
A Review of Food Texture Modification among Individuals with Cerebral Palsy: The Challenges among Cerebral Palsy Families
 , , ,
, , ,  ,
,  , and
, and
Abstract
1. Introduction
- Explore the challenges of individuals with CP and their caregivers when preparing modified textured food.
- Explore the components of nutrition management emphasizing food texture modification.
2. Materials and Methods
2.1. Identifying Research Questions
- What are the challenges of individuals with cerebral palsy (CP) and their caregivers when preparing modified textured food?
- What are the components of nutrition management in the recommendation of food texture modification?
2.2. Identifying Relevant Studies
2.3. Selection of Studies
2.4. Charting Information and Data from the Studies
2.5. Collating, Summarizing, and Reporting the Results
3. Results
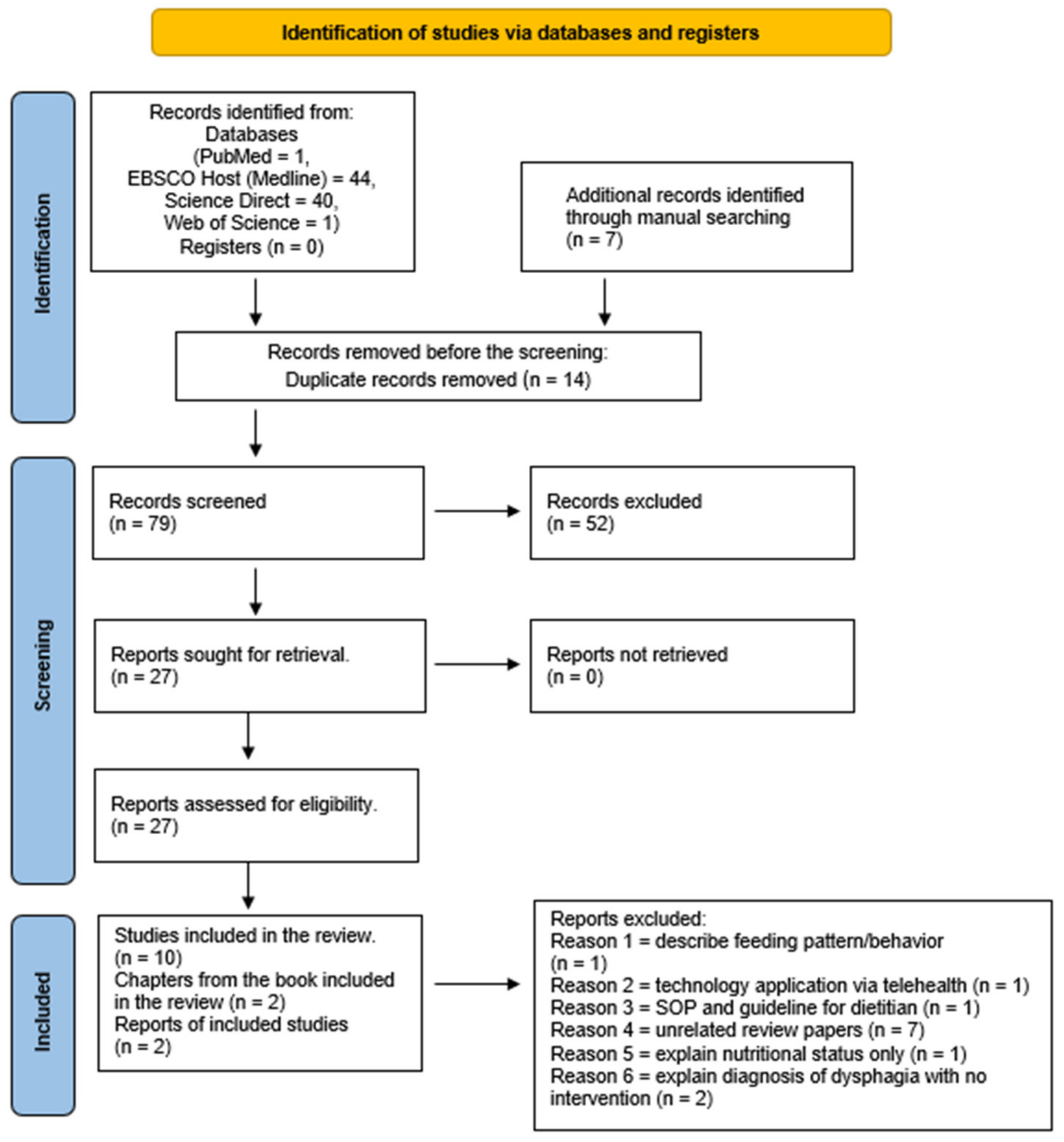
3.1. Characteristics of Selection Studies
3.2. Challenges of Feeding Problems among Individuals and Families with CP
3.3. Nutrition Intervention Focusing on Food Texture Modification
4. Discussion
4.1. Challenges of Feeding Problems among Individuals with CP
4.2. Challenges of Feeding Problems among Families with CP
4.3. Nutrition Management with Food Texture Modification
5. Conclusions
Limitations and Future Studies
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Mesh Terms from the Cochrane Database
| Cerebral Palsy | “Cerebral Palsy” OR “Monoplegic Cerebral Palsy” OR “Hypotonic Cerebral Palsy” OR “Atonic Cerebral Palsy” OR “Quadriplegic Cerebral Palsy” OR “Diplegic Cerebral Palsy” OR “Dystonic Cerebral Palsy” OR “Infantile Cerebral Palsy” OR “Congenital Cerebral Palsy” OR “Spastic Cerebral Palsy” OR “Little Disease”Textures, textured |
| Dysphagia | “Dysphagia” OR “Oropharyngeal Dysphagia” OR “Swallowing Disorders” OR “Deglutition Disorders” OR Esophageal Dysphagia” |
Appendix B. Search String Strategy
| Database | Concept | Keywords |
| PubMed | #1 | “Cerebral Palsy” OR “Spastic Cerebral Palsy” |
| #2 | “Food texture modification” OR “Food consistency modification” OR “Feeding behavior” | |
| #3 | Dysphagia OR “Swallowing Difficulties*” OR “Deglutition Disorders*” | |
| #4 | Challenges* OR Barriers* OR Practices* | |
| #1 AND #2 AND #3 AND #4 | ((“Cerebral Palsy”[All Fields] OR “Spastic Cerebral Palsy”[All Fields]) AND “loattrfull text”[Filter] AND ((“Food texture modification”[All Fields] OR ((“food”[MeSH Terms] OR “food”[All Fields]) AND (“consistence”[All Fields] OR “consistences”[All Fields] OR “consistencies”[All Fields] OR “consistency”[All Fields] OR “consistent”[All Fields] OR “consistently”[All Fields]) AND (“modification”[All Fields] OR “modifications”[All Fields])) OR “Feeding behavior”[All Fields]) AND “loattrfull text”[Filter]) AND ((“deglutition disorders”[MeSH Terms] OR (“deglutition”[All Fields] AND “disorders”[All Fields]) OR “deglutition disorders”[All Fields] OR “dysphagia”[All Fields] OR “dysphagias”[All Fields] OR “swallowing difficulties*”[All Fields] OR “deglutition disorders*”[All Fields]) AND “loattrfull text”[Filter]) AND ((“challenges*”[All Fields] OR “barriers*”[All Fields] OR “practices*”[All Fields]) AND “loattrfull text”[Filter])) AND (fft[Filter]) | |
