
The Impact of the Quality of Nutrition and Lifestyle in the Reproductive Years of Women with PKU on the Long-Term Health of Their Children




Abstract
:1. Introduction
2. Nutritional Vulnerability of Women with PKU in Their Reproductive Years
2.1. Distal, Social, and Economic Causes of Nutritional Vulnerability in Adult Women with PKU
2.2. Proximal Causes Directly Related to Nutritional Vulnerability in Adult Women with PKU
2.3. Health of Women with PKU
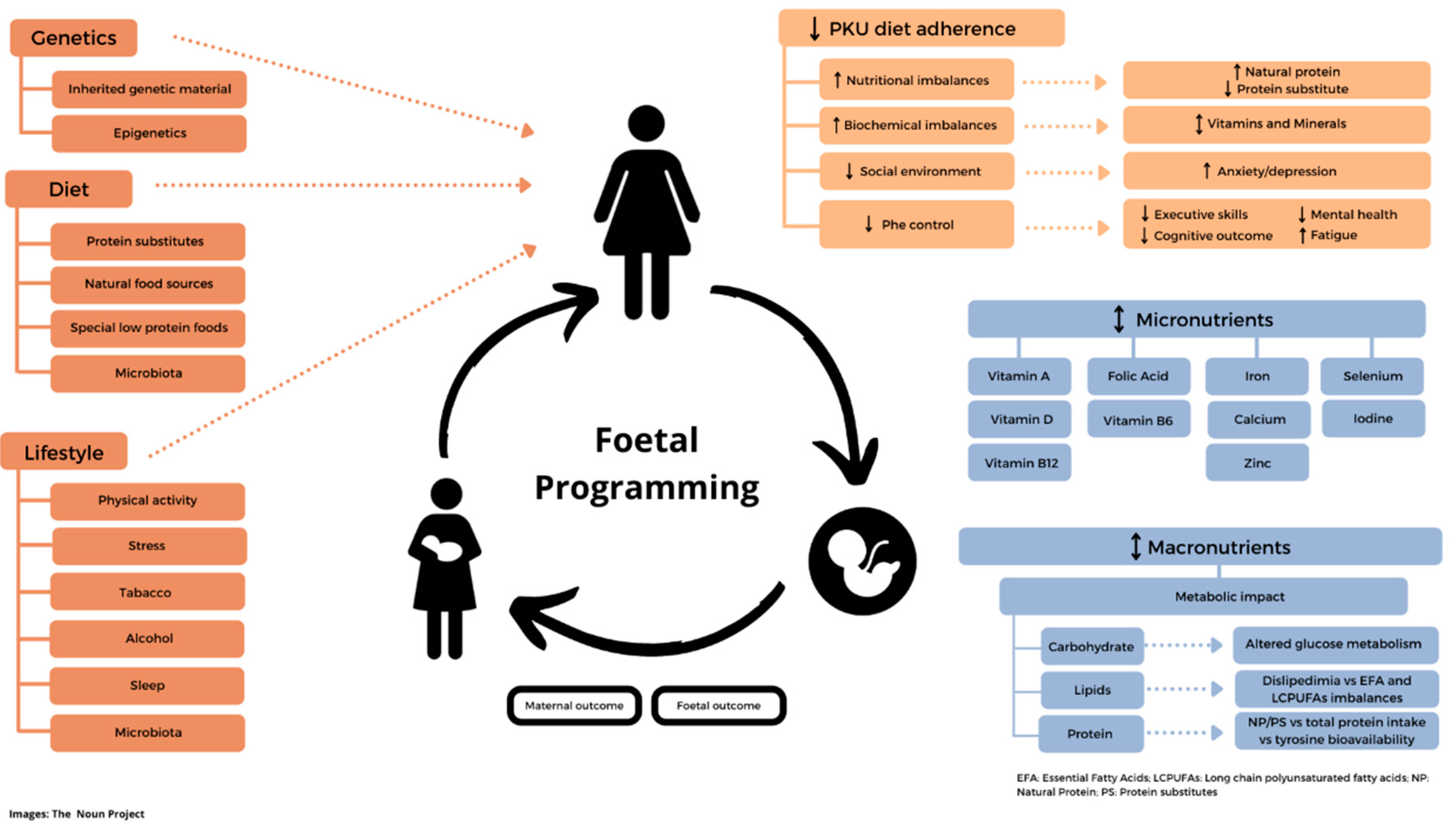
2.4. Nutrition, Foetal Metabolic Programming, and Epigenetics
2.5. Role of Key Micronutrients in Reproductive Nutrition
2.6. Interventions to Improve Nutritional Health in the Reproductive Years of Women with PKU
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- MacDonald, A.; Van Wegberg, A.M.J.; Ahring, K.; Beblo, S.; Bélanger-Quintana, A.; Burlina, A.; Campistol, J.; Coşkun, T.; Feillet, F.; Giżewska, M.; et al. PKU Dietary Handbook to Accompany PKU Guidelines. Orphanet J. Rare Dis. 2020, 15, 171. [Google Scholar] [CrossRef]
- Levy, H.L.; Lenke, R.R.; Koch, R. Lack of Fetal Effect on Blood Phenylalanine Concentration in Maternal Phenylketonuria. J. Pediatr. 1984, 104, S0022–S3476. [Google Scholar] [CrossRef]
- Davidson, D.C. Maternal Phenylketonuria. Postgrad. Med. J. 1989, 65 (Suppl. 2), S10–S20. [Google Scholar] [PubMed]
- Van Wegberg, A.M.J.; MacDonald, A.; Ahring, K.; Bélanger-Quintana, A.; Blau, N.; Bosch, A.M.; Burlina, A.; Campistol, J.; Feillet, F.; Giżewska, M.; et al. The Complete European Guidelines on Phenylketonuria: Diagnosis and Treatment. Orphanet J. Rare Dis. 2017, 12, 162. [Google Scholar] [CrossRef] [Green Version]
- Murphy, E. Pregnancy in Women with Inherited Metabolic Disease. Obstet. Med. 2015, 8, 61–67. [Google Scholar] [CrossRef] [Green Version]
- Ford, S.; O’Driscoll, M.; MacDonald, A. Reproductive Experience of Women Living with Phenylketonuria. Mol. Genet. Metab. Rep. 2018, 17, 64–68. [Google Scholar] [CrossRef]
- Public Health England. Health Matters: Reproductive Health and Pregnancy Planning. Available online: https://www.gov.uk/government/publications/health-matters-reproductive-health-and-pregnancy-planning/health-matters-reproductive-health-and-pregnancy-planning (accessed on 1 February 2022).
