
Effects of 8-Week Online, Supervised High-Intensity Interval Training on the Parameters Related to the Anaerobic Threshold, Body Weight, and Body Composition during Pregnancy: A Randomized Controlled Trial

 ,
,  ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
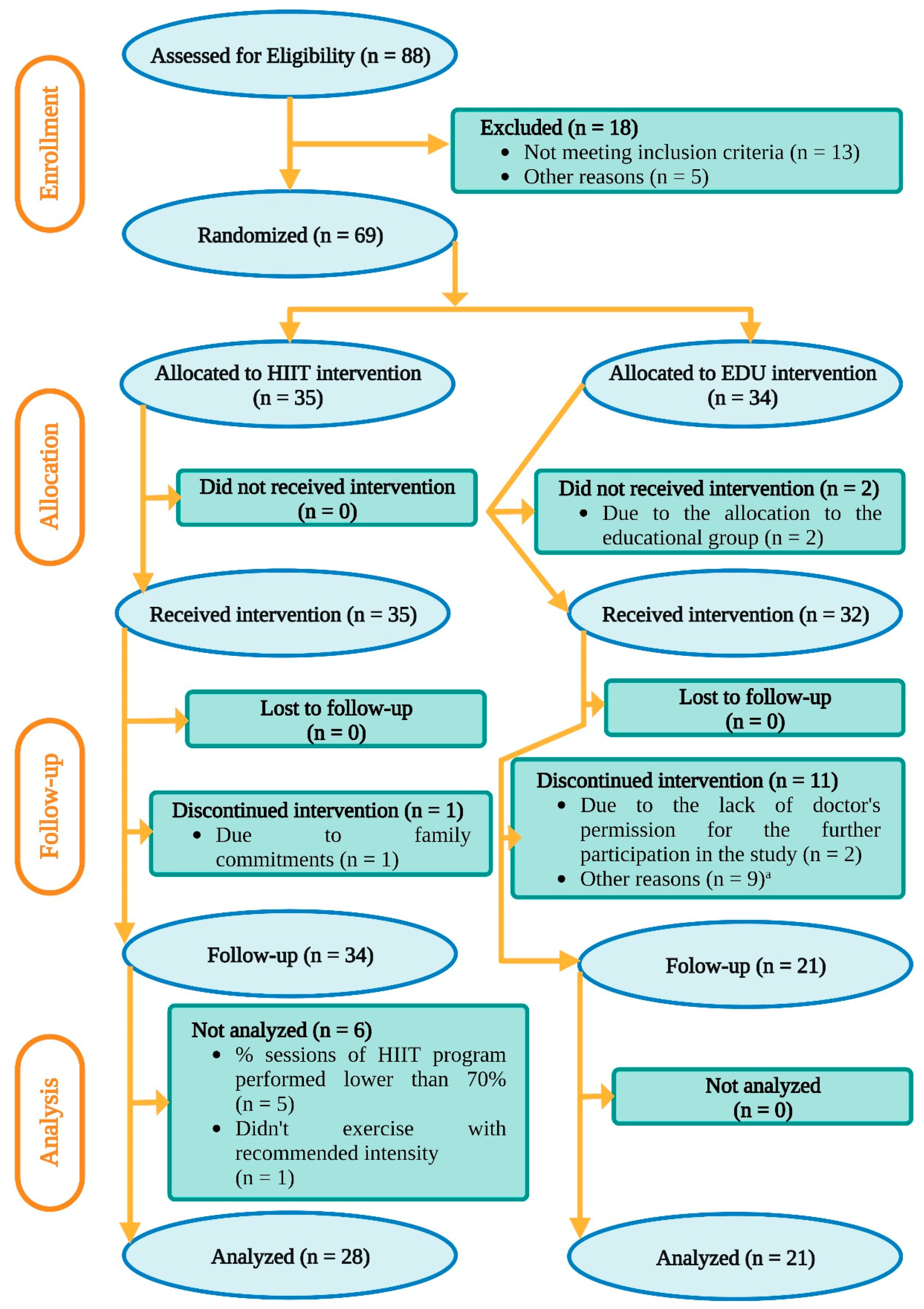
2.1. Ethics, Recruitment, and Flow of the Participants through the Study
2.2. Cardiopulmonary Exercise Test
2.3. Body Composition
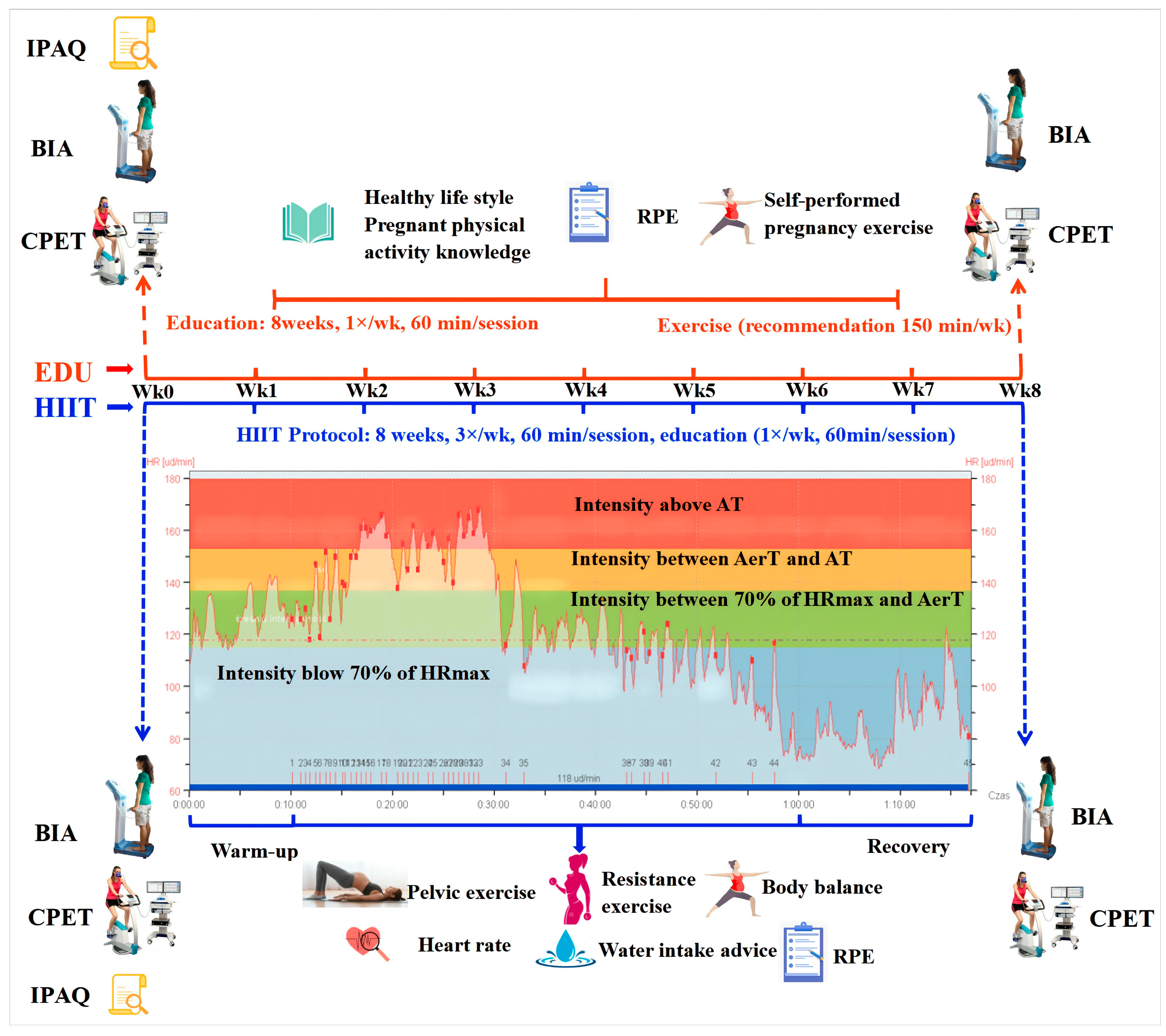
2.4. High-Intensity Interval Training
2.5. Statistical Analysis
3. Results
3.1. Parameters Related to the Anaerobic Threshold
3.2. Body Composition
3.3. Relationship of the Body Composition and the Parameters Related to the Anaerobic Threshold with the Intervention Characteristics
4. Discussion
4.1. Parameters Related to the Anaerobic Threshold
4.2. Body Weight and Composition
4.3. Correlation of the Changes in the Parameters Related to the Anaerobic Threshold and Body Composition with the Characteristics of the Exercise Intervention
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thoma, M.E.; Declercq, E.R. All-Cause maternal mortality in the US Before vs during the COVID-19 pandemic. JAMA Netw Open 2022, 5, e2219133. [Google Scholar] [CrossRef] [PubMed]
- Wolff, D.; Nee, S.; Hickey, N.S.; Marschollek, M. Risk factors for Covid-19 severity and fatality: A structured literature review. Infection 2021, 49, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Salvadori, A.; Fanari, P.; Marzullo, P.; Codecasa, F.; Tovaglieri, I.; Cornacchia, M.; Terruzzi, I.; Ferrulli, A.; Palmulli, P.; Brunani, A.; et al. Playing around the anaerobic threshold during COVID-19 pandemic: Advantages and disadvantages of adding bouts of anaerobic work to aerobic activity in physical treatment of individuals with obesity. Acta Diabetol. 