| EBSCO Host (Medline) | (“Cerebral Palsy” OR “Spastic Cerebral Palsy” ) AND ( “Food texture modification” OR “Food consistency modification” OR “Feeding behavior”) AND (Dysphagia OR “Swallowing Difficulties*” OR “Deglutition Disorders*”) AND (Challenges* OR Barriers* OR Practices*) | |
| Science Direct | (“Cerebral Palsy”) AND (“Food texture modification” OR “Feeding behavior”) AND (Dysphagia OR “Swallowing Difficulties” OR “Deglutition Disorders”) AND (Challenges OR Barriers OR Practices) | |
| Web of Science | #1 | ALL = (“Cerebral Palsy” OR “Spastic Cerebral Palsy”) |
| #2 | ALL = (“Food texture modification” OR “Food consistency modification” OR “Feeding behavior”) | |
| #3 | ALL = (Dysphagia OR “Swallowing difficulties*” OR “Deglutition disorders*”) | |
| #4 | ALL = (Challenges* OR Barriers* OR Practices*) | |
| #1 AND #2 AND #3 | ALL = (“Cerebral Palsy” OR “Spastic Cerebral Palsy”) AND ALL = (“Food texture modification” OR “Food consistency modification” OR “Feeding behavior”) AND ALL = (Dysphagia OR “Swallowing difficulties*” OR “Deglutition disorders*”) | |
| (*) served as truncation or wild card for the variation of keywords used. | ||
References
- Morris, C. Development of the gross motor function classification system (1997). Dev. Med. Child Neurol. 2008, 50, 5. [Google Scholar] [CrossRef]
- Cans, C.; Dolk, H.; Platt, M.; Colver, A.; Prasauskiene, A.; Krkgeloh-Mann, I. Recommendations from the SCPE collaborative group for defining and classifying cerebral palsy. Dev. Med. Child Neurol. 2007, 49, 35. [Google Scholar] [CrossRef]
- McIntyre, S.; Taitz, D.; Keogh, J.; Goldsmith, S.; Badawi, N.; Blair, E. A systematic review of risk factors for cerebral palsy in children born at term in developed countries. Dev. Med. Child Neurol. 2013, 55, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Palisano, R.; Rosenbaum, P.; Walter, S.; Russell, D.; Wood, E.; Galuppi, B. Reliability of a System, Function in Children with Cerebral Palsy. Dev. Med. Child Neurol. 1997, 39, 214–223. [Google Scholar] [CrossRef] [PubMed]
- de Zabarte Fernández, J.M.M.; Arnal, I.R.; Segura, J.L.P.; Romero, R.G.; Martínez, G.R. Nutritional status of a population with moderate-severe cerebral palsy: Beyond the weight. An. Pediatría 2020, 92, 192–199. [Google Scholar] [CrossRef]
- Speyer, R.; Michou, E.; Cordier, R.; Wilkes-Gillan, S. Prevalence of drooling, swallowing, and feeding problems in cerebral palsy across the lifespan: A systematic review and meta-analyses. Dev. Med. Child Neurol. 2019, 61, 1249–1258. [Google Scholar] [CrossRef]
- Calis, E.A.; Veugelers, R.; Sheppard, J.J.; Tibboel, D.; Evenhuis, H.M.; Penning, C. Dysphagia in children with severe generalized cerebral palsy and intellectual disability. Dev. Med. Child Neurol. 2008, 50, 625–630. [Google Scholar] [CrossRef] [PubMed]
- Erasmus, C.E.; Hulst, K.; Rotteveel, J.J.; Willemsen, M.A.A.P.; Jongerius, P.H. Clinical practice: Swallowing problems in cerebral palsy. Eur. J. Pediatr. 2012, 171, 409–414. [Google Scholar] [CrossRef]
- Pavithran, J.; Puthiyottil, I.V.; Kumar, M.; Nikitha, A.V.; Vidyadharan, S.; Bhaskaran, R.; Jaya, A.C.; Thankappan, K.; Subramania, I.; Sundaram, K.R. Exploring the utility of fibreoptic endoscopic evaluation of swallowing in young children- A comparison with videofluoroscopy. Int. J. Pediatr. Otorhinolaryngol. 2020, 138, 110339. [Google Scholar] [CrossRef]