- Stephenson, J.; Heslehurst, N.; Hall, J.; Schoenaker, D.A.J.M.; Hutchinson, J.; Cade, J.E.; Poston, L.; Barrett, G.; Crozier, S.R.; Barker, M.; et al. Before the Beginning: Nutrition and Lifestyle in the Preconception Period and Its Importance for Future Health. Lancet 2018, 391, 1830–1841. [Google Scholar] [CrossRef]
- MacDonald, A.; Singh, R.H.; Rocha, J.C.; van Spronsen, F.J. Optimising Amino Acid Absorption: Essential to Improve Nitrogen Balance and Metabolic Control in Phenylketonuria. Nutr. Res. Rev. 2019, 32, 70–78. [Google Scholar] [CrossRef]
- Pena, M.J.; Almeida, M.F.; van Dam, E.; Ahring, K.; Bélanger-Quintana, A.; Dokoupil, K.; Gokmen-Ozel, H.; Lammardo, A.M.; MacDonald, A.; Robert, M.; et al. Special Low Protein Foods for Phenylketonuria: Availability in Europe and an Examination of Their Nutritional Profile. Orphanet J. Rare Dis. 2015, 10, 162. [Google Scholar] [CrossRef] [Green Version]
- Wood, G.; Evans, S.; Pointon-Bell, K.; Rocha, J.C.; MacDonald, A. Special Low Protein Foods in the UK: An Examination of Their Macronutrient Composition in Comparison to Regular Foods. Nutrients 2020, 12, 1893. [Google Scholar] [CrossRef]
- Couce, M.L.; Sánchez-Pintos, P.; Vitoria, I.; De Castro, M.-J.; Aldámiz-Echevarría, L.; Correcher, P.; Fernández-Marmiesse, A.; Roca, I.; Hermida, A.; Martínez-Olmos, M.; et al. Carbohydrate Status in Patients with Phenylketonuria. Orphanet J. Rare Dis. 2018, 13, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moretti, F.; Pellegrini, N.; Salvatici, E.; Rovelli, V.; Banderali, G.; Radaelli, G.; Scazzina, F.; Giovannini, M.; Verduci, E. Dietary Glycemic Index, Glycemic Load and Metabolic Profile in Children with Phenylketonuria. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Levy, H.; Lamppu, D.; Anastosoaie, V.; Baker, J.L.; DiBona, K.; Hawthorne, S.; Lindenberger, J.; Kinch, D.; Seymour, A.; McIlduff, M.; et al. 5-Year Retrospective Analysis of Patients with Phenylketonuria (PKU) and Hyperphenylalaninemia Treated at Two Specialized Clinics. Mol. Genet. Metab. 2020, 129, 177–185. [Google Scholar] [CrossRef]
- Kanufre, V.; Almeida, M.F.; Barbosa, C.S.; Carmona, C.; Bandeira, A.; Martins, E.; Rocha, S.; Guimas, A.; Ribeiro, R.; MacDonald, A.; et al. Metabolic Control of Patients with Phenylketonuria in a Portuguese Metabolic Centre Comparing Three Different Recommendations. Nutrients 2021, 13, 3118. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.S.; Lichter-Konecki, U. Phenylketonuria (PKU): A Problem Solved? Mol. Genet. Metab. Rep. 2016, 6, 8–12. [Google Scholar] [CrossRef]
- Weglage, J.; Fromm, J.; van Teeffelen-Heithoff, A.; Möller, H.E.; Koletzko, B.; Marquardt, T.; Rutsch, F.; Feldmann, R. Neurocognitive Functioning in Adults with Phenylketonuria: Results of a Long Term Study. Mol. Genet. Metab. 2013, 110, S44–S48. [Google Scholar] [CrossRef]
- Cazzorla, C.; Bensi, G.; Biasucci, G.; Leuzzi, V.; Manti, F.; Musumeci, A.; Papadia, F.; Stoppioni, V.; Tummolo, A.; Vendemiale, M.; et al. Living with Phenylketonuria in Adulthood: The PKU ATTITUDE Study. Mol. Genet. Metab. Rep. 2018, 16, 39–45. [Google Scholar] [CrossRef]
- Wood, G.; Pinto, A.; Evans, S.; Daly, A.; Adams, S.; Costelloe, S.; Gribben, J.; Ellerton, C.; Emm, A.; Firman, S.; et al. Special Low Protein Foods Prescribed in England for PKU Patients: An Analysis of Prescribing Patterns and Cost. Nutrients 2021, 13, 3977. [Google Scholar] [CrossRef]
- Bik-Multanowski, M.; Didycz, B.; Mozrzymas, R.; Nowacka, M.; Kaluzny, L.; Cichy, W.; Schneiberg, B.; Amilkiewicz, J.; Bilar, A.; Gizewska, M.; et al. Quality of Life in Noncompliant Adults with Phenylketonuria after Resumption of the Diet. J. Inherit. Metab. Dis. 2008, 31 (Suppl. 2), S415–S418. [Google Scholar] [CrossRef]
- Green, B.; Browne, R.; Firman, S.; Hill, M.; Rahman, Y.; Kaalund Hansen, K.; Adam, S.; Skeath, R.; Hallam, P.; Herlihy, I.; et al. Nutritional and Metabolic Characteristics of UK Adult Phenylketonuria Patients with Varying Dietary Adherence. Nutrients 2019, 11, 2459. [Google Scholar] [CrossRef] [Green Version]
- Rohde, C.; von Teeffelen-Heithoff, A.; Thiele, A.G.; Arelin, M.; Mütze, U.; Kiener, C.; Gerloff, J.; Baerwald, C.; Schultz, S.; Heller, C.; et al. PKU Patients on a Relaxed Diet May Be at Risk for Micronutrient Deficiencies. Eur. J. Clin. Nutr. 2014, 68, 119–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacDonald, A.; Gokmen-Ozel, H.; van Rijn, M.; Burgard, P. The Reality of Dietary Compliance in the Management of Phenylketonuria. J. Inherit. Metab. Dis. 2010, 33, 665–670. [Google Scholar] [CrossRef] [PubMed]
- Ford, S.; O’Driscoll, M.; MacDonald, A. Living with Phenylketonuria: Lessons from the PKU Community. Mol. Genet. Metab. Rep. 2018, 17, 57–63. [Google Scholar] [CrossRef]
- Corrales, P.; Vidal-Puig, A.; Medina-Gómez, G. Obesity and Pregnancy, the Perfect Metabolic Storm. Eur. J. Clin. Nutr. 2021, 75, 1723–1734. [Google Scholar] [CrossRef]
- Rodrigues, C.; Pinto, A.; Faria, A.; Teixeira, D.; van Wegberg, A.M.J.; Ahring, K.; Feillet, F.; Calhau, C.; MacDonald, A.; Moreira-Rosário, A.; et al. Is the Phenylalanine-Restricted Diet a Risk Factor for Overweight or Obesity in Patients with Phenylketonuria (PKU)? A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 3443. [Google Scholar] [CrossRef] [PubMed]
