
No Association between Low-Calorie Sweetener (LCS) Use and Overall Cancer Risk in the Nationally Representative Database in the US: Analyses of NHANES 1988–2018 Data and 2019 Public-Use Linked Mortality Files

Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source and Population
2.2. The Food and Nutrient Database for Dietary Studies (FNDDS)
2.3. Health Behaviors and Diet Quality Measures
2.4. Comparing LCS Consumers and Nonconsumers by Demographics and Diet Quality Measures
2.5. Analytical Methods to Assess Cancer Mortality Risk
3. Results
3.1. Participant Characteristics for 1988–1994 and 1999–2018 NHANES Surveys
3.2. Characteristics of LCS Consumers and Non Consumers in 1988–1994 and 1999–2018 NHANES
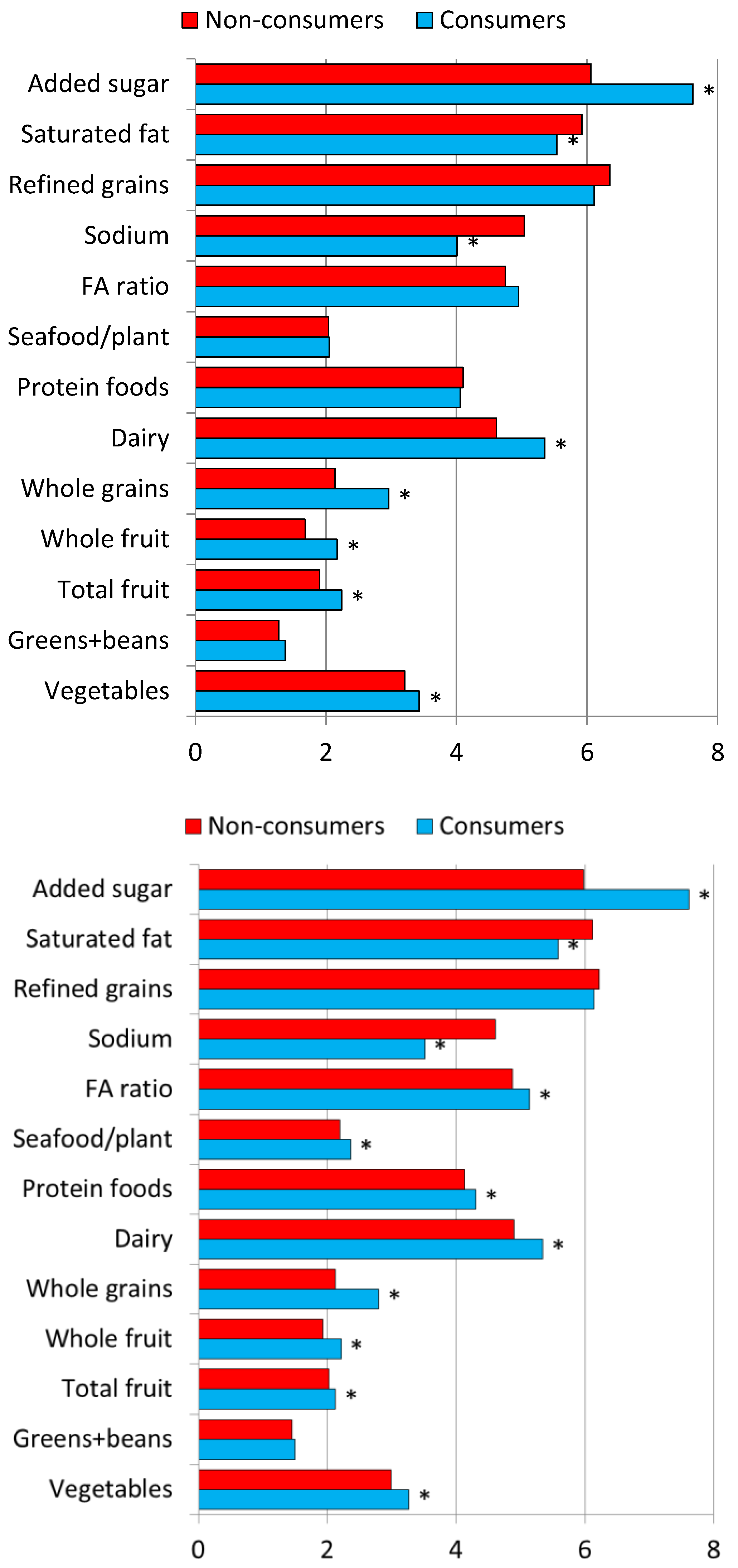
3.3. Comparing LCS Consumers and Nonconsumers by Diet Quality (HEI-2015)
3.4. Cancer Mortality Hazard Ratio Associations with Aspartame, Saccharin, and LCS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fitch, C.; Keim, K.S. Position of the Academy of Nutrition and Dietetics: Use of nutritive and nonnutritive sweeteners. J. Acad. Nutr. Diet. 2012, 112, 739–758. [Google Scholar] [CrossRef] [PubMed]
- Gardner, C.; Wylie-Rosett, J.; Gidding, S.S.; Steffen, L.M.; Johnson, R.K.; Reader, D.; Lichtenstein, A.H.; American Heart Association Nutrition Committee of the Council on Nutrition; Physical Activity and Metabolism; Council on Arteriosclerosis; et al. Nonnutritive sweeteners: Current use and health perspectives: A scientific statement from the American Heart Association and the American Diabetes Association. Diabetes Care 2012, 35, 1798–1808. [Google Scholar] [CrossRef] [PubMed]
- Sylvetsky, A.C.; Jin, Y.; Clark, E.J.; Welsh, J.A.; Rother, K.I.; Talegawkar, S.A. Consumption of Low-Calorie Sweeteners among Children and Adults in the United States. J. Acad. Nutr. Diet. 2017, 117, 441–448.e2. [Google Scholar] [CrossRef] [PubMed]
- Rogers, P.J.; Appleton, K.M. The effects of low-calorie sweeteners on energy intake and body weight: A systematic review and meta-analyses of sustained intervention studies. Int. J. Obes. 2021, 45, 464–478. [Google Scholar] [CrossRef]
- Rogers, P.J.; Hogenkamp, P.S.; de Graaf, C.; Higgs, S.; Lluch, A.; Ness, A.R.; Penfold, C.; Perry, R.; Putz, P.; Yeomans, M.R.; et al. Does low-energy sweetener consumption affect energy intake and body weight? A systematic review, including meta-analyses, of the evidence from human and animal studies. Int. J. Obes. 2016, 40, 381–394. [Google Scholar] [CrossRef]
- Olivier, B.; Serge, A.H.; Catherine, A.; Jacques, B.; Murielle, B.; Marie-Chantal, C.-L.; Sybil, C.; Jean-Philippe, G.; Sabine, H.; Esther, K.; et al. Review of the nutritional benefits and risks related to intense sweeteners. Arch. Public Health 2015, 73, 41. [Google Scholar] [CrossRef]