- Narawane, A.; Rappazzo, C.; Hawney, J.; Eng, J.; Ongkasuwan, J. Videofluoroscopic Swallow Study Findings and Correlations in Infancy of Children with Cerebral Palsy. Ann. Otol. Rhinol. Laryngol. 2022, 131, 478–484. [Google Scholar] [CrossRef]
- Ward, E.C.; Sharma, S.; Burns, C.; Theodoros, D.; Russell, T. Managing Patient Factors in the Assessment of Swallowing via Telerehabilitation. Int. J. Telemed. Appl. 2012, 2012, 132719. [Google Scholar] [CrossRef]
- Mustaffa Kamal, R.; Ward, E.C.; Cornwell, P.; Sharma, S. Provision of dysphagia services in a developing nation: Infrastructural challenges. Int. J. Speech Lang. Pathol. 2015, 17, 594–604. [Google Scholar] [CrossRef] [PubMed]
- Arvedson, J. Feeding children with cerebral palsy and swallowing difficulties. Eur. J. Clin. Nutr. 2013, 67 (Suppl. S2), S9–S12. [Google Scholar] [CrossRef] [PubMed]
- Sousa, K.T.D.; Ferreira, G.B.; Santos, A.T.; Nomelini, Q.S.S.; Minussi, L.O.D.A.; de Almeida Rezende, É.R.M.; Nonato, I.L. Assessment of Nutritional Status and Frequency of Complications Associated to Feeding in Patients with Spastic Quadriplegic Cerebral Palsy. Rev. Paul Pediatr. 2020, 38, e2018410. [Google Scholar] [CrossRef]
- Marques, J.M.; Sá, L. Feeding a child with cerebral palsy: Parents’ difficulties. Rev. Enferm. Ref. 2016, IV, 11–19. [Google Scholar] [CrossRef]
- Mohd Nordin, N.A.; Hui Shan, E.; Zanudin, A. The Unmet Needs of Parents of Highly Dependent Children with Cerebral Palsy. Int. J. Environ. Res. Public Health 2019, 16, 5145. [Google Scholar] [CrossRef] [PubMed]
- Grammatikopoulou, M.G.; Daskalou, E.; Tsigga, M. Diet, feeding practices, and anthropometry of children and adolescents with cerebral palsy and their siblings. Nutrition 2009, 25, 620–626. [Google Scholar] [CrossRef] [PubMed]
- Benfer, K.A.; Weir, K.A.; Boyd, R.N.; Bell, K.L.; Ware, R.S.; Davies, P.S.W. Food and fluid texture consumption in a population-based cohort of preschool children with cerebral palsy: Relationship to dietary intake. Dev. Med. Child Neurol. 2015, 57, 1056–1063. [Google Scholar] [CrossRef]
- Jaafar, N.H.; Othman, A.; Hussin, Z.; Majid, N.A.; Harith, S. Needs Assessment and Effectiveness of Integrated Nutrition Training Programme for Caregivers of Individuals with Neurological Impairments. Ph.D. Thesis, Universiti Sains Malaysia, Penang, Malaysia, 2019. [Google Scholar]
- Chen, S.T.; Soo, K.L.; Azriani, A.R.; Van Rostenberghe, H.; Sakinah, H. Nutrition Module Intervention to Improve Nutrition Knowledge, Attitude and Practice of Trainers for Persons with disabilities in rehabilitation centers in Malaysia. Int. J. Food Sci. Nutr. Diet. 2015, 5, 183–189. [Google Scholar]
- Parr, J.; Pennington, L.; Taylor, H.; Craig, D.; Morris, C.; McConachie, H.; Cadwgan, J.; Sellers, D.; Andrew, M.; Smith, J.; et al. Parent-delivered interventions used at home to improve eating, drinking and swallowing in children with neurodisability: The FEEDS mixed-methods study. Health Technol. Assess. 2021, 25, 1. [Google Scholar]
- Omar, O.M.; Khalila, M.; El-Ghanyb, H.M.A.; Abdallaha, A.M.; Omar, T.E.I. Intervention program to improve feeding, swallowing, and nutritional problems in children with cerebral palsy. Alex. J. Pediatr. 2017, 30, 85. [Google Scholar] [CrossRef]
