in Pre-Conditioned Older Women: A Randomized Clinical Trial. Nutrients 2018, 10, 563. [Google Scholar] [CrossRef] [Green Version]
- Brosnan, J.T.; Brosnan, M.E. Creatine: Endogenous metabolite, dietary, and therapeutic supplement. Annu Rev. Nutr. 2007, 27, 241–261. [Google Scholar] [CrossRef] [Green Version]
- Wyss, M.; Kaddurah-Daouk, R. Creatine and creatinine metabolism. Physiol. Rev. 2000, 80, 1107–1213. [Google Scholar] [CrossRef]
- Van Loon, L.J.; Oosterlaar, A.M.; Hartgens, F.; Hesselink, M.K.; Snow, R.J.; Wagenmakers, A.J. Effects of creatine loading and prolonged creatine supplementation on body composition, fuel selection, sprint and endurance performance in humans. Clin. Sci. 2003, 104, 153–162. [Google Scholar] [CrossRef]
- Greenhaff, P.L.; Bodin, K.; Soderlund, K.; Hultman, E. Effect of oral creatine supplementation on skeletal muscle phosphocreatine resynthesis. Am. J. Physiol. 1994, 266, E725–E730. [Google Scholar] [CrossRef]
- Hultman, E.; Söderlund, K.; Timmons, J.A.; Cederblad, G.; Greenhaff, P.L. Muscle creatine loading in men. J. Appl. Physiol. 1996, 81, 232–237. [Google Scholar] [CrossRef]
- Kreider, R.B.; Kalman, D.S.; Antonio, J.; Ziegenfuss, T.N.; Wildman, R.; Collins, R.; Candow, D.G.; Kleiner, S.M.; Almada, A.L.; Lopez, H.L. International Society of Sports Nutrition position stand: Safety and efficacy of creatine supplementation in exercise, sport, and medicine. J. Int. Soc. Sports Nutr. 2017, 14, 18. [Google Scholar] [CrossRef]
- Ribeiro, A.S.; Avelar, A.; Kassiano, W.; Nunes, J.P.; Schoenfeld, B.J.; Aguiar, A.F.; Trindade, M.C.C.; Silva, A.M.; Sardinha, L.B.; Cyrino, E.S. Creatine supplementation does not influence the ratio between intracellular water and skeletal muscle mass in resistance-trained men. Int. J. Sport Nutr. Exerc. Metab. 2020, 30, 405–411. [Google Scholar] [CrossRef]
- Lang, F.; Busch, G.L.; Ritter, M.; Völkl, H.; Waldegger, S.; Gulbins, E.; Häussinger, D. Functional significance of cell volume regulatory mechanisms. Physiol. Rev. 1998, 78, 247–306. [Google Scholar] [CrossRef]
- Antonio, J.; Candow, D.G.; Forbes, S.C.; Gualano, B.; Jagim, A.R.; Kreider, R.B.; Rawson, E.S.; Smith-Ryan, A.E.; VanDusseldorp, T.A.; Willoughby, D.S.; et al. Common questions and misconceptions about creatine supplementation: What does the scientific evidence really show? J. Int. Soc. Sports Nutr. 2021, 18, 13. [Google Scholar] [CrossRef]
- Wickremasinghe, D.; Kuruvilla, S.; Mays, N.; Avan, B.I. Taking knowledge users’ knowledge needs into account in health: An evidence synthesis framework. Health Policy Plan. 2016, 31, 527–537. [Google Scholar] [CrossRef] [Green Version]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. J. Clin. Epidemiol. 2021, 134, 178–189. [Google Scholar] [CrossRef]
- Study Quality Assessment Tools. Available online: study-quality-assessment-tools (accessed on 21 January 2022).