- Sylvetsky, A.C. Metabolic Effects of Low-Calorie Sweeteners: A Brief Review. Obesity 2018, 26, S25–S31. [Google Scholar] [CrossRef]
- Fowler, S.P.; Williams, K.; Resendez, R.G.; Hunt, K.J.; Hazuda, H.P.; Stern, M.P. Fueling the obesity epidemic? Artificially sweetened beverage use and long-term weight gain. Obesity (Silver Spring) 2008, 16, 1894–1900. [Google Scholar] [CrossRef]
- de Koning, L.; Malik, V.S.; Rimm, E.B.; Willett, W.C.; Hu, F.B. Sugar-sweetened and artificially sweetened beverage consumption and risk of type 2 diabetes in men. Am. J. Clin. Nutr. 2011, 93, 1321–1327. [Google Scholar] [CrossRef]
- Nettleton, J.A.; Lutsey, P.L.; Wang, Y.; Lima, J.A.; Michos, E.D.; Jacobs, D.R., Jr. Diet soda intake and risk of incident metabolic syndrome and type 2 diabetes in the Multi-Ethnic Study of Atherosclerosis (MESA). Diabetes Care 2009, 32, 688–694. [Google Scholar] [CrossRef]
- Ludwig, D.S. Artificially sweetened beverages: Cause for concern. JAMA 2009, 302, 2477–2478. [Google Scholar] [CrossRef] [PubMed]
- Swithers, S.E. Artificial sweeteners produce the counterintuitive effect of inducing metabolic derangements. Trends Endocrinol. Metabol. 2013, 24, 431–441. [Google Scholar] [CrossRef] [PubMed]
- Suez, J.; Korem, T.; Zeevi, D.; Zilberman-Schapira, G.; Thaiss, C.A.; Maza, O.; Israeli, D.; Zmora, N.; Gilad, S.; Weinberger, A.; et al. Artificial sweeteners induce glucose intolerance by altering the gut microbiota. Nature 2014, 514, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.J.; Khan, T.A.; McGlynn, N.; Malik, V.S.; Hill, J.O.; Leiter, L.A.; Jeppesen, P.B.; Rahelić, D.; Kahleová, H.; Salas-Salvadó, J.; et al. Relation of Change or Substitution of Low- and No-Calorie Sweetened Beverages with Cardiometabolic Outcomes: A Systematic Review and Meta-analysis of Prospective Cohort Studies. Diabetes Care 2022, 45, 1917–1930. [Google Scholar] [CrossRef] [PubMed]
- Mela, D.J. Is There an Academic Bias against Low-Energy Sweeteners? Nutrients 2022, 14, 1428. [Google Scholar] [CrossRef]
- Drewnowski, A.; Rehm, C.D. The use of low-calorie sweeteners is associated with self-reported prior intent to lose weight in a representative sample of US adults. Nutr. Diabetes 2016, 6, e202. [Google Scholar] [CrossRef]
- Lim, U.; Subar, A.F.; Mouw, T.; Hartge, P.; Morton, L.M.; Stolzenberg-Solomon, R.; Campbell, D.; Hollenbeck, A.R.; Schatzkin, A. Consumption of aspartame-containing beverages and incidence of hematopoietic and brain malignancies. Cancer Epidemiol. Biomark. Prev. 2006, 15, 1654–1659. [Google Scholar] [CrossRef]