2021, 58, 1329–1341. [Google Scholar] [CrossRef] [PubMed]
- Wasserman, K. The anaerobic threshold: Definition, physiological significance and identification. Adv. Cardiol. 1986, 35, 1–23. [Google Scholar] [PubMed]
- Snowden, C.P.; Prentis, J.M.; Anderson, H.L.; Roberts, D.R.; Randles, D.; Renton, M.; Manas, D.M. Submaximal cardiopulmonary exercise testing predicts complications and hospital length of stay in patients undergoing major elective surgery. Ann. Surg. 2010, 251, 535–541. [Google Scholar] [CrossRef]
- Henriksson, P.; Sandborg, J.; Söderström, E.; Leppänen, M.H.; Snekkenes, V.; Blomberg, M.; Ortega, F.B.; Löf, M. Associations of body composition and physical fitness with gestational diabetes and cardiovascular health in pregnancy: Results from the HealthyMoms trial. Nutr. Diabetes 2021, 11, 16. [Google Scholar] [CrossRef]
- Cai, C.; Ruchat, S.M.; Sivak, A.; Davenport, M.H. Prenatal exercise and cardiorespiratory health and fitness: A meta-analysis. Med. Sci. Sports Exerc. 2020, 52, 1538–1548. [Google Scholar] [CrossRef]
- Ahmadi, M.N.; Lee, I.M.; Hamer, M.; del Pozo Cruz, B.; Chen, L.J.; Eroglu, E.; Lai, Y.-J.; Ku, P.W.; Stamatakis, E. Changes in physical activity and adiposity with all-cause, cardiovascular disease, and cancer mortality. Int. J. Obes. 2022, 46, 1849–1858. [Google Scholar] [CrossRef]
