Development and Validation of a New Home Cooking Frequency Questionnaire: A Pilot Study

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
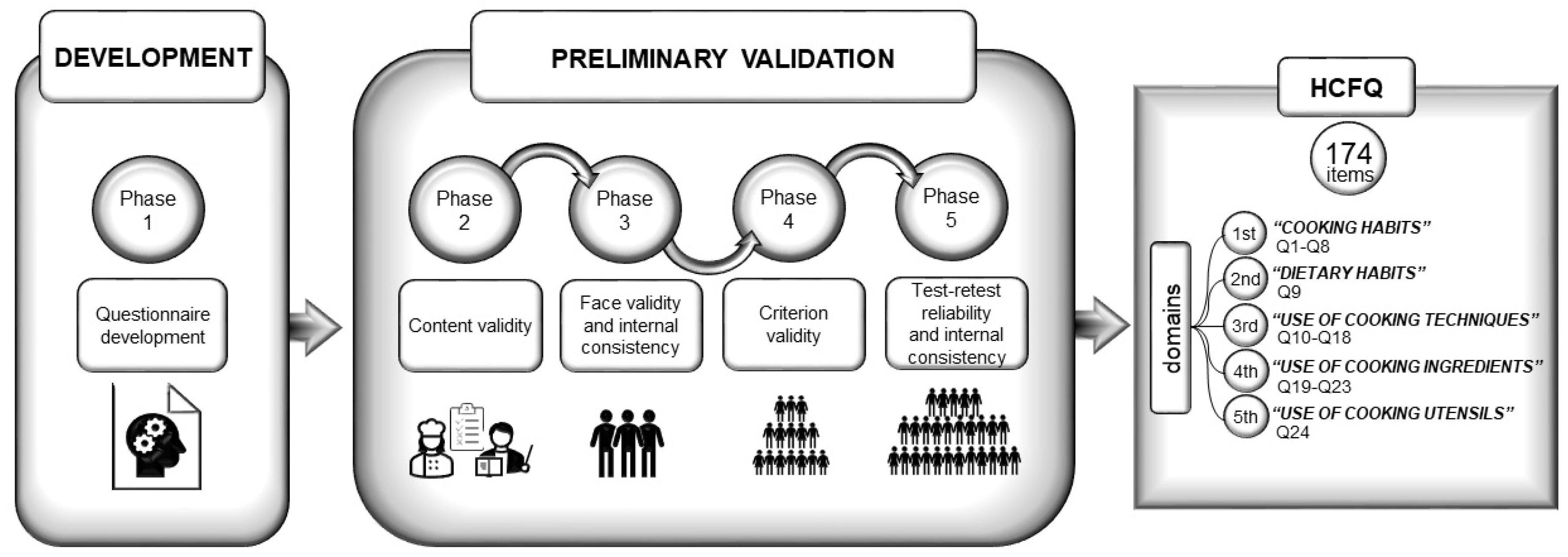
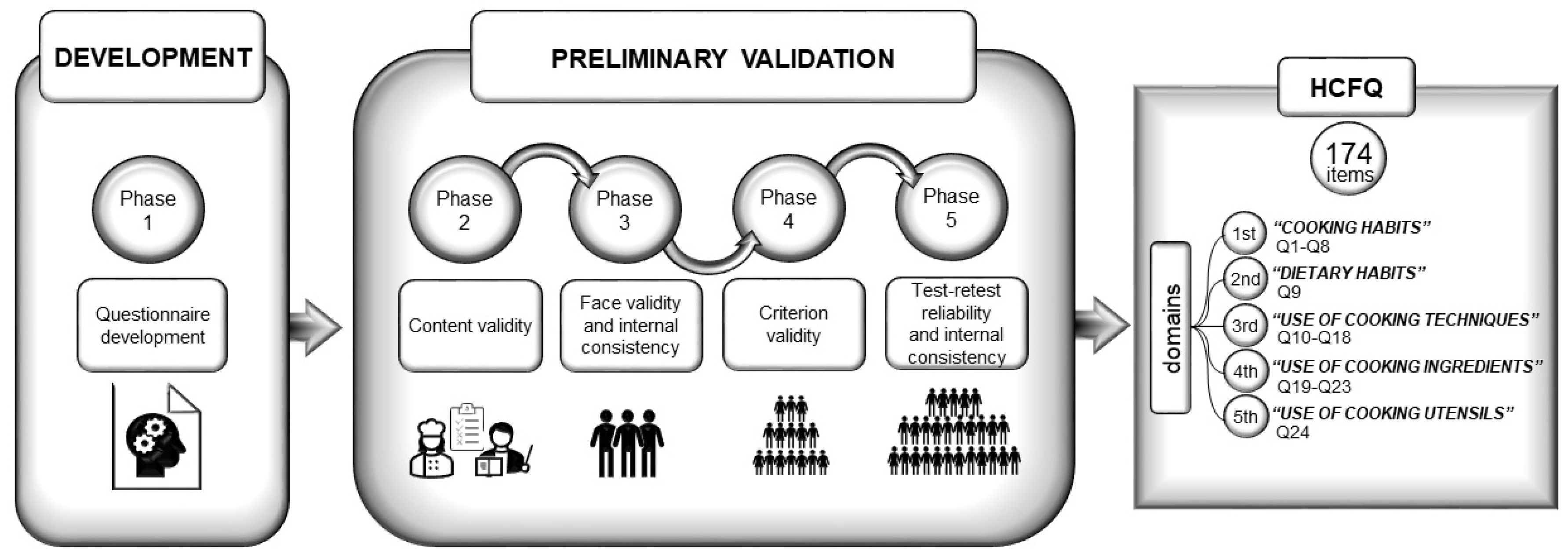
2.1. Phase 1: Questionnaire Development
2.2. Phase 2: Content Validity
2.3. Phase 3: Face Validity and Internal Consistency
2.4. Phase 4: Criterion Validity
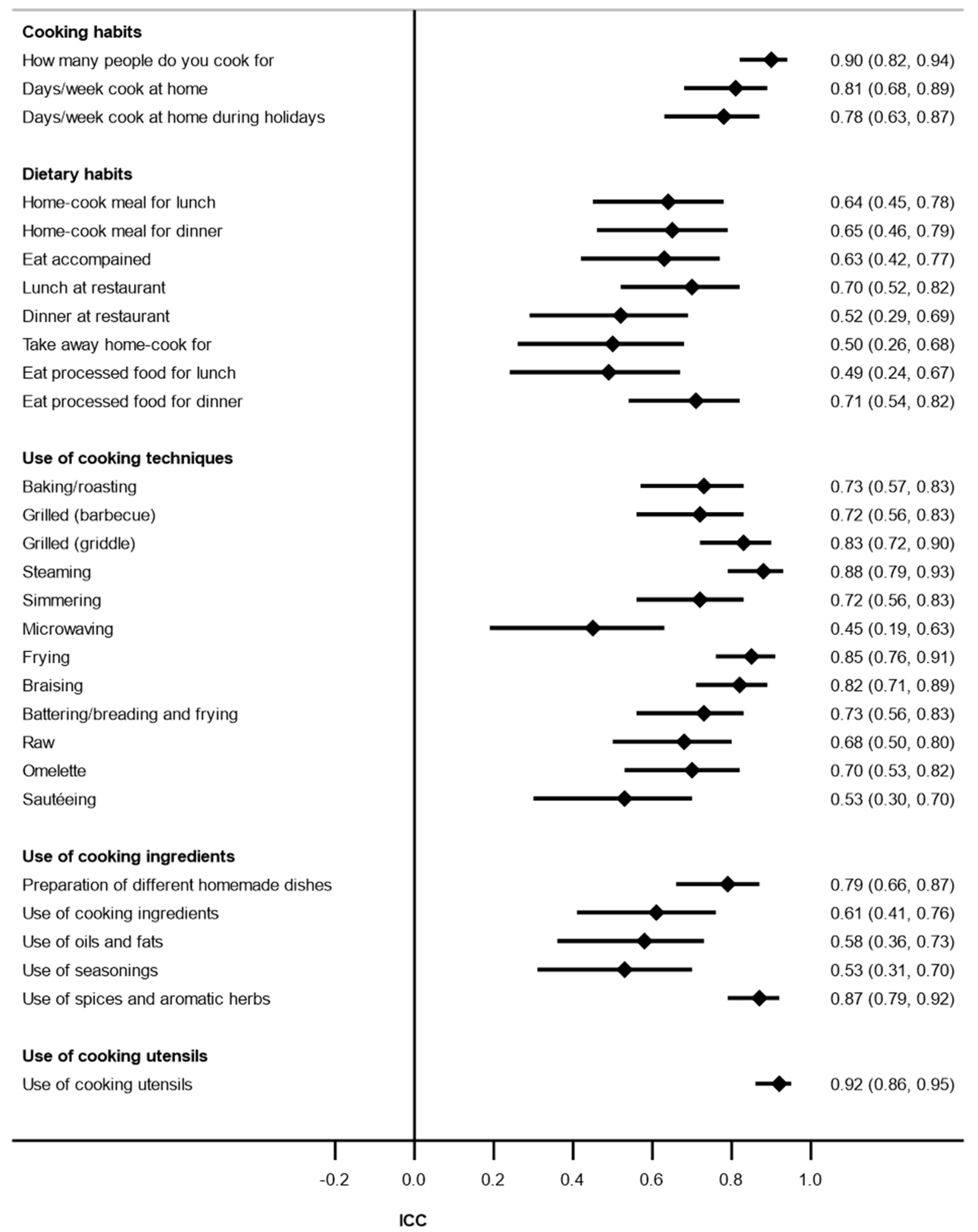
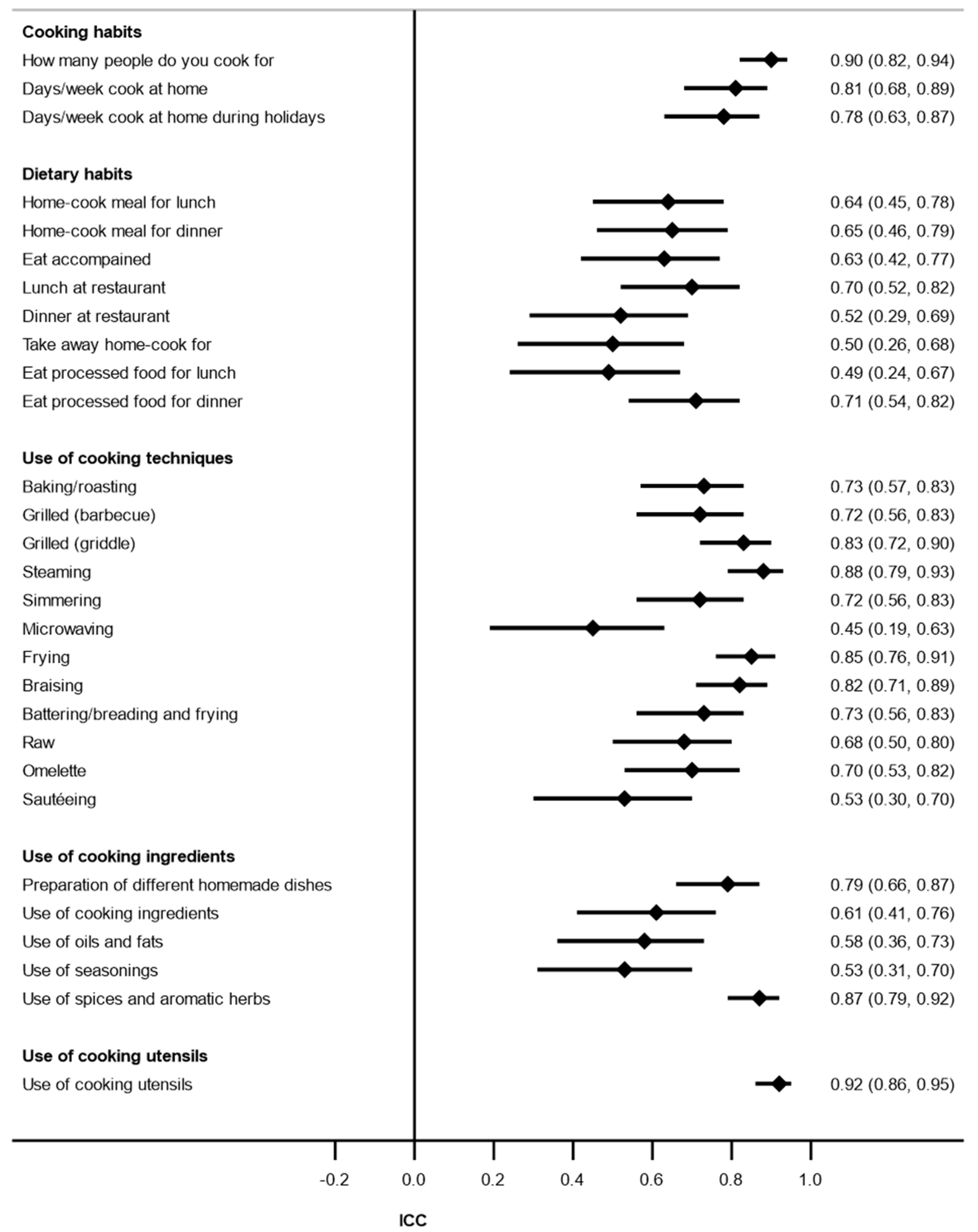
2.5. Phase 5: Test–Retest Reliability and Internal Consistency
3. Results
3.1. Phase 1: Questionnaire Development
3.2. Phase 2: Content Validity
3.3. Phase 3: Face Validity and Inter-Item Reliability
3.4. Phase 4: Criterion Validity
3.5. Phase 5: Test Stability and Internal Consistency
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mills, S.; White, M.; Brown, H.; Wrieden, W.; Kwasnicka, D.; Halligan, J.; Robalino, S.; Adams, J. Health and social determinants and outcomes of home cooking: A systematic review of observational studies. Appetite 2017, 111, 116–134. [Google Scholar] [CrossRef]
- Reicks, M.; Kocher, M.; Reeder, J. Impact of cooking and home food preparation interventions among adults: A systematic review (2011–2016). J. Nutr. Educ. Behav. 2018, 50, 148–172.e1. [Google Scholar] [CrossRef]
- Ricanati, E.H.; Golubi, M.; Yang, D.; Saager, L.; Mascha, E.J.; Roizen, M.F. Mitigating preventable chronic disease: Progress report of the Cleveland Clinic’s Lifestyle 180 program. Nutr. Metab. 2011, 8, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Eisenberg, D.M.; Righter, A.C.; Matthews, B.; Zhang, W.; Willett, W.C.; Massa, J. Feasibility pilot study of a teaching kitchen and self-care curriculum in a workplace setting. Am. J. Lifestyle Med. 2019, 13, 319–330. [Google Scholar] [CrossRef]
- Dasgupta, K.; Hajna, S.; Joseph, L.; Da Costa, D.; Christopoulos, S.; Gougeon, R. Effects of meal preparation training on body weight, glycemia, and blood pressure: Results of a phase 2 trial in type 2 diabetes. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Polak, R.; Tirosh, A.; Livingston, B.; Pober, D.; Eubanks, J.E.; Silver, J.K.; Minezaki, K.; Loten, R.; Phillips, E.M. Preventing Type 2 diabetes with home cooking: Current evidence and future potential. Curr. Diabetes Rep. 2018, 18, 99–105. [Google Scholar] [CrossRef]