- Marinovich, M.; Galli, C.L.; Bosetti, C.; Gallus, S.; La Vecchia, C. Aspartame, low-calorie sweeteners and disease: Regulatory safety and epidemiological issues. Food Chem. Toxicol. 2013, 60, 109–115. [Google Scholar] [CrossRef]
- European Food Safety Authority. Outcome of the public consultation on a draft protocol for the assessment of hazard identification and characterisation of sweeteners. EFSA Support. Publ. 2020, 17, 1803E. [Google Scholar] [CrossRef]
- Agence Nationale de Securite’ Sanitaire de l’Alimentation; de l’Environnement et du Travail. Evaluation des Benefices et des Risques Nutritionnels des Edulcorants Intenses. Maisons-Alfort: Agence Nationale de Securite Sanitaire de l’Alimentation, de l’Environnement et du Travail. 2015. Available online: https://www.anses.fr/fr/system/files/NUT2011sa0161Ra.pdf (accessed on 2 March 2022).
- U.S. Food and Drug Administration. Additional Information about High-Intensity Sweeteners Permitted for Use in Food in the United States. Available online: https://www.fda.gov/food/food-additives-petitions/additional-information-about-high-intensity-sweeteners-permitted-use-food-united-states (accessed on 21 November 2022).
- Schernhammer, E.S.; Bertrand, K.A.; Birmann, B.M.; Sampson, L.; Willett, W.C.; Feskanich, D. Consumption of artificial sweetener–and sugar-containing soda and risk of lymphoma and leukemia in men and women. Am. J. Clin. Nutr. 2012, 96, 1419–1428. [Google Scholar] [CrossRef]
- Debras, C.; Chazelas, E.; Srour, B.; Druesne-Pecollo, N.; Esseddik, Y.; Szabo de Edelenyi, F.; Agaësse, C.; De Sa, A.; Lutchia, R.; Gigandet, S.; et al. Artificial sweeteners and cancer risk: Results from the NutriNet-Santé population-based cohort study. PLoS Med. 2022, 19, e1003950. [Google Scholar] [CrossRef] [PubMed]
- Andreeva, V.A.; Salanave, B.; Castetbon, K.; Deschamps, V.; Vernay, M.; Kesse-Guyot, E.; Hercberg, S. Comparison of the sociodemographic characteristics of the large NutriNet-Santé e-cohort with French Census data: The issue of volunteer bias revisited. J. Epidemiol. Community Health 2015, 69, 893–898. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC); National Center for Health Statistics (NCHS). About the National Health and Nutrition Examination Survey (NHANES). Available online: https://www.cdc.gov/nchs/nhanes/about_nhanes.htm (accessed on 21 November 2022).
- Centers for Disease Control and Prevention (CDC); National Center for Health Statistics (NCHS). 2019 Public-Use linked Mortality Files. Available online: https://www.cdc.gov/nchs/data-linkage/mortality-public.htm (accessed on 21 November 2022).