- Robertson, L.V.; McStravick, N.; Ripley, S.; Weetch, E.; Donald, S.; Adam, S.; Micciche, A.; Boocock, S.; MacDonald, A. Body Mass Index in Adult Patients with Diet-Treated Phenylketonuria. J. Hum. Nutr. Diet. Off. J. Br. Diet. Assoc. 2013, 26 (Suppl. 1), 1–6. [Google Scholar] [CrossRef] [PubMed]
- Rocha, J.C.; van Rijn, M.; van Dam, E.; Ahring, K.; Bélanger-Quintana, A.; Dokoupil, K.; Gokmen Ozel, H.; Lammardo, A.M.; Robert, M.; Heidenborg, C.; et al. Weight Management in Phenylketonuria: What Should Be Monitored. Ann. Nutr. Metab. 2016, 68, 60–65. [Google Scholar] [CrossRef] [Green Version]
- Silveira, A.M.; Lima, P.L.; Alves, M.R.A.; Soares, R.D.L.; de Kanufre, V.C.; de Rodrigues, V.M.; Starling, A.L.P.; de Norton, R.C.; de Aguiar, M.J.B. Overweight/Obesity in Adolescents with Phenylketonuria: Protective and Predisposing Factors. J. Pediatr. 2021, 98, 104–110. [Google Scholar] [CrossRef]
- Tonon, T.; Martinez, C.; Poloni, S.; Nalin, T.; Macdonald, A.; Schwartz, I.V.D. Food Neophobia in Patients with Phenylketonuria. J. Endocrinol. Metab. 2019, 9, 108–112. [Google Scholar] [CrossRef]
- Bilder, D.A.; Kobori, J.A.; Cohen-Pfeffer, J.L.; Johnson, E.M.; Jurecki, E.R.; Grant, M.L. Neuropsychiatric Comorbidities in Adults with Phenylketonuria: A Retrospective Cohort Study. Mol. Genet. Metab. 2017, 121, 1–8. [Google Scholar] [CrossRef]
- Viau, K.; Wessel, A.; Martell, L.; Sacharow, S.; Rohr, F. Nutrition Status of Adults with Phenylketonuria Treated with Pegvaliase. Mol. Genet. Metab. 2021, 133, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Luu, S.; Breunig, T.; Drilias, N.; Kuhl, A.; Scott Schwoerer, J.; Cody, P. A Survey of Eating Attitudes and Behaviors in Adolescents and Adults with Phenylalanine Hydroxylase Deficiency. WMJ 2020, 119, 37–43. [Google Scholar] [PubMed]
- Evans, S.; Daly, A.; Chahal, S.; Ashmore, C.; MacDonald, J.; MacDonald, A. The Influence of Parental Food Preference and Neophobia on Children with Phenylketonuria (PKU). Mol. Genet. Metab. Rep. 2018, 14, 10–14. [Google Scholar] [CrossRef]
- Evans, S.; Daly, A.; Chahal, S.; MacDonald, J.; MacDonald, A. Food Acceptance and Neophobia in Children with Phenylketonuria: A Prospective Controlled Study. J. Hum. Nutr. Diet. Off. J. Br. Diet. Assoc. 2016, 29, 427–433. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, A.; Harris, G.; Rylance, G.; Asplin, D.; Booth, I.W. Abnormal Feeding Behaviours in Phenylketonuria. J. Hum. Nutr. Diet. 1997, 10, 163–170. [Google Scholar] [CrossRef]
- MacDonald, A.; Rylance, G.W.; Asplin, D.A.; Hall, K.; Harris, G.; Booth, I.W. Feeding Problems in Young PKU Children. Acta Paediatr. Suppl. 1994, 407, 73–74. [Google Scholar] [CrossRef]
- De Cosmi, V.; Scaglioni, S.; Agostoni, C. Early Taste Experiences and Later Food Choices. Nutrients 2017, 9, 107. [Google Scholar] [CrossRef] [Green Version]
- Robertson, L.; Adam, S.; Ellerton, C.; Ford, S.; Hill, M.; Randles, G.; Woodall, A.; Young, C.; Macdonald, A. Dietetic Management of Adults with Phenylketonuria (PKU) in the UK: A Care Consensus Document. Nutrients 2022, 14, 576. [Google Scholar] [CrossRef]
- Das, A.M.; Goedecke, K.; Meyer, U.; Kanzelmeyer, N.; Koch, S.; Illsinger, S.; Lücke, T.; Hartmann, H.; Lange, K.; Lanfermann, H.; et al. Dietary Habits and Metabolic Control in Adolescents and Young Adults with Phenylketonuria: Self-Imposed Protein Restriction May Be Harmful. JIMD Rep. 2014, 13, 149–158. [Google Scholar] [CrossRef] [Green Version]
- Hochuli, M.; Bollhalder, S.; Thierer, C.; Refardt, J.; Gerber, P.; Baumgartner, M.R. Effects of Inadequate Amino Acid Mixture Intake on Nutrient Supply of Adult Patients with Phenylketonuria. Ann. Nutr. Metab. 2017, 71, 129–135. [Google Scholar] [CrossRef]
- Wild, J.; Shanmuganathan, M.; Hayashi, M.; Potter, M.; Britz-McKibbin, P. Metabolomics for Improved Treatment Monitoring of Phenylketonuria: Urinary Biomarkers for Non-Invasive Assessment of Dietary Adherence and Nutritional Deficiencies. Analyst 2019, 144, 6595–6608. [Google Scholar] [CrossRef] [PubMed]
- Weigel, C.; Kiener, C.; Meier, N.; Schmid, P.; Rauh, M.; Rascher, W.; Knerr, I. Carnitine Status in Early-Treated Children, Adolescents and Young Adults with Phenylketonuria on Low Phenylalanine Diets. Ann. Nutr. Metab. 2008, 53, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Daly, A.; Evans, S.; Pinto, A.; Ashmore, C.; Rocha, J.C.; MacDonald, A. A 3 Year Longitudinal Prospective Review Examining the Dietary Profile and Contribution Made by Special Low Protein Foods to Energy and Macronutrient Intake in Children with Phenylketonuria. Nutrients 2020, 12, 3153. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.; White, F.J.; Cleary, M.A.; Wraith, E.; Lam, W.K.; Walter, J.H. Increased Risk of Vitamin B12 Deficiency in Patients with Phenylketonuria on an Unrestricted or Relaxed Diet. J. Pediatr. 2000, 136, 545–547. [Google Scholar] [CrossRef]
- Demirdas, S.; van Spronsen, F.J.; Hollak, C.E.M.; van der Lee, J.H.; Bisschop, P.H.; Vaz, F.M.; Ter Horst, N.M.; Rubio-Gozalbo, M.E.; Bosch, A.M. Micronutrients, Essential Fatty Acids and Bone Health in Phenylketonuria. Ann. Nutr. Metab. 2017, 70, 111–121. [Google Scholar] [CrossRef]