- Shaw, C.; Moore, M.; Camel, S.; Douglas, C.C. Assessment of International Dysphagia Guidelines for use in Child Nutrition Programs. J. Child. Manag. 2019, 42, 1–13. [Google Scholar]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.; Colquhoun, H.; Kastner, M.; Levac, D.; Ng, C.; Sharpe, J.P.; Wilson, K.; et al. A scoping review on the conduct and reporting of scoping reviews. BMC Med. Res. Methodol. 2016, 16, 15. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.D.J.; Godfrey, C.; McInerney, P.; Baldini Soares, C.; Khalil, H.; Parker, D. Chapter 11: Scoping Reviews. In Joanna Briggs Institute Reviewer’s Manual; Aromataris, E., Munn, Z., Eds.; Joanna Briggs Institute: Adelaide, Australia, 2017. [Google Scholar]
- Kraus, S.; Breier, M.; Dasí-Rodríguez, S. The art of crafting a systematic literature review in entrepreneurship research. Int. Entrep. Manag. J. 2020, 16, 1023–1042. [Google Scholar] [CrossRef]
- Taylor, C.; Kong, A.C.; Foster, J.; Badawi, N.; Novak, I. Caregivers’ Feeding Experiences and Support of Their Child with Cerebral Palsy. J. Child Fam. Stud. 2022, 31, 819–830. [Google Scholar] [CrossRef]
- Gonzalez-Rozo, N.; Perez-Molina, J.J.; Quinones-Pacheco, Y.B.; Flores-Fong, L.E.; Rea-Rosas, A.; Cabrales-deAnda, J.L. Factors associated with oropharyngeal dysphagia diagnosed by videofluoroscopy in children with cerebral palsy. Rev. Gastroenterol. Mex 2022, 87, 44–51. [Google Scholar] [CrossRef]
- Ron, A.G.; Tobosoa, R.M.G.; Gascóna, M.B.; Santosa, M.T.; Vecinob, R.; Pinedob, A.B. Nutritional status and prevalence of dysphagia in cerebral palsy: Usefulness of the Eating and Drinking Ability Classification System scale and correlation with the degree of motor impairment according to the Gross Motor Function Classification System. Neurologia 2021, in press. [Google Scholar] [CrossRef]
- Mahmoud, H.; El-Hadidy, E.I.; El-Maksoud, G.M.A.; Abd-Elhamid, A.A. Oral-Motor Functions and Gross Motor Abilities in Spastic Cerebral Palsy. Int. J. Recent Adv. Multidiscip. Res. 2019, 6, 5418–5422. [Google Scholar]
- Remijn, L.; van den Engel-Hoek, L.; Satink, T.; de Swart, B.J.; Nijhuis-van der Sanden, M.W. “Everyone sees you sitting there struggling with your food”: Experiences of adolescents and young adults with cerebral palsy. Disabil. Rehabil. 2019, 41, 1898–1905. [Google Scholar] [CrossRef]
- Gyoung, Y.; Oh, B.M.; Seo, H.G.; Shin, H.I.; Bang, M.S. Dysphagia-Related Quality of Life in Adults with Cerebral Palsy on Full Oral Diet Without Enteral Nutrition. Dysphagia 2019, 34, 201–209. [Google Scholar]
- Arslan, S.S.; Ilgaz, F.; Demir, N.; AyşeKaraduman, A. The Effect of the Inability to Intake Chewable Food Texture on Growth, Dietary Intake and Feeding Behaviors of Children with Cerebral Palsy. J. Dev. Phys. Disabil. 2018, 30, 205–214. [Google Scholar] [CrossRef]
- Benfer, K.A.; Weir, K.A.; Bell, K.L.; Ware, R.S.; Davies, P.S.W.; Boyd, R.N. Oropharyngeal dysphagia in preschool children with cerebral palsy: Oral phase impairments. Res. Dev. Disabil. 2014, 35, 3469–3481. [Google Scholar] [CrossRef]
- Fleet, S.E.; Davidson, R.D. Pediatric Feeding Disorders: Feeding Children Who Can’t or Won’t Eat. In Encyclopedia of Human Nutrition; Elsevier: Amsterdam, The Netherlands, 2013; pp. 21–27. [Google Scholar]