- Davenport, M.H.; Ruchat, S.-M.; Poitras, V.J.; Jaramillo Garcia, A.; Gray, C.E.; Barrowman, N.; Skow, R.J.; Meah, V.L.; Riske, L.; Sobierajski, F.; et al. Prenatal exercise for the prevention of gestational diabetes mellitus and hypertensive disorders of pregnancy: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1367. [Google Scholar] [CrossRef]
- Morales-Suárez-Varela, M.; Clemente-Bosch, E.; Peraita-Costa, I.; Llopis-Morales, A.; Martínez, I.; Llopis-González, A. Maternal physical activity during pregnancy and the effect on the mother and newborn: A systematic review. J. Phys. Act. Health 2021, 18, 130–147. [Google Scholar] [CrossRef]
- de Castro, R.; Antunes, R.; Mendes, D.; Szumilewicz, A.; Santos-Rocha, R. Can group exercise programs iImprove health outcomes in pregnant women? An updated systematic review. Int. J. Environ. Res. Public Health 2022, 19, 4875. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; He, J.; Szumilewicz, A. Pregnancy activity levels and impediments in the era of COVID-19 based on the health belief model: A cross-sectional study. Int. J. Environ. Res. Public Health 2022, 19, 3283. [Google Scholar] [CrossRef] [PubMed]
- Szumilewicz, A.; Worska, A.; Santos-Rocha, R.; Oviedo-Caro, M.Á. Evidence-based and practice-oriented guidelines for exercising during pregnancy. In Exercise and Sporting Activity During Pregnancy: Evidence-Based Guidelines; Santos-Rocha, R., Ed.; Springer International Publishing: Cham, Germany, 2022; pp. 157–181, 231–308, 275–361. [Google Scholar]
- Szumilewicz, A.; Santos-Rocha, R.; Worska, A.; Piernicka, M.; Yu, H.; Pajaujiene, S.; Shojaeian, N.; Oviedo Caro, M. How to HIIT while pregnant? The protocols characteristics and effects of high intensity interval training implemented during pregnancy—A systematic review. Balt J. Health Phy. Act. 2022, 14, 1–16. [Google Scholar] [CrossRef]