- Zong, G.; Eisenberg, D.M.; Hu, F.B.; Sun, Q. Consumption of meals prepared at home and risk of type 2 diabetes: An analysis of two prospective cohort studies. PLoS Med. 2016, 13, e1002052. [Google Scholar] [CrossRef] [Green Version]
- Cahill, L.E.; Pan, A.; Chiuve, S.E.; Sun, Q.; Willett, W.C.; Hu, F.B.; Rimm, E.B. Fried-food consumption and risk of type 2 diabetes and coronary artery disease: A prospective study in 2 cohorts of US women and men. Am. J. Clin. Nutr. 2014, 100, 667–675. [Google Scholar] [CrossRef]
- Sayon-Orea, C.; Bes-Rastrollo, M.; Gea, A.; Zazpe, I.; Basterra-Gortari, F.J.; Martinez-Gonzalez, M.A. Reported fried food consumption and the incidence of hypertension in a Mediterranean cohort: The SUN (Seguimiento Universidad de Navarra) project. Br. J. Nutr. 2014, 112, 984–991. [Google Scholar] [CrossRef] [Green Version]
- Barzegar, F.; Kamankesh, M.; Mohammadi, A. Heterocyclic aromatic amines in cooked food: A review on formation, health risk-toxicology and their analytical techniques. Food Chem. 2019, 280, 240–254. [Google Scholar] [CrossRef]
- Sampaio, G.R.; Guizellini, G.M.; da Silva, S.A.; de Almeida, A.P.; Pinaffi-Langley, A.C.C.; Rogero, M.M.; de Camargo, A.C.; Torres, E.A.F.S. Polycyclic aromatic hydrocarbons in foods: Biological effects, legislation, occurrence, analytical methods, and strategies to reduce their formation. Int. J. Mol. Sci. 2021, 22, 6010. [Google Scholar] [CrossRef]
- Tricker, A.R.; Preussmann, R. Carcinogenic N-nitrosamines in the diet: Occurrence, formation, mechanisms and carcinogenic potential. Mutat. Res. Toxicol. 1991, 259, 277–289. [Google Scholar] [CrossRef]
- Davis, K.E.; Prasad, C.; Vijayagopal, P.; Juma, S.; Imrhan, V. Advanced glycation end products, inflammation, and chronic metabolic diseases: Links in a chain? Crit. Rev. Food Sci. Nutr. 2016, 56, 989–998. [Google Scholar] [CrossRef]