- Miller, C.K.; Maybee, J.; Prager, J.; Pentiuk, S. Feeding and Swallowing Disorders. In Kendig’s Disorders of the Respiratory Tract in Children, 9th ed.; Wilmott, R.W., Deterding, R., Li, A., Ratjen, F., Sly, P., Zar, H.J., Bush, A., Eds.; Elsevier: Philadelphia, PA, USA, 2019; pp. 1106–1113.e1. [Google Scholar]
- Rempel, G. The Importance of Good Nutrition in Children with Cerebral Palsy. Phys. Med. Rehabil. Clin. N. Am. 2015, 26, 39–56. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.A.; Navathe, A.S. Nutrition and Feeding for Children with Developmental Disabilities. In Pediatric Gastrointestinal and Liver Disease, 4th ed.; Wyllie, R., Hyams, J.S., Eds.; W.B. Saunders: Saint Louis, MO, USA, 2011; pp. 1020–1032.e3. [Google Scholar]
- Seo, H.G.; Yi, Y.G.; Choi, Y.A.; Leigh, J.H.; Yi, Y.; Kim, K.; Bang, M.S. Oropharyngeal Dysphagia in Adults With Dyskinetic Cerebral Palsy and Cervical Dystonia: A Preliminary Study. Arch. Phys. Med. Rehabil. 2019, 100, 495–500.e1. [Google Scholar] [CrossRef]
- Sheppard, J.J. Dysphagia Disorders Survey and Dysphagia Management Staging Scale (Adult and Pediatric Applications): User’s Manual: Australian Edition; The Centre for Developmental Disability: Ryde, Australia, 2003. [Google Scholar]
- Reilly, S.; Skuse, D.; Wolke, D. Schedule for Oral Motor Assessment: Administration Manual; Whurr Publishers Ltd.: London, UK, 2000. [Google Scholar]
- Morris, S.E. Pre-Speech Assessment Scale: A Rating Scale for the Measurement of Pre-Speech Behaviors from Birth through Two Years; JA Preston Corp.: Clifton, NJ, USA, 1982. [Google Scholar]
- Thomas-Stonell, N.; Greenberg, J. Three treatment approaches and clinical factors in the reduction of drooling. Dysphagia 1988, 3, 73–77. [Google Scholar] [CrossRef]
- Penagini, F.; Mameli, C.; Fabiano, V.; Brunetti, D.; Dilillo, D.; Zuccotti, G.V. Dietary Intakes and Nutritional Issues in Neurologically Impaired Children. Nutrients 2015, 7, 9400–9415. [Google Scholar] [CrossRef]
- Morgan, A.T.; Omahoney, R.; Francis, H. The use of pulse oximetry as a screening assessment for paediatric neurogenic dysphagia. Dev. Neurorehabil. 2008, 11, 25–38. [Google Scholar] [CrossRef]
- Salghetti, A.; Martinuzzi, A. Dysphagia in cerebral palsy. East. J. Med. 2012, 17, 188–193. [Google Scholar]
- Jonsson, U.; Eek, M.N.; Sunnerhagen, K.S.; Himmelmann, K. Health Conditions in Adults With Cerebral Palsy: The Association With CP Subtype and Severity of Impairments. Front. Neurol. 2021, 12, 732939. [Google Scholar] [CrossRef] [PubMed]
- Wilson, E.M.; Hustad, K.C. Early Feeding Abilities in Children with Cerebral Palsy A Parental Report Study. J. Med. Speech Lang. Pathol. 2010, nihpa57357. [Google Scholar]
- Usman, H.; Asghar, M. Frequency of Feeding Problems in Children with Cerebral Palsy Address of Correspondence. J. Islamabad Med. Dent. Coll. 2017, 6, 31–34. [Google Scholar]
- Sharp, W.G.; Volkert, V.M.; Scahill, L.; McCracken, C.E.; McElhanon, B. A Systematic Review and Meta-Analysis of Intensive Multidisciplinary Intervention for Pediatric Feeding Disorders: How Standard Is the Standard of Care? J. Pediatr. 2017, 181, 116–124.e4. [Google Scholar] [CrossRef] [PubMed]
- Swallowing Instrumental Assessment—PORTAL MyHEALTH. Available online: http://www.myhealth.gov.my/en/swallowing-instrumental-assessment/ (accessed on 27 August 2022).