- Davenport, M.H.; Ruchat, S.-M.; Sobierajski, F.; Poitras, V.J.; Gray, C.E.; Yoo, C.; Skow, R.J.; Jaramillo Garcia, A.; Barrowman, N.; Meah, V.L.; et al. Impact of prenatal exercise on maternal harms, labour and delivery outcomes: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 53, 99. [Google Scholar] [CrossRef]
- Wowdzia, J.B.; McHugh, T.L.; Thornton, J.; Sivak, A.; Mottola, M.F.; Davenport, M.H. Elite athletes and pregnancy outcomes: A systematic review and meta-analysis. Med. Sci. Sports Exerc. 2021, 53, 534–542. [Google Scholar] [CrossRef]
- Pivarnik, J.M.; Ayres, N.A.; Mauer, M.B.; Cotton, D.B.; Kirshon, B.; Dildy, G.A. Effects of maternal aerobic fitness on cardiorespiratory responses to exercise. Med. Sci. Sports Exerc. 1993, 25, 993–998. [Google Scholar] [CrossRef]
- Feito, Y.; Heinrich, K.M.; Butcher, S.J.; Poston, W.S.C. High-intensity functional training (HIFT): Definition and research implications for improved fitness. Sports 2018, 6, 76. [Google Scholar] [CrossRef]
- Wu, Z.-J.; Wang, Z.-Y.; Gao, H.-E.; Zhou, X.-F.; Li, F.-H. Impact of high-intensity interval training on cardiorespiratory fitness, body composition, physical fitness, and metabolic parameters in older adults: A meta-analysis of randomized controlled trials. Exp. Gerontol. 2021, 150, 111345. [Google Scholar] [CrossRef]
- WHO Guidelines on Physical Activity and Sedentary Behaviour. Available online: https://www.who.int/publications/i/item/9789240015111 (accessed on 25 November 2020).