- Procházková, D.; Jarkovský, J.; Vinohradská, H.; Konečná, P.; Machačová, L.; Doležel, Z. Controlled Diet in Phenylketonuria and Hyperphenylalaninemia May Cause Serum Selenium Deficiency in Adult Patients: The Czech Experience. Biol. Trace Elem. Res. 2013, 154, 178–184. [Google Scholar] [CrossRef]
- Sumanszki, C.; Kiss, E.; Simon, E.; Galgoczi, E.; Soos, A.; Patocs, A.; Kovacs, B.; Nagy, E.V.; Reismann, P. The Association of Therapy Adherence and Thyroid Function in Adult Patients with Phenylketonuria. Ann. Nutr. Metab. 2019, 75, 16–23. [Google Scholar] [CrossRef]
- Marciniak, A.; Patro-Małysza, J.; Kimber-Trojnar, Ż.; Marciniak, B.; Oleszczuk, J.; Leszczyńska-Gorzelak, B. Fetal Programming of the Metabolic Syndrome. Taiwan. J. Obstet. Gynecol. 2017, 56, 133–138. [Google Scholar] [CrossRef]
- Sedaghat, K.; Zahediasl, S.; Ghasemi, A. Intrauterine Programming. Iran. J. Basic Med. Sci. 2015, 18, 212–220. [Google Scholar]
- Fleming, T.P.; Watkins, A.J.; Velazquez, M.A.; Mathers, J.C.; Prentice, A.M.; Stephenson, J.; Barker, M.; Saffery, R.; Yajnik, C.S.; Eckert, J.J.; et al. Origins of Lifetime Health around the Time of Conception: Causes and Consequences. Lancet 2018, 391, 1842–1852. [Google Scholar] [CrossRef]
- Roseboom, T.; de Rooij, S.; Painter, R. The Dutch Famine and Its Long-Term Consequences for Adult Health. Early Hum. Dev. 2006, 82, 485–491. [Google Scholar] [CrossRef]
- Zhu, Z.; Cao, F.; Li, X. Epigenetic Programming and Fetal Metabolic Programming. Front. Endocrinol. 2019, 10, 764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sookoian, S.; Gianotti, T.F.; Burgueño, A.L.; Pirola, C.J. Fetal Metabolic Programming and Epigenetic Modifications: A Systems Biology Approach. Pediatr. Res. 2013, 73, 531–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaenisch, R.; Bird, A. Epigenetic Regulation of Gene Expression: How the Genome Integrates Intrinsic and Environmental Signals. Nat. Genet. 2003, 33, 245–254. [Google Scholar] [CrossRef]
- Reichetzeder, C. Overweight and Obesity in Pregnancy: Their Impact on Epigenetics. Eur. J. Clin. Nutr. 2021, 75, 1710–1722. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Fernandez, J.; Ochoa, J.J.; Lopez-Frias, M.; Diaz-Castro, J. Impact of Early Nutrition, Physical Activity and Sleep on the Fetal Programming of Disease in the Pregnancy: A Narrative Review. Nutrients 2020, 12, 3900. [Google Scholar] [CrossRef]
- Lammi-Keefe, C.J.; Couch, S.C.; Kirwan, J.P. Handbook on Nutrition and Pregnancy, 2nd ed.; Humana Press: New York, NY, USA, 2018. [Google Scholar] [CrossRef]
- Barker, D.J.P. Fetal Programming of Coronary Heart Disease. Trends Endocrinol. Metab. 2002, 13, 364–368. [Google Scholar] [CrossRef]
- Tiffon, C. The Impact of Nutrition and Environmental Epigenetics on Human Health and Disease. Int. J. Mol. Sci. 2018, 19, 3425. [Google Scholar] [CrossRef] [Green Version]
- Hodgetts, V.A.; Morris, R.K.; Francis, A.; Gardosi, J.; Ismail, K.M. Effectiveness of Folic Acid Supplementation in Pregnancy on Reducing the Risk of Small-for-Gestational Age Neonates: A Population Study, Systematic Review and Meta-Analysis. BJOG 2015, 122, 478–490. [Google Scholar] [CrossRef]
- Rajendram, R.; Preedy, V.R.; Patel, V.B. Diet, Nutrition, and Fetal Programming; Humana Press: New York, NY, USA, 2017. [Google Scholar] [CrossRef]
- Tian, X.; Anthony, K.; Neuberger, T.; Diaz, F.J. Preconception Zinc Deficiency Disrupts Postimplantation Fetal and Placental Development in Mice. Biol. Reprod. 2014, 90, 83. [Google Scholar] [CrossRef]
- Nafee, T.M.; Farrell, W.E.; Carroll, W.D.; Fryer, A.A.; Ismail, K.M.K. Epigenetic Control of Fetal Gene Expression. BJOG 2008, 115, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Hanson, M.A.; Bardsley, A.; De-Regil, L.M.; Moore, S.E.; Oken, E.; Poston, L.; Ma, R.C.; McAuliffe, F.M.; Maleta, K.; Purandare, C.N.; et al. The International Federation of Gynecology and Obstetrics (FIGO) Recommendations on Adolescent, Preconception, and Maternal Nutrition: “Think Nutrition First”. Int. J. Gynaecol. Obstet. Off. Organ Int. Fed. Gynaecol. Obstet. 2015, 131, S213–S253. [Google Scholar] [CrossRef] [Green Version]
- Hvas, A.M.; Nexo, E.; Nielsen, J.B. Vitamin B12 and Vitamin B6 Supplementation Is Needed among Adults with Phenylketonuria (PKU). J. Inherit. Metab. Dis. 2006, 29, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Stølen, L.H.; Lilje, R.; Jørgensen, J.V.; Bliksrud, Y.T.; Almaas, R. High Dietary Folic Acid and High Plasma Folate in Children and Adults with Phenylketonuria. JIMD Rep. 2014, 13, 83–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vugteveen, I.; Hoeksma, M.; Monsen, A.-L.B.; Fokkema, M.R.; Reijngoud, D.-J.; van Rijn, M.; van Spronsen, F.J. Serum Vitamin B12 Concentrations within Reference Values Do Not Exclude Functional Vitamin B12 Deficiency in PKU Patients of Various Ages. Mol. Genet. Metab. 2011, 102, 13–17. [Google Scholar] [CrossRef]
- Hieronimus, B.; Ensenauer, R. Influence of Maternal and Paternal Pre-Conception Overweight/Obesity on Offspring Outcomes and Strategies for Prevention. Eur. J. Clin. Nutr. 2021, 75, 1735–1744. [Google Scholar] [CrossRef]
- World Health Organization. Anemia in Women and Children. Available online: https://www.who.int/data/gho/data/themes/topics/anaemia_in_women_and_children (accessed on 20 October 2021).