- Caramico-Favero, D.C.O.; Guedes, Z.C.F.; Morais, M.B.D. Food Intake, Nutritional Status and Gastrointestinal Symptoms in Children with Cerebral Palsy. Arq. Gastroenterol. 2018, 55, 352–357.53. [Google Scholar] [CrossRef] [PubMed]
- Rajikan, R.; Zakaria, N.M.; Manaf, Z.A.; Yusoff, N.A.M.; Shahar, S. The effect of feeding problems on the growth of children and adolescents with cerebral palsy. J. Fundam. Appl. Sci. 2018, 9, 787–804. [Google Scholar] [CrossRef]
- Nur, F.T.; Handryastuti, S.; Poesponegoro, H.D. Feeding Difficulties in Children with Cerebral Palsy: Prevalence and Risk Factor. KnE Life Sci. 2019, 4, 206–214. [Google Scholar] [CrossRef]
- Lowesa, L.; Clarkb, T.S.; Noritz, G. Factors associated with caregiver experience in families with a child with cerebral palsy. J Pediatr. Rehabil Med. 2016, 9, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Sleigh, G. Mothers’ voice A qualitative study on feeding children with cerebral palsy. Child Care Health Dev. 2005, 31, 373–383. [Google Scholar] [CrossRef]
- Polack, S.; Adams, M.; O’banion, D.; Baltussen, M.; Asante, S.; Kerac, M.; Gladstone, M.; Zuurmond, M. Children with cerebral palsy in Ghana: Malnutrition, feeding challenges, and caregiver quality of life. Dev. Med. Child Neurol. 2018, 60, 914–921. [Google Scholar] [CrossRef]
- Yousafzai, A.K.; Pagedar, S.; Wirz, S.; Filteau, S. Beliefs about feeding practices and nutrition for children with disabilities among families in Dharavi, Mumbai. Int. J. Rehabil. Res. 2003, 26, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Raina, P.; O’Donnell, M.; Rosenbaum, P.; Brehaut, J.; Walter, S.D.; Russell, D.; Swinton, M.; Zhu, B.; Wood, E. The health and well-being of caregivers of children with cerebral palsy. Pediatrics 2005, 115, e626–e636. [Google Scholar] [CrossRef]
- Kamaralzaman, S.; Ying, T.C.; Mohamed, S.; Toran, H.; Satari, N.; Abdullah, N. The economic burden of families of children with cerebral palsy. Malays. J. Public Health Med. 2018, 1, 156–165. [Google Scholar]
- Adams, M.S.; Khan, N.Z.; Begum, S.A.; Wirz, S.L.; Hesketh, T.; Pring, T.R. Feeding difficulties in children with cerebral palsy: Low-cost caregiver training in Dhaka, Bangladesh. Child Care Health Dev. 2012, 38, 878–888. [Google Scholar] [CrossRef]
- IDDSI—Home. Available online: https://iddsi.org/ (accessed on 27 January 2022).
- Lam, P.; Stanschus, S.; Zaman, R.; Cichero, J.A. The International Dysphagia Diet Standardisation Initiative (IDDSI) framework the Kempen pilot. Br. J. Neurosci. Nurs. 2017, 13, S18–S26. [Google Scholar] [CrossRef]
- Wu, X.S.; Miles, A.; Braakhuis, A. The Effectiveness of International Dysphagia Diet Standardization Initiative–Tailored Interventions on Staff Knowledge and Texture-Modified Diet Compliance in Aged Care Facilities: A Pre-Post Study. Curr. Dev. Nutr. 2022, 6, nzac032. [Google Scholar] [CrossRef] [PubMed]
- Jahan, I.; Muhit, M.; Hardianto, D.; Laryea, F.; Amponsah, S.K.; Chhetri, A.B.; Smithers-Sheedy, H.; McIntyre, S.; Badawi, N.; Khandaker, G. Epidemiology of Malnutrition among Children with Cerebral Palsy in Low- and Middle-Income Countries: Findings from the Global LMIC CP Register. Nutrients 2021, 13, 3676. [Google Scholar] [CrossRef] [PubMed]
- Vikram, K.; Vanneman, R. Maternal education and the multidimensionality of child health outcomes in India. J. Biosoc. Sci. 2020, 52, 57–77. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, T.; Iskandar, M.M.; Baeghbali, V.; Ngadi, M.O.; Kubow, S. 3D Food Printing Applications Related to Dysphagia: A Narrative Review. Foods 2022, 11, 1789. [Google Scholar] [CrossRef]
- Smith, R.; Bryant, L.; Hemsley, B. Allied Health Professionals’ Views on the Use of 3D Food Printing to Improve the Mealtime Quality of Life for People with Dysphagia: Impact, Cost, Practicality, and Potential. Am. J. Speech Lang. Pathol. 2022, 31, 1868–1877. [Google Scholar] [CrossRef]


{kind=link}
| Patient or Population | Cerebral Palsy |
|---|---|
| Concept | Food texture modification |
| Context | swallowing difficulties (dysphagia) |
| Keywords | Synonyms | Variation |
|---|---|---|
| Texture | Consistency | Textures, textured |
| Composition | ||
| Constitution | ||
| Modification | Adjustment | Modify, modification |
| Adaptation | ||
| Difficulty | Complication | Difficulties, complications, obstacles, struggles |
| Obstacle | ||
| Struggle | ||
| Disorders | Complications | Disorder, complication, complicated |
| Swallowing | Deglutition | |
| Challenges | Demand | |
| Objection | ||
| Threat |
| Author and Year | Location | Study Design | Sample Size and Age | Method | Findings/Key Points | Remark |
|---|---|---|---|---|---|---|
| Taylor (2022) [29] | Australia | Qualitative-semi-structured interview | Caregivers with CP aged less than 18 years (n = 11) | In-depth interviews by telephone | Child-centered world–worry due to choking and concern about safety and body weight, food preparation, food, and liquid modification, positioning, and longer feeding time. Making decisions–problem-solving depends on the child’s health status, seeking knowledge to treat feeding problems. Knowing their child–unique feeding feeds affect the food preparation process. Seeking and receiving support–family support, healthcare professionals’ intervention, financial issues, and social support. | Healthcare support is essential in managing feeding problems among individuals with CP. |
