
Validation of a Food Knowledge Questionnaire on Tanzanian Women of Childbearing Age

 , ,
, ,  , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Questionnaire Design
2.2. Study Setting for the Validation
2.3. Sampling
2.4. Questionnaire Administration
2.5. Descriptive Statistics
2.6. Construct Validity
2.7. Content Validity
3. Results
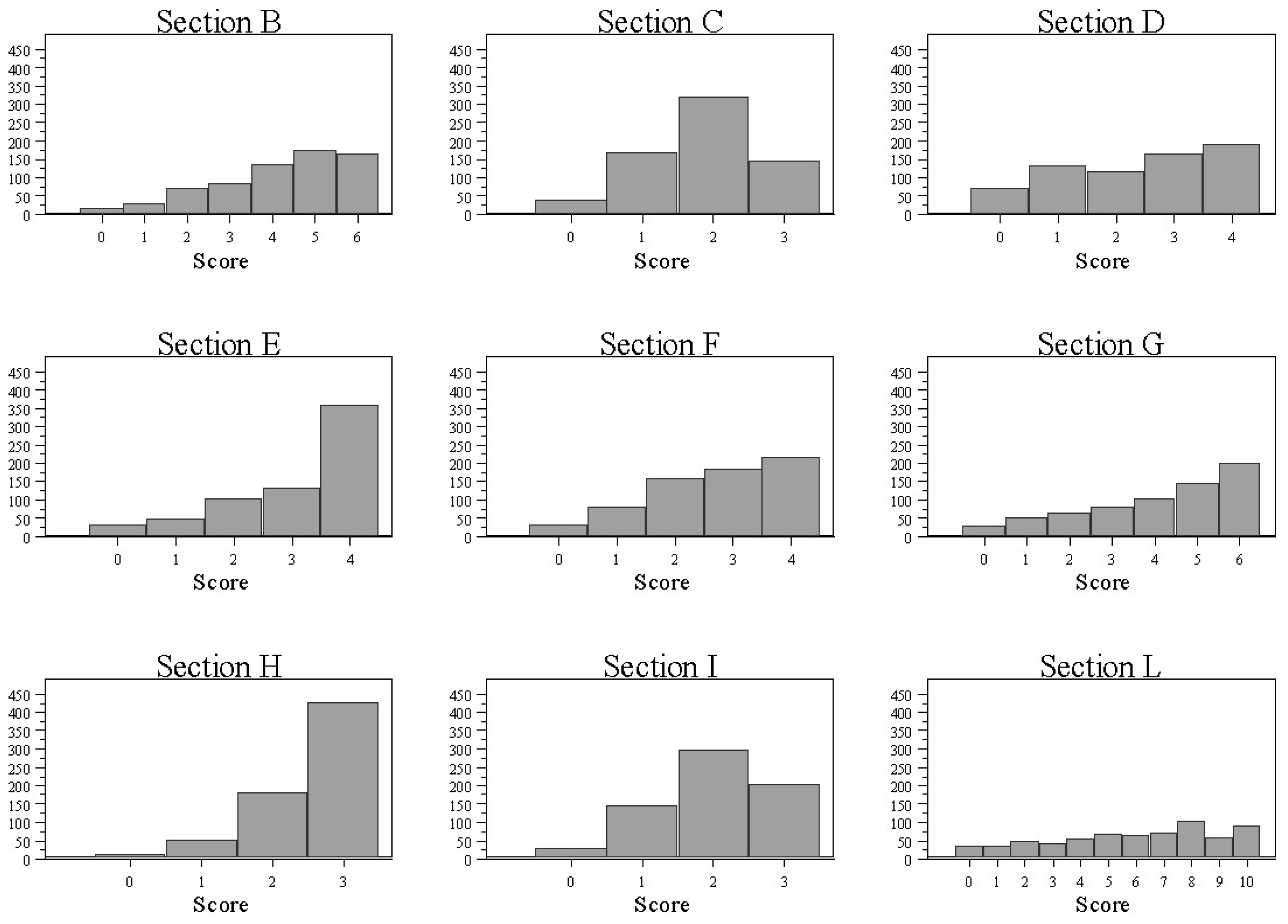
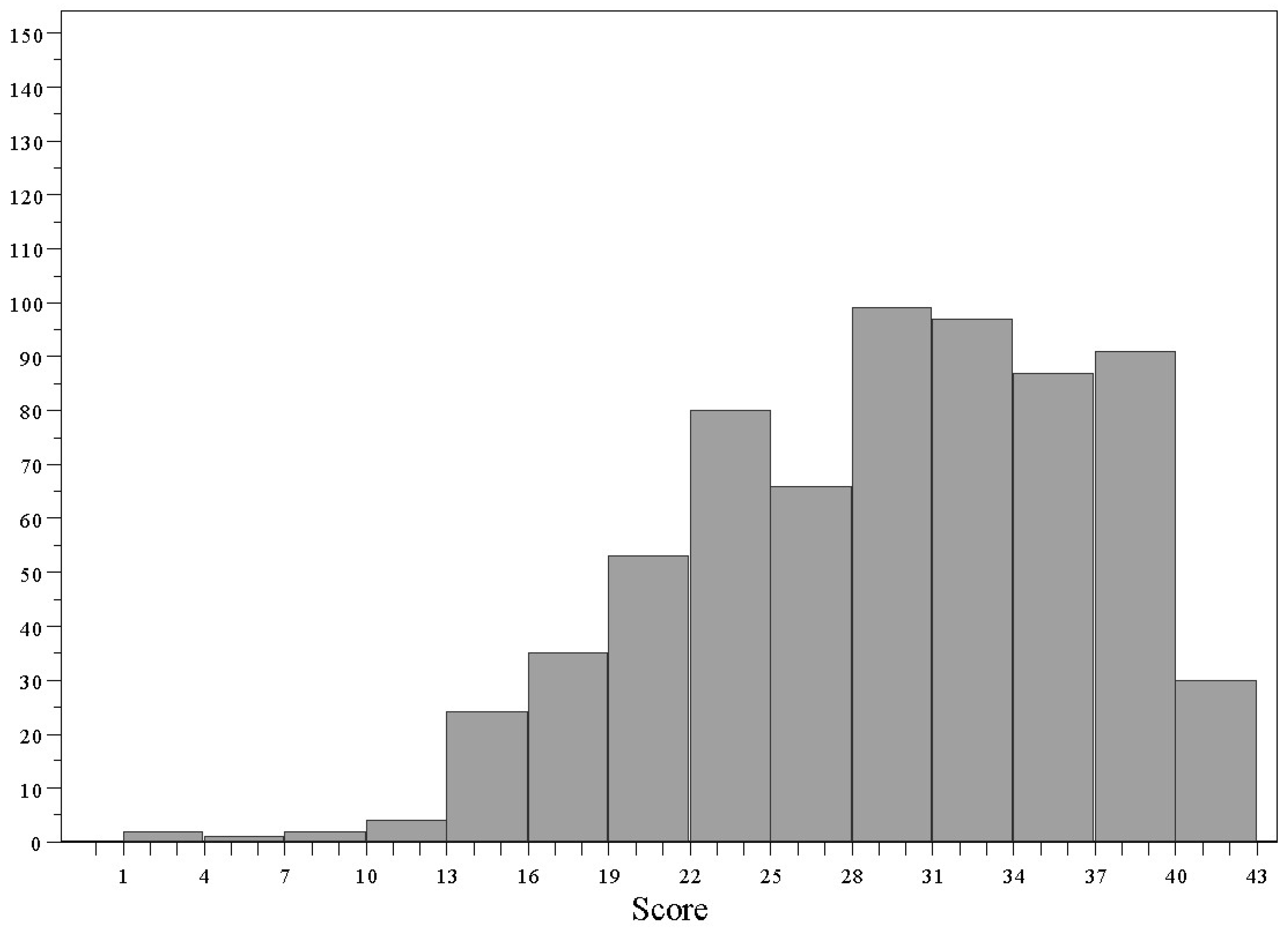
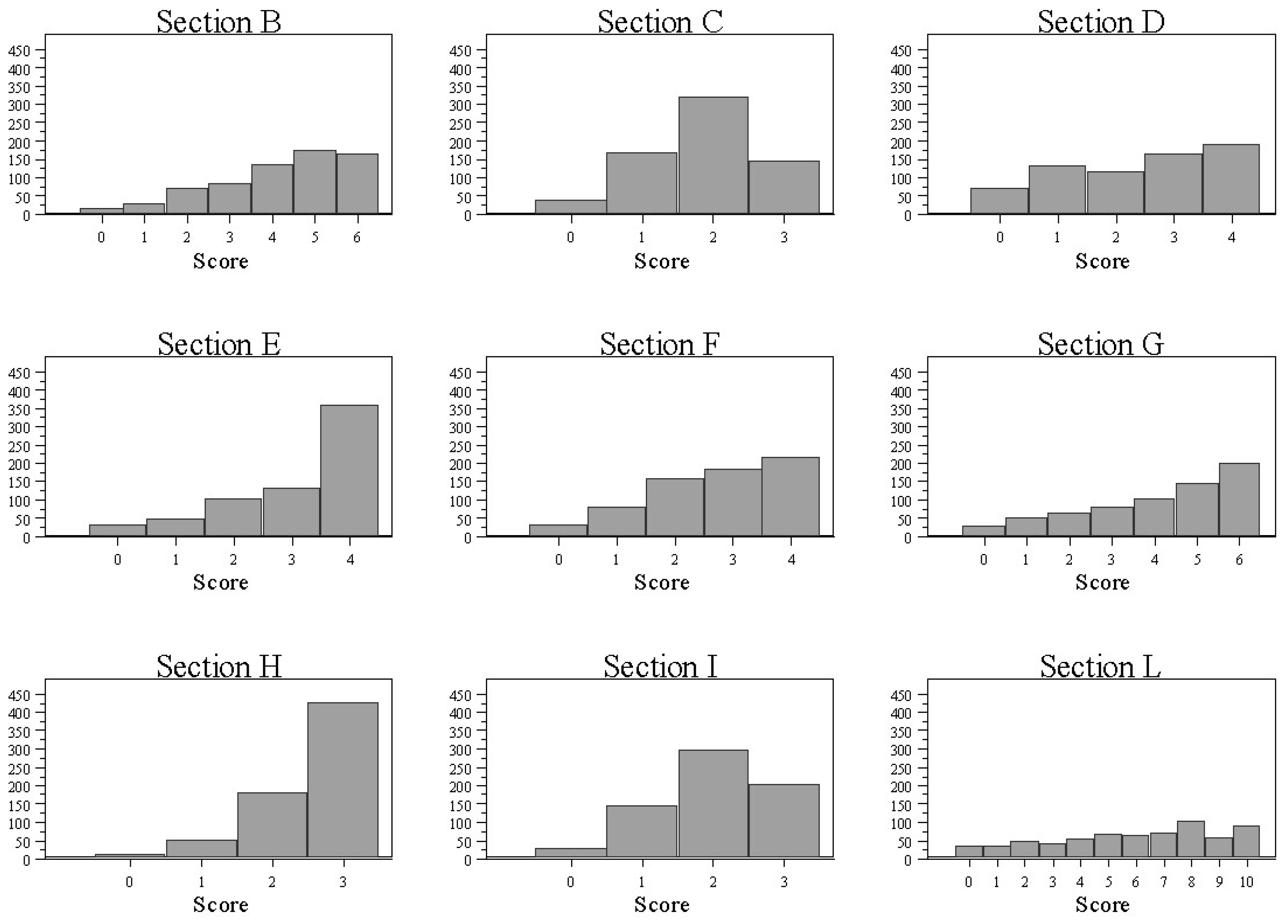
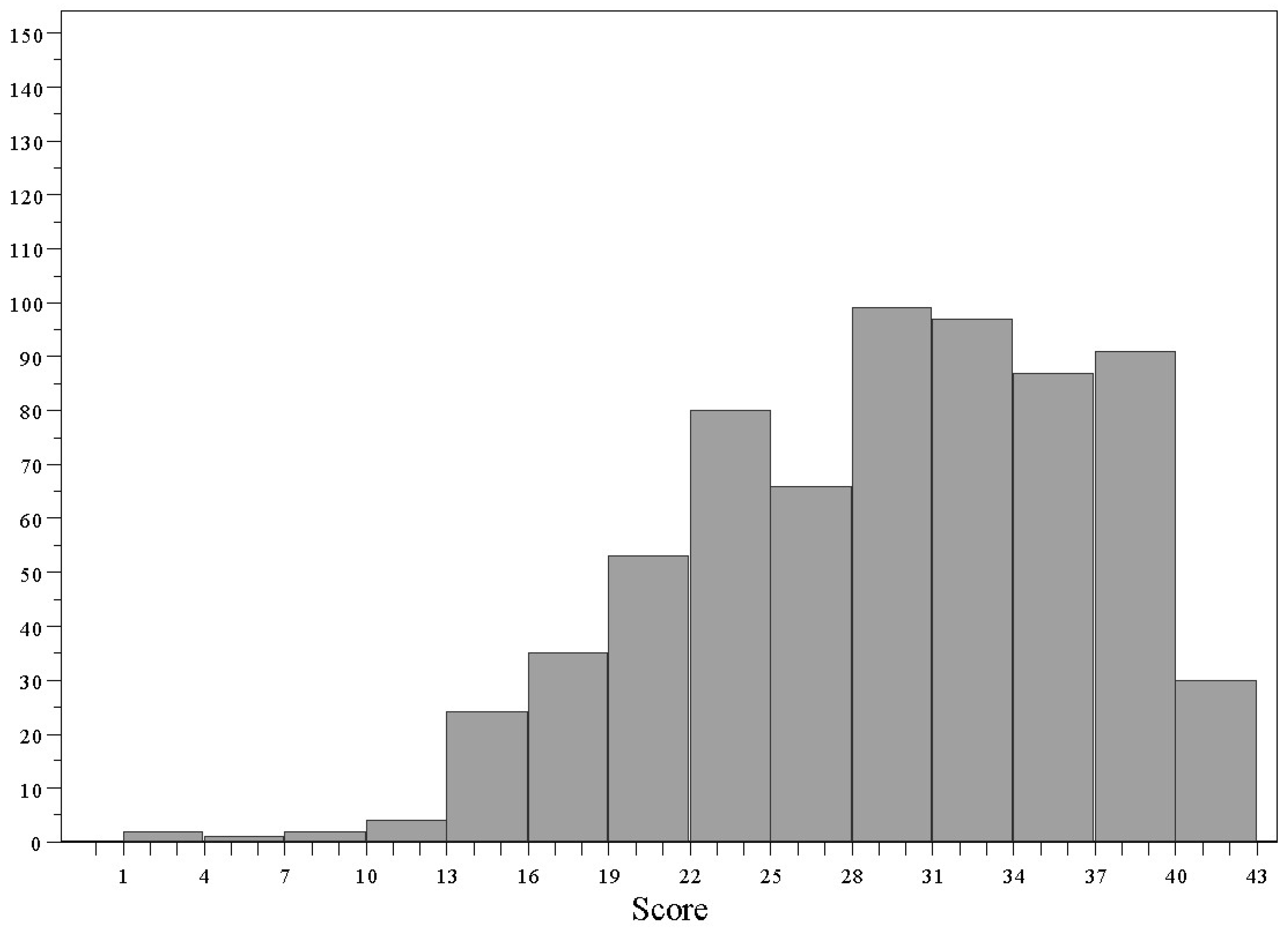
Section Scores and Total FKQ Scores
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rosi, A.; Martini, D.; Grosso, G.; Bonaccio, M.L.; Scazzina, F.; Angelino, D. Validation of a nutrition knowledge questionnaire in Italian