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and Child Undernutrition and Overweight in Low-Income and Middle-Income Countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Young, M.F.; Oaks, B.M.; Tandon, S.; Martorell, R.; Dewey, K.G.; Wendt, A.S. Maternal Hemoglobin Concentrations across Pregnancy and Maternal and Child Health: A Systematic Review and Meta-Analysis. Ann. N. Y. Acad. Sci. 2019, 1450, 47–68. [Google Scholar] [CrossRef] [Green Version]
- Rao, R.; Tkac, I.; Townsend, E.L.; Gruetter, R.; Georgieff, M.K. Perinatal Iron Deficiency Alters the Neurochemical Profile of the Developing Rat Hippocampus. J. Nutr. 2003, 133, 3215–3221. [Google Scholar] [CrossRef] [Green Version]
- Green, B.; Rahman, Y.; Firman, S.; Adam, S.; Jenkinson, F.; Nicol, C.; Adams, S.; Dawson, C.; Robertson, L.; Dunlop, C.; et al. Improved Eating Behaviour and Nutrient Intake in Noncompliant Patients with Phenylketonuria after Reintroducing a Protein Substitute: Observations from a Multicentre Study. Nutrients 2019, 11, 2035. [Google Scholar] [CrossRef] [Green Version]
- Levie, D.; Korevaar, T.I.M.; Bath, S.C.; Murcia, M.; Dineva, M.; Llop, S.; Espada, M.; van Herwaarden, A.E.; de Rijke, Y.B.; Ibarluzea, J.M.; et al. Association of Maternal Iodine Status with Child IQ: A Meta-Analysis of Individual Participant Data. J. Clin. Endocrinol. Metab. 2019, 104, 5957–5967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stroup, B.M.; Ney, D.M.; Murali, S.G.; Rohr, F.; Gleason, S.T.; van Calcar, S.C.; Levy, H.L. Metabolomic Insights into the Nutritional Status of Adults and Adolescents with Phenylketonuria Consuming a Low-Phenylalanine Diet in Combination with Amino Acid and Glycomacropeptide Medical Foods. J. Nutr. Metab. 2017, 2017, 6859820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, X.; Diaz, F.J. Acute Dietary Zinc Deficiency before Conception Compromises Oocyte Epigenetic Programming and Disrupts Embryonic Development. Dev. Biol. 2013, 376, 51–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duttaroy, A.K.; Basak, S. Maternal Dietary Fatty Acids and Their Roles in Human Placental Development. Prostaglandins. Leukot. Essent. Fatty Acids 2020, 155, 102080. [Google Scholar] [CrossRef] [PubMed]
- Yi, S.H.L.; Kable, J.A.; Evatt, M.L.; Singh, R.H. A Cross-Sectional Study of Docosahexaenoic Acid Status and Cognitive Outcomes in Females of Reproductive Age with Phenylketonuria. J. Inherit. Metab. Dis. 2011, 34, 455–463. [Google Scholar] [CrossRef] [Green Version]
- Gramer, G.; Haege, G.; Langhans, C.-D.; Schuhmann, V.; Burgard, P.; Hoffmann, G.F. Long-Chain Polyunsaturated Fatty Acid Status in Children, Adolescents and Adults with Phenylketonuria. Prostaglandins. Leukot. Essent. Fatty Acids 2016, 109, 52–57. [Google Scholar] [CrossRef]
- Stroup, B.M.; Nair, N.; Murali, S.G.; Broniowska, K.; Rohr, F.; Levy, H.L.; Ney, D.M. Metabolomic Markers of Essential Fatty Acids, Carnitine, and Cholesterol Metabolism in Adults and Adolescents with Phenylketonuria. J. Nutr. 2018, 148, 194–201. [Google Scholar] [CrossRef] [Green Version]
- Giovannini, M.; Biasucci, G.; Agostoni, C.; Bellù, R.; Riva, E. Fatty Acid Supplementation in a Case of Maternal Phenylketonuria. J. Inherit. Metab. Dis. 1994, 17, 630–631. [Google Scholar] [CrossRef]
- Koletzko, B.; Boey, C.C.M.; Campoy, C.; Carlson, S.E.; Chang, N.; Guillermo-Tuazon, M.A.; Joshi, S.; Prell, C.; Quak, S.H.; Sjarif, D.R.; et al. Current Information and Asian Perspectives on Long-Chain Polyunsaturated Fatty Acids in Pregnancy, Lactation, and Infancy: Systematic Review and Practice Recommendations from an Early Nutrition Academy Workshop. Ann. Nutr. Metab. 2014, 65, 49–80. [Google Scholar] [CrossRef]
- Aune, D.; Saugstad, O.D.; Henriksen, T.; Tonstad, S. Maternal Body Mass Index and the Risk of Fetal Death, Stillbirth, and Infant Death: A Systematic Review and Meta-Analysis. JAMA 2014, 311, 1536–1546. [Google Scholar] [CrossRef] [Green Version]
- Poston, L.; Caleyachetty, R.; Cnattingius, S.; Corvalán, C.; Uauy, R.; Herring, S.; Gillman, M.W. Preconceptional and Maternal Obesity: Epidemiology and Health Consequences. Lancet Diabetes Endocrinol. 2016, 4, 1025–1036. [Google Scholar] [CrossRef]