- Centers for Disease Control and Prevention (CDC); National Center for Health Statistics (NCHS). The Third National Health and Nutrition Examination Survey (NHANES III, 1988–1994) Reference Manuals and Reports. Available online: https://www.cdc.gov/nchs/data/nhanes/nhanes3/cdrom/main.pdf (accessed on 21 November 2022).
- Centers for Disease Control and Prevention (CDC); National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey. NHANES Questionnaires, Datasets, and Related Documentation. Available online: https://wwwn.cdc.gov/nchs/nhanes/Default.aspx (accessed on 21 November 2022).
- Centers for Disease Control and Prevention (CDC); National Center for Health Statistics (NCHS). NCHS Research Ethics Review Board (ERB) Approval. Available online: https://www.cdc.gov/nchs/nhanes/irba98.htm (accessed on 21 November 2022).
- Ahuja, J.K.A.; Montville, J.B.; Omolewa-Tomobi, G.; Heendeniya, K.Y.; Martin, C.L.; Steinfeldt, L.C.; Anand, J.; Adler, M.E.; LaComb, R.P.; Moshfegh, A.J. USDA Food and Nutrient Database for Dietary Studies, 5.0.; U.S. Department of Agriculture, Agricultural Research Service, Food Surveys Research Group: Beltsville, MD, USA, 2012.
- Drewnowski, A.; Rehm, C.D. Socio-demographic correlates and trends in low-calorie sweetener use among adults in the United States from 1999 to 2008. Eur. J. Clin. Nutr. 2015, 69, 1035–1041. [Google Scholar] [CrossRef] [PubMed]
- USDA Food and Nutrition Service. Healthy Eating Index. Available online: https://www.fns.usda.gov/healthy-eating-index-hei (accessed on 21 November 2022).
- U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2015–2020, 9th ed.; U.S. Government Printing Office: Washington, DC, USA, 2015.
- Toews, I.; Lohner, S.; de Gaudry, D.K.; Sommer, H.; Meerpohl, J.J. Association between Intake of Non-Sugar Sweeteners and Health Outcomes: Systematic Review and Meta-Analyses of Randomised and Non-Randomised Controlled Trials and Observational Studies. BMJ 2019, 364, k4718. Available online: https://www.bmj.com/content/364/bmj.k4718 (accessed on 21 November 2022). [CrossRef]
- Andrade, L.; Lee, K.M.; Sylvetsky, A.C.; Kirkpatrick, S.I. Low-calorie sweeteners and human health: A rapid review of systematic reviews. Nutr. Rev. 2021, 79, 1145–1164. [Google Scholar] [CrossRef]
- National Cancer Institute. Age and Cancer Risk. Available online: https://www.cancer.gov/about-cancer/causes-prevention/risk/age (accessed on 21 November 2022).
- Normand, M.; Ritz, C.; Mela, D.; Raben, A. Low-energy sweeteners and body weight: A citation network analysis. BMJ Nutr. Prev. Health 2021, 4, 319–332. [Google Scholar] [CrossRef]


{kind=link}
| Exclusion Description | NHANES III 1988–1994 | All 1988–2018 | ||
|---|---|---|---|---|
| Exclusions n | Total Exclusions | Exclusions n | Total Exclusions | |
| Total sample | 19,215 | 76,324 | ||