- Mottola, M.F.; Davenport, M.H.; Ruchat, S.-M.; Davies, G.A.; Poitras, V.J.; Gray, C.E.; Jaramillo Garcia, A.; Barrowman, N.; Adamo, K.B.; Duggan, M.; et al. 2019 Canadian guideline for physical activity throughout pregnancy. Br. J. Sports Med. 2018, 52, 1339. [Google Scholar] [CrossRef]
- DiPietro, L.; Al-Ansari, S.S.; Biddle, S.J.H.; Borodulin, K.; Bull, F.C.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; et al. Advancing the global physical activity agenda: Recommendations for future research by the 2020 WHO physical activity and sedentary behavior guidelines development group. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 143. [Google Scholar] [CrossRef]
- Mota, P.; Bø, K. ACOG Committee Opinion No. 804: Physical activity and exercise during pregnancy and the postpartum period. Obstet. Gynecol. 2021, 137, 375–376. [Google Scholar] [CrossRef] [PubMed]
- Wisløff, U.; Støylen, A.; Loennechen, J.P.; Bruvold, M.; Rognmo, Ø.; Haram, P.M.; Tjønna, A.E.; Helgerud, J.; Slørdahl, S.A.; Lee, S.J.; et al. Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients. Circulation 2007, 115, 3086–3094. [Google Scholar] [CrossRef] [PubMed]
- Devin, J.L.; Sax, A.T.; Hughes, G.I.; Jenkins, D.G.; Aitken, J.F.; Chambers, S.K.; Dunn, J.C.; Bolam, K.A.; Skinner, T.L. The influence of high-intensity compared with moderate-intensity exercise training on cardiorespiratory fitness and body composition in colorectal cancer survivors: A randomised controlled trial. J. Cancer Surviv. 2016, 10, 467–479. [Google Scholar] [CrossRef] [PubMed]
- Buckinx, F.; Gouspillou, G.; Carvalho, L.P.; Marcangeli, V.; El Hajj Boutros, G.; Dulac, M.; Noirez, P.; Morais, J.A.; Gaudreau, P.; Aubertin-Leheudre, M. Effect of high-intensity interval training combined with l-citrulline supplementation on functional capacities and muscle function in dynapenic-obese older adults. J. Clin. Med. 2018, 7, 561. [Google Scholar] [CrossRef] [PubMed]
- Nosek, B.A.; Alter, G.; Banks, G.C.; Borsboom, D.; Bowman, S.D.; Breckler, S.J.; Buck, S.; Chambers, C.D.; Chin, G.; Christensen, G.; et al. Promoting an open research culture. Science 2015, 348, 1422–1425. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sc.i Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Cheng, H.L. A simple, Easy-to-Use Spreadsheet for Automatic Scoring of the International Physical Activity Questionnaire (IPAQ) Short Form; ResearchGate: Sydney, Australia, 2016. [Google Scholar]
- Fan, M.; Lyu, J.; He, P. Guidelines for data processing and analysis of the international physical activity questionnaire (IPAQ).2005. Zhonghua Liuxingbingxue Zazhi 2014, 35, 961–964. [Google Scholar]
- Ross, R.M. ATS/ACCP statement on cardiopulmonary exercise testing. Am. J. Respir. Crit. Care Med. 2003, 167, 1451. [Google Scholar] [CrossRef]
- Beaver, W.L.; Wasserman, K.; Whipp, B.J. A new method for detecting anaerobic threshold by gas exchange. J. Appl. Physiol. 1986, 60, 2020–2027. [Google Scholar] [CrossRef]
- Baldari, C.; Guidetti, L. VO (2max,) ventilatory and anaerobic thresholds in rhythmic gymnasts and young female dancers. J. Sports Med. Phys. 2001, 41, 177. [Google Scholar]
- Emerenziani, G.P.; Gallotta, M.C.; Meucci, M.; Di Luigi, L.; Migliaccio, S.; Donini, L.M.; Strollo, F.; Guidetti, L. Effects of aerobic exercise based upon heart rate at aerobic threshold in obese elderly subjects with type 2 diabetes. Int. J. Endocrinol. 2015, 2015, 695297. [Google Scholar] [CrossRef] [PubMed]