- Gesink Law, D.C.; Maclehose, R.F.; Longnecker, M.P. Obesity and Time to Pregnancy. Hum. Reprod. 2007, 22, 414–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchi, J.; Berg, M.; Dencker, A.; Olander, E.K.; Begley, C. Risks Associated with Obesity in Pregnancy, for the Mother and Baby: A Systematic Review of Reviews. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2015, 16, 621–638. [Google Scholar] [CrossRef] [PubMed]
- Strauss, A. Obesity in Pregnant Women: Maternal, Fetal, and Transgenerational Consequences. Eur. J. Clin. Nutr. 2021, 75, 1681–1683. [Google Scholar] [CrossRef]
- Edwards, S.M.; Cunningham, S.A.; Dunlop, A.L.; Corwin, E.J. The Maternal Gut Microbiome during Pregnancy. MCN. Am. J. Matern. Child Nurs. 2017, 42, 310–317. [Google Scholar] [CrossRef]
- Raymond, J.L.; Morrow, K. Krause and Mahan’s Food & The Nutrition Care Process, 15th ed.; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Moszak, M.; Szulińska, M.; Bogdański, P. You Are What You Eat-The Relationship between Diet, Microbiota, and Metabolic Disorders-A Review. Nutrients 2020, 12, 1096. [Google Scholar] [CrossRef] [Green Version]
- Verduci, E.; Carbone, M.T.; Borghi, E.; Ottaviano, E.; Burlina, A.; Biasucci, G. Nutrition, Microbiota and Role of Gut-Brain Axis in Subjects with Phenylketonuria (PKU): A Review. Nutrients 2020, 12, 3319. [Google Scholar] [CrossRef]
- Bruinenberg, V.M.; Gordijn, M.C.M.; MacDonald, A.; van Spronsen, F.J.; Van der Zee, E.A. Sleep Disturbances in Phenylketonuria: An Explorative Study in Men and Mice. Front. Neurol. 2017, 8, 167. [Google Scholar] [CrossRef]
- Poggiogalle, E.; Jamshed, H.; Peterson, C.M. Circadian Regulation of Glucose, Lipid, and Energy Metabolism in Humans. Metabolism 2018, 84, 11–27. [Google Scholar] [CrossRef] [Green Version]
- Grandner, M.A. Sleep, Health, and Society. Sleep Med. Clin. 2020, 15, 319–340. [Google Scholar] [CrossRef]
- Dean, S.V.; Lassi, Z.S.; Imam, A.M.; Bhutta, Z.A. Preconception Care: Nutritional Risks and Interventions. Reprod. Health 2014, 11 (Suppl. 3), S3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization. Increasing Fruit and Vegetable Consumption to Reduce the Risk of Noncommunicable Diseases. Available online: https://www.who.int/elena/titles/fruit_vegetables_ncds/en/ (accessed on 26 November 2021).
- EFSA. Dietary Reference Values for Nutrients Summary Report. EFSA Support. Publ. 2017, 14, e15121. [Google Scholar] [CrossRef] [Green Version]
- Zmora, N.; Suez, J.; Elinav, E. You Are What You Eat: Diet, Health and the Gut Microbiota. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 35–56. [Google Scholar] [CrossRef] [PubMed]
- Burda, B.U.; Chambers, A.R.; Johnson, J.C. Appraisal of Guidelines Developed by the World Health Organization. Public Health 2014, 128, 444–474. [Google Scholar] [CrossRef]
- Gao, Y.; Sheng, C.; Xie, R.-H.; Sun, W.; Asztalos, E.; Moddemann, D.; Zwaigenbaum, L.; Walker, M.; Wen, S.W. New Perspective on Impact of Folic Acid Supplementation during Pregnancy on Neurodevelopment/Autism in the Offspring Children—A Systematic Review. PLoS ONE 2016, 11, e0165626. [Google Scholar] [CrossRef] [Green Version]
- Thiele, A.G.; Rohde, C.; Mütze, U.; Arelin, M.; Ceglarek, U.; Thiery, J.; Baerwald, C.; Kiess, W.; Beblo, S. The Challenge of Long-Term Tetrahydrobiopterin (BH4) Therapy in Phenylketonuria: Effects on Metabolic Control, Nutritional Habits and Nutrient Supply. Mol. Genet. Metab. Rep. 2015, 4, 62–67. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Cardiovascular Disease: Risk Assessment and Reduction, including Lipid Modification. Available online: https://www.nice.org.uk/guidance/cg181 (accessed on 18 January 2022).
- Watson, N.F.; Badr, M.S.; Belenky, G.; Bliwise, D.L.; Buxton, O.M.; Buysse, D.; Dinges, D.F.; Gangwisch, J.; Grandner, M.A.; Kushida, C.; et al. Recommended Amount of Sleep for a Healthy Adult: A Joint Consensus Statement of the American Academy of Sleep Medicine and Sleep Research Society. Sleep 2015, 38, 843–844. [Google Scholar] [CrossRef]
 broken line-arrows-potentially lower/higher.
broken line-arrows-potentially lower/higher.
broken line-arrows-potentially lower/higher.