| Dietary recall incomplete | 2882 | 2882 | 9418 | 9418 |
| Pregnant or lactating female | 385 | 3267 | 2198 | 11,616 |
| Dietary intake missing kcal = 0 | 0 | 3267 | 6 | 11,622 |
| Not mortality eligible | 10 | 3277 | 92 | 11,714 |
| Told by doctor had diabetes | 1292 | 4569 | 8145 | 19,859 |
| Told by doctor had MI * | 583 | 5152 | 1941 | 21,800 |
| Told by doctor had CHF * | 203 | 5355 | 723 | 22,523 |
| Told by doctor had stroke | 230 | 5585 | 1118 | 23,641 |
| Told by doctor had cancer | 867 | 6452 | 3790 | 27,431 |
| Education level missing | 81 | 6533 | 119 | 27,550 |
| Current smoking missing | 1 | 6534 | 58 | 27,608 |
| Physical activity level missing | 220 | 6754 | 228 | 27,836 |
| BMI missing | 23 | 6777 | 424 | 28,260 |
| Mortality Analysis n | 12,438 | 48,064 | ||
| Characteristics | 1988–1994 NHANES | 1999–2018 NHANES | 1988–2018 NHANES | |
|---|---|---|---|---|
| n = 15,948 | n = 48,754 | n = 64,702 | ||
| LCS consumers | 29.87 (0.54) | 29.11 (0.44) | 29.26 (0.37) | |
| Gender | Female | 51.56 (0.44) | 50.76 (0.28) | 50.92 (0.24) |
| Race/ethnicity | NH White | 76.36 (1.25) | 68.40 (1.03) * | 69.92 (0.86) |
| NH Black | 10.95 (0.63) | 11.28 (0.58) | 11.22 (0.48) | |
| MexAmerican | 4.98 (0.40) | 8.17 (0.54) * | 7.56 (0.44) | |
| Other Hispanic | 4.24 (0.63) | 5.38 (0.42) | 5.16 (0.36) | |
| Other | 3.47 (0.42) | 6.77 (0.31) * | 6.14 (0.26) | |
| PIR | <1.35 | 19.22 (0.97) | 23.10 (0.58) * | 22.36 (0.51) |
| 1.35–1.85 | 10.81 (0.52) | 9.91 (0.25) | 10.08 (0.22) | |
| >1.85 | 69.96 (1.12) | 66.99 (0.69) * | 67.56 (0.60) | |
| Education | <HS | 58.98 (1.20) | 41.75 (0.68) * | 45.04 (0.60) |
| Some college | 20.73 (0.68) | 31.36 (0.39) * | 29.33 (0.33) | |
| >BA | 20.29 (0.86) | 26.89 (0.70) * | 25.63 (0.59) | |
| Physical activity | Sedentary | 21.55 (0.74) | 26.88 (0.44) * | 25.88 (0.38) |
| Moderate | 44.41 (0.71) | 33.86 (0.38) * | 35.85 (0.33) | |
| Vigorous | 34.04 (0.78) | 39.25 (0.52) * | 38.27 (0.44) | |
| Smoking, current | 28.48 (0.82) | 20.67 (0.45) * | 22.17 (0.39) | |
| Obesity | 22.06 (0.71) | 35.35 (0.45) * | 32.78 (0.40) | |
| Diabetes | 5.36 (0.25) | 10.71 (0.20) * | 9.68 (0.18) | |
| Mean (SE) | Mean (SE) | Mean (SE) | ||
| Age (y) | 44.52 (0.48) | 47.01 (0.20) * | 46.53 (0.18) | |
| BMI (kg/m2) | 26.50 (0.11) | 28.72 (0.07) * | 28.29 (0.06) |
| Variables | NHANES 1988–1994 | NHANES 1999–2018 | |||||
|---|---|---|---|---|---|---|---|
| Consumers | Nonconsumers | Consumers | Nonconsumers | ||||
| n = 3979 (29.87%) | n = 11,969 (70.13%) | n = 12,474 (29.11%) | n = 36,280 (70.89%) | ||||
| Gender | Female | 60.21 (1.09) | 47.87 (0.56) | <0.0001 | 57.08 (0.58) | 48.17 (0.35) | <0.0001 |
| Race/ethnicity | White-NH | 86.53 (0.73) | 72.03 (1.52) | <0.0001 | 79.91 (0.86) | 63.67 (1.13) | <0.0001 |
| Black-NH | 6.87 (0.53) | 12.69 (0.72) | <0.0001 | 6.62 (0.40) | 13.19 (0.67) | <0.0001 | |