- Clarke, R.E.; Dordevic, A.L.; Tan, S.M.; Ryan, L.; Coughlan, M.T. Dietary advanced glycation end products and risk factors for chronic disease: A systematic review of randomised controlled trials. Nutrients 2016, 8, 125. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Wang, P.; Xu, X.; Zhou, G. Influence of various cooking methods on the concentrations of volatile N-nitrosamines and biogenic amines in dry-cured sausages. J. Food Sci. 2012, 77, 560–565. [Google Scholar] [CrossRef]
- Uribarri, J.; Woodruff, S.; Goodman, S.; Cai, W.; Chen, X.U.E.; Pyzik, R.; Yong, A.; Striker, G.E. Advanced glycation end products in foods and a practical guide to their reduction in the diet. J. Am. Diet. Assoc. 2010, 110, 911–916. [Google Scholar] [CrossRef] [Green Version]
- De La Cruz-Ares, S.; Cardelo, M.P.; Gutiérrez-Mariscal, F.M.; Torres-Peña, J.D.; García-Rios, A.; Katsiki, N.; Malagón, M.M.; López-Miranda, J.; Pérez-Martínez, P.; Yubero-Serrano, E.M. Endothelial dysfunction and advanced glycation end products in patients with newly diagnosed versus established diabetes: From the CORDIOPREV study. Nutrients 2020, 12, 238. [Google Scholar] [CrossRef] [Green Version]
- Condrasky, M.D.; Williams, J.E.; Catalano, P.M.; Griffin, S.F. Development of psychosocial scales for evaluating the impact of a culinary nutrition education program on cooking and healthful eating. J. Nutr. Educ. Behav. 2011, 43, 511–516. [Google Scholar] [CrossRef]
- Barton, K.L.; Wrieden, W.L.; Anderson, A.S. Validity and reliability of a short questionnaire for assessing the impact of cooking skills interventions. J. Hum. Nutr. Diet. 2011, 24, 588–595. [Google Scholar] [CrossRef]
- Vrhovnik, L. A pilot study for the development of a food skills survey tool. Master’s Thesis, Queen’s University, Kingston, ON, Canada, 2012. [Google Scholar]
- Lahne, J.; Wolfson, J.A.; Trubek, A. Development of the Cooking and Food Provisioning Action Scale (CAFPAS): A new measurement tool for individual cooking practice. Food Qual. Prefer. 2017, 62, 96–105. [Google Scholar] [CrossRef]
- Lavelle, F.; McGowan, L.; Hollywood, L.; Surgenor, D.; McCloat, A.; Mooney, E.; Caraher, M.; Raats, M.; Dean, M. The development and validation of measures to assess cooking skills and food skills. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, L.G.; Kichler, E.J.; Seabrook, J.A.; Matthews, J.I.; Dworatzek, P.D.N. Validity and reliability of a food skills questionnaire. J. Nutr. Educ. Behav. 2019, 51, 857–864. [Google Scholar] [CrossRef]