students attending the University of Parma. Public Health Nutr. 2020, 23, 1527–1531. [Google Scholar] [CrossRef] [PubMed]
- Debela, B.L.; Demmler, K.M.; Rischke, R.; Qaim, M. Maternal nutrition knowledge and child nutritional outcomes in urban Kenya. Appetite 2017, 116, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, L.B.; Vasconcelos, S.M.; Correia, L.O.; Ferreira, R.C. Nutrition knowledge assessment studies in adults: A systematic review. Cien Saude Colet. 2016, 21, 449–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fadare, O.; Amare, M.; Mavrotas, G.; Akerele, D.; Ogunniyi, A. Mother’s nutrition-related knowledge and child nutrition outcomes: Empirical evidence from Nigeria. PLoS ONE 2019, 14, e0212775. [Google Scholar] [CrossRef]
- Kimani, E.N. Women’s Knowledge and Food Security; University of Nairoby Journal Systems: Nairoby, Kenia, 2015. [Google Scholar]
- Charles Shapu, R.; Ismail, S.; Ahmad, N.; Ying, L.P.; Abubakar Njodi, I. Knowledge, Attitude, and Practice of Adolescent Girls towards Reducing Malnutrition in Maiduguri Metropolitan Council, Borno State, Nigeria: Cross-Sectional Study. Nutrients 2020, 12, 1681. [Google Scholar] [CrossRef] [PubMed]
- Wallace, L.J.; Summerlee, A.J.; Dewey, C.E.; Hak, C.; Hall, A.; Charles, C.V. Women’s nutrient intakes and food-related knowledge in rural Kandal province, Cambodia. Asia Pac. J. Clin. Nutr. 2014, 23, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Conti, M.V.; Campanaro, A.; Coccetti, P.; De Giuseppe, R.; Galimberti, A.; Labra, M.; Cena, H. Potential role of neglected and underutilized plant species in improving women’s empowerment and nutrition in areas of sub-Saharan Africa. Nutr. Rev. 2019, 77, 817–828. [Google Scholar] [CrossRef] [PubMed]
- Conti, M.V.; Gnesi, M.; De Giuseppe, R.; Cena, H. The development of a food knowledge questionnaire for tanzanian women of childbearing age. Nutrition 2021, 90, 111218. [Google Scholar] [CrossRef] [PubMed]
- Save the Children. Changing the Story (of the Nigerian Child). 2016. Available online: https://nigeria.savethechildren.net/sites/nigeria.savethechildren.net/files/library/Changing%20the%20story%20of%20the%20Nigerian%20Girl%20Child.pdf (accessed on 12 October 2021).