- Skinner, J.S.; McLellan, T.H. The transition from aerobic to anaerobic metabolism. Res. Q Exerc. Sport 1980, 51, 234–248. [Google Scholar] [CrossRef] [PubMed]
- Golovin, M.S.; Aizman, R.I. Physiological and biochemical indicators of physical performance during exercise test (treadmill and bicycle ergometer). Hum. Sport Med. 2022, 22, 14–21. [Google Scholar] [CrossRef]
- McLester, C.N.; Nickerson, B.S.; Kliszczewicz, B.M.; McLester, J.R. Reliability and agreement of various inBody body composition analyzers as compared to dual-energy X-Ray absorptiometry in healthy men and women. J. Clin. Densitom. 2020, 23, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Santos-Rocha, R.; Corrales Gutiérrez, I.; Szumilewicz, A.; Pajaujiene, S. Exercise testing and prescription in pregnancy. In Exercise and Physical Activity During Pregnancy and Postpartum: Evidence-Based Guidelines; Santos-Rocha, R., Ed.; Springer International Publishing: Cham, Germany, 2022; pp. 219–274. [Google Scholar]
- Wood, G.; Murrell, A.; van der Touw, T.; Smart, N. HIIT is not superior to MICT in altering blood lipids: A systematic review and meta-analysis. BMJ Open Sport Exerc. Med. 2019, 5, e000647. [Google Scholar] [CrossRef] [PubMed]
- Borg, G. Borg’s Perceived Exertion And Pain Scales; Human Kinetics: Champaign, IL, USA, 1998. [Google Scholar]
- Persinger, R.; Foster, C.; Gibson, M.; Fater, D.C.; Porcari, J.P. Consistency of the talk test for exercise prescription. Med. Sci. Sports Exerc. 2004, 36, 1632–1636. [Google Scholar]
- Santos-Rocha, R.; Szumilewicz, A.; Perales, M.; Pajaujiene, S. Pregnancy and Postnatal Exercise Specialist EuropeActive Standards EQF Level 5; EuropeActive: Brussels, Belgium, 2016. [Google Scholar]
- Szumilewicz, A.; Arntzen, A.; Bogdanova, A.; Harrison, M.; Huffen, C.; Kingsbury, D.; Pajaujiene, S.; Pratt, B.; Santos Rocha, R.; Silva, D. “Online Provision of Fitness Services” Lifelong Learning Qualification (EQF Level 3); EuropeActive: Brussels, Belgium, 2021. [Google Scholar]
- Szumilewicz, A.; Kuchta, A.; Kranich, M.; Dornowski, M.; Jastrzębski, Z. Prenatal high-low impact exercise program supported by pelvic floor muscle education and training decreases the life impact of postnatal urinary incontinence: A quasiexperimental trial. Medicine 2020, 99, e18874. [Google Scholar] [CrossRef]
- Sloth, M.; Sloth, D.; Overgaard, K.; Dalgas, U. Effects of sprint interval training on VO2max and aerobic exercise performance: A systematic review and meta-analysis. Scand J. Med. Sci. Sports 2013, 23, e341–e352. [Google Scholar] [CrossRef]
- Boereboom, C.L.; Phillips, B.E.; Williams, J.P.; Lund, J.N. A 31-day time to surgery compliant exercise training programme improves aerobic health in the elderly. Tech. Coloproctology 2016, 20, 375–382. [Google Scholar] [CrossRef]
- Soma-Pillay, P.; Nelson-Piercy, C.; Tolppanen, H.; Mebazaa, A. Physiological changes in pregnancy. Cardiovasc. J. Afr. 2016, 27, 89–94. [Google Scholar] [CrossRef]
- Melzer, K.; Schutz, Y.; Boulvain, M.; Kayser, B. Physical activity and pregnancy: Cardiovascular adaptations, recommendations and pregnancy outcomes. Sports Med. 2010, 40, 493–507. [Google Scholar] [CrossRef] [PubMed]