- Mathews, D.R.; Kunicki, Z.J.; Colby, S.E.; Franzen-Castle, L.; Kattelmann, K.K.; Olfert, M.D.; White, A.A. Development and testing of program evaluation instruments for the iCook 4-H curriculum. J. Nutr. Educ. Behav. 2019, 51, S21–S29. [Google Scholar] [CrossRef] [Green Version]
- Wolfson, J.A.; Ishikawa, Y.; Hosokawa, C.; Janisch, K.; Massa, J.; Eisenberg, D.M. Gender differences in global estimates of cooking frequency prior to COVID-19. Appetite 2021, 161, 105117. [Google Scholar] [CrossRef]
- Raber, M.; Ranjit, N.; Strong, L.L.; Basen-Engquist, K. Home cooking quality assessment tool validation using community science and crowdsourcing approaches. J. Nutr. Educ. Behav. 2022; in press. [Google Scholar] [CrossRef]
- Trakman, G.L.; Forsyth, A.; Hoye, R.; Belski, R. Developing and validating a nutrition knowledge questionnaire: Key methods and considerations. Public Health Nutr. 2017, 20, 2670–2679. [Google Scholar] [CrossRef] [Green Version]
- Gleason, P.M.; Harris, J.; Sheean, P.M.; Boushey, C.J.; Bruemmer, B. Publishing nutrition research: Validity, reliability, and diagnostic test assessment in nutrition-related research. J. Am. Diet. Assoc. 2010, 110, 409–419. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T.; Owen, S.V. Focus on research methods: Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Res. Nurs. Health 2007, 30, 459–467. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T. The content validity index: Are you sure you know what’s being reported? Critique and recommendations. Res. Nurs. Health 2006, 29, 489–497. [Google Scholar] [CrossRef] [Green Version]
- Davis, L.L. Instrument review: Getting the most from a panel of experts. Appl. Nurs. Res. 1992, 5, 194–197. [Google Scholar] [CrossRef]
- Waltz, C.F.; Strickland, O.L.; Lenz, E.R. Measurement in Nursing and Health Research, 3rd ed.; Springer Publising Co.: New York, UK, USA, 2005. [Google Scholar]