- Field, A.; Naughton, R.J.; Haines, M.; Lui, S.; Corr, L.D.; Russell, M.; Page, R.M.; Harper, L.D. The demands of the extra-time period of soccer: A systematic review. J. Sport Health Sci. 2020, in press. [Google Scholar] [CrossRef]
- Del Favero, S.; Roschel, H.; Artioli, G.; Ugrinowitsch, C.; Tricoli, V.; Costa, A.; Barroso, R.; Negrelli, A.L.; Otaduy, M.C.; da Costa Leite, C.; et al. Creatine but not betaine supplementation increases muscle phosphorylcreatine content and strength performance. Amino Acids 2012, 42, 2299–2305. [Google Scholar] [CrossRef]
- Kaviani, M.; Abassi, A.; Chilibeck, P.D. Creatine monohydrate supplementation during eight weeks of progressive resistance training increases strength in as little as two weeks without reducing markers of muscle damage. J. Sports Med. Phys. Fit. 2019, 59, 608–612. [Google Scholar] [CrossRef]
- Claudino, J.G.; Mezencio, B.; Amaral, S.; Zanetti, V.; Benatti, F.; Roschel, H.; Gualano, B.; Amadio, A.C.; Serrao, J.C. Creatine monohydrate supplementation on lower-limb muscle power in Brazilian elite soccer players. J. Int. Soc. Sport Nutr. 2014, 11, 6. [Google Scholar] [CrossRef] [Green Version]
- Nunes, J.P.; Ribeiro, A.S.; Schoenfeld, B.J.; Tomeleri, C.M.; Avelar, A.; Trindade, M.C.; Nabuco, H.C.; Cavalcante, E.F.; Junior, P.S.; Fernandes, R.R.; et al. Creatine supplementation elicits greater muscle hypertrophy in upper than lower limbs and trunk in resistance-trained men. Nutr. Health 2017, 23, 223–229. [Google Scholar] [CrossRef]
- Yáñez-Silva, A.; Buzzachera, C.F.; Piçarro, I.D.C.; Januario, R.S.B.; Ferreira, L.H.B.; McAnulty, S.R.; Utter, A.C.; Souza-Junior, T.P. Effect of low dose, short-term creatine supplementation on muscle power output in elite youth soccer players. J. Int. Soc. Sports Nutr. 2017, 14, 5. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.C.; Lin, S.C.; Hsu, S.C.; Yang, M.T.; Chan, K.H. Effects of Creatine Supplementation on Muscle Strength and Optimal Individual Post-Activation Potentiation Time of the Upper Body in Canoeists. Nutrients 2017, 9, 1169. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.C.; Fang, C.C.; Lee, Y.H.; Yang, M.T.; Chan, K.H. Effects of 4-Week Creatine Supplementation Combined with Complex Training on Muscle Damage and Sport Performance. Nutrients 2018, 10, 1640. [Google Scholar] [CrossRef] [Green Version]
- Fransen, J.C.; Zuhl, M.; Kerksick, C.M.; Cole, N.; Altobelli, S.; Kuethe, D.O.; Schneider, S. Impact of creatine on muscle performance and phosphagen stores after immobilization. Eur. J. Appl. Physiol. 2015, 115, 1877–1886. [Google Scholar] [CrossRef]
- Backx, E.M.P.; Hangelbroek, R.; Snijders, T.; Verscheijden, M.L.; Verdijk, L.B.; de Groot, L.; van Loon, L.J.C. Creatine Loading Does Not Preserve Muscle Mass or Strength During Leg Immobilization in Healthy, Young Males: A Randomized Controlled Trial. Sports Med. 2017, 47, 1661–1671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, T.P.; Candow, D.G.; Farthing, J.P. Effect of Preexercise Creatine Ingestion on Muscle Performance in Healthy Aging Males. J. Strength Cond. Res. 2016, 30, 1763–1766. [Google Scholar] [CrossRef] [PubMed]