- Headey, D.; Heidkamp, R.; Osendarp, S.; Ruel, M.; Scott, N.; Black, R.; Shekar, M.; Bouis, H.; Flory, A.; Haddad, L.; et al. Standing Together for Nutrition consortium. Impacts of COVID-19 on childhood malnutrition and nutrition-related mortality. Lancet 2020, 396, 519–521. [Google Scholar] [CrossRef]
- Parmenter, K.; Wardle, J. Development of a general nutrition knowledge questionnaire for adults. Eur. J. Clin. Nutr. 1999, 53, 298–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bukenya, R.; Ahmed, A.; Andrade, J.M.; Grigsby-Toussaint, D.S.; Muyonga, J.; Andrade, J.E. Validity and reliability of general nutrition knowledge questionnaire for adults in Uganda. Nutrients 2017, 9, 172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Process of Translation and Adaptation of Instruments. 2016. Available online: http://www.who.int/substance_abuse/research_tools/translation/en/ (accessed on 30 October 2016).
- Oikos East Africa. Available online: https://www.istituto-oikos.org/tanzania-en (accessed on 12 October 2021).
- Available online: https://www.opendatakit.org/ (accessed on 12 October 2021).
- StataCorp. Stata Statistical Software: Release 13; StataCorp: College Station, TX, USA, 2013. [Google Scholar]
- Kline, P. Handbook of Psychological Testing; Routledge: Abingdon, UK, 2013. [Google Scholar]
- Conti, M.V.; De Giuseppe, R.; Monti, M.C.; Mkindi, A.G.; Mshanga, N.H.; Ceppi, S.; Msuya, J.; Cena, H. Indigenous vegetables: A sustainable approach to improve micronutrient adequacy in Tanzanian women of childbearing age. Eur. J. Clin. Nutr. 2021, 75, 1475–1482. [Google Scholar] [CrossRef] [PubMed]
- Öztürk, H.N.; Türker, P.F. Fetal programming: Could intrauterin life affect health status in adulthood? Obstet. Gynecol. Sci. 2021, 64, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Global Nutrition Report 2021. Available online: https://globalnutritionreport.org/resources/nutrition-profiles/africa/eastern-africa/united-republic-tanzania/ (accessed on 12 October 2021).
- Tanzania Food and Nutrition Center. Tanzania Assessment for Scaling Up Nutrition. 2012. Available online: https://www.who.int/nutrition/landscape_analysis/TanzaniaLandscapeAnalysisFinalReport.pdf (accessed on 12 October 2021).

{kind=link}
{kind=link}
| Age in years, mean (SD) | 33.9 (10.9) | |
| Marital status, n (%) | Married | 472 (70.3%) |
| Single | 106 (15.8%) | |
| Widowed | 47 (7.0%) | |
| Partnered | 32 (4.8%) | |
| Divorced | 14 (2.1%) | |
| Religion, n (%) | Christian | 413 (61.6%) |
| Muslim | 258 (38.6%) | |
| Education, n (%) | None | 35 (5.2%) |
| Primary schooling | 331 (49.3%) | |
| Secondary schooling | 200 (29.8%) | |
| High school | 18 (2.7%) | |
| Tertiary schooling/technical | 26 (3.9%) | |
| Diploma | 36 (5.4%) | |
| Graduate | 14 (2.1%) | |
| Postgraduate | 11 (1.6%) | |
| Nutrition-related qualification (yes), n (%) | 16 (2.4%) | |