- Ong, M.J.; Wallman, K.E.; Fournier, P.A.; Newnham, J.P.; Guelfi, K.J. Enhancing energy expenditure and enjoyment of exercise during pregnancy through the addition of brief higher intensity intervals to traditional continuous moderate intensity cycling. BMC Pregnancy Childbirth 2016, 16, 161. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine; National Research Council (US) Committee to Reexamine IOM Pregnancy Weight Guidelines. The National Academies Collection: Reports funded by National Institutes of Health. In Weight Gain During Pregnancy: Reexamining the Guidelines; Rasmussen, K.M., Yaktine, A.L., Eds.; National Academies Press (US), National Academy of Sciences: Washington, DC, USA, 2009. [Google Scholar]
- Larciprete, G.; Valensise, H.; Vasapollo, B.; Altomare, F.; Sorge, R.; Casalino, B.; De Lorenzo, A.; Arduini, D. Body composition during normalpregnancy: Reference ranges. Acta Diabetol. 2003, 40, s225–s232. [Google Scholar] [CrossRef] [PubMed]
- Merkx, A.; Ausems, M.; Budé, L.; de Vries, R.; Nieuwenhuijze, M.J. Weight gain in healthy pregnant women in relation to pre-pregnancy BMI, diet and physical activity. Midwifery 2015, 31, 693–701. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Rexrode, K.M.; van Dam, R.M.; Li, T.Y.; Hu, F.B. Abdominal Obesity and the Risk of All-Cause, Cardiovascular, and Cancer Mortality. Circulation 2008, 117, 1658–1667. [Google Scholar] [CrossRef]
- Sahakyan, K.R.; Somers, V.K.; Rodriguez-Escudero, J.P.; Hodge, D.O.; Carter, R.E.; Sochor, O.; Coutinho, T.; Jensen, M.D.; Roger, V.L.; Singh, P.; et al. Normal-weight central obesity: Implications for total and cardiovascular mortality. Ann. Intern. Med. 2015, 163, 827–835. [Google Scholar] [CrossRef]
- Snijder, M.B.; Dekker, J.M.; Visser, M.; Bouter, L.M.; Stehouwer, C.D.A.; Yudkin, J.S.; Heine, R.J.; Nijpels, G.; Seidell, J.C. Trunk fat and leg fat have independent and opposite associations with fasting and postload glucose levels: The hoorn study. Diabetes Care 2004, 27, 372–377. [Google Scholar] [CrossRef]
- Yu, H.; He, J.; Wang, X.; Yang, W.; Sun, B.; Szumilewicz, A. A comparison of functional features of Chinese and US mobile apps for pregnancy and postnatal care: A systematic app store search and content analysis. Public Health Front. 2022, 10, 1–12. [Google Scholar] [CrossRef]
- Martin-Arias, A.; Brik, M.; Vargas-Terrones, M.; Barakat, R.; Santacruz, B. Predictive factors of compliance with a program of supervised exercise during pregnancy. Acta Obstet Gynecol. Scand. 2019, 98, 807–808. [Google Scholar] [CrossRef]
- Wackerhage, H.; Gehlert, S.; Schulz, H.; Weber, S.; Ring-Dimitriou, S.; Heine, O. Lactate thresholds and the simulation of human energy metabolism: Contributions by the cologne sports medicine group in the 1970s and 1980s. Front. Physiol. 2022, 13, 899670. [Google Scholar] [CrossRef]
- Anderson, J.; Pudwell, J.; McAuslan, C.; Barr, L.; Kehoe, J.; Davies, G.A. Acute fetal response to high-intensity interval training in the second and third trimesters of pregnancy. Appl. Physiol. Nutr. Metab. 2021, 46, 1552–1558. [Google Scholar] [CrossRef] [PubMed]