- Chami, J.; Candow, D.G. Effect of Creatine Supplementation Dosing Strategies on Aging Muscle Performance. J. Nutr. Health Aging 2019, 23, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Candow, D.G.; Chilibeck, P.D.; Gordon, J.; Vogt, E.; Landeryou, T.; Kaviani, M.; Paus-Jensen, L. Effect of 12 months of creatine supplementation and whole-body resistance training on measures of bone, muscle and strength in older males. Nutr. Health 2021, 27, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Candow, D.G.; Chilibeck, P.D.; Gordon, J.J.; Kontulainen, S. Efficacy of Creatine Supplementation and Resistance Training on Area and Density of Bone and Muscle in Older Adults. Med. Sci. Sports Exerc. 2021, 53, 2388–2395. [Google Scholar] [CrossRef] [PubMed]
- Domingues, W.J.R.; Ritti-Dias, R.M.; Cucato, G.G.; Wolosker, N.; Zerati, A.E.; Puech-Leão, P.; Coelho, D.B.; Nunhes, P.M.; Moliterno, A.A.; Avelar, A. Effect of Creatine Supplementation on Functional Capacity and Muscle Oxygen Saturation in Patients with Symptomatic Peripheral Arterial Disease: A Pilot Study of a Randomized, Double-Blind Placebo-Controlled Clinical Trial. Nutrients 2021, 13, 149. [Google Scholar] [CrossRef] [PubMed]
- Dover, S.; Stephens, S.; Schneiderman, J.E.; Pullenayegum, E.; Wells, G.D.; Levy, D.M.; Marcuz, J.A.; Whitney, K.; Schulze, A.; Tein, I.; et al. The Effect of Creatine Supplementation on Muscle Function in Childhood Myositis: A Randomized, Double-blind, Placebo-controlled Feasibility Study. J. Rheumatol. 2021, 48, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Jiaming, Y.; Rahimi, M.H. Creatine supplementation effect on recovery following exercise-induced muscle damage: A systematic review and meta-analysis of randomized controlled trials. J. Food Biochem. 2021, 45, e13916. [Google Scholar] [CrossRef] [PubMed]
- Northeast, B.; Clifford, T. The Effect of Creatine Supplementation on Markers of Exercise-Induced Muscle Damage: A Systematic Review and Meta-Analysis of Human Intervention Trials. Int. J. Sport Nutr. Exerc. Metab. 2021, 31, 276–291. [Google Scholar] [CrossRef]
- Harmon, K.K.; Stout, J.R.; Fukuda, D.H.; Pabian, P.S.; Rawson, E.S.; Stock, M.S. The Application of Creatine Supplementation in Medical Rehabilitation. Nutrients 2021, 13, 1825. [Google Scholar] [CrossRef]
- Candow, D.G.; Chilibeck, P.D.; Forbes, S.C. Creatine supplementation and aging musculoskeletal health. Endocrine 2014, 45, 354–361. [Google Scholar] [CrossRef]
- Candow, D.G.; Forbes, S.C.; Chilibeck, P.D.; Cornish, S.M.; Antonio, J.; Kreider, R.B. Effectiveness of Creatine Supplementation on Aging Muscle and Bone: Focus on Falls Prevention and Inflammation. J. Clin. Med. 2019, 8, 488. [Google Scholar] [CrossRef] [Green Version]
- De Guingand, D.L.; Palmer, K.R.; Snow, R.J.; Davies-Tuck, M.L.; Ellery, S.J. Risk of Adverse Outcomes in Females Taking Oral Creatine Monohydrate: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 1780. [Google Scholar] [CrossRef]
- Stares, A.; Bains, M. The Additive Effects of Creatine Supplementation and Exercise Training in an Aging Population: A Systematic Review of Randomized Controlled Trials. J. Geriatr. Phys. Ther. 2020, 43, 99–112. [Google Scholar] [CrossRef]