| Work activity (yes), n (%) | 443 (66.0%) | |
| Number of children, median (IQR) | 2 (2) | |
| Disabled persons in the family (yes), n (%) | 30 (4.5%) | |
| Monthly income in TZS (individual), median (IQR) | 100,000 (150,000) | |
| Monthly income in TZS (family), median (IQR) | 250,000 (250,000) | |
| Weekly expenditure for food in TZS, median (IQR) | 30,000 (20,000) | |
| Control of food expenditure, n (%) | Mother | 445 (66.3%) |
| Father | 132 (19.7%) | |
| Children | 13 (1.9%) | |
| Mother and father | 76 (11.3%) | |
| Mother and children | 4 (0.6%) | |
| Other | 1 (0.2%) | |
| Currently on a diet (yes), n (%) | 91 (13.6%) | |
| Section | Item | Wrong, n (%) | Not Sure, n (%) | Correct, n (%) | Note |
|---|---|---|---|---|---|
| B | 1A | 313 (46.7%) | 45 (6.7%) | 313 (46.7%) | |
| 1B | 49 (7.3%) | 14 (2.1%) | 608 (90.6%) | DES+/MCA | |
| 1C | 88 (13.1%) | 48 (7.2%) | 535 (79.7%) | ||
| 2 | 108 (16.1%) | 77 (11.5%) | 486 (72.4%) | ||
| 3 | 78 (11.6%) | 63 (9.4%) | 530 (79.0%) | ||
| 4A | 118 (17.6%) | 49 (7.3%) | 504 (75.1%) | ||
| 4B | 212 (31.6%) | 59 (8.8%) | 400 (59.6%) | EFA | |
| 4C | 122 (18.2%) | 105 (15.7%) | 444 (66.2%) | ||
| 4D | 258 (38.5%) | 43 (6.4%) | 370 (55.1%) | EFA | |
| 5A | 221 (32.9%) | 85 (12.7%) | 365 (54.4%) | MCA | |
| 5B | 332 (49.5%) | 126 (18.8%) | 213 (31.7%) | EFA | |
| 5C | 145 (21.6%) | 157 (23.4%) | 369 (55.0%) | MCA | |
| 5D | 169 (25.2%) | 144 (21.5%) | 358 (53.4%) | MCA | |
| C1 | 1A | 478 (71.2%) | 14 (2.1%) | 179 (26.7%) | |
| 1B | 48 (7.2%) | 25 (3.7%) | 598 (89.1%) | ||
| 1C | 168 (25.0%) | 34 (5.1%) | 469 (69.9%) | ||
| 1D | 131 (19.5%) | 16 (2.4%) | 524 (78.1%) | MCA | |
| 1E | 31 (4.6%) | 6 (0.9%) | 634 (94.5%) | DES+ | |
| 2A | 279 (41.6%) | 14 (2.1%) | 378 (56.3%) | MCA | |
| 2B | 38 (5.7%) | 21 (3.1%) | 612 (91.2%) | DES+ | |
| 2C | 300 (44.7%) | 210 (31.3%) | 161 (24.0%) | EFA | |
| 2D | 38 (5.7%) | 115 (17.1%) | 518 (77.2%) | ||
| 2E | 71 (10.6%) | 37 (5.5%) | 563 (83.9%) | ||
| 2F | 40 (6.0%) | 20 (3.0%) | 611 (91.1%) | DES+ | |
| 2G | 46 (6.9%) | 72 (10.7%) | 553 (82.4%) | EFA | |
| 2H | 35 (5.2%) | 75 (11.2%) | 561 (83.6%) | EFA | |
| 3A | 104 (15.5%) | 71 (10.6%) | 496 (73.9%) | ||
| 3B | 65 (9.7%) | 21 (3.1%) | 585 (87.2%) | DES+ | |
| 3C | 272 (40.5%) | 66 (9.8%) | 333 (49.6%) | ||
| 3D | 111 (16.5%) | 67 (10.0%) | 493 (73.5%) | ||
| 3E | 37 (5.5%) | 23 (3.4%) | 611 (91.1%) | DES+ | |
| 3F | 159 (23.7%) | 185 (27.6%) | 327 (48.7%) | (MCA) | |
| 4A | 301 (44.9%) | 237 (35.3%) | 133 (19.8%) | MCA | |
| 4B | 135 (20.1%) | 14 (2.1%) | 522 (77.8%) | ||
| 4C | 170 (25.3%) | 43 (6.4%) | 458 (68.3%) | MCA | |
| 4D | 33 (4.9%) | 17 (2.5%) | 621 (92.6%) | DES+ | |
| 4E | 22 (3.3%) | 11 (1.6%) | 638 (95.1%) | DES+ | |
| 4F | 70 (10.4%) | 98 (14.6%) | 503 (75.0%) | ||
| 4G | 386 (57.5%) | 20 (3.0%) | 265 (39.5%) | MCA | |
| 5A | 142 (21.2%) | 111 (16.5%) | 418 (62.3%) | ||