| Gonzalez (2022) [30] | Mexico | Case-control study | Eight months–15 years of age Control (CP with no OPD, n = 30) Case (CP with OPD, n = 30) | All patients undergo VFSS–testing with three consistencies: nectar, thin liquid, and puree consistency. GMFCS Weight, Height and BMI | OPD related to degree V GMFCS Longer feeding length above 30 min, lack of ability to keep the lips together, coughing during or after meals, choking all through or after meals The process of swallowing food in bolus form was significantly difficult (p < 0.05). It took a longer time in CP with OPD than with CP without OPD as perceived by the mother. | The Association between OPD documented by VFSS and the severity of gross motor function impairment ought to be due to a greater neurologic injury that led to feeding problems. |
| Garcia (2021) [31] | Spain | A descriptive, cross-sectional, open-label study | n= 44 (children and adolescents with CP) | GMFCS Dysphagia screening EDACS | Patients with more significant feeding difficulties (higher EDACS levels) presented more severe functional impairment (higher GMFCS levels) BMI values indicated poorer nutritional status in patients with higher EDACS levels and severe GMFCS. | Medical history interviews should include questions addressing the ability to bite, chew, and swallow and to manage different textures of foods and fluids, as well as red flags indicating dysphagia. |
| Mahmoud (2019) [32] | Egypt | Correlation-al study | Individuals with CP (n = 100) from 1–4 years. | SOMA GMFM | Eating capability was substantially related to gross motor functional abilities. Children’s capacity to consume food textures with advancing complexity was best in those with GMFCS I and progressively reduced as GMFCS level increased (or gross motor functional capacity decreased). | Future research investigating the occurrence of OPD using evaluation of feeding skills, relationship with capability on food textures, and effect on nutritional status throughout the full range of gross motor function capabilities are required. |
| Remijn (2019) [33] | Netherlands | Qualitative study | Participants with spastic CP (n = 10), aged 15–23 years | Semi-structured in-depth interviews | Perceived eating and drinking difficulties food textures influenced problems with swallowing and mastication Challenges in a physical and social context challenges in the accessibility as a wheelchair user, menu choices were determined primarily by texture over taste preferences, dependency on others Dealing with eating and drinking difficulties adaptation or avoidance of foods, perseverance to keep trying or giving up to try or acceptance of help Negative feeling feelings of shame, frustration, distress, and fear concerning choking | Healthcare providers and the food industry play a vital role in the CP population that needs food texture modification in their daily diet. |
| Yi (2019) [34] | Korea | A cross-sectional, interview-based survey study | Adults with CP on full oral diet (n = 117) Healthy individuals (n = 117) | SWAL-QOL GMFCS MACS FOIS | The majority of CP participants receiving complete oral diets had pharyngeal symptoms (choking on food, choking on liquid, coughing when food became stuck, coughing, clearing the throat, and food sticking in the throat) Most participants needed modification or restriction of certain foods due to longer meal durations and lower BMI. | In adults with CP, dysphagia symptoms are frequent and can profoundly affect swallowing related QOL. |
| Serel (2018) [35] | Turkey | Cross-sectional study | A study group with individuals with CP (n= 50 control group (n= 35), aged 18–90 months | 24-h diet recall BPFAS GMFCS | Children with CP had a greater incidence of choking and vomiting during meals. Caregivers perceived the mealtime behavior of children with CP was greater problematic. Caregivers may fail to prepare correct food consistency. Lower energy intake in children with CP due to types of diet given, energy loss at some point of feeding. Types of diet taken were liquidized or pureed food. Children with CP whose diets consisted of food textures Levels 3 to 5 according to IDDSI classification had poorer growth and nutritional status. CP whose diet is fully composed of liquidized or pureed meals with no lumps may no longer meet their energy or nutrient due to decreased energy density and reduced calorie intake. | Parental reported the need for the preparation of appropriate food texture, preparation time constraints, and the child’s behavior during mealtime. The feeding issues of the inability to take chewable meals may contribute to the growth, dietary status, negative feeding behaviors, and greater problematic perceptions by caregivers among children with CP. |
| Marques (2016) [15] | Portugal | A mixed descriptive and exploratory study | CP with their families (n = 104) | Anthropometric Parents Questionnaire (Qualitative study) Family APGAR score | Parents stated that feeding issues were an unbalanced diet, meal monotony, shame, difficult access to tailored outside food, insufficient technical equipment, food spilling, choking, vomiting, time, cooking meals separately, and costs. Food aspiration is one of these risks, leading to severe problems such as pneumonia, airway obstruction, and even death. Parents regularly pick food that is quicker to cook, with equal consistency, which leads to no variety in food/nutrients. | Food consistency should be tailored to the child’s constraints and to minimize the risk of food aspiration. |