- Wynd, C.A.; Schmidt, B.; Schaefer, M.A. Two quantitative approaches for estimating content validity. West J. Nurs. Res. 2003, 25, 508–518. [Google Scholar] [CrossRef]
- Cicchetti, D.V.; Sparrow, S.A. Developing criteria for establishing interrater reliability of specific items: Applications to assessment of adaptive behavior. Am. J. Ment. Defic. 1981, 86, 127–137. [Google Scholar]
- Kline, P. A Handbook of Test Construction (Psychology Revivals): Introduction to Psychometric Design; Taylor & Francis: Abingdon, UK, 2015. [Google Scholar]
- Schönberg, S.; Asher, R.; Stewart, S.; Fenwick, M.J.; Ashton, L.; Bucher, T.; Van der Horst, K.; Oldmeadow, C.; Collins, C.E.; Shrewsbury, V.A. Development of the Home Cooking EnviRonment and Equipment Inventory observation form (Home-cookeriTM): An assessment of content validity, face validity, and inter-rater agreement. Nutrients 2020, 12, 1853. [Google Scholar] [CrossRef]
- Rattray, J.; Jones, M.C. Essential elements of questionnaire design and development. J. Clin. Nurs. 2007, 16, 234–243. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Cronbach’s alpha. Br. Med. J. 1997, 314, 572. [Google Scholar] [CrossRef] [Green Version]
- Carvajal, A.; Centeno, C.; Watson, R.; Martínez, M.; Rubiales, Á.S. How is an instrument for measuring health to be validated? An. Sist. Sanit. Navar. 2011, 34, 63–72. [Google Scholar]
- Streiner, D.L.; Norman, G.R.; Cairney, J. Health Measurement Scales: A Practical Guide to Their Development and Use, 5th ed.; Oxford University Press (OUP): Oxford, UK, 2015. [Google Scholar]
- Martínez-González, M.A.; Sánchez-Villegas, A.; Toledo, E.; Faulin, J. Análisis de concordancia, validez y pronóstico. In Bioestadística Amigable; Elsevier: Barcelona, Spain, 2020. [Google Scholar]
- Terwee, C.B.; Bot, S.D.M.; de Boer, M.R.; van der Windt, D.A.W.M.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C.W. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Monsivais, P.; Aggarwal, A.; Drewnowski, A. Time spent on home food preparation and indicators of healthy eating. Am. J. Prev. Med. 2014, 47, 796–802. [Google Scholar] [CrossRef] [Green Version]