- Pham, M.T.; Rajić, A.; Greig, J.D.; Sargeant, J.M.; Papadopoulos, A.; McEwen, S.A. A scoping review of scoping reviews: Advancing the approach and enhancing the consistency. Res. Synth. Methods 2014, 5, 371–385. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Authors (Year) | Design | QACIS Score | Participants | Creatine Dose (g/day) | Duration (Days) | Training Exercise | Evaluation Exercise | Outcome Measures (Muscle-Related) | Main Findings (Muscle-Related) |
|---|---|---|---|---|---|---|---|---|---|
| del Favero et al. [23] | RP DB | 85.71 | 34 healthy untrained males 18–30 years old | 2 × 10 g | 10 | N/A | Squat exercise Bench press | Muscle power output by a linear encoder 1RM | Muscle power output: Squat exercise: CR > PL (p = 0.003) Bench-press: CR > PL (p = 0.039) 1RM in CR: Post > pre Squat exercise: p = 0.027 Bench-press: p < 0.0001 No change in PL |
| Kaviani et al. [24] | RP DB | 85.71 | 18 healthy untrained males 23 ± 3 years old | 0.07 g/kg | 56 | Bench press Leg press Biceps curl Tricep extension Shoulder press Lat pull-down | 1RM of left exercise | Check 1RM every two weeks for eight weeks CK | 1RM CR > PL within two weeks after bench, leg, and shoulder presses (p < 0.05) By six weeks, 1RM CR > PL in above three items and tricep extension (p < 0.05) Eight weeks, then same as six weeks, no significant difference in biceps curls and lat pull-downs CK, CR > PL (p ≤ 0.05) |
| Authors (Year) | Design | QACIS Score | Participants | Creatine Dose (g/day) | Duration (Days) | Training Exercise | Evaluation Exercise | Outcome Measures (Muscle-Related) | Main Findings (Muscle-Related) |
|---|---|---|---|---|---|---|---|---|---|
| Claudinoet al. [25] | RP DB | 71.43 | 23 healthy male elite soccer player 18.3 ± 0.9 years old | 4 × 5 g × 7 days 5 g × 42 days | 49 | Whole-body resistance training Jumping Specific training for soccer | Countermovement jump (CMJ) test | Countermovement jump test | CMJ test: CR > PL (p = 0.23) Reduction in jump performance, PL > CR (p = 0.05) |
| Nunes et al. [26] | RP DB | 85.71 | 43 healthy trained males 22.7 ± 3 years old | 0.3 g/kg × 7 days 0.03 g/kg × 49 days | 56 | Whole-body resistance training | N/A | DXA for lean soft tissue | ↑ Lean soft tissue (LST) in upper limbs, lower limbs, and trunk, CR > PL (p < 0.001) ULLST (7.1 + 2.9%) > LLLST (3.2 + 2.1%) and TLST (2.1 + 2.2%). |
| Yáñez-Silva et al. [27] | RP DB | 71.43 | 20 healthy trained male elite soccer players 17.0 ± 0.5 years old | 0.03 g/kg | 14 | Soccer training for skill development and anaerobic and aerobic performance development | Wingate anaerobic test |
Peak power output (PPO), mean power output (MPO), fatigue index (FI), and total work | ↑ PPO, MPO, and total work in CR vs. PL (p ≤ 0.05) |
| Wang et al. [28] | RP DB | 85.71 | 17 healthy trained male high school canoeists 16.6 years old | 4 × 5 g × 6 days | 6 | Bench row Complex training bouts Overhead medicine ball throw test | As left | 1RM of bench row Complex training bouts to determine the optimal individual timing of PAP Distance of overhead medicine ball throw test | ↑ Maximal strength, CR vs. PL (p ≤ 0.05) ↓ Optimal individual PAP time, CR vs. PL (p ≤ 0.05) No effect on explosive power |