| Benfer (2015) [18] | Australia | A cross-sectional, population-based cohort study | Young children with CP (n = 99) aged 18 to 36 months | 3-day weighed food records. PEDI DDS CFQ Swallowing Safety Recommendation | Modified food/fluid textures are common in children’s diets with CP. Modifications to diets limit their child’s ability on food textures, indicating parents are generally excluding foods/fluids for which they perceive their child has difficulty. Children with severe GMFCS consume a lower proportion of chewable foods and more fluids. Purees and fluids are likely more efficiently eaten by children with lower gross motor function. | Training parents to detect safety concerns on food/fluid textures with higher density may be more clinically meaningful and effective than focusing on identifying specific oromotor impairments to achieve adequate energy intake. |
| Benfer (2014) [36] | Australia | Cross-sectional study | Cerebral palsy (n = 130 Typical children (n = 40), aged 18–36 months | DDS SOMA PSAS Parent-report 3-day weighed food record GMFCS Feeding questionnaire | Oral phase impairments associated with GMFCS level. For solid food, children with CP had difficulty biting (70%), cleaning behaviors (70%), and chewing problems (65%). | Increasing energy density with the correct food texture improves nutritional outcomes. |
| Author & Year | Location | Book Chapter & Report | Key Points | Remark | ||
| Fleet (2022) [37] | USA | Encyclopedia of Human Nutrition (Third Edition), Academic Press, 2013, Pages 21–27 Pediatric feeding disorders: feeding children who can’t or won’t eat | Positioning, food texture, bolus size, rate, and the amount of food presented can determine the safest and most efficient feeding method. | The goal of safe oral feeding is attainable in most children when those involved in the care of children understand the complexity of eating and the associated medical and psychological conditions that comprise a feeding disorder. | ||
| Miller (2021) [38] | USA | Reference Module in Food Science Cerebral palsy: nutritional aspects | Changes in the texture of solids and liquids may be necessary to ensure safety. Management strategies for daily mealtime feeding include positioning, modification of the sensory properties of the food, oral motor facilitation techniques, and equipment adaptations. The International Dysphagia Diet Standardization Initiative (IDDSI) Framework provides a common terminology to describe food textures and liquid thickness. | All interdisciplinary plans, including nutrition, should be safe, promote growth or weight gain without excessive energy expenditure and reflect the family’s resources in time and skill, addressing their concerns and expectations. | ||
| Rempel (2015) [39] | Canada | Physical Medicine and Rehabilitation Clinics of North America Volume 26, Issue 1, Pages 39–56 Good Nutrition in Children with Cerebral Palsy | Valuable information in understanding a child’s feeding challenges WHO: Persons involved with feeding; differences in feeding styles WHAT: The type, texture, viscosity, quantity, and quality of the food consumed WHEN: The timing, frequency, and duration of meals WHERE: The feeding environment, distractions HOW: The feeding routine, technique, adaptive equipment, and positioning Nutritional factors that require food texture modification help in the development of children with CP. | Consideration of the multidimensional aspects of feeding and the contribution of family members in setting goals and carrying out the nutritional intervention. | ||
| Cohen (2011) [40] | USA | Pediatric Gastrointestinal and Liver Disease (Fourth Edition) Pages 1020–1032.e3 Chapter 92—Nutrition and Feeding for Children with Developmental Disabilities | Taste and texture can be different if the individual is identified as safe to eat orally. Decreased feeding efficiency happens in individuals with CP: chewing and swallowing take 12 to 15 times longer than in typical individuals, and lead to insufficient caloric and nutritional needs. Individuals with sensory-based problems had greater issues with foods that require chewing and may separate foods of thicker textures and pocket them in their mouths. In addition, they frequently have a sensory integration defect with the texture and taste of foods. | Caregivers must be adequately instructed, trained, and reassured, and appropriate follow-up must be arranged to verify the patient’s progress and alter the routine to obtain an optimal outcome. | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamal, S.; Kamaralzaman, S.; Sharma, S.; Jaafar, N.H.; Chern, P.M.; Hassan, N.I.; Toran, H.; Ismail, N.A.S.; Yusri, G.; Hamzaid, N.H. A Review of Food Texture Modification among Individuals with Cerebral Palsy: The Challenges among Cerebral Palsy Families. Nutrients 2022, 14, 5241. https://doi.org/10.3390/nu14245241
Kamal S, Kamaralzaman S, Sharma S, Jaafar NH, Chern PM, Hassan NI, Toran H, Ismail NAS, Yusri G, Hamzaid NH. A Review of Food Texture Modification among Individuals with Cerebral Palsy: The Challenges among Cerebral Palsy Families. Nutrients. 2022; 14(24):5241. https://doi.org/10.3390/nu14245241
Chicago/Turabian StyleKamal, Sakinah, Sazlina Kamaralzaman, Shobha Sharma, Nurul Hazirah Jaafar, Phei Ming Chern, Nurul Izzaty Hassan, Hasnah Toran, Noor Akmal Shareela Ismail, Ghazali Yusri, and Nur Hana Hamzaid. 2022. "A Review of Food Texture Modification among Individuals with Cerebral Palsy: The Challenges among Cerebral Palsy Families" Nutrients 14, no. 24: 5241. https://doi.org/10.3390/nu14245241
APA StyleKamal, S., Kamaralzaman, S., Sharma, S., Jaafar, N. H., Chern, P. M., Hassan, N. I., Toran, H., Ismail, N. A. S., Yusri, G., & Hamzaid, N. H. (2022). A Review of Food Texture Modification among Individuals with Cerebral Palsy: The Challenges among Cerebral Palsy Families. Nutrients, 14(24), 5241. https://doi.org/10.3390/nu14245241