| Mex. American | 2.85 (0.20) | 5.89 (0.54) | <0.0001 | 5.34 (0.45) | 9.33 (0.60) | <0.0001 | |
| Other Hispanic | 2.74 (0.44) | 4.88 (0.79) | 0.0041 | 3.66 (0.33) | 6.09 (0.48) | <0.0001 | |
| PIR | <1.35 | 11.86 (0.84) | 22.39 (1.16) | <0.0001 | 14.80 (0.57) | 26.57 (0.66) | <0.0001 |
| 1.35–1.85 | 8.46 (0.69) | 11.82 (0.59) | <0.0001 | 7.79 (0.33) | 10.79 (0.29) | <0.0001 | |
| >1.85 | 79.67 (1.23) | 65.79 (1.30) | <0.0001 | 77.41 (0.72) | 62.64 (0.77) | <0.0001 | |
| Education | <HS | 49.89 (1.86) | 62.87 (1.28) | <0.0001 | 35.08 (0.87) | 44.49 (0.72) | <0.0001 |
| Some college | 23.21 (1.26) | 19.67 (0.80) | 0.0227 | 31.82 (0.63) | 31.17 (0.48) | 0.4098 | |
| BA | 26.90 (1.43) | 17.46 (0.95) | <0.0001 | 33.11 (1.00) | 24.34 (0.70) | <0.0001 | |
| Physical activity | Sedentary | 21.88 (1.06) | 21.42 (0.80) | 0.6729 | 26.22 (0.62) | 27.15 (0.49) | 0.1530 |
| Moderate | 43.64 (0.90) | 44.74 (0.84) | 0.3147 | 36.78 (0.59) | 32.67 (0.47) | <0.0001 | |
| Vigorous | 34.48 (1.25) | 33.85 (0.81) | 0.6075 | 37.00 (0.74) | 40.18 (0.58) | 0.0001 | |
| Smoking | Current smokers | 20.42 (1.08) | 31.91 (0.89) | <0.0001 | 15.40 (0.48) | 22.84 (0.54) | <0.0001 |
| Obesity | Prevalence | 29.34 (1.31) | 18.96 (0.65) | <0.0001 | 43.14 (0.75) | 32.15 (0.50) | <0.0001 |
| Diabetes | Prevalence | 11.92 (0.82) | 2.57 (0.20) | <0.0001 | 19.18 (0.48) | 7.23 (0.18) | <0.0001 |
| BMI | Kg/m2 | 27.64 (0.16) | 26.01 (0.11) | <0.0001 | 30.03 (0.10) | 28.18 (0.07) | <0.0001 |
| Age | Mean age years | 46.96 (0.80) | 43.48 (0.48) | <0.0001 | 51.50 (0.26) | 45.16 (0.20) | <0.0001 |
| LCS food, beverage | Mean LCS grams/day | 469 (13) | 0 | <0.0001 | 568 (9) | 0 | <0.0001 |
| Variables | NHANES 1988–1994 | NHANES 1999–2018 | ||||
|---|---|---|---|---|---|---|
| Consumers | Nonconsumers | Consumers | Nonconsumers | |||
| n | n = 3979 | n = 11,969 | n = 12,474 | n = 36,280 | ||
| Energy. kcal/day | 2037 (29) | 2259 (21) | <0.0001 | 2045 (12) | 2213 (9) | <0.0001 |
| HEI 2015 | 51.88 (0.41) | 49.09 (0.33) | <0.0001 | 51.91 (0.23) | 49.55 (0.19) | <0.0001 |
| Added sugar tsp eq/day | 13.71 (0.39) | 20.20 (0.43) | <0.0001 | 13.65 (0.18) | 20.70 (0.20) | <0.0001 |
| Alcohol g/day | 8.11 (0.59) | 11.81 (0.70) | <0.0001 | 8.92 (0.38) | 11.62 (0.30) | <0.0001 |
| Fiber g/day | 17.11 (0.30) | 16.54 (0.15) | 0.0952 | 16.95 (0.16) | 16.39 (0.13) | 0.0014 |
| LCS Type | Age | Gender | n | Event n | Tertial 1 | Tertile 2 | Tertile 3 | Group Trend | |
|---|---|---|---|---|---|---|---|---|---|
| HR (LCL, UCL) | HR (LCL, UCL) | HR (LCL, UCL) | Beta (LCL, UCL) | p | |||||
| Aspartame (mg) | 19–50 | All | 8511 | 322 | 0.38 (0.18, 0.82) | 0.57 (0.27, 1.23) | 1.54 (0.91, 2.62) | 1.03 (0.83, 1.27) | 0.7825 |
| Male | 4133 | 162 | 0.44 (0.17, 1.14) | 1.19 (0.51, 2.77) | 1.46 (0.55, 3.89) | 1.10 (0.81, 1.50) | 0.5494 | ||