| 5B | 64 (9.5%) | 38 (5.7%) | 569 (84.8%) | MCA | |
| 5C | 208 (31.0%) | 43 (6.4%) | 420 (62.6%) | ||
| 5D | 122 (18.2%) | 93 (13.9%) | 456 (68.0%) | ||
| 5E | 44 (6.6%) | 27 (4.0%) | 600 (49.4%) | DES+ | |
| 5F | 290 (43.2%) | 62 (9.2%) | 319 (47.5%) | ||
| 6A | 21 (3.1%) | 31 (4.6%) | 619 (92.3%) | DES+ | |
| 6B | 326 (48.6%) | 36 (5.4%) | 309 (46.1%) | MCA | |
| 6C | 23 (3.4%) | 37 (5.5%) | 611 (91.1%) | (DES+) | |
| 6D | 192 (28.6%) | 35 (5.2%) | 444 (66.2%) | ||
| 6E | 153 (22.8%) | 45 (6.7%) | 473 (70.5%) | MCA | |
| 6F | 46 (6.9%) | 39 (5.8%) | 586 (87.3%) | (DES+) | |
| 6G | 73 (10.9%) | 35 (5.2%) | 563 (83.9%) | ||
| 6H | 392 (58.4%) | 36 (5.4%) | 243 (36.2%) | EFA | |
| 6I | 138 (20.6%) | 49 (7.3%) | 484 (72.1%) | ||
| 6L | 74 (11.0%) | 17 (2.5%) | 580 (86.4%) | DES+ | |
| 7A | 139 (20.7%) | 60 (8.9%) | 472 (70.3%) | ||
| 7B | 325 (48.4%) | 183 (27.3%) | 163 (24.3%) | EFA | |
| 7C | 142 (21.2%) | 32 (4.8%) | 497 (74.1%) | MCA | |
| 7D | 209 (31.2%) | 47 (7.0%) | 415 (61.9%) | ||
| 7E | 224 (33.4%) | 75 (11.2%) | 372 (55.4%) | MCA | |
| 7F | 79 (11.8%) | 41 (6.1%) | 551 (82.1%) | ||
| C2 | 1 | 63 (9.4%) | 18 (2.7%) | 590 (87.9%) | (DES+) |
| 2 | 401 (59.8%) | 74 (11.0%) | 196 (29.2%) | EFA | |
| 3 | 139 (20.7%) | 105 (15.7%) | 427 (63.6%) | ||
| 4 | 365 (54.4%) | 140 (20.9%) | 166 (24.7%) | EFA | |
| 5 | 109 (16.2%) | 253 (37.7%) | 309 (46.1%) | EFA | |
| 6 | 259 (38.6%) | 191 (28.5%) | 221 (32.9%) | EFA | |
| D | 1A | 83 (12.4%) | 117 (17.4%) | 471 (70.2%) | EFA |
| 1B | 242 (36.1%) | 111 (16.5%) | 318 (47.4%) | ||
| 1C | 259 (38.6%) | 184 (27.4%) | 228 (34.0%) | ||
| 2A | 178 (26.5%) | 30 (4.5%) | 463 (69.0%) | MCA | |
| 2B | 6 (0.9%) | 21 (3.1%) | 644 (96.0%) | DES+ | |
| 2C | 16 (2.4%) | 227 (33.8%) | 428 (63.8%) | EFA | |
| 3A | 135 (20.1%) | 75 (11.2%) | 461 (68.7%) | MCA | |
| 3B | 112 (16.7%) | 200 (29.8%) | 359 (53.5%) | ||
| 3C | 110 (16.4%) | 127 (18.9%) | 434 (64.7%) | ||
| 4A | 125 (18.6%) | 152 (22.7%) | 394 (85.7%) | ||
| 4B | 213 (31.7%) | 149 (22.2%) | 309 (46.1%) | ||
| 4C | 226 (33.7%) | 147 (21.9%) | 298 (44.4%) | ||
| 4D | 107 (16.0%) | 99 (14.8%) | 465 (69.3%) | ||
| 4E | 88 (13.1%) | 102 (15.2%) | 481 (71.7%) | ||
| 5A | 144 (21.5%) | 104 (15.5%) | 423 (63.0%) | ||
| 5B | 67 (10.0%) | 74 (11.0%) | 530 (79.0%) | ||
| 5C | 102 (15.2%) | 68 (10.1%) | 501 (74.7%) | ||
| 6A | 79 (11.8%) | 66 (9.8%) | 526 (78.4%) | EFA | |
| 6B | 80 (11.9%) | 65 (9.7%) | 526 (78.4%) | EFA | |
| 6C | 89 (13.3%) | 72 (10.7%) | 510 (76.0%) | EFA | |
| 6D | 84 (12.5%) | 79 (11.8%) | 508 (75.7%) | EFA |
| Factor | Item ID (Former) | Item ID (Final) | Factor Loading | Uniqueness | ||
|---|---|---|---|---|---|---|
| Section | Item | Section | Item | |||
| B (Explained Variance: 48.1%) | B | 1A | B | 1A | 0.609 | 0.629 |
| B | 1C | B | 1B | 0.641 | 0.589 | |
| B | 2 | B | 2B | 0.685 | 0.531 | |
| B | 3 | B | 3B | 0.776 | 0.398 | |