| Wang et al. [29] | RP DB | 92.86 | 30 healthy trained males 20 ± 2 years old | 4 × 5 g × 6 days 2 g × 28 days | 34 | Complex training: Half-squat Vertical jump Squat jump | Body composition 1RM half-squat 30 m sprint and CMJ test | CMJ test Sprint test 1RMCK | 1RM, CR > PL (p ≤ 0.05) CK, CR < PL (p ≤ 0.05) CMJ test: No significant difference in CR or PL |
| Ribeiro et al. [15] | RP DB | 85.71 | 30 healthy trained male elite soccer players 21.8 ± 4.2 years old | 4 × 5 g × 5 days 3 g × 51 days | 56 | Whole-body resistance training | N/A | Bioelectrical impedance device for ICW and ECW DXA for skeleton muscle mass | ↑ Skeletal muscle mass, total body water, intracellular water in CR vs. PL (p ≤ 0.05) |
| Authors (Year) | Design | QACIS Score | Participants | Creatine Dose (g/day) | Duration (Days) | Training Exercise | Evaluation Exercise | Outcome Measures (Muscle-Related) | Main Findings (Muscle-Related) |
|---|---|---|---|---|---|---|---|---|---|
| Fransen et al. [30] | RP DB | 92.86 | 25 healthy untrained males/females 24 ± 4 years old Short arm casting for seven days | 20 g | 7 | N/A | Forearm wrist flexion ergometer | Ergometry incremental protocol to fatigue and two constant load (CL1 and CL2) exercise bouts Magnetic resonance spectroscopy (MRS) for PCr | No difference in any work and power data, after casting, CR vs. PL (p = 0.57) Work production in CL1 tended (p = 0.073) to attenuate in CR vs. PL, no difference in CL2 ↓ PCr after casting in PL (p = 0.003), no change in C R (p = 0.31) |
| Backx et al. [31] | RP DB | 92.86 | 27 healthy untrained males 23 ± 1 years old Long leg casting for seven days | 20 g × 5 days 5 g × 16 days | 21 | N/A | Knee extension | Muscle biopsy Computed tomography (CT) for cross-sectional area (CSA) 1RM | ↓ Quadricep muscle CSA after casting, no differences between groups (p = 0.76) ↓ Leg muscle strength, after casting, no differences between groups (p = 0.20) When non-responders to creatine loading were excluded (n = 6), responders (n = 8) still showed no signs of preservation of muscle mass or strength during casting |
| Authors et al.(Year) | Design | QACIS Score | Participants | Creatine Dose (g/day) | Duration (Days) | Training Exercise | Evaluation Exercise | Outcome Measures (Muscle-Related) | Main Findings (Muscle-Related) |
|---|---|---|---|---|---|---|---|---|---|
| Baker et al. [32] | RC DB | 85.71 | Nine healthy untrained males 54.8 ± 4.3 years old | 20 g | 1 | N/A | Leg press Chest press Cycle ergometer | 1RM Muscle endurance test (three sets at 70% baseline 1RM to muscle fatigue; 1 min rest between sets) | ↓ In the number of repetitions performed across sets, with no differences between CR and PL (p > 0.05) CR had no effect on the rating of perceived exertion (leg press: CR, 9.1 ± 0.7; PL, 8.9 ± 0.6; chest press: CR, 9.0 ± 1.0; PL, 8.8 ± 0.8) (p > 0.05) |
| Chami et al. [33] | RP DB | 92.86 | 33 healthy untrained males 58.5 ± 4.7 years old | 0.3 g/kg 0.1 g/kg | 10 | N/A | Leg press Chest press Handgrip Walk backward as fast as possible on an elevated board | 1RM Muscle endurance (maximal number of repetitions performed for one set at 80% and 70% 1RM for the leg and chest presses, respectively) Physical performance (balance and falls) | ↑ Muscle strength and endurance in all groups, but no difference in groups CR-H, CR-M, and PL (p > 0.05) |