| Female | 4378 | 160 | 0.35 (0.11, 1.16) | 0.46 (0.18, 1.17) | 1.28 (0.65, 2.50) | 0.95 (0.74, 1.23) | 0.7151 | ||
| 51+ | All | 3927 | 656 | 0.86 (0.61, 1.23) | 0.65 (0.37, 1.14) | 0.99 (0.68, 1.44) | 0.95 (0.85, 1.08) | 0.4396 | |
| Male | 1862 | 384 | 0.72 (0.38, 1.36) | 0.28 (0.13, 0.56) | 1.01 (0.56, 1.81) | 0.84 (0.68, 1.03) | 0.0884 | ||
| Female | 2065 | 272 | 1.06 (0.69, 1.63) | 0.95 (0.48, 1.88) | 1.24 (0.78, 1.97) | 1.06 (0.91, 1.22) | 0.4677 | ||
| 19+ | All | 12,438 | 978 | 0.70 (0.49, 0.99) | 0.72 (0.49, 1.06) | 1.32 (0.94, 1.85) | 1.00 (0.89, 1.13) | 0.9755 | |
| Male | 5995 | 546 | 0.61 (0.37, 1.02) | 0.55 (0.32, 0.94) | 1.50 (0.74, 3.05) | 0.98 (0.77, 1.24) | 0.8547 | ||
| Female | 6443 | 432 | 0.83 (0.52, 1.34) | 0.81 (0.52, 1.26) | 1.15 (0.81, 1.65) | 1.00 (0.89, 1.12) | 0.9777 | ||
| Saccharin (mg) | 19–50 | All | 8511 | 322 | 1.09 (0.51, 2.33) | 1.32 (0.68, 2.56) | 0.91 (0.50, 1.65) | 1.03 (0.87, 1.23) | 0.7394 |
| Male | 4133 | 162 | 0.69 (0.20, 2.39) | 2.29 (1.12, 4.66) | 0.50 (0.13, 1.85) | 1.07 (0.82, 1.40 | 0.6116 | ||
| Female | 4378 | 160 | 1.48 (0.60, 3.68) | 0.75 (0.36, 1.54) | 1.03 (0.45, 2.37) | 0.98 (0.78, 1.24) | 0.8741 | ||
| 51+ | All | 3927 | 656 | 0.90 (0.57, 1.43) | 0.87 (0.59, 1.29) | 0.77 (0.47, 1.25) | 0.92 (0.81, 1.05 | 0.2201 | |
| Male | 1862 | 384 | 1.26 (0.80, 1.97) | 0.55 (0.24, 1.25) | 0.51 (0.24, 1.05) | 0.81 (0.69, 0.96) | 0.0150 | ||
| Female | 2065 | 272 | 0.73 (0.39, 1.36) | 0.90 (0.48, 1.71) | 1.20 (0.75, 1.91) | 1.02 (0.86, 1.20) | 0.8433 | ||
| 19+ | All | 12,438 | 978 | 1.11 (0.77, 1.59) | 0.96 (0.61, 1.51) | 0.84 (0.57, 1.25) | 0.96 (0.86, 1.08) | 0.5084 | |
| Male | 5995 | 546 | 1.03 (0.71, 1.50) | 1.14 (0.57, 2.28) | 0.63 (0.33, 1.20) | 0.93 (0.79, 1.10) | 0.4115 | ||
| Female | 6443 | 432 | 1.07 (0.60, 1.90) | 0.90 (0.57, 1.43) | 0.98 (0.63, 1.53) | 0.99 (0.86, 1.12) | 0.8180 | ||
| Age | Gender | n | Event n | Tertile 1 | Tertile 2 | Tertile 3 | Group Trend | |
|---|---|---|---|---|---|---|---|---|
| HR (LCL, UCL) | HR (LCL, UCL) | HR (LCL, UCL) | Beta (LCL, UCL) | p | ||||
| 19–50 | All | 8511 | 322 | 0.75 (0.37, 1.49) | 0.83 (0.44, 1.56) | 1.29 (0.77, 2.16) | 1.03 (0.87, 1.22) | 0.7328 |
| Male | 4133 | 162 | 0.34 (0.11, 1.12) | 1.46 (0.69, 3.08) | 0.86 (0.25, 3.02) | 1.01 (0.75, 1.37) | 0.9330 | |
| Female | 4378 | 160 | 1.32 (0.61, 2.85) | 0.51 (0.24, 1.10) | 1.26 (0.62, 2.54) | 0.98 (0.79, 1.23) | 0.8746 | |
| 51+ | All | 3927 | 656 | 0.95 (0.68, 1.31) | 0.80 (0.58, 1.08) | 0.95 (0.19, 1.50) | 0.94 (0.84, 1.06) | 0.3349 |
| Male | 1862 | 384 | 0.86 (0.57, 1.31) | 0.64 (0.36, 1.16) | 0.78 (0.40, 1.53) | 0.87 (0.73, 1.03) | 0.0926 | |
| Female | 2065 | 272 | 1.02 (0.59, 1.75) | 0.93 (0.63, 1.38) | 1.20 (0.70, 2.05) | 1.02 (0.88, 1.18) | 0.8492 | |
| 19+ | All | 12,438 | 978 | 0.99 (0.72, 1.36) | 0.73 (0.52, 1.03) | 1.16 (0.85, 1.57) | 0.98 (0.89, 1.09) | 0.6871 |