- Halse, R.E.; Wallman, K.E.; Dimmock, J.A.; Newnham, J.P.; Guelfi, K.J. Home-Based Exercise Improves Fitness and Exercise Attitude and Intention in Women with GDM. Med. Sci. Sports Exerc. 2015, 47, 1698–1704. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M.; Frederick, C.M.; Lepes, D.; Rubio, N.; Sheldon, K.M. Intrinsic motivation and exercise adherence. Int. J. Sport Psychol. 1997, 28, 335–354. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| The Characteristics of HIIT Intervention | |||||
|---|---|---|---|---|---|
| Week Number | Time of Workout Interval (s) | Time of Rest Interval (s) | Number of Sets (Workout + Rest Intervals) | Time between Sets (s) | Number of Cycles (Exercises) |
| Week 1 | 30 | 60 | 4 | 60 | 4 |
| Week 2 | 30 | 60 | 4 | 30 | 4 |
| Week 3 | 45 | 45 | 4 | 60 | 4 |
| Week 4 | 45 | 45 | 4 | 45 | 4 |
| Week 5 | 45 | 45 | 4 | 30 | 4 |
| Week 6 | 30 | 30 | 4 | 60 | 4 |
| Week 7 | 30 | 30 | 4 | 30 | 4 |
| Week 8 | 30 | 15 | 4 | 30 | 4 |
| Parameters Related to the Anaerobic Threshold at Baseline | Group (Mean ± SD 6) | |||
|---|---|---|---|---|
| EDU 2 (n = 21) | HIIT 3 (n = 28) | p | Cohen’s f | |
| HR/AT 1 (beat⸳min−1) | 151 ± 10 | 153 ± 9 | 0.56 | 0.09 |
| Time between the HR/AerT 4 and HR/AT 5 (s) | 92.76 ± 24.19 | 79.48 ± 29.83 | 0.10 | 0.24 |
| Time above the HR/AT (s) | 140.74 ± 52.05 | 128.07 ± 47.83 | 0.38 | 0.13 |
| VO2/AT 7 (mL⸳kg−1⸳min−1) | 19.13 ± 2.86 | 20.38 ± 2.93 | 0.14 | 0.22 |
| %VO2max/AT 8 (%) | 79.18 ± 7 | 78.96 ± 7 | 0.16 | 0.20 |
| Body Composition | Group | |||||
|---|---|---|---|---|---|---|
| EDU 2 (n = 21) | HIIT 3 (n = 28) | p | Cohen’s f | |||
| Median | Range (Min–Max) | Median | Range (Min–Max) | |||
| BMI 1 (kg⸳m−2) | 25.23 | (22.4–27.5) | 23.75 | (22.4–26.9) | 0.11 | 0.24 |
| Weight (kg) | 70.90 | (65.1–78.3) | 67.10 | (61.8–72.0) | 0.17 | 0.20 |
| %FM 5 | 32.9 | (30–40) | 30.3 | (30–30) | 0.14 | 0.22 |
| %FFM 4 | 67 | (60–70) | 70 | (70–80) | 0.14 | 0.22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, H.; Santos-Rocha, R.; Radzimiński, Ł.; Jastrzębski, Z.; Bonisławska, I.; Szwarc, A.; Szumilewicz, A. Effects of 8-Week Online, Supervised High-Intensity Interval Training on the Parameters Related to the Anaerobic Threshold, Body Weight, and Body Composition during Pregnancy: A Randomized Controlled Trial. Nutrients 2022, 14, 5279. https://doi.org/10.3390/nu14245279
Yu H, Santos-Rocha R, Radzimiński Ł, Jastrzębski Z, Bonisławska I, Szwarc A, Szumilewicz A. Effects of 8-Week Online, Supervised High-Intensity Interval Training on the Parameters Related to the Anaerobic Threshold, Body Weight, and Body Composition during Pregnancy: A Randomized Controlled Trial. Nutrients. 2022; 14(24):5279. https://doi.org/10.3390/nu14245279
Chicago/Turabian StyleYu, Hongli, Rita Santos-Rocha, Łukasz Radzimiński, Zbigniew Jastrzębski, Iwona Bonisławska, Andrzej Szwarc, and Anna Szumilewicz. 2022. "Effects of 8-Week Online, Supervised High-Intensity Interval Training on the Parameters Related to the Anaerobic Threshold, Body Weight, and Body Composition during Pregnancy: A Randomized Controlled Trial" Nutrients 14, no. 24: 5279. https://doi.org/10.3390/nu14245279
APA StyleYu, H., Santos-Rocha, R., Radzimiński, Ł., Jastrzębski, Z., Bonisławska, I., Szwarc, A., & Szumilewicz, A. (2022). Effects of 8-Week Online, Supervised High-Intensity Interval Training on the Parameters Related to the Anaerobic Threshold, Body Weight, and Body Composition during Pregnancy: A Randomized Controlled Trial. Nutrients, 14(24), 5279. https://doi.org/10.3390/nu14245279