| Candow et al. [34] | RP DB | 92.86 | 35 healthy untrained males 56.9 years old | 2 × 0.05 g/kg | 365 | Resistance training three times per week for one year | Chest press Hack squat | Maximal strength DXA | After 12 months of training, both groups experienced similar changes in muscle thickness and muscle strength, with no difference between CR and PL |
| Candow et al. [35] | RP DB | 78.57 | 70 healthy untrained males/females 58 ± 6 years old | 0.1 g/kg | 365 | Resistance training three times per week for one year | N/A | pQCT | ↑ Lower leg muscle density in CR (Δ + 0.83 ± 1.15 mg·cm−3; p = 0.016) compared to PL (Δ − 0.16 ± 1.56 mg·cm−3),with no changes in the forearm muscle |
| Authors (Year) | Design | QACIS Score | Participants | Creatine Dose (g/day) | Duration (Days) | Training Exercise | Evaluation Exercise | Outcome Measures (Muscle-Related) | Main Findings (Muscle-Related) |
|---|---|---|---|---|---|---|---|---|---|
| Domingues et al. [36] | RP DB | 85.71 | 29 symptomatic PAD males/females 64 ± 8 years old | 4 × 5 g × 7 days 5 g × 49 days | 56 | N/A | Six min walk test | Functional capacity (total walking distance) was assessed by the six min walk test Calf muscle StO2 was assessed through near-infrared spectroscopy | No significant differences were found for function capacity (PL: Pre 389 ± 123 m vs. post-loading 413 ± 131 m vs. post-maintenance 382 ± 99 m; CR: Pre 373 ± 149 m vs. post-loading 390 ± 115 m vs. post-maintenance 369 ± 115 m, p = 0.170) and the calf muscle StO2 parameters (p > 0.05) |
| Dover et al. [37] | RC DB | 85.71 | 13 juvenile dermatomyositis males/females 13 (7–14) years old | < 40 kg → 0.15 g/kg > 40 kg → 4.69 g/m2 | 28–180 | N/A | Wingate anaerobic test Cycle ergometer submaximal test to measure aerobic capacity Maximal jump test Handgrip strength test | Muscle function Aerobic capacity Muscle strength Fatigue Physical activity Quality of life assessed by questionnaires | No significant changes in muscle function, strength, aerobic capacity, disease activity, fatigue, physical activity or quality of life in CR vs. PL No significant adverse effects |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, S.-H.; Chen, K.-L.; Hsu, C.; Chen, H.-C.; Chen, J.-Y.; Yu, S.-Y.; Shiu, Y.-J. Creatine Supplementation for Muscle Growth: A Scoping Review of Randomized Clinical Trials from 2012 to 2021. Nutrients 2022, 14, 1255. https://doi.org/10.3390/nu14061255
Wu S-H, Chen K-L, Hsu C, Chen H-C, Chen J-Y, Yu S-Y, Shiu Y-J. Creatine Supplementation for Muscle Growth: A Scoping Review of Randomized Clinical Trials from 2012 to 2021. Nutrients. 2022; 14(6):1255. https://doi.org/10.3390/nu14061255
Chicago/Turabian StyleWu, Shih-Hao, Kuan-Lin Chen, Chin Hsu, Hang-Cheng Chen, Jian-Yu Chen, Sheng-Yan Yu, and Yi-Jie Shiu. 2022. "Creatine Supplementation for Muscle Growth: A Scoping Review of Randomized Clinical Trials from 2012 to 2021" Nutrients 14, no. 6: 1255. https://doi.org/10.3390/nu14061255
APA StyleWu, S.-H., Chen, K.-L., Hsu, C., Chen, H.-C., Chen, J.-Y., Yu, S.-Y., & Shiu, Y.-J. (2022). Creatine Supplementation for Muscle Growth: A Scoping Review of Randomized Clinical Trials from 2012 to 2021. Nutrients, 14(6), 1255. https://doi.org/10.3390/nu14061255