- Raber, M.; Wolfson, J. Perspective the challenging task of measuring home cooking behavior. J. Nutr. Educ. Behav. 2021, 53, 267–269. [Google Scholar] [CrossRef]
- Gibson, R.S. Measuring food consumption of individuals. In The Principles of Nutritional Assessment; Gibson, R., Ed.; Oxford University Press: Oxford, UK, 2005; pp. 41–64. [Google Scholar]
- van Dongen, K.C.W.; Linkens, A.M.A.; Wetzels, S.M.W.; Wouters, K.; Vanmierlo, T.; van de Waarenburg, M.P.H.; Scheijen, J.L.J.M.; de Vos, W.M.; Belzer, C.; Schalkwijk, C.G. Dietary advanced glycation endproducts (AGEs) increase their concentration in plasma and tissues, result in inflammation and modulate gut microbial composition in mice; evidence for reversibility. Food Res. Int. 2021, 147, 110547. [Google Scholar] [CrossRef]
- Uribarri, J.; Cai, W.; Woodward, M.; Tripp, E.; Goldberg, L.; Pyzik, R.; Yee, K.; Tansman, L.; Chen, X.; Mani, V.; et al. Elevated serum advanced glycation endproducts in obese indicate risk for the metabolic syndrome: A link between healthy and unhealthy obesity? J. Clin. Endocrinol. Metab. 2015, 100, 1957–1966. [Google Scholar] [CrossRef]
- Scheijen, J.L.J.M.; Hanssen, N.M.J.; van Greevenbroek, M.M.; Van der Kallen, C.J.; Feskens, E.J.M.; Stehouwer, C.D.A.; Schalkwijk, C.G. Dietary intake of advanced glycation endproducts is associated with higher levels of advanced glycation endproducts in plasma and urine: The CODAM study. Clin. Nutr. 2018, 37, 919–925. [Google Scholar] [CrossRef]
- Luevano-Contreras, C.; Durkin, T.; Pauls, M.; Chapman-Novakofski, K. Development, relative validity, and reliability of a food frequency questionnaire for a case-control study on dietary advanced glycation end products and diabetes complications. Int. J. Food Sci. Nutr. 2013, 64, 1030–1035. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Domains of the HCFQ | S-CVI-Ave | S-CVI-UA | ||
|---|---|---|---|---|
| Relevance | Clarity | Relevance | Clarity | |
| Cooking habits | 0.98 | 0.96 | 0.86 | 0.79 |
| Dietary habits | 0.98 | 0.93 | 0.87 | 0.60 |
| Use of cooking techniques | 0.99 | 0.96 | 0.93 | 0.78 |
| Use of cooking ingredients | 0.99 | 1.00 | 0.97 | 0.99 |
| Use of cooking utensils | 0.96 | 0.99 | 0.75 | 0.93 |
| Whole questionnaire | 0.99 | 0.97 | 0.93 | 0.85 |