| Male | 5995 | 546 | 0.67 (0.45, 1.00) | 0.86 (0.50, 1.49) | 1.07 (0.54, 2.11) | 0.96 (0.79, 1.16) | 0.6555 | |
| Female | 6443 | 432 | 1.17 (0.68, 1.98) | 0.80 (0.56, 1.14) | 1.16 (0.77, 1.75) | 1.00 (0.89, 1.13) | 0.9817 | |
| Age | Gender | n | Event n | Tertile 1 | Tertile 2 | Tertile 3 | Group Trend | |
|---|---|---|---|---|---|---|---|---|
| HR (LCL, UCL) | HR (LCL, UCL) | HR (LCL, UCL) | Beta (LCL, UCL) | p | ||||
| 19–50 | All | 31,565 | 458 | 0.61 (0.33, 1.13) | 0.68 (0.40, 1.16) | 0.89 (0.53, 1.51) | 0.91 (0.77, 1.08) | 0.2791 |
| Male | 16,057 | 232 | 0.29 (0.10, 0.84) | 1.22 (0.65, 2.28) | 0.63 (0.21, 1.89) | 0.92 (0.71, 1.19) | 0.5133 | |
| Female | 15,508 | 226 | 0.99 (0.50, 1.97) | 0.38 (0.19, 0.78) | 0.86 (0.42, 1.80) | 0.86 (0.68, 1.10) | 0.2309 | |
| 51+ | All | 16,499 | 1332 | 0.84 (0.67, 1.06) | 0.84 (0.67, 1.06) | 0.77 (0.57, 1.05) | 0.91 (0.84, 1.00) | 0.0446 |
| Male | 7753 | 793 | 0.81 (0.57, 1.14) | 0.65 (0.45, 0.93) | 0.74 (0.46, 1.21) | 0.87 (0.76, 0.99) | 0.0352 | |
| Female | 8746 | 539 | 0.89 (0.65, 1.22) | 0.99 (0.71, 1.37) | 0.95 (0.61, 1.47) | 0.98 (0.53, 1.51) | 0.7680 | |
| 19+ | All | 48,064 | 1790 | 0.81 (0.65, 1.01) | 0.79 (0.63, 0.99) | 0.85 (0.64, 1.11) | 0.92 (0.88, 1.10) | 0.0382 |
| Male | 23,810 | 1025 | 0.68 (0.50, 0.91) | 0.75 (0.53, 1.07) | 0.85 (0.54, 1.34) | 0.90 (0.79 1.02) | 0.1010 | |
| Female | 24,254 | 765 | 0.91 (0.64, 1.29) | 0.87 (0.64, 1.18) | 0.82 (0.54, 1.23) | 0.93 (0.83, 1.05) | 0.2436 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fulgoni, V.L., III; Drewnowski, A. No Association between Low-Calorie Sweetener (LCS) Use and Overall Cancer Risk in the Nationally Representative Database in the US: Analyses of NHANES 1988–2018 Data and 2019 Public-Use Linked Mortality Files. Nutrients 2022, 14, 4957. https://doi.org/10.3390/nu14234957
Fulgoni VL III, Drewnowski A. No Association between Low-Calorie Sweetener (LCS) Use and Overall Cancer Risk in the Nationally Representative Database in the US: Analyses of NHANES 1988–2018 Data and 2019 Public-Use Linked Mortality Files. Nutrients. 2022; 14(23):4957. https://doi.org/10.3390/nu14234957
Chicago/Turabian StyleFulgoni, Victor L., III, and Adam Drewnowski. 2022. "No Association between Low-Calorie Sweetener (LCS) Use and Overall Cancer Risk in the Nationally Representative Database in the US: Analyses of NHANES 1988–2018 Data and 2019 Public-Use Linked Mortality Files" Nutrients 14, no. 23: 4957. https://doi.org/10.3390/nu14234957
APA StyleFulgoni, V. L., III, & Drewnowski, A. (2022). No Association between Low-Calorie Sweetener (LCS) Use and Overall Cancer Risk in the Nationally Representative Database in the US: Analyses of NHANES 1988–2018 Data and 2019 Public-Use Linked Mortality Files. Nutrients, 14(23), 4957. https://doi.org/10.3390/nu14234957