broken line-arrows-potentially lower/higher.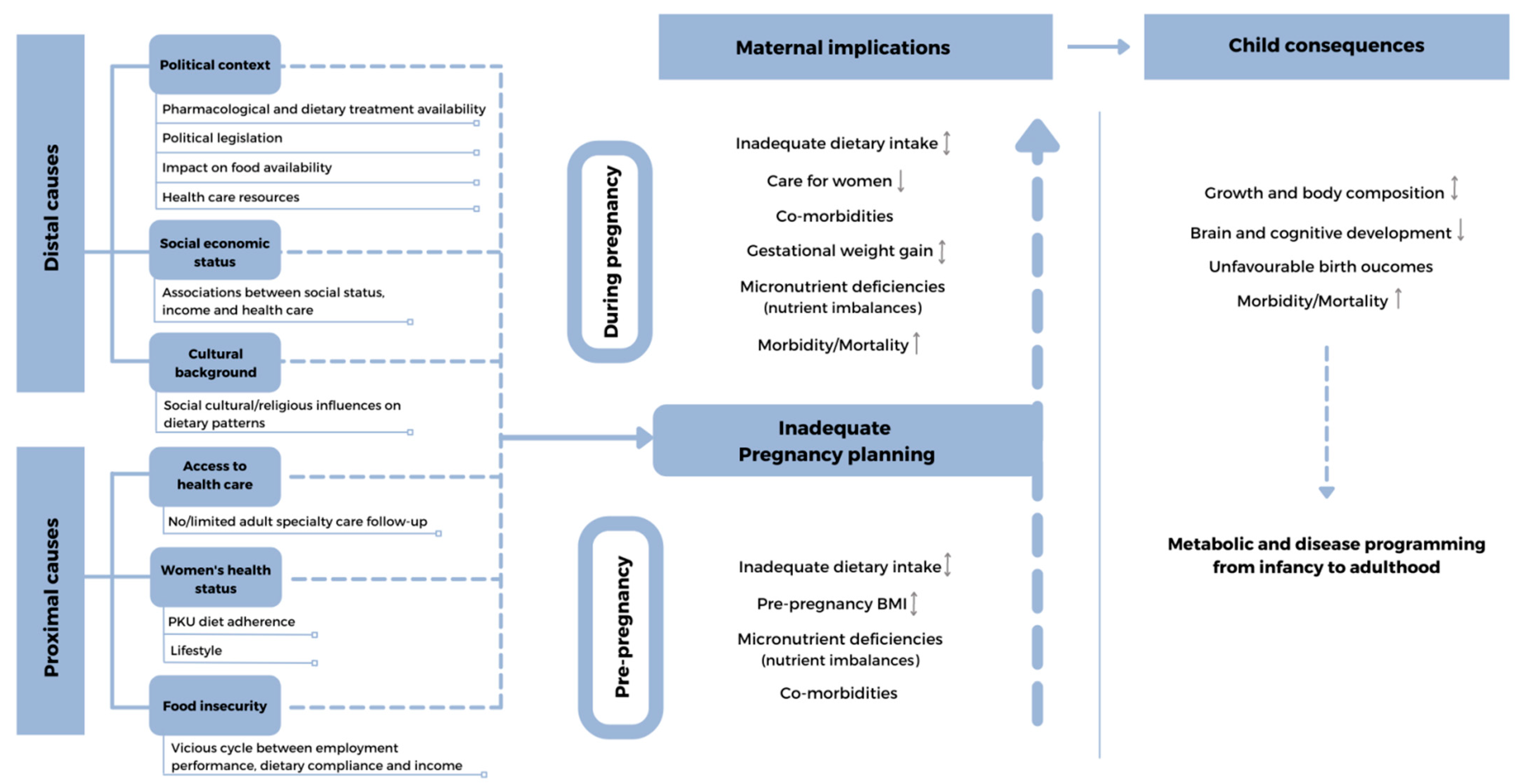 broken line-arrows-potentially lower/higher.
broken line-arrows-potentially lower/higher.
broken line-arrows-potentially lower/higher.
broken line-arrows-potentially lower/higher.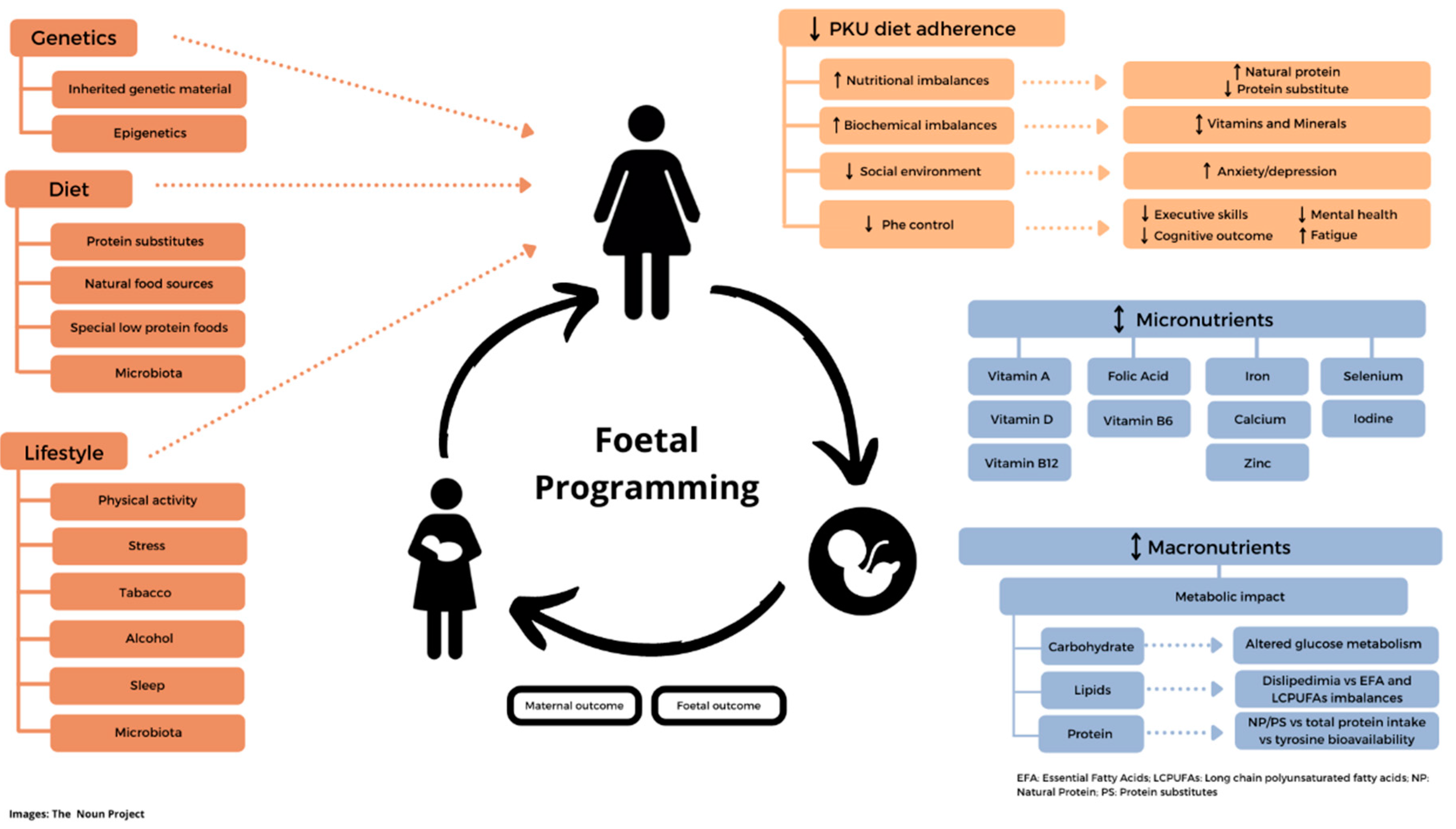

{kind=link}
{kind=link}
| Intervention | Recommendation/Action by Individual Women with PKU or Health Care Teams |
|---|---|
| Prevention of overweightand obesity | Substantial weight loss is particularly difficult in women with PKU due to the catabolic effect of lowering energy intake on PKU and impact on metabolic control and may take months and even years to achieve. Ideally, healthy weight should be established before or during adolescence and pre-pregnancy. Undertake regular preconception assessments of weight, BMI, nutritional monitoring, dietary patterns/intake, and lifestyle. Women with PKU should try and maintain an adequate balance between energy intake and expenditure. Increase amount and range of fruits, vegetables, and plant foods whilst limiting the intake of total fats, free sugars, and sodium. Decrease snacks and late-night eating. Encourage breakfast. Reduce sedentary activity such as television or computer viewing. |
| Regular exercise | Higher levels of preconception physical activity are associated with a lower risk of gestational diabetes and pre-eclampsia [97]. Address sedentary lifestyles early in life by promoting physical activity. Encourage 10,000 steps daily of unstructured activity in the light-to-moderate intensity range that are usually part of daily living (e.g., cycling, climbing stairs, and walking). Sports and structured activities: encourage 150 min per week of structured activities (that range from a moderate to vigorous intensity) [97]. Pedometers or similar apps can be used as forms of motivational support. |
| Improve quality of Phe-restricted diet | Promote adherence to dietary treatment and explore individual resistance to maintaining a Phe-restricted diet. Promote dietary diversification within the limits of dietary restriction. Encourage at least 400 g/day of fruit and vegetables, equivalent to 5/daily portions [98]. A range of different fruits and vegetables will provide different nutrients, phytochemicals, and fibre [90]. The EFSA recommends 25 g/day of fibre [99]. To help achieve this, a high intake of fruit and vegetables and wholegrain cereals (within natural protein allowance) is necessary. Focus on fat quality rather than quantity; monounsaturated and polyunsaturated fat sources provide health benefits associated with triglyceride and cholesterol metabolism. Avoid trans fats and lower saturated fat intake [90]. Give careful guidance on the choice of SLPF’s as some may contain increased amounts of saturated and trans fats when compared to regular foods [11]. Ensure an adequate intake of essential fatty acids such as omega-3 and omega-6, with an emphasis on the optimal ratio of omega-3/omega-6. Encourage less added salt at the meal table and in cooking. Replace salt with herbs and spices. Provide social support to adults with PKU to help attain financial assistance to help purchase basic foods. |
| Encourage a healthy gut/gut microbiota | Assess gut health (particularly check for presence of gastro-intestinal reflux and constipation) at least annually. Fibre sources, including fruit and vegetables, augment microbiota diversity and are beneficial for gut health [90]. Fibre fermentation end-products and short-chain fatty acids (SCFA) have a role in preventing gut dysbiosis associated with metabolic dysfunction and immune response. SCFA, acetate, propionate, and butyrate are important modulators of gut microbiota [100]. Probiotic foods or supplements may offer additional protection. No controlled supplement trials of probiotics have been conducted in women with PKU. |