| Domains of the HCFQ | I-CVI a Relevance | κ* for Relevance b | I-CVI a Clarity | κ* for Clarity b | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1.00 | 0.83 | 0.67 | 0.5 | Excellent | Good | Fair | Poor | 1.00 | 0.83 | 0.67 | 0.5 | Excellent | Good | Fair | Poor | |
| Cooking habits | 85.7 | 14.3 | 0 | 0 | 100 | 0 | 0 | 0 | 78.6 | 21.4 | 0 | 0 | 100 | 0 | 0 | 0 |
| Dietary habits | 87.5 | 12.5 | 0 | 0 | 100 | 0 | 0 | 0 | 60.0 | 40.0 | 0 | 0 | 100 | 0 | 0 | 0 |
| Use of cooking techniques | 93.3 | 4.8 | 1.9 | 0 | 98.1 | 0 | 1.9 | 0 | 78.2 | 20.0 | 1.8 | 0 | 98.2 | 0 | 1.8 | 0 |
| Use of cooking ingredients | 96.7 | 3.3 | 0 | 0 | 100 | 0 | 0 | 0 | 98.6 | 1.4 | 0 | 0 | 100 | 0 | 0 | 0 |
| Use of cooking utensils | 75.0 | 25.0 | 0 | 0 | 100 | 0 | 0 | 0 | 93.3 | 6.7 | 0 | 0 | 100 | 0 | 0 | 0 |
| Whole questionnaire | 92.8 | 6.2 | 1.0 | 0 | 99.0 | 0 | 1.0 | 0 | 84.9 | 14.2 | 0.9 | 0 | 99.1 | 0 | 0.9 | 0 |
| n (%) | ||
|---|---|---|
| Yes | No | |
| Q1. The questionnaire is interesting | 17 (100%) | 0 (0%) |
| Q2. The questionnaire helps you to know your cooking habits | 17 (100%) | 0 (0%) |
| Q3. The questionnaire includes all aspects about cooking habits | 13 (93%) | 1 (7%) |
| Q4. The questionnaire is too long | 3 (18%) | 14 (82%) |
| Q5. The instructions given throughout the questionnaire are well understood | 15 (88%) | 2 (12%) |
| Q6. There are questions difficult to understand or answer | 1 (7%) | 14 (93%) |
| Q7. The number of response options is adequate and sufficient | 15 (88%) | 2 (12%) |
| Q8. Other comments or ideas to improve the questionnaire | 2 (12%) | 15 (88%) |
| Domains of the HCFQ | Cronbach Alpha (Phase 3) | Cronbach Alpha (Phase 5) | ||
|---|---|---|---|---|
| Value | n | Value | n | |
| Cooking habits | 0.76 | 13–17 | 0.68 | 51 |
| Dietary habits | 0.56 | 17 | 0.63 | 51 |
| Use of cooking techniques | 0.89 | 14–17 | 0.76 | 51 |
| Use of cooking ingredients | 0.91 | 16–17 | 0.86 | 51 |
| Use of cooking utensils | 0.74 | 15–17 | 0.60 | 51 |
| Whole questionnaire | 0.94 | 13–17 | 0.90 | 51 |
| Cooking Techniques | ICC (95% CI) | p Value |
|---|---|---|
| Baking/Roasting | 0.14 (−0.36; 0.57) | 0.285 |