| B | 4A | B | 4A | 0.679 | 0.539 | |
| B | 4C | B | 4B | 0.755 | 0.430 | |
| C (Explained Variance: 55.2%) | C | 1A | C | 1A | 0.676 | 0.543 |
| C | 1B | C | 1B | 0.737 | 0.457 | |
| C | 1C | C | 1C | 0.810 | 0.344 | |
| D (Explained Variance: 61.5%) | C1 | 5A | D | 1A | 0.827 | 0.316 |
| C1 | 5C | D | 1B | 0.826 | 0.318 | |
| C1 | 5D | D | 1C | 0.609 | 0.630 | |
| C1 | 5F | D | 1D | 0.850 | 0.277 | |
| E (Explained Variance: 69.6%) | C1 | 6D | E | 1A | 0.818 | 0.332 |
| C1 | 6F | E | 1B | 0.728 | 0.469 | |
| C1 | 6G | E | 1C | 0.900 | 0.190 | |
| C1 | 6I | E | 1D | 0.881 | 0.225 | |
| F (Explained Variance: 50.5%) | D | 3B | F | 1A | 0.804 | 0.654 |
| D | 3C | F | 1B | 0.724 | 0.475 | |
| C1 | 4B | F | 2A | 0.693 | 0.520 | |
| C1 | 4F | F | 2B | 0.609 | 0.629 | |
| G (Explained Variance: 61.4%) | C1 | 3A | G | 1A | 0.755 | 0.430 |
| C1 | 3C | G | 1B | 0.774 | 0.401 | |
| C1 | 3D | G | 1C | 0.843 | 0.290 | |
| C1 | 7A | G | 2A | 0.799 | 0.362 | |
| C1 | 7D | G | 2B | 0.725 | 0.475 | |
| C1 | 7F | G | 2C | 0.799 | 0.362 | |
| H (Explained Variance: 54.8%) | C1 | 2D | H | 1A | 0.630 | 0.603 |
| C1 | 2E | H | 1B | 0.833 | 0.307 | |
| C1 | 6C | H | 2A | 0.745 | 0.445 | |
| I (Explained Variance: 45.6%) | C2 | 1 | I | 1 | 0.753 | 0.434 |
| C2 | 3 | I | 2 | 0.751 | 0.436 | |
| C1 | 3F | I | 3A | 0.488 | 0.762 | |
| L (Explained Variance: 59.1%) | D | 1B | L | 1A | 0.655 | 0.571 |
| D | 1C | L | 1B | 0.732 | 0.464 | |
| D | 4A | L | 1C | 0.848 | 0.281 | |
| D | 4B | L | 1D | 0.758 | 0.426 | |
| D | 4C | L | 1E | 0.785 | 0.383 | |
| D | 4D | L | 2A | 0.877 | 0.231 | |
| D | 4E | L | 2B | 0.687 | 0.528 | |
| D | 5A | L | 2C | 0.780 | 0.392 | |
| D | 5B | L | 0.718 | 0.485 | ||
| D | 5C | L | 0.817 | 0.332 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conti, M.V.; Gnesi, M.; De Giuseppe, R.; Giampieri, F.; Monti, M.C.; Mshanga, N.; Kinabo, J.; Msuya, J.; Cena, H. Validation of a Food Knowledge Questionnaire on Tanzanian Women of Childbearing Age. Nutrients 2022, 14, 691. https://doi.org/10.3390/nu14030691
Conti MV, Gnesi M, De Giuseppe R, Giampieri F, Monti MC, Mshanga N, Kinabo J, Msuya J, Cena H. Validation of a Food Knowledge Questionnaire on Tanzanian Women of Childbearing Age. Nutrients. 2022; 14(3):691. https://doi.org/10.3390/nu14030691
Chicago/Turabian StyleConti, Maria Vittoria, Marco Gnesi, Rachele De Giuseppe, Francesca Giampieri, Maria Cristina Monti, Naelijwa Mshanga, Joyce Kinabo, John Msuya, and Hellas Cena. 2022. "Validation of a Food Knowledge Questionnaire on Tanzanian Women of Childbearing Age" Nutrients 14, no. 3: 691. https://doi.org/10.3390/nu14030691
APA StyleConti, M. V., Gnesi, M., De Giuseppe, R., Giampieri, F., Monti, M. C., Mshanga, N., Kinabo, J., Msuya, J., & Cena, H. (2022). Validation of a Food Knowledge Questionnaire on Tanzanian Women of Childbearing Age. Nutrients, 14(3), 691. https://doi.org/10.3390/nu14030691