| Ensure a vitamin/mineral enriched protein substitute is taken in prescribed amounts | Explore any patient barriers to taking a protein substitute as prescribed. Give protein substitute in at least 3/daily doses and spread evenly throughout the day to minimise blood Phe fluctuations and to aid bioavailability of nutrient absorption. Protein substitutes help ensure that many macro- and micro-nutrient requirements are met. Meta-analyses confirm that supplementation or fortification with the ‘big four’ micronutrients (vitamin A, iron, zinc, and iodine) is efficacious to reduce the risk of infectious disease and improves growth and cognitive outcome in infants. |
| Give nutrition supplementsin the peri-conceptual period | Give 400 mg/day of folic acid in the periconceptual period to reduce the risk of neural tube defects by up to 72% [4,101]. Folic acid supplementation will also decrease the risk of pre-eclampsia, miscarriage, low-birth weight, being small for gestational age, a stillbirth, neonatal death, and autism in children [61,102]. A minimum of 4–6 weeks of folic acid supplementation is required to reach adequate levels before neurulation begins three weeks after conception. There is no information about adherence with folic acid supplementation in women with MPKU. |
| General lifestyle factors | Discourage smoking. While there are no published trials showing that reducing smoking before conception improves outcomes, indirect evidence suggests that smoke-free legislation in different countries has been associated with substantial reductions in preterm births [8]. Encourage moderate alcohol consumption in case of unplanned pregnancy. Maternal alcohol consumption can result in a range of foetal alcohol spectrum disorders [8]. Evaluate sources and perceived levels of stress, mood, and support systems. Offer psychological support and counselling. Encourage attendance of ‘online’ group mindfulness/support sessions. |
| Use of sapropterin | Sapropterin can liberate a woman’s diet and increase natural food sources and nutrient intake in sub-groups of responsive women, but education and careful monitoring is needed, as changes in food patterns may have a negative impact on nutrient adequacy [32,103]. |
| Maintain regular nutritional monitoring | Monitor nutritional intake at each dietetic review. Assess food patterns and check for any disordered eating or maladaptive eating practices. Monitor weight, BMI, and abdominal circumference at each face-to-face review. Review the condition of the hair, skin, and nails. Assess patients’ biochemical nutritional status at least once a year. Assess for risk of comorbidities by monitoring lipid profile, blood pressure, and HbA1c [104]. Monitor blood Phe levels (according to European PKU guidelines) [4]. |
| Encourage good sleep hygiene | Evaluate sleep patterns. Adults should aim to sleep at least 7 h per night to maintain optimal health [105]. Eating at late hours in the day has a negative effect on glucose, lipid, and energy metabolism [94], although a late-night dose of protein substitute may help decrease Phe fluctuations. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gama, M.I.; Pinto, A.; Daly, A.; Rocha, J.C.; MacDonald, A. The Impact of the Quality of Nutrition and Lifestyle in the Reproductive Years of Women with PKU on the Long-Term Health of Their Children. Nutrients 2022, 14, 1021. https://doi.org/10.3390/nu14051021
Gama MI, Pinto A, Daly A, Rocha JC, MacDonald A. The Impact of the Quality of Nutrition and Lifestyle in the Reproductive Years of Women with PKU on the Long-Term Health of Their Children. Nutrients. 2022; 14(5):1021. https://doi.org/10.3390/nu14051021
Chicago/Turabian StyleGama, Maria Inês, Alex Pinto, Anne Daly, Júlio César Rocha, and Anita MacDonald. 2022. "The Impact of the Quality of Nutrition and Lifestyle in the Reproductive Years of Women with PKU on the Long-Term Health of Their Children" Nutrients 14, no. 5: 1021. https://doi.org/10.3390/nu14051021
APA StyleGama, M. I., Pinto, A., Daly, A., Rocha, J. C., & MacDonald, A. (2022). The Impact of the Quality of Nutrition and Lifestyle in the Reproductive Years of Women with PKU on the Long-Term Health of Their Children. Nutrients, 14(5), 1021. https://doi.org/10.3390/nu14051021