| Grilling (barbecue) | − | − |
| Grilling (griddle) | 0.60 (0.21; 0.82) | 0.002 |
| Steaming | 0.65 (0.29; 0.85) | 0.001 |
| Simmering | −0.06 (−0.38; 0.34) | 0.625 |
| Microwave | 0.36 (−0.13; 0.70) | 0.071 |
| Frying | 0.55 (0.07; 0.81) | 0.001 |
| Braising | 0.09 (−0.41; 0.54) | 0.357 |
| Battered/Breaded and fried | 0.21 (−0.22; 0.60) | 0.176 |
| Raw | 0.65 (0.29; 0.85) | 0.001 |
| Omelet | 0.69 (0.33; 0.87) | 0.001 |
| Sautéeing | 0.31 (−0.08; 0.65) | 0.047 |
| Cooking Habits Domain | ƙ | p Value |
|---|---|---|
| Plan weekly menus | 0.60 | <0.001 |
| Weekly grocery shopping | 1.00 | <0.001 |
| Cook at home | 0.92 | <0.001 |
| Percentage of dishes cooked at home | 0.53 | <0.001 |
| Batch cooking | 0.44 | 0.002 |
| Hours/week cooking at home | 0.60 | <0.001 |
| Hours/week cooking at home during holidays | 0.49 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goni, L.; Gil, M.; de la O, V.; Martínez-González, M.Á.; Eisenberg, D.M.; Pueyo-Garrigues, M.; Vasilj, M.; Gayoso, L.; Etxeberria, U.; Ruiz-Canela, M. Development and Validation of a New Home Cooking Frequency Questionnaire: A Pilot Study. Nutrients 2022, 14, 1136. https://doi.org/10.3390/nu14061136
Goni L, Gil M, de la O V, Martínez-González MÁ, Eisenberg DM, Pueyo-Garrigues M, Vasilj M, Gayoso L, Etxeberria U, Ruiz-Canela M. Development and Validation of a New Home Cooking Frequency Questionnaire: A Pilot Study. Nutrients. 2022; 14(6):1136. https://doi.org/10.3390/nu14061136
Chicago/Turabian StyleGoni, Leticia, Mario Gil, Víctor de la O, Miguel Ángel Martínez-González, David M. Eisenberg, María Pueyo-Garrigues, Maria Vasilj, Lucía Gayoso, Usune Etxeberria, and Miguel Ruiz-Canela. 2022. "Development and Validation of a New Home Cooking Frequency Questionnaire: A Pilot Study" Nutrients 14, no. 6: 1136. https://doi.org/10.3390/nu14061136
APA StyleGoni, L., Gil, M., de la O, V., Martínez-González, M. Á., Eisenberg, D. M., Pueyo-Garrigues, M., Vasilj, M., Gayoso, L., Etxeberria, U., & Ruiz-Canela, M. (2022). Development and Validation of a New Home Cooking Frequency Questionnaire: A Pilot Study. Nutrients, 14(6), 1136. https://doi.org/10.